
Abstract
The term intimate partner violence (IPV) describes actual or threatened physical, sexual, or psychological violence that occurs within a relationship or is perpetrated by a current or former partner or spouse (Saltzman, Fanslow, McMahon, & Shelley, 2002). IPV can include a number of components, including physical violence, sexual violence, and psychological or emotional violence (Saltzman et al., 2002). These forms of violence can be common responses to conflict within relationships and can have significant effects upon the mental, physical, and social well-being of those involved. Although IPV is often unreported, prevalence within the adult population is estimated to be high, with rates varying between countries (World Health Organization [WHO], 2005). For example, one multi-country study conducted by WHO found that between 3% and 54% of women report having experienced physical or sexual violence by an intimate partner in the previous year (WHO, 2005). Additionally, between 10% and 50% of women report having experienced violence from partners or ex-partners at some point in their lives (Watts & Zimmerman, 2002).
Rates of relationship abuse vary according to age, sex, and previous experience of violence (Archer, 2000; Foshee et al., 1996, 1998). The prevalence of relationship violence is higher in adolescents than in adults, with females aged 12 to 18 years having the highest victimization rate (Home Office, 1999; Wolfe et al., 2003). This form of violence is called dating violence and perpetrators are most likely to be peers (Schewe & O’Donohue, 2006). Approximately, 20% of young women have experienced violence from a dating partner (Bergman, 1992; O'Keeffe, Brockopp, & Chew, 1986). First episodes of violence frequently occur in adolescence (Henton, Cate, Koyal, Lloyd, & Christopher, 1983). In younger dating samples, relatively higher proportions of aggression by women against men have been described, although results vary according to the measurement methods used and must be interpreted with caution (Archer, 2000).
Early experiences of dating violence are linked to poor health outcomes such as sexually transmitted infections (Campbell, 2002; Exner-Cortens, Eckenrode, & Rothman, 2013; WHO, 2005), teenage pregnancy (Campbell, 2002), substance misuse (Roberts & Klein, 2003; Tyler & Melander, 2012), cancer, coronary heart disease, attempted suicide (Exner-Cortens et al., 2013; WHO, 2005), depression (Campbell, 2002; Roberts & Klein, 2003; Wolitzky-Taylor et al., 2008), and symptoms of post-traumatic stress disorder (Campbell, 2002; Wolitzky-Taylor et al., 2008). Relationship violence during pregnancy is also associated with adverse maternal and neonatal health outcomes including preterm delivery (Campbell, 2002), low birth weight (Campbell, 2002; Murphy, Schei, Myhr, & DuMont, 2001), and foetal death (Campbell, 2002). Moreover, adolescents who have experienced dating violence in the past are more likely to be perpetrators or victims of IPV as adults (Chiodo et al., 2012; Krug, Dahlberg, Mercy, Zwi, & Lozano, 2002; Loh & Gidycz, 2006).
Educational and skills-based interventions can be delivered in a number of environments including the community, schools, and higher education establishments (Wolfe & Jaffe, 1999). Schools play an important role in the development of social behavior and provide an appropriate environment to target children and adolescents in the prevention of dating violence and other forms of relationship violence (Adi, McMillan, Kiloran, & Stewart-Brown, 2007; Mytton, Di Giuseppi, Gough, Taylor, & Logan, 2006; Park-Higgerson, Perumean-Chaney, Bartolucci, Grimley, & Singh, 2008). College-based interventions can reduce incidences of sexual assault and possibly IPV among participants (Luthra & Gidycz, 2006). Programs delivered within home (Foshee et al., 2012) and community (Salazar & Cook, 2006; Wolfe et al., 2003) settings can raise awareness about abuse, promote positive relationships, enable help seeking and peer support, challenge discriminative viewpoints and encourage the development of protective skills (Wolfe & Jaffe, 1999). These interventions work by providing participants with the skills to communicate effectively; deal constructively with stress, disappointment, and rejection; resolve conflicts and promote healthier relationships (Wolfe & Jaffe, 1999). They may also provide young people with skills to protect themselves from the risk of relationship violence and to improve low self-esteem, which is linked to the likelihood of being a victim of relationship violence (Gidycz, Rich, Orchowski, King, & Miller, 2006).
The high prevalence of relationship violence and the severity and duration of its health consequences render this area an important public health issue. To date, many review studies have focused either on IPV or domestic violence in adult populations (Ramsay et al., 2009; Wood, Bellis, & Watts, 2010) or on the prevention of sexual abuse (Zwi et al., 2009) or general violence (Mytton et al., 2006) in children. We have found only one systematic review of interventions to prevent dating and relationship violence in young people (Whitaker et al., 2006), which reviewed only primary prevention programs, included nonrandomized (e.g., pre- and post-interventions) as well as randomized studies, and summarized results narratively. Our review builds upon these findings by limiting included studies to randomized controlled trials (RCTs) and quasi-RCTs, including primary and secondary prevention programs, and summarizing results in a meta-analysis. Given that interventions to prevent relationship violence based in schools and universities are becoming increasingly widespread, this review is important for strengthening the evidence base, providing a clearer idea of what works, and helping to inform future policy, practice, and research in this area.
Method
We searched the Cochrane Central Register of Controlled Trials (CENTRAL), Ovid MEDLINE, EMBASE, CINAHL, PsycINFO, Sociological Abstracts, Social Sciences Citation Index, Education Resource Information Center [ERIC], National Criminal Justice Reference Service Abstracts, metaRegister of Controlled Trials (mRCT), ZETOC, and WorldCat. There were no restrictions on language or date of publication. The search was carried out on May 7, 2012. Details of the search strategy are available from the original research article from the Cochrane Collaboration. We also hand searched reference lists of key articles included in the review and issues of the Journal of Interpersonal Violence and Child Abuse and Neglect published between 2005 and 2012. Finally, we contacted authors of key studies and asked them to share any published, unpublished, and ongoing work relevant to the review.
We included studies if they were RCTs, cluster-RCTs or quasi-RCTs; included participants aged 12–25 years; and were conducted in any setting. Studies with a wider age range of participants were included if we could extract or obtain data for those aged 12–25 years or if more than 80% of participants were aged 12–25 years. Programs could be applied universally or to specifically targeted high-risk groups. We compared all interventions with a control intervention including no intervention, placebo intervention (e.g., provision of first aid classes), or standard care. Studies had to provide a full description of the measurement scale used. Interventions that only screened for the occurrence of dating or relationship violence and then referred to a support agency were also excluded.
Primary outcome measures were episodes of relationship and dating violence experienced; injuries resulting from relationship and dating violence; self-reported subjective improvement in mental well-being; and adverse events (e.g., an increase in the number of episodes of relationship or dating violence reported). Secondary outcome measures were improvements in behavior or knowledge about relationship and dating violence; improvements in access to (or knowledge of) help or support services; and attainment of protective skills. We divided all outcomes into short-term (assessed between 0–6 months following the intervention) medium-term (assessed 6–12 months following the intervention) and long-term (assessed >12 months following the intervention) outcomes.
Two review authors (G.F. and C.H.) independently screened the titles and abstracts of articles against inclusion criteria. If there was insufficient information in the title and abstract to make such decisions, we retrieved the full text. Two authors (G.F. and C.H., S.H., J.N., or D.S.) independently extracted data from all included studies and entered results into Review Manager 5 (Review Manager [RevMan], 2011). We assessed the risk of bias in each study for each of the following domains: sequence generation; allocation concealment; blinding; incomplete outcome data; and selective outcome reporting.
We used risk ratios (RRs) to summarize dichotomous data. We reported continuous data as mean differences (MDs) where the same scale was used for measurement and standardized mean differences (SMDs) where different scales were used to measure the same outcome. For cluster-RCTs we followed the guidance outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins & Green, 2011). We used an intraclass correlation coefficient (ICC) to describe the relative variability in outcomes within and between clusters. Among our included cluster-RCTs, only Wolfe et al. (2009) used an ICC. For our analyses, we adopted a higher ICC of 0.15, based on two similar reviews: first, a review of school-based programs to prevent violence that used ICC values of 0.1 and 0.2 (Mytton et al., 2006) and second, a meta-analysis of multicomponent preventive interventions for children at risk of antisocial behavior (Conduct Problems Prevention Research Group [CPPRG], 1999), which used an ICC value of 0.15. We used the ICC to calculate a design effect for each cluster-RCT. In the meta-analyses, we calculated SMD effect sizes. These were weighted using the generic inverse variance function, and we used random-effects assumptions. Several studies identified for inclusion in the review had multiple intervention groups. In these cases, to avoid double counting and creating unit-of-analysis errors, we made single pair-wise comparisons, that is, we made comparisons between the combined intervention group and the combined control group. For dichotomous outcomes, we summed the sample sizes and number of outcomes across groups. For continuous outcomes, we combined means and standard deviations (SDs; Higgins & Green, 2011).
We assessed statistical heterogeneity using the I 2 statistic, using a cutoff of 50% to represent substantial heterogeneity (Higgins & Green, 2011). We also used the χ 2 test of homogeneity to determine the strength of evidence for genuine heterogeneity. We combined studies in meta-analysis across all settings and irrespective of duration or intensity. These aspects were explored in subgroup analysis and no differential effect was found. Where there was substantial heterogeneity, we computed pooled estimates only for those trials that could be analyzed together and for which the necessary statistical data were available. In our protocol, we agreed that if substantial heterogeneity was indicated we would exclude studies from meta-analysis and report results narratively. However, for two of our outcomes we nevertheless went ahead with meta-analysis despite high heterogeneity. Firstly, a pooled result was still deemed to be useful despite high heterogeneity, particularly for the main outcome of episodes of relationship and dating violence. Secondly, much of the heterogeneity was due to one or two small, outlying studies; and thirdly, heterogeneity was only marginally above our threshold (57% for episodes of relationship and dating violence and 52% for knowledge of relationship and dating violence). We discuss the implications of conducting meta-analyses on studies with a high degree of heterogeneity in our discussion.
We carried out data synthesis using Review Manager 5 (RevMan, 2011). We used a random-effects model where there was no severe funnel plot asymmetry unless studies had similar interventions measuring the same outcomes, when we used a fixed-effect analysis. Where there was significant funnel plot asymmetry, we used both fixed-effect and random-effects models and reported the degree of agreement between the results of the two models. We calculated overall effects using the inverse variance method (Higgins & Green, 2011).
We carried out subgroup analyses for intervention setting (i.e., school, university, or community settings), the target audience (i.e., general population or high-risk population), the timing of outcome assessment, and the duration of the intervention. We ran sensitivity analyses restricting analyses to the following: studies with a low risk of selection bias (as determined by the quality of the random sequence generation); studies with a low risk of assessment bias (as determined by the quality of blinding of assessors); and studies with a low risk of attrition bias (as determined by the completeness of the data).
Results
Results of the Search
Our search identified 22,184 articles of which 95 appeared to meet our inclusion criteria based on titles and abstracts. Correspondence with authors yielded an additional three eligible studies that had not been identified by our search strategy. Of the 98 articles identified, full texts were unavailable for 17 articles. A more detailed evaluation of the full text of the remaining 81 articles revealed 41 articles (representing 38 studies) that were eligible for inclusion in our review and 40 that were excluded. Of the 38 studies included in our review, 33 were included in the meta-analysis. Figure 1 shows a study flow diagram.
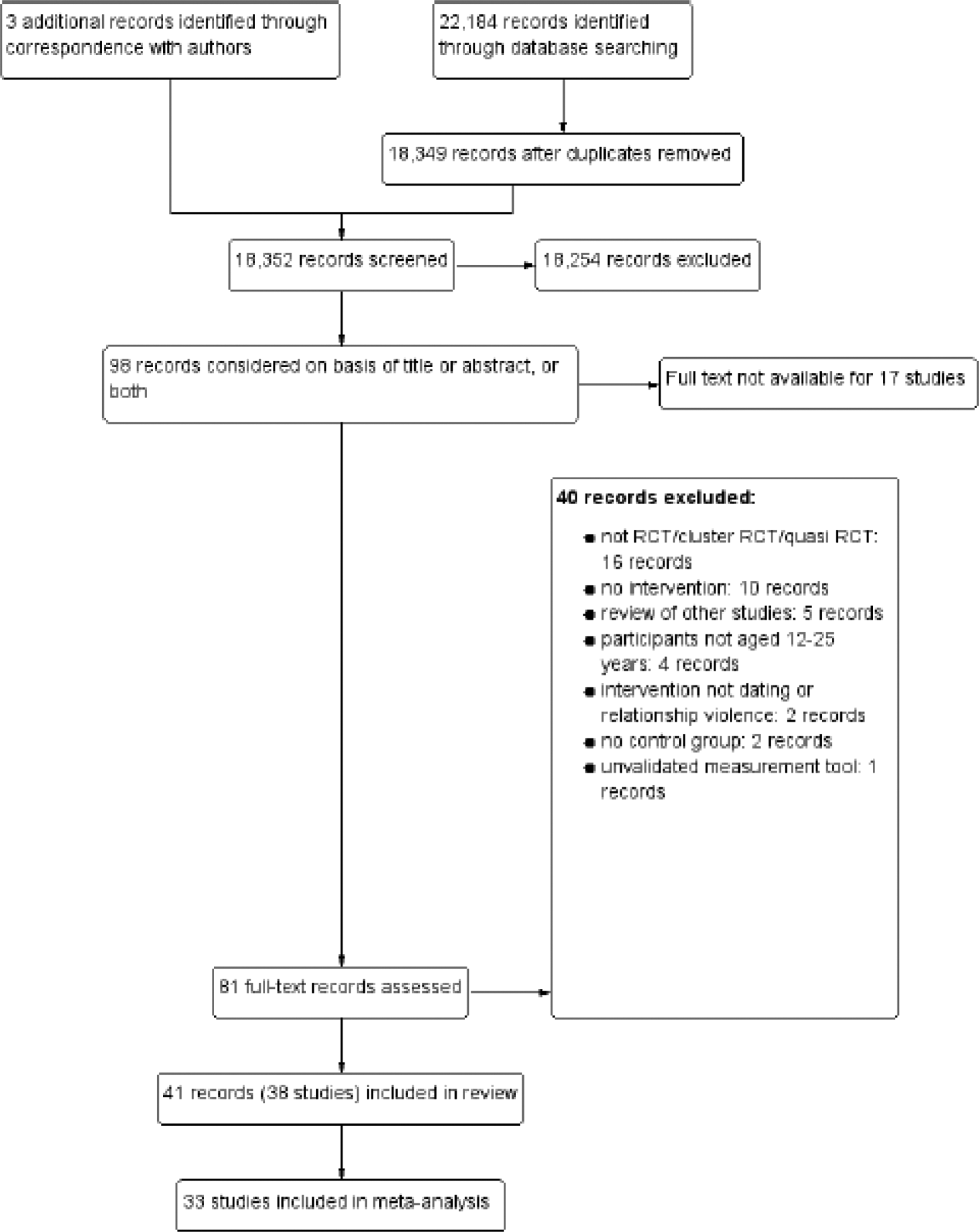
Study flow diagram.
Of the 38 studies included, 18 were RCTs, 18 were cluster-RCTs and two were quasi-RCTs. With the exception of one study conducted in the Republic of Korea (Yom & Eun, 2005), all included studies were carried out in the United States. The majority of studies were conducted in educational settings (25 in universities and 10 in high schools). Three studies were conducted in community settings including health clinics (Florsheim, McArthur, Hudak, Heavin, & Burrow-Sanchez, 2011), prisons (Salazar & Cook, 2006), and community centers (Wolfe et al., 2003). Five studies targeted high-risk individuals such as adjudicated adolescent males (Salazar & Cook, 2006), individuals or couples known to be at high risk of dating aggression (Schewe & O’Donohue, 1996; Stephens & George, 2009; Woodin & O’Leary, 2010), and individuals with a history of maltreatment (Wolfe et al., 2003). Interventions were predominantly educational, although five provided an additional component on self defense (Florsheim et al., 2011; Gidycz et al., 2006; Orchowski, Gidycz, & Raffle, 2008; Wolfe et al., 2003; Wolfe et al., 2009) and one provided a component on communication skills (MacGowan, 1997). The duration of interventions ranged from a single, 50-min session to 18 sessions delivered over 4 months (Wolfe et al., 2003). In the majority of studies, the control group received no intervention or standard care, or were “wait list controls” (i.e., receiving the intervention after completion of data collection). A number of studies provided the control groups with placebo interventions such as presentations, videos or plays on career development, multicultural issues (Lanier, Elliott, Martin, & Kapadia, 1998), sexually transmitted infections (Pinzone, 1998), stress management (Saberi, 1999), and other similar issues (Yom & Eun, 2005). One study showed the control group an episode of a situation comedy television program (Kuffel & Katz, 2002).
Of the outcomes we were interested in, 17 studies reported episodes of relationship or dating violence. Of these, eight used the Sexual Experiences Survey (SES), five used the Revised Conflict Tactics Scale (CTS), and the remaining four used other scales. Eight studies had sufficient data to be included in the meta-analysis. Several studies included measures of changes in attitudes, and we included this outcome in our results even though we did not state it separately in our predefined outcomes because we had assumed this to be a subcomponent of behavior and knowledge. Sixteen studies assessed attitude changes, 6 assessed behavior change, 12 assessed change in knowledge, and 7 assessed skills to prevent relationship and dating violence. Thirty studies assessed short-term outcomes (0–6 months following intervention); 4 studies assessed medium-term outcomes (6–12 months following intervention); and 4 studies assessed long-term outcomes (more than 12 months following intervention). Because such a significant majority of studies assessed short-term outcomes, we analyzed all studies together and conducted subgroup analyses to assess whether effects differed when mediumterm, longterm, or both, were excluded from the analyses. If a study had multiple follow-up points, we chose the longest duration of follow-up. For the majority of studies, the risk of selection bias (due to inadequate random sequence generation or allocation concealment) was unclear, the risk of attrition and reporting bias was low, and the risk of performance bias (due to inadequate blinding of participants and personnel) was high (Figure 2).

Summary of risk of bias.
Effects of Interventions
We included 38 studies in the review, of which we included 33 in the meta-analyses. The following five studies were excluded: Andersen (1992) used nonparametric (Mann–Whitney U) analyses; Foshee et al. (1998) did not report the number of participants in each arm or any tests of significance; Shultz, Scherman, and Marshall (2000) did not report the number of participants in each group; and Holcomb, Savage, Seehafer, and Waalkes (2002) and Woodin and O’Leary (2010) reported F-statistics, which could not be used to extract evidence of effect as the statistic was not associated with a direct comparison of the intervention under study (and therefore not equivalent to a t-test).
Episodes of relationship and dating violence
Seventeen studies measured episodes of relationship and dating violence. We conducted one meta-analysis of categorical data and one of continuous data. The analysis of categorical data included eight studies (3,405 participants) and showed substantial heterogeneity (I 2 = 57%; χ 2 16.35; degrees of freedom = 7; p value .02). Despite this, we felt it important to conduct a meta-analysis because episodes of relationship and dating violence was our most important outcome and because the I 2 value of 57% was only marginally above our originally defined threshold of 50%. It is likely that much of the heterogeneity is attributable to two outlying studies (Stephens & George, 2009; Gidycz, Orchowski & Berkowitz, 2011). Using a random-effects model, the RR was 0.77 (95% CI: [0.53, 1.13]; Figure 3). The analysis of continuous data included five studies (3,171 participants) and showed no heterogeneity (I 2 = 0%). Using a fixed-effect model, the SMD was −0.05 (95% CI: [−0.19, 0.09]; Figure 4).
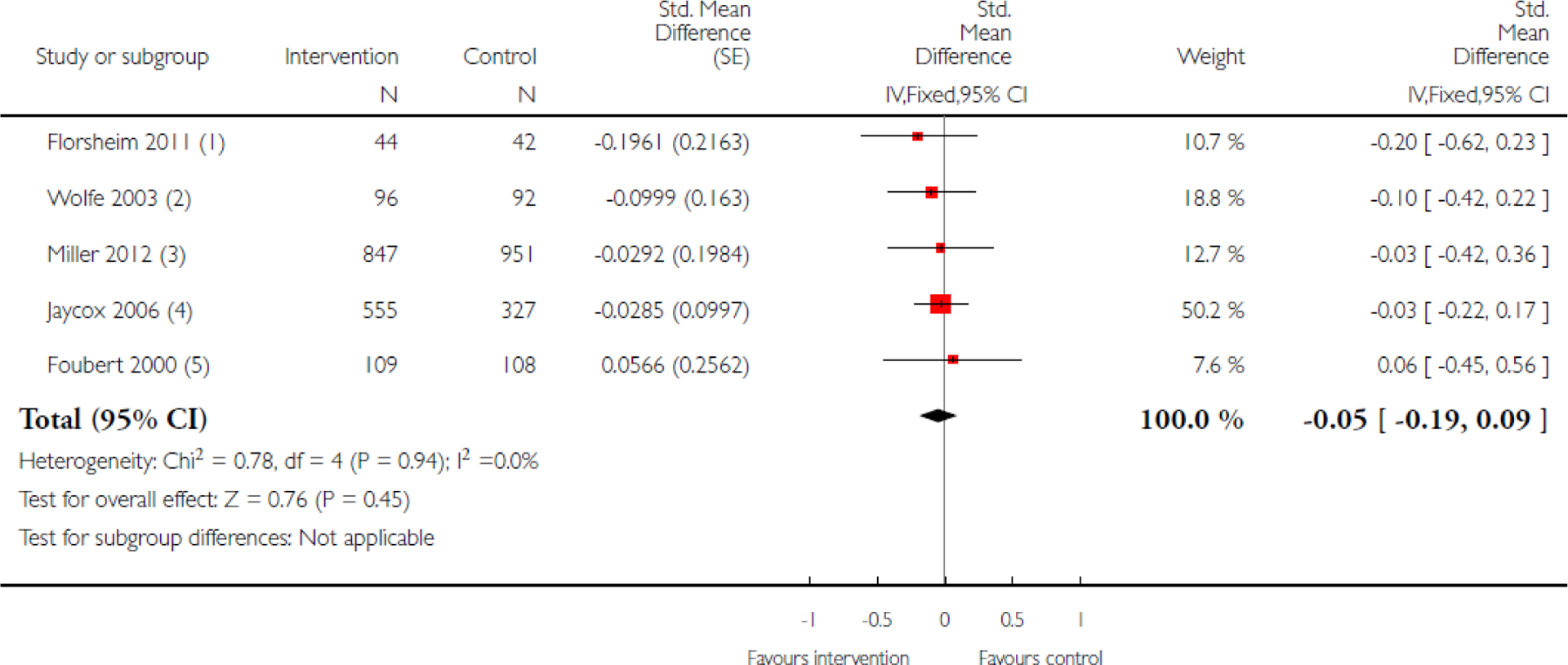
Episodes of relationship violence (scores). Notes: Higher scores indicate a greater frequency of violence. (1) Interpersonal violence scale. (2) Conflict in adolescent dating relationships inventory. (3) Revised conflict tactics scale. (4) Revised conflict tactics scale. (5) Sexual experiences survey.

Episodes of relationship violence (events). (1) High-risk and low-risk men combined. (2) Number of students experiencing physical dating violence.
Attitudes toward relationship and dating violence
The meta-analysis for attitudes toward relationship and dating violence included 22 studies (5,256 participants) with evidence of moderate heterogeneity (I 2 = 48%). Using a fixed-effect model, the SMD was 0.06 (95% CI: [−0.03, 0.15]). Because of the moderate level of heterogeneity, a random-effects model was also conducted, which produced an SMD of 0.08 (95% CI: [−0.06, 0.22]; Figure 5).

Attitudes toward relationship violence. Notes: Higher scores indicate less accepting attitude. (1) Gender-equitable norm scale. (2) General attitudes toward rape scale. (3) Justification of interpersonal violence. (4) Rape empathy scale. (5) Illinois rape myth acceptance scale (RMAS). (6) Attitudes toward relationships. (7) Knowledge and attitude of sexual violence questionnaire.
Behavior in relationship and dating violence
We included four studies (887 participants) in the meta-analysis for behavior in relationships and dating violence. There was no heterogeneity (I 2 = 0%). Using a fixed-effect model the SMD was −0.07 (95% CI: [−0.31, 0.16]; Figure 6).

Behavior toward relationship violence. Notes: Higher scores indicate more positive behavior. (1) Dating behavior survey. (2) Dating behavior survey. (3) Dating behavior survey. (4) Behavioral intent to rape survey.
Knowledge of relationship and dating violence
We included 10 studies (6,206 participants) in the meta-analysis for knowledge of relationship and dating violence. Heterogeneity was high (I 2 = 52%; χ 2 18.81; degrees of freedom 9; p value .03) and likely to be the result of the different scales used to assess knowledge. Using a random-effects model, the SMD was 0.44 (95% CI: [0.28, 0.60]). We discuss the implications of the high level of heterogeneity in the discussion (Figure 7).

Knowledge of relationship violence. Notes: Higher scores indicate better knowledge. (1) Recognition of abusive behavior. (2) Sexual assault awareness survey. (3) 7th grade inventory of knowledge. (4) Authors’ own knowledge scale. (5) Authors’ own knowledge questionnaire. (6) Sexual assault awareness survey. (7) Knowledge and attitude of sexual violence questionnaire (knowledge component). (8) Ohio University sexual assault risk reduction program knowledge measure. (9) Comprehension of consent/coercion measure.
Skills related to relationship and dating violence
We included seven studies (1,369 participants) in the meta-analysis for skills related to relationship and dating violence. The I 2 was low at 0%, with a χ 2 statistic of 5.26 (degrees of freedom 6) and a nonsignificant p value (.51). Care must be taken when assessing χ 2 tests on a meta-analysis of a small number of studies, as the test has low power. A nonsignificant result should, therefore, not be interpreted as evidence of no heterogeneity (Higgins & Green, 2011). Using a fixed-effect model, the SMD was 0.03 (95% CI: [−0.11, 0.17]; Figure 8).
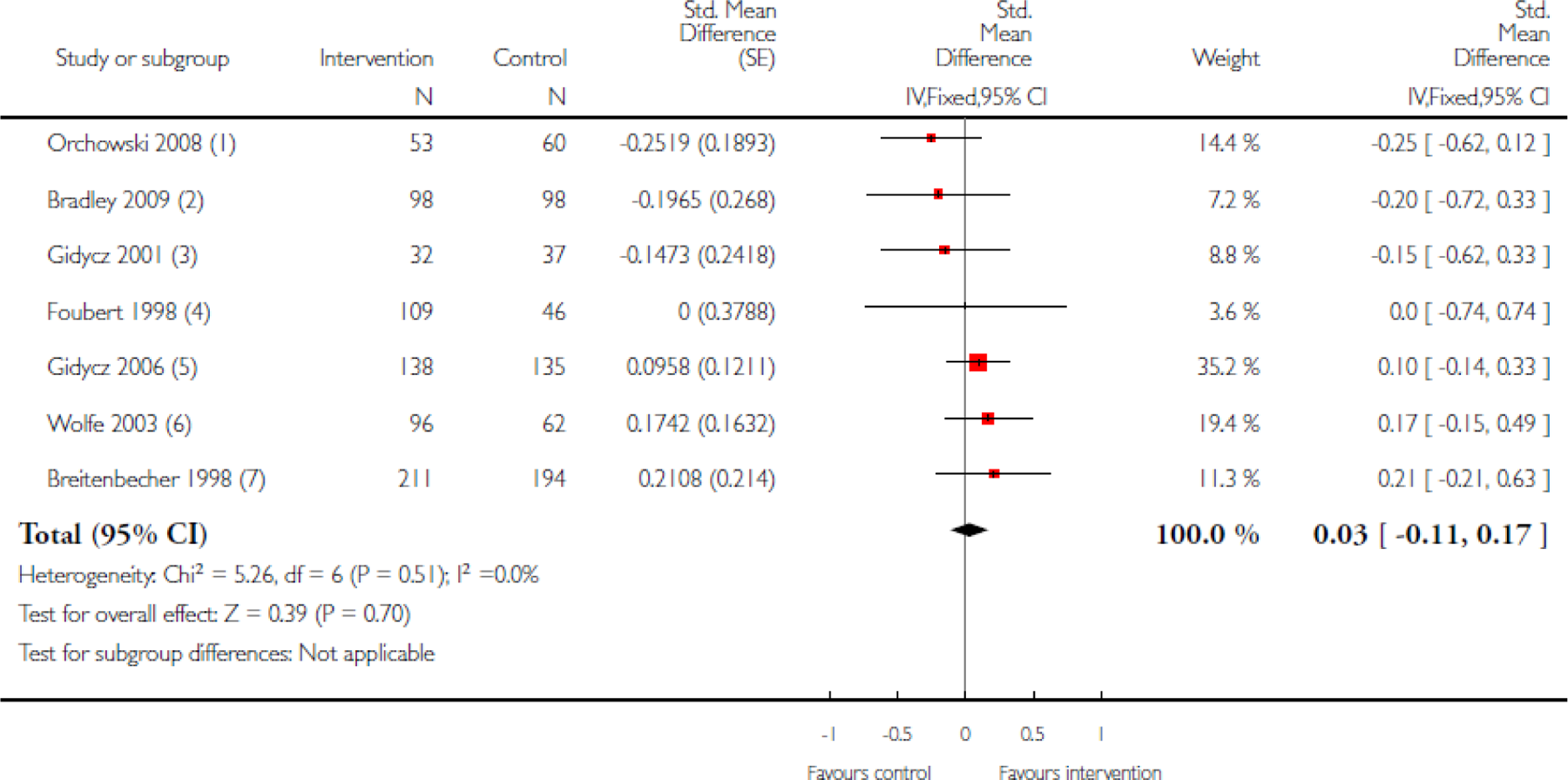
Skills related to relationship violence. Notes: Higher scores indicate better skills. (1) Sexual communication survey. (2) Sexual communication survey. (3) Sexual communication survey. (4) Behavioral intent to rape survey. (5) Sexual communication survey. (6) Adolescent interpersonal competence questionnaire. (7) Sexual communication survey.
Subgroup Analyses
Subgroup analyses were conducted to assess the effects (if any) of the setting, type of audience (general or high-risk), timing of outcome assessment and duration of intervention. For delivery setting, there was a statistically significant difference in subgroups when university-based interventions were compared with community- and school-based interventions for the outcome of knowledge of relationship violence (χ 2 6.27, p value = .01). For audience type, we found significant differences between interventions aimed at general and high-risk audiences in the episodes of relationship violence experienced and attitudes toward relationship violence. Subgroup analyses by timing of outcome assessment showed no change in outcomes. Two subgroup analyses were conducted to assess the effect of intervention duration. First, we categorized studies according to total contact time (≥1 hr; 1–5 hrs; ≥5 hrs). Second, we categorized studies according to the total number of sessions (1 session, 2–5 sessions, and >5 sessions). We found no significant differences for any of the outcomes in either model.
Sensitivity Analyses
As assessment bias and attrition bias was deemed to be low in the majority of studies (37 and 30 studies, respectively), we did not run sensitivity analyses for these domains. Limiting our analysis to the six studies at low risk of selection bias made no significant difference to results for episodes of relationship violence, attitudes, or behavior. However, a difference was seen in knowledge about relationship violence: for this outcome, only one study was at low risk of selection bias (Miller et al., 2012), the results of which showed an SMD of −0.01 (95% CI: [−0.40, 0.38]) compared to the pooled result of 0.43 (95% CI: [0.25, 0.61]). Excluding quasi-RCTs (which are at high risk of allocation bias) from the analysis made no significant difference to the pooled results of any outcomes assessed.
Discussion
Summary of Main Results
The effectiveness of interventions to prevent relationship and dating violence can be quantified by a number of different outcomes. We assessed changes in the episodes of relationship violence experienced, behaviors, attitudes, knowledge, and protective skills attained. For all outcomes apart from knowledge change, meta-analyses showed no evidence of a statistically significant effect. In the meta-analysis for knowledge of relationship violence, interventions appeared to have a beneficial effect. However, there was substantial heterogeneity (I 2 = 57%) between studies and when we excluded studies at moderate or high risk of selection bias, only one study remained which showed no evidence of any effect. Overall, therefore, this review has found no evidence of effectiveness of interventions on the outcomes reported.
The outcomes addressed by the studies included in our review can be categorized into two groups: direct measures, which we included as our primary outcomes, and proxy measures, which we included as our secondary outcomes. Health outcomes, which constituted two of our primary outcomes, were not assessed by any of the included studies. This noticeable absence is an important finding in itself, especially given that associations between violence and health have been extensively documented, and represents a significant gap in the existing literature. Assessing the frequency of dating and relationship violence is another direct measure. This outcome is challenging to measure for a number of reasons. The stigma associated with relationship violence in some settings may lead to fear of disclosing or reporting episodes of violence. In some cases, violent behavior may be long-standing and may be perceived as “normal,” with victims blaming themselves for the violent behavior of their partner and not seeking support. Peer pressure or the fear of retaliation may prevent victims from seeking help and, especially among adolescents, there may be poor knowledge about support services available. When cases are reported, information may not be available to researchers due to the nondisclosure of personal and sensitive information by officials. Large studies with long follow-up periods are required in order to capture all events reliably.
Proxy measures such as changes in attitudes, behavior, knowledge, and skills are more commonly reported outcomes. These measures contribute to violence but require translation into action in order for a reduction in violence to occur. Further research is required to assess whether, and if so, how, changes in these proxy measures translate into reduced rates of relationship violence.
Limitations
The aim of our review was to provide a comprehensive and unbiased summary of the existing evidence on interventions to prevent dating and relationship violence in adolescents and young adults. However, our results should be interpreted with caution for two main reasons. First, the studies included in our review varied greatly on several aspects. Participants ranged from general (low-risk) high school and university students to individuals with risk factors for experiencing or perpetrating relationship violence. Our subgroup analyses comparing general to high-risk audiences revealed mixed results. Interventions appeared to be more effective at reducing the episodes of relationship violence experienced in high-risk audiences: the RR was not statistically significant in general audiences but indicated a small but statistically significant reduction in risk in high-risk audiences. However, when assessing changes in attitudes, the SMD was not statistically significant for general audiences and favored the control group in high-risk audiences. Notably, for both outcomes, the high-risk “subgroup” consisted of a single study. It is possible, therefore, that there were factors other than the type of participants that made these particular studies differ from others, and their results may not be generalizable to all studies with high-risk audiences.
Interventions also varied in delivery settings, types of outcomes assessed, duration of intervention, and duration of follow-up. The subgroup analysis by intervention setting was significant only for one outcome (knowledge of relationship violence) and in one setting (university vs. school and community). Given that for the remaining 17 subgroup and outcome combinations the results were nonsignificant, we feel that the single significant outcome has arisen by chance. Intervention duration ranged from single 50-min sessions to twenty-one 75-min sessions, and subgroup analyses showed no significant differences in effect by total contact hours or total number of sessions. The majority of studies assessed outcomes immediately following the intervention, with a further assessment between 1 and 12 months later. In order to determine more reliably whether interventions are effective and if so, whether their effects are long lasting and reduce the incidence of relationship violence in later adulthood, longer follow-up is required.
The second reason for interpreting our results with caution relates to methodological aspects of our review. Individual studies used a wide range of measurement scales to assess outcomes. We presented our results as SMDs, which assume that each of the assessment measures can be standardized and have comparable SDs. This method also renders the translation of results into a quantifiable improvement or deterioration in outcomes challenging. For example, it is difficult to define what a 0.03-point improvement in the combined skills score means in practice and what level of statistically significant change is clinically significant.
Completeness and Applicability of Evidence
All of the studies included in this review came from high-income countries. With the exception of Yom and Eun (2005), all studies were conducted in North America. There are a number of possible reasons for this. First, the term “dating” may be less frequently used outside of North America. However, our search strategy included the term “relationship” and other synonyms, which should have identified a broader range of titles. Second, the concept of dating itself may be less common outside of North America. In some lowerincome countries marriage occurs at a younger age, so that if violence in a relationship occurs it is more likely to be classed as IPV rather than dating or relationship violence. Finally, relationship violence may be less commonly reported and less researched in other cultures.
Most studies followed participants up to a maximum of 12 months and provide little evidence on the long-term effectiveness of these interventions. The majority of studies assessed changes in proxy measures such as attitudes and knowledge rather than episodes of violence and behavioral change. Further studies are required to explore the interaction of knowledge and attitudes with behavior, skills, and episodes of relationship violence.
The quality of most studies in this review was limited by unclear methods of random sequence generation, allocation concealment, and assessor blinding. Another significant concern was the cluster or quasi-cluster randomization methods used in 19 of the included studies. Participants were randomized by schools or classes to decrease the risk of cross contamination and for practicality. Only one study used an ICC to account for the effect of clustering, though the ICC used was low compared to ICCs of other similar studies. The results of the cluster-RCTs included in this reviews are, therefore, likely to overestimate the effects of the interventions. Finally, many included studies had small numbers of participants and short periods of follow-up, which is likely to affect their quality adversely by decreasing their statistical power and increasing the risk of type I and type II errors.
Eighteen studies that appeared by title or abstract to meet our eligibility criteria could not be assessed because full texts were not available despite requesting interlibrary loans, contacting authors, and corresponding with universities in the case of doctoral theses. We do not know how the results of these studies would have affected our results. It is possible that the irretrievable studies are in themselves the result of a publication bias; in other words, it may be that the very reason we found these studies difficult to access is that they are studies with inconclusive or negative findings that are less likely to be published or more difficult to retrieve. Failure to include these studies therefore may have overestimated the effect sizes of interventions and introduced bias into this review (Higgins & Green, 2011).
Combining all outcome assessments up to 12 months into one outcome in our analysis may also have had an effect on our results. For example, it is possible that the effectiveness of interventions was greatest immediately following the intervention, with effects gradually wearing off. However, the substantial differences in outcome assessments made it difficult to assess the effects separately. There was an insufficient number of studies to perform a separate analysis of outcomes assessed between 6 and 12 months as planned.
The ICC of 0.15 that we used to adjust for the effect of clustering is likely to lead to conservative estimates of effect. However, we felt this to be the most appropriate ICC based on a review of ICCs used in meta-analyses of similar topics. It would have been preferable if individual studies had ascertained their own ICCs, or if different ICCs were available depending on whether randomization occurred at class or school level.
Agreements and Disagreements With Other Studies or Reviews
Whitaker et al., 2006 conducted a systematic review of primary prevention programs for the perpetration of partner violence. The authors found that 9 of the 11 included studies reported at least one positive intervention effect for knowledge, attitude, or behavior and concluded that such prevention programs are promising. This finding differs from the lack of evidence of an effect found in our review. However, the review by Whitaker et al. (2006) included observational (nonrandomized) trials, which may have influenced results. Results were summarized narratively, rather than by means of a meta-analysis. To our knowledge, no other systematic reviews on this topic have been conducted.
Conclusions
Implications for Practice
There is currently a wide range of interventions based on educational and community settings aimed at the prevention of dating and relationship violence in adolescents and young adults. The studies included in this review showed no evidence that these interventions reduce episodes of violence or improve attitudes, behaviors, and skills related to relationship violence. There was evidence of a small increase in knowledge, but this result must be interpreted with caution due to high heterogeneity among studies. Most studies had methodological shortcomings, which may have led to overestimation of their effects, especially when cluster randomization was used. Importantly, our results show no evidence of effect, rather than evidence of no effect. Therefore, current interventions should not necessarily be stopped, but rather further research and more methodologically sound studies should be conducted.
Implications for Research
Further evidence is required to assess the effectiveness of interventions to prevent dating and relationship violence. The current evidence is predominantly focused on assessing changes in attitudes and knowledge. Research into the effects of interventions on incidence of relationship or dating violence, and exploration of the relationship between attitudes and knowledge and skills, behavior and episodes of violence are needed. It is possible that in order to reduce the occurrence of relationship violence effectively, a number of interventions across both educational and community settings as well as within homes and families is required. Exploring these themes will require larger RCTs with longer follow-up periods.
Researchers should consider using existing reliable and validated scales such as the Rape Myth Acceptance Scale (RMAS; Burt, 1980) or the Revised CTS (Straus, Hamby, Boney-McCoy, & Sugarman, 1996). New measurement scales developed by authors have often not been adequately validated, and the use of multiple different scales renders the comparison of results from different studies difficult.
Although RCTs are preferable to cluster-RCTs, in practice it is often more feasible to conduct the latter. In this case, authors should adjust results using an ICC to avoid overestimating the effect of the interventions. We identified ICCs from a number of meta-analyses on similar topics by searching CENTRAL. However, a wider and more systematic search would be helpful in ascertaining the range of ICCs used across cluster-RCTs and establishing the most appropriate ICC figure to use.
With one exception, all studies were conducted in North America. Interventions addressing relationship violence are likely to be highly culturally sensitive and it is important to understand what types of interventions are effective in different settings. Further studies are, therefore, required from high-, middle-, and low-income countries in Europe, Asia, Africa, and Australasia.
Footnotes
Acknowledgments
We thank Geraldine Macdonald, Director of the Institute of Child Care Research, Queens University, Belfast, for editorial comments; Laura MacDonald, former Managing Editor, Cochrane Developmental, Psychosocial and Learning Problems Group, for guidance on writing up our findings; Margaret Anderson, Trials Seach Co-ordinator for the Cochrane Developmental, Psychosocial and Learning Problems Group, for developing and carrying out the search strategy; Marialena Trivella, Senior Medical Statistician and Cochrane Training Co-ordinator at the UK Cochrane Centre, and Rafael Perera, Lecturer in Medical Statistics at the Department of Primary Care Health Sciences, University of Oxford, for their statistical advice.
Authors’ Note
This article is based on a Cochrane review first published in the Cochrane Library 2013, Issue 6. Cochrane reviews are regularly updated as new evidence emerges and in response to feedback, and the Cochrane Library should be consulted for the most recent version of the review. The results of a Cochrane review can be interpreted differently, depending on people’s perspectives and circumstances. Please consider the conclusions presented carefully. They are the opinions of the review author, and are not necessarily shared by the Cochrane Collaboration.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.