
Abstract
Objective:
This study explored the feasibility of stepped care trauma-focused cognitive behavioral therapy (SC-TF-CBT) relative to TF-CBT with children (aged 8–12).
Method:
Children (N = 33) with post-traumatic stress symptoms (PTSS) were randomly assigned (2:1) to SC-TF-CBT or TF-CBT. SC-TF-CBT consisted of Step 1, parent-led therapist-assisted treatment, and Step 2 (nine TF-CBT sessions). TF-CBT consisted of 12 therapist-directed sessions. Baseline, post-Step 1, posttreatment, and 3-month follow-up assessments occurred. Cost-related data were collected throughout the treatment.
Results:
In all, 64% (intent-to-treat) to 82% (completers) responded to Step 1. Group × Time interactions were not statistically significant for PTSS (p = .888), severity (p = .576), and internalizing (p = .862)/externalizing (p = .974) symptoms, indicating comparable improvements in outcomes across both conditions. There were no significant differences in parental treatment credibility (p = .440), expectations (p = .664), and satisfaction (p = .768). SC-TF-CBT total costs were significantly lower than TF-CBT (Effect Size [ES] = 1.61, confidence interval [CI] = [0.65, 2.59], p < .0001).
Conclusion:
Step 1 may be a viable service delivery approach although further research is needed.
Between 68% and 80% of children are exposed to potentially traumatic events with an estimated one third exposed to more than one type of trauma (Copeland, Keeler, Angold, & Costello, 2007; Finkelhor, Ormrod, & Turner, 2009). Trauma-focused cognitive behavioral therapy (TF-CBT) is a well-established evidence-based practice for children exposed to traumatic events (Silverman et al., 2008). TF-CBT has demonstrated superiority to active treatments and wait-list conditions (Cohen, Deblinger, Mannarino, & Steer, 2004; Deblinger, Stauffer, & Steer, 2001; King et al., 2000) but lasts 3–6 months and requires therapist-delivered weekly face-to-face sessions. This treatment approach may be difficult for some families to access, especially low-income families with limited resources (Bringewatt & Gershoff, 2010). Due to the prevalence of trauma and barriers to treatment, new service delivery approaches that incorporate effective interventions are needed.
Limited access to effective treatment, parents’ desire to be the primary person helping their child, and treatment costs are potential barriers to children receiving trauma-focused treatment. Inaccessibility may be due to the limited number of trained clinicians, inconvenient scheduling, or transportation (Bringewatt & Gershoff, 2010). Davis, Ressler, Schwartz, Stephens, and Bradley (2008) found that lack of transportation, costs, health, childcare and family care, and work schedules were the highest rated barriers among low-income urban African American children with undiagnosed post-traumatic stress disorder (PTSD). Parents have reported that a major barrier to seeking treatment for themselves and their children is their desire to solve the problem independently (Thurston & Phares, 2008).
To address treatment barriers, new service delivery approaches such as stepped care interventions have been developed (e.g., Tolin, Diefenbach, & Gilliam, 2011). Stepped care provides interventions in steps with different levels of intensity. First-line treatments are less intensive (e.g., less costly, less therapist time, and more convenient for patients) than traditional interventions where trained providers deliver treatment. Preestablished criteria are used to indicate when a patient is stepped up to receive additional treatment or if treatment should end. For patients who do not improve after the first step, subsequent interventions are available, and the resources (i.e., therapist time and costs) are reserved for those needing more intensive treatment. Some stepped care models have all patients start with a lower intensity of care and proceed through the steps as needed (Bower & Gilbody, 2005). However, stepped care interventions, also known as adaptive interventions, can have baseline tailoring variables (specified characteristics) that are used to assign patients to the best intensity or type of care initially and then change subsequent treatment options as variables change (Collins, Murphy, & Strecher, 2007).
Based on CBT for childhood trauma (Cohen et al., 2004; Scheeringa, Weems, Cohen, Amaya-Jackson, & Guthrie, 2011), the use of minimal therapist assistance (Salloum, 2010), telehealth, bibliotherapy (Lyneham & Rapee, 2006), computer-assisted treatments (Khanna & Kendall, 2008), and a stepped care model for young children after trauma (Salloum, Robst, et al., 2014), we developed a version of stepped care TF-CBT (SC-TF-CBT). This version of SC-TF-CBT consists of a first-line parent-led therapist-assisted treatment (i.e., Step 1) and standard TF-CBT (i.e., Step 2) for children who need to step up. For minimal therapist assistance in Step 1, we chose three therapist sessions as prior TF-CBT studies have used the criteria of attending at least three sessions to be considered in the completer analyses (Cohen et al., 2004). We added phone support distributed throughout the intervention to allow enough time for the therapist to support and coach the parent to complete a trauma-focused workbook with the child during 11 at-home parent–child meetings. Given the pilot nature of this study, and limited data on what tailoring variables would be best to match children at baseline to Step 1 or standard TF-CBT, we randomly assigned all children at baseline to Step 1 or standard TF-CBT. Therapists provided treatment across conditions as therapist skill was assumed equal. The therapist dose response was not assumed. We assumed the combination of treatment components in Step 1 would be comparable to therapist-led treatment in standard care but that not all children would respond to Step 1. If a substantial number of children respond to Step 1 and maintain treatment gains, efficiency in delivering treatment would be improved as not all children would have to receive therapist-directed treatment. SC-TF-CBT is designed to be more efficient and cost effective than standard treatment while maintaining comparable changes in outcomes as standard treatment. Thus, the current study tests a new service delivery approach (e.g., SC-TF-CBT) designed to achieve results comparable to a widely used evidence-based practice (e.g., TF-CBT) while potentially improving accessibility, efficiency, and cost-effectiveness of treatment for children after trauma.
The primary aims and hypotheses of this pilot study were as follows: (1) To examine whether SC-TF-CBT (Step 1 plus Step 2 if needed) is comparable over time to TF-CBT in terms of child outcomes (post-traumatic stress as the primary outcome, severity of global functional impairment, internalizing and externalizing symptoms, and depression diagnosis). It was hypothesized that the improvements in all child outcomes would change at similar rates over time for children in SC-TF-CBT and TF-CBT. (2) To compare parent credibility of treatment between conditions at baseline and parent satisfaction at posttreatment. It was hypothesized that parental credibility and expectation of treatment scores at baseline would not significantly differ, and there would be no significant difference in parent satisfaction scores at posttreatment. (3) To gather preliminary data on the cost of delivering SC-TF-CBT compared to TF-CBT. It was hypothesized that the cost of delivering SC-TF-CBT would be significantly less than the cost of delivering standard TF-CBT.
The secondary aims related to the general knowledge about the implementation of SC-TF-CBT were to (1) establish an estimate of the percentage of children who respond to Step 1, (2) examine whether treatment response to Step 1 was maintained at posttreatment and 3-month follow-up, and (3) pilot the feasibility of stepping up nonresponders to Step 2.
Method
Participants
Participants were recruited from July 2011 to May 2013 at a community-based nonprofit trauma counseling program located in an urban setting. When the parent or guardian seeking child trauma treatment called for services, an agency intake worker completed a prescreening assessment to see whether the participants met the initial eligibility criteria (e.g., age, parents able to participate, not in substance abuse treatment, spoke English, and the child was on medication, if the regimen was stable for at least 4 weeks) and whether the parent was interested in participating. Referrals primarily came from child welfare organizations (e.g., child protection, child investigation, and child welfare case managers), victims’ services programs (e.g., domestic violence and victim advocate programs), the agency’s programs (e.g., former clients and crisis call center), schools and mental health centers. Further screening of all inclusion and exclusion criteria occurred at the baseline assessment after consent and assent were obtained. Consecutive admission occurred. Inclusion criteria included (a) the child was between 8 and 12 years of age at the time of enrollment; (b) similar to prior TF-CBT studies (e.g., Cohen et al., 2004; King et al., 2000), the child had experienced at least one trauma with at least five Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) defined PTSD symptoms; (c) the parent/guardian was willing and able to participate in treatment (e.g., no serious medical or mental health condition or had means of transportation). Exclusion criteria were (a) parent/guardian or child had any condition that would limit the caregiver’s ability to understand CBT and the child’s ability to follow instructions (e.g., psychosis and mental retardation), (b) parent/guardian had substance use disorder within the past 3 months, (c) child/parent was suicidal, (d) child/parent was not fluent in English, (e) the child was not on a stable medication regimen for at least 4 weeks prior to admission (if applicable), (f) the parent/guardian treatment participant was the perpetrator, or the perpetrator lived in the home, and (g) in cases of siblings, one was randomly selected to participate and the other one was referred to agency services.
Procedures and Research Design
This study was approved by the university’s institutional review board. Parents/guardians provided written informed consent and children provided assent. Since SC-TF-CBT is in the early stages of development and TF-CBT is well established, there was a 2 (SC-TF-CBT) to 1 (TF-CBT) randomization ratio for this pilot randomized clinical trial. A statistician independent of the study developed a computerized randomized block procedure using Splus (v8.2) that was used by the first author to assign cases to a condition. Once it was determined by the blinded independent evaluator (IE) that the parent and child met study criteria, the first author assigned the parent–child dyad to a treatment based on the randomized list. After the parent learned that they met study criteria, he or she was provided with a one-page description of treatment, completed the Expectancy Rating Form (ERF; Borkovec & Nau, 1972), and began treatment the following week. As shown in Figure 1, 33 parent–child dyads out of 156 parents who were prescreened participated and were randomized to treatments.

Flowchart of enrollment and retention. Note. aThe guardian and child reported that the child became suicidal when the guardian initiated contact again with the child's perpetrator, which occurred after the first parent-child meeting. bThe non-responder to Step Two was referred for additional treatment and to a psychiatrist, but the parent did not follow up with these recommendations. At the follow-up assessment, the child was hospitalized due to suicidality and the ADIS was not completed.
The blinded IE, a master’s-level clinician, trained by the first, fourth, and last author, administered the measures. Assessments occurred at baseline (2 hours), after Step 1 (45 minutes), posttreatment (1.5 hours), and at 3-month follow-up (1.5 hours). All assessments with the child and parent occurred independently. Parent comfort level ending after Step 1 was completed by the parent with a research assistant. Parents were compensated US$25.00 for the baseline assessment and US$50.00 for each of the three remaining assessments.
Measures
Child measures
Anxiety Disorders Interview Schedule Child/Parent Version (ADIS-IV-C/P; Silverman & Albano, 1996) is a clinician-administered interview that was used to assess trauma exposure, child PTSD, and depression. Diagnoses were based on independent reports from children/parents combined with an overall clinical severity rating (CSR) of ≥4 (range = 0–8). There was good interrater reliability for the child (κ = .88, p < .001) and parent (κ = .96, p < .001) PTSD module between an IE and research assistant across 43.8% interviews.
University of California Los Angeles (UCLA) PTSD Index for DSM-IV (UCLA PTSD-Index; Steinberg et al., 2013) is a child self-report of frequency of post-traumatic stress symptoms, which consisted of the 17-items that corresponded with DSM-IV PTSD symptoms. Total scores ranged from 0 to 68 and 38 is the clinical cutoff score (α = .88).
Clinical Global Impression–Severity (CGI-Severity) is a widely used 7-point clinician rating of severity of psychopathology (0 = no illness to 6 = extremely severe symptoms; National Institute of Mental Health, 1985). Interrater reliability was .85.
CGI-Improvement (Guy, 1976) a modified 8-point version (Salloum, Robst, et al., 2014; Research Unit on Pediatric Psychopharmacology, 2001) was used to rate treatment improvement (e.g., 1 = free of symptoms, 2 = much improved, 3= improved, to 8 = very much worse). The CGI-Improvement ratings were reviewed by an IE and the last author who were both blinded to condition.
Child Behavior Checklist (Achenbach & Rescorla, 2001) for children of age 6–18 years measures internalizing and externalizing symptoms based on parent reports. T scores were used (scores ≥ 63 indicate clinical range).
Parent measure
Structured Clinical Interview for DSM-IV-TR Axis I Disorders (First, Spitzer, Miriam, & Williams, 2002) was used at baseline to assess for substance abuse, psychosis, PTSD, and depression for exclusion criteria and for descriptive purposes.
Process measures
The ERF (Borkovec & Nau, 1972) adapted version consists of 4 items on a 10-point scale about parents’ expectations of treatment credibility and success and 1 item rating (0–100%) parental expectations of improvement (α = .89).
Client Satisfaction Questionnaire (CSQ; Nguyen, Attkisson, & Stegner, 1983) is a widely used 8-item self-report of treatment satisfaction completed by parents at posttreatment. Scores range from 8 (very dissatisfied) to 32 (very satisfied) (α = .93).
The Parent Comfort Level Ending after Step 1 involves 1-item administered after Step 1 where parents were asked “Do you feel like your child needs more trauma-focused treatment, or do you feel like you could comfortably stop treatment at this point?”
Cost measures
The Therapist/Patient Time Tracking System (Salloum & Robst, 2011) tracks therapist and patient time related to treatment participation and was completed by the therapist after every treatment activity related to delivering both treatments (e.g., face-to-face therapy, phone calls, and documentation). Parents reported homework and waiting for appointment times to the therapist.
Cost Characteristics Information (Robst & Salloum, 2011) estimates costs associated with the treatment that are not directly related to participation in treatment such as lost income due to missing work to attend therapy, travel costs, and payment for treatment.
Interventions
Four community therapists provided treatment and were assigned clients in both conditions based on parents/guardians’ scheduling needs. Two therapists had a master’s degree in social work and two therapists had a master’s degree in counseling. Therapists’ experience post-master’s was 5 months, 9 months, 2 years and 5 months, and 4 years and 10 months, and they treated 3, 11, 17, and 2 clients, respectively. All the therapists provided treatment in both conditions except for one (the least experienced) who provided treatment to only three children assigned to SC-TF-CBT. Group supervision occurred weekly and was overseen by the first author, who is a social worker, and TF-CBT consultation from the fifth author was provided as needed. Therapists completed a fidelity checklist after every session and therapy sessions were audiotaped (see Treatment Fidelity section). The average number of therapist-led sessions was 2.91 (2.07) for SC-TF-CBT and 9.82 (3.84) for TF-CBT.
SC-TF-CBT
Step 1 was a parent-led therapist-assisted CBT treatment where the parent and child met with the therapist 3 times (60 minutes) every other week. At each therapy session, the parent was given one section of a three-part parent–child workbook called Stepping Together (Salloum, Scheeringa, Cohen, & Amaya-Jackson, 2010) that was based on the Preschool PTSD Treatment manual (Scheeringa et al., 2011). The therapist reviewed with the child and parent the parts of the workbook to be completed at home parent–child meetings. The parent and child completed the workbook at home by having 11 parent–child meetings during Step 1. Workbook activities consisted of learning skills (e.g., identifying feelings, rating feelings, and relaxation), developing a trauma narrative and a fear hierarchy of trauma reminders, and completing exposures. In the first meeting with the therapist, the therapist provided psychoeducation about the effects of trauma, helped the parent and child establish a behavior plan if needed, provided an overview of the relaxation skills that were reviewed in the workbook, explored motivation and potential barriers to completing the workbook, and provided Part 1 of the workbook to the parent. The first section of the workbook is called “Just for You” which provides psychoeducational information to the parent and provides an overview of the book. In Meetings 1–4 (i.e., Part 1 of the workbook), behavior management, relaxation, affect identification and regulation, and a trauma narrative of what happened along with the child creating a “scary ladder” (i.e., stress hierarchy) of trauma reminders from easy, less stressful reminders to the worst reminder, the most stressful reminder are addressed. In Meetings 5–8 (Part 2), the parent and child address safety and safety planning and the child, with the parent present, engages in processing the trauma narrative through exposure. The child starts at the bottom of the scary ladder and in each meeting addresses through exposure a more difficult stress reminder. Exposure activities include three steps: (1) the child draws the reminder; (2) the child imagines the reminder for 30 seconds; and (3) the child, with the parent, engages in an in vivo exposure related to the trauma reminder. In the second therapist meeting, the therapist works with the parent and child to establish the in vivo activities based on the child’s scary ladder. In the third therapist meeting, the therapist reviews the parent–child workbook with the child and parent and then provides supportive counseling to the parent. In Meetings 9–11 (Part 3), the parent and child complete the exposure activities for the worst reminder, address relapse prevention skills, review the entire book, and celebrate the completion of the workbook and parent–child meetings. In addition to the workbook, a website was available for video demonstrations and psychoeducation, and weekly 10- to 15-minute phone support was provided. All the parents/guardians assigned to SC-TF-CBT had Internet access for the web-based component (for more detail about SC-TF-CBT, see Salloum, Scheeringa et al., 2014; Salloum & Storch, 2011).
After Step 1, an assessment occurred to determine “early responder status” which indicated whether the child entered the maintenance phase or Step 2. Responder status was defined as four or fewer symptoms on the ADIS-P/C, or ≤38 on the UCLA PTSD-Index and a rating on the CGI-Improvement of 1, 2, or 3. Responders entered the 6-week maintenance phase where the parent and child practiced the skills they learned. Nonresponders received Step 2, which consisted of nine TF-CBT sessions (see below for information about TF-CBT). The main difference in treatment components between Step 1 and the components of TF-CBT provided in Step 2, and standard TF-CBT is that Step 1 utilizes systematic exposure activities such as imaginal exposure and in vivo exposures, whereas in vivo exposure was not used in standard TF-CBT (see standard TF-CBT for more about TF-CBT). Since children are entering either the maintenance phase (e.g., early responders) or Step 2 (e.g., nonearly responders), the entire SC-TF-CBT is approximately 12–15 weeks, which is similar to the time children and parents often spend in standard TF-CBT.
Standard TF-CBT
Standard TF-CBT consisted of 12 (90 minutes) weekly therapist-led in-office sessions based on the components of TF-CBT (e.g., skill building and trauma narration; see Cohen, Mannarino, & Deblinger, 2006). While the intervention is based on cognitive behavioral therapy methods, there are several core values involved in the implementation of TF-CBT which include a components-based intervention, respecting cultural values, adaptability, family involvement, centrality of the therapeutic relationship, and emphasizing self-efficacy of children and families. The core goals of TF-CBT are to improve trauma-related symptoms (e.g., PTSD, depression, anxiety, etc.) and adaptive functioning. Handouts from Treating Trauma and Traumatic Grief in Children and Adolescents, which is the treatment manual for TF-CBT, were used, including information sheets for parents and children about domestic violence and child sexual abuse, relaxation, affective modulation, and practicing the cognitive triangle (Cohen et al., 2006). All the following components of TF-CBT were provided to participants who received TF-CBT in this study: psychoeducation, parenting skills, relaxation, affective expression and modulation, cognitive coping and processing, trauma narrative, cognitive coping and processing of the traumatic experience, conjoint child–parent sessions, and enhancing future safety and development.
Data Analysis
For continuous outcomes, changes in mean values as a function of group assignment were evaluated using mixed effects models with SAS Proc Mixed (v9.4) (Littell, Milliken, Stroup, Wolfinger, & Schabenberger, 2006). The advantages of these models are that they include all cases, not just those with complete data points. The main outcome of interest is the Group × Time interaction, an index of whether the groups change at similar rates over time (e.g., preassessment, postassessment, and 3-month follow-up data). The presence of a nonsignificant interaction would suggest that the magnitude of improvement was comparable across the two groups. For the binary outcomes, we used generalized estimating equations (GEEs) using SAS Proc Genmod (v9.4) and reported data based on those who completed treatment and the intent-to-treat (ITT) sample using last observation carried forward (LOCF). Similar to Tolin, Diefenbach, and Gilliam (2011), the time frame in which comparable changes were examined included from pre-to-post to follow-up.
Costs were analyzed instead of cost-effectiveness based on the findings below that children receiving SC-TF-CBT and TF-CBT improved at the same rate. Costs were compared after the completion of treatment (e.g., cost data include all costs of delivering SC-TF-CBT: Steps 1 and 2, and of delivering standard TF-CBT). Missing data for the cost analyses were limited (there were only two instances where times were missing for patient time). In these cases, we used the median time in the data set for that activity. Cost-effectiveness ratios are based on a difference in treatment efficacy, and in the absence of such differences can be reduced to a comparison of costs. Statistical significance of cost differences was assessed using SAS Proc Genmod (v9.4) with a log link to account for the nonnormal distribution of costs.
Results
Participant Flow and Sample Description
Figure 1 provides a flowchart of prescreening, enrollment, and retention. Reasons for parents declining to participate (29.5%) included 14 wanted regular agency services and did not want to participate in research, 12 unknown, 6 were not comfortable being part of the child’s treatment, 5 wanted the sibling to be in the study also, 5 had scheduling difficulties, 3 were not sure whether the child would talk with them; and 1 wanted treatment to focus on self-esteem, not on trauma (see Table 1 for sample description, and significant levels at baseline between the two conditions). In terms of the success of randomization of assignment, only parents’ age was significant. Although not reaching significance, race and parental depression differed in means. Also, there were more children who were sexually abused in SC-TF-CBT than standard TF-CBT, although when interpersonal trauma and noninterpersonal trauma were compared, there were no statistically significant differences. There were no significant differences in demographics, child and parent measures, or number of child index traumas at baseline between the 24 completers and 9 noncompleters, and dropout rates by condition were not significantly different.
Demographics, Exposure to Trauma, and Comparison of Variables After Randomization by Condition.
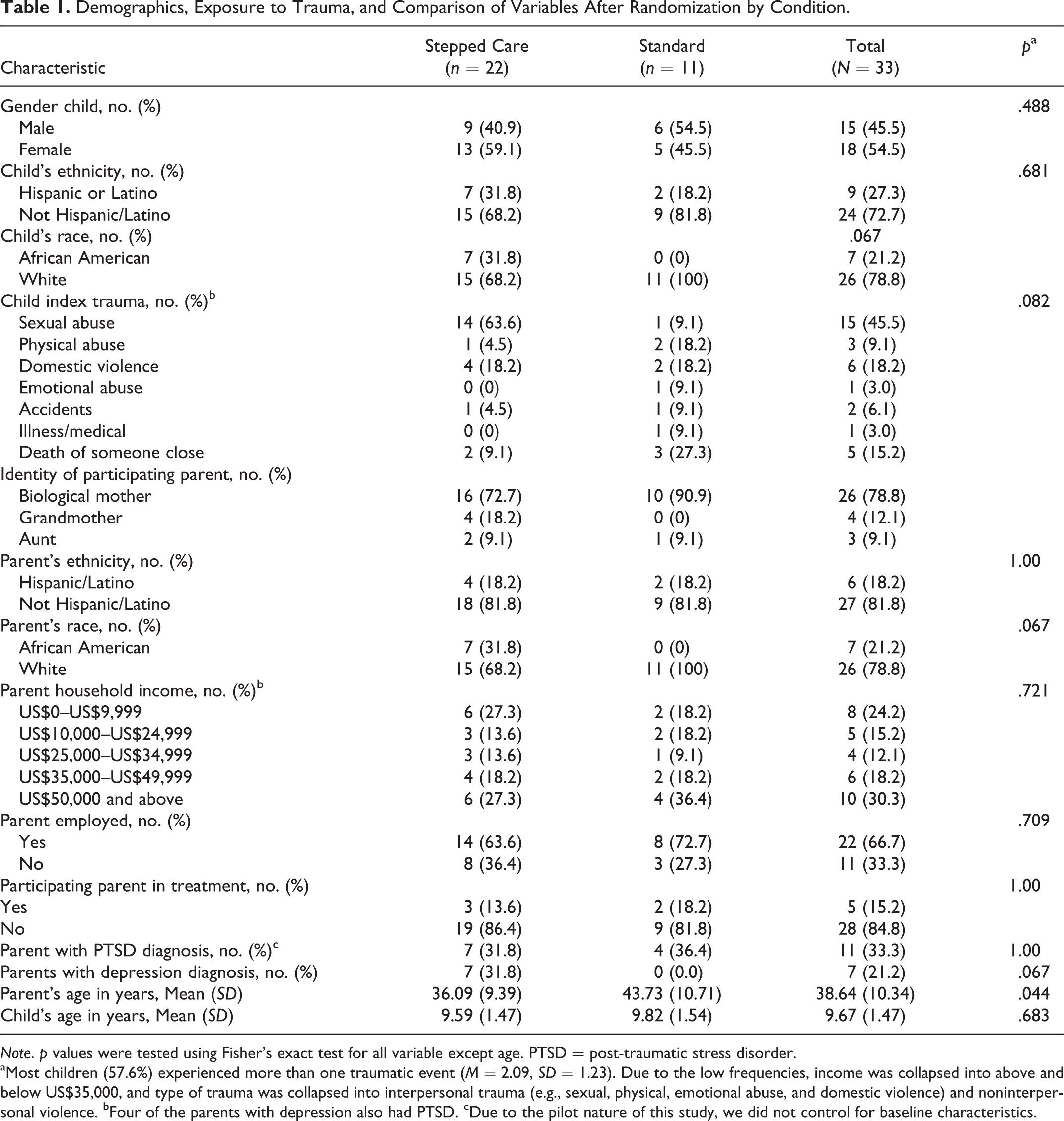
Note. p values were tested using Fisher’s exact test for all variable except age. PTSD = post-traumatic stress disorder.
aMost children (57.6%) experienced more than one traumatic event (M = 2.09, SD = 1.23). Due to the low frequencies, income was collapsed into above and below US$35,000, and type of trauma was collapsed into interpersonal trauma (e.g., sexual, physical, emotional abuse, and domestic violence) and noninterpersonal violence. bFour of the parents with depression also had PTSD. cDue to the pilot nature of this study, we did not control for baseline characteristics.
Treatment Fidelity and Number of Sessions
Forty-seven (39.2%) of 120 of the therapy sessions were randomly reviewed by a master of social work intern and the first author using fidelity checklists. Interrater agreement was .87 (p < .001) for SC-TF-CBT sessions and .92 (p < .001) for TF-CBT sessions.
Child outcomes (Aim 1)
Table 2 provides the estimated means and standard deviations for the child continuous outcomes by condition. The analyses on UCLA PTSD Index revealed statistically significant declines across the follow-up period (estimated [Est.] = −0.88, SE = 0.15, p < .001) but no main effects of treatment group (Est. = −2.53, SE = 4.59, p = .587) or a Group × Time interaction (Est. = 0.03, SE = 0.24, p = .888). At the final time point, the groups were not statistically different from one another, t(20) = −0.29, p = .777; d = .13. For CSR PTSD, there were statistically significant declines across the follow-up period (Est. = −0.16, SE = 0.02, p < .001) but no main effects of treatment group (Est. = −0.18, SE = 0.45, p = .697) or a Group × Time interaction (Est. = 0.002, SE = 0.03, p = .942). At the final time point, the groups were not statistically different from one another, t(19) = 0.13, p = .900; d = .06. Considering CGI-Severity ratings, statistically significant declines across the follow-up period were observed (Est. = −0.13, SE = 0.01, p < .001) but no main effects of treatment group (Est. = −0.44, SE = 0.38, p = .259) or a Group × Time interaction (Est. = 0.01, SE = 0.02, p = .576). At the final time point, the groups were not statistically different from one another, t(18) = 0.13, p = .897; d = .06. For the CGI-Improvement scores, we analyzed changes from the postassessment to follow-up. The mixed model results indicated no statistically significant effect of time (Est. = 0.004, SE = 0.01, p = .755), group (Est. = 0.22, SE = 0.45, p = .621), or the Group × Time interaction (Est. = −0.02, SE = 0.02, p = .224). At the final time point, the groups were not statistically different from one another, t(18) = −1.14, p = .268; d = .54.
Estimated Means and SD for Continuous Outcomes by Condition.

Note. N = 33; stepped care TF-CBT n = 22; standard TF-CBT n = 11. The means (M) and standard deviation (SD) are for the intent-to-treat analysis (N = 33). PTSD = post-traumatic stress disorder; PTSD-index = UCLA PTSD Index for DSM-IV; CSR-PTSD = clinical severity rating for PTSD on the Anxiety Disorders Interview Schedule; CGI-Severity = clinical Global Impression–Severity; internalizing and externalizing = CBCL T scores for internalizing and externalizing symptoms; CGI-Improvement = clinical Global Impression–Improvement; TF-CBT = trauma-focused cognitive behavioral therapy.
For internalizing symptoms, the mixed model analyses revealed significant declines over the follow-up period (Est. = −0.52, SE = 0.11, p < .001) but no main effects of treatment group (Est. = 5.44, SE = 3.38, p = .123) or a Group × Time interaction (Est. = 0.03, SE = 0.17, p = .862). At the final time point, the groups were not statistically different from one another, t(21) = 1.22, p = .237; d = .53. Similar results were observed for externalizing symptoms. The mixed model analyses revealed significant declines over the follow-up period (Est. = −0.28, SE = 0.08, p = .002) but no main effects of treatment group (Est. = −1.81, SE = 4.16, p = .668) or a Group × Time interaction (Est. = 0.004, SE = 0.13, p = .974). At the final time point, the groups were not statistically different from one another, t(21) = −0.40, p = .693; d = .17.
Clinical significance
For the child PTSD diagnosis, the GEE model analyses revealed significant declines over the follow-up period (Est. = −0.23, SE = 0.06, p < .001) but no main effects of treatment group (Est. = −0.16, SE = 0.87, p = .852) or a Group × Time interaction (Est. = 0.06, SE = 0.11, p = .587). There were no significant differences at posttreatment between SC-TF-CBT (86.4% baseline to 9.1%) and TF-CBT, 90.9% baseline to 9.1%; χ2(1) = .02, p = 1.00; LOCF: SC-TF-CBT = 32% versus TF-CBT = 27%, χ2(1) = .07, p = .56, and the differences at follow-up were not statistically significant, SC-TF-CBT = 0% versus TF-CBT = 9.1%, χ2(1) = 1.58, p = .40; LOCF: SC-TF-CBT = 27% versus TF-CBT = 27%, χ2(1) = .00, p = .66.
For the child depression diagnosis, the GEE model analyses revealed significant declines over the follow-up period (Est. = −0.10, SE = 0.03, p = .003) but no main effects of treatment group (Est. = −0.68, SE = 0.70, p = .337) or a Group × Time interaction (Est. = 0.03, SE = 0.06, p = .685). There were no significant differences at posttreatment between SC-TF-CBT (59.1% baseline to 13.6%) and TF-CBT, 45.5% baseline to 9.1%; χ2(1) = .32, p = 1.00; LOCF: SC-TF-CBT = 31% versus TF-CBT = 18%, χ2(1) = .69, p = .41, and the differences at follow-up were not statistically significant, SC-TF-CBT = 4.5% versus TF-CBT = 9.1%, χ2(1) = .06, p = 1.00; LOCF: SC-TF-CBT = 27% versus TF-CBT = 18%, χ2(1) = .33, p = .57.
Parent acceptability (Aim 2)
At baseline, there were no significant group differences in ERF scores, t(31) = −.78, p = .440, or the parent’s expectations of improvement ratings, t(31) = .44, p = .664. For the CSQ scores at posttreatment, no significant differences, F(1, 22) = .07, p = .768, were observed between SC-TF-CBT (n = 15, M = 30.80, SD = 3.32) and TF-CBT (n = 9, M = 30.44, SD = 2.65) groups.
Cost outcomes (Aim 3)
Costs were 62.4% lower (p < .0001) for children in SC-TF-CBT (n = 22, M = US$870.74, SD = 445.30) compared to those in TF-CBT (n = 11, M = US$2,312.69, SD = 741.89). Direct and indirect costs to parents/patients and providers were significantly lower for children in SC-TF-CBT. Patient/parent indirect costs were lower for SC-TF-CBT due to the overall lower time requirements, particularly for office visits. Effect sizes were 1.61 for total costs (confidence interval [CI] = [0.65, 2.59]), 1.71 for payer direct costs (CI [0.69, 2.73]), 1.40 for patient indirect costs (CI [0.48, 2.34]), and 0.95 for provider indirect costs (CI [0.19, 1.72]; see Table 3).
Differential Costs per Patient Between Stepped Care TF-CBT and Standard TF-CBT.
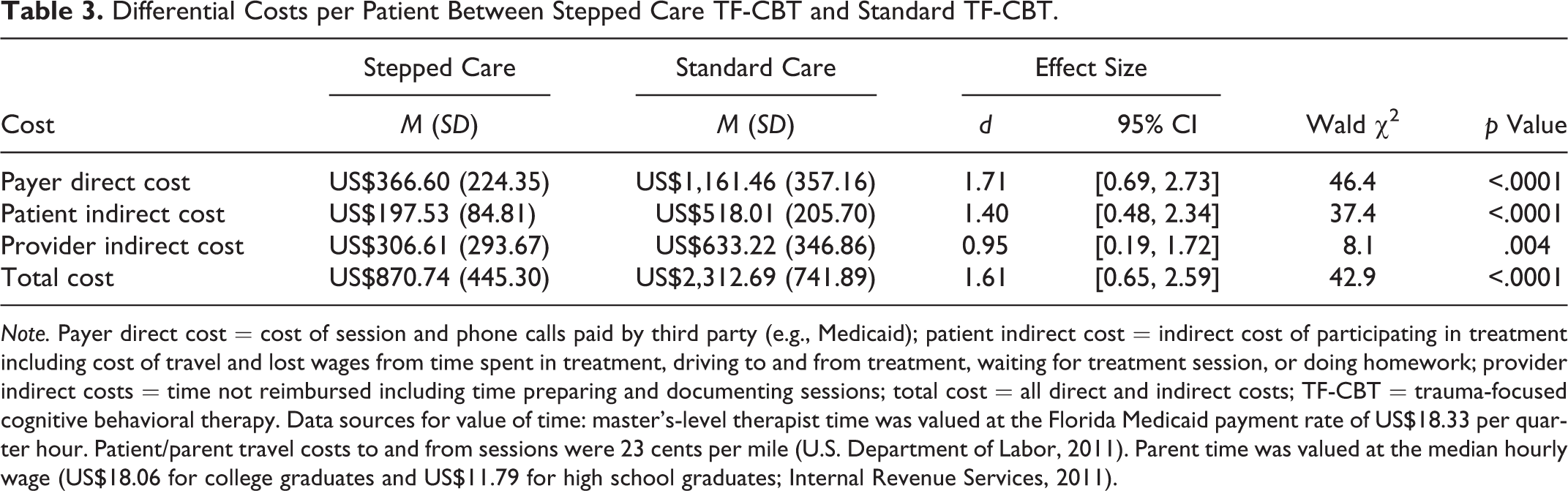
Note. Payer direct cost = cost of session and phone calls paid by third party (e.g., Medicaid); patient indirect cost = indirect cost of participating in treatment including cost of travel and lost wages from time spent in treatment, driving to and from treatment, waiting for treatment session, or doing homework; provider indirect costs = time not reimbursed including time preparing and documenting sessions; total cost = all direct and indirect costs; TF-CBT = trauma-focused cognitive behavioral therapy. Data sources for value of time: master’s-level therapist time was valued at the Florida Medicaid payment rate of US$18.33 per quarter hour. Patient/parent travel costs to and from sessions were 23 cents per mile (U.S. Department of Labor, 2011). Parent time was valued at the median hourly wage (US$18.06 for college graduates and US$11.79 for high school graduates; Internal Revenue Services, 2011).
Early responder status for Step 1 (Secondary Aims 1–3)
Of the Step 1 completers, 14 responded (82%; 64% = ITT) and 3 children did not respond (see Figure 1). Of the 14 responders, the early response status was maintained at post- and follow-up assessment, with 85.7% (12 children) having CGI-Improvement ratings 1 or 2. Neither of the two children who had the more modest rating of a 3 (Improved) met the criteria for PTSD at follow-up. Of the responders, 10 parents (71.4%) felt like they could comfortably stop treatment. The other four responders ended treatment based on their responder status, proceeded to the maintenance phase, and maintained improvement at follow-up. Of the nonresponders, one parent reported that she could comfortably stop and chose not to continue, and two parents indicated more treatment was needed, but only one of these two continued with Step 2.
Discussion and Applications to Social Work
In the current study, improvements in all child outcomes changed at similar rates over time for children in SC-TF-CBT and TF-CBT as hypothesized. This finding that SC-TF-CBT may be comparable to TF-CBT is encouraging for developing a stepped care model that could be more accessible, efficient, and cost-effective than the current standard treatment without a decrease in efficacy. If future research on SC-TF-CBT supports this finding, SC-TF-CBT could be offered as an alternative delivery system to address treatment barriers. Providing an evidence-based treatment in steps also provides a more tailored approach such that children only receive the necessary treatment dosage rather than all children receiving the full-package standard care treatment. Due to the pilot nature of this study, the age of the caregiver was not controlled for in the outcome analysis. While parental depression diagnosis and race were not statistically different, more parents/guardians in SC-TF-CBT met criteria for major depression (36% vs. 0%) and were African American (32% vs. 0%) than standard TF-CBT. Maternal depression may be a moderator of child trauma treatment outcomes (Weems & Scheeringa, 2013), and African American youth have higher dropout rates in trauma-focused treatments than other groups (Fraynt et al., 2014). Future studies will need to examine differing outcomes for different groups and characteristics, including type of trauma. Also, it is of note that the comparison is mainly of Step 1 of SC-TF-CBT compared to TF-CBT. It is possible that with larger samples and fewer early responders of Step 1, results may differ. Theoretically, the outcome of those receiving Step 2, which contains the components of TF-CBT, should be comparable to the standard TF-CBT, although it is possible that the nonearly responders have specific characteristics that result in less favorable outcomes for Step 2.
In terms of parent acceptability of SC-TF-CBT, there were no differences in parents’ expectations of treatment credibility and efficacy or in satisfaction levels. However, the satisfaction levels of noncompleters were not included. Also, 9 (6%) parents reported concerns about being hesitant and uncomfortable with the parent and child talking to each other and declined to participate. For families where abuse was perpetrated by another member or where they have not talked about what happened, the idea of the parent leading the treatment may be of concern for both the parent and the child. These dyads may not be appropriate for Step 1 or additional treatment readiness time may be needed with the therapists prior to starting parent-led meetings. Of the participants who were excluded during the prescreening process, 14 (12.17%) did not want to participate in research but rather wanted regular agency services. The reason for declining to participate was unknown for an additional 10 parents (10.43%). Reasons for declining to participate could be due to parents not wanting to participate in the lengthy assessments that are not part of typical of community care, parents not wanting to be randomized to treatments, parents being in a state of crisis when calling for trauma treatment for his or her child and wanting regular services, prescreeners not fully explaining the study or the parents fully understanding the study, or possibly that some of these parents did not want to lead the treatment. A recent state-wide community-based study on standard TF-CBT suggests that a total of 29.87% (72 or 241) participated in an open trial of TF-CBT (Webb, Hayes, Grasso, Laurenceau, & Deblinger, 2014), compared to 21.15% (33 of the 156) who participated in the current randomized trial. Given the exclusion criteria of research studies, many of the children who are typically seen in community-based treatment are excluded. It will be important for future community-based studies on SC-TF-CBT to explore parents’ and children’s reason for declining to participate.
Consistent with the need for low-cost first-line treatments within stepped care models (Bower & Gilbody, 2005), there was a significant difference in cost between SC-TF-CBT and TF-CBT. SC-TF-CBT cost 62.4% less than TF-CBT, and there were large effect sizes for direct and indirect costs. In this study, health-care-related costs such as hospitalizations or pediatric visits, costs over time, including usage beyond the follow-up were not collected, and such costs may have altered the results. Further, the cost savings analysis of the stepped care trauma-focused model to standard TF-CBT will need to be conducted once the model can be refined such that the nonresponders of Step 1 are matched to the appropriate treatment at baseline or receive enough treatment after Step 1 to respond, as spending less on treatment yet remaining impaired is not a cost savings, given the long-term effects of PTSD symptoms on health and functioning.
Findings suggest that Step 1 may be a feasible first-line service delivery method as the treatment response rate was 64–82% and gains were maintained over time. However, the feasibility of nonresponders stepping up will need further exploration as only one of the three children stepped up to the more intensive treatment with the one child not responding. Larger samples are needed to establish estimates of early responders to Step 1, but this pilot trial lends support to the efficacy of Step 1 for a substantial number of children. Having all children receive Step 1 first may not be the most efficient or clinically appropriate method for those children who will not respond to Step 1 or who drop out of Step 1. It will be important to explore if there are factors at baseline that could be used to match children to the most effective treatment (e.g., Step 1 or TF-CBT), and then once treatment begins, if there are variables that could be used to effectively tailor treatment intensity and dosage to the child’s needs.
The promising results suggest several implications for future research on SC-TF-CBT. Studies on SC-TF-CBT with larger sample sizes are needed to test treatment moderators and characteristics of early responders/nonresponders of Step 1. Future trials will need to include impairment for inclusion and randomized block designs to ensure that treatment conditions are balanced in regard to severity, impairment, and comorbidity. While no therapist-dose response was assumed when comparing Step 1 to standard TF-CBT, it would be important for future research to examine the moderating role of therapist alliance. Therapist alliance has been shown to predict TF-CBT but not treatment as usual or nonspecific treatment (Ormhaug, Jensen, Wentzel-Larsen, & Shirk, 2014). Also possible active agents in Step 1 such as parents’ sense of efficacy in helping the child, or the strength of the parent–child relationship will need to be examined. The trajectories of the three nonresponders raise important questions about the feasibility of Step 2. For example, was the one parent who did not think more treatment was needed satisfied with treatment gains or did she or her child not want to participate in further treatment? For the nonresponder of Step 2, it is not clear whether an initial higher dosage of TF-CBT would have led to response, and/or the child needed adjunctive therapy. If SC-TF-CBT is established as an evidence-based treatment and is acceptable to parents and therapists, future trials will need to be conducted by IEs where the developers are not providing the supervision. Step 1 clinicians have to be trained in TF-CBT as they are the same therapists who will provide Step 2, which contains the components of TF-CBT. Therefore, whether there are separate therapists for SC-TF-CBT or standard TF-CBT, those providing Step 1 will be providing both treatments. Thus, even if study therapists are assigned different treatments, close monitoring of fidelity to Steps 1 and 2 in SC-TF-CBT is needed. Lastly, we do not know why the parent who reported that more treatment was needed did not participate in Step 2, although insights into these questions will be important for refining the model.
There were several study limitations. First, the small sample size limits the generalizability of the findings and did not allow exploration of treatment moderators, or predictors of Step 1 response/nonresponse. Moreover, we were limited in our ability to establish that randomization was successful and control for slight differences between groups. Second, follow-up assessments were only at 3 months posttreatment. Longer follow-up assessments comparing the equivalence of SC-TF-CBT to TF-CBT are needed. Third, the child’s perception of treatment credibility and improvement expectations or comfort level ending after Step 1 was not gathered. Fourth, a control group was not included in the current research design to compare any positive developments over time that may occur naturally. However, prior studies have shown CBT for children after trauma to be superior to wait-list conditions (King et al., 2000; Scheeringa et al., 2011). Fifth, the first author was involved in reviewing the fidelity to the interventions. Future studies should include an independent rating of fidelity and random review of core components of the intervention such that all components are reviewed. While 39.17% of the audiotapes of sessions were reviewed, the random procedures utilized in this trial did not ensure that all components of the intervention were reviewed. Lastly, cost data did not include other mental health or health services used.
Despite these limitations, the results of this pilot study are encouraging and warrant future research on SC-TF-CBT. Having an alternative to the therapist-directed “full treatment” package model for all children would have significant implications for practice. First, many social workers are first-line providers to child victims of violence and trauma and having such a model that is accessible, efficient, and effective would potentially allow for more children in need to be provided care. Second, Bringewatt and Gershoff (2010) highlight barriers to access children’s mental health services and call for easily accessible services in “low-stigma” settings. It may be that a parent-led therapist-assisted first-line approach that empowers the parent to help the child at home offers one approach to improving access and lowering stigma of mental health treatment. Third, the role of the therapist in Step 1 is more of a coach and supporter than of the traditional primary provider of the treatment. Step 1 is in line with a strengths-based approach as the parent-led therapist-assisted treatment recognizes the strengths of the parent as a critical partner in the healing process, and values the parent–child relationship. New service delivery approaches are needed that make evidence-based treatment for children after trauma more accessible, and SC-TF-CBT may be an approach to improve care for all children in need, especially for those who may not otherwise receive services.
Footnotes
Acknowledgments
The authors would like to thank Melissa Thompson, MSW, Fabrienne McDowell, LMHC, Karen J. Allen, LMHC, Angela Claudio Torres, LMHC, Awneet Chandhok, LMHC, Debbie Lyublanovits, LMHC, Vicki Hummer, LCSW, Kelsy Pierson, MSW, Tia Burr, Kyra Synder, David Broughton, Sunny Hall, and Tom Marko at the Crisis Center of Tampa Bay where the study treatment occurred; Victoria Swaidan, BA, and Katherine Dillon, BA, research assistants at the University of South Florida; David Tolin, PhD, at The Institute of Living, Yale University School of Medicine for his contributions on the development of SC-TF-CBT and Mary Lee’s House, The Center for Child Protection and Advocacy in Tampa, FL.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Alison Salloum, PhD, was awarded a contract from the Crisis Center of Tampa Bay to conduct this study, and Dr. John Robst worked under this contract. Dr. Salloum also has grant support from the National Institute of Mental Health. Dr. Michael S. Scheeringa receives grant support from the Administration for Children and Families. Dr. Judith A. Cohen receives grant support from Substance Abuse and Mental Health Services Administration, National Institute of Mental Health and receives book royalties from Guilford Press. Dr. Eric A. Storch receives grant support from the International OCD Foundation, National Institute of Health and the Agency for Health Care Research and Quality. Dr. Storch also receives support from the Fulbright Scholar Program.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Crisis Center of Tampa Bay.