
Abstract
Objective: This pragmatic randomized study was conducted to compare the effectiveness of telephone and face-to-face counseling in influencing problematic gambling beliefs and behaviors. Method: Ninety-two participants from diverse ethnic backgrounds who had been affected by problem gambling were provided with psychological interventions delivered either by telephone or conventional face-to-face counseling over a 3-month period. Results: A significant overall time effect between pre- and postintervention assessments was found for total hours, money and proportion of income spent, and the attitudes and beliefs scores. There was no significant difference in effect size between the two groups. Conclusion: This study provides preliminary evidence that both face-to-face and telephone counseling interventions might be equally effective in terms of short-term clinical outcomes measured postintervention.
Introduction
Gambling is fast becoming a major social and public health issue worldwide affecting between 0.2% and 5.3% of adult population (for a recent review on gambling-related problems, see Hodgins, Stea, & Grant, 2011). For instance, it is estimated that approximately 0.9% and 2–3%, respectively, of the adult population of the United Kingdom (Wardle et al., 2011) and New Zealand (Abbott & Volberg, 2000) meet the criteria for “problem gambling.” It is generally estimated that between five and seven other people are negatively affected by each problem gambler (Adams et al., 2004). Problem gambling means the individual meets three or four of the Diagnostic and Statistical Manual IV (DSM-IV) criteria (American Psychiatric Association, 2000) and has the following problems: high rates of gambling-related fantasy, lying, using gambling to escape, and preoccupation with gambling. Problem gambling has consistently been associated with bankruptcy, crime and incarceration, depression, suicidal ideation, substance abuse, breakdown of the family unit, and disruption to the family and community (Bellringer et al., 2008; Brown & Raeburn, 2001; Rankine & Haign, 2003). “Pathological gambling” refers to a condition in which individuals meet five or more of the DSM-IV (American Psychiatric Association, 2000) criteria. A person suffering from pathological gambling shows persistent and recurrent maladaptive gambling behavior resulting in significant dysfunction in the areas of work, study, and social and family relationships (Alegria et al., 2009). Although problem and pathological gambling are often referred to as challenging issues for social workers (Gilligan, 2007; Kemshall, 2010; Momper, 2010; Yeung, Ho, Lo, & Chan, 2010), the topic has not been studied extensively.
Based on international experience, it is estimated that on average, about 15% at most of problem gamblers receive counseling and very few at-risk individuals seek intervention (National Research Council, 1999; Productivity Commission, 2010; Suurvali, Hodgins, & Cunningham, 2010), often very late in the development of their problem (Tavares et al., 2002) and usually only as the result of a crisis (Evans & Delfabbro, 2005; Pulford et al., 2009). One study showed that over 80% of participants with gambling problems said that they had not sought help for various reasons, such as wanting to handle the problem on their own and believing themselves capable of doing so, and not considering their gambling to be serious enough to merit intervention (Hodgins & el-Guebaly, 2000). Many types of interventions for problem gambling, such as cognitive–behavioral therapy (CBT) and motivational interviewing (Prochaska & DiClemente, 1986) have been developed. While a number of clinical trials have been performed to examine their efficacy or effectiveness (Carlbring, Jonsson, Josephson, & Forsberg, 2010; Dowling, Smith, & Thomas, 2007; Myrseth, Litlerè, Støylen, & Pallesen, 2009; Oei, Raylu, & Casey, 2010; Problem Gambling Research and Treatment Centre, 2011; Toneatto & Dragonett, 2008), few studies have examined the effectiveness of different modalities of delivery. Individually based gambling interventions are most often delivered through either telephone or face-to-face counseling. Moreover, most studies are designed to examine whether an intervention is efficacious under ideal experimental conditions. To date, pragmatic clinical trials, which are designed to investigate how effective an intervention for problem gamblers is in everyday social work practice, are still rare in the social work context, although less so in other disciplines such as psychiatry (Hotopf, 2002; Hotopf, Churchill, & Lewis, 1999).
Research postulates that the effectiveness of an intervention will vary across different delivery channels (Echeburua, Fernandez-Montalvo, & Baez, 2000; Tzelepis et al., 2011), so it would not be surprising to find that telephone and face-to-face counseling for problem gambling have different outcomes. Face-to-face counseling is the conventional mode of social work or psychological intervention and has been widely used in supporting individuals with problem gambling (Griffins & Cooper, 2003). Although new modalities of counseling (such as Microsoft Networking, e-mail, and Facebook) have recently been introduced, face-to-face counseling remains the dominant approach. However, there is limited support for the idea that it is superior to interventions delivered over the telephone (Coman, Burrows, & Evans, 2001). On the contrary, various studies illustrate various advantages and disadvantages in the use of telephone over face-to-face counseling, demonstrating that the latter is not the perfect intervention. Easy access is the most often cited advantages of telephone counseling (Haas, Benedict, & Kobos, 1996; Karatzias, Chouliara, Power, & Kilfedder, 2011). While face-to-face sessions are restricted in a formal counseling setting, telephone counseling provides easy access to support for problem gamblers who cannot attend personally (e.g., because they live in remote areas) or are not ready to do so, such as those with social phobia (Cheers, 2000; Haas et al., 1996; Jackson & Thomas, 2005; Marotta, 2005; Shepherd, 1987). As telephone counseling allows immediate contact, it is almost always the first mode of intervention for a person with problem gambling or his or her significant others in times of need (Marotta, 2005). Gambling information and support can be accessed over the phone from anywhere, especially with the advent of the mobile phone, helping clients to save time and travel costs and allowing a high degree of flexibility of participation (King, Bambling, Beid, & Thomas, 2006; Reese, Conoley, & Brossart, 2002). Anonymity is another benefit, allowing those who feel threatened by face-to-face contact (perhaps, due to high levels of shame) or who are not ready to commit to this to avoid attending the session in person. There is evidence that the primary barriers to help seeking for both adolescent and adult problem gamblers are feelings of shame and fear of identification (Evans & Delfabbro, 2005; Gupta & Derevensky, 2000). Telephone counseling, since it is anonymous, can be a good option for an individual to access professional treatment, and may also help them to express their views and feelings about the current crisis more easily and in more detail (Coman et al., 2001). However, counselors point out that telephone counseling lacks visual cues such as facial expressions and body language, which they claim are an integral part of the therapeutic dynamic (Coman et al., 2001; Hunt, 1993). The interpretation of silence in phone conversations can be extremely difficult for the counselor. He or she has to make an extra effort to “tune in” to the properties of the client’s verbal expression in terms of tone, pitch, timbre, intensity, and the nature of silences. Also, counselors or social workers must express their empathy verbally rather than through body language such as nodding and eye contact (Hunt, 1993).
Research demonstrates that mode of the delivery of an intervention is an important factor that warrants consideration in counseling research (Echeburua et al., 2000). There is a pressing need to investigate ways of delivering interventions for problem gambling so as to provide accessible, responsive, and effective services. The present study therefore set out to conduct a pragmatic clinical trial to compare the effectiveness of interventions delivered by telephone and face-to-face counseling in reducing the harm caused by problem gambling. Ethical approval for this study was obtained from the University of Auckland Human Participants Ethics Committee (UAHPEC203/2006). The clinical trial registration details include the Australian New Zealand Clinical Trials Registry: ACTRN12610000826044.
Study Method
Participants
Participants were recruited from the general community through advertisements and media announcements at three specific locations in New Zealand; Auckland, Hawkes Bay, and Christchurch. These locations were chosen as they are broadly representative of participants from the North and South Island (in terms of urban/rural spread and different ethnic population bases) and have a large population size to assist with recruitment. Only individuals who had concerns about their gambling on pokies (also known as electronic gambling machines [EGMs] in New Zealand and Australia or slot machine-style games in the United Kingdom) were recruited, because the majority of clients presenting to government-funded problem gambling services report that these were the activities that concern them the most. It should be noted that EGMs are not limited to casinos in New Zealand but are also widely available in pubs and clubs.
People were eligible for inclusion in the trial if they were (1) aged 16 or older; (2) currently experiencing problem gambling with EGMs; (3) residing in one of the three specified locations; (4) willing to either attend face-to-face intervention sessions or receive telephone calls; and (5) willing to participate in this study. People were excluded if they exhibited any one of the following conditions: (1) they were at immediate risk of causing harm to themselves or others; (2) they were categorized as a “sensitive case” because they were involved in court action against the gambling industry or problem gambling agencies; (3) they refused random allocation; or (4) they were part of the existing clientele of government-funded intervention services. Such individuals were referred to these existing services.
Each potential participant completed a self-report problem gambling screen that addresses the DSM-IV criteria of problem or pathological gambling (American Psychiatric Association, 2000). This screen is considered a stringent measure of problem or pathological gambling for the purposes of making a diagnosis and evaluating intervention outcomes (Cox, Enns, & Michaud, 2004; Stinchfield, Govoni, & Frisch, 2001). The scale has 10 items and the score is calculated as the total number of affirmative responses. A total score of 3–4 indicates problem gambling and a score of 5 or above pathological gambling (Toce-Gerstein, Gerstein, & Volberg, 2003). Participants in this study were required to have a score of 3 or more, which is regarded as the subthreshold for pathological gambling (Cox et al., 2004). Potential participants who did not meet the inclusion criteria (e.g., they scored less than 3 on the DSM-IV screen) were referred to existing problem gambling services in their local area.
Measures
Gambling behaviors
Each participant’s gambling behaviors were measured by collecting the total number of hours spent, total spend, and proportion of total income spent on gambling over the last 4 weeks. These variables are commonly used in gambling research and are regarded as the most sensitive, direct, and meaningful measures of any change to gambling behavior in intervention outcome studies (Toneatto & Ladouceur, 2003).
Gambling attitudes and beliefs
Participants’ attitudes to and beliefs about gambling were measured using the Gambling Attitudes and Beliefs survey (GABS; Breen & Zuckerman, 1999), which assesses general attitudes toward gambling and has been constructed to capture a wide range of cognitive biases, irrational beliefs, and attitudes (Toneatto & Ladouceur, 2003). The GABS demonstrated good internal consistency (Cronbach’s α = .93) and predictive validity in a sample of university students who were active gamblers (Breen & Zuckerman, 1999). It consists of a 35-item questionnaire, with respondents indicating the extent to which they agree with each item using a 4-point Likert-type scale ranging from strongly disagree (1) to strongly agree (4). The total score is the unweighted sum of the responses to all items. Higher GABS scores predict willingness to gamble risking real money.
Self-reported satisfaction and self-rated effectiveness of the intervention
At postintervention, participants were asked “How would you rate your satisfaction with the counseling sessions provided?” Responses were collected using a 5-point scale ranging from not satisfied (1) to extremely satisfied (5). Self-reported effectiveness of intervention was measured by asking “How would you rate the effectiveness of the counseling for your gambling problem?” Again, a 5-point response scale was used ranging from not effective (1) to extremely effective (5).
Interventions
A total of 20 practitioners (including social workers, certified counselors, and those with dual qualifications) from different ethnic groups were made available to provide counseling. Each was a currently practicing clinician within a government-funded problem gambling service, with relevant training and experience in working with individuals affected by problem gambling, including their significant others. All of the participating counselors also had experience with both face-to-face and telephone counseling. To ensure consistency of approach within this randomized study, an intervention manual was produced which set out a consistent basic therapeutic process (such as rapport building, assessments, raising insight/awareness, instilling hope, acknowledging feelings, setting goals, advising on budget management, and avoiding high-risk situations) for problem gambling interventions. The manual did not dictate any particular counseling approach. A 1-day training workshop based on the manual was provided to all participating practitioners. In order to ensure the integrity of the intervention, the counselors were required to submit their midway and termination intervention notes for monitoring purposes, ensuring that both approaches were following a similar process.
Study Procedures
Figure 1 presents a flow diagram of participants through each stage of the trial. In this study, two main recruitment approaches were employed: feature articles and advertising in major community newspapers and advertising on local TV, radio, and websites. Informed consent was requested following an introduction to the research and after it had been ascertained that the potential participant was eligible. Each participant was randomly allocated to one of the two groups (face-to-face and telephone intervention). Allocation concealment was achieved using a central telephone service (i.e., a research call center) via a web-based computer system. Randomization was stratified according to practitioner, to ensure that roughly equal numbers of participants were allocated to each counselor and randomized across both intervention approaches. Each participant was asked if they would prefer to work with a practitioner from a similar ethnic background (i.e., New Zealand European, Maori, Pacific Islander, Chinese, or Korean). Due to limited resources, a gender match was not offered. Participants could attend up to six telephone or face-to-face sessions over a 3-month period. The research team was notified by the practitioner on termination of the intervention for each participant. Assessments were undertaken at two points: (1) commencement of intervention (baseline) and (2) 1 or 2 weeks after termination (postintervention measure). Data were collected by independent investigators who were blind to intervention allocation.

Flow diagram of progress through the stages of the study.
Data Analysis
The data analyses were performed on an intention-to-treat basis, assuming that nonobserved data were randomly missing. Demographic information, mental health status, gambling behaviors, and psychological functioning data were summarized for participants undergoing each of the intervention approaches. Outcome measures were then summarized for each group at each assessment. Differences in each variable between the two groups at each stage were examined using chi-square (χ2) analyses for categorical variables and analyses of variance (ANOVAs) for continuous variables. In the second stage, repeated-measures multivariate analyses of covariance (MANCOVAs) were performed to compute a preliminary estimate of the intervention effect in each group. The mixed model was used to compare the intervention effects between the two groups, while adjusting for their ethnicities and other stratification factors (for randomization) in the regression model. Other potential covariates such as whether or not participants had received counseling before, and their health histories, were adjusted in the regression model if they were statistically significant. Cohen’s d statistic was also calculated to determine effect size of each outcome. In the MANCOVA procedure, extreme values (outliers outside ± 2SD) were removed before analysis to reduce their potential effect on the distribution. As some participants had dropped out at the postintervention assessment stage, the missing data for each outcome measure were imputed using the baseline value. After imputation, the data set was analyzed using standard techniques for complete data. All statistical analyses were performed using the statistical analysis system SAS v9.1.3 (SAS Institute Inc., Cary, NC) as well as the S-PLUS. All statistical tests were two-tailed and a 5% significance level was used throughout.
Results
Descriptive Summary of Demographics
The characteristics of the 92 participants allocated to each of the two intervention groups are shown in Table 1. No significant differences were found between the groups on any demographic or other descriptive variable (p = .087–1.000). In terms of the DSM-IV criteria, the overall extent of problem gambling among participants was similar in both groups. Although some had received counseling for problem gambling before, there was no significant difference in the proportion of such participants between the two groups.
Characteristics of Participants in the Two Groups

Descriptive Summary of Outcome Measures at Baseline and Postintervention Assessments
A descriptive summary of the outcome measures at baseline and postintervention assessments is displayed in Table 2. To confirm the equivalence of the randomly allocated groups, the gambling behaviors and psychological functioning of the group members prior to the intervention phase were also compared. An independent-samples ANOVA indicated no significant differences between those allocated to the face-to-face and to the telephone groups in terms of total money and proportion of income spent on gambling over the last 4 weeks. However, the difference in total hours spent gambling over the last 4 weeks between the face-to-face (M = 20.7, SD = 20.4) and the telephone group (M = 39.0, SD = 59.1) was significant, F = 4.33, p < .04. No significant difference was found in attitudes and beliefs about gambling.
Time Effects Between Baseline and Postintervention Assessments by Outcome Measure for the Whole Sample

Note. GABS—higher score indicating higher inclination to gamble.
Intervention Effect at Different Stages and Differences Between Groups
The intervention effects of the outcome measures for the whole sample are presented in Table 2. A significant overall time effect between pre- and postintervention assessments (p < .05) was found for most of the outcome measures. Significant differences were found for total money spent over the last 4 weeks, F(1, 89) = 5.70, p < .05; total hours spent gambling over the last 4 weeks, F(1, 90) = 5.94, p < .05; proportion of total income spent over the last 4 weeks, F(1, 84) = 7.60, p < .01 and GABS score, F(1, 90) = 14.01, p < .001, between baseline and postintervention.
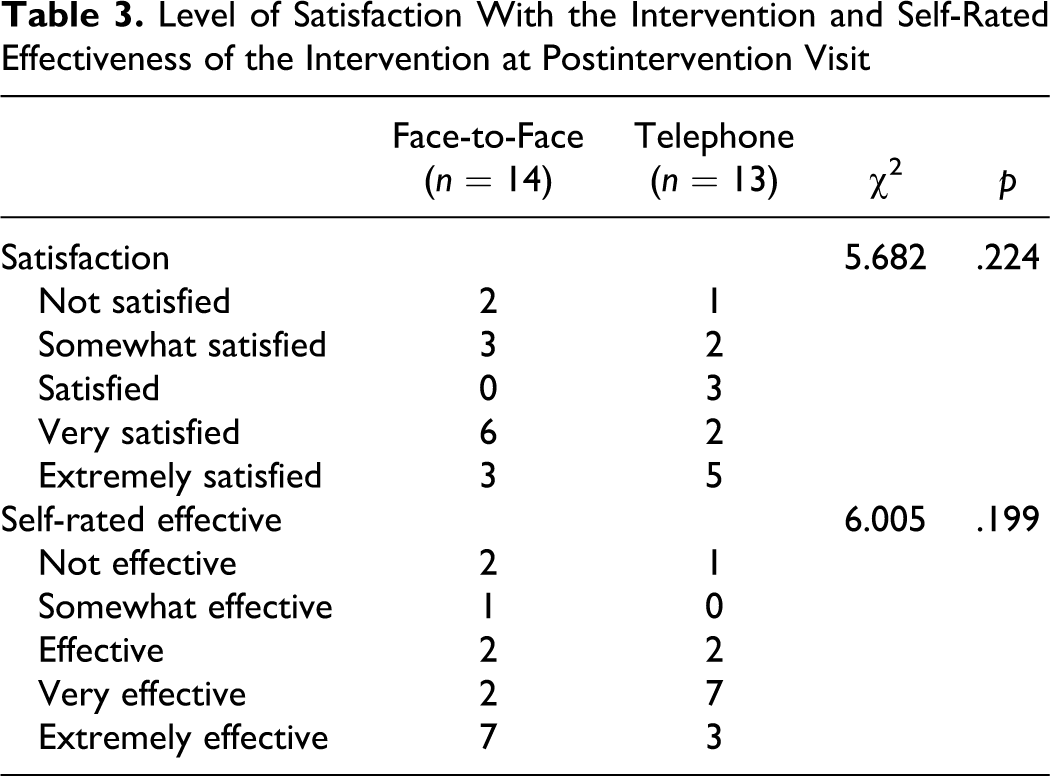
Repeated-measures MANOVA revealed no significant interaction (group × time) effect in the comparison of those allocated to the face- to-face and telephone groups for all outcome measures after imputation between pre- and postintervention assessments. Finally, as shown in Figure 1, there was no significant difference between the groups in terms of the number of intervention sessions attended. Similarly, as illustrated in Table 3, there were no significant between-group differences in self-reported satisfaction and effectiveness.
Level of Satisfaction With the Intervention and Self-Rated Effectiveness of the Intervention at Postintervention Visit
Participants Remaining in the Postintervention Groups and Dropouts
A comparison in terms of demographic features, gambling behaviors, and cognitive ratings was also made between those who were contactable for postintervention measures and those who had left the study. No statistically significant differences were found between them in terms of age, gender, GABS, proportion of total income spent, and number of hours spent on gambling over the last 4 weeks.
Discussion and Applications to Social Work
This study compared the effectiveness of two different intervention modalities, face-to-face and telephone counseling, in controlling gambling behaviors and reducing the harm caused by problem gambling. Two major findings emerge. First, the observed short-term primary data indicate a significant reduction in the amount of money and time spent gambling between pre- and postintervention measures for both groups. A time effect between pre- and postintervention assessments was also found for all outcome measures. Second, there were no statistically significant differences between the face-to-face and telephone interventions in terms of the changes in overall pre- and postintervention outcome scores. This provides preliminary evidence to support the proposition that the clinical outcomes for the telephone intervention were similar to those for the face-to-face counseling. The clients who participated in this study could be considered representative of people with gambling problems in the wider population; the mean DSM-IV criterion score of 7.4 (SD = 1.89) for all participants is consistent with other samples in previous community-based studies (Crisp et al., 2004; Hodgins & el-Guebaly, 2004). An additional strength of the present study was the ethnic match between counselors and participants (for those who wished it), which is not often available in treatment research on problem gambling.
However, the findings of this study should be treated cautiously, due to its limitations. First, due to the lack of a control group, it was not possible to examine the efficacy of the two intervention modalities. However, the purpose of this pragmatic study was to compare effectiveness rather than to examine efficacy (MacPherson, 2004). Second, there were high rates of dropout or attrition that may limit the internal validity of the results (e.g., the participants who were still contactable for the postintervention assessments might be susceptible to self-selection bias) or cause the treatment size effect to be overestimated (Westphal, 2006). On the other hand, the findings can still be considered acceptable as the data analyses were based on the principle of “intention to treat.” This interpretation is further supported by the fact that there was no difference between the groups in the number of intervention sessions attended by participants and their self-reported satisfaction and effectiveness. Furthermore, these results are consistent with a similar randomized controlled study on patients with obsessive compulsive disorder, in that the clinical outcome of CBT delivered by telephone was equivalent to that of an intervention delivered face-to-face (Lovell et al., 2006). In another recent study, smokers randomly allocated to receive six counseling sessions over the phone were more able to achieve abstinence at a 7-day point than controls who received self-help manuals in the post. A closer examination of the number of sessions attended by participants (see Figure 1; 39.1% [face-to-face] and 34.8% [telephone] attending six or more sessions) in this study also suggests that it is comparable to the help-seeking behavior of clients presenting to problem gambling services in New Zealand; national user statistics indicate that 37.3% of clients receive between 3 and 10 hr of counseling (Ministry of Health, 2006).
Previous studies show that drop-out rates in the field of addiction are very high with regard to both provision of clinical services and research, and that efforts to reinforce intervention adherence are only partially successful (Pulford, Adams, & Sheridan, 2006; 2007). Poor adherence to treatment is often considered a serious challenge in problem gambling interventions (Ledgerwood & Petry, 2005; Toneatto & Ladouceur, 2003). A recent systematic review of current research on dropout from psychological interventions for pathological gambling concludes that there is limited or inconsistent evidence about the specific variables that predict dropout (Melville, Casey, & Kavanagh, 2007). Based on a cognitive model of dropout among individuals with drug dependence, common reasons for poor adherence to interventions are relapse, legal problems, issues involving the family, lack of understanding of the intervention itself, logistical problems (such as transport and childcare), or the counselor–client relationship (Dunn, Delfabbro, & Harvey, 2011; Gu et al., 2012; Liese & Beck, 1997). However, we would argue that the more appropriate question may be “what service model best caters for the reality of this presentation?” In other words, we should ask how problem gambling counselors or social workers can reorganize their services (e.g., How should the first in-take session be structured? What are the questions we should ask or avoid?) to engage users in a way that best maximizes their brief episodes of involvement. Social workers need to rethink how to approach the intake or first-contact session (either face-to-face or on the telephone) in a way that will better motivate clients to deal with addiction-related problems. One of the possible practice models to aid further discussion is motivational interviewing (for reviews on the concept and practice evidence see Burke, Arkowitz, & Menchola, 2003; Miller & Rollnick, 2002; Rubak, Sandbaek, Lauritzen, & Christensen, 2005). In relation to problem gambling, a motivational interview has been found to be superior to a control interview in reducing gambling behavior (Diskin & Hodgins, 2009), while in two randomized control trials (RCTs) a motivational interview combined with a self-help workbook was found to be superior to a waitlist control, in reducing gambling behavior (Hodgins, Currie, & el-Guebaly, 2001; Hodgins, Currie, Currie, & Fick, 2009) with another RCT showing that a motivational enhancement intervention achieved a significantly greater reduction in dollars wagered over time compared to the control condition (Petry, Weinstock, Morasco, & Ledgerwood, 2009). Furthermore, social workers need to enable potential clients and/or concerned significant others (such as family members and colleagues) to seek help as early as possible when needed, regardless of which mode of contact is used. Social workers or human-services professionals in general will benefit from basic training in the detection of the early warning signs of problem gambling and the harm it causes, and in screening for problem gambling in a variety of practice settings (Problem Gambling Research and Treatment Centre, 2011). Based on the authors’ experience, clients are less reluctant to seek help for their gambling problems if they know there is a hope of recovering or gaining control of their behavior and if they know the service is free, confidential, provided by professionals and informed by evidence-based practice.
In conclusion, this pragmatic study provides some hints that both types of intervention might produce equally effective short-term clinical outcomes in terms of postintervention measures and that telephone counseling may be a cost-effective intervention that needs to be carefully tested in future studies. One of the challenges for funders and service providers is how to reduce barriers to making both service modalities available to the public and how to provide them in a complementary fashion. In addition to telephone and face-to-face interventions, technological advances mean that counseling can be delivered through other means such as Facebook, Twitter, YouTube, WhatsApp, or texting. Future studies should evaluate the effectiveness of different modes of problem gambling service delivery so as to improve the match between these interventions and the needs and presentation patterns of potential clients.
Footnotes
Acknowledgments
The project was undertaken in three centers: the Centre for Gambling Studies, the Clinical Trials Research Unit, and the Survey Research Unit, all of the University of Auckland, New Zealand. The opinions expressed herein are those of the authors and do not necessarily reflect the views of the funding agency.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors are grateful for the funding support of the Ministry of Health of New Zealand to conduct the present clinical trial.