
Abstract
For many women, house cleaning is an important way to participate in the labor market. In Brazil, there are 2 types of domestic workers: housekeepers have relatively secure employment and house cleaners are day laborers. The aim of this hypothesis-generating study was to describe the sociodemographic, occupational and health profile of a sample of domestic workers in Brazil. House cleaners received lower wages, had longer daily working hours and worked in a larger number of homes each week in comparison to housekeepers. About 51% of the domestic workers in this sample reported the use of pain medication and 34% reported spinal problems. Musculoskeletal symptoms were frequent in the lower back and upper limbs. Forty-seven percent reported high blood pressure. This study highlights the vulnerability of domestic workers, especially house cleaners, regarding workload, salary, and health conditions. Level of education is a contributing factor to this vulnerability.
Introduction
Historically, women have been assigned to household activities and childcare. Their work opportunities have been limited to services related to care and cleaning, which are occupations that offer lower wages and less social security than male-identified occupations.1,2
In high-income countries, the workforce in the cleaning sector is largely made up of immigrants and ethnic minorities, who receive low wages and tend to have a low level of schooling.3-7 In the United States, newly arrived immigrant women are commonly directed toward cleaning and other service occupations. In these jobs, they often work long periods without breaks and they are frequently exposed to harmful chemical agents.1,8
Cleaning work is also common in low- and middle-income countries in Latin America, where domestic workers account for 12% of the total active workforce. 9 A study carried out by the International Labor Organization in 117 countries indicated that Brazil is the country with the largest number of domestic workers in the world. 10 In Brazil, patriarchal culture and social inequality establish a complex dynamic, in which cleaning work is one of the most important options for the inclusion of women in the labor force. This is especially true for women with less education, migrant women and women of African descent.11,12
Pinto et al. 13 studied gender-related differences in work demands on Brazilian men and women from different social classes. The Brazilian Longitudinal Study of Adult Health (ELSA-Brazil) is the largest study of adult health ever conducted in Brazil. It studied public employees (8218 women and 6887 men), from 6 higher education and research institutions, the majority of whom had a high level of education. In this population, social position tended to be lower among women than men. 13 The study illustrated how the dynamics of work and family life are strongly maintained by gender relationships that involve different demands for men and women, 14 leading to a high prevalence of work–family conflict. 15 Around 80% of this highly educated population, employed by higher education and research institutions, reported having a monthly housekeeper, which was associated with healthier food habits among men, reinforcing that in a society with marked gender inequality, men depend on women to perform household chores, especially preparing meals. 15
Social security for domestic workers was ensured in Brazil only in 2015 through Complementary Law n° 150/2015. 16 This law established that the provision of services for more than 2 days a week in the same residence corresponds to a labor relationship that needs to be formalized, ensuring worker rights and payment of the monthly minimum wage. Other benefits include Severance Indemnity Fund, payment for overtime, vacations, no reduction in salary, lunch break, weekly rest, additional payment for working night shifts, prior notice in the event of dismissal. 16 However, this law does not apply to workers who work at a different home each day. Those workers still lack rights.
These legal changes have increased costs to employers, who have increasingly opted for independent, occasional, nonemployed service providers: the house cleaners. These domestic workers receive payment by the day at prices determined by the informal market. 17 If they want sickness benefits or social security retirement, they must pay by themselves, which is not realistic given their low wages. Many who work informally can’t afford to pay for these benefits.
The number of informal domestic workers (house cleaners) has increased since these legal changes. Another contributor to this increase has been the economic crisis that occurred in the last decade in Brazil. House cleaners seek clients through a network of referrals, companies, cooperatives, and online applications (apps). Often, companies that use apps to offer daily cleaning services do not formally hire the workers. This phenomenon is known as the “uberization” of work, 18 resulting in processes with new forms of control, management, and work organization, promoting work “flexibility” and placing the worker as an available subordinate self-manager with no labor rights.
Hence, the role of housekeeper and house cleaners are different in the household and in society. Housekeepers develop long-term relationships with their employers. Studies about these relationships in Brazil showed that domestic workers perceive that their relationship with the employers are permeated by feelings of slavery, discrimination, not belonging to the family, resentment, and symbolic distances,19,20 and these feelings are more frequent among house cleaners than among housekeepers.
Qualitative research with domestic workers has found that working relationships with employers are associated with ambiguous feelings. While they see themselves as employees, the proximity to the family, sometimes, brings an intimacy that is contradictory. In addition to legal issues relating to low wages and unpaid overtime, they have informed researchers about their experience of intense resentment and humiliation. 19 On the other hand, house cleaners for daily pay usually do not have long-term contracts, so the emotional demands might be lower than occur for the housekeepers. 20
Research on domestic cleaning has been limited, due to the lack of recognition and the devaluation of the occupation as well as the difficulty experienced by researchers in gaining access to the domestic work environment. Cleaning services have been the object of study, especially in Europe, the United States, Canada, New Zealand, Taiwan, Australia, Singapore, India, and Brazil. However, these studies were carried out with workers at hospitals or companies that offer specialized cleaning services. Studies found that such workers have cardiovascular diseases, 21 breathing problems, 22 dermatological diseases, 23 mental health problems, 24 musculoskeletal disorders,25-27 skin disorders, risk of infection. 28 Although the cited studies showed high prevalence of some diseases among cleaners, the evidence of association between cleaning work was demonstrated only for respiratory and dermatologic diseases, and musculoskeletal disorders. 28
Despite their large numbers, housekeepers and house cleaners have been overlooked by social and scientific research but are heavy users of physical rehabilitation services in Brazil, accounting for 22.4% of the total number of workers. 29 The work environment of cleaners is diverse and includes institutions, hospitals, schools, and companies. However, domestic cleaners work in a very intimate, employer-controlled environment, which may explain why little is known about their working conditions. Housekeepers and house cleaners perform housework that is similar in nature. However, the work differs in some important respects. House cleaners more often than housekeepers are hired to perform functions such as bathroom cleaning and window washing. By law, housekeepers have greater access to social security.
The aim of the present study was to describe the sociodemographic and occupational profile as well as the prevalence of health problems and musculoskeletal symptoms in Brazilian housekeepers and house cleaners, as well as to suggest hypotheses for future research.
Methods
Type of Study
This it as a hypothesis-generating study that uses a convenience sampling method reported in accordance with the recommendations of the Strengthening the Reporting of Observational studies in Epidemiology initiative. 30 Because this study uses a convenience sample, findings must be described as preliminary. Hypotheses generated by this study must be tested by larger studies using probabilistic sampling. The study was conducted in a municipality in the state of São Paulo, Brazil, in 2018, after having received approval from the Research Ethics Committee of the Federal University of São Carlos (certificate number: 79234617.0.0000.5504).
Participants and Setting
The sample was selected from workers in a municipality in the state of São Paulo, Brazil. To invite the domestic workers, the lead researcher contacted social workers from the primary care services and used social media to reach a greater number of participants. The potential participants (n = 185) were contacted by telephone to explain the purpose of the study. Those who met the inclusion criteria were invited to participate. At least 2 attempts were made to contact each potential participant to avoid bias in recruiting participants.
The inclusion criteria were performing paid work as a housekeeper or house cleaner, being female, aged 18 to 60 years and having a work routine of at least 20 h a week. Participants who performed other paid professional activities in addition to cleaning work were not included. After the screening process, 49 individuals were included in the study, 20 of whom were housekeepers and 29 were house cleaners.
Data Collection Instruments
The participants answered a standardized questionnaire developed by the researchers, addressing personal information (date of birth, education level, skin color/ethnicity, marital status, and number of children), occupational characteristics (work history, job seniority, first job, current job, work routine, breaks, work and rest activities, such as combing the hair which exposes the upper limb to a biomechanically stressful situation), health-related characteristics (diagnosed diseases, musculoskeletal symptoms, use of medications), and nonoccupational risk factors (body weight and height, smoking habit, use of tobacco and alcohol, and physical activity during leisure time). 31 This questionnaire was structured and comprehensive, addressing specific issues such as what tasks were performed at work and about the work routines.
The body mass index (BMI) was calculated, body mass in kilograms divided by the square of height in meters (kg/m2), 32 from self-reported information obtained with the questionnaires. The BMI categories recommended by the World Health Organization were used: underweight (< 18.5 kg/m2), adequate weight (≥ 18.5 and <25 kg/m2), overweight (≥ 25 and <30 kg/m2), and obesity (≥30 kg/m2). 33
The age at which the participants started working was classified as above or below 16 years old, as Brazilian legislation allows paid work beginning at this age. Individuals between 14 and 16 years of age can only work as an underage apprentice. 34 First job was divided into 2 categories: domestic employment (housekeeper, nanny maid, or house cleaner) and other (farm work, commercial or industrial work).
Data Analysis
The data were analyzed using the SPSS program (version 22.0). Descriptive analysis of the data was performed, including mean, standard deviation, absolute and relative frequencies for all variables, including the sociodemographic, economic, work and health profile of these participants. The nonparametric chi-square test (χ2) of independence was used for comparisons between groups regarding categorical variables.
Results
Table 1 displays the sociodemographic data of the sample. House cleaners were younger than housekeepers. Educational level was low in both groups. The majority completed only a primary school education. Most workers were White, married, had children and/or began working before 16 years of age, performing housework (Table 1). Housekeepers reported that they started working on average at 16.2 (SD 4.9) years, ranging from 7 to 27 years; and house cleaners started at a mean age of 15.4 (SD 5.6) ranging from 8 to 36 years. Although there is great variability in the age at which housekeepers and house cleaners started working, both groups have a history of child labor.
Sociodemographic Data of Housekeepers and House Cleaners. Data Presented as n (%), Unless Otherwise Stated.
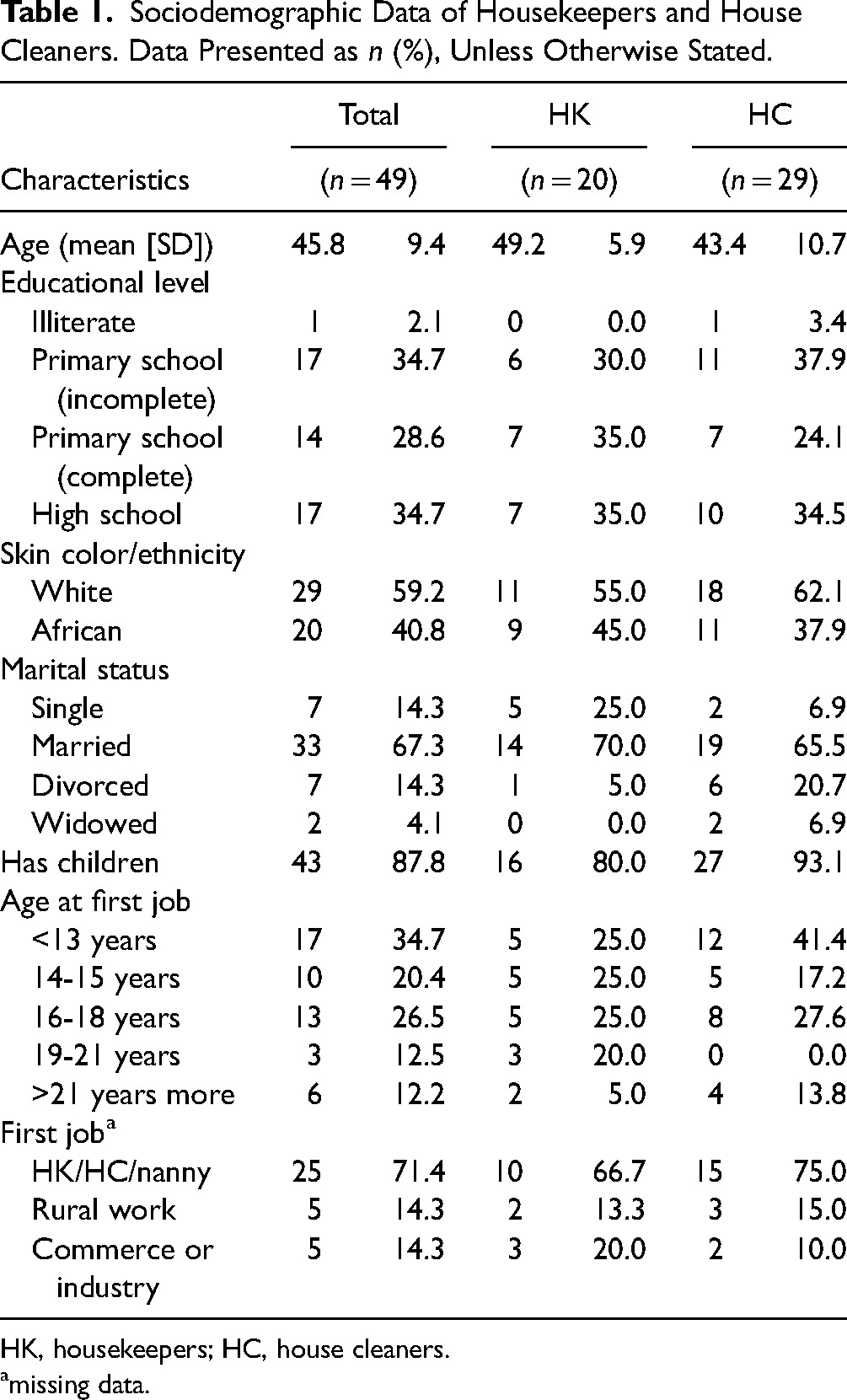
HK, housekeepers; HC, house cleaners.
missing data.
Table 2 displays the occupational characteristics of the sample. The average number of hours worked each day was 8.5. The average number of workdays per week was 4.1 and the average number of hours worked per week was 34.5. Most workers reported income between 100% and 200% of the minimum wage. House cleaners had a lower income, lower weekly working hours, more work hours per workday and worked in more homes compared to housekeepers. Bus was the main means of commuting in both groups, but most housekeepers received bus fare from the employer. More than half of the study participants had up to 30 min for lunch, but almost three-fourth did not take rest breaks lasting more than 10 min during the workday. All workers cleaned bathrooms, swept floors, and dusted furniture. Housekeepers cooked and did the laundry more often than house cleaners. House cleaners cleaned windows more frequently than housekeepers (Table 2). Most of the participants perform unpaid domestic work at their own homes. Only 55% of the housekeepers and 31% of the house cleaners have support from other family members in performing unpaid housework.
Occupational Characteristics of Domestic Workers. Data Presented as n (%), Unless Otherwise Stated.

HK = housekeepers; HC = house cleaners; MMW: monthly minimum wage = R$ 1045
missing data.
Table 3 displays the health problems reported by the participants. High blood pressure and spinal problems were the most prevalent health conditions among those asked about. The survey was not comprehensive in that it did not ask about some conditions, such as cancer. The survey included an “other” option. No one chose to respond to it. There is no way of knowing whether this means that none of the respondents had any other condition or whether they simply did not report the “other” conditions that they had. The use of pain medication was reported by 51% of the sample, and do not practicing physical activity in the leisure time was reported by 79%.
Health Problems Reported by Domestic Workers. Data Presented as n (%).

Table 4 displays the nonoccupational risk factors reported by the participants. Most participants were overweight or obese, but few reported using tobacco and/or alcohol. Most do not engage in physical activity during leisure time.
Nonoccupational Risk Factors Reported by Domestic Workers. Data Presented as n (%).

HK = housekeepers; HC = house cleaners.
missing data.
Table 5 displays data related to musculoskeletal symptoms. The most affected regions were the lower back and upper limbs. Workers were asked whether they experienced symptoms while performing specific activities. The prevalence of lower back symptoms was high when using a squeegee, sweeping, ironing and resting outside of work. Upper limbs symptoms were related to combing the hair, cleaning windows, wringing clothes, and hanging clothes. Lower limbs symptoms were related to ironing and resting outside of work. House cleaners reported more wrist symptoms related to washing activities and fewer symptoms in the lower back related to ironing in comparison to housekeepers.
Musculoskeletal Symptoms When Performing Cleaning Activities, Self-Care and Resting According to Body Region. Data Presented as n (%).
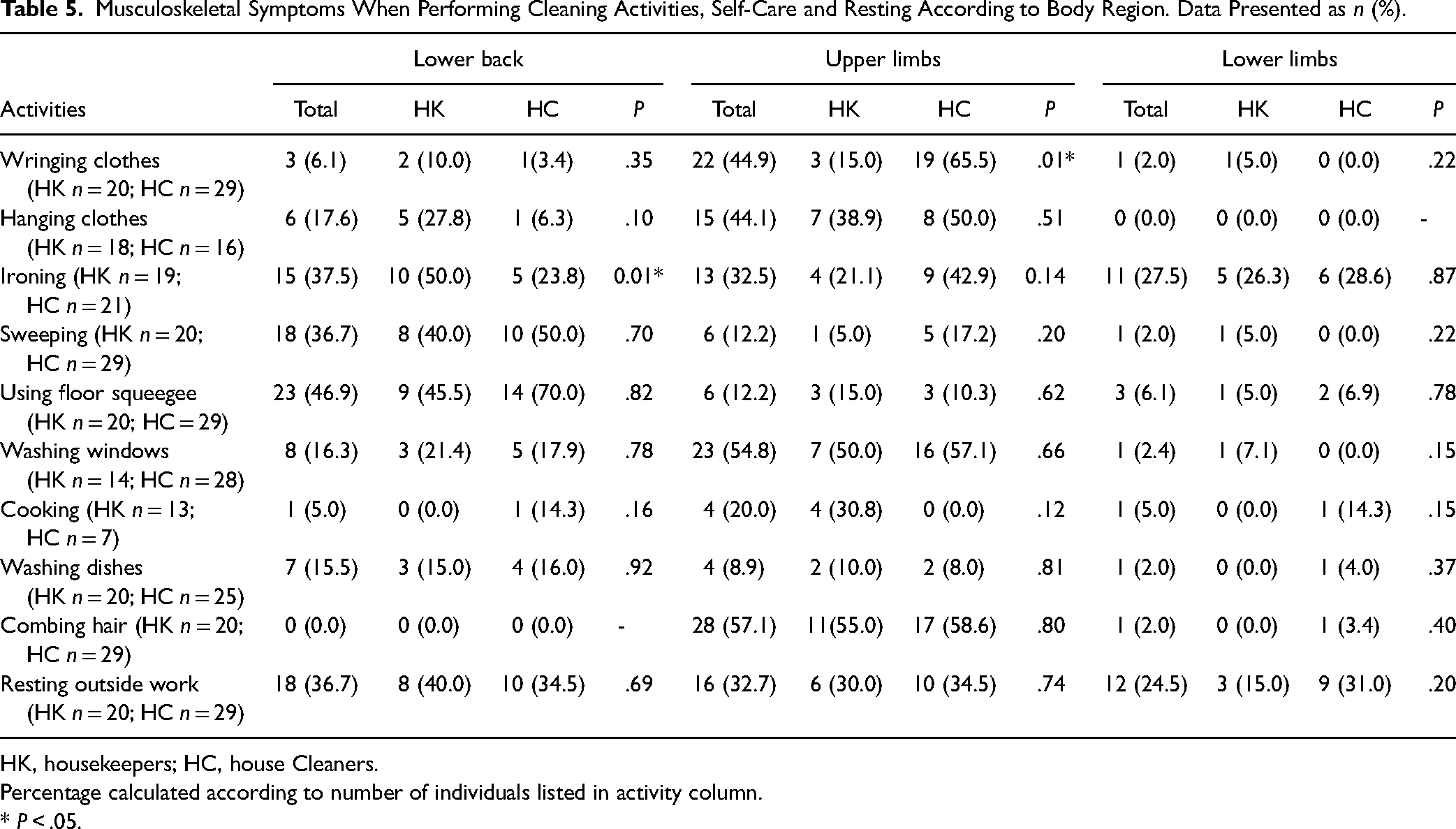
HK, housekeepers; HC, house Cleaners.
Percentage calculated according to number of individuals listed in activity column.
* P < .05.
Discussion
The present study described the sociodemographic, occupational and health profile of a convenience sample of Brazilian housekeepers and house cleaners. Possible explanations are offered for the results obtained from this sample. Such explanations are, in effect hypotheses to be tested in a study with a larger probabilistic sample. This caveat is explicitly stated frequently below. It is intended even where not stated. Workers in this convenience sample had a low educational level, started working early and most had started in domestic service positions similar to the ones in which they still worked.
Ergonomic Risk Factors and Musculoskeletal Pain
More than one-third of housekeepers and over 60% of house cleaners reported use of pain medication. The body region most affected was the lower back. Around 45% of housekeepers reported back problems, compared to only 28% of house cleaners. If verified by a larger, probabilistic sample, this could, in part, be because housekeepers were older on average, but it is possible that the greater weekly workload of housekeepers contributes as well. Previous studies have reported these health conditions as being frequent among domestic workers.17,35
Although housekeepers and house cleaners perform similar activities, differences were found in the activity-related symptoms: house cleaners reported wrist symptoms related to washing activities and housekeepers reported symptoms in the lower back related to ironing. Housekeepers did more laundry and cooked more than house cleaners. House cleaners had a greater focus on cleaning-related activities, such as washing windows. The most strenuous household chores include cleaning the kitchen, the bathroom, scrubbing and making the beds. 7 Differences in activities can lead to differences in health outcomes, as house cleaners performed strenuous activities more often during the week because their chores did not have as much variability as housekeepers.
Lower back symptoms were highly prevalent in the sample and mainly related to ironing, sweeping, and using a floor squeegee. Housekeepers who did ironing reported lower back symptoms at twice the rate of house cleaners who did ironing. If verified by a larger, probabilistic sample, this finding may be related to the work organization and personal factors. Housekeepers, in general, work in family houses with more people (and more clothes) than the house cleaners, probably increasing the time spent in this activity. Besides this, in our sample, housekeepers are older than house cleaners and may report more low back pain due to degenerative adaptations. House cleaners have a considerably higher rate of lower back symptoms associated with using the floor squeegee than housekeepers. This finding may be related to the physical effort during work as house cleaners’ work in each house once or twice a week, and housekeepers work three to 5 times a week. Therefore, we hypothesize that house cleaners exert greater physical effort to clean the floor because the degree of dirt may be greater. Future research could investigate whether house cleaners work in dirtier homes on average.
Upper limbs and lower back symptoms in cleaners have been reported in previous studies.36-38 An investigation carried out with school cleaners in China also indicated a high frequency of musculoskeletal symptoms (in the shoulder, elbow, and lower back). 25 Likewise, Naik and Khan 26 identified high frequency of injuries in the upper limbs and lower back among Indian cleaners. Recent studies show that the use of household appliances, such as an upright vacuum cleaner is physically intense work, and can affect the upper limbs. 37 The analyses of different types of vacuum cleaners showed that the effects on the musculoskeletal system depends on the weight, motion pattern, and floor type. 38 The static vertical load acting on the handle generates elbow flexion and shoulder flexion moments to maintain the height of the handle and continue the back-and-forth vacuuming motions. The greater demands for elbow flexion and shoulder flexion moments resulted in the significantly greater muscular loads of the involved muscles. 39
The present study also described symptoms during rest and self-care activities. House cleaners had pain in the lower limbs when resting outside work at twice the rate of housekeepers. This finding may be related to the duration of the workday, as house cleaners spent around 9 hr per day working, mainly in a standing position. Reports of shoulder pain during resting time were highly prevalent in both groups. The prevalence of lower back symptoms at rest was also high in both groups.
Excessive workload is another important issue in this group of workers. Although the house cleaners in our sample had a lower weekly workload, they worked more hours on each workday. Their work intensity may be greater, as they cannot distribute the volume of tasks over the course of several days. Despite being younger than housekeepers, house cleaners used analgesics at twice the rate. It is possible that their longer workdays may explain this result.
Workload and Blood Pressure
Sixty percent of housekeepers reported hypertension. This was over 50% greater than the fraction of house cleaners reporting this condition. In addition, about one-third of house cleaners and 45% of housekeepers reported use of blood pressure medication. It is possible that the higher rates of hypertension and use of medication among house keepers are due to their higher average age and/or their high levels of occupational physical activity in this sample. 2 The relationship between cardiovascular events, psychosocial aspects, and excessive workload has also been described in the literature.18,35,40-42 Occupational physical activity may elevate 24 hr blood pressure and heart frequency when the recovery time is not sufficient due to organizational and psychosocial constraints. Continuous elevated cardiovascular workload can be associated with elevated risk of cardiovascular events. 21 Hypertension puts this population at risk of noncommunicable diseases, as do nonoccupational risk factors, such as obesity and not practicing physical activity during leisure time.
Impact of Education and Employment Opportunities
The socioeconomic profile of domestic workers may reflect limited employment opportunities for women with low schooling and income. 2 In Brazil, about 54% of all women aged 35 to 54 had completed high school. Among White women, this number rises to 64% and for Black women, it drops to 46%. 43
The age at which Brazilians graduate high school is between 17 and 18 years old. Many study participants started working at a younger age. In our sample, the proportion of women who completed high school (35%) was similar to the national data (34%). Among our participants, there was little difference in high school completion by race. However, when stratified by age, younger women have managed to achieve better levels of education. Data from 2019 showed that 25.1% of women aged between 25 and 34 completed high school in Brazil. These values drop to 24.4% in the 35 to 44 age group; 19.4% in the 45 to 54 age group; 15.5% in the age group between 55 and 64 years old and 9.5% in women over 65 years old. 43 If this result holds true for a larger probabilistic sample, it would likely be due to recent public policies that expanded access to education.
The early age at which participants started working in paid domestic work and their continued work in this occupation may be related to the low educational level of the group. In a vicious cycle, girls are sent to work at a young age to help support their socially vulnerable families. They drop out of school, which limits their work opportunities. Hence, they remain in domestic work.
The average age in our sample, above 46 years, is consistent with data from the Continuous National Household Sample Survey, which showed that 78% of the domestic workers have between 30 and 59 years. 44 The recent expansion of access to education has provided younger people with opportunities in the labor market that were not available to those over 40 when they were younger. However, the lower average age of house cleaners in our sample may, if confirmed by a study using a probabilistic sample, be explained by multiple factors. Two of these may include the fact that the house cleaner category emerged as a work option in the context of the economic crisis and the possibility that older domestic workers may be more likely to obtain the more secure and stable jobs. 45 Longitudinal studies are necessary to investigate how public policies in favor of education have interacted with age and race to affect domestic workers.
Race of Housekeepers and Housecleaners
Of the total, 40.8 percent of the workers in our sample were Black, according to their self-report. National data from the same year indicate that 63% of Brazilian domestic workers were Black, and 55.5% of Brazilians were Black. According to data from the last Brazilian census (2022), the proportion of Black people was 32% and White people was 67% in the city where we conducted our study. 46 This means that the 40.8% of Black women in our sample of domestic workers is an overrepresentation of the percentage of Black women in this city.
We found a slightly higher percentage of Whites among house cleaners. The national data from 2019 indicate that among domestic workers over 16 years, 59% of Black women are housekeepers, whereas only 53% of White women are housekeepers. 36 During slavery, the private/domestic space allowed Black women to achieve a certain autonomy and status. Today, paid domestic work still grants a degree of autonomy to some Black women who have few other opportunities. Nevertheless, domestic work often places women in an unprotected employment relationship, with socioeconomic vulnerability. 36
Marital Status and Gender Division of Nonpaid Labor
In our sample, domestic workers were married at about twice the rate of women in the general Brazilian population. Given the large number of women in the sample who started work at an age at which it is likely that they were not married, we can provide 2 hypotheses. First, that women in domestic service get married at higher rates, in part, because they feel a need to have another income to their households because domestic service does not pay enough to support them. Second, women start young but leave domestic service and return when they get married. If these preliminary findings are confirmed by a larger study with a rigorous probabilistic sample, higher rates of marriage among domestic workers might be explained by the fact that getting married and having children entails higher expenses, leading women to go into the workforce to support their families.
When women go into the workplace, the demands of domestic labor and childcare in their homes do not disappear. This means that they perform similar tasks in paid and unpaid work. In our survey, more than 95% of domestic workers reported being responsible for housework at home. Only 55% of housekeepers and 31% of house cleaners reported that other family members help with housework. House cleaners tend to work longer in their homes than domestic workers, perhaps because their work outside the home is less steady. 45
Worldwide, women spend a greater number of hours on unpaid labor than men. This can generate work–family conflict and may be associated with health problems, especially mental health problems. 47 A study carried out in Canada found higher levels of psychological distress among the lower income women when compared to higher income women; and work–family conflict contributed to this distress. 1 Public policies aimed at improving women's mental health must prioritize the most vulnerable women, such as single mothers. Policies should provide health and social care assistance, including education for the mother and the child, and professional training that will allow domestic workers to seek new work opportunities. In addition, policies should encourage formalized employment, ensuring the workers’ rights as paid rest, vacation and sickness absence, and better remuneration.
Occupational Differences Between Housekeepers and House Cleaners
Our preliminary findings showed some occupational differences between housekeepers and house cleaners. Housekeepers received a monthly wage, usually worked in only one residence, and had their employment relationship recognized by the employer. They performed almost all daily maid work, such as hanging clothes, ironing, dusting furniture, cooking, and washing dishes. In contrast, house cleaners were paid by the day, worked at different locations during the week and carried out activities, such as cleaning bathrooms and washing windows. Our findings suggest that the Brazilian policy that provides social security for housekeepers, while making other forms of domestic work illegal, has differentially affected the occupational hazards and health of Brazilian domestic workers. A larger study with a probabilistic sample is necessary to confirm these preliminary findings.
House cleaners, paid per day, can choose to work as many days as they are offered or fewer. To the extent that they can afford to decline some of the offers of work they receive, they can distribute their working time. This can create an impression of control over their work, but it does not provide stability. 44 House cleaners may be able to increase their earnings by working in several different locations but only to the extent that the vicissitudes of the informal market permit. Daily wage rates vary according to market competition, region, and individual oral contract. House cleaners face the challenges of a precarious work relationship and no assurance of labor rights. 15
House cleaners, in our sample, had lower wages, whereas housekeepers had work stability and access to transportation assistance. This assistance is essential because they travel long distances, as many work opportunities are outside their neighborhoods, and the bus is the main means of commuting. In Brazil, geosocial inequality between employers and domestic workers is a fact. This means that domestic workers need to travel long distances, making cheaper transport such as cycling or even walking unavailable, and the most economical option is public transport. The lack of legal protections leaves house cleaners in unsafe work environments in which they have very limited rights. Lack of rights aggravates the health outcomes and injuries experienced by some domestic workers, due to low income, no paid vacation, no paid weekly rest, and no paid time to access health services.
Policy and Legislation
As indicated above, in 2015, Brazil passed labor legislation on domestic work that differentiates between housekeepers and house cleaners according to the number of days they work. The legislation gives housekeepers the right to a written employment contract, minimum wage, limitation of 8 hr of work per day, lunch breaks, overtime pay, obligation for employers to register workers in social security, and compensation for unfair dismissal.
At the beginning of the pandemic, after the data collection for this study was completed, both housekeepers and house cleaners, were laid off en masse, leading to the recognition that one of the most exposed and vulnerable occupations was that of domestic worker. Most had no employment relationship and, therefore, did not have access to unemployment insurance and other social security benefits. 48 The massive layoff brought about discussion and social mobilization that made it possible to highlight the precariousness of domestic work and the importance of improvements for domestic workers, not only in Brazil but in other countries. 49
The legislation was an advance, but it needs to be improved by providing a clear definition of roles and tasks, length of service, and financial incentives for these workers and their employers to enroll in social security is essential. The current Brazilian political scenario is challenging, but promising, due to the recent inauguration of President Lula da Silva, from the Workers’ Party, which was in power and promulgated the domestic work law and fostered the debate on domestic workers. In 2022, the new government created a National Secretariat for Care and Family under the Ministry of Development and Social Assistance, Family and Fight Against Hunger. The objective of this secretariat is to build a Plan National Care Authority, ensuring decent and protected work for people engaged in paid care work, including domestic workers.
It is essential to ensure that domestic workers are recognized. It must be a priority for this government to think about strategies of social protection for house cleaners not yet covered by the law. New working relationships need be discussed and, as appropriate, regulated, as in the case of use of online platforms that mediate the contracting of domestic and care work, need to be regulated in order to make domestic work decent work rather than precarious or informal.
It is also necessary to guarantee access to quality public services, such as daycare centers for children, for the families of domestic workers.
Finally, all initiatives that become part of public policies for domestic workers must be based on evidence and systematically monitored and evaluated to understand the impact of public policies for this working population. The impact of public policies on health and education could also be investigated in epidemiological studies using national databases.
Limitations
One of the limitations of this study was failure to obtain a probabilistic sample. Attempts were made to obtain a larger convenience sample, by contacting all identified potential participants but only 26% agreed to participate. The inability to contact many potential participants was mainly due to the nonexistent telephone numbers. The use of a convenience sample does not make it possible to generalize the results for all domestic workers in Brazil. This nonrepresentative sample can be used to generate hypotheses to be explored in future studies with a larger probabilistic sample.
Self-reported data were used, which is also a limitation of our study, due to biases which affect self-reported data (eg, selection and recall bias). Selection bias could present due to the convenience sample. Recall bias could be happening because the participants may not accurately remember previous events or omit details, specifically, those with more pain may be more accurately aware of their work activities than those with less pain because the pain itself forces such awareness. Characteristics of the domestic workers, such as difficulties with access to health care and schooling may also impact the reliability of the data. Another limitation was the way by which work activities were evaluated, which did not enable a more detailed analysis of the ergonomic exposure. This limitation is related to the difficulty in carrying out assessments at the job site (homes of employers). The lack of psychosocial data is also a limitation of this study.
In Brazil, people under 18 years cannot participate in research without approval of their guardians. It is very difficult to get consent from guardians by a method that satisfies an ethics committee in a study in which first contact is via telephone. Despite the importance of protecting minors from risks related to research, the inability to collect data from underage workers is a study limitation because child labor was a subject of this study.
Implications for Future Studies
The preliminary findings of the present study suggest directions for future contributions to the scarce literature on assessment of different conditions of domestic work. By describing activities performed at work and those that cause musculoskeletal symptoms, this study offers preliminary findings whose further investigation can contribute to health and work policies directed at cleaners. Future studies with a prospective design should be conducted to investigate the relationship between health conditions and occupational and nonoccupational risk factors, as well as the occurrence of symptoms during specific work tasks in larger probabilistic samples.
Qualitative studies may be useful to understand their trajectories of the lives; and the reason for starting to work at a young age. In future studies, physical activity should be investigated with direct measurement through physical assessment. Medical records should be used in addition to or instead of self-report to improve reliability of health data.
Conclusion
In this sample, housekeepers and house cleaners were very similar in terms of sociodemographic and health data. The groups differed mainly with regards to work characteristics and types of exposure. House cleaners were younger than housekeepers, were exposed to more working hours per day, did not have work stability or a fixed wage and performed cleaning activities, such as washing windows, which can harm the lower back and upper limbs. Housekeepers performed more ironing, which was associated with lower back symptoms. Ergonomic attention should also be given to these workers, for example, providing information for the employers about ergonomic appliances and the need of recovery time. These preliminary findings may indicate the need for policies that ensure rights and offer opportunities for better working conditions. Thus, a recommendation for an expansion of the national policy (Complementary Law n° 150/2015 16 ) related to the protection of labor rights to cover, rather than alienate, all domestic workers should be further developed.
Highlights
▪ In this sample, domestic workers started work early in life, mainly doing activities related to house cleaning, and have completed a primary school education, but not much more
▪ In this sample, Brazilian domestic workers with no formal labor relationships (house cleaners) were younger, reported lower income and had no social security, are exposed to ergonomics risk factors,
▪ In this sample, domestic workers were exposed to ergonomic risk factors and experienced lower back and upper limb symptoms when performing work activities. House cleaners reported more wrist symptoms related to washing activities and fewer symptoms in the lower back related to ironing in comparison to housekeepers. More than one-third of housekeepers and over 60% of house cleaners reported use of pain medication.
▪ A high proportion of housekeepers in our sample use blood pressure medication. It is possible that this is due to their older average age than house cleaners and their higher level of occupational physical activity or both.
▪ Of less interest to the audience of NEW SOLUTIONS is that fact that many in this sample are obese and do not practice leisure time physical activity. The authors believe that this information is a necessary part of a comprehensive health profile.
Footnotes
Acknowledgments
We would like to thank the participants who cooperated with the recognition of their profession.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Coordination for the Advancement of Higher Education Personnel—Finance Code 001.
Ethics Approval
The study was conducted in a municipality in the state of São Paulo, Brazil, in 2018, after having received approval from the institutional review board (certificate number: 79234617.0.0000.5504).