
Abstract
Purpose:
To evaluate the claim, made repeatedly during Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition debates over eliminating the bereavement exclusion (BE), that “uncomplicated” depressive reactions have elevated suicidality like other major depressive disorder (MDD), so exclusions risk missing suicidal cases.
Method:
We found no published evidence assessing suicide risk specifically in uncomplicated depression. Using data from four epidemiological surveys, we calculated suicide attempt rates both concurrently and predictively for those with histories of no MDD, uncomplicated MDD, and standard MDD.
Results:
Both concurrently and predictively, uncomplicated MDD suicide attempt rates were no greater than no-MDD history rates and less than standard MDD rates.
Discussion:
Excluding uncomplicated cases from MDD poses no risk of missing elevated suicidal rates typical of depression. The “suicide” argument used to support BE elimination was spurious.
DSM-5’s Elimination of the Bereavement Exclusion and the Suicide Risk Question
The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) major depressive disorder (MDD) bereavement exclusion (BE) excluded “uncomplicated” depressive reactions during grief from MDD diagnosis, even though the number of symptoms might otherwise qualify the reaction as a depressive disorder. It specified (in somewhat confusing double-negative terms) that, when a depressive episode satisfies the DSM’s symptom and duration criteria for MDD, which essentially require any five of the nine specified symptoms enduring for 2 weeks, but the episode follows the death of a loved one, the episode can be considered a depressive disorder only if:
E. The symptoms are not better accounted for by Bereavement, i.e., after the loss of a loved one, the symptoms persist for longer than 2 months or are characterized by marked functional impairment, morbid preoccupation with worthlessness, suicidal ideation, psychotic symptoms, or psychomotor retardation. (American Psychiatric Association, 2000, p. 356)
The BE was an attempt to avoid false positive diagnoses. Physicians throughout medical history have observed that intense normal sadness in response to life events can include many of the same symptoms of general distress that occur in depressive disorder, but that such stressors can also trigger pathological depressive reactions (Horwitz & Wakefield, 2007). The BE offered guidelines to discriminate the likely normal responses from the likely pathological conditions.
Although the DSM has contained an exclusion for uncomplicated depression during bereavement, there has not been an exclusion for uncomplicated depression in response to any other major stressor (e.g., job loss, marital dissolution, romantic betrayal, financial ruin, and negative medical diagnosis), even though it would appear that the same rationale applies. The unique status of bereavement-related depressions was finally challenged and shown to be indefensible by two studies that demonstrated that uncomplicated depressive reactions to other stressors are very similar to uncomplicated depressive grief reactions on a large range of validator variables (Kendler, Myers, & Zisook, 2008; Wakefield, Schmitz, First, & Horwitz, 2007). At that point, an inconsistency in the DSM was revealed; although bereavement-related and other stressor-related uncomplicated reactive depressive episodes were homogeneous in nature and should be classified similarly, the bereavement-related episodes were classified as normal responses and excluded from MDD diagnosis despite fulfilling standard criteria, whereas the others were automatically considered MDD.
To resolve the inconsistency, either the DSM had to eliminate the BE and classify all the uncomplicated cases as disorders or it had to extend the exclusion to other major stressors and thus have a general “uncomplicated reactive depression exclusion.” So, “eliminate or extend” is how the question about the fate of the BE was ultimately posed by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association, 2013) Task Force itself (Kendler, 2011; Parker, 2013; Wakefield, 2011). Wakefield and colleagues argued for extending the exclusion to other stressors, whereas Kendler and colleagues argued for eliminating the BE. Based on various arguments put forward by those favoring the BE's elimination about the harm an extended exclusion would cause and the harm that the BE itself was already causing, the DSM-5 depressive disorders work group proposed eliminating the BE (Fawcett, 2010). This proposal was perhaps the most controversial of all the DSM-5 proposals, and it triggered a quite vigorous debate (First, 2011; Frances, 2010; Lamb, Pies, & Zisook, 2010; Pies, 2009; Wakefield, 2011; Wakefield & First, 2012; Zisook, 2010, 2013; Zisook, Shear, & Kendler, 2007). In the end, the proposal to eliminate the BE from the DSM-5 diagnostic criteria for MDD was approved by the American Psychiatric Association, and the exclusion was eliminated from DSM-5.
A note added to the text, however, does implicitly acknowledge that the issue of distinguishing normal depressive symptoms during grief from the development of a depressive disorder is general to all stressors: “Responses to a significant loss (e.g., bereavement, financial ruin, losses from a natural disaster, a serious medical illness or disability) may include the feelings of intense sadness, rumination about the loss, insomnia, poor appetite, and weight loss noted in Criterion A, which may resemble a depressive episode.” (American Psychiatric Association, 2013, p. 161). Thus, throughout this article, we address the broader extended exclusion that applies to uncomplicated reactions to all stressors, because that is now the acknowledged alternative to eliminating the BE. It is such a broader exclusion that has been recently receiving empirical support in terms of concurrent and predictive validity (Wakefield, 2013; Wakefield & Schmitz, 2013a, 2013b).
The elimination of the BE is perhaps the most controversial change in the DSM since the decision to eliminate homosexuality back in Diagnostic and Statistical Manual of Mental Disorders, Third Edition (DSM-III; American Psychiatric Association, 1980) because it seems to many to fly in the face of common sense about human nature. Along with other controversial DSM-5 decisions, it will no doubt be raised again as an issue in the planned interim “DSM-5.1” online partial revision to address areas of emerging evidence. Thus, despite the DSM-5 decision, this must be considered an ongoing area of research and debate that has not yet been resolved either scientifically or in terms of what will ultimately appear in the MDD criteria. The stakes are high for research as well as practice, because if diagnostic categories are in fact mixing together conditions of different etiologies some of which result from normal pathways to distress and others due to mental disorders, the results of outcome studies are likely to be less interpretable and decisive. Moreover, further knowledge is needed because clinicians will now be faced with the question of how best to respond to patients who meet the old BE. With the demise of the BE, the responsibility for figuring out how to diagnose and treat such patients has been placed squarely on the clinician’s shoulders. The note added to the criteria indicates the clinician’s judgment must be the arbiter of this decision but offer no criteria by which the clinician—or researchers—can be guided.
Of all the arguments put forward to support the elimination of the exclusion, perhaps the most troubling was the “missed suicidality” argument. It was argued that people who are depressed generally have high suicide rates, so people who are depressed but excluded from MDD diagnosis by the BE are, like others who are depressed, at elevated risk of suicide attempt. Consequently, as a result of exclusion, some might not get the help they need to prevent such attempts. The claim that the BE leads to missing suicidal cases was especially serious, given that the alternative was to expand the exclusion and, it seemed, risk even more missed suicide cases.
In this article, we offer the first in-depth empirical evaluation of whether an extended exclusion of all uncomplicated episodes from MDD does risk diagnostically missing suicidal cases. We first briefly document the use of the “suicide risk” argument by proponents of eliminating the BE, which include some of the leading figures in the field of depression and grief. We review the evidence they cited to support their concern, and we evaluate the relevance and strength of that evidence. We ask whether there was any evidential basis for the claims that were made.
We then proceed to the main task of this article, which is to directly test whether the eliminationists’ claims are true or false. For this purpose, we present an empirical analysis of suicide attempt risk among varying lifetime histories of depression using data from all four of the major publicly available national U.S. epidemiological data sets. We ask what the truth of the matter is about suicide risk and uncomplicated depression. The results should be of interest to suicide researchers and to clinicians in general, beyond those concerned about the narrow topic of the BE.
Suicide is of course a worldwide problem of major proportions and great complexity, which has a vast research literature. Our discussion here is limited to the specific topic of suicide attempt and the BE. We focus on this problem and do not attempt to address the broader problem of suicide.
A caveat is that recent research has confirmed what common sense would suggest, that the current BE’s 2-month duration limitation for normal grief-related depressive feelings is much too short. The DSM-5 mood disorders work group agreed, with the Chair stating that the work group concluded that the 2-month limit was “pulled out of the air. There was no evidence behind it that we can see” (Fawcett, 2012). The exclusion's duration threshold used to be set at a year, and a series of recent empirical investigations of the duration requirement’s validity suggest that that is closer to a valid cut point (Wakefield, Schmitz, & Baer, 2011a, 2011b; Wakefield & Schmitz, 2012). To be conservative, in the analyses presented here we adopt a 6-month durational threshold for reclassifying an otherwise uncomplicated episode as MDD. This is the only way our criteria diverge from those of the DSM.
Claims of Elevated Suicide Risk Among BE-Excluded MDD: Evaluating the Cited Evidence
We start by reviewing the claims put forward by proponents of BE elimination about suicide risks due to the BE, and evaluating the evidence they cited in support of their statements. The use of suicide risk to argue for pathologizing all depressive feelings during grief goes back at least to 1993, when Zisook and Schuchter (1993) published their second article on the results of a longitudinal study of depression in widows and widowers. On the basis of that study’s findings, they argued for eliminating the BE in DSM-IV. Referring to their reported results, Zisook and Schuchter stated, “Among those bereaved who had a major depressive syndrome at 2 months, feelings of worthlessness, thoughts of death, and actual thoughts of ending their lives were frequent” (1993, p. 370). Before addressing the suicide risk claim, it should be noted that this argument is confused as an argument against the BE because individuals manifesting worthlessness or suicidal ideation would by definition not be considered uncomplicated MDD and would not be excluded from MDD by the BE in the first place.
With regard to suicidal ideation, Zisook and Schuchter’s statement about suicide risk in depression during grief did not match their own data reported in the same article. Zisook and Schuchter claimed that among the depressed, “actual thoughts of ending their lives were frequent.” However, looking at their table 2 (1993, p. 368), among those satisfying MDD criteria at 2 months, 5% (N = 3) reported suicidal ideation, whereas among those not satisfying MDD criteria, 2% (N = 4) reported suicidal ideation, a difference that was not statistically significant. They report these same Ns and percentages of suicidal ideation for MDD and non-MDD groups 1 year later, so likely these are the same individuals with ongoing suicidal ideation but still with no significant difference at 13 months between the groups who were versus were not depressed at 2 months. Contrary to Zisook and Schuchter’s statement, their own data indicate that suicidal ideation in the bereaved is not significantly elevated among the depressed group in comparison to those without depression.
In the debate over the BE in DSM-5, Zisook has continued to argue that the risk of suicide among BE-excluded cases is a reason for eliminating the BE. In a review article, Zisook, Shear, and Kendler (2007) cited the risk of suicide as a reason for not waiting for depressive feelings that are excludable to subside on their own without early treatment:
[E]arly treatment of depression may be vitally important. For example, a recent study demonstrated that both lack of a partner and time in depression were significant predictors of suicidality among people meeting criteria for MDE (21). These findings, along with data indicating that early depression responds well to antidepressant medication, underscore the fact that the validity of the bereavement exclusion for the diagnosis of MDE is not an academic issue. (p.104)
The study cited by Zisook, Shear, and Kendler (2007) to support their concern about BE suicide attempt risk is an 18-month follow-up study of 269 MDD hospital inpatients and outpatients (Sokero et al., 2005). The sample includes highly pathological cases, of whom “preceding the follow-up phase, 15% of the cohort had attempted suicide during the index episode and 24% before that” (pp. 316–317), so that more than half of suicide attempters during follow-up had attempted suicide during or before the index episode. Moreover, mean time in depression for attempters was 8.6 months, and DSM-IV BE-excluded cases (even allowing our 6-month maximum duration) would not generally approach this duration. Finally, this generally highly pathological sample included few individuals with mild depressions, but among the mild cases none attempted suicide—an enlightening result, given that Zisook, Shear, and Kendler suggest that bereavement-related depressions are often mild (p. 105). So, on multiple grounds, the cited data are inappropriate and misleading in an argument about potential suicidality in BE-excluded cases.
The logic of Zisook et al.’s argument seems to be that depressed people without partners are generally more likely to commit suicide, and individuals grieving the loss of their partners do not have partners, thus depressed bereaved individuals are at elevated risk for suicide, thus BE-excluded cases—which are bereaved and depressed—are at elevated risk for suicide. This reasoning ignores the crucial fact that BE-excluded individuals are specifically selected to avoid suicide risk by prohibiting suicidal ideation and other risky symptoms. Zisook et al.’s generalizations based on a severe population with ample previous suicide attempts are not relevant to assessing the suicide risk in the BE group.
In another study by Shear et al. (2011), on which Zisook was a coauthor, the authors explain why they agree that the BE should be eliminated. They argue that early intervention even during acute grief is warranted because “Bereavement may increase the risk of suicide. [148,149] Earlier treatment to reduce suicide risk is likely the most effective long term preventative intervention available [150,151]…” (Shear et al., 2011, p. 111). Like Zisook et al., Shear et al. infer from a general suicide risk in bereavement that there must be an elevated suicide risk in excluded cases but fail to mention that BE exclusion requires that there be no suicidal ideation and also screens for many other relevant indicators, such as a sense of worthlessness. Shear et al. cite two references to support their contention that bereavement poses a suicide risk (Ajdacic-Gross et al., 2008; Stroebe, Stroebe, & Abakoumkin, 2005). Both studies concern increased suicide risk in general during bereavement, and neither address cases in which suicidal ideation is absent or that meet the BE’s criteria for exclusion. Thus, both are simply irrelevant to assessing suicidal risk in uncomplicated cases. Shear et al. also cite two studies about the usefulness of early treatment for prevention of suicide in general, not bereavement-related suicide let alone uncomplicated depression lacking in suicidal ideation. These are vacuous citations introduced without scholarly thoughtfulness about exactly the point the citations support.
To appreciate the degree of lack of fit between Shear’s point and her citations, consider her citing Stroebe, Stroebe, and Abakoumkin (2005) who compared a group of 60 bereaved individuals to married controls and concluded, “Bereaved persons are at excess risk of suicidal ideation compared to nonbereaved people. Heightened suicidal ideation in bereavement is associated with extreme emotional loneliness and severe depressive symptoms” (p. 2178). First of all, Stroebe et al.’s entire study is based on suicidal ideation as a proxy for suicidality, but suicidal ideation is not allowed in the excluded cases that are Shear et al.’s target, so the study is not relevant. Indeed, Stroebe et al. remark that “Although few of those with suicidal ideation will act on their thoughts, ideation would seem a precursor to suicidal acts” (2005, p. 2178), in effect affirming the effectiveness of an ideation question for screening out suicide attempt. Second, the heightened suicidal ideation that Stroebe et al. found in bereavement is associated with severe depressive symptoms but not more moderate depressive symptoms, whereas excluded cases are very unlikely to have severe depression. So, once again, the findings of the study do not fit the context of their citation.
In a further article, Shear (2011) defends the elimination of the BE by asserting that major depression in the context of bereavement resembles other major depression, that the standard DSM depression criteria have been developed by experts and stood the test of time and thus should be applied during bereavement, that “negative consequences have not been found to be lower or different in any way when depression occurs in response to a life event,” and that “among the things we have learned are that MDD is associated with a high mortality from suicide (as many as 15% of people with severe MDD die by suicide).” She thus implies that one might conceivably expect a 15% suicide rate or similarly heightened rate among BE-excluded cases, because they too satisfy the standard DSM MDD criteria. No citation is provided for these startling claims about suicide potential. However, the source of the 15% rate is well known (Guze & Robins, 1970) and has long been repudiated (Bostwick & Pankratz, 2000). It was the rate for a very severe population of hospitalized depressed individuals many of whom had bipolar disorder, and the statistics were biased in several other ways as well. For outpatients satisfying DSM MDD criteria, the suicide rate is closer to 2% (Bostwick & Pankratz, 2000). For uncomplicated depression in the general population, the rate is unknown until the present study. That Shear thinks that the 15% rate is relevant to the BE population indicates that she is assuming homogeneity between the BE-excluded cases and other MDD, including the most severe cases.
The claim by those who defend the BE is that stress-related uncomplicated depressive episodes are a different and less pathological kind of condition from standard MDD. Consequently, citing generalizations about standard MDD to argue for the pathologicality of uncomplicated cases without any further evidence, as the eliminationsts regularly do, directly begs the question at issue.
Zisook (2010), in arguing for elimination of the BE, said to a general audience on public radio that “I’d rather make the mistake of calling someone depressed who may not be depressed, than missing the diagnosis of depression, not treating it, and having that person kill themselves.” His assertion ignored the screening for suicidal ideation that is built into the assessment for exclusion, and he offered no evidence to back up his concern about suicidal cases among uncomplicated depression. Such public assertions without scientific basis are inappropriate in our view. Nor has he abandoned these claims and pronouncements with time. In a recent Scientific American blog explaining why the BE was eliminated, Zisook (2013) states that BE-excluded cases are “sometimes life-threatening.”
We conclude that proponents of eliminating the BE claimed there is a threat of suicide in excluded bereavement-related depressions with no specific evidence about BE-excluded cases to back up their assertions, citing as evidence studies that do not support the specific claims about uncomplicated depression that they made. They also ignored the compelling counterargument that excluded cases are already screened for suicidal ideation.
However, lack of evidence for a claim is not evidence against the claim. Rhetoric aside, is there any scientific evidence pertaining to the suicide risk in uncomplicated depression? The only previously published evidence we know of comes from our own studies of uncomplicated depression. That evidence, while slim, provides no basis for supposing an elevated suicide rate in bereavement-excluded depression and suggests the opposite.
For example, among those individuals who had only DSM-IV-excludable bereavement-related depressions in the National Comorbidity Survey (NCS; N = 31), not one reported a lifetime suicide attempt (Wakefield & Schmitz, 2013c). Similarly, for all nonbereavement uncomplicated cases in the NCS using a 6-month instead of 2-month duration threshold (N = 169), there are no suicide attempts (Wakefield & Schmitz, 2013a). This is the best data available until now, and it suggests that the screening for suicidal ideation is effective in eliminating suicide attempt cases from excluded cases.
However, the issue that is of concern to the eliminationists is not just that at the time of diagnosis a patient might be concurrently suicidal, but that in the period after the person is excluded from diagnosis their depressive feelings might develop into suicidality. The NCS data analyses used cross-sectional lifetime measures, so in principle, they cover the situation in which an uncomplicated depressive episode occurs at one time and suicide attempt develops later. Nonetheless, on this key and clinically crucial point, longitudinal studies would be more reassuring. The subject clearly requires both more comprehensive concurrent analysis and a predictive study that evaluates excluded cases at some time after diagnosis. We now turn to an epidemiologic analysis that addresses the questions of whether there are elevated concurrent or predictive suicide attempt risks in BE-excluded individuals.
Aims of the Study
This study addresses four questions about the risk of suicide in those with uncomplicated depression, whether bereavement related or other stressor related:
Concurrent validity of the BE criteria. How often do uncomplicated cases attempt suicide concurrently with their diagnosis? Does uncomplicated status effectively screen out those at risk of suicide attempt during the given episode?
Predictive validity of the BE criteria. How often do uncomplicated cases attempt suicide subsequent to their diagnosis? Does uncomplicated status effectively screen out those at risk of future suicide attempt?
Concurrent and predictive validity of the “no suicidal ideation” component. Does “no suicidal ideation” by itself successfully screen out those at risk of suicide attempt during the given episode and over time?
Concurrent and predictive validity of the rest of the criteria for uncomplicated depression, without the “no suicidal ideation” requirement. Is the screening benefit of the uncomplicated criteria due entirely to the no suicidal ideation component, or do the rest of the BE criteria add something?
Method
Samples
To evaluate the risk of suicide attempt among uncomplicated MDD cases, we used four separate data sets. Due to methodological differences between the data sets, we analyzed them separately, rather than pooling them into a single data set. All four data sets allowed us to test the concurrent validity of the uncomplicated/complicated distinction. In addition, two of the data sets are longitudinal in nature and allowed us to test the predictive power of the uncomplicated depression exclusion to indicate future suicide attempts subsequent to the initial diagnosis. To keep the analyses comparable across data sets, all of the analytic samples that we used were restricted to adult respondents between the ages of 18 and 54. To avoid confounding suicidality in bipolar disorder with suicidality in major depression, we eliminated bipolar cases from all of the samples.
Three of the four data sets utilized “skip out” procedures, such that if the respondent did not answer “yes” to having had the depression screener symptoms (sadness or loss of interest) then the respondent was not asked further depression questions about specific symptoms, including about suicide attempt. Thus, we could not validly estimate suicide attempt rates relative to the overall samples of the surveys because many had not been asked the relevant question. However, all four data sets asked the relevant suicide attempt questions if the respondent answered “yes” to having a period of sadness or loss of interest, so we estimated all rates relative to those reporting some period of sadness. (In one case, the National Comorbidity Survey–Replication [NCS-R], the “attempt” question was only asked of those who had experienced sadness if the “ideation” question had been answered “yes,” so we could not compare suicide attempt risk among those having and not having ideation.) Data were weighted to account for selection and nonresponse effects and to provide nationally representative estimates. Statistical analyses (one-tailed or two-tailed t-tests depending on the context) were performed using the survey estimation procedures in Stata 12 (Stata Corporation, 2011), which calculate weighted coefficients and use Taylor series linearization to calculate standard errors.
Cross-Sectional Data Sets
Two data sets were used exclusively for the tests of the concurrent suicide attempt hypotheses. First, the National Comorbidity Survey (NCS) is a community-based epidemiological survey administered between September 14, 1990, and February 6, 1992, to 8,098 persons aged 15–54 years who are representative of the U.S. population (Kessler et al., 1994). After removing bipolar cases and selecting those of age 18–54 who reported a sadness episode, the analytic sample consisted of 4,070 cases. Second, the National Comorbidity Survey-Replication (NCS-R), also a community-based epidemiological survey of a nationally representative U.S. sample, was administered between February 2001 and December 2002 to 9,282 persons of age 18 years or older (Kessler et al., 2003). After removing all bipolar cases and selecting those of age 18–54 who reported a sadness episode, the analytic sample consisted of 4,060 cases.
Longitudinal Data Sets
Two additional data sets were longitudinal and were used to evaluate hypotheses about both the concurrent and the predictive power of the BE to indicate suicide attempts. Here, we used longitudinal community data from the two-wave Epidemiologic Catchment Area Study (ECA; Robins & Regier, 1991) as well as the longitudinal community data from the two-wave National Epidemiologic Survey on Alcohol and Related Conditions (NESARC; Grant et al., 2009).
The ECA sampled respondents aged 18–98 at five sites (Baltimore, Durham, Los Angeles, St. Louis, and New Haven). Respondents were interviewed face to face twice, approximately 12 months apart (Wave 1 and Wave 2), between 1980 and 1985. Lifetime and 1-year DSM-III diagnostic data were obtained at both waves. We restricted the overall sample to cases between the age of 18 and 54 who reported no bipolar episode in their lifetime and reported a sadness episode, and because we were interested in whether suicide attempt would occur at a time subsequent to the remission of the index diagnosed episode, we eliminated cases in which one episode overlapped between the two waves. For the analyses of concurrent validity, only Wave 1 information was required, resulting in an analytic sample of 3,135 cases. For the analyses of predictive validity, our analytic sample includes only cases with valid responses at both waves, and our restrictions yielded an analytic sample of 2,118 cases.
Finally, we used longitudinal community data on the general U.S. population from the two-wave NESARC. A structured diagnostic instrument was administered to respondents aged 18 and older in two face-to-face interviews 3 years apart (Wave 1 and Wave 2) between August 2001 and September 2005. We restricted the sample to those of age 18–54 who had no lifetime bipolar disorder and no continuous episode across waves and to those who reported sadness episodes. As in the ECA, only Wave 1 information was required for the NESARC concurrent validity tests, with an analytic sample of 7,963 cases. For the analyses of the predictive validity hypotheses, valid responses from both waves were required; and with our restrictions applied, the analytic sample consisted of 2,398 cases.
MDD Diagnostic Criteria
The four data sets each used the version of the DSM diagnostic criteria for MDD that was available at the time the data were collected. The different versions were mostly consistent in that a respondent must report at least one symptom from each of the five or more symptom groups, with one of the five endorsed symptoms being from the sad/blue/gloomy group or the group with loss of interest in usual activities (the depressive episode screener questions). These symptoms could not be due to organic causes or psychotic episodes, and the respondent never had mania or hypomania.
The ECA used criteria from the DSM-III, which did not include the now-standard “distress or role impairment” criterion assessing clinical significance. However, the diagnostic algorithm of the ECA incorporated a severity criterion based on service use or interference with life that was applied at both the symptom and syndrome levels, likely resulting in identifying more severe cases of MDD than would result from applying the current clinical significance criterion.
The NCS used criteria from the DSM-III-R (American Psychiatric Association, 1987), which also did not contain criteria for assessing a clinical significance criterion. Both the ECA and the NCS incorporated DSM-based BEs for their respondents. However, we suspended the BE for each of these data sets in order to examine the entire set of uncomplicated depressions including the bereavement-related ones and thus made all the data sets comparable in this regard.
The NCS-R and the NESARC both used DSM-IV criteria for identifying cases of MDD and thus included a clinical significance criterion. However, the NCS-R did not ask about bereavement triggers at all and did not incorporate a BE. The NESARC created a distinct BE based on identifying brief, bereavement-triggered depressive episodes. As with the ECA and NCS, we suspended this criterion in the NESARC to allow for a more comparable analytic sample and to address the question of the relation of uncomplicated MDD to suicide attempt.
Uncomplicated Versus Complicated Depressive Episodes
To address concurrent predictive validity, we divided respondents who answered affirmatively to at least one of the depression screener questions (sadness, loss of interest) into three groups: no history of MDD, uncomplicated MDD, and all other MDD (or “complicated” MDD). The no history group did not meet criteria for MDD, even though they had reported having a sadness episode. The uncomplicated MDD group was identified based on DSM-IV criteria for the BE but applied to all MDD cases and using an adjusted duration limit of 6-month duration rather than the DSM-IV’s 2-month limitation. Thus, we identified an episode as uncomplicated MDD if the respondent met the symptom and duration criteria for MDD but did not have any of the following symptoms during the target episode: sense of worthlessness, suicidal ideation, psychotic ideation, marked functional impairment, psychomotor retardation, and episode duration greater than 6 months. The “all other MDD” (or “complicated MDD”) group consisted of all MDD cases that did not meet the criteria for uncomplicated MDD, that is, possessed one or more of the six listed pathosuggestive symptoms.
Suicidal Ideation
To address the effectiveness of the no suicidal ideation requirement for uncomplicated episode by itself, we also examined whether respondents reporting no suicidal ideation during the depressive episode possessed an elevated risk of attempting suicide, and whether this feature of the uncomplicated criteria fully explained the risk of suicide attempt by those with uncomplicated depression. As such, we divided the cases meeting criteria for MDD into two groups, those reporting suicidal ideation during the depressive episode (e.g., in NESARC: “During that time when your mood was at its lowest, did you think about committing suicide?”) and those not reporting suicidal ideation, and calculated the rates of suicide attempt (e.g., in NESARC: “During that time when your mood was at it’s lowest, did you attempt suicide?”) in each group. However, the NCS-R data set was not suitable for this analysis, because the interview structure was set up so that respondents were only asked about attempting suicide if they answered affirmatively to a question regarding suicidal ideation, making it impossible to analyze suicide attempt for those not reporting suicide ideation. So, the analyses regarding the impact of suicidal ideation were limited to the ECA, NCS, and NESARC data sets.
Results
Age and gender for the different MDD groups for the four data sets are presented in Table 1. In the ECA and NESARC data sets, there were higher proportions of females in the two MDD groups, compared with the no history of MDD group, but for the NCS and NCS-R data sets, that difference was only significant between the no history of MDD group and the all other MDD group. The mean age in all groups was around 34 years, with a few slight differences between groups.
Percentage Female, Mean Age for Each Group.

Note. MDD = major depressive disorder; ECA = Epidemiological Catchment Area; NCS = National Comorbidity Survey; NCS-R = National Comorbidity Survey–Replication; NESARC = National Epidemiologic Survey on Alcohol and Related Conditions; n = group sample size. The 95% confidence intervals are shown in brackets. All Other MDD: at least one complicated symptom (worst time of sadness/lost interest): move or talk much more slowly than usual; feel worthless nearly all the time; think about committing suicide; marked impairment; duration of longest episode greater than 6 months. The ECA does not use impairment in the criteria for complicated symptoms, because of the questionnaire structure within the syndrome severity questions. No History MDD: answered screener question “yes,” but did not meet MDD criteria. Bipolar cases removed from all samples; age restricted to 18–54 years.
Superscript letters indicate significant difference, p < .05, two-tailed t-test.
Concurrent Validity
The results from all four data sets for the analyses of concurrent validity of the criteria for uncomplicated MDD are presented in Figure 1. The criteria clearly confirm the concurrent validity of the uncomplicated/complicated distinction in indicating suicide attempt. There are two crucial findings. First, the idea that the uncomplicated group has an elevated suicide attempt rate that should be of concern is clearly refuted. In all four data sets, the uncomplicated groups have substantially lower suicide attempt rates than the no-MDD history groups. In three of the four data sets, the uncomplicated rate is significantly lower than the no history rate (ECA, 0.1% vs. 5.2%; NCS, 0.6% vs. 2.0%; NCS-R, 0% vs. 0.5%); and in the fourth, it is substantially though not quite statistically significantly lower (NESARC, 1.8% vs. 3.2%). Thus, uncomplicated cases actually have less chance of suicide attempt than a random member of the general population who has felt sad for a period. Effect sizes assessed as Cohen’s d for these results were small to moderate in size, ranging from .02 (NESARC) to .33 (ECA).
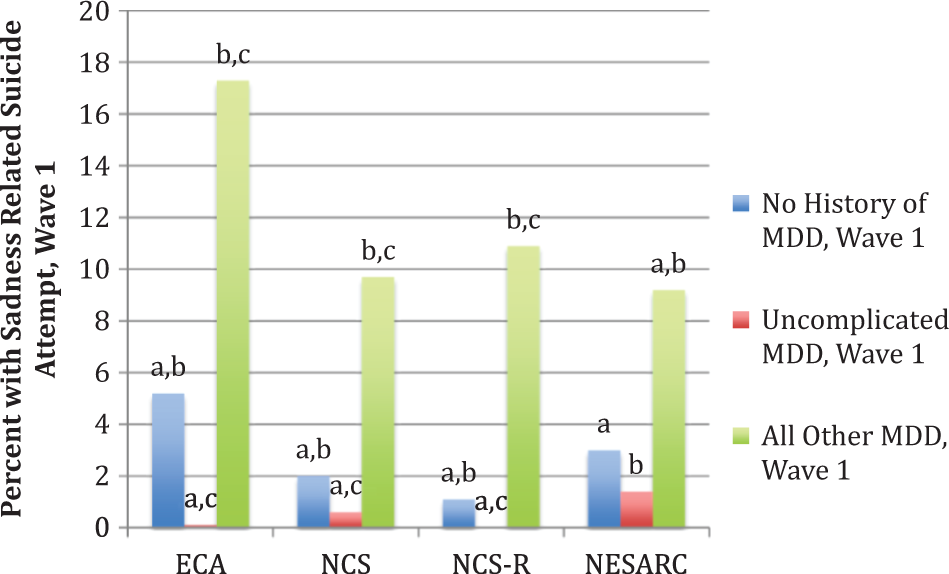
Among those who reported sadness episodes, the percentage who attempted suicide during the index episode for those with varying lifetime MDD histories in the given community study (concurrent analysis; only the first wave of the longitudinal data sets was used). Samples restricted to age 18–54 years. Letters at the top of the columns indicate significant differences between the specific groups, p < .05, one-tailed t-test. Suicide attempt: only examined for respondents answering affirmatively to at least one depression screener question. No history of MDD group answered affirmatively to a depression screener question but did not meet MDD criteria. Criteria for uncomplicated MDD: none of move or talk more slowly than usual; feel worthless nearly all the time; thought about committing suicide; marked impairment; psychotic ideation; duration greater than 6 months. MDD = major depressive disorder; ECA = Epidemiological Catchment Area Study; NCS = National Comorbidity Survey; NCS-R = National Comorbidity Survey-Replication; NESARC = National Epidemiologic Survey on Alcohol and Related Conditions.
Second, in all four data sets, both the uncomplicated and the no history groups have substantially and significantly lower risk of suicide attempt than do all other MDD, with generally moderate effect sizes found in the comparisons (Cohen’s d ranging from .18 to .30). The other MDD have rates ranging from about 9% to about 17%, confirming the high suicide attempt potential of depressive disorder. However, this standard feature of depression does not apply to uncomplicated depression, which has no elevation (and actually the opposite) relative to those with a sadness episode but no MDD at all.
The question then arises as to whether the concurrent results for suicide attempt are due strictly to the fact that no suicidal ideation is one of the criteria for uncomplicated depression, or whether the other uncomplicated criteria play a role. For concurrent validity, Figure 2 shows the suicide attempt rates for those who did versus did not have suicidal ideation. For all four data sets, the rate of suicide attempt among those who experienced suicidal ideation approached about a quarter of the group (between about 23% and 26%). In contrast, the rates for those without suicidal ideation in the three groups for which this could be calculated (other than the NCS-R) are significantly lower and extremely small by comparison (between 0.1% and 0.6%), confirming that suicidal ideation is a powerful predictor of risk of suicide attempt (Cohen’s d values—ECA: .50; NCS: .31; NESARC: .45). Of great interest is the fact that, for the group reporting sadness episodes, suicidal ideation is a more powerful predictor of suicide attempt than is MDD status.

Among those who reported sadness episodes, the percentage who attempted suicide during the index episode for those with versus those without suicidal ideation in the index episode in the given community study (concurrent analysis; only the first wave of the longitudinal data sets was used). Samples restricted to age 18–54 years. Asterisks at the top of the columns indicate significant differences between the two groups, p < .05, one-tailed t-test. Suicide attempt: only examined for respondents answering affirmatively to at least one depression screener question. The NCS-R skipped the suicide attempt question for all persons reporting not having thought about suicide, so there were no cases in the “do not have suicidal ideation” group for that data set. ECA = Epidemiological Catchment Area Study; NCS = National Comorbidity Survey; NCS-R = National Comorbidity Survey-Replication; NESARC = National Epidemiologic Survey on Alcohol and Related Conditions.
Comparing rates across Figures 1 and 2, in two data sets, the concurrent rates for “no suicide attempt” in Figure 2 do not differ significantly from the rates for uncomplicated depression in Figure 1. However, in the third case (the ECA), the rate for uncomplicated depression is significantly lower than the rate for no suicidal ideation alone, suggesting an additional impact of other uncomplicated symptoms. Thus, although for concurrent prediction of suicide attempt it appears that no suicidal ideation is doing the lion’s share of the work, it also appears that the rest of the uncomplicated criteria have some incremental validity in predicting lowered suicide attempt rates.
This raises the question of whether the rest of the uncomplicated criteria by themselves predict low suicide attempt rates. To answer this question, we performed a post hoc analysis in which we recalculated the rates of suicide attempt for the uncomplicated group in each of the four data sets after taking the no suicidal ideation requirement out of the diagnostic criteria set. We found that, despite this change, in no case was the revised suicide attempt rate greater than the no history rates. On the other hand, with the no suicidal ideation criterion removed, there were no significant difference between uncomplicated and no history suicide attempt rates in any of the data sets (analyses not shown), whereas before the uncomplicated rate had been significantly lower in three cases. We conclude that the other criteria do have an impact of their own, independent of no suicidal ideation. This makes sense because, for example, criteria like “no sense of worthlessness” would be expected to independently predict less suicide attempt risk.
Predictive Validity
Our predictive analyses involve both 1-year (ECA) and 3-year (NESARC) follow-up periods. This sort of analysis addresses the possibility that exclusion of uncomplicated depression from MDD diagnosis might miss subsequently emerging cases of suicidal feeling. One can imagine that some cases are not manifesting ideation at the time of diagnosis but are inclined to develop it later. If concerns about missing suicidal cases due to an uncomplicated depression exclusion should be supported in the data, it is in the predictive analysis that one would expect it to be most likely to do so. However, the results point in a different direction.
The predictive validity of the uncomplicated/complicated distinction is strongly confirmed (Figure 3). There are again two crucial findings. First, uncomplicated depression predicts substantially and significantly less suicide attempt than does no MDD history. Thus, the claim that uncomplicated depression has elevated suicide attempt rates over the general population is disconfirmed, and indeed the opposite is true. Whether looking ahead 1 year or 3 years, uncomplicated MDD cases have much less of a chance of suicide attempt than do random members of the general population experiencing sadness episodes. Second, there is a substantial and significant difference between the suicide attempt rates of uncomplicated versus all other depression, although with somewhat smaller effect sizes than were found for some of the concurrent validity tests (Cohen’s d: ECA: .07; NESARC: .14). The standard view that depression is associated with elevated risk for subsequent suicide attempt is upheld but not with respect to the subtype of uncomplicated depression.
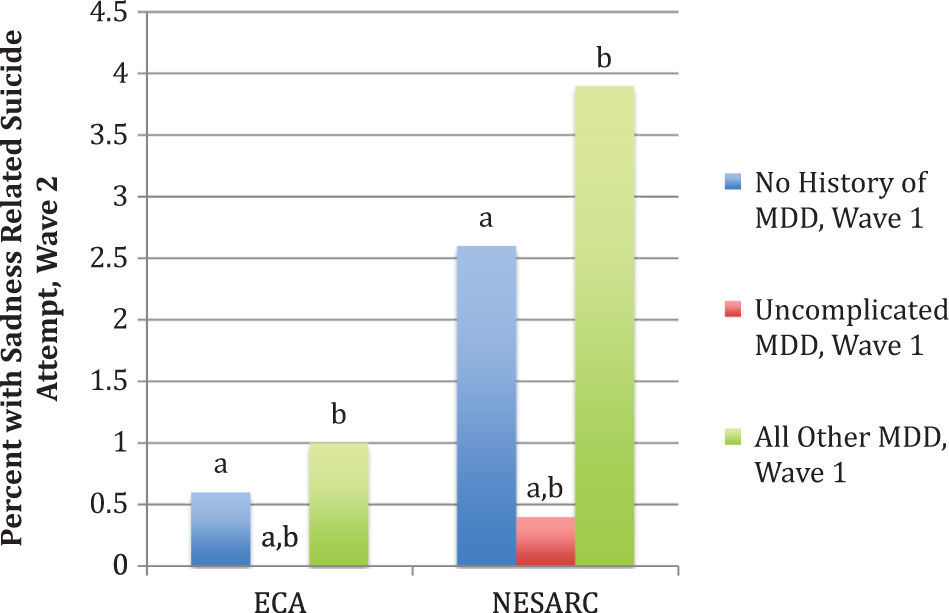
Among those who reported sadness episodes, the percentage who attempted suicide during the follow-up Wave 2 of the given community study for varying lifetime MDD histories at Wave 1. Samples restricted to age 18–54 years. Letters at the top of the columns indicate significant differences between the specific groups, p < .05, one-tailed t-test. Suicide attempt: only examined for respondents answering affirmatively to at least one depression screener question. No history of MDD group answered affirmatively to a depression screener question but did not meet MDD criteria. Criteria for uncomplicated MDD: none of move or talk more slowly than usual; feel worthless nearly all the time; thought about committing suicide; marked impairment; psychotic ideation; duration greater than 6 months. MDD = major depressive disorder ECA = Epidemiological Catchment Area Study; NESARC = National Epidemiologic Survey on Alcohol and Related Conditions.
One surprising result is that, unlike the results for concurrent validity, the predictive validity rates for no-MDD history and complicated MDD are not significantly different in either data set. Over time, the difference between initial lifetime depression and nondepression when it comes to suicide attempt is ameliorated to the point that within the 1- to 3-year framework of the follow-up periods the chances of a suicide attempt are not influenced by whether or not one had a previous lifetime depressive episode. Yet, if one had a lifetime uncomplicated depression, it does influence the outcome over several years. In both data sets, the rates for uncomplicated depression remain significantly below both those who had other depressions and those who had no depression. During the follow-up periods, someone who had remitted from an uncomplicated depression actually had significantly and substantially less of a chance over the next year or 3 years of attempting suicide than someone from the general population.
One would like to know whether this striking result is due entirely to the use of the screener no suicidal ideation when diagnosing uncomplicated depression or has something to do with the broader criteria that prohibit other symptoms that might be related to long-term suicide risk such as sense of worthlessness and psychomotor retardation. To explore this question, we first reanalyzed the predictive data dividing the sample into “no suicidal ideation” versus “suicidal ideation” groups. The results are presented in Figure 4. In both data sets, the no suicidal ideation group is significantly and substantially lower than the suicidal ideation groups in later suicide attempts (ECA 1-year follow-up, 0.4% vs. 1.5%; NESARC 3-year follow-up, 2.2% vs. 6.7%, both significantly different at p < .05 level, but with relatively smaller effect sizes; Cohen’s d: ECA: .08; NESARC: .16).

Among those who reported sadness episodes, the percentage who attempted suicide during the follow-up Wave 2 of the given community study for those with versus those without suicidal ideation at Wave 1. Samples restricted to age 18–54 years. Asterisks at the top of the columns indicate significant differences between the two groups, p < .05, one-tailed t-test. Suicide attempt: only examined for respondents answering affirmatively to at least one depression screener question. ECA = Epidemiological Catchment Area Study; NESARC = National Epidemiologic Survey on Alcohol and Related Conditions.
In a post hoc analysis, we reanalyzed the data after eliminating no suicidal ideation from the uncomplicated criteria. The results were that despite this change the uncomplicated depressed had significantly lower suicide attempt rates than did the other MDD, and their rate was still either lower (ECA) or not higher (NESARC) than the no history rate. Indeed, for both data sets, the suicide attempt rates for uncomplicated depression calculated with the standard criteria including no suicidal ideation were not significantly different from the rates calculated without using that criterion (analyses not shown). Clearly, it is not just the no suicidal ideation requirement but also the rest of the uncomplicated criteria that are playing a major role in reducing later suicide attempt rates.
The useful impact of the other uncomplicated criteria as screeners is brought home if one compares the rates across Figures 3 and 4. For both data sets, the predictive suicide attempt rates are significantly lower for uncomplicated depression than they are for no suicide ideation applied alone. Using the full uncomplicated criteria thus has incremental validity over the ideation screener alone in excluding from MDD those with the lowest possible risk of later suicide attempt.
Discussion and Applications to Social Work
We used four major epidemiological data sets to explore the relationship between uncomplicated depression and suicide attempt risk among those who experienced a period of sadness. Our results decisively falsify the claim, made by proponents of elimination of the BE in DSM-5, that exclusion of uncomplicated depression would risk missing suicidal MDD cases. In terms of both concurrent risk during the uncomplicated episode and predictive risk over 1- and 3-year follow-up periods, our results indicated that those depressive episodes that satisfy the demanding requirements for being uncomplicated depression predict rates of suicide attempt that are no more than, and often less than, those of the general population. The no suicidal ideation component of the uncomplicated criteria by itself reduced suicide attempt rates to background population levels, but the additional uncomplicated criteria reduced it further.
In the course of our examination, it emerged that the standard wisdom that suicidal ideation is an excellent predictor of suicide attempt was strongly confirmed. It turned out to be simply false that excluding uncomplicated depression from MDD diagnosis poses a risk that the elevated rates of suicide among MDD patients will lead to missing suicidal cases, because uncomplicated depression does not share the elevated MDD rates. Proponents of BE elimination in effect engaged in fear mongering in raising the specter of suicide without any relevant evidence.
This study is unusually strong in using all four of the major nationally representative epidemiologic data sets available for public use, including four that allow for estimating rates of concurrent within-episode suicide attempt and two that allow for estimating the suicide attempt rate over a follow-up period. The study has several limitations, however. Due to the idiosyncratic skip patterns in the data sets, we could not present overall population rates, but rather presented rates within the set of respondents who reported periods of sadness. A major limitation is the use of suicide attempt rates as a proxy for suicide rates, although this is a common practice. Furthermore, all four of the studies used in this analysis were (in their first waves in the case of the longitudinal studies) cross sectional and relied on the memory of the respondent, which can be fallible.
Our results strongly diverged from the claims of those who favored the elimination of the BE and from the results of the studies they cited in support of their claims. This is because those studies did not actually address uncomplicated depression at all and are irrelevant to the issue they were claimed to address. Our study, in contrast, directly examines the issue of suicide attempt in uncomplicated depression. Despite all the citations by eliminationists, there have been no previous direct studies of this issue.
As a conceptual caveat, it should be noted that in this analysis we have not explicitly linked the suicide attempt question to the broader issue of whether uncomplicated cases are suffering from intense normal sadness or a depressive disorder. We did not assume that elevated suicide rates imply depressive pathology rather than normal sadness or that lack of elevated rates indicated the contrary. From a strictly conceptual perspective, the link is not ironclad. Other features, such as recurrence rates, would certainly have to be assessed in such an argument. Moreover, normal conditions can certainly elevate suicidal ideation or attempts; normal bereavement is commonly associated with thoughts of wanting to join the lost individual and a sense of meaninglessness that can increase the likelihood of suicidal ideation, and stressed or humiliated individuals may entertain nondisordered rationales for attempting suicide.
Nonetheless, suicidality is generally viewed as a prima facie indicator of likely disorder, given retrospective studies showing that 90% of suicide attempters qualify for a DSM diagnosis, most frequently major depression (Mann et al., 2008). One might argue that such statistics ultimately beg the question of whether the DSM MDD conditions suffered by suicidal individuals are in fact disorders or normal distress. But wherever one falls on the disorder/nondisorder question, given that lives are potentially at stake, the suicide attempt issue carries an importance that to some extent transcends the disorder/nondisorder issue. We approached the suicide attempt question in this pragmatic spirit. Consequently, the discussion of the suicide attempt question proceeded without reference to the broader theoretical analysis of the disorder/normal sadness issue. However, in the end, our findings provide one more point of support for the viability of considering the uncomplicated/complicated distinction to reflect the normal/disordered distinction.
The results of this study demonstrate that, while no diagnostic screen is perfect, the diagnostic criteria for uncomplicated depression successfully screen out those who are likely to attempt suicide. They do this so successfully that, if one wants to avoid missing suicidal cases, one might as well equally worry about anyone who has been sad without meeting the MDD criteria. While clinical judgment is always essential when dealing with a depressed patient, any concern that excluding uncomplicated depression from MDD diagnosis would open the floodgates to missed cases of suicide attempt due to the known elevated rates of major depression can be set aside. The implications for the broader BE debate are clear: Fear of suicide attempt should not be a consideration in deciding whether uncomplicated cases should be excluded from MDD. The fact that proponents of BE elimination partly based their argument on the incendiary issue of suicide potential without any scientific basis for their claims makes one worry that all the striving for positioning within the DSM is pushing psychiatry toward being more like a pseudoscience than a serious scientific discipline.
The findings reported here regarding concurrent and predictive suicide attempt rates in uncomplicated versus complicated depression have direct implications for clinical practice with stressed individuals. In particular, unless there are specific indications otherwise, the clinician can be reassured that properly screened individuals with uncomplicated depression triggered by a stressor are unlikely to attempt suicide either during the diagnosed episode or subsequently. Since suicide threat is a major reason for referring patients for medication rather than psychotherapy, the knowledge that suicide is not a threat in a subset of MDD cases can allow the therapist to be more open to various alternative strategies—from lifestyle changes to psychotherapy to medication (Berk, Sarris, Coulson, & Jacka, 2013; Lampe, Coulston, & Berk, 2013; Malhi, Hitching, Berk, et al., 2013; Malhi, Hitching, Coulston, et al., 2013)—that are individually tailored to the patient in a stepped fashion (Malhi et al., 2009; Mcgorry et al., 2007).
The present findings, combined with recent findings that uncomplicated depression does not have elevated recurrence rates (Wakefield & Schmitz, 2013b, 2013d), should influence prognosis evaluation and thus informed consent when the clinician and patient review treatment options and evaluate their potential costs and benefits. Unipolar depression is predicted shortly to be the second leading cause of worldwide burden of disease (Mathers & Loncar, 2006), and distinguishing relatively benign subtypes could allow better and more cost-effective targeting of prevention and intervention efforts. It could allow less clinician focus in selected cases on such threats as suicide attempt and recurrence and more focus on issues of adaptation and resilience in the face of major stressors and changing environments. In addition, these findings suggest the fruitfulness of continued attempts to distinguish MDD subtypes that have different implications for clinical practice (Goldberg, 2011). Such distinctions may be crucial for fruitful treatment research leading to improvements in care (Østergaard, Jensen, & Bech, 2011; Wakefield, 2012).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.