
Abstract
Objective: This pilot study examined the effect of structural family therapy (SFT) on children’s impairment and depressive symptomatology and mothers’ depressive symptomatology and anxiety for 31 families served by a community mental health clinic. Method: A one group predesign/postdesign, with a baseline and two follow-up time points, was used. Results: A series of repeated measures analyses of variance showed significant improvement for mothers’ depression, F(2, 36) = 6.93, p = .003, η2 = .278, and anxiety, F(2, 34) = 6.44, p = .004, η2 = .275. Mothers’ ratings of their children’s impairment significantly improved, F(2, 42) = 6.27, p = .005, η2 = .270, though children’s self-rated impairment and depressive symptomatology did not change. Results were confirmed using random regression analyses. Conclusion: SFT has promise for simultaneously addressing mothers’ and children’s needs in community mental health settings. However, structural barriers impacting feasibility were identified and discussed.
Introduction
Literature consistently demonstrates the reciprocal nature of child and maternal mental health (Diaz-Caneja & Johnson, 2004; Dover, Leahy, & Foreman, 1994; Kaufman et al., 1998; Kovacs, Devlin, Pollack, Richards, & Mukerji, 1997; Lyons-Ruth, Wolfe, Lyubchik, & Steingard, 2000; Oyserman, Bybee, Mowbray, & Hart-Johnson, 2005; Puig-Antich et al., 1989; Rishel, Greeno, Marcus, & Anderson, 2006). Between 40 and 70% of children whose mothers experience mental health problems meet criteria for a psychiatric disorder (Beardslee, Keller, Lavori, Staley, & Sacks, 1993; Beardslee, Versage, & Giadstone, 1998; Weissman et al., 2006) and evidence suggests as many as 60% of mothers seeking behavioral health services for their children meet criteria for depression or anxiety disorder at the time the child presents for treatment (Kaufman et al., 1998; Rishel, Greeno, Marcus, & Anderson, 2006; Rishel, Greeno, Marcus, Sales, et al., 2006; Swartz et al., 2005). If both family members do not receive treatment, each continues to suffer, often with long-term consequences (Barkley, Guevremont, Anastopoulos, & Fletcher, 1992; Beardslee, Gladstone, Wright, & Cooper, 2003; Breslau & Davis, 1986; Civic & Holt, 2000; Coiro, 2001; Cummings & Davies, 1994; Downey & Coyne, 1990; Elgar, McGrath, Waschbusch, Stewart, & Curtis, 2004; Goodman & Gotlieb, 1999; Hammen & Brennan, 2003; Harrison & Sofronoff, 2002; Mclennan, Kotelchuck, & Cho, 2001; Pfefferle & Spitznagel, 2009; Weissman, Warner, Wickramaratne, Moreau, & Oflson, 1997; Weissman et al., 2004).
When children receive mental health treatment, it is often because their parents, typically mothers, seek help for them (Broadhurst, 2003; Logan & King, 2001). Mothers seeking help for their children are more likely to perceive caregiver burden and family stress as a result of their children’s behavioral health needs (Alegria et al., 2004; Angold et al., 1998; Verhulst & van der Ende, 1997) and commonly attribute their own mental health symptomatology to the stress associated with caring for a behaviorally disturbed child (Anderson et al., 2006; Nicholson, Sweeney, & Geller, 1998a, 1998b). As a result, mothers believe their own symptoms will improve if their children get better (Anderson et al., 2006) and are unlikely to receive treatment or accept referrals for care to address their own needs (Ferro, Verdeli, Pierre, & Weissman, 2000; Kaufman et al., 1998; Rishel, Greeno, & Anderson, 2008; Swartz et al., 2005).
Family therapy offers an important opportunity to simultaneously address both family members’ needs, as it acknowledges the reciprocal relationship between child and maternal mental health, as well as the emphasis mothers place on the interrelated status of their own and their children’s needs. Family approaches cover a range of different interventions based on varying theoretical sources. Structural family therapy (SFT), specifically designed by Salvador Minuchin for low income, multiproblem families, is grounded in family systems theory and places central importance on establishing a healthy organizational hierarchy within the family system (Doherty & McDaniel, 2010; Goldenberg & Goldenberg, 2008; Minuchin, 1984; Minuchin, Colapinto, & Minuchin, 2007). Through his early clinical work in an inpatient facility for juvenile delinquents, Minuchin observed that improvement achieved through individual therapy often disappeared when juveniles returned home. Therefore, he began to focus on changing families rather than individuals, asserting that the family’s patterns of transaction play a pivotal role in maintaining positive and problem behaviors (Minuchin, 1984; Minuchin et al., 2007). The structural model aligns with and supports social work values as it addresses the presenting problem in the context of systems and the social environment.
The core elements of SFT are well standardized and widely used by clinicians (Cottrell & Boston, 2002). Though only two identified studies systematically tested SFT, they provide empirical support for its utility in treating child and adolescent behavioral health problems (Barkley et al., 1992; Szapocznik et al., 1989). Additionally, SFT provides central theoretical underpinnings for efficacious systemic family approaches, such as brief strategic family therapy (Robbins & Szapocznik, 2000; Szapocznik et al., 2003) and multisystemic family therapy (Henggeler, Schoenwald, Bourdin, Rowland, & Cunningham, 1998). These intensive community-based interventions have a strong evidence base for treating severe behavioral challenges among adolescents, including substance abuse, delinquency, emotional disturbances, and conduct disorders (Austin, Macgowen, & Wagner, 2005; Borduin et al., 1995; Coatsworth, Santisteban, McBride, & Szapocznik, 2001; Curtis, Ronan, & Borduin, 2004; Henggeler, Melton, Brondino, Scherer, & Hanley, 1997; Henggeler, Pickrel, & Brondino, 1999; Henggeler et al., 1986; Henggeler & Sheidow, 2009; Hoagwood, Burns, Kiser, Ringeisen, & Schoenwald, 2001; Robbins & Szapocznik, 2000; Robbins et al., 2002; Rowland et al., 2005; Santisteban et al., 2003; Timmons-Mitchell, Bender, Kishna, & Mitchell, 2006; Waldron, 1997). Systemic community-based family models, which often require low caseloads (4–6 families per clinician), around the clock commitment from clinicians, and expensive training, are rarely available to consumers served in community mental health settings (Drake et al., 2001; Henggeler et al., 1999; Hunsley & Lee, 2007; Ogden & Halliday-Boykins, 2004; Painter, 2009; Rowland et al., 2005; Shadish & Baldwin, 2003).
It is likely that the basic, yet robust SFT model is valuable when used for its original purpose as a short, focused therapy for interpersonal and behavioral problems experienced by multiple problem, low-income families, like those typically served in community mental health settings (Segal, Hodges, & Hardiman, 2002). Additionally, it may be useful for addressing less severe behavioral health problems treated in routine outpatient settings, which could prevent more serious problems and the use of more intensive, restrictive interventions (Painter, 2009). SFT’s systemic orientation also suggests it should address mothers’ mental health symptomatology for the same reasons it affects children. In the only identified study assessing mother’s mental health symptomatology, Barkley, Guevremont, Anastopoulos, and Fletcher (1992) found that mothers receiving SFT experienced a significant decline in depressive symptomatology; though 90% of these mothers were married and their husbands also participated in treatment. The impact of SFT has not been examined among a more diverse sample of mothers.
In order to examine the effect of SFT on children’s and mothers’ mental health symptomatology, the intervention was delivered and pilot tested within a semirural community mental health clinic. The structural model was selected for its relevance to consumers served by this clinic and because it was designed to be easily trained (Minuchin, 1974; Minuchin et al., 2007; Segal et al., 2002). Researchers collaborated with administrators and clinicians at the clinic to implement SFT with the best chance of sustainability. This article reports the results of a one group prepilot/postpilot test of the effect of SFT on children’s impairment and depressive symptomatology and mothers’ depressive symptomatology and anxiety. Thirty-one families met eligibility criteria, and children and mothers completed outcome measures at baseline and 3- and 6-month follow-ups.
Method
Participants and Setting
This work reports findings from a pilot study testing the effect of SFT on children’s and mothers’ mental health symptomatology. The study was conducted at a community mental health center located in a disadvantaged, semirural community. The facility delivers a wide range of services to lower income populations experiencing high rates of unemployment, poverty, mental illness, substance abuse, and frequent family crisis.
As part of a one group prepilot/postpilot test of SFT delivered in a community mental health clinic, women who initiated behavioral health treatment for their children were consecutively recruited between January 1, 2009 and December 31, 2009. They were asked if they would like to participate in a pilot test of a family therapy model or receive usual care (individual therapy) for their children. Mothers provided informed consent and children provided assent prior to participation. All study procedures were approved by an Institutional Review Board.
Families were eligible if the presenting child was between the ages of 5 and 17 and if mothers were over the age of 18; were the biological-, step-, or adoptive mother living with the child presenting for services; had no mental or physical condition that precluded their understanding of study procedures; and if they received at least three treatment sessions during the 6-month study period. A low threshold for treatment dosage was set due to the low dosage typical in community settings, where, on average, consumers receive 4.3 sessions (Hansen, Lambert, & Forman, 2002). One hundred and eighteen families were approached, 54 families agreed to participate, and 31 families received at least three sessions of SFT with multiple family members attending, as described in detail below. Demographic and baseline clinical characteristics for the presenting children and their mothers are shown in Table 1.
Sample Characteristics.
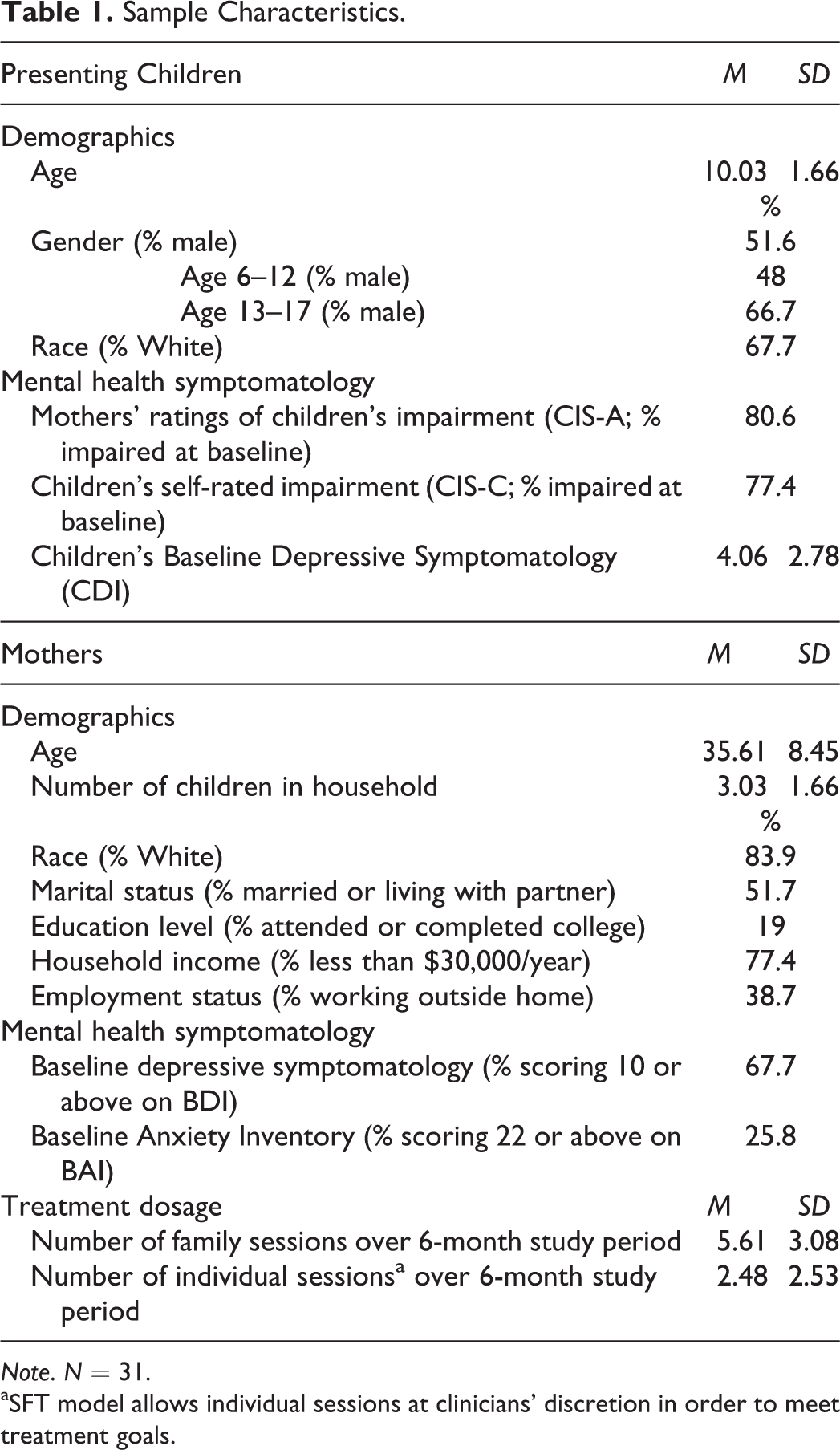
Note. N = 31.
aSFT model allows individual sessions at clinicians’ discretion in order to meet treatment goals.
Children and mothers completed a series of standardized instruments at three equal intervals over the 6-month study period. These assessments were conducted in participants’ homes by a trained interviewer and generally took about an hour to complete. Mothers received 25 dollars and children received 10 dollars for their participation at each time point. There were no significant differences in demographic or baseline clinical characteristics between families who completed all time points and those who were lost to follow-up.
Seventy-four percent (74%; n = 23) of participating families completed all three time points. The results of power analyses using G Power v. 3.1 (Faul, Erdfelder, Buchner, & Land, 2009) indicate that for a one-way repeated measures analyses of variance (ANOVA), a sample size of 23 is adequate to detect a relatively small effect (.30) with the required power level, .80, for a two-tailed distribution. Results also suggest that a samples size of 31 is adequate to detect a relatively small effect (.30) at the .80 power level for a two-tailed distribution with random effects modeling. These findings indicate that the current study had a sufficient number of subjects to detect a relatively small effect, allowing for accurate rejection of the null hypothesis 80% of the time.
Treatment and Procedures
Structural family therapy (SFT)
SFT is a pragmatic, short-term intervention designed to address family relationship problems. The SFT model contends that presenting symptoms or behavior problems experienced by one member of the family system can be understood as stemming from the family’s underlying patterns of transactions. These transactions are governed by a clear set of hierarchical organizing principles, where parents hold the authority for the care and safety of children (Minuchin, 1974).
The structural approach maintains that healthy families are characterized by three distinct subsystems: the parental subsystem, the parent/child subsystem, and the sibling subsystem (Minuchin, 1974; Minuchin & Fishman, 1981; Vetere, 2001). Each subsystem has clear roles and boundaries; though the boundaries cannot be so rigid that natural adaptation through the life course cannot occur. SFT asserts that families adopt dysfunctional patterns when generational boundaries are not maintained or when a family’s stress exceeds their ability to adapt. This approach posits that these dysfunctional patterns can be moved toward healthier structures through therapy (Colapinto, 1982; Minuchin, 1974; Minuchin & Fishman, 1981).
The structural family model facilitates modification of the family structure through joining (Colapinto, 1982; Vetere, 2001), a process in which the therapist creates a new subsystem with the family group. The therapist encourages families to enact their problems in session in order to explore the family structure (Minuchin, 1974; Minuchin & Fishman, 1981) and push the limits of the family system, altering their patterns of transaction and increasing their capacity to tolerate stress, while making sure not to exceed their ability to innovate and adapt (Colapinto, 1982; Minuchin et al., 2007; Vetere, 2001). Once the dysfunctional patterns of transaction are outgrown, individual behaviors identified as presenting problems, lose their support in the system, and become unnecessary (Minuchin, 1974; Minuchin et al., 2007).
SFT requires that all family members attend some sessions, but individual sessions and sessions with family subsystems are allowed as part of the therapy, at the clinician’s discretion. When participants agreed they wanted SFT instead of usual care, they agreed to bring their whole family. Families included in the study had at least three family sessions, along with additional individual sessions initiated by the clinician. Participating families brought between 2 and 8 people to family sessions, with an average of 2.8 people per session.
Intervention implementation and training
The implementation effort was coled by a member of the research team and two directors of clinical services at the agency. The member of the research team is a nationally recognized expert in the field of family therapy and was trained in the structural model by Braulio Montalvo at the Philadelphia Child Guidance Center. The clinical director who collaborated in developing adaptations and providing training supervises the agency’s family-based program, a model of care based on principles of SFT that is offered to families in their homes by teams of trained practitioners and has substantial experience in training and teaching. The effort to implement the intervention was led by the agency’s director of Outpatient Services who ensured that families of presenting children were offered the opportunity to obtain the treatment and supervised reporting of progress at weekly clinical meetings and additional SFT-related meetings as needed.
Effectiveness research often requires adaptations in order to make interventions applicable for particular consumer populations or practice settings (Proctor et al., 2009). The standardized central tenets of the SFT model, described above, were retained, but adaptations were made to increase maternal engagement, modernize the intervention’s approach to gender roles making it more applicable for single mothers, and make the treatment more deployable with the context of low-intensity outpatient therapy. Adaptations included: (1) structuring the treatment around four sessions, renewable contracts; (2) adopting a strengths based, collaborative orientation to treatment; (3) strengthening the focus on engagement, especially of the mother; and (4) emphasizing elements of treatment that directly address the children’s problems as well as the mothers’ problems. These adaptations overtly solicited mothers’ perceptions of their own and their children’s problems in order to collaboratively set goals and explore any inconsistencies between maternal and clinician perceptions. Clinicians solicited maternal feedback throughout therapeutic efforts to restructure the family and utilized treatment to provide enhanced support for maternal functioning.
Four master’s level, licensed mental health professionals were qualified to provide SFT. These clinicians completed training that included 10, 90-min sessions held weekly at the agency. The training incorporated didactic information, case studies, video, role-play interviews, discussions, and selected readings. Each clinician received weekly supervision throughout the duration of the study and held monthly meetings to discuss cases. Clinicians were self-selected to participate in the training. This allowed those clinicians who were motivated to learn and presumably interested in implementing a new intervention to participate.
A multifaceted approach was used to monitor model fidelity. Fidelity was assessed through weekly supervision, monthly clinical staff meetings, and an adherence measure completed by clinicians at the end of a subset of family sessions. The 18-item adherence measure was completed for a random subset of 21 participating families, representing 117 SFT sessions. The adherence measure consisted of 12 items related to core therapeutic principles of SFT, including communication and affect, joining, and enactments and task assignments. Clinicians endorsed the principles and tasks they utilized in each SFT session. On average, clinicians endorsed 76.05% of those items. The additional 6 items were designed as a tool for clinicians to identify family structure and dysfunctional patterns of transaction. The implementation team consistently reviewed completed adherence measures, and fidelity concerns were discussed during supervision and staff meetings as necessary.
Measures
Children’s Mental Health Symptomatology
Columbia Impairment scale (CIS)
The CIS (Bird et al.1993) is a 13-item instrument designed to provide a global assessment of children’s impairment. There are two versions, one self-rated (CIS-C) and one parent-rated (CIS-A). A score of 15 is the threshold for impairment. The CIS-C has demonstrated good test–retest reliability (intra class coefficient of .63), significant discriminant validity (p < .001) when comparing clinical and community subjects at two separate time points, and acceptable concurrent validity (r = .48; Bird et al., 1993). The parent-rated version of the scale has demonstrated higher levels of validity when compared to the children’s self-rated version (Bird et al., 1993).
Children’s Depression Inventory (CDI)—short form
The CDI-short form uses 10 items to evaluate child respondents’ depressive symptomatology. Scores range from 0 to 20 with higher scores indicating more depressive symptomatology; however, no cut points have been reported. The CDI, suitable for children ages 6–17, demonstrates excellent test–retest reliability (r = .87, p < .001), criterion validity, t(46) = 2.48, p < .002, and concurrent validity, r(26) = −.64, p < .001; Saylor, Finch, Spirito, & Bennett, 1984.
Mothers’ Mental Health Symptomatology
Beck Depression Inventory (BDI)
The BDI is a 21-item instrument that assesses symptoms and attitudes correlated with depression (Beck, Ward, Mendelson, Mock, & Erbaugh, 1961). Scores of 10 or above indicate depressive symptomatology (Beck, Steer, & Brown, 1987). Meta-analyses report that the BDI demonstrates consistently high α coefficients among both psychiatric (.86) and nonpsychiatric (.81) samples as well as strong concurrent validity (Beck, Steer, & Garbin, 1988).
Beck Anxiety Inventory (BAI)
The BAI (Beck, Epstein, Brown, & Steer, 1990) is a 21-item scale developed to reliably discriminate anxiety from depression. A score of 22 or above indicates anxiety (Beck & Steer, 1990). The BAI has demonstrated high internal consistency (α = .92) and test–retest reliability over 1 week, r(81) = .75, and has been found to discriminate anxious diagnostic groups from nonanxious diagnostic groups.
Data Analysis
A series of one-way repeated measure ANOVA were performed on children’s mental health symptomatology (CIS-A, CIS-C, and CDI) and mothers’ mental health symptomatology (BDI, BAI) as a function of time spent receiving SFT. Post hoc pairwise comparisons using the Bonferroni adjustment were conducted in order to find the pattern of difference on scores depending on time spent in SFT. As ANOVA does not tolerate missing data, analyses were confirmed using random regression analyses. This statistical technique offers an improvement on the ANOVA as missing data for the eight families who did not participate across all three time points can be modeled based on completed time points, treating subjects as random effects. Treating subjects as random effects improves the generalizability, as well as strengthens the sensitivity of the model (Singer, 1998). In this study, data were not missing at random; missing cases represented attrition. This somewhat weakens the applicability of these models to the data. The results of the more conservative ANOVAs and the results of random regression analyses are presented.
Descriptive statistical analyses were conducted in order to check assumptions required for these statistical tests. Variables that did not meet assumptions were appropriately transformed. Adjustments were reported if the sphericity assumption was not met when conducting repeated measure ANOVAs. As assessments were administered by a trained research associate, there was very little missing data. None of the measures were missing more than 1.5% of the total items at any time point. Missing values analysis module was used to identify missing data and mean imputation, the most straightforward and commonly used method for handling missing data was utilized to fill the missing data points (Allison, 2001; Newton & Rudestam, 1999). Data analyses were conducted using Statistical Package for the Social Sciences (SPSS) v. 18 and Statistical Analysis System (SAS) v. 9.2.
Results
Children’s Mental Health Symptomatology
Results of one-way repeated measures ANOVAs for children’s mental health symptomatology were equivocal. Mothers’ ratings of their children’s impairment significantly improved as a function of time spent in SFT, F(2, 42) = 6.27, p = .005, partial η2 = .270; see Table 2. Mothers’ ratings of their children’s impairment significantly decreased from baseline to 3 months (p = .003). No other significant differences were found. The effect size for the improvement in mothers’ rating of their children’s impairment was .27, which is consistent with an effect size of .25 reported in a meta-analysis of the effect of systemic family therapy on child behavioral outcomes (Shadish, Montgomery, Wilson, Bright, & Okwumabua, 1993). However, results indicate that there were no significant differences on children’s self-rating of their impairment or depressive symptomatology depending on time spent in SFT.
One-Way Repeated Measures ANOVA Results.
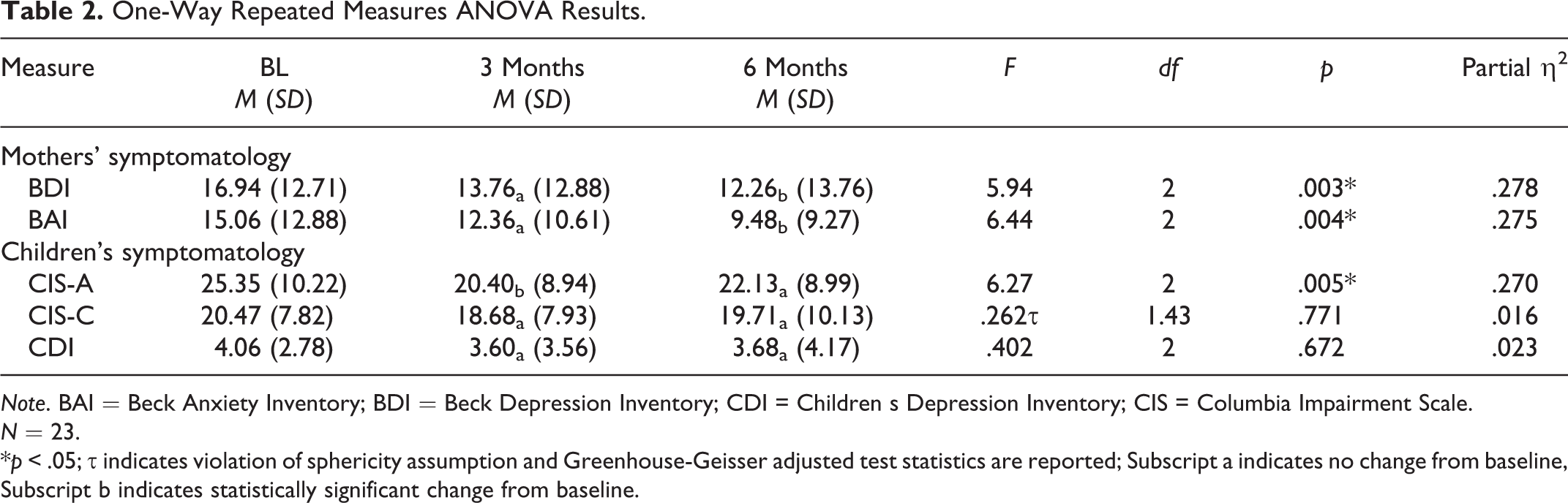
Note. BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; CDI = Children s Depression Inventory; CIS = Columbia Impairment Scale.
N = 23.
*p < .05; τ indicates violation of sphericity assumption and Greenhouse-Geisser adjusted test statistics are reported; Subscript a indicates no change from baseline, Subscript b indicates statistically significant change from baseline.
Random regression analyses confirmed the findings of the one-way repeated measures ANOVAs. Separate random regression models were conducted for each dependent variable. Table 3 reports the β coefficient of time for each model.
Random Effects Modeling Results.
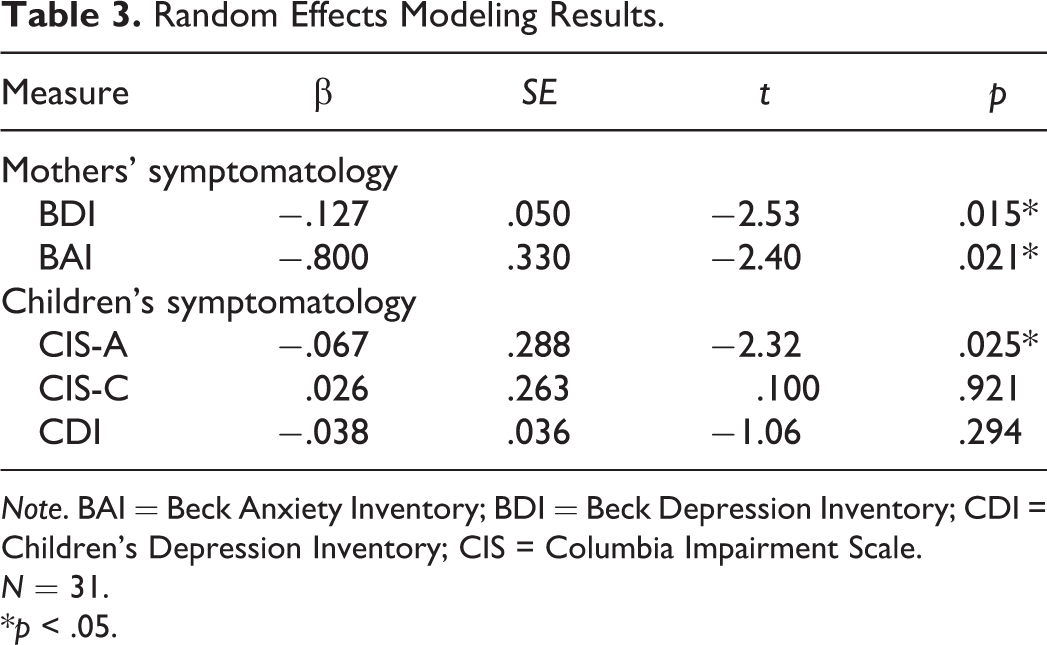
Note. BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; CDI = Children's Depression Inventory; CIS = Columbia Impairment Scale.
N = 31.
*p < .05.
Mothers’ Mental Health Symptomatology
Results of the one-way repeated measures ANOVAs presented in Table 2 demonstrate significant differences on mothers’ depression, F(2, 36) = 6.93, p = .003, partial η2 = .278, and anxiety, F(2, 34) = 6.44, p = .004, partial η2 = .275, depending on time spent in SFT. Mothers’ depressive symptomatology (p = .015) and anxiety (p = .027) significantly decreased from baseline to 6 months. Mothers’ depressive symptomatology and anxiety decreased between baseline and 3 months as well, approaching statistical significance with respective p values of .056 and .052. The effect size of .28 for improvement in both depressive symptomatology and anxiety is consistent with findings from Shadish, Montgomery, Wilson, Bright, and Okwumabua (1993) meta-analysis, indicating that effects sizes for systemic family therapy were .25 to .26; though the meta-analysis only examined child outcomes.
Random effects modeling confirmed the findings of the one-way repeated measures ANOVAs. Separate random regression models were conducted for each dependent variable and Table 3 reports the β coefficient of time for each model.
Discussion and Applications to Social Work
This work tested the effect of SFT offered within a semirural community mental health clinic on the mental health symptomatology of children and their mothers. While the one group pretest/posttest design allows only tentative conclusions, results suggest systemic family approaches are promising for simultaneously addressing children’s and mothers’ needs in outpatient community mental health settings. However, structural barriers impacting feasibility and effective practice were identified and are discussed.
Results of this pilot study demonstrate that mothers’ depressive symptomatology and anxiety significantly improved with time spent receiving SFT and offer particularly important and relevant implications for engaging and treating mothers. Mothers seeking care for their children’s mental health problems often have mental health problems themselves but are unlikely to seek treatment as they view their own needs as related to their children’s behavioral health problems (Anderson et al., 2006; Ferro et al., 2000; Kaufman et al., 1998; Nicholson et al., 1998a, 1998b; Rishel et al., 2008; Swartz et al., 2005). Systemic family models may provide care for some mothers with serious problems that are known to cause a lot of difficulty for them as individuals and for their families. Perhaps more importantly, these mothers might not otherwise receive any mental health treatment. Mothers are committed to improving their children’s lives and are willing to come to therapy to help their children (Anderson et al., 2006). It may be easier for some mothers to commit to care for their children’s benefit than for their own. Offering systemic family models provides a natural point of engagement for this hard to reach population and is consistent with mothers’ views of their own needs and their perceptions of treatment.
While results suggest that mothers likely benefited from SFT, the intervention’s effect on children’s mental health symptomatology was equivocal. Children’s self-rated impairment and self-rated depressive symptomatology did not change; though mothers’ ratings of their children’s impairment significantly improved. As noted, the parent-rated version of the Child Impairment scale has been found to have higher validity when compared to children’s self-report (Bird et al., 1993); though recent psychometrics work questioned the construct validity of the empirically validated one-factor structure for a community mental health sample of mothers (Singer, Eack, & Greeno, 2011). Despite mothers’ ratings suggesting children’s improvement, the change was not clinically significant as, on average, mothers rated their children as impaired across all three time points. In addition, depressed mothers generally perceive their children as more difficult and themselves as having poorer competence as parents (Teti & Gelfand, 1991). It may be that as these mothers’ depressive symptomatology improved, their perceptions of their children’s problems improved as well. However, it is also likely that these findings relate to the documented challenges of implementing empirically supported treatments within the context of routine practice settings (Merrill, Tobert, & Wade, 2003; Proctor et al., 2009).
This work shows that it is feasible to offer SFT as part of routine outpatient community mental health care, but barely. Structural barriers emerged when implementing SFT in this community setting. The main problems stem from realities of the community mental health setting and key features of systemic family models. Low treatment intensity is a major problem in community mental health and a substantial barrier to delivering evidence-based treatment in outpatient community settings. Families participating in this study received an average of 5.6 family sessions. While higher than the average dose received by consumers in routine treatment settings (4.3 sessions), it is still drastically lower than the number of sessions typically required in efficacy trials (13–17; Hansen et al., 2002). Participants’ average treatment dosage suggests that families received a treatment session once every 3–4 weeks. The effect of treatment dosage was examined and found to have no effect on children’s or mother’s mental health symptomatology, suggesting all families received too few sessions to see a dose response. Though the low treatment intensity appeared to address mothers’ needs, it may not have been enough to treat children’s severe impairment. Furthermore, it is likely that the length of time between sessions prevented families from receiving the assistance and guidance necessary to change dysfunctional patterns of transactions likely supporting the children’s presenting problems.
Participating families’ treatment intensity was limited by clinician availability. Evidence suggests that clinicians working in community mental health settings maintain average caseloads of 40–50 consumers (Hromco, Moore, & Nikkel, 2003); however clinicians at the study site had caseloads of between 80 and 90 consumers. This makes it very difficult to provide weekly sessions commonly called for when offering empirically supported treatment. Anything that can be done to reduce caseloads and increase intensity of service seems a good thing when offering empirically supported treatment modalities that allow community mental health consumers to obtain state-of-the-art care.
Additionally, family treatments are difficult to practice. While simultaneously treating multiple family members is an effective, key feature of systemic family models, it is simply more difficult to work with multiple consumers than it is to work with one consumer at a time. This is exacerbated for clinicians in the community mental health setting who engage hard to reach populations often experiencing economic disadvantage as well as multiple family problems. In this case, it may be that the adaptations focused on maternal engagement unintentionally caused clinicians to pay more attention to mothers’ needs to the detriment of the presenting children’s needs. If complex, labor-intensive family models are to be feasible in community mental health settings, clinicians must receive adequate time with families and adequate compensation. Despite the increased difficulty of practicing these models, family therapy is only reimbursed at a slightly higher rate than individual therapy. Offering family treatment can be cost effective (Crane, 2007), but clinicians must receive an incentive for the greater workload required in family sessions. Structural changes related to caseloads and reimbursement rates are needed to increase the feasibility of systemic family models in community mental health settings.
Limitations
This study is not without limitations. The one group predesign/postdesign only allows for tentative conclusions about the effect of SFT. The sample was small and not all families who agreed to participate received enough treatment to meet inclusion criteria. Additionally, families receiving SFT were self-selected. It may be that these families had more severe, complicated problems than families who chose not to participate. The modest number of families who were lost to attrition during the study period discontinued treatment and could not be located for follow-up assessment. As a result, participants were not asked about their reasons for attrition, which would have provided important feasibility and implementation data. Finally, this work was conducted in one semirural community mental health clinic that put a high priority on delivering empirically supported treatment and had a long-standing collaboration with a University-based mental health services research team. These conditions are not typical of community mental health settings and limit the generalizability of study findings.
Despite these limitations, this study answers the call for social work researchers to test empirically supported treatments in routine community settings and, in doing so, offers important practical information to social workers who comprise 60% of mental health professionals in the United States and typically serve vulnerable populations, like those receiving community mental health services (Austin, 1999; Brekke, Ell & Palinkas, 2007; Proctor & Rosen, 2008). The gap between what is known about efficacious interventions and the actual use of empirically supported treatments in routine practice settings remains wide and persistent (Fixen, Naoom, Blase, Friedman, & Wallace, 2005; Gonzalez, Ringeisen & Chambers, 2002; Panzano & Herman, 2005; Torrey & Gorman, 2005). This compromises consumers’ quality of care and threatens clinicians’ ability to reduce health disparities and address family well-being and individual functioning in society (Proctor, 2004). The findings from this pilot test inform and influence social work practitioners and administrators in community mental health settings by offering a greater understanding of systemic family treatments that are effective and allow social workers to enhance their tool kit and tailor treatment for consumers’ specific needs. “Real world” studies, like this one, cannot replace controlled trials, but provide valuable information on transporting empirically supported treatments to community mental health settings (Merrill, Tolbert, & Wade, 2003).
Conclusion
This pilot study examined the effect of SFT, an empirically supported systemic family model, on the mental health symtpomatology of presenting children and their mothers receiving care at a semirural community mental health clinic. Despite a strong body of evidence documenting the efficacy of intensive community-based systemic family treatments that have structural underpinnings, limited work has explored the effectiveness of systemic approaches, like SFT, developed to treat multiproblem families in routine outpatient settings (Painter, 2009) and only one other identified study examined the impact of SFT on maternal mental health symptomatology (Barkley et al., 1992). Results suggest SFT offers a promising approach for simultaneously addressing children’s and mothers’ mental health needs, as mothers’ depressive symptomatology and anxiety improved and children’s impairment decreased according to their mothers. Findings also indicate that systemic approaches offer an important opportunity to engage and treat mothers who otherwise may not receive care. It is possible, though difficult, to offer SFT in routine, outpatient community settings. Structural barriers related to high caseloads and inadequate reimbursement rates make offering this promising and potentially cost saving therapy unattractive and may have impacted children’s outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by NIMH R24 MH 0066872: Collaboration to promote engagement of low-income clients, Carol Anderson, PI.