
Abstract
Professional social workers and other mental health providers have for many years been involved in delivering treatment and support services focused on the needs of adults with severe mental illnesses living in the community. While some models have evolved largely through practice experience, others have developed through research paradigms in which program developers have attempted to systematically test their models by employing randomized trials and other rigorous approaches to assess impacts. Critical time intervention (CTI) is a time-limited care coordination model intended to prevent homelessness and other adverse outcomes among adults with severe mental illness during periods of transition. After briefly tracing its roots in assertive community treatment—a pioneering earlier model of community care—this article describes CTI, the evidence for its effectiveness, preliminary efforts toward its broad dissemination, and offers thoughts about its further development and potential for adaptation.
Keywords
Since the “deinstitutionalization era” dawned in the United States roughly 50 years ago, the need to provide effective community support and treatment for adults with severe mental illness has proved to be a vexing problem. Homelessness and social exclusion, frequent rehospitalization, and elevated risks of morbidity and mortality continue to define the lives of persons living with severe mental illness as they try to make a life for themselves in our communities. Furthermore, this sad state of affairs contributes to continued stigma toward persons with mental illness and exasperation on the part of many citizens who, confronted with the evidence before them, are tempted to conclude that a return to long-term institutional care is indicated.
Given the social work profession’s traditional biopsychosocial emphasis as well as its history of delivering services to disenfranchised members of the community, it is not surprising that professional social workers, alongside psychiatrists, psychologists, and other mental health providers, have for many years been involved with service delivery and development of interventions focused on the needs of adults with severe mental illnesses living in the community. While some program models have been based solely on fundamentals of practice wisdom, others have developed through research paradigms in which program developers have attempted to systematically test their models by employing randomized trials and other rigorous approaches to assess efficacy.
This article describes the background, testing, and dissemination of critical time intervention (CTI), an intervention designed to address the needs of one subgroup of persons with severe mental illness, those who have experienced recurrent homelessness. After briefly tracing its roots in an earlier pioneering model of community care for persons with severe mental illness (assertive community treatment [ACT]), we summarize the CTI model, the evidence for its effectiveness, preliminary efforts toward its broad dissemination, and thoughts about the model’s further development and potential for adaptation.
ACT
The ACT model (originally known as training in community living or TCL) emerged during the early 1970s at the Mendota Mental Health Institute in Madison, Wisconsin, as a strategy to reduce readmissions of patients with severe mental illness who were being discharged from inpatient care to community living as part of a new policy emphasizing care in the community rather than the hospital. In the community, it was hypothesized persons with illness could develop and practice independent living skills, have the opportunity to interact with healthy role models, and enjoy an improved quality of life. The model emphasized enhancing client self-determination, working with families and significant others as well as community agencies and other sources of support. There was minimal reliance on hospital care and, most importantly, an assertive orientation to follow up with clients to minimize dropout and loss to follow-up. A multidisciplinary team staffed similarly to the inpatient hospital ward provided services. Key figures Mary Ann Test (a research psychologist and faculty member at the University of Wisconsin’s School of Social Work), Deborah Allness (a hospital social worker), and psychiatrists Leonard Stein and Arnold Marx (Dixon, 2000; Freeman, 2001).
The model they pioneered, now known as ACT, has evolved into a widely studied approach that has been broadly applied in the United States and elsewhere. Its defining principles include the provision in the client’s home of comprehensive treatment services (including medication prescribing, administration, and monitoring) by a multidisciplinary team; services are available around the clock; an emphasis on assistance with daily living activities; a small staff to client ratio (approximately 1:10); and no fixed limit on the length of time that services are provided (Monroe-Devita, Teague, & Moser, 2011).
Critical to widespread impact of the model on the field was early research to test its efficacy. This included a National Institute of Mental Health (NIMH)-funded randomized controlled trial (RCT) that demonstrated superior outcomes over 12 months for the experimental group in the domains of rehospitalization, symptom reduction, employment, social relationships, and subjective life satisfaction (Stein & Test, 1980). Furthermore, the researchers also made an effort to assess cost-effectiveness, perhaps one of the first such efforts attempted in community mental health research (Weisbrod, Test, & Stein, 1980). A second phase of the study involved reducing program support and following subjects in the community for another 12 months. All improvements (other than employment) eroded. Significantly, this finding has contributed to an enduring belief among many subsequent implementers that the intervention would need to be delivered indefinitely in order to be effective. However, this appears to be a misinterpretation of the views of the model’s developers who were aware of the possibility that services might effectively be reduced in intensity over time (Stein, Barry, Dien, Hollingsworth, & Sweeny, 1999)
In the 20 years following the publication of Stein, Test, and colleagues’ original study (1980), the effectiveness of the ACT model has been supported by much subsequent research including numerous randomized trials of various replications and adaptations of the original model, most focusing on the provision of ACT to adults with severe mental disorders (schizophrenia spectrum, bipolar disorder, depression with psychosis), often with comorbid substance use problems as such problems have become increasingly common in this population. A Cochrane meta-analysis concluded that provision of ACT (compared with standard community care) was associated with: reduced hospitalization; more likely continued contact with treatment services; and better housing outcomes. Weaker effects were found on employment, client satisfaction, social functioning, and social integration (Marshall & Lockwood, 2000).
In the wake of widespread efforts to expand and improve community treatment of persons with severe mental illness, implementation of ACT has grown significantly. Though formal program fidelity standards have been systematically developed and promoted, significant program drift has occurred in some places; many programs that identify themselves as ACT do not appear to conform closely to the model used in original studies and replications or as described in fidelity standards endorsed by ACT researchers, trainers, and the national ACT Association (Mancini et al., 2009).
Despite strong promotion of the model by the National Alliance for the Mentally Ill, the U.S. Substance Abuse and Mental Health Services Administration, and other important groups, the ACT model has not been without its critics. Influenced in part by the mental health consumer movement, the field has recently begun to focus increasingly on “recovery” (including the importance of self-determination and social integration) as a key outcome for persons with severe mental illness. ACT has sometimes been cited by consumer advocates as inconsistent with this outcome in part because of its emphasis on adherence to psychiatric treatment and the growing use of ACT as a vehicle for delivering mandated outpatient treatment (itself a controversial policy) in some states (Gomory, 2001, 2002). Furthermore, it has become clear that even in public systems that have invested heavily in the development of this model (as in New York with over 75 teams and 5,000 persons served at any one time), cost and capacity limitations present significant problems. As a “time-unlimited” model, the typical length of stay in these services is often quite long and this has led to few openings and long waiting lists for entry. This in turn has stimulated efforts at the policy level to emphasize systematic efforts to assess readiness for discharge, and promote step-down to less intensive services (Donahue et al., 2012).
CTI
CTI is a model that draws on many of the same strategies pioneered by ACT (in vivo services, assertive outreach, and engagement to persons with severe psychiatric disabilities and social disadvantage) but with a significantly less intensive model and a more limited set of goals. CTI was originally developed in large municipal shelters for homeless men in New York city in the early 1990s at a time when that city, as well as other large urban areas in the United States were struggling under the weight of a newly emerging homelessness crisis (Valencia, Susser, & McQuiston, 1996). Causes of the explosion in urban homelessness of the time are debated; however, it is clear that significant reductions in the supply of both inpatient psychiatric hospital beds and inexpensive housing, growing income inequality plus a severe cocaine epidemic were strong contributors (Jencks, 1995; O’Flaherty, 1996).
These shelters housed up to 1,000 men, many with untreated mental illness and substance abuse and medical problems including HIV and TB infection. Over time, on-site mental health, medical, and social service teams were introduced and learned to effectively engage and stabilize shelter users with high levels of psychiatric and social need. As housing alternatives in the community slowly became available, these teams began to refer these men on to permanent housing, including single-room occupancy buildings, congregate housing, and supportive apartments. What the teams found, unfortunately, was that many became homeless again despite strong discharge plans and referrals to community services (Caton, Wyatt, & Felix, 1992).
Why didn’t their tenure in housing last? A variety of reasons were hypothesized. One is that transitions are especially challenging for mentally ill individuals, especially those who have a combination of risk factors for homelessness including poverty, low social support, substance use, and other health problems. Further compounding this was the loss of supportive relationships they had in the shelter and the neighborhood, a further set of losses for people who have typically experienced many throughout their lives. Furthermore, the community services that existed were often fragmented, poorly integrated, difficult to access, and not always welcoming of these individuals. Taken together, the discontinuity of care and support experienced during the transition period was especially challenging and, in our view, increased the likelihood of the occurrence of recurrent homelessness.
CTI was designed to augment the existing on-site program so that support and continuity of care would be enhanced during the critical time of transition from shelter to community housing by maintaining continuity of care while gradually passing primary responsibility to supports in the community. The rationale was that a time-limited intervention might have a durable impact if it could strengthen an ongoing network of community support. The intervention model was intended to be simple and adaptable so that it could potentially be applied in a variety of settings and “critical times” in which discontinuity of support was a key problem.
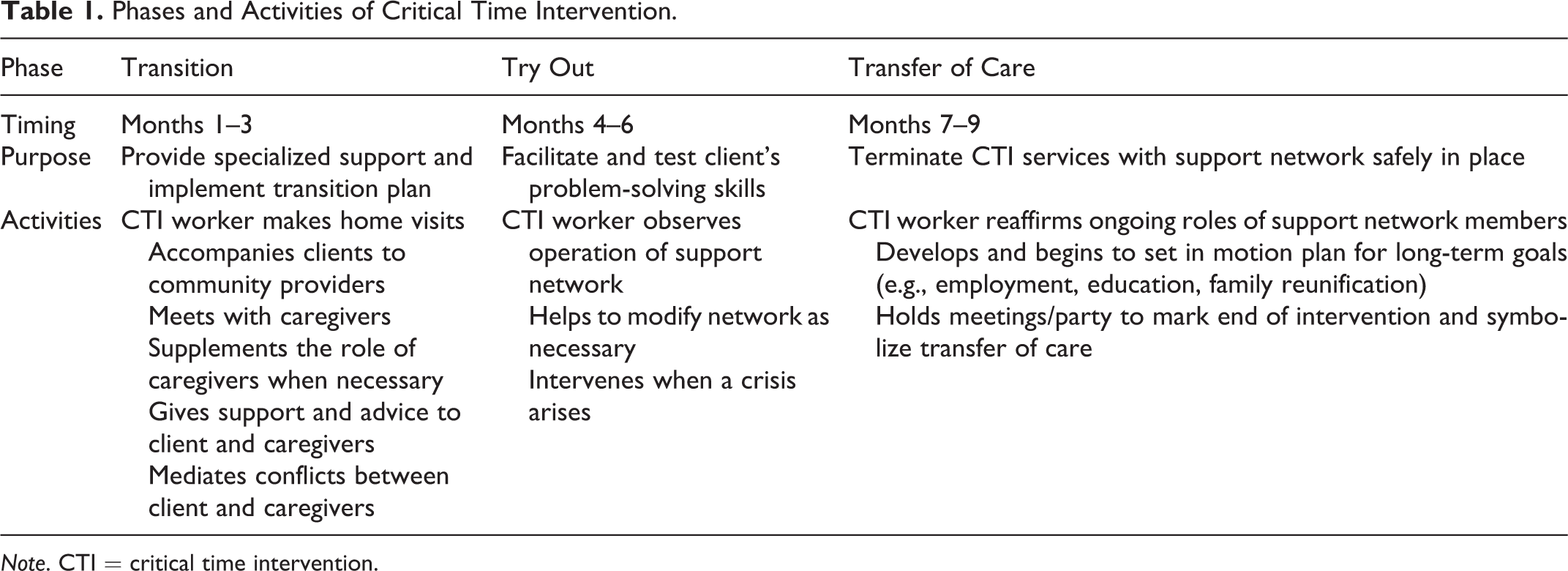
Briefly, CTI is generally delivered in three phases over 9 months, with each stage lasting approximately 3 months (see Table 1). The explicit aims are to provide direct emotional and practical assistance to the client and to strengthen his or her long-term ties with various formal and informal sources of support. During the first phase, a CTI worker (typically a bachelor’s or master’s level social worker) provides extensive support for clients, targeting areas critical for successful community transition. The CTI worker, ideally building on a relationship that has begun before the client’s discharge from the institution, aims to engage the client and identify, assess, and link him or her to both formal service providers (residential programs, mental health services) and informal networks of community support (family and friends). During the second phase, the CTI worker continues to provide direct assistance but encourages clients and their support networks to resolve issues on their own, providing backup support when necessary. In the final phase, the CTI worker transfers care and responsibilities to both the client and the formal and informal caregivers, aiming to reach consensus about a viable plan that will ensure ongoing support. Thus, responsibility for providing support is gradually transitioned away from the worker, in a planned way, to enduring supports within the community. Further detail on the model is available in previous publications (Herman, Conover, Felix, Nakagawa, & Mills, 2007; Herman & Mandiberg, 2010; Valencia et al., 1996)
Phases and Activities of Critical Time Intervention.
Note. CTI = critical time intervention.
Evidence for Efficacy
The impact of CTI in preventing recurrent homelessness was first tested in a randomized trial conducted at a large municipal shelter in New York city. Ninety-six homeless men with psychotic disorders were randomly assigned to receive usual discharge planning and follow-up services or usual services plus 9 months of CTI. All research participants were then followed for 18 months by trained interviewers blind to group assignment. In an intent-to-treat analysis, CTI was associated with a statistically significant threefold reduction in the risk of post discharge homelessness over the follow-up period (Susser et al., 1997). The observed effect persisted after the intervention ended, consistent with the notion that CTI successfully strengthened clients’ connection to ongoing community support. A subsequent economic analysis supported the cost-effectiveness of the intervention (Jones et al., 2003).
Following on these encouraging results, a second study was designed to test the model with a similar population of previously homeless adults with severe mental illness (SMI) following discharge from inpatient treatment in two state-operated psychiatric hospitals (Herman et al., 2011). In this study, 150 men and women diagnosed with schizophrenia spectrum disorders and having homelessness histories were randomly assigned to receive usual discharge planning and follow-up services or usual services plus 9 months of CTI. Like the earlier trial, assignment to treatment condition was independent of housing status at discharge. The intervention was delivered by state hospital bachelor’s level social workers operating under supervision by master’s level clinicians attached to the research team. Subjects in both groups were followed for 18 months by interviewers blind to treatment condition. An intent-to-treat analysis adjusting for potential confounders including prehospitalization homelessness found that the prevalence of homelessness among subjects assigned to the CTI condition at the study end point was approximately five times lower than among subjects assigned to the comparison condition. A subsequent analysis demonstrated that assignment to CTI was also associated with a significantly reduced risk of rehospitalization (Tomita & Herman, 2012). These results appeared to reconfirm a durable impact of the time-limited intervention when applied by trained workers in a typical practice setting.
Mechanisms of Effect: Cracking the Lid of the Black Box
Considerable recent conceptual and methodological work has focused on the many intricacies involved in studying complex health and social interventions such as ACT and CTI as well as the limitations inherent in the use of traditional randomized trials in these contexts. Typically described as interventions that have multiple interacting components, complex interventions also may have a high degree of flexibility permitted (or required) in their delivery (Craig et al., 2013). Some contend that in evaluating such interventions it is especially critical to explicate program theories and logic models that can clarify how interventions work (Bonell, Fletcher, Morton, Lorenc, & Moore, 2012; Hawe, Shiell, & Riley, 2004). They convincingly argue that current emphasis on “accrediting” program models as “evidence-based” or not based on the results of a small number of “black box” randomized trials is of limited utility because it typically fails to furnish policy makers and practitioners with sufficient information to make useful decisions about where, how, and when to implement the intervention and does not provide researchers and program developers with guidance about how the intervention might be enhanced or how other approaches might apply its active ingredients. Studies that aim to systematically explore mechanisms of action in social work interventions including psychosocial interventions for persons with severe mental illness are rare.
Although at a preliminary stage, several secondary analyses using data from our two completed trials have begun to illuminate possible mechanisms of effect of CTI. As noted above, we have hypothesized that a key element in the model is the establishment of an effective relationship between worker and client before he or she is discharged from the institution. In order to examine this notion in our second trial, we compared the outcomes of participants assigned to CTI who received three or more predischarge contacts by the worker with experimental participants who received fewer than three such contacts. We employed an instrumental variables approach (Greenland, 2000) to obtain an unbiased estimate of the impact of receiving this version of the intervention while controlling for the impact of all possible confounders. In this analysis, we found that the impact on the risk of homelessness of receipt of CTI with three or more predischarge contacts was roughly twice as great as the overall impact we observed (Herman et al., 2011). In addition, we observed for those persons who received three or more predischarge contacts the impact of the intervention was evident sooner during the course of follow-up than it was among persons who were provided CTI but who received fewer than three such contacts. While far from conclusive, these findings are consistent with the idea that the impact of CTI may be maximized via the maintenance of a continuous relationship between worker and client that spans the period of transition from institution to community.
Further exploratory analyses have begun to examine another of CTI’s potential mechanisms—its effort to mobilize ongoing support from clients’ social networks including family members. Previous research has suggested that many persons with severe mental illness, including those who have been chronically homeless continue to have connections with family members (Dixon, 1999). However, such relationships are often strained by the emotional and financial pressures associated with the mental illness of a family member, simple lack of information or understanding regarding the most effective ways to support the person in managing the illness, and limited access to formal resources that might serve to support the individual and the family (Lucksted, McFarlane, Downing, & Dixon, 2012). In a secondary analysis of data from our most recent trial, we found that participants assigned to the CTI condition reported greater frequency of family contact and greater improvement in satisfaction with family relationships than did those assigned to the usual services group over the 18-month follow-up period. A mediation analysis employing mixed-effects regression models showed that greater improvement in satisfaction with family relations mediated the impact of CTI on the risk of psychiatric rehospitalization but only at a modest level (Tomita, Lukens, & Herman, 2014). This provides some support for the hypothesis that CTI’s effect may indeed partially operate by strengthening clients’ support networks, including support provided by family members.
A further analysis of data from this trial examined the impact of CTI on selected indicators of community integration. Community integration has been defined as having three components: physical integration (extent to which an individual participates in activities and uses community goods and services), social integration (extent to which an individual engages in social interactions with community members), and psychological integration (extent to which an individual feels a part of the community) Wong & Solomon, 2002. Although improving community integration itself was not a primary goal of the intervention, we hypothesized that CTI might have an impact on this outcome since, as noted above, the intervention aims to strengthen ties to formal and informal supports in the community. Our findings did not demonstrate a significant association between assignment to the CTI condition and either of the domains of social integration we measured. Interestingly, there was also no association between social integration and housing stability during the follow-up period (Baumgartner & Herman, 2012). A limitation of this study is that the measures of integration we employed were rather limited and omitted potentially important areas (such as psychological integration and interactions with persons who the study respondents did not know), so it is possible that our findings may have underestimated the impact of CTI on integration. Nonetheless, we found no evidence that CTI’s positive impact on residential or rehospitalization outcomes is explained by an improvement in community integration.
The need for data that can inform efficient targeting of complex interventions has been noted in many domains, and the area of homelessness prevention is no exception (Culhane, Metraux, & Byrne, 2011). To identify the target group for CTI, we relied primarily on epidemiologic studies and clinician reports to identify groups who appear to be at especially high risk of recurrent homelessness and other adverse outcomes following institutional discharge. Another important question is whether there are particular individual-level characteristics that can predict who will be more or less likely to benefit from the intervention. We so far have little solid information to go on. However, an unusual reanalysis of outcome data from the first trial confirms the need to explore this issue more fully (Lennon, McAllister, Kuang, & Herman, 2005). This study applied latent class growth analysis to identify latent classes of homelessness outcome trajectories among the 96 men in the study (half of whom received CTI and half of whom received usual services only). Four latent classes were found in the usual services group, but just three classes in the CTI group; the usual services group (but not the CTI group) had a small group of continuously homeless men. In addition, the size of the “never-homeless” class was approximately 20% greater in the CTI group. The timing of patterns of outcomes in other classes also differed by experimental group. While the small sample size precluded a systematic analysis of individual characteristics associated with these classes, this exploratory work suggests how future research might employ similar methods to identify subgroups that would potentially be more or less likely to benefit from the intervention.
By focusing on the experience of social workers and other mental health providers who have direct experience delivering CTI, several recent publications by practice researcher Fang-Pei Chen have begun to shed further light on how the intervention operates as well as identifying key issues for further research. Her methodology involved applying a grounded theory approach in a series of intensive semi-structured one-to-one interviews with staff who were applying the CTI model with homeless and formerly homeless persons with severe mental illness during their transition from homelessness to housing. Her results demonstrate the significant degree to which structural factors of the host organization as well as dominant agency values and philosophy influenced the ways in which workers operationalized key components and strategies of the CTI model. For instance, the CTI model encourages a harm reduction approach to client substance use, teaching workers that, rather than promoting “abstinence only,” among clients who use drugs or alcohol, the worker should aim to help the client and relevant caregivers minimize the risk of allowing substance use to lead to loss of housing. This proved to be problematic in contexts in which one or more of the organizations in which the work is occurring does not endorse this treatment philosophy.
She also provides examples of how practitioners adapt and add to the model in ways that may or may not be consistent with the designers’ intent. For instance, she discovered that workers in one agency had instituted a “graduates group” for clients who had completed the intervention through which they offered ongoing contact with staff and other clients. While a literal reading of the CTI model (i.e., strict time limit on services after which responsibility for supports is passed to others) might suggest that this adaptation is inconsistent with the model, a more nuanced interpretation might view the graduates group as a creative and effective example of mobilizing ongoing natural supports that persist following the end of the formal intervention period.
This work supports the importance of CTI workers establishing a close working relationship with clients as a necessary condition for the effective delivery of the model and explored in some detail how workers go about building and maintaining such relationships, emphasizing the use of informal, “friendship-like” interactions in contributing to the development of trust on the part of service recipients. This trust appeared to contribute to enhanced client–worker communication that, in turn, faciliated identification of and amelioration of important potential barriers to housing stability (Chen & Ogden, 2012). Chen’s work is also instructive on the subject of how CTI workers go about developing effective ongoing supports for service recipients by interacting with other supporters and caregivers in the community, emphasizing the specific collaborative techniques involved as well as tensions that sometimes arise between CTI workers and collaborators when boundary or turf issues emerge. (Chen, 2013). Finally, this research provides insights into significant issues relevant to the all-important area of implementation of CTI and other empirically supported social work interventions by examining how closely workers follow the ideal model and identifying how key model elements are adapted in response to constraints and needs of the service delivery settings in which they operate (Chen, 2012).
Effectiveness Research
The findings described above were all derived from tightly controlled randomized trials (albeit carried out in typical service delivery settings). Effectiveness trials attempt to evaluate the impact of intervention models as they are applied under “real-world” service delivery conditions, often with larger samples than are available in typical efficacy studies. One such CTI study has been implemented at eight Department of Veterans’ Affairs medical centers scattered throughout the United States. In a quasi-experimental study, 278 homeless men and women with SMI were recruited and followed for 1 year after discharge from inpatient psychiatric treatment, receiving standard case management services in the community. Following this, case managers were trained in the CTI model via face-to-face trainers who had received instruction in CTI from the model developers and a second group of 206 subjects were recruited and offered CTI after discharge. Controlling for baseline differences between cohorts, investigators found that the CTI cohort had on average 19% more days housed than did the first cohort over the 1-year follow-up period (p < .002) as well as significantly fewer days in institutional settings and lower alcohol, drug, and overall psychiatric symptom scores (Kasprow & Rosenheck, 2007). While these encouraging results suggest that the model can in fact be effectively delivered in standard treatment systems, clearly more empirical work of this kind is needed.
Dissemination and Implementation Research
As has been extensively documented (and lamented), the gap between development and testing of empirically supported interventions in social work and allied fields and their broad implementation in typical service delivery settings is great. This behooves intervention developers and researchers, if they are committed to maximizing the impact of their work, to directly engage in research and other activities directly related to the broad dissemination and implementation processes that drive uptake of empirically supported models of care (Proctor & Rosen, 2008). Our small development team, recognizing that we lack the requisite resources and experience to carry out this work on our own, has adopted a collaborative approach to this critically important undertaking. Working with trainers, implementation specialists, and other researchers, we have launched a series of activities intended to develop and test the tools and mechanisms needed to support broader implementation of CTI.
We have partnered with two large training organizations (the Center for Social Innovation, Inc. and the Center for Urban Community Services) that train and consult with mental health and homeless service providers throughout the United States. The collaborative has designed and tested a training curriculum for CTI that has been delivered both through traditional face-to-face methods and via an instructor-led online course that includes multimedia self-paced elements. With the support of the NIMH, the group recently completed a randomized trial comparing the impact of these two training modalities on trainee satisfaction, knowledge gains, and knowledge retention. In the next phase of the study, researchers assessed the CTI implementation process, including an assessment of fidelity to the model over time. An effort was also made to compare the cost of training between conditions.
Nineteen agencies (including 179 individual workers) serving homeless persons from across the United States were randomly assigned to either the face-to-face or the online training condition. The face-to-face condition included a limited number of follow-up telephone coaching contacts by implementation consultants, while the implementation support provided in the online condition was limited to a web-based “community of practice” model (Wenger, McDermott, & Snyder, 2002). Assessments were carried out before training and 6 months after its completion. Among the key findings were that although training satisfaction was significantly higher in the face-to-face group, knowledge gains and retention were strong and did not differ significantly between conditions. Implementation rates were high in both groups, with a modest advantage to the face-to-face training condition. Fidelity ratings were comparable across conditions with providers in the face-to-face condition demonstrating slightly higher scores. The team concluded that while both modes of training were effective in transferring needed technical information to workers about the model, the enhanced implementation support provided in the face-to-face condition contributed to higher rates of program uptake. Costs associated with delivering face-to-face training were significantly higher (US$2,700 per agency for the online training compared to US$8,116 per agency for the on-site training and consultation). Based on these findings, we believe that a hybrid form of training that combines web-based content delivery and customized in vivo implementation support may be ideal from a cost-effectiveness perspective (Olivet, 2013).
Model Adaptations
Although CTI was originally developed and tested with persons with severe mental illness who were chronically homeless, we have argued elsewhere that the model has the potential to be effectively adapted for use in different settings and with other populations when relevant “critical times” can be identified (Herman & Mandiberg, 2010). Other investigators have recently begun to such adaptations including work with persons being released from correctional institutions (Draine & Herman, 2007; Jarrett et al., 2012), homeless families and children (Samuels et al., 2006), persons using domestic violence shelters (Lako et al., 2013), young adults aging out of residential treatment centers, and other vulnerable groups during periods of transition. CTI has also recently been adapted for use in Latin America to improve social integration and quality of life among individuals with psychoses and to reduce unmet needs from the perspective of the service users over the long term (Baumgartner, da Silva, Valencia, & Susser, 2012). Known as CTI-TS (for “task shifting”), it is targeted to the period of transition when users first connect (or reconnect) to mental health services. It is currently being tested in Rio de Janeiro, Santiago, and Buenos Aires in an NIMH-funded pilot RCT led by investigators at Columbia University and at the University of Chile in Santiago.
Future Directions
Although considerable progress has been made over the almost 20 years of work on CTI, much remains to be done. From a research perspective, important unanswered questions remain about the model’s mechanisms of effect, subgroup impacts, active ingredients, and cost-effectiveness. Furthermore, with the exception of a single quasi-experimental study in the Veterans Affairs system, there has yet to be a carefully evaluated large-scale effectiveness study in a major service delivery system. Such a project would, in turn, permit a systematic assessment of a model for measuring CTI fidelity that could ideally be used to promote ongoing quality improvement. Finally, as noted above, rigorous efficacy studies of further adaptations of CTI with different target populations are clearly warranted and some are currently underway.
To promote this research and to support further dissemination and implementation of the model, several training and research groups have recently joined together to launch the CTI Global Network. The broad goal of the network, based at the Silberman School of Social Work at Hunter College, is to coordinate and mobilize the efforts of providers, trainers, researchers, and funders to support the further growth and development of CTI through ongoing collaboration, information sharing, advocacy, and research. Its specific aims are to promote interest in and uptake of CTI among service providers, policy makers, and funders in the United States and internationally; to build capacity among service providers to effectively adapt and implement CTI with various high-risk populations; to develop and disseminate tools and information needed for effective implementation of CTI, including manuals, case studies, funding models, and fidelity measures; and to enhance communication and information exchange between providers, trainers, and researchers in order to improve service quality and to identify promising adaptations and enhancements to CTI.
Footnotes
Author’s Note
This article was presented at the Islandwood Roundtable on Science in Social Work, July 17–18, 2013, Bainbridge Island, WA. It was invited and accepted by the editor. The author gratefully acknowledges his colleagues Ezra Susser, Elie Valencia and Sarah Conover whose original development of the CTI model provides the foundation on which this work stands.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research described was supported in part by a research grant from the National Institute of Mental Health (R01MH59716, Daniel Herman, Principal Investigator).