
Abstract
Based on policy analysis and individual interviews, the author analyzes the care workers’ precarious situations in home-based elder care in Slovenia, a post-socialist, European Union country characterized by a rapidly aging population and delays in adapting a long-term care system to this new social risk. Employment and quasi-employment positions which coexist in home-based care can be sorted along two continuums: between public and market service; between formal and informal work. The author argues that working conditions in home-based care differ according to the position of the care worker on these two continuums, that is, being employed in public services, being self-employed, working in informal care markets, holding a status of family assistant, or being an informal family caregiver. Although the working conditions in public services are deteriorating, the analysis shows that precarity is more severe in market and informal care, while formalization and socialization of care bring about less precarious conditions.
Introduction
Studies1–3 show that current changes in social policies in the European Union (EU), which have developed in response to new social risks related to the aging of the population follow the logic of deinstitutionalization of care for the elderly and the foregrounding of home-based care in order to reduce public costs. This is shown in the policies of a reduction in the range of public services and promotion of market services, which is accompanied by cash-for-care benefits 4 and the promotion of services that do not replace but only complement informal family care. With the aim of reducing informal care markets and creating new employments for hard-to-employ groups, these policies are accompanied by various public subsidies, such as voucher schemes, tax relief, and incentives for the purchase of services. As such, there is a growing trend toward a mixed service economy, the growth of commercial markets with the concept of “small-entrepreneurialism” and the globalization of care work through determining the range of work permits available for immigrant care workers. Critical studies estimate that such arrangements have caused the greater deregulation and precarization of care work.5,6 More specifically, as argued in this article, these policies structure home-based care as a markedly fragmented work field, involving coexistence and competition among various work arrangements, which bind care workers to various extents and modes of precarization. This article analyzes how fragmentation and precarization of home-based care work has been shaped by elderly care policies and experienced by care workers in Slovenia, an Eastern European country with one of the fastest aging populations in Europe and delays in adapting the long-term care system to this new social risk. As shown by recent studies2,7,8 in Eastern European countries, despite considerable differences among them, are neglecting elder-care policies, lagging behind in organization of home-based care services and have in common a high poverty rate of the elderly as a consequence of the syndrome of low pensions. 9 All these conditions impact on working conditions in home-based care. Research presented in this article points to the two dimensions of segmentation of home-based care in Slovenia: (1) According to the degree of service marketization, where work can proceed as a public, a public/private, or a completely market service; (2) According to the degree of the formalization of care workers’ status, where work can be formalized by a written contract in the employment status; or the care worker holds the hybrid status of a family assistant, or works informally without a contract, either on the informal market or as an unpaid family caregiver. The analysis stems from the thesis that while working conditions in this field are always precarious, the degree of precarization varies in range and form according to the position of the caregiver in these two dimensions. In the following, we first present the theoretical and methodological framework; next the socioeconomic situation and elder-care system in Slovenia are outlined; that is followed by an analysis of various statuses and the kinds of precarization that appear in home-based care; finally, the findings are discussed from the perspective of their consequences for the studies of precarization of work and the social organization of home-based care.
Theoretical Framework: Troubling (de)Familization of Care
The theoretical framework of the analysis is inspired by the feminist reflection of social policies, in particular the policies of (de)familization and commodification of care, with the assumption that working conditions in home-based care are strongly influenced by the ways in which the state structures the system of care through social policies.10–12 Familialistic policies presume the traditional family model of industrial capitalism and establish the importance of the informal unpaid work of family members, mostly women, in care provision. Because of the shift in family and employment patterns toward the dual-earner model in Europe from the 1970s on and because of gender equality politics framing the equality of women as equal participation in the labor market, a need for defamilization of care occurs. Consequently, a considerable proportion of care has to be provided by either the state or the market.13,14 Defamilialistic policies aim to unburden families/women of informal unpaid care by providing public services or cofinancing market mechanisms. Defamilization of care through its socialization by providing universal public services presupposes the formalization and commodification of care work—formerly unpaid informal care in the family is transformed into paid formal employment in care services—while the care itself gains the status of a social right and is not fully commodified but is (depending on the regulations of eligibility for services) publicly subsidized for users. On the other hand, with defamilization of care through its marketization by promoting financial benefits (i.e., cash-for-care benefits) over public service organization, work as well as care services become commodified. 15 Policy measures favoring the state’s provision of financial benefits support private solutions for organization of care, either in the form of familization where the financial benefits are directed to a family caregiver or in the form of marketization where care is bought on the formal or informal care markets. The relationship between financial benefits and organization of public services influences the level of (de)formalization and (de)professionalization of care. Research16–18 proved that favoring financial benefits over public services promotes the rise of informal care markets and migrant care work, because users tend to organize needed care with the financial resources available to them in the most economically efficient way. Particularly in the situation of long-term and intense care, they follow the logic of obtaining the maximum range of care services and a maximum of the care worker’s time for a minimum of money. Care in the informal market is cheaper than in the formal one, due to social contributions that the employers have to pay for the care workers who perform care through the formal market. However, the lines between formal and informal care work are becoming increasingly blurred. 19 On one hand, there is a growing flexibility in formal care services since the policies encourage the provision of care based on contracts other than employment contracts and not necessarily through labor organizations. For example, we are witnessing an expansion of the self-employed care workers, mini jobs, and the employment of (migrant) care workers directly by the families, either formally or, even more often, informally. 9 In these cases, we can talk about pseudo formal employments. On the other hand, social policies have introduced partial payment, limited labor rights, and a contractual relationship for informal family caregivers. In Slovenia, for example, it was carried out through the status of family assistant, which actually amounts to a policy of introducing payment for family care. Such cases involve hybrid positions between formal and informal care work, 3 with the key problem being low payments for care work and limited labor-related social rights. The policies of introducing pseudo and hybrid employments are actually compromise policies of defamilizing care: they enable the state to withdraw from the organization of public services, but for care workers this often means precarious working and living situations.
In contrast to Kalleberg’s approach to precariousness that takes job insecurity as the key dimension of precarious employment relations, 20 in this analysis, a wider approach has been adopted which considers several dimensions of job quality, such as wages, working time, job security, social security, and work/family balance in assessing the precariousness of particular work arrangements. This approach grasps precariousness beyond the destandardization of work thesis and involves multiple elements such as instability, lack of protection, insecurity, and social or economic vulnerability.21,22 It relates precariousness closely to social rights that are dependent on employment status. In a wider approach, precarious conditions are related to work that is low paid, with earnings that are at or below the poverty level; insecure, meaning that there is uncertainty regarding the continuity of employment, with a high risk of job loss; with minimal worker’s control, such that the worker, either individually or collectively, has no say about their working conditions, wages, or the pace of work; and unprotected, meaning that the work is not protected by law or collective agreements with respect to occupational safety and health, social protection, discrimination, or other rights provided to workers in more secure employment relationships. 23 Precariousness has been often linked to certain demographic characteristics of the workers—such as their gender, ethnicity/race, and citizenship status—which often predisposes them to be channeled into unfavorable jobs. 24 Numerous studies show that care work, and in particular home-based care, is a typical example of feminized, ethnicized, racialized, and labor-intensive work domains, with poor conditions and low payment.2,25,26
A Note on Sample and Methodology
Given that the purpose of the study not intended for statistical generalizations but for a qualitative exploration of the “how” and “why” of a phenomenon in a real-life context, the qualitative method was chosen as an approach which enables the study of hard-to-reach social phenomena which are not well covered in official statistics (i.e., work in the private sphere of households, family care, illicit work, migrant workers) by using smaller samples and to delve more deeply into the explanation of the phenomena. The collection of empirical material in this work was based on the analysis of policies and on individual semi-structured interviews. Policy analysis, a that can be positioned as a macro analysis, traces the ways how the state structures the national system of elderly care by shaping relationships between the different sectors of care (state, market, family), setting criteria of eligibility for services and financial benefits, defining professional standards and ways of financing services. It reveals the ways of (de)familization of care and what forms of care predominate (paid/unpaid, formal/informal). The macro analysis was confronted with a micro perspective of lived experiences of care workers that was acquired through the interviews carried out as part of the two research projects. In the research Care Work between Individualization, Socialization and Globalization (2015–2017), the sample consisted of forty-four care workers (in a variety of positions: informal family caregivers, family assistants, care workers in public and private organizations, self-employees, care workers in informal markets, including migrant care workers) and, to avoid one-sided information, eleven heads of private and public organizations that offer care services. In the research Perspectives for the Desegmentation of the Labor Market (2014–2016), the sample included eight care workers, two employers (a public service and a market one), and the Head of the Union of Social Carers. Both samples were constructed based on the policy analysis which provided the range of existing work arrangements in home-based care. The guiding rationale for selecting the respondents was to include diverse types of working arrangements. Respondents were largely women (only five were men), between forty-five and sixty-five years (two were thirty-nine and one was forty-one years), who had finished occupational or secondary school (only one held a university degree). Eight respondents were migrant care workers from countries of the former Yugoslavia, between thirty-six and forty-three years who had finished primary school. For recruiting respondents, the snowball and link-tracing methods were used. The workers were asked about their experiences with regard to working conditions and reasons for engaging in a certain form of work. In both projects, the interviews were carried out in 2015, and were recorded, transcribed, and coded. The coding items referred to the dimensions of job quality, such as wages, working time, job security, social security, work/family balance, and worker’s control over the work conditions. The analysis was focused on searching for similarities and differences in and between the different categories of care workers and in constant confrontation of the narratives with the policy framework.
Contextualization: The System of Elder Care in a Post-Socialist Context
Slovenia began its political and economic transition while still part of Yugoslavia in the late 1980s and accelerated the process after the secession in the early 1990s. In 2004, it joined the EU, and in 2010, it became a member of the Organisation for Economic Co-operation and Development. The socialist system’s legacy included the full employment of women and a comprehensive social protection system. The welfare system and its benefits were financed by obligatory contributions from employers, while the provision of services was dominated by a highly decentralized public sector. The system of self-management left the country with relatively open market arrangements and a relatively good level of economic development. Overall, and unlike in most other transitional countries, the social protection system managed to endure the transitional shock comparatively well, maintaining the vital income of the population facing new transition-related risks, and retaining one of the lowest risk-of-poverty rates in the EU. 9 However, Slovenia was hit hard by the 2008 economic crisis, due to its dependence on exports, and lost many of its comparative advantages. Despite the recent economic growth from 2014 on, according to the National Statistical Office data, 27 nowadays it is characterized by a relatively high unemployment rate (9.4 percent) and 13.9 percent of the risk-of-poverty rate, which for women aged fifty-nine years and older reaches 20.8 percent and is one of the highest in the EU. Neoliberal austerity policy of cutting public costs caused a considerable reduction of the social protection system and individualization of social risks. During the 2008 economic crises, destandardization of work became a salient public issue as the share of nonstandard employments, in particular fixed-term jobs and self-employments, reached 41 percent of all employees. Given that labor law provides for only limited social security and workers’ rights for the employed in such jobs compared to standard, that is, open-ended, full-time employments, these labor market developments were fully discussed within the framework of precarization of work.
Number of Employees and Users in Public Home-Based Care in the Period 1998–2015.
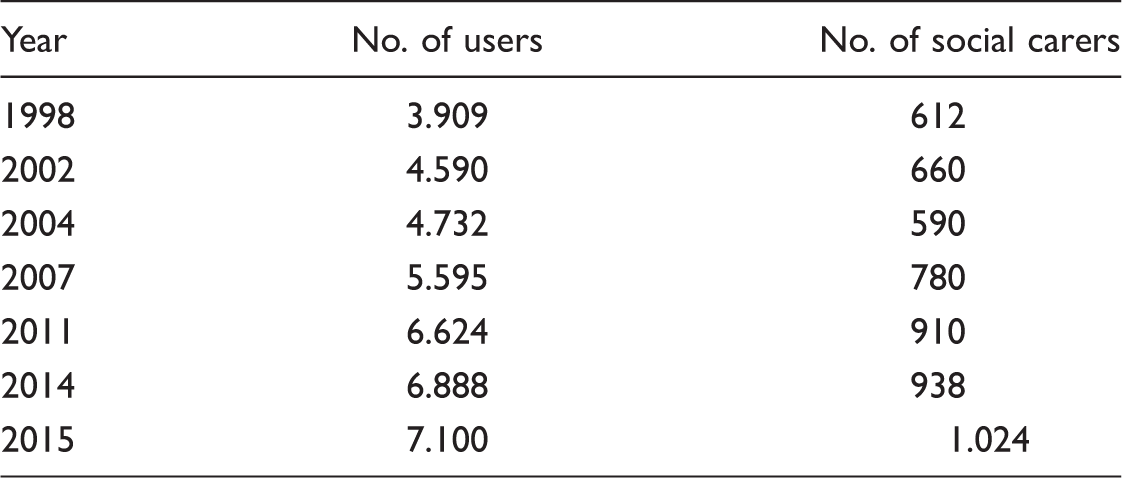
Source: IRSSV, Evaluation report of public home-based care service, 2015.
According to the traditional gender script, women in Slovenia vastly outnumber men in elderly care, however, given that women mostly work full-time, e family care is not able to compensate for insufficient public services. The state compensates for this with a scarce needs-tested cash-for-care allowance granted to the elderly by which they are expected to organize their own care either in the family or in the market. The familization of care, coupled with the high full-time employment rate of women and the cash-for-care provision, has led to the expansion of commercial and informal care markets.
Segmented Home-Based Care Services
In Slovenia, home-based care services are divided between the state and the market services, and between the formal and the informal services. Although formal care services can be provided by the state and market companies or, increasingly, by self-employed care workers, in the context of family and informal care markets, the same services acquire the status of semiformal or informal work.
In the next subsections this article first looks into the modes of precariousness seen in employment statuses within formal care, that is, in public and in the “legal” market services; then it addresses the modes of precarity seen in the hybrid or informal care statuses within the family and in informal markets.
Between the State and the Market Service
The state service of home-based care started to become established in the 1990s, when due to the high unemployment rate among older women, caused by transitional economic restructuring, this service began to be carried out as a form of active employment policy. From its very start, home-based elder care as a form of community work put care workers in a precarious situation in terms of payment and employment stability, as well as the lower standards of labor rights that apply for those employed within community work projects. Ten years later, the service was professionalized through the adoption of a set of standards of knowledge and skills that were needed by professional social caregivers. The public system of home-based care means that the municipality is responsible for the organization, accessibility and quality of services, and also for cofinancing 50 percent of the costs of these services, while the rest is paid by the users.
Annual evaluations of the public system of home-based care
30
show that
most social caregivers are employed in standard employment, involving an
open-ended (94.3 percent) and full-time contract (89.4 percent) with transport
between the users, coordination activities, and lunch break included in their
work time. This means that through the processes of professionalization and
formalization, care work in public services was gradually transformed from its
initial insecure employment to standard employment. The formal definition of
such service encompasses household help, assistance in maintaining personal
hygiene, and maintaining social contacts. However, the respondents in our study
emphasized that such work is highly demanding, as it includes field work and
work in private homes with the most vulnerable people, such as the bedridden,
the terminally and severely ill, and with their relatives. The work is performed
during weekends and holidays, and in split shifts. Such working hours prevent
the caregivers from balancing their professional and private lives. Lifting of
heavy physical loads is a daily activity. The care workers are responsible for
assessing the user’s need for further assistance from community nurses and
social services, and have to undertake additional training (e.g., to work with
people with dementia), carry out administrative duties, and receive regular
supervision. This shows that while social care requires a low educational level,
it involves physically difficult, complex, and responsible work. The care
workers, related union and employers noted the mismatch between the difficulty
of the work and the level of payment, since the collective agreement means that
this is a minimum wage profession. Although care workers in public service have
stable employment, they belong to the working poor. Workers report in interviews
that when ill they often do not take sick leave, because doing so would reduce
their already low income to a point at which they would not be able to cover
their monthly costs. In particular, workers in single parent families with
school-age children cannot cover all their monthly costs, such as paying for
their health insurance. As Darcy
f
(48, social carer) says: My gross salary is EUR 789.15 and I can’t survive on that. I get food
packages from Karitas. We use my daughter’s scholarship to pay the
bills … I’m very thrifty, the problem is heating, I usually borrow money
to pay for it, I’m always in debt. They got us smart phones and distributed stickers to the users. He has a
blue sticker that he sticks to a wooden thing. When I come to the user,
I hold my phone against it and it registers my arrival. And when I
leave, it registers my leaving. (Angelca, 50, public
agency)
Underpayment, intensification of work, nonstandard working hours, and lack of control over working conditions represent the key features of the precarity in public home-based care, and represent a continuation of the devaluing of traditionally female unpaid work. This situation also shows that even in terms of standard employment in the public sector, such work is being reorganized, intensified, prolonged, low paid, and sometimes even unpaid.
Since the public home-based care services only cover a small share of the needs,
a significant number of private initiatives have emerged on the market, which
however, is segmented by the care policies into private care providers holding
state concessions, and self-employed individuals with work permits. A private
care provider who is granted a state concession becomes part of the public care
services network, with 50 percent of the coverage costs coming from public
funds, thus representing a 50 percent subsidy for the users.
31
Those
employed by a private care provider holding a concession have the same working
conditions as the employees in public institutions. However, the number of
concessions is limited by the national program, and typically concessions are
obtained by large companies. Smaller private service providers mainly work as
self-employed individuals, and cannot compete with larger companies in tenders
for concessions, being thus limited to obtaining work licences. As such, the
costs of services offered by these providers are not subsidized by the state
from public funds, and are fully payable by the users, making the self-employed
caregivers uncompetitive with the concessionaires in terms of price. Considering
the low purchasing power of elderly people, this causes additional precarization
of the self-employed. They also face competition from the informal care market
providers who, by not paying taxes, can ask a lower price than that set by the
self-employed, who have to pay fixed monthly taxes regardless of their actual
work load and incomes. As a consequence, self-employed care workers in
interviews report that they are usually underemployed; their income is very
unpredictable, and they hardly earn a living in this job. As Maja (39,
self-employed) says: There’s a big crisis in the markets and I only have three hours a week
for now. A lot of people work unofficially. Mostly pensioners. I’m sure
they have low pensions, but with their low prices they’re crowding us
out of the market. After I pay my taxes, I’m in the
red. I come home and leave again, and then come back for a couple of hours in
between, and go out again in the evening. I also work all weekends. So
there’s no rhythm of going to work and then coming home and being with
your family.
Semiformal and Informal Forms of Home-Based Care
As the European model of social citizenship is based on formal and standard participation in the labor market, and the ensuing social rights, informal forms of work represent a high risk of precarization of life. With care work always being stretched between formal and informal work, the boundaries between formal and informal care set by care and employment policies are of vital importance with regard to providing access to full social citizenship for those who provide care. Social policies establish various mechanisms for the partial formalization of family care work, allowing care workers limited access to social rights compared to those related to employment status. In terms of childcare, an example of this is paid parental leave, and in elder care it is the status of family assistant.
Slovenia introduced this status in 2004. It represents the right of the
beneficiary of institutional care to choose instead a family assistant who
offers them care at home. To obtain this status, the family assistant, who is
usually a close female family member living with the care receiver, has to leave
the labor market. Although this status does not involve the establishment of a
working relationship as regulated under the labor law, the family assistant has
the right to receive a payment to the amount of the minimum wage, for the income
lost due to leaving the labor market. However, the payment of family assistant
is actually done by the care receivers with their cash-for-care transfers, while
the difference is covered by the municipality, which later recovers these funds
from any inheritance.
32
Interviews indicate the excessive workload of family
assistants, who provide 24/7 care which makes the assistants themselves
experience health problems, burnout, and social isolation. As witnessed by
Valentina (52, family assistant), who has cared for her bedridden mother for the
last ten years: My workday starts at 6 or 6.30 a.m. and ends at one or two at night. And
I sleep at my mother’s. I wake up twice or three times a night to change
her diapers, and if she feels bad, I quickly take her blood pressure,
sugar. I have to wake up.
As the status of family assistant has a narrower range of labor rights than
standard employment, it is defined as a semiformal or hybrid status.
3
On the other
hand, a family caregiver who performs the same work as unpaid labor, without
holding this formal status, is in the position of an informal family care
worker. The work of home care not provided by the state through public services
and, except for the well-offs, also not by the market because of the high prices
automatically fall to family members as informal unpaid care work, which
represents the invisible foundation of the welfare system, taken for granted and
considered to be outside the economy (see Figure 1). Our interviews show that
informal unpaid care work significantly contributes to the precarization of life
and the paid work of a family carer, in the form of physical, psychological,
social, and financial burdens. Family caregivers are mainly women, aged between
forty-five and sixty-five who take on informal care without any financial
compensation and none of the social rights related to their work that can be
extremely intensive (in terms of content) and extensive (in terms of time). As
described by Karla (65, family care-giver), who takes care of her
ninety-five-year-old mother: I’ve washed and ironed for her for about fifteen years now, and I’ve
cooked for her since I retired, which was seven years ago. But the fact
is that as she gets on, she needs more and more, every year more. Yeah,
everything that goes with daily care, everything one needs. Starting in
the morning, when she opens her eyes, I bandage her legs, get her up,
dress her, wash her, make her breakfast. Employment
arrangements in home-based care.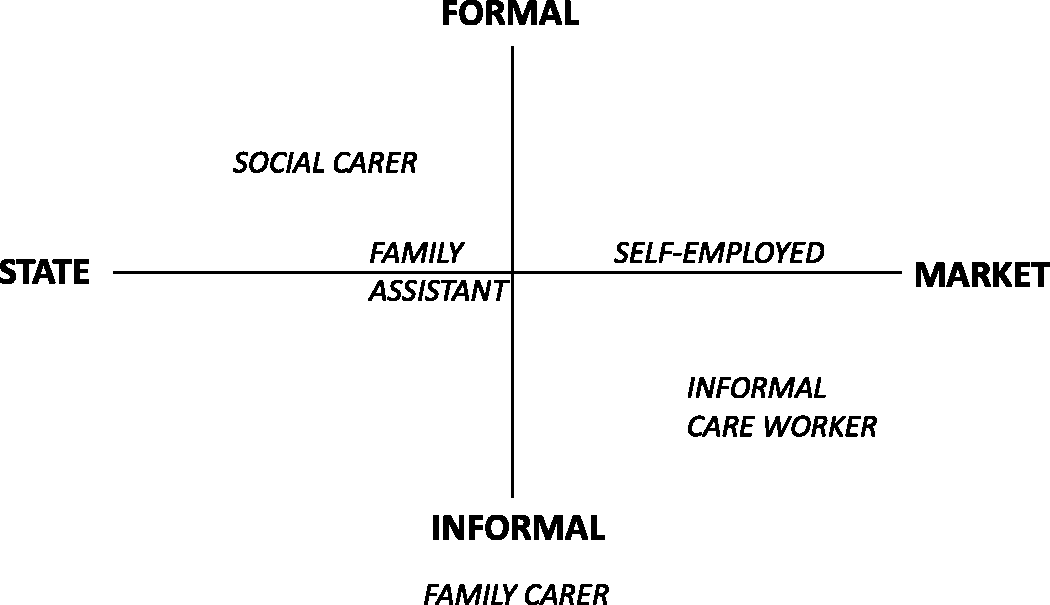
Another form of informal, but paid, home-based care is carrying out on informal care markets that enter at points where the state and its policies are missing. 34 Care workers on informal care markets are mostly not professionally trained, they work without a contract and get cash-in-hand payments. Because such workers waive their social security and labor rights, they can offer the lowest price in the market. As opposed to many EU countries, where home-based care is often provided by migrant care workers, in Slovenia and other Easter European countries, this form of care has been mainly performed by local unemployed women, working poor and poor pensioners (with migrant women accounting for a lower share than elsewhere), to whom informal care markets represent a survival strategy. 35 With the informal care market being extremely flexible, the situation of these care workers is particularly precarious. The interviews show that informal paid care workers perform a wide range of care activities, from intensive care to physical labor, cleaning and household chores. They may be hired for a couple of hours a day, while those providing intensive care are often hired as live-in care workers performing their duties on a 24/7 basis. Not only is such work illegal and criminalized, but the care workers are completely unprotected, having no labor rights or any social security with regard to their years of service, pension, and health insurance. We are thus faced with the paradox of the people that perform care themselves being completely excluded from social security.
Conclusion
The research results have implications for both, the studies of precarity and the organization of home-based care in Slovenia. In research and in politics, the precarization of labor, which in Slovenia is high and has been increasing, is considered exclusively within the framework of labor destandardization, in which the only criterion of precarization is the frequency of unstable, nonpermanent employments. However, the presented study shows that nonstandard employment is only the tip of the iceberg, as the precarization of work and life is also influenced by the level of income, workload and work intensity, the organization of work time, labor-related social rights, the possibilities of balancing work and family life and so forth. Including these elements in the analysis reveals how contemporary working conditions in some work fields and for some groups of workers are changing also when it comes to the so-called safe standard employment. Our study also shows that, in addition to the general reasons for precarization (such as globalization and the need for greater competitiveness with internal labor flexibilization, the characteristics of post-industrial service economy and so forth), different fields of work also have their own specific logic of generating precarity. This is why qualitative sectorial analyses or even analyses of individual organizations appear to be relevant for the development of concrete strategies of reducing precarity. Especially important seems to be an analysis of the interplay of labor market policies and specific sectorial policies that structure a sector since it is not only the labor market policies that cause precarization and can therefore also limit it. This study provides a concrete example of how, through the social policies that structure the social organization of elderly care, the state establishes the conditions for precarious situations of care workers in home-based care. Although their situations are precarious in all the presented positions, the degree of precariousness increases the closer the caregivers are to the market and the more they engage in informal care. In contrast, the more their care work is formalized and closer to the public service, the less their situation is precarious. This makes very clear the direction of any social and employment policies that aim to create quality employment is due to the aging population and is a considerably growing field of work. Following the example of most of the EU countries, it can be achieved by establishing a new source of financing long-term care in the form of mandatory insurance for long-term care. It would provide resources for the expansion of the public network of care services (a measure that was pointed out as urgent by numerous interviewees in our research), enabling the employees more secure and stable working conditions, and the users, who, as a rule, are in a vulnerable position, more affordable professionalized formal services. A greater extent and accessibility of public services would decrease the demand for the most precarious informal services in the informal economy and at the same time enable a greater defamilization of care, which is, among others, also the necessary condition for the equal participation of women in the labor market. However, the Act on Long-term Care has been in preparation in Slovenia for the last fifteen years—which clearly shows the lack of political will to tackle this problem.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was made possible by research grant of the Slovenian Research Agency who funded two fundamental research projects “Perspectives for the Desegmentation of the Labour Market” (2014–2016) and “Care Work Between Individualisation, Socialisation and Globalisation (2015–2017).”