
Abstract
Objective:
This study examines the effect of an ecological and contextually responsive approach, during initial intake call, on engagement for multistressed families seeking child mental health services in an urban setting.
Methods:
Using a randomized design, parents were allocated to phone Intake As Usual (IAU) or Enhanced Engagement Phone Intake (EEPI). IAU consisted of a lengthy mandated standardized phone intake interview. EEPI, wrapped around the standard intake, was a flexible approach, attuning to the parent’s concerns, help-seeking experience, and stressors and incorporating problem-solving and motivational interviewing.
Results:
Controlling for child gender, child age, income, and marital status, parents in the EEPI condition were 3 times more likely to attend their initial face-to-face agency appointment and subsequent treatment services.
Conclusions:
This study contributes to building the evidence base for early engagement approaches responsive to families’ broader ecological context to ensure that vulnerable children and families access and receive benefits of treatment.
Keywords
Internationally, government bodies and leading researchers have identified the prevention and treatment of child mental health problems as an urgent public health priority (Centers for Disease Control & Prevention [CDC], 2013; Health Canada, 2002; Loeber & Farrington, 2001; Patel, Flisher, Hetrick, & McGorry, 2007; Reppucci, Fried, & Schmidt, 2002; Sanders, 1995; U.S. Department of Health and Human Services, 1999; U.S. Public Health Service, 2000; Waddell, McEwan, Shepherd, Offord, & Hua, 2005; World Health Organization, 2003). Though there is variability across studies and reporting methods, the prevalence of child mental health disorders has been estimated at 14–26% (Brandenburg, Friedman, & Silver, 1990; Costello, Egger, & Angold, 2005; Manion, 2010; Offord & Lipman, 1996; Willms, 2002) and even greater in disadvantaged and urban families (Kazdin, Mazurick, & Bass, 1993; McLoyd, 1998; Tolan & Henry, 1996; Webster-Stratton & Hammond, 1998). Yet only a small percentage of these children and families receive available services (Katakoka, Zhang, & Wells, 2002; National Institute of Mental Health [NIMH], 2001; Offord et al., 1987; Waddell et al., 2005). The gap between child mental health needs and service reach in the United States and Canada is comparable with approximately 75% of children who need mental health services not receiving them (Manion, 2010; NIMH, 2001; Offord et al., 1987). This article addresses the critical need to reduce this gap in urban multistressed families with children with conduct problems by focusing on increasing engagement during initial contact for services, a key time point that significantly influences service access. The current study examines the effect of an ecological and contextually responsive approach used during a phone intake interview on engagement for multistressed families seeking child mental health services.
Conduct disorder (CD) and attention-deficit hyperactivity disorder are among the most prevalent mental health diagnoses (CDC, 2013; Kazdin, Siegel, & Bass, 1990; Loeber & Farrington, 2001; Offord, Boyle, & Racine, 1991; Robbins, 1991). Worldwide analyses have shown average rates of CD to be approximately 6%, with a range from 5% to 14% (Merikangas, Nakamura, & Kessler, 2009). Conduct problems can account for nearly 50% of clinic referrals (Kazdin, 1995) and are highly represented in public service sectors (Garland et al., 2001). Early conduct problems foreshadow increasingly serious problems across the life span, contributing to the development of social patterns that take the child or youth along a path that limits life choices and full participation in their communities. As they become adolescents, children with an early history of aggression are at high risk for antisocial behavior and related social problems including delinquency, violence, drug use, school failure, depression, and risky sexual behavior (Conduct Problems Prevention Research Group, 1992; Dishion, Patterson, Stoolmiller, & Skinner, 1991; Fergusson, Horwood, & Ridder, 2005; Loeber & Farrington, 2001). Without treatment, these disorders may persist into adulthood with a range of negative consequences (Moffitt, Caspi, Harrington, & Milne, 2002; Odgers et al., 2008), underscoring the need for early intervention and cost-effective evidence-based treatments.
The attendant social and financial burdens of CD profoundly impact not only the child and family but also the larger community including education, social, and policing systems. Without adequate intervention, the lifetime cost of one case of CD is estimated to exceed US$1.5 million (Cohen, 1998). Clearly, an early history of conduct problems has immense negative consequences for individual youths, for their families, and for others in their environment as well as for society at large in terms of both human and economic costs.
While the cause, consequences, and continuity of CD appear to be complex and multifactorial, parenting and family functioning play a key role, either directly or as mediating influences, in the development and maintenance of conduct problems (Burke, Loeber, & Birmaher, 2002; Loeber & Stouthamer-Loeber, 1986; Patterson, 1982; Stormshak, Bierman, McMahon, & Lengua, 2000). The family environments of children with CD have been shown to be highly coercive with patterns of harsh and/or unresponsive parenting marked by low levels of parent involvement and supervision and inconsistent discipline (Murray & Farrington, 2010; Odgers et al., 2008; Patterson, 1982; Webster-Stratton & Taylor, 2001). Having a child with conduct problems and coercive interactions contributes to parent stress and low mood through a reciprocal dynamic whereby the influence of parents on child behavior is, to an extent, reliant on the characteristics and behaviors of a child (Grusec, 2011; Stern & Smith, 1999). Parents of children with externalizing behaviors report more negative feelings about parenting and more negative impact on their social life, in addition to higher levels of child-related stress (Donenberg & Baker, 1993; Harpin, 2005). Furthermore, externalizing comorbidities have been shown to increase parental strain and the prevalence of disturbances in family and marital functioning as well as parent–child relationships (Harpin, 2005).
Engaging these multistressed parents in mental health services for their children with conduct and co-occurring problems is critical. Strengthening parenting skills and modifying coercive family interactions are at the heart of evidence-based intervention. Not only are adult caregivers the ones who bring children to treatment, but their engagement in services is essential to achieving change in children with conduct problems. Parenting programs informed by social learning and cognitive behavioral strategies are the most extensively validated intervention for children’s social, emotional, and behavioral problems including early onset conduct problems specifically (Brestan & Eyberg, 1998; Centers for Disease Control & Prevention (CDC), 2004; deGraaf, Speetjens, Smit, de Wolff, & Tavecchio, 2008; Eyberg, Nelson, & Boggs, 2008; Furlong et al., 2012; Gardner, Burton, & Klimes, 2006; Webster-Stratton & Taylor, 2001) and among the most economical interventions available to promote children’s mental health (CDC, 2004; Foster, Prinz, Sanders, & Shapiro, 2008; Mihalopoulos, Vos, Pirkis, & Carter, 2011).
What is concerning, however, is that these programs are not necessarily reaching the children and families they are designed to help. Among families seeking services for child mental health problems, a high number do not actually begin treatment after initially contacting a community agency or, if they do, have high rates of attrition at different time points over the course of treatment (Kazdin, Holland, & Crowley, 1997; Kazdin & Mazurick, 1994; McKay & Bannon, 2004). Initial engagement and retention issues pose serious challenges across children’s service sectors. Attrition rates of 40–60% have been reported in the literature (Armbruster & Fallon, 1994; Harrison, McKay, & Bannon, 2004; Kazdin et al., 1997; Kazdin & Mazurick, 1994; McKay, McCadam, & Gonzales, 1996a) with even higher rates (50–75%) for the most vulnerable families who face multiple barriers to accessing services (Kazdin et al., 1993).
Parents’ initial decision to seek service is profoundly influenced by their beliefs about the child’s problem, perceived value of treatment, perception of barriers, and past experiences in service systems (Kerkorian, McKay, & Bannon, 2006; Owens et al., 2002; Raviv, Sharvit, Raviv, & Rosenblat-Stein, 2009). For example, the odds of a child being brought in for an initial appointment decreases if parents report skepticism about the helpfulness of treatment (McKay, Pennington, Lynn, & McCadam, 2001). Ongoing attrition rates as treatment progresses have been shown to be associated with parents feeling overwhelmed, experiencing multiple stressors (Friors & Mellor, 2009; Harrison et al., 2004), and family difficulties (Gopalan et al., 2010). Johnson, Mellor, and Brann (2008) found the highest levels of dropout occurred for families with higher levels of psychosocial difficulties and problems involving family dynamics. Similarly, Attride-Stirling, Davis, Farrell, Groark, and Day (2004) found that parents who discontinued their child’s mental health treatment were more likely to have begun with multiple family problems and reported being both isolated and overwhelmed by the many problems they faced.
Further, evidence also suggests that low-income urban families are less likely to initially engage or be retained in treatment services (McKay, Stoewe, McCadam, & Gonzales, 1998; Snell-Johns, Mendez, & Smith, 2004). The vulnerability of these families is amplified by interrelated adversities in their broader social ecology including issues such as poverty, social isolation, community violence, racism, and lack of access to resources (Attar, Guerra, & Tolan, 1994; Bell & Doucet, 2003; Coulton & Pandey, 1992; Gustafsson, Larsson, Nelson, & Gustafsson, 2009; Ingoldsby & Shaw, 2002; Stern & Smith, 1995; Stern, Smith, & Jang, 1999; Tolan & Henry, 1996).
Rates of initial no show and ongoing attrition are especially high among families seeking services for child conduct problems (Gopalan et al., 2010; Kazdin et al., 1997). Early dropouts are characterized by more severe child conduct problems (Kazdin & Mazurik, 1994), and it has been found that families of children with conduct problems are more inconsistent in treatment attendance and less likely to be retained in treatment than others (Watt, Hoyland, Best, & Dadds, 2007). Not surprisingly, when families drop out of treatment, children with conduct problems are more likely to have poor outcomes compared to children who remained in treatment (Kazdin & Wassell, 1998; Lanier et al., 2011). Children from urban multistressed families are at a higher risk for both child conduct and other mental health problems, while simultaneously experiencing more barriers to service access.
Kazdin’s (1996) influential barriers to treatment model suggests that families seeking or participating in treatment can experience multiple barriers that highlight both environmental and social contexts. Past research has divided barriers to service into structural or practical and perceptual categories. Practical barriers are associated with the demands of daily life and include obstacles such as child care concerns (Gross, Julion, & Fogg, 2001; Lamb-Parker et al., 2001; Mendez, Carpenter, LaForett, & Cohen, 2009), transportation, scheduling conflicts (Fawley-King, Haine-Schlagel, Trask, Zhang, & Garland, 2013; Garvey, Julion, Fogg, Kratovil, & Gross, 2006; Heinrichs, Bertram, Kuschel, & Hahlweg, 2005; Mendez et al., 2009), and lack of time (Barlow, Kirkpatrick, Stewart-Brown, & Davis, 2005). These barriers may be linked to or compounded by other factors, such as low socioeconomic status and/or single parenthood (Baker, Arnold, & Meagher, 2011; Heinrichs et al., 2005; Williams et al., 1995). Although a range of practical barriers have been shown to interfere with parent engagement, families will often work around these as long as the treatment offered matches the parent’s preference for services (Bannon & McKay, 2005). Structural barriers would include agency-level factors, such as inconvenient hours, waiting lists, and providers not contacting the family, significant issues that have been demonstrated as barriers to accessing services at a systems level (Harrison et al., 2004; Staudt, 1999). Consequently, these factors both hamper families’ abilities to initially engage in a program and prevent their continuation.
Perceptual barriers encompass beliefs within the individual and family that impact willingness to participate, including attitudes toward services and cultural norms. Beliefs about mental health, stigma, parent expectations, perceptions of treatment relevance and demands, and cognitive attributions have been found to be particularly salient barriers (Kazdin, 2000; Kazdin et al., 1997; Kazdin & Wassell, 2000; Morrissey-Kane & Prinz, 1999; Nock & Kazdin, 2001). Moreover, evidence suggests that when parents have previously sought help, feeling disrespected by providers was highly predictive of reporting doubt about the utility of treatment as a barrier. Together, these variables accounted for the endorsement of a greater number of barriers to access in the future (Kerkorian et al., 2006). On the flip side, parents with positive expectations that the proposed treatment is a good match and will be helpful for their child perceive fewer barriers to treatment, which is associated with subsequent higher rates of participation (Nock, Ferriter, & Holmberg, 2007; Nock & Kazdin, 2001). For minority group families, differences in child-rearing beliefs and practices, perceived racial discrimination, doubts concerning provider cultural competence, community social stigma, and shame have been reported as barriers to treatment (Coombs, Levene & Augimeri, 2006; Enang, 2001; Li & Browne, 2000; McMiller & Weisz, 1996; Wood & Newbold, 2012).
Interventions to Increase Engagement
Multiple strategies to increase parent engagement include interactions that build readiness for treatment, attend to families’ negative prior experience, expectations of services, and address potential structural and perceptual barriers (Berger & Shepard-Umaschi, 2011). In a seminal series of studies on phone engagement for a family therapy program for drug-abusing youth and their families (strategic structural systems engagement [SSSE]), the rates of initial attendance at an intake appointment were significantly higher for families who received SSSE. Based on structural family theory, the SSSE targeted family interaction patterns that might be a barrier to the family coming for treatment, with the practitioner beginning to establish an alliance with the parents, promote self-efficacy, and use reframing strategies (Santisteban et al., 1996). There were mixed findings on retention with significantly increased ongoing participation and family therapy completion favoring SSSE in two studies, but no difference between conditions in a third (Coatsworth, Santisteban, McBride, & Szapocznik, 2001; Santisteban et al., 1996; Szapocznik et al., 1988).
In a second influential series of studies, McKay and colleagues (McKay et al., 1996a; McKay, Nudelman, McCadam, & Gonzales, 1996b; McKay et al., 1998) demonstrated the significance of the first telephone contact with families for increasing initial engagement and involvement in treatment for inner city families. The telephone intervention aimed to clarify the need for services, maximize the caregiver’s investment and self-efficacy in seeking help, address previous experiences with mental health services and attitudes toward them, and create strategies to overcome practical barriers (McKay et al., 1998; McKay et al., 2004). These studies indicate that the phone engagement increased attendance at a first face-to-face interview between 24% and 29%. However, significant differences between conditions for ongoing service participation occurred only when the phone engagement was combined with additional focused engagement strategies in the initial interview (McKay et al., 1996b, 1998). Cavaleri, Gopalan, McKay, Messam, and Elwyn (2010) extended this work to multiple child mental health agencies through a learning collaborative showing that these strategies elicited an increase in client engagement for initial appointments (5–21%) as well as ongoing treatment attendance (2–16%) for the four of five agencies that implemented them.
Recent studies also have demonstrated the benefits of using motivational interviewing techniques to engage families in children’s mental health treatment (Ingoldsby, 2010; Sterrett, Jones, Zalot, & Shook, 2010). Power and colleagues (2010) retrospectively examined pretreatment phone contact using nonjudgmental strategies from motivational interviewing to promote attendance at an initial treatment session for referred families in a large urban setting. They found that 82% of families who spent more than 10 min on the phone with a clinician attended an initial session and only 18% of families who spent less than 10 min on the phone attended the initial session.
Taken together, the research findings indicate that focused strategies including addressing barriers at the start of a treatment program can enhance engagement in services (see Gopalan et al., 2010, Ingoldsby, 2010; McKay & Bannon, 2004; Mendez et al., 2009; Staudt, 2003). However, findings on the impact of phone engagement strategies on retention over the continuum of service have been more mixed than on initial appointment show rates (e.g., McKay et al., 1996b, 1998; Santisteban et al., 1996). Furthermore, research suggests that evidence-based interventions are least likely to benefit the most disadvantaged children and families because they often fail to address the broader ecological context and factors that undermine parents’ well-being and ability to engage in needed services (McKay & Bannon, 2004; Stern et al., 1999; Stern & Smith, 1995). The experience of multiple adversities places children in double jeopardy: These adversities disrupt parenting with negative consequences for children’s development and decrease the likelihood of participation in and completion of the very services that target enhancing skilled parenting and the development of healthy family relationships and child well-being.
Current Study
This study’s conceptual framework was guided by a social–ecological model (Bronfenbrenner, 1986, 1997) based on an understanding that families are embedded in interdependent social and environmental contexts and Kazdin’s “barriers to treatment” model, which shows that families experience barriers that make independent contributions to attrition beyond the known stressors (e.g., poverty, single parenthood, and parent depression) that predict dropout. Rather than concentrating on dropout as primarily a client function, this perspective focuses on the clinician’s knowledge and skill in fostering a meaningful, responsive engagement process.
Embedded in an ongoing university–community collaboration, this research was a randomized controlled study in a Canadian urban multicultural setting in a children’s mental health center in Toronto, Ontario. The Ontario mental health system typically involves a multistep process for accessing universally available services that are paid for by the government. A unique aspect of the study is the development of a contextually responsive enhanced engagement component within a lengthy government mandated structured phone intake screening process.
Child Development Institute (CDI), the community agency partner, offers two evidence-based, manualized, gender-specific interventions for latency age children with serious conduct problems. The model, Stop Now and Plan (SNAP®), has been rigorously evaluated with positive treatment and cost–benefit effects (Augimeri, Farrington, Koegl, & Day, 2007; Burke & Loeber, 2014; Farrington & Koegl, 2015; Pepler et al., 2010). The core treatment components in both interventions are concurrent parenting and child groups, based on social learning and cognitive–behavioral theory within a social–ecological framework. Some clients also receive family and/or individual counseling. CDI serves disadvantaged and highly stressed families from culturally diverse backgrounds and has experienced the attrition issues described in the literature. Annual baseline attrition rates from phone intake to a first face-to-face appointment for the 2 years prior to the study were similar to those described in the literature (41% SNAP boys and 46% SNAP girls; Koegl, 2006; Couch, 2007).
Our research hypotheses were as follow: (1) parents who receive an Enhanced Engagement Phone Intake (EEPI) will show for the first face-to-face assessment interview significantly more often than parents in the standard condition who receive phone Intake As Usual (IAU) and (2) parents who receive the EEPI are more likely to continue in treatment subsequent to the initial face-to-face appointment relative to parents in the standard IAU condition.
Method
Consent and Procedures
Ethics approval was obtained through the University of Toronto Health Sciences Research Ethics Board. The study was conducted over a 2-year period (October 2009–September 2011) within an urban children’s mental health center, which was the community partner agency. Using the program N Query Advisor (Hodges & Pihlstrom, 1998) with power set at 80% and probability at .05, we determined a sample of 144 participants (72 per group) was needed to detect a moderate effect size. Based on the agency’s annual baseline referral and attrition rates, we projected 16–24 months would be sufficient to obtain the sample.
The agency intake is a multistep process reflecting the provincial requirements described subsequently. When parents first call CDI seeking services for their child, a government-mandated service inquiry record (SIR) is administered to ensure that the referred child meets basic admission criteria for programs offered (e.g., age, presenting concerns, and catchment area). If there is not a match, the family is referred to an agency that would better meet their needs.
Consent for the study was obtained during the initial SIR screening call for those deemed appropriate for intake screening and programming. Parents were invited to participate in a study examining the best way to ensure families get the help they need when seeking services for their child. Callers were given the opportunity to ask questions and were informed of their right to refuse to participate without jeopardizing service. These informed verbal consents were documented in line with the approved ethics protocol.
Measures
SIR
Using government-mandated screening tool, the agency collects information on parent gender, marital status, child gender, child age, number of presenting concerns, and child’s prior mental health diagnosis.
Brief Child and Family Phone Interview (BCFPI)
The BCFPI is a mandated computer-assisted intake telephone interview based on the Diagnostic Interview Schedule for Child Version IV (DISC-IV) and the Ontario Child Health Study’s self-report scales (Cunningham, Boyle, Hong, Pettingill, & Bohaychuk, 2009). The BCFPI screens for attention-deficit hyperactivity disorder, oppositional defiant disorder, CD, separation anxiety, generalized anxiety, and major depression in children and adolescents, as well as parental mental health problems. It correlates moderately to highly with the DISC-IV subscales (Cunningham et al., 2009). The BCFPI includes a family functioning subscale adapted from the General Functioning Scale of the McMaster Family Assessment Device rated on a 4-item response scale from strongly agree to strongly disagree, with a demonstrated high internal consistency (α > .80; Boyle et al., 2009). The scales have been demonstrated as equivalent for males and females, and over a 13-month period, the BCFPI showed test–retest reliabilities higher than .50 for all disorders with the exception of major depression (Boyle et al., 2009). Two additional scales are created to assess severe and extreme cases. Severe is defined as scoring in the clinical range (70 and greater) on three of the four following scales: Total Child Mental Health Problems, Child Global Functioning, Global Family Situation, and Managing Mood and Self Harm (six mood questions and three self-harm questions). Extreme is defined as scoring clinical on all four scales. The BCFPI also asks parents to indicate the extent to which six barriers (i.e., transportation, financial burden, service availability, location and time, child care services, and literacy) could impede their participation in treatment.
Study Design and Intake Conditions
Using a randomized stratified design, consented parents were allocated to either EEPI, the experimental condition, or IAU, the control condition. A random number generator was utilized to assign each sequential intake to either the EEPI or IAU condition. The sample was stratified on child gender to ensure that there was no bias reflecting agency history of a higher volume of calls requesting service for boys than girls.
Standard intake (IAU) consisted of the government-mandated computer-assisted administration of the BCFPI (Cunningham et al., 2009) to assess the referred child and family mental health issues and needs followed by a brief discussion of available agency services, the SNAP program, and any practical barriers. If the child meets admission criteria, an appointment is scheduled for the first face-to-face interview at the agency. Admission criteria for the program include (a) children between 6 and 11 years of age, and (b) scoring in the clinical range (70 or greater) on the externalizing scales of the BCFPI, or (c) having police contact. Children are excluded from the program if they demonstrate a significant developmental delay.
The experimental intake (EEPI) comprised a 10- to 15-min enhanced engagement component that was wrapped around the administration of the BCFPI. The enhanced engagement protocol was guided by McKay and colleagues’ work and shared similar goals and strategies. The threefold goals of the EEPI were to (1) develop rapport between the parent and the intake worker (IW) based on a shared understanding of family needs and concerns, (2) identify and address likely barriers to the family’s participation in treatment, and (3) increase parental self-efficacy, hope, and treatment motivation. The IW conducting an EEPI took an ecological and contextually responsive approach when attuning to the caller’s concerns, help-seeking experience, and stressors. This approach aims to convey that the caller is heard and understood, to clarify needs, and to explore and support the parent in problem-solving potential barriers to treatment attendance. Starting the call by overviewing the purpose and what will happen during the interview, the IW conducting an EEPI socializes the parent to the intake process in a transparent and collaborative manner. The IW also goes beyond identifying and problem-solving practical barriers that are included on the standard BCFPI to following cues from the parents’ responses to probe for the range and complexity of barriers identified in the literature (e.g., perceptual, parent mental health, cultural, and systemic). During the interview process, the IW incorporates strategies of motivational interviewing (Miller & Rollnick, 2002) when indicated, finishing up with four questions that specifically target intent to pursue treatment and hope. The intent of the EEPI protocol is not to provide a rigid structured script but to guide and allow the IW the flexibility to meet the goals of the EEPI in a family responsive manner.
Pilot testing
The EEPI protocol was piloted by the agency with five families prior to implementation to test for feasibility. The combination of the BCFPI administration and the enhanced component took an average of 45 min to 1 hr. This timing was equivalent to the administration time for the BCFPI alone, which varied according to how much a particular parent expanded on his or her answers or wanted to talk. All the parents in the pilot were receptive and responded positively when asked if they were ready to proceed with the next step to the face-to-face interview.
IWs
IWs included agency staff and interns in the helping professions doing a practicum at CDI, the majority of them were master of social work (MSW) students. A new cohort of practicum students was trained in each of the 2 study years. Two agency staff, one in each condition, and 11 interns were involved in the study as IWs. All but two were female. The two cohorts of four social work students in each year were randomly assigned to condition once the practicum office notified the principal investigator of the placement and prior to the researchers knowing who they were. Three other interns were assigned to IAU as their placement dates did not coincide with the beginning of the academic year and EEPI training dates. All interns committed a half-day per week to being available for phone intakes. Intakes were assigned to IWs based on matching the parent’s preferred interview time to the IW’s availability with an attempt to balance assignments. All interns received the same introduction to the agency and to the scientist–practitioner model.
Training and fidelity
IWs for both conditions were trained in the administration of the BCFPI, using the agency standard training procedures. Each IW had an individual review to ensure that equivalent standards were met across both conditions. IWs for the EEPI condition were introduced to the research literature on engagement barriers, factors related to attrition, and effective engagement strategies and trained in the structured protocol for EEPI interviews designed to incorporate the empirical findings. During the training workshops, a variety of case examples were used to illustrate scenarios IWs might encounter followed by role-plays of intake phone calls. The project director and agency clinical director provided ongoing review and supervision conducted on site reflective of CDI’s supervision protocols and at a level typical for intake screening. IWs also had access to the manager of research who conducts the standard training on the BCFPI and addresses any issues that arise.
IWs in both conditions audiotaped their side of the intake interview calls for fidelity checks. A subset of tapes (n = 32) was rated on 5-point Likert-type scales on specific elements of engagement (e.g., hope, efficacy, and collaboration) by an MSW student blind to condition. The rater provided examples to illustrate ratings that were reviewed by the project director or principal investigator. We also conducted a check for contamination between conditions through an online survey. IWs as usual were not aware of the specific study hypotheses or the difference in the training and materials. Both IAU and EEPI workers indicated that they had not talked with one another about the study. Moreover, as reported in fidelity outcomes, only IWs in the EEPI condition used motivational interviewing questions designed to increase parental intention to participate, suggesting IAU workers were not aware of them.
Outcome Variables
Engagement was measured on the basis of no show or attendance at the initial face-to-face interview following phone intake and at subsequent points in treatment. According to CDI policy, families are considered “no show” after two consecutive cancellations or failures to come for appointments, and no response to two follow-up contact attempts. We measured subsequent points in treatment as (1) any treatment attendance after the first face-to-face agency appointment (e.g., group, family, or individual) and (2) attendance rate at the parent and child group sessions. Since prior agency research has shown that completion of eight or more sessions is associated with more positive treatment outcomes (Koegl, Farrington, Augimeri, & Day, 2008), we further examined whether there was a difference between conditions for program completion.
Sample
Of the total 165 consecutive callers during the study period, consent was asked of 151, with 14 callers not asked, either because the call was a crisis situation (5) and needed to be responded to in an urgent fashion that did not allow implementation of the study protocols or because of language barriers (9). Of the remaining 151 callers, 117 (78%) consented to take part in the study. Thirty-four (22%) callers declined to participate for the following reasons: chose not to be part of a research study (n = 7), were too busy (n = 21), ill (n = 2), overwhelmed (n = 2), other (1), or did not meet study criteria (1). An additional 18 were lost after randomization but prior to receiving the phone interview, 3 in each condition were referred elsewhere, and IWs were unable to contact the rest. Ninety-nine callers (EEPI: n = 45; IAU: n = 54) received the intake interview, constituting the final sample for analysis (see Figure 1 for study participant flow chart).
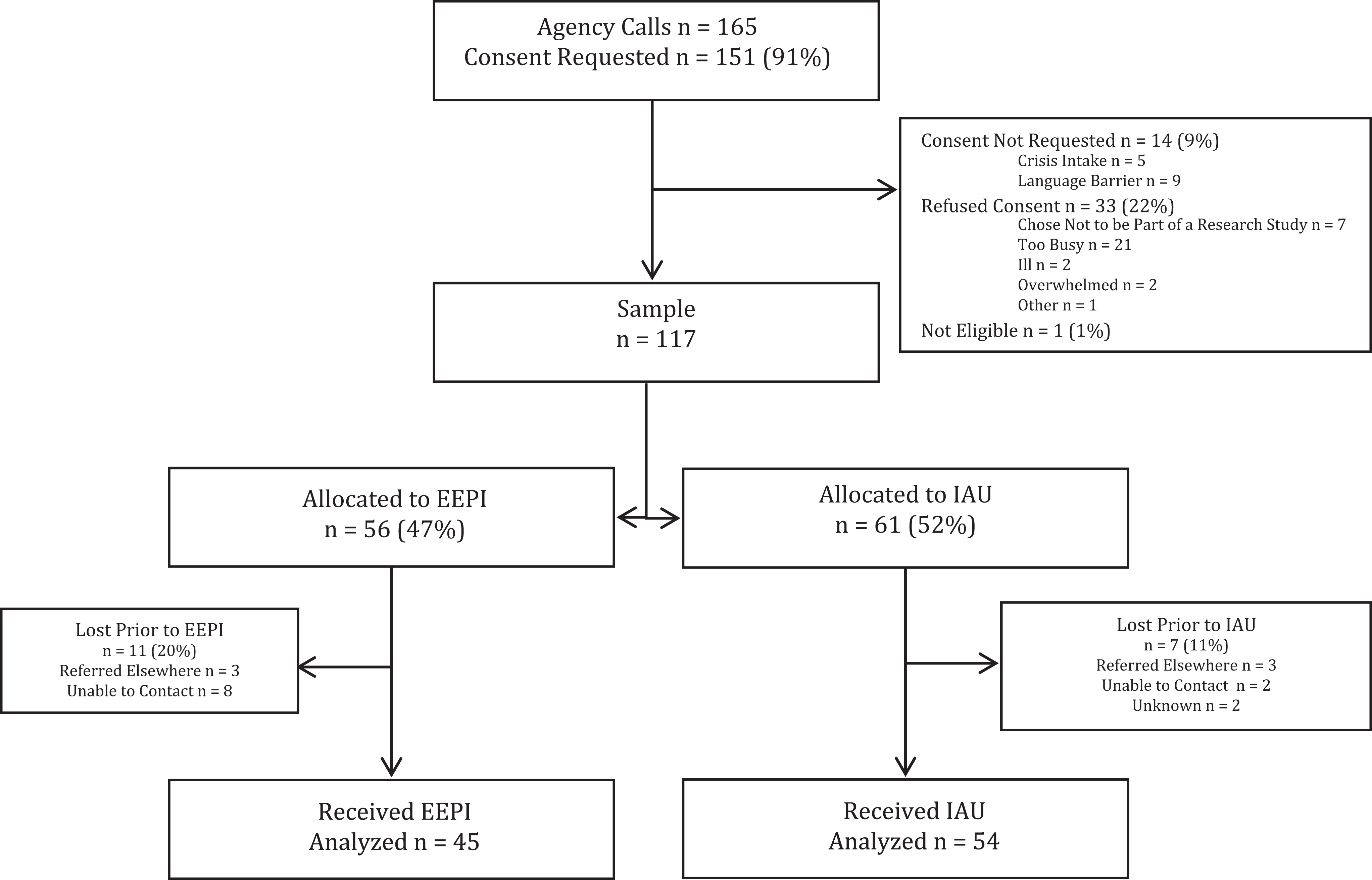
Flow of study participants.
Demographics
Parent and child demographic variables were included for analysis. Of the 117 parents who agreed to participate in this study, all but 2 (1 grandmother and 1 relative) identified as the child’s parent. Ninety-four percent of parents were female. About 50% reported being married or in a common-law relationship and half reported being a single parent, divorced, or separated. For the most part, parents were referred to services by their child’s school or day care (57%), child welfare (11%), a mental health professional (10%), or through a website or internal referral (8%). For the child sample, 70% were boys and 30% were girls. Child age at intake ranged between 5 and 12 years and averaged 8.69 years (standard deviation [SD] = 1.76). The majority of the parents (73%) reported that their child did not have a mental health diagnosis prior to the study. The number of concerns reported by parents ranged from 1 to 7, with an average of 2.72 concerns. About 22% of parents reported four or more concerns.
Data Analysis Method
Univariate and bivariate analyses were conducted to examine sample characteristics between conditions. The effect of intake condition on parent participation in the initial face-to-face interview and subsequent treatment was analyzed using logistic and linear regressions.
Results
Bivariate analyses were conducted to examine differences in parents’ and children’s characteristics between participants who were lost prior to commencement of the intake conditions (n = 18) and those who participated (n = 99). Using the limited demographic information collected during the brief screening call on the SIR, we found no significant differences on marital status, child’s gender, child’s age, child’s prior mental health diagnosis, or number of presenting concerns between parents who did not participate in the interview and those who did.
For those who received a phone intake in the EEPI or IAU condition (n = 99), the majority of participants (96%) were female. Forty-eight percent reported being married or in a common-law relationship. Participants were Caucasian Canadian and Caucasian European (40%) and multiethnic (35%) and others identified only their nationality. Most parents reported having an educational status higher than secondary. About 35% of participants had an income below CA$29,999, with 42% reporting an income above CA$50,000. Nineteen percent of parents reported four or more presenting concerns at intake, with the majority of participants (83%) indicating one or more practical barriers to receiving services. Child characteristics reported by parents indicated the majority were boys (69%) between 5 and 12 years old. At intake, children on average were 8.62 years old (SD = 1.76). The majority of the parents (72%) reported their child did not have a mental health diagnosis (see Table 1).
Sociodemographic Description of Sample by Condition.
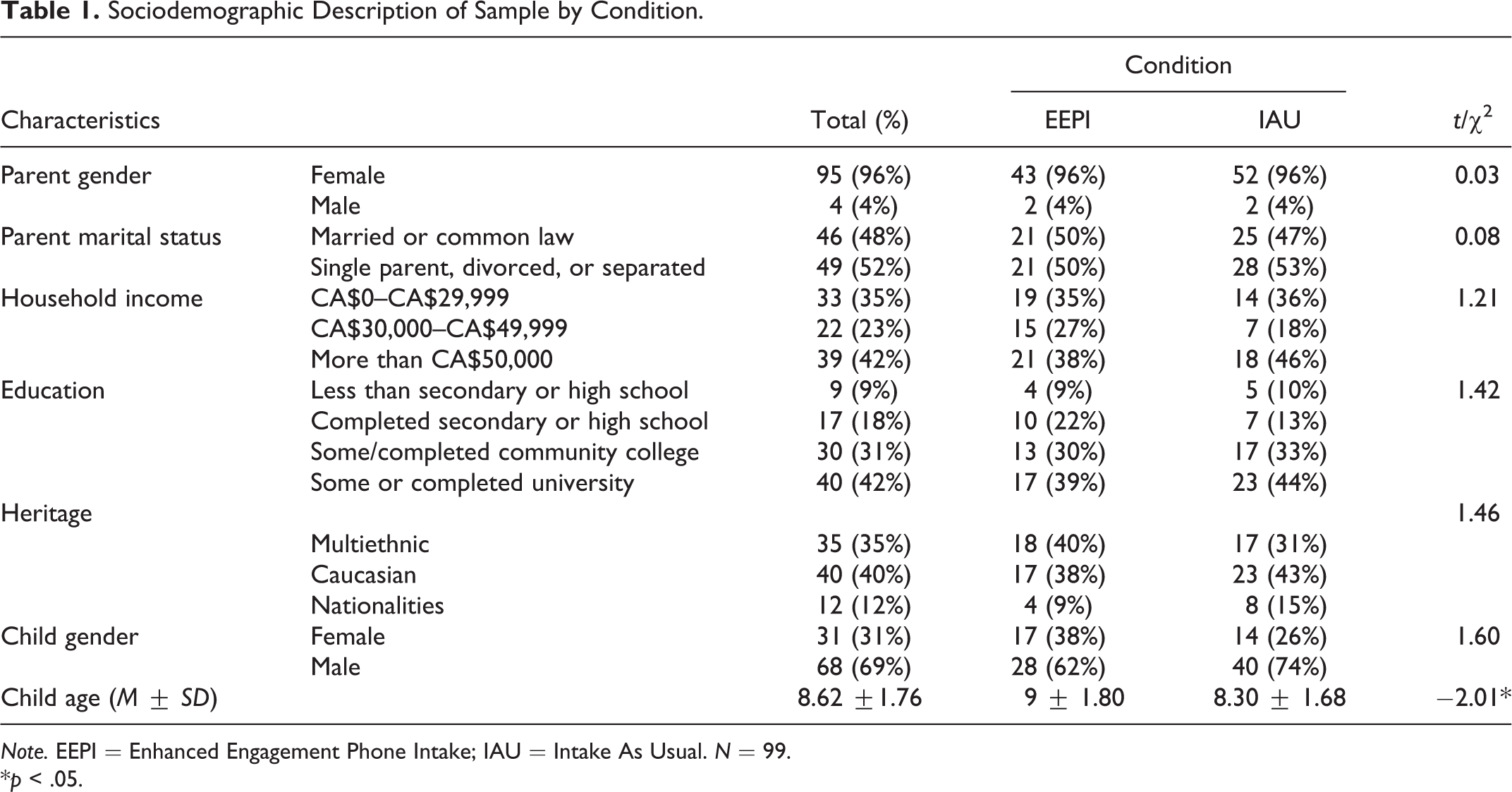
Note. EEPI = Enhanced Engagement Phone Intake; IAU = Intake As Usual. N = 99.
*p < .05.
Family and child functioning were assessed (see Table 2). The majority of families were highly stressed, scoring in the clinical range (70 and greater) on family global functioning (66%), child global functioning (58%), child conduct problems (65%), and externalizing behavior (68%). Parents reported child cruelty to animals (18%) and fire setting (2%). Twenty-seven percent of children had been exposed to traumatic events. Nearly half of the children scored clinical on more than one child externalizing behavior scale indicating comorbidity (49%) with 30% comorbid across externalizing and internalizing scales. While 59% of children were reported to bully their peers, many children were also reported to be victims of bullying behavior (84%). Twenty-two percent of families were categorized as “severe” and scored in the clinical range on three of the four scales: Total Child Mental Health Problems, Child Global Functioning, Family Global Functioning, and Self Harm. About 16% of families were classified as “extreme” and scored clinical on all four scales.
Family Ecology.

Note. EEPI = Enhanced Engagement Phone Intake; IAU = Intake As Usual. N = 99. Percentages may not add to 100% due to missing data.
Bivariate statistics were conducted to examine any differences between conditions and demographics information, comparing the 45 (45%) families in the EEPI condition with the 54 (55%) families in the IAU condition. Using χ2 analyses, we found no significant differences between conditions for parent gender, marital status, income, parent educational status, child gender, prior child mental health diagnosis, and number of concerns. Independent sample t-tests revealed a significant difference between conditions on child’s age at intake. Children in the EEPI condition were slightly older (M = 9, SD = 1.80) than children in the IAU condition (M = 8.30, SD = 1.68), t(97) = −2.01, p < 0.05. Based on Cohen’s (1988) criteria, the effect size was moderate for age at intake (d = .40). Although we did not consider it developmentally meaningful from a theoretical or clinical perspective, we controlled for age in subsequent analyses.
Differences between mental health indicators and conditions were also analyzed. No significant differences were found between conditions and family global functioning, parent mental health, child global functioning, total child mental health, mood and self-harm, noncooperativeness, conduct, attention/impulsivity, externalizing behavior, internalizing behavior, comorbidity externalizing behaviors, comorbidity internalizing behaviors, bullying others, being bullied, fire setting, animal cruelty, child trauma exposure, and practical barriers (i.e., none, one or more barriers). There were also no differences in the proportions of children rated in the severe and extreme categories.
Hypotheses
To answer the first hypothesis that parents who receive the EEPI will show for the first face-to-face assessment interview significantly more often than parents in the standard condition who receive phone IAU, χ2 analyses were used. Results approached significance between condition and first face-to-face, χ2 = 3.59; df = 1; p < .058. Specifically, 76% of parents in the EEPI condition attended their initial agency appointment compared to 57% of parents in the IAU condition. We conducted logistic regression to test our hypothesis that the condition predicts the likelihood that a parent attends a face-to-face interview. Controlling for child gender, child age, income, and marital status, we found that the odds of attending a first face-to-face interview for parents in the EEPI condition was 3.19 times higher than for parents in the IAU condition, b = 2.13, Wald χ2(5) = 10.64, p < .05 (see Table 3).
Predictors for Attendance of First Face-to-Face Interview.

Note. CI = confidence interval; SE = standard error; OR = odds ratio.
*p < .05.
The second hypothesis posited that parents who receive the EEPI are more likely to continue in treatment subsequent to the initial face-to-face appointment relative to parents in the standard IAU condition. χ2 analyses were conducted to examine the difference in service attendance and dosage by condition. When examining between the conditions and participation in any treatment service, significant differences were found, χ2 = 3.81; df = 1; p < .05, with a moderate effect size (d = .40). Seventy-one percent of parents who receive an EEPI participate in service compared to 52% of parents in IAU. Controlling for child gender, child age, income, and marital status, parents in the EEPI condition are 3.10 times more likely to attend treatment service than parents in the IAU condition, b = 2.26, Wald χ2(5) = 7.33, p < .05 (see Table 4). This study confirms a strong and positive association between the EEPI condition and use of any service by parents. There were no significant differences between the conditions and number of parenting or child group sessions attended or for completion rates.
Predictors for Attendance of Any Treatment Service.

Note. CI = confidence interval; SE = standard error; OR = odds ratio.
*p < .05.
Fidelity Outcomes
IWs in the EEPI condition were significantly more likely to instill hope (M = 3.93, SD = 0.96) than IAU workers (M = 2.78, SD = 1.20), t(24) = −2.60, p < .05 (see Table 5). The magnitude of the effect size (d = 1.06) was large. There was also a statistically significant difference between conditions, χ2 = 21.93; df = 1; p < .001, with a large effect size (d = 3.52) on asking questions drawn from motivational interviewing to increase parents’ intention to pursue treatment and hopefulness. Specifically, it was found all IWs in the EEPI condition asked these questions, while none in the IAU did. Ratings were higher though not significant for the EEPI condition on dimensions of fostering parental efficacy, socialize, match, overall engaging style, being nonjudgmental, and collaborative. Active listening and validating scores were higher though likewise not significant in the IAU condition (see Table 5).
Differences in Means for Fidelity Measures by Condition.

Note. EEPI = Enhanced Engagement Phone Intake; IAU = Intake As Usual; SD = standard deviation. N = 32.
*p < .05.
Discussion and Applications to Practice
This study was conducted at an urban multicultural child mental health center that offers an evidence-based program to multistressed families whose children exhibit externalizing and comorbid disorders. The results reinforce prior findings in the literature on the positive effects of phone engagement interventions. Even in the current study’s context, in which we had a lengthy government-mandated standardized instrument, we were able to incorporate engagement strategies with positive impact. The attrition rate from the intake phone interview to the first face-to-face appointment was 24% for parents in the EEPI condition versus 43% for parents in the IAU condition. These rates are consistent with those found in other phone engagement studies (Cavaleri, Gopalan, McKay, Messam, & Elwyn 2010; Coatsworth et al., 2001; McKay et al., 1996a, 1996b, 1998; Santisteban et al., 1996). Further, even though other investigators have reported mixed findings with regard to the impact of phone engagement strategies on continuing in treatment, we found that parents who received the EEPI were significantly more likely to have attended any treatment service in the SNAP program, whether core groups or family/individual counselling. The two logistic regressions showed that after controlling for child age, child gender, income, and marital status, the odds of attending the first face-to-face and any continued treatment service were significantly higher for parents in the EEPI condition.
There were no differences however between conditions specifically on number of group sessions attended or on completion. Once families began services at CDI, attrition was extremely low and most families completed service with only four dropouts in total, limiting the variability for analyses of ongoing attendance. The low ongoing dropout rate in this study contrasts with the higher rates typically found in the literature, both for child mental health services overall and more specifically for evidence-based parenting groups (Thomas & Zimmer-Gembeck, 2007).
Fidelity findings indicated that IWs in the EEPI condition implemented the protocol consistent with their training. While ratings varied, EEPI workers on average were rated higher on engaging tone and style, promoting parental efficacy, collaboration, attending to expectations and treatment match, and using nonjudgemental language; these dimensions have all been suggested as important elements for parent engagement (Gopalan et al., 2010; McKay et al., 1996b, 1998; Szapocznik et al., 1988; Thompson, Bender, Lantry, & Flynn, 2007; Watt, Dadds, Best, & Daviess, 2012). The significant finding for motivational interviewing questions indicates evidence of no contamination between conditions as EEPI workers were uniquely trained to incorporate these questions. The significant finding on hope may reflect a second unique aspect of the EEPI protocol with a specific emphasis in training on tapping into a caller’s motivation to get their child help, conveying hope to often overwhelmed and discouraged parents that they had come to the right place to get that help and encouraging the parent to believe that change is possible. While previous investigators have identified the potential importance of hope for increasing caregiver initial engagement in family-based intervention (Coatsworth et al., 2001; Szapocznik et al., 1988; Watt et al., 2012), it has not been systematically assessed in parent engagement research.
Importantly, during the study, enhanced engagement procedures were easily integrated into everyday agency practice. The phone IWs included the agency’s regular phone intake staff and students doing a practicum at the agency and selected through regular agency procedures, not by the research investigator. Though IWs who conducted the EEPI received specialized training in enhanced engagement strategies, ongoing supervision was reflective of typical agency practice, thus practical for real-world implementation. Other than training itself, incorporating the EEPI into an agency’s standard intake procedures would not require additional resources or add agency burden, increasing the likelihood of sustainability. The caveat here is that to monitor the impact of engagement strategies (e.g., attendance rates) with ongoing feedback to IWs and supervisors would be important. Cavaleri et al. (2007) found that not having a data collection system was one of the top barriers to sustaining engagement practices for agencies that had participated in a learning collaborative to improve service use.
We underscore that it is as important to train and devote resources to evidence-based engagement as it is to evidence-based treatment if children and families are to benefit from the advances that have been made in addressing children’s mental health problems. Those involved in the initial contact with a family are in a unique position to influence future engagement and the likelihood that high-risk, multistressed families and their children receive needed supports.
This study focused on increasing client attendance rates at the first face-to-face appointment following a two-step phone intake process (e.g., brief screening and structured intake interview). However, there were a number of dropouts between the two calls, with 15% of parents not reaching the full phone intake interview. Unfortunately, each additional step potentially adds another obstacle that families must navigate in order to receive the help they are seeking. This barrier may be of particular concern to families facing multiple daily stresses and demands. Losing some parents right at the point they reach out for help draws attention to the organization of services and systemic barriers families often confront and the importance of simplifying and enhancing access procedures. From the very first contact, focus needs to be on engaging and collaborating with families with basic strategies to build rapport and a shared understanding of family needs, identify and address barriers, and foster treatment motivation and hopefulness. Streamlining the intake process may have considerable payoffs for parents and agency capacity to respond to potential clients. In a follow-up qualitative study our team conducted on help seeking and engagement decision making with parents who had participated in this study, one of the themes that emerged was the tenacity needed to navigate the maze of services and jump through hoops to get their children the help needed.
This study highlights implications not only for policy and practice but for the ongoing integration of evidence-based engagement practices into social work education. Commonly, both academic and practicum learning tend to focus more on establishing and maintaining a therapeutic alliance with individuals and families once they enter treatment. Equal importance needs to be placed on understanding the need for early engagement approaches during the initial intake contact and on effective skills training.
While not significant between conditions, the effect of the EEPI in increasing first face-to-face attendance rates showed a strong statistical trend. As in much real-world research, issues in the broader context impacted the study. In this case, the agency referral rates were initially lower than the typical rate due to renegotiation of community protocols unrelated to the research. Thus, the sample size computed by the power analysis was not attained in the anticipated time, and we were unable to extend into another year, given the funding and logistic constraints for training an additional cohort of practicum students as IWs. Despite this limitation, we view the increased odds and the first agency appointment attendance rate of parents who received an EEPI compared to IAU as clinically meaningful. Another limitation is that in our logistic regressions, we were unable to control for ethnic minority status, given the overlapping categories with a number of parents identifying their heritage as a nationality, which could be inclusive of diverse ethnicities. This is not surprising in Toronto, given the diversity of ethnic and minority status and the multiple ways that individuals identify.
Even though some promising directions emerged in the fidelity data, these findings need to be interpreted cautiously. Only the IW’s side of the conversation was taped, making it challenging to code some parts of the interviews. Our ability to assess interrater reliability and increase confidence in the external validity of the results was limited because a second rater left the study after training for a job opportunity in another city. Additionally, the coded tape sample was a subset of the full sample and the small sample size might have decreased the likelihood of finding more significant differences. Next steps include further investigation with a larger sample of the taped calls to shed more light on what were the core components of the EEPI protocol that contributed to increasing parent engagement.
In an effort to address the compelling need to close the gap between calling and coming to service, we evaluated a contextually responsive approach for enhancing engagement for multistressed families seeking child mental health services in an urban setting. The key finding is that incorporating a brief enhanced engagement component into an intake call increases the odds threefold that children and their parents will attend their initial agency appointment and any continued treatment service subsequent to the initial appointment. These results add to our knowledge on implementation feasibility and effectiveness of early engagement strategies in the “real world” of community practice. This study contributes to building the evidence for an engagement approach responsive to families’ broader ecological context to ensure that vulnerable children and families access and receive the benefits of evidence-based treatment.
Footnotes
Acknowledgments
The authors gratefully acknowledge Reet Mae, Leena Augimeri, Lina Catania, and the dedicated students who contributed as research assistants and intake workers throughout this study. We thank our colleague Mary McKay for sharing her expertise over the course of this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Social Sciences and Humanities Research Council of Canada, Standard Research Grant 410-2008-1424 (PI: Stern).