
Abstract
Objective: We review all available controlled outcome studies of solution-focused brief therapy (SFBT) to evaluate evidence of its effectiveness. Method: Forty-three studies were located and key data abstracted on problem, setting, SFBT intervention, design characteristics, and outcomes. Results: Thirty-two (74%) of the studies reported significant positive benefit from SFBT; 10 (23%) reported positive trends. The strongest evidence of effectiveness came in the treatment of depression in adults where four separate studies found SFBT to be comparable to well-established alternative treatments. Three studies examined length of treatment and all found SFBT used fewer sessions than alternative therapies. Conclusion: The studies reviewed provide strong evidence that SFBT is an effective treatment for a wide variety of behavioral and psychological outcomes and, in addition, it may be briefer and therefore less costly than alternative approaches.
Since its development in the mid-1980s (de Shazer et al., 1986), solution-focused brief therapy (SFBT) has become a widely used therapeutic approach practiced in a broad range of settings in North America, Europe, and Asia. SFBT evolved from the innovative clinical work of a small group of therapists at the Brief Family Therapy Center in Milwaukee, Wisconsin, directed by Steve de Shazer and Insoo Kim Berg. They and their colleagues used insights gleaned from disciplined observation of therapy sessions along with descriptive and follow-up studies of cases to develop and shape the approach into what it is today (de Shazer et al., 2007; Lipchik, Derks, LaCourt, & Nunnally, 2012). SFBT has become widely accepted among social workers and other human service professionals because of its focus on strengths and solutions rather than deficits and problems, and because it provides a rational framework for doing therapy briefly (often less than six sessions) in a managed care environment.
But, policy makers and funders need to know whether an approach is effective before they fund it, practitioners need to consider the evidence base for an approach before they use it, and clients want to know whether the approach being recommended is effective. We decided to critically examine the evidence base for SFBT to ascertain the extent to which SFBT has been shown to be effective, in what settings, and with what types of clients and presenting problems. Although evidence consists of a broad range of descriptive, quantitative and qualitative research, as well as clinical observations, we decided to limit our review to experimental and quasi-experimental studies because they provide the strongest internal validity for assessing intervention outcomes.
Previous Reviews
Five previous reviews of SFBT effectiveness have been published to date. Gingerich and Eisengart (2000) conducted the first systematic review of SFBT outcome research based on 15 controlled studies. Five of the studies met their criteria for well-controlled studies—random (or matched) assignment to groups, sample size of 40 or more, use of objective measures, and some assurance of treatment fidelity—and all five reported significant benefit from SFBT, with four showing SFBT to be significantly better than no treatment or standard institutional services. The fifth study found no significant differences in outcomes between SFBT and interpersonal therapy, considered by many to be an empirically supported treatment (Weissman, Markowitz, & Klerman, 2000). Gingerich and Eisengart concluded “the five studies provide initial support for the efficacy of SFBT” (p. 493). Although this review was important historically, its findings are now dated.
The first meta-analytic review was conducted by Stams, Dekovic, Buist, and de Vries (2006) and included 21 studies comprising a total of 1,421 participants. They found an overall small to medium effect size (d = .37), with somewhat larger effects in more recent studies and in studies of behavioral problems versus marital or psychiatric problems. Although they found SFBT effects to be no larger than other approaches, they found SFBT outcomes occurred sooner than with other approaches. The 21 studies in this review included some nonexperiemental studies, whereas other controlled studies available at the time were left out, compromising the validity of its conclusions.
Corcoran and Pillai (2009) located 10 experimental and quasi-experimental studies of SFBT outcomes and computed the overall effect size for each. Effect sizes ranged from 3.03 to −1.07; five of the studies had overall effect sizes above .20, leading the authors to conclude that the evidence for SFBT effectiveness is equivocal and more research needs to be conducted. The exclusion of unpublished and non-English studies, and studies with insufficient data to compute effect sizes, led to the exclusion of approximately 20 studies available at the time, which limits the overall generalizability of the findings of this review.
A second meta-analytic review conducted by Kim (2008) included 22 SFBT studies involving 1,349 participants. He found a mean effect size of .11 for externalizing behavior outcomes, .26 for internalizing behaviors, and .26 for family and relationship outcomes. Only the effect size for internalizing behavior problems reached statistical significance. This review included several nonexperimental studies, and studies in which SFBT was used as an organizational intervention, or indirect intervention such as parenting or coaching. As with all meta-analyses, Kim had to exclude studies (n = 13) because of insufficient information to compute effect sizes, even though these studies may have been well designed and produced useful information in evaluating SFBT effectiveness. Although the analysis of internalizing and externalizing outcomes is useful, the exclusion of studies because effect size could not be computed and the inclusion of other nonexperimental studies limits its value as a comprehensive assessment of controlled studies of SFBT outcomes.
Finally, Kim and Franklin (2009) reviewed seven outcome studies conducted in American school settings during the period 2000–2007 and found that effect sizes were generally positive although modest, averaging .50. Again, the selection criteria for this review excluded dissertation studies, studies conducted in other countries, and studies appearing before 2000, limiting the generalizability of findings somewhat.
These five reviews included a combined total of 44 studies. Four studies were included in all four reviews, whereas 31 were included in only one of the reviews, suggesting that the reviews used widely different selection criteria. More specifically, some reviews included studies of within treatment outcomes as well as end of treatment outcomes, other reviews included studies where there was minimal or no experimental control, and most of the reviews appear to have excluded unpublished studies. Reviewers also varied in what they considered to be SFBT; some included studies where the specification of SFBT was vague or general, and others included studies where the SFBT intervention was indirect, such as training staff and looking to see if client behavior changed as a result. A significant limitation of the meta-analytic reviews is the necessary exclusion of studies for which effect sizes could not be computed. Finally, none of the reviews included the Helsinki Psychotherapy Study by Knekt and Lindfors reported in 2004, the most rigorous study of SFBT outcomes yet conducted.
With such wide variability in selection criteria it is difficult to reach reliable conclusions about the empirical support for SFBT. Consistent with requirements for a systematic review, we decided to include all controlled studies, published and unpublished, as well as studies in any language to insure the generalizability of findings. Such a comprehensive review provides a sound basis on which to reach reliable conclusions about the effectiveness of SFBT.
Method
Although we considered doing a meta-analytic review because of the rigorous, systematic methodology employed in abstracting and synthesizing findings, we decided against it for several reasons. There is considerable variability in the techniques and modalities used to implement SFBT, the populations and problems with which it is used, and the measures of outcomes. We felt this diversity was too great for a meta-analysis to produce meaningful results (Higgins & Green, 2011; Slavin, 1995). A single effect size would gloss over relative differences in effectiveness with different modalities, problems, and measures and could also suggest more precision in results than is warranted. In addition, we did not want to exclude otherwise excellent studies that failed to report information needed to compute effect sizes.
Perhaps most importantly, we wanted to gather, analyze, and report information from our review in a format that would be of practical value to practitioners and policy makers as they make decisions about which intervention approach to use in a particular field of practice and how best to implement it. Synthesizing findings from many studies into a single number as is done in meta-analyses is useful for making generalizations about the overall effectiveness of a particular approach, but it provides no information on the specifics of the intervention, the problem addressed, or the outcomes achieved. Practitioners need to know how an intervention was used, whether the subjects studied were similar to the practitioner’s clients and whether the outcomes and measures used are relevant for the client’s situation. Effect sizes are useful for establishing general conclusions about an intervention approach; qualitative information about individual studies is needed to judge the validity of those studies’ findings with clients in clinical settings.
Accordingly, we decided to undertake a systematic qualitative review. A systematic review implies specific inclusion criteria, a comprehensive and explicit search strategy, and to the extent possible objective criteria in synthesizing and reporting study findings (Higgins & Green, 2011).
Selection Criteria
Our objective was to review (1) all available, (2) controlled (high internal validity) studies of the (3) end-of-treatment outcomes of (4) SFBT used in psychotherapy and behavior change applications.
We reviewed all studies in any language, published or unpublished, that met our search criteria. Systematic reviews often include unpublished studies found in conference proceedings, dissertations, and research reports, and evaluate their methodological quality and results just as they would any published study (Higgins & Green, 2011; Lipsey & Wilson, 2001; Petticrew & Roberts, 2006). We felt it was particularly important to include unpublished studies in our review since much of the research on SFBT has been carried out in clinical as opposed to academic settings, and as doctoral dissertations. The inclusion of doctoral dissertations in particular helps to reduce publication bias since dissertations are usually written regardless of their outcomes. Consequently, dissertations often show lower effect sizes than published studies (Slavin, 1995).
We limited our review to controlled studies where subjects receiving SFBT were compared with subjects who did not. Some of the studies used random assignment to groups whereas others used a nonequivalent control group design in which subjects were thought to be comparable to the experimental group. We also included single subject multiple baseline studies with six subjects or more. Whereas true experiments have higher internal validity because they use random assignment, nonequivalent control group, and single-subject studies are often more naturalistic and therefore may have stronger external validity.
By end-of-treatment outcomes we mean cognitive and behavioral changes in the client observed at the end of treatment or later. This excludes studies where the outcome was only subjective, such as client satisfaction, or where the assessment of outcomes occurred during treatment as opposed to the end of treatment.
We constructed our operational definition of SFBT by drawing from descriptions that have appeared in the literature (Beyebach, 2000; de Shazer & Berg, 1997; de Shazer et al., 2007; Gingerich & Eisengart, 2000; Smock, McCollum, & Stevenson, 2010; Trepper et al., 2012). We defined SFBT as including the following techniques, and studies had to explicitly mention one or more of these techniques to be included in our review: (1) search for presession change, (2) goal setting, (3) miracle question, (4) scaling questions, (5) search for exceptions, (6) relationship questions, (7) consulting break, (8) compliments, (9) homework assignment or task, and (10) focus on what is better.
We further limited our review to psychotherapy and behavior change studies focused on problematic conditions or behaviors in individuals, families, or small groups. These are the kinds of problems that are often treated in health and mental health settings, and in other settings where treatment is supported by public funds (e.g., schools, corrections). We excluded studies of organizational interventions, and indirect interventions such as staff training and coaching.
Search Strategy
We used several strategies to create the initial pool of candidate studies. First, we searched five electronic databases (PsycINFO, Medline, ERIC, Ebscohost: Megafile, Advanced Search Premier, Social Work Abstracts, and Dissertation Abstracts) using the terms solution focus* OR solution oriented* AND research OR study for the period up to and including April, 2012. Then, if they were not already included, we added studies that had been included in previous reviews noted above, and the 13 studies Kim (2008) excluded from his review because of insufficient data to calculate effect sizes. Finally, we searched an exhaustive list of SFBT research studies maintained by Macdonald (2012), and queried members of the solution-focused therapy Listserv (http://www.sft-l.sikt.nu/). Our search resulted in a total of 1,452 candidate studies (Figure 1).

Flow diagram showing the number of studies at each step in the selection process.
We then reviewed the title and abstract of the candidate studies and discarded 1,391 that clearly did not meet one or more of the selection criteria. Finally, we reviewed the full reports of the remaining studies and excluded those that did not meet our search criteria. When we had questions about a particular study we discussed them until we reached consensus based on further specification of our selection criteria. Studies were excluded if they did not include one or more components of SFBT as defined above, directed the intervention toward someone (e.g., teacher) other than the person (e.g., student) whose outcomes were measured, or measured within treatment rather than end-of-treatment outcomes. Eighteen studies were excluded at this step, leaving 43 studies for abstraction and analysis.
Data Abstraction and Analysis
We extracted data from each of the selected studies using a data abstraction form (available from the first author) that recorded problem type, setting (including country if outside the United States), SFBT techniques used, modality and duration of SFBT, type of comparison group and treatment used, sample size, key features of the study design, outcomes and measures used, pre–post change in the SFBT group, and comparison of SFBT with the control group.
The SFBT techniques used in a study can be used as a general indicator of treatment fidelity—the more techniques employed the more complete the implementation of SFBT. Likewise, the number of therapy sessions indicates the amount of treatment provided, an important consideration since SFBT is intended to be a short-term treatment.
The quality of the study design is an important factor in assessing the trustworthiness of the findings, therefore key design features of each study are reported including the use of random assignment or matching, use of selection/exclusion criteria, sample size, fidelity assessment, use of an alternative treatment for the comparison group, therapist experience, objective measures, and follow-up.
We decided to reduce the data on pre–post change and comparison group contrast to a categorical variable with three levels: no change or difference (0 or ≈), a positive or negative trend (+ or −), or a statistically significant change or difference (+* or −*). Although information is lost in converting quantitative data to categorical, this format provides a shorthand way to describe a study’s overall outcome that allows for comparison among studies as well as aggregation across studies in a field of practice. Interpretation of pre–post change is straightforward; however, the comparison group contrast can be variously interpreted. When studies used a wait-list or “treatment as usual” comparison group, SFBT needs to outperform the comparison group to be considered effective. However, when the comparison group received an alternative treatment known to be effective SFBT must be at least as good as (not significantly different from) the comparison group to be considered effective. To alert the reader to this important distinction, the comparison treatment and group contrast are shown with a shaded background in the tables when an alternative treatment is used.
We report the abstracted information for each study in summary tables grouped by field of practice; these tables provide the “raw data” for our qualitative analysis and synthesis of the findings. The tables also give readers the essential information about each study, so they can determine its applicability to their situation and can consult the original source for more detail if desired. In addition, the tables allow readers to make their own judgments about the research evidence in a particular field of practice.
Findings
Forty-three studies (one study appears in two groups) met our selection criteria and fell into six fairly distinct groupings according to field of practice:
Child academic and behavior problems (14 studies)
Adult mental health (10 studies)
Marriage and family (6 studies)
Occupational rehabilitation (5 studies)
Health and aging (5 studies)
Crime and delinquency (4 studies).
Child Academic and Behavior Problems (14 Studies)
Almost a third of the SFBT outcome studies have been conducted with children with academic and behavior problems; 11 of the 14 were carried out in school settings (Table 1). Since SFBT was usually seen as an addition to whatever educational and social services the child was receiving an alternative treatment was used in only one study.
Child Academic and Behavior Problems.

Note. SFBT = solution-focused brief therapy.
Gray shade = alternative treatment.
aP = Presession change, G = goals, M = miracle question, S = scaling question, E = exceptions, R = relationship questions, B = consulting break, C = compliments, H = homework, F = focus on what is better.
bR = randomized, M = matching, S = selection criteria, L = large sample (20+ per group), F = fidelity assessment, A = alternative treatment, E = experienced therapists, O = objective measures, F = follow-up.
c0 = no change/difference; + or − = positive (desired direction) or negative trend; +* or −* = statistically significant positive or negative change; ≈ = approximately equal.
dTwo multiple baseline series with three subjects each.
eTwo multiple baseline series with three subjects each.
Behavior outcomes
Four studies evaluated the impact of SFBT on behavior outcomes. The first, a Canadian study of youth with emotional and behavioral disorders, compared a 5-day per week residential program using SFBT with an intensive in-home family preservation program (Wilmshurst, 2002). The SFBT group improved significantly on externalizing behaviors similar to the alternate treatment group, but did not change on internalizing behaviors whereas the alternate group showed a significant improvement. Both groups showed significant and comparable improvement on two other measures of social competence and behavior problems. Interestingly, this is the only study we found that showed an alternative treatment to have a significantly better outcome than SFBT.
A Lithuanian study of foster care adolescents found that 31% of the adolescents who received SFBT experienced reliable and clinically significant reduction in behavior problems, and were significantly better off than the untreated control group (Cepukiene & Pakrosnis, 2011). A study of fifth and sixth grade children with school-related behavior problems found that SFBT significantly reduced internalizing and externalizing problems, and that scores moved from the clinical to the normal range (Franklin, Moore, & Hopson, 2008). Another study of school children receiving SFBT showed a trend toward reduced behavior problems, but this was no different than the control group who received a cognitive behavioral parenting intervention (Corcoran, 2006).
Academic outcomes
Four studies explored the impact of SFBT on academic outcomes. In a study of seventh and eighth graders at risk for academic failure and/or poor school attendance the SFBT group had a significantly improved grade point average (GPA) as compared with the no treatment group (Newsome, 2004). In another study, SFBT outperformed usual homework support on 26 of the 38 measures of academic and sociobehavioral outcomes, with an average effect size of .45 versus .30 for the comparison group (Daki & Savage, 2010). Two multiple baseline studies found that students receiving SFBT improved their assignment completion and accuracy (Fearrington, McCallum, & Skinner, 2011; Yarbrough, 2004).
Psychological outcomes
Six studies of children examined psychological outcomes such as self-esteem and self-efficacy. A study of fourth and fifth graders found that an SFBT group intervention resulted in significant improvement in self-esteem (Springer, Lynch, & Rubin, 2000). A study of second grade students added SFBT to the standard teaching curriculum on self-esteem but found that it did not add significantly to the self-esteem of students when compared with students who received the standard curriculum (Cook, 1998). A third study of an SFBT classroom guidance intervention showed a positive but insignificant trend on self-esteem (Leggett, 2004).
An SFBT group intervention used with socially withdrawn Norwegian 12- and 13-year-olds resulted in significant improvement in the children’s self-efficacy (Kvarme et al., 2010). In another study, SFBT was integrated into a 16-week drug abuse prevention group for predominantly Mexican American eighth grade girls with the result that the SFBT group scored significantly higher than the no treatment comparison group on measures of drug use, attitudes and knowledge of drugs, as well as social competence and behavior (Froeschle, Smith, & Ricard, 2007).
Finally, a single-session SFBT intervention was compared with two other interventions that included both solution focused and problem-solving components in a study of high school students seeking counseling for personal problems (Littrell, Malia, & Vanderwood, 1995). Students in all three groups showed significant improvement in alleviation of concerns, attainment of goals, and intensity of feelings, and there were no differences between groups.
Eight studies found SFBT to have significant positive outcomes and five additional studies observed positive trends due to SFBT. The one study that compared SFBT to an alternative treatment found significant benefit from SFBT that was comparable to the alternative treatment. On the other hand, the studies of children with academic and behavioral problems often used convenience samples, fewer than half used random assignment, and the outcome measures tended to be less well established than those in other fields such as adult mental health. Nevertheless, the fact that 12 of the 13 studies found positive trends or statistically significant change due to SFBT provides promising evidence of the effectiveness of SFBT with children.
Adult Mental Health (10 Studies)
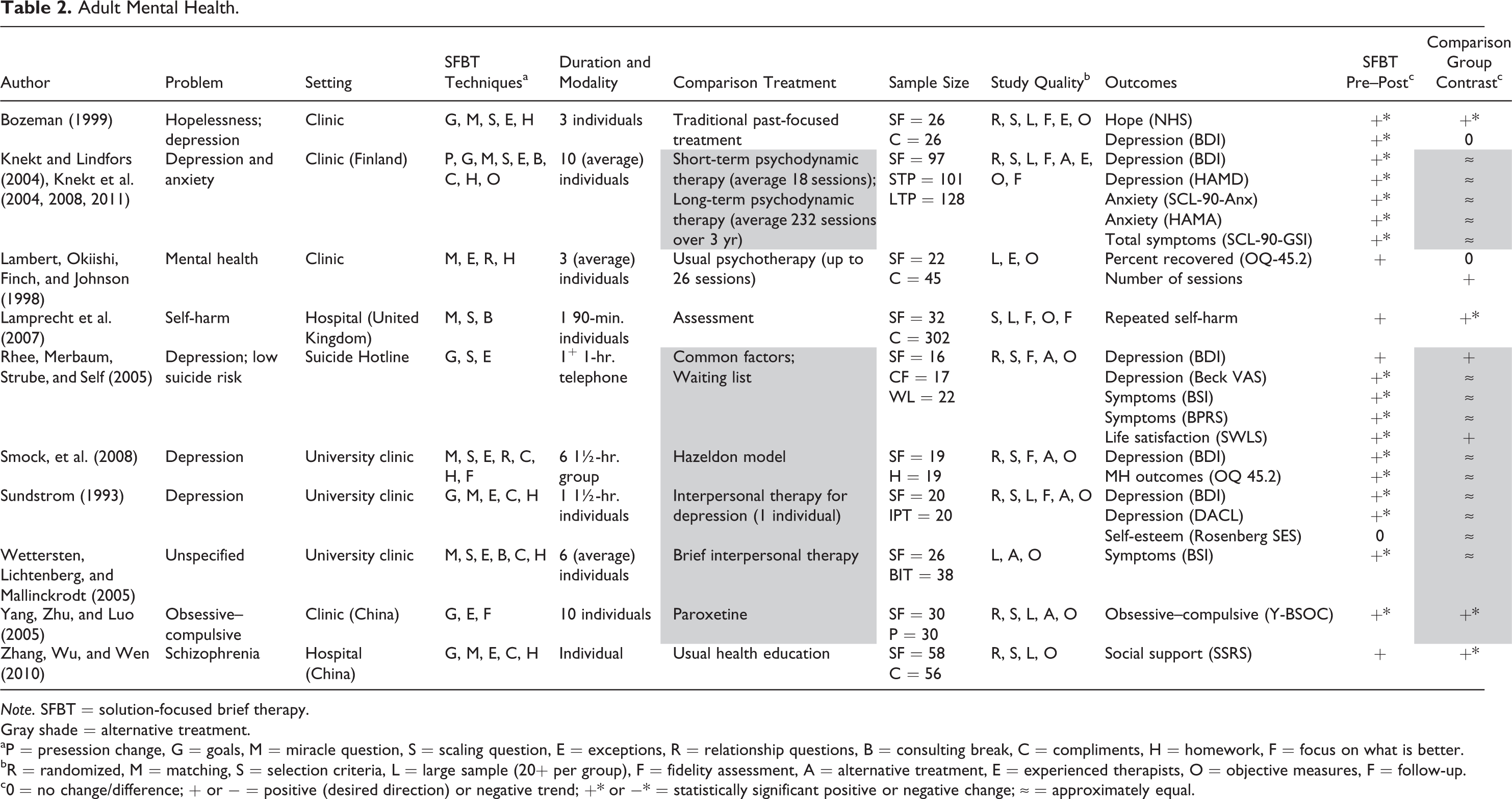
Five of the 10 studies in adult mental health focused on depression, one study focused on self-harm, one on obsessive–compulsive disorder, one on schizophrenia, and two studies focused on general mental health outcomes (Table 2).
Adult Mental Health.
Note. SFBT = solution-focused brief therapy.
Gray shade = alternative treatment.
aP = presession change, G = goals, M = miracle question, S = scaling question, E = exceptions, R = relationship questions, B = consulting break, C = compliments, H = homework, F = focus on what is better.
bR = randomized, M = matching, S = selection criteria, L = large sample (20+ per group), F = fidelity assessment, A = alternative treatment, E = experienced therapists, O = objective measures, F = follow-up.
c0 = no change/difference; + or − = positive (desired direction) or negative trend; +* or −* = statistically significant positive or negative change; ≈ = approximately equal.
Depression
Smock et al. (2008) used six sessions of SFBT group therapy with Level 1 substance abusers and found significant improvement on both depression and general mental health outcomes and at the end of treatment the SFBT patients were comparable to patients who had received a 6-week adaptation of the Hazeldon model (an alternative treatment). Similarly, Sundstrom (1993) found a single session of SFBT with mildly depressed college students produced a significant improvement in depression, a result comparable to the comparison group who received a single session of interpersonal therapy for depression (an alternative therapy). Rhee, Merbaum, Strube, and Self (2005) compared SFBT with a manualized common factors therapy for callers to a suicide hotline. SFBT callers showed significant improvement in depression, psychiatric symptoms, and satisfaction with life, and were comparable to the callers who received the alternative therapy. Bozeman (1999) found that patients receiving three sessions of SFBT became significantly less depressed, but were not significantly different from comparison group patients who received a past-focused treatment (it is unclear if this was an alternative treatment).
The Helsinki Psychotherapy Study (Knekt & Lindfors, 2004; Knekt et al., 2008b) included 326 psychiatric outpatients suffering from depressive or anxiety disorders severe enough to have caused dysfunction in work ability for at least 1 year. Patients were randomly assigned to SFBT (average of 10 sessions), short-term psychodynamic psychotherapy (average of 18 sessions), or long-term psychodynamic psychotherapy (average of 232 sessions). Each therapy approach was delivered by experienced therapists; the SFBT intervention used all nine SFBT techniques and was the most complete implementation of SFBT in the studies we reviewed. Outcomes were assessed using multiple standardized measures at baseline and periodically thereafter for 36 months, providing a follow-up period for the two short-term therapies of more than 2 years.
At 6 months, a period approximately equal to the end of treatment for SFBT and the short-term psychotherapy group, significant improvements were noted in depression and anxiety for both short-term approaches, whereas there was little to no change in the long-term psychotherapy group. At 3 years, however, the long-term psychotherapy group in the Helsinki study had caught up to and surpassed the two short-term groups on all outcome measures. Most of the differences in outcomes between the two short-term groups and the long-term group at 3 years were statistically significant, although in some cases they may not be considered clinically significant.
The five studies examining the impact of SFBT on depression all showed improvement in depression as measured by Beck Depression Inventory; four of the five outcomes were statistically significant. Four of the studies compared SFBT with well-established alternative treatments and in all cases SFBT was found to be comparable to the alternative treatment. We regard this as strong evidence of the effectiveness of SFBT with depressed clinic populations.
Other outcomes
In a quasi-experimental study, Lambert, Okiishi, Finch, and Johnson (1998) compared the weekly progress of outpatients who received SFBT from an experienced therapist with the weekly progress of patients reported in earlier study who received treatment from trainees. The expectation was that patients receiving SFBT would recover sooner than patients receiving standard outpatient care. Scores on the Outcome Questionnaire (OQ-45) showed that indeed 45% of the SFBT patients had recovered after three sessions, whereas patients receiving ordinary care from trainees required 25 sessions, suggesting that SFBT produces outcomes much sooner than ordinary mental health therapy. Recovery was defined as moving at least 15 points on the OQ-45 and moving from the dysfunctional range into the functional range. The findings must be taken with caution, however, because of the differing experience of the therapists in the two groups and the nonequivalent control group.
A single 90-min session of SFBT was found to significantly reduce subsequent reinjury by patients who had been hospitalized for self-harm behavior—only 6% of the SFBT patients repeated self-harm in the following year compared to 13% for untreated patients (Lamprecht et al., 2007).
Ten weeks of combined SFBT and Paroxetine with obsessive–compulsive outpatients in China produced significant improvement in compulsive behavior and was significantly better than Paroxetine alone (Yang, Zhu, & Luo, 2005). A study of convalescing Chinese patients with schizophrenia found that SFBT resulted in significantly improved social support and was superior to treatment as usual (Zhang, Wu, & Wen, 2010). In a study exploring working alliance and therapeutic outcome, six sessions of SFBT produced significant improvement in psychological symptoms and was comparable to open-ended brief interpersonal therapy (Wettersten, Lichtenberg, & Mallinckrodt, 2005).
The studies of adult mental health outcomes, particularly those of depression, adhere closely to the design requirements for establishing evidence-based practice, characterized by large samples, random assignment, relatively complete implementations of SFBT, the use of well-established outcome measures, and comparison with alternative treatments. The Helsinki Psychotherapy Study is particularly exemplary in that it employed an unusually large sample, used experienced therapists in all treatments, and followed patients over a 5-year period. In sum, the evidence of SFBT effectiveness in adult mental health is strong and reliable.
Marriage and Family (6 Studies)
Two of the studies of marriage and family outcomes focused on families that included a diagnosed schizophrenic member (Chung & Yang, 2004; Eakes, Walsh, Markowski, Cain, & Swanson, 1997); one looked at families who had a child diagnosed with autism spectrum disorder (Kenney, 2010); two included couples experiencing marital distress (Huang, 2001; Naude, 1999); and one studied parenting in families with adolescent children (Zimmerman, Jacobsen, MacIntyre, & Watson, 1996). All but one of these studies used a marital, family, or group implementation of SFBT (Table 3).
Marriage and Family.

Note. SFBT = solution-focused brief therapy; AM = Antidepressant medication only.
Gray shade = alternative treatment.
aP = presession change, G = goals, M = miracle question, S = scaling question, E = exceptions, R = relationship questions, B = consulting break, C = compliments, H = homework, F = focus on what is better.
bR = randomized, M = matching, S = selection criteria, L = large sample (20+ per group), F = fidelity assessment, A = alternative treatment, E = experienced therapists, O = objective measures, F = follow-up.
c0 = no change/difference; + or − = positive (desired direction) or negative trend; +* or −* = statistically significant positive or negative change; ≈ = approximately equal.
dOne multiple baseline study across three subjects.
eFour multiple baseline studies across two subjects each.
SFBT significantly reduced family burden and expressed emotion in one study of families including members with diagnosed schizophrenia (Chung & Yang, 2004), and in another study significantly improved family environment and outperformed medication as an alternative treatment (Eakes et al., 1997). A multiple baseline study of three parents of children with autism spectrum disorder suggested that SFBT led to reduced parental stress (Kenney, 2010).
SFBT couple therapy resulted in significantly less depression and improved marital adjustment, and this effect appeared comparable to standard medication treatment (Huang, 2001). A multiple baseline study with eight couples also suggested SFBT led to improved marital adjustment (Naude, 1999).
Together, these six studies show that SFBT has promise as an intervention for improving family system outcomes, particularly in families experiencing stress related to having a member with a diagnosed mental illness. However, because most of these studies used small samples and nonrandomized designs their findings should be taken as preliminary; additional research in this area is needed.
Occupational Rehabilitation (5 Studies)
Five studies examined the impact of SFBT on return to work and related psychological outcomes for sick-listed employees. Four of the studies were carried out in Europe where countries often provide services to sick-listed workers to enable them to return to work (Table 4).
Occupational Rehabilitation.

Note. SFBT = solution-focused brief therapy; STP = short-term psychodynamic therapy; LTP = long-term psychodynamic therapy.
Gray shade = alternative treatment.
aP = presession change, G = goals, M = miracle question, S = scaling question, E = exceptions, R = relationship questions, B = consulting break, C = compliments, H = homework, F = focus on what is better.
bR = randomized, M = matching, S = selection criteria, L = large sample (20+ per group), F = fidelity assessment, A = alternative treatment, E = experienced therapists, O = objective measures, F = follow-up.
c0 = no change/difference; + or − = positive (desired direction) or negative trend; +* or −* = statistically significant positive or negative change; ≈ = approximately equal.
Work outcomes
As expected, the primary outcome in these studies was return to work and reducing the number of sick days. In the one American study, Cockburn, Thomas, and Cockburn (1997) found that 68% of orthopedic patients who received SFBT plus the usual rehab program returned to work within 1 week after completing treatment, compared to 21% who received only the rehab program; at 30 days the difference was 100% versus 70%, again favoring SFBT. These differences were all statistically significant. In a Swedish study, Thorslund (2007) found that 60% of sick-listed workers who received SFBT returned to work within 3 months as compared with 13% who were wait-listed; again these changes were statistically significant. Nystuen and Hagen (2006) found that 39% of the workers who received SFBT had returned to work within 6 months following treatment as compared with 27% of the treatment as usual group, although this difference was not significant. Wells, Devonald, Graham, and Molyneux (2010) found a similar positive but nonsignificant trend in return to work when comparing SFBT with usual psychological services.
The Helsinki Psychotherapy Study of psychiatric outpatients suffering from depressive or anxiety disorders also examined return to work outcomes, since all of the patients had been sick listed for a year or more due to their psychiatric condition (Knekt & Lindfors, 2004; Knekt et al., 2008b). SFBT was compared with short-term and long-term psychodynamic psychotherapy treatments. After 7 months those who received SFBT improved significantly on the three work ability measures, and comparable gains were made by the short-term psychotherapy group; both short-term groups were superior to the long-term group who was receiving weekly sessions. By the end of the third year the long-term psychotherapy group, who had just completed their treatment (average of 232 therapy sessions), showed a positive trend in comparison to the SFBT group (who had received 10 sessions); differences were statistically significant in one of the three measures.
Psychological outcomes
Most of the occupational rehabilitation studies also looked at psychological outcomes as well. Cockburn et al. (1997), Nystuen and Hagen (2006), and Thorslund (2007) found SFBT produced significant gains in psychological functioning when compared to treatment as usual, however, Wells et al. (2010) found no significant differences between SFBT and usual psychological assessment services. Knekt and Lindfors (2004) Knekt et al. (2008a, 2011) found SFBT produced significant improvements in depression and anxiety, comparable to short-term psychotherapy, an alternative treatment.
To summarize, SFBT produced positive changes (some of them significant) in the three studies in which pre–post change was reported, outperformed wait-list or treatment as usual in three of four studies, and performed as well as an alternative short-term treatment in the large and rigorous Helsinki study. These five studies used relatively complete implementations of SFBT, and most employed random assignment and large samples. As a result, there is strong evidence of the effectiveness of SFBT with occupational rehabilitation populations.
Health and Aging (5 Studies)
The five studies in health and aging are a diverse group, both in populations and problems studied and the outcomes that were examined (Table 5). SFBT reduced aggressive and wandering behaviors in nursing home residents with dementia (Ingersoll-Dayton, Schroepfer, & Pryce, 1999), improved mental health outcomes in older adults with self-identified problems (Seidel & Hedley, 2008), improved adjustment to illness and depression in cancer patients (Nairn, 2004), improved blood glucose readings in Type 1 diabetes patients (Viner, Christie, Taylor, & Hey, 2003), and improved fatigue and quality of life in adults with Crohn’s disease (Vogelaar et al., 2011). Pre–post improvement in the SFBT groups sometimes, but not always, reached statistical significance, and in two studies SFBT was significantly better than outcomes in the no-treatment control groups. Five sessions of SFBT seemed to produce better outcomes than 10 sessions of an alternative problem-solving therapy (Vogelaar et al., 2011), although this difference did not reach statistical significance.
Health and Aging.

Note. SFBT = solution-focused brief therapy.
Gray shade = alternative treatment.
aP = presession change, G = goals, M = miracle question, S = scaling question, E = exceptions, R = relationship questions, B = consulting break, C = compliments, H = homework, F = focus on what is better.
bR = randomized, M = matching, S = selection criteria, L = large sample (20+ per group), F = fidelity assessment, A = alternative treatment, E = experienced therapists, O = objective measures, F = follow-up.
c0 = no change/difference; + or − = positive (desired direction) or negative trend; +* or −* = statistically significant positive or negative change.
All five of the studies in health and aging found positive outcomes from SFBT, four of them reached statistical significance. On the other hand, this is a heterogeneous group of studies—each looked at a different client population, examined a different problem, and employed different outcome measures—and as a result there was no opportunity to see if SFBT outcomes could be replicated in different settings by different investigators. All things considered, we believe the consistently positive findings from these five studies demonstrate that SFBT has strong potential for improving behavioral and psychological outcomes related to health and aging that may in turn lead to improved physical health.
Crime and Delinquency (4 Studies)
Three of the four studies in crime and delinquency dealt with juveniles (Table 6). Seagram (1997) found that juveniles in secure custody in Canada who received SFBT significantly reduced their antisocial tendencies and increased their problem solving; they also had fewer behavior reports during incarceration and lower recidivism following release although these differences were not statistically significant. Two Korean studies of an SFBT group intervention found it resulted in significantly lower stress and improved coping among delinquents (Ko, Yu, & Kim, 2003), and significantly reduced aggressiveness among youth probationers (Shin, 2009).
Crime and Delinquency.

Note. SFBT = solution-focused brief therapy.
Gray shade = alternative treatment.
aP = presession change, G = goals, M = miracle question, S = scaling question, E = exceptions, R = relationship questions, B = consulting break, C = compliments, H = homework, F = focus on what is better.
bR = randomized, M = matching, S = selection criteria, L = large sample (20+ per group), F = fidelity assessment, A = alternative treatment, E = experienced therapists, O = objective measures, F = follow-up.
c0 = no change/difference; + or − = positive (desired direction) or negative trend; +* or −* = statistically significant positive or negative change; ≈ = approximately equal.
In the only study with adult offenders, Lindfors and Magnusson (1997) found that a social networking SFBT intervention with high-recidivism Swedish prisoners resulted in significantly lower recidivism 1 year later—53% versus 76% for the untreated controls.
All four of the studies involving juvenile and adult offenders found statistically significant improvements due to SFBT. Most notably, the Swedish study of adult prisoners (Lindfors & Magnusson, 1997) found a significant decrease in recidivism over a 1-year follow-up period, an objective and ultimately important outcome. All of the studies had sample sizes of 20 or larger, three used random assignment, and three used relatively complete implementations of SFBT. Together these findings provide credible evidence that SFBT can be effective with these populations.
Discussion and Applications to Social Work
Overall Effectiveness of SFBT
Of the 43 studies reviewed, 32 (74%) reported significant positive benefit from SFBT, and an additional 10 (23%) reported positive trends. Only one study reported no observable benefit from SFBT. Limiting the analysis to only randomized studies, 20 of the 24 (83%) showed significant benefit from SFBT, suggesting that the better designed studies provide the strongest evidence of effectiveness. Overall, evidence from the 43 studies suggests that SFBT consistently produces positive benefits to clients across fields of practice.
SFBT consistently produces positive outcomes, but how does that compare with alternative treatments known to be effective? Ten of the 43 studies compared SFBT with alternative treatments; 6 found SFBT to be approximately equivalent to (not significantly different from) the alternative treatment, 1 found SFBT to be significantly superior to the alternative treatment (Paroxetine), and 3 studies showed a trend that SFBT was superior to the alternate treatment (two of these used medication). Most of these comparative studies used random assignment and were otherwise well designed and carried out, lending validity to their results. Thus, not only does SFBT consistently produce positive outcomes, but those outcomes appear to be at least as good as those from a variety of alternative treatments, and better in some instances.
All 43 studies appear to have been conducted by different investigators or groups of investigators, which provides evidence of replicability of results. The most rigorous assessment of replicability occurred in adult mental health where five studies used SFBT with depressed outpatients and used the same outcome measure (Beck Depression Inventory). Four of these five studies showed statistically significant benefit from SFBT and found the results comparable to alternative treatments, providing strong evidence of the effectiveness of SFBT with depressed outpatient populations. The fact that a sizeable number of independent investigators have found positive outcomes suggests that SFBT effects are robust and consistent across diverse fields of practice.
The one study that provides the most rigorous test of effectiveness, as noted earlier, is the Helsinki Psychotherapy Study (Knekt & Lindfors, 2004; Knekt et al., 2008a, 2008b, 2011). This study used a large sample, a randomized design, well-established alternative treatments, highly experienced therapists who had allegiance to their respective approaches, an array of objective and well-established outcome measures, and an extensive follow-up period. The fact that this study found statistically significant benefits from SFBT, comparable to the alternative short-term treatment, further strengthens the reliability of SFBT outcomes.
Together, the above analyses provide strong evidence for the effectiveness of SFBT across a range of fields of practice, and particularly in the field of adult mental health.
Length of Treatment
SFBT evolved as a form of brief therapy and has often been recommended because it can achieve results with less time and cost than other approaches (De Jong & Berg, 2008; de Shazer et al., 1986). Three of the studies we reviewed addressed this issue.
The Helsinki Psychotherapy Study (Knekt & Lindfors, 2004; Knekt et al., 2008a, 2008b, 2011) compared SFBT (average of 10 sessions) with short-term psychodynamic psychotherapy (average of 18.5 sessions), long-term psychodynamic psychotherapy (average of 232 sessions), and psychoanalysis (average of 896 sessions). The two short-term therapies achieved comparable outcomes within 6 months (approximate end of treatment), and improvements in the long-term group did not begin to appear until the second year and by the end of the third year (end of treatment) were significantly better on several of the outcome measures. The psychoanalysis group performed significantly better on several outcome measures at the end of 5 years (end of treatment).
The Helsinki study provides clear evidence that SFBT requires many fewer sessions and usually over a shorter period of time than alternative therapies, however, the longer term therapies showed some incremental benefits later on. There were no data on whether these differences were clinically significant, however. There is also the issue of comparing outcomes of the different treatments at widely different follow-up periods, that is, psychoanalysis outcomes at end of treatment were compared with SFBT and short-term psychotherapy at 4.5 years after end of treatment.
The second of the studies examined the number of sessions needed to achieve recovery in adult mental health outpatients according to the OQ-45 by comparing SFBT delivered by an experienced clinician with open-ended treatment provided by trainees from a previous study (Lambert, Okiishi, Finch, & Johnson, 1998). They found that the trainees needed “almost three times the number of sessions to achieve the outcome attained . . . by the private practice therapist” (p. 67). The third study, a randomized study of fatigued Chron’s disease patients, found 5 sessions of SFBT achieved better outcomes than 10 sessions of a problem-solving therapy, although the differences were not statistically significant (Vogelaar et al., 2011).
These three studies all found SFBT required fewer sessions than alternative therapies, lending support to the assertion that SFBT is indeed briefer and less costly.
Potential Publication Bias
Since we included dissertations (many of them unpublished) in our review we were able to examine the possibility of publication bias, that is, that the published literature tends to include only studies that show positive results, whereas dissertations are completed regardless of positive or negative findings. As best we could determine 17 of the 43 studies were conducted as dissertations, 11 (65%) of which reported significant positive outcomes; this compares with 21 of 26 (81%) nondissertation studies reporting significant outcomes. Seven of the dissertation studies were subsequently published and six (86%) of those reported significant positive outcomes, whereas, only 5 of the 10 (50%) unpublished studies reported significant outcomes.
These data are consistent with the view that there may indeed be a higher rate of null results in studies originally conducted as dissertations, with the implication that the published literature tends not to include studies with null outcomes and therefore makes the evidence of effectiveness appear more consistent than it really is. While we cannot be sure if this is the case in our review, we are convinced that the inclusion of dissertations added useful information, and allowed for the inclusion of well-executed studies which may not have been published.
Implementation of SFBT
An important consideration in evaluating a treatment’s effectiveness is whether it was implemented completely and with fidelity. This is particularly important with respect to SFBT which is still relatively new and evolving to some extent. The first of what might be considered a treatment manual appeared in 2007 (de Shazer et al., 2007), and the first actual manual in 2012 (Trepper et al., 2012), both of these coming after most of the studies in our review had been carried out, so the question of exactly what the SFBT intervention consisted of in the 43 studies is pertinent.
A review of the tables shows that 30 of the studies implemented four to six techniques; four studies implemented three or fewer, and eight studies implemented seven or more techniques. Six techniques were implemented in 25 or more studies: specific goals, miracle question, scaling question, search for exceptions, compliments, and homework. A review of the sources we used to derive our list of SFBT techniques suggests that these six techniques are “core” to the SFBT method, thus it is reasonable to conclude that most of the studies implemented most of the core SFBT techniques, suggesting that treatment fidelity was fairly high.
Clinical Implications
The empirical evidence for SFBT is strong, particularly in the fields of mental health and occupational rehabilitation, thus practitioners can feel confident using SFBT in the context of evidence based practice. This evidence is strongest in the more traditional psychotherapy fields where interventions can be implemented consistently in the office setting, and the outcome measures are well-established (valid and reliable). This is consistent with the fact that SFBT was developed in a clinic setting. There is growing evidence of effectiveness of SFBT in nontraditional settings; however, and we expect the evidence will increase as SFBT becomes better adapted to these settings and the outcomes can be measured more reliably and validly. The evidence base for SFBT is growing and practitioners will want to keep abreast of developments in the future.
There is growing evidence that SFBT is briefer than other approaches. The economic implications of this for funders and policy makers are obvious, but brevity also benefits clients who can achieve their goals sooner and move on with their lives. And, although none of the studies addressed this directly, there is much anecdotal evidence to suggest that clients prefer the practical, time limited, strengths-based approach to intervention that SFBT provides. Client preference is an important consideration in the decision to use an intervention approach.
Studies that had the most complete and consistent implementation of SFBT (used the most techniques) seem to have had the best results. Fortunately, practitioners now have the benefit of a well-developed treatment manual to guide their implementation (Trepper et al., 2012), and we recommend its use highly. The best guarantee of successful results with SFBT is implementing it faithfully as intended.
Limitations
The vote-counting approach used in our analysis classifies a study as “positive” regardless of the size or statistical significance of the results (Higgins & Green, 2011), thus a quasi-experiment showing a nonsignificant trend is given the same weight as a rigorously designed experiment showing clinically significant effect sizes. We have controlled for this by clearly distinguishing positive trends from statistically significant differences. We have tried to supplement this analysis by noting individual studies (e.g., Helsinki Psychotherapy Study) and fields of practice (e.g., mental health; occupational rehabilitation) where the quality of the research is stronger and therefore the results should be accorded more weight. Further, the tables report the design characteristics and significance of results for each study, allowing readers to make their own determination of the relative weight assigned to each of the studies that interest them.
Conclusion
We set out to locate and review all available controlled outcome studies of SFBT in order to evaluate evidence of its effectiveness. We used explicit selection criteria to identify qualifying studies, we systematically abstracted the data from each study to provide a basis for critical review and analysis, and we report the abstracted data from each study so readers so can evaluate them for themselves and reach their own conclusions. Because we included unpublished studies, studies in any language, and studies that would be excluded from a meta-analysis, we believe the findings from our review provide a comprehensive and valid basis for evaluating the effectiveness of SFBT overall, and for the six fields of practice.
Based upon our review of the studies, we conclude there is strong evidence that SFBT is an effective treatment for a wide variety of behavioral and psychological outcomes and, in addition, it appears to be briefer and less costly than alternative approaches.
Our review also makes it clear that the number and sophistication of SFBT studies has steadily increased over the past several decades, and we hope this trend continues. We also hope that the findings from our review provide added incentive to funders and researchers to conduct larger and more rigorous studies, on the order of the Helsinki Psychotherapy Study, to further add to our understanding of SFBT effectiveness and efficiency.
Footnotes
Acknowledgments
We gratefully acknowledge translation assistance provided by Yu-Ling Chiu, Hunhui Oh, Okmi Baik, and Seok Joo Kim.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.