
Abstract
Purpose:
The purpose of this study was to examine the effectiveness of a trauma-informed approach that was adapted for psychiatric residential treatment (PRT) for children aged 5–17.
Methods:
Data were extracted from case files of 100 youths who received traditional PRT and 105 youths who received trauma-informed PRT (TI-PRT). Outcome measures included change in functional impairment, physical restraints and locked seclusion room incidents, length of time in care, and discharge placement type.
Results:
Results of a repeated measures analysis of variance demonstrated that youth who received TI-PRT experienced greater improvements in functional impairment. Results of a zero-inflated Poisson showed that youth in TI-PRT had fewer seclusion room incidents. Finally, the average length of time in care was significantly shorter for the TI-PRT group.
Discussion:
The results support trauma-informed PRT as a promising approach for helping youth achieve greater stability in functioning and for addressing issues of long-standing concern in residential care settings.
An estimated 15% of children and adolescents in out-of-home care are placed in some form of residential treatment (U.S. Department of Health and Human Services, 2014). Youth served in residential treatment often have extensive trauma histories including exposure to family and community violence (den Dunnen et al., 2012; James, 2011). Using clinical data collected from 56 sites throughout the United States, Briggs et al. (2012) found that 92% of youth in residential treatment compared to 77% of youth receiving community-based services met criteria for complex trauma resulting from exposure to multiple traumatic events. Youths receiving residential services also exhibited higher mean levels of functional impairment compared to those receiving community-based services. These findings suggest that the population of children and adolescents in residential treatment are highly likely to suffer from trauma-related impairments.
Child welfare researchers and service providers are increasingly recognizing trauma that stems from systemic involvement (Conradi & Wilson, 2010; LeBel, Huckshorn, & Caldwell, 2010). Systemic trauma can result from emotional and psychological stress experienced as a consequence of being removed from the home, enduring multiple placement changes, and instability of relationships or, in some instances, practices that are implemented in treatment settings (LeBel et al., 2010). Due to the combination of high rates of complex trauma coupled with a heightened risk for retraumatization that characterizes youth in residential treatment, trauma-focused interventions are increasingly being considered as a critical component to effective treatment (A. D. Brown, McCauley, Navalta, & Saxe, 2013). Yet, the evidence base for trauma-informed approaches in residential settings remains underdeveloped. The purpose of the current study was to examine the effectiveness a trauma-informed approach that was implemented in psychiatric residential treatment (PRT) facilities serving trauma-affected children and adolescents.
Review of Relevant Literature
Trauma treatment refers to clinical interventions that are designed to address specific types of trauma, whereas trauma-informed approaches encompass delivering services and creating a culture within the service setting that is designed to help clients recover from the effects of prior trauma and to minimize risks for clients to be retraumatized (Bloom & Sreedhar, 2008; Ko et al., 2008). Trauma-informed approaches typically include the use of trauma-focused assessments and clinical treatments.
In addition to helping treat trauma-related impairments in youth, trauma-informed approaches are thought to hold promise for addressing issues of long-standing concern among child welfare service providers. The use of behavior management methods of locked seclusion room placements and physical restraints are recognized as concerning practices with potential to retraumatize previously maltreated youth (Huckshorn, 2004), which has resulted in initiatives to reduce their use in child serving settings (Hodas, 2006; LeBel et al., 2010). In residential facilities, often reserved for treatment of youths with challenging behavioral and mental health needs, seclusion/restraints are utilized as a means to maintain the safety of the youth and others in the treatment setting. Results from two national surveys showed that 76% of 224 responding residential facilities reported having used seclusion/restraints in the past year (J. D. Brown et al., 2012). Trauma-informed approaches that recognize the impact of trauma on youth’s behavioral and emotional responses and that emphasize creating a supportive therapeutic environment which discourages the use of coercive practices are thought to potentially minimize the use of physical behavior management methods (Azeem, Aujla, Rammerth, Binsfeld, & Jones, 2011; Fallot & Harris, 2002).
Residential treatment has long been considered a placement of last resort to be used only after less restrictive community-based interventions have failed and, when placement occurs, efforts should be made to keep the length of stay to a minimum (Pecora et al., 2010). Trauma-informed approaches may also hold promise for helping youth achieve positive outcomes within a shorter time frame (Greenwald et al., 2012). Shorter treatment duration may result from more effective treatment of existing issues and/or the use of approaches that minimize the occurrence of negative experiences in the treatment setting that have potential to exacerbate existing problems. Research on the effects of trauma treatments and approaches in residential care settings provide some evidence supporting their promise in reducing trauma-related impairments (Greenwald et al., 2012; Hodgdon, Kinniburgh, Gabowitz, Blaustein, & Spinazzola, 2013; Raider, Steele, Delillo-Storey, Jacobs, & Kuban, 2008; Soberman, Greenwald, & Rule, 2002), the use of physical restraints (A. D. Brown et al., 2013; Hodgdon et al., 2013), and the duration of treatment and increasing rates of discharge to lower level care (Greenwald et al., 2012).
Trauma-Focused Treatments
Children and adolescents receiving residential services may have access to evidence-supported trauma-focused therapies as a component of treatment. For example, eye movement desensitization and reprocessing (EMDR; Shapiro, 2005) and trauma-focused cognitive–behavioral therapy (TF-CBT; Cohen, Mannarino, & Deblinger, 2006) are both considered appropriate for delivery in residential settings. Each has demonstrated efficacy in treating posttraumatic stress symptoms and internalizing and externalizing behavior problems in children and adolescents (Cary & McMillen, 2012; Rodenburg, Benjamin, Roos, Meijer, & Jan Stams, 2009; Seidler & Wagner, 2006). However, few studies of trauma-focused treatments have specifically examined outcomes using samples of youth in residential settings. In a small controlled trial (n = 29) with adolescent boys in residential or day treatment programs for conduct problems, Soberman, Greenwald, and Rule (2002) found that boys receiving EMDR experienced significantly greater reductions in memory-related distress and posttraumatic stress compared with boys in the control group. Using a sample of 20 adolescents, Raider, Steele, Delillo-Storey, Jacobs, and Kuban (2008) found that those who were randomly assigned to receive Structured Sensory Intervention for Traumatized Children, Adolescents, and Parents, a trauma-focused group therapy, demonstrated significantly greater reductions in trauma symptoms, depression, aggression, and defiance compared with those assigned to a waitlist.
Hodgdon et al. (2013) noted that treating trauma-affected youths in residential care requires an overarching approach that goes beyond hourly treatment sessions. Just as a child receiving weekly trauma therapy would be less likely to benefit if outside of the sessions he or she was consistently exposed to a hostile and unsafe family environment, for children in residential care, the treatment environment, which serves as their living space, is critical to effective treatment. Creating a trauma-informed environment provides youth with the safety and support needed to facilitate the recovery process (Ambramovitz & Bloom, 2003). In recent years, trauma-informed approaches have begun to be adapted for residential settings.
Trauma-Informed Approaches for Residential Treatment Settings
Attachment Regulation and Competency (ARC; Blaustein & Kinniburgh, 2010), the Fairy Tale Model (Greenwald, 2009), the Sanctuary Model (Ambramovitz & Bloom, 2003; Bloom, 1997; Bloom & Sreedhar, 2008), and Trauma Systems Therapy (TST; Saxe, Ellis, & Kaplow, 2007) each represent trauma-informed approaches that have been adapted for use in residential care and that have published preliminary findings from outcomes evaluations. Although the models differ in the precise implementation methods and service elements, each includes both clinical and organizational components designed to simultaneously provide individualized and/or group-based treatment while creating trauma-informed environments in both the treatment and caregiver systems. Each model is grounded in common principles that emphasize understanding how trauma affects children’s development and the importance of establishing a therapeutic treatment environment that fosters a sense of emotional and physical safety.
Outcomes research on these approaches, while producing some promising results, remains in the early phases. Results from one group pre- and posttest evaluations of TST (A. D. Brown et al., 2013), ARC (Hodgdon et al., 2013), and the Fairy Tale Model (Greenwald et al., 2012) have each demonstrated evidence of significant reductions in various forms of impairment. Findings from one study using a nonrandomized comparison group design showed that after 6 months adolescents treated in units that were using the Sanctuary Model had significantly better scores on measures of coping strategies and internal locus of control and reduced verbal aggression compared to adolescents in the comparison units (Rivard, Bloom, McCorkle, & Abramowitz, 2005). Results from three out of four of the previously mentioned evaluations also showed significant reductions in physical restraints among adolescents (A. D. Brown et al., 2013; Greenwald et al., 2012; Hodgdon et al., 2013) and children (A. D. Brown et al., 2013). Greenwald et al. (2012) further found significant declines in lengths of stay and increases in discharges to lower level care settings over a 1-year period among adolescents in facilities that were using an approach that integrated the Fairy Tale and Positive Peer Culture models (Vorrath & Brendtro, 1985).
The Current Study
Despite the emergence of models with some promising preliminary findings, there remains no thoroughly established or standard approach to providing trauma-informed residential treatment (Greenwald et al., 2012). Among the known challenges to effectively integrating evidence-based models in community-based agencies are limited accessibility of training and implementation resources, high costs, and a lack of model fit within the service setting. In response, some agencies are drawing upon available evidence to adapt their own approaches to fit the specific needs and circumstances of their service settings.
The currently described study was an independently conducted evaluation of outcomes in the psychiatric residential facilities of a large Midwestern Behavioral Health Agency that began implementing trauma-informed programming in 2012. The model was adapted in consultation with national trauma experts and a network that provides education, consultation, and training in trauma-informed services. Similar to the previously described models, the approach is grounded in trauma knowledge and trauma-informed principles of care and includes both clinical and organizational components.
Intervention Description: Trauma-Informed PRT (TI-PRT)
Prior to the agency integrating trauma-informed programming, the PRT facilities provided 24 hr supervision and services to meet youths’ daily needs. Youths either attended public school or an on-campus school depending upon their educational and behavioral needs. The program provided ongoing clinical services including individual therapy and family therapy when feasible. In addition to stabilizing psychiatric symptoms, services focused on improving self-concept and teaching effective social and problem-solving skills. The agency also used a family-centered approach that focused on the inclusion of families in decision making and treatment planning. The TI-PRT model included all of the same service components as the traditional PRT along with several trauma-focused enhancements described below. Table 1 provides a comparison of the traditional PRT and TI-PRT model components.
Comparison of Traditional Psychiatric Residential Treatment (PRT) and Trauma-Informed Psychiatric Residential Treatment (TI-PRT).
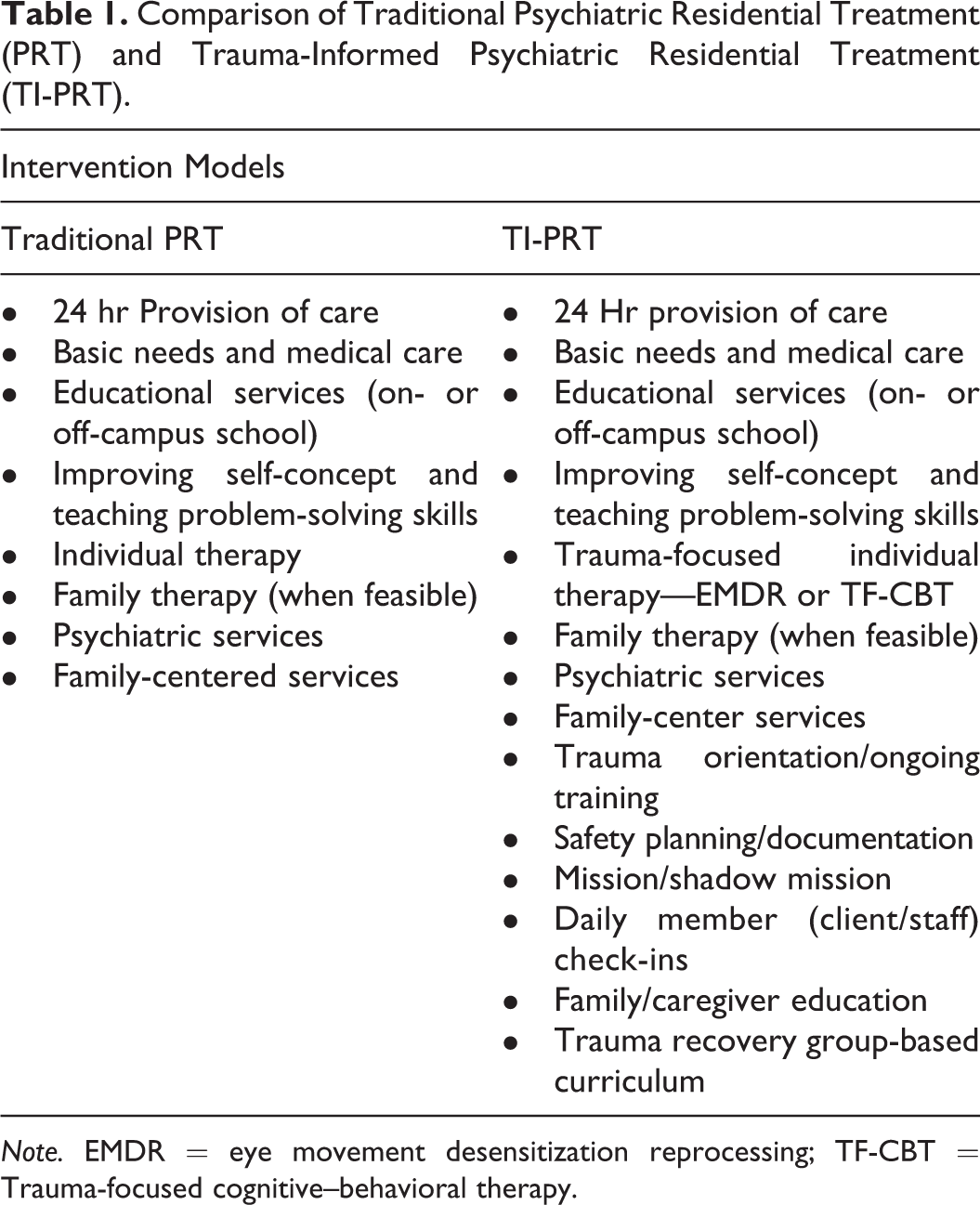
Note. EMDR = eye movement desensitization reprocessing; TF-CBT = Trauma-focused cognitive–behavioral therapy.
TI-PRT organizational components
All TI-PRT staff receive orientation, ongoing training, and supervision in understanding trauma and in working effectively with trauma-affected youth. Central to the approach is the creation of a supportive, therapeutic environment within the treatment setting where the program staff and youth are all viewed as members of a shared community. A key element of creating a trauma-informed culture and setting the stage for recovery involves working to achieve a sense of safety and self-awareness. All members, including the staff and youth, engage in safety planning in which they identify stressors, physiological cues triggered by stress, and strategies to proactively respond in stressful situations. Each member documents his or her safety plan and keeps it with them at all times. Additionally, members identify a mission (i.e., goals and objectives that they hope to accomplish) and a shadow mission (underlying thoughts and behaviors that undermine their achieving the mission). Member check-ins occur daily among youth and staff to discuss any issues or red flags that may be triggering psychological or physiological stress.
TI-PRT clinical components
Youth receive individual trauma-focused therapy including EMDR or TF-CBT and participate in a trauma recovery group-based curriculum 2 times per week. The trauma recovery curriculum is a multimodal, multilayered program based on a combination of trauma treatments (for more information see http://midwesttrauma.org/programs.html). The curriculum initially focuses on helping youth achieve a sense of psychological and physical safety and trust through psychoeducation and supplementary exercises. The next phases focus on helping youth recognize the impacts of trauma, teaching effective coping strategies, and establishing a sense of hopefulness and goals for the future. The groups are led by staff who are trained in the curriculum and are comprised of approximately 8–10 youth matched by age. Program staff and therapists also work with caregivers to provide trauma education and teach skills to help them support their child’s treatment.
Within the treatment environment and as part of the individual treatment and trauma recovery groups, the youth are consistently exposed to prosocial and adaptive processes versus power and control. Although all youth are encouraged to participate in member activities, as a critical aspect of creating a culture of safety and support, participation is optional and members may opt out without threat of consequences.
Model Training and Implementation Monitoring
Fidelity to the TI-PRT model was assessed using a training and implementation checklist created for the project. The checklist was completed by a program administrator in charge of supervising the integration of trauma-informed programming throughout the agency. At the start of data collection, approximately 85% of unit staff had received the initial training in understanding trauma and trauma-informed care. It was noted that turnover created challenges to getting 100% of staff trained, but that training was being provided as part of the new hire orientation. All staff received ongoing supervision through weekly team meetings, individual supervision, clinical team meetings, and leadership meetings. One hundred percent of youth and approximately 94% of the PRT staff had documented safety plans. Daily member check-ins were reported to be occurring as planned approximately 95% of the time. Trauma recovery groups were also reported to be occurring 2 times per week for 1 hr as planned. Overall, it appeared that the agency had successfully trained the majority of the staff and had achieved a high level of model integration.
Purpose and Study Hypotheses
The purpose of this study was to examine the effects of a TI-PRT model compared with a traditional PRT model that was previously used within an agency. The following four hypotheses were tested:
Method
Sample Characteristics
The agency serving as the study site provides a wide range of programs and services aimed at helping families and children achieve improved functioning, well-being, and permanency. The PRT programs are reserved for treatment of children and adolescents with severe behavioral and emotional problems. Data for this study were extracted from the case records of 205 children and adolescents who received either traditional PRT (n = 100) or TI-PRT (n = 105) services. All youths treated and discharged within the study time frame with complete service records were considered for inclusion. Records that contained missing data on key study variables were excluded.
The majority of the sample (86.3%) had experienced at least one prior out-of-home placement. Ages ranged from 5 to 17 years (M = 10.53, SD = 2.68) and 58% of the sample was male. The majority of the sample was White (69.3%) followed by multiracial (13.7%) and Black (11.2%). Sample characteristics for the TI-PRT and traditional PRT are summarized in Table 2 along with results of bivariate analyses of group differences. The TI-PRT group was slightly older than those in the comparison group. No statistically significant differences were found between groups on other sample characteristics.
Sample Demographics and Trauma History.

Note. PRT = psychiatric residential treatment; TI-PRT = trauma-informed psychiatric residential treatment; CAFAS = Child and Adolescent Functional Assessment Scale.
Study Design and Procedures
All study procedures were approved by a Midwestern university institutional review board. A quasi-experimental design was used to compare the effects of TI-PRT with traditional PRT. Data for the comparison group were extracted from the files of 100 youth who discharged from one of the PRT facilities prior to starting trauma-informed programming. In nine instances during the first round of data collection, a child had two or more separate records due to reentering PRT following a previous discharge from the facility. It was decided to retain the earliest service record for the child and to exclude records for any subsequent reentries. Following extracting data for nine additional cases, the final sample was comprised of records of 100 youth who had been discharged from one of the PRT facilities within a 13-month period prior to the agency initiating trauma-informed programming. Data collection for youth in the TI-PRT group began 12 months following implementation to allow for training and full integration of the model. Data collection occurred in three separate waves over a period of 9 months until a sample size necessary to achieve adequate statistical power was obtained. In total, 118 children and adolescents were treated in one of the TI-PRT facilities during the 9-month observation period. Five cases were excluded due to missing data and an additional eight were excluded due to having been previously treated in one of the traditional PRT facilities. The final TI-PRT sample was comprised of 105 youth with complete treatment records. Due to limited issues with missing data or treatment dropout and the use of naturalistic sampling methods, a participant flowchart depicting sampling procedures has not been included.
Measures
Child and Adolescent Functional Assessment Scale (CAFAS)
Functional impairment was assessed by master’s-level clinicians employed by the agency at the time of admission and again at discharge using the CAFAS (Hodges, Xue, & Wotring, 2004). The CAFAS assesses domains of impairment in daily functioning within different contexts (Hodges, 2003). The assessment includes eight subscales, School/Work, Home, and Community, Behavior Toward Others, Moods/Emotions, Self-Harmful Behavior, Substance Use, and Thinking. Subscale scores are summed to compute a total functional impairment score ranging from 0 to 240 with increasing values indicating higher levels of impairment. Prior tests of internal consistency of the CAFAS ranged from .63 to .78 (Breda, 1996; Hodges & Wong, 1996, 1997) and interrater reliability scores indicated an acceptable to a high level of agreement (intraclass correlation coefficient = .74 to .99; Hodges & Wong, 1996, 1997). For this study, differences in pre- and posttreatment scores were used to assess changes in functional impairment between groups. Internal consistency with the current study sample was high (α = .80).
Behavior management incidents
Unit staff who are involved in any behavioral management incidents including physical restraints and seclusion room placements are required to complete an incident report form for each occurrence. The number of physical restraints and seclusion room incidents was extracted from each child’s case record and two variables were created from the summed count of each type of incident.
Length of stay
Length of stay was computed by subtracting discharge dates from admission dates. Because the minimal length of stay was 5 weeks, this measure was converted into months.
Discharge placement
Discharge outcomes were coded as either community based or institutional. Community-based discharge placements included reunification with the biological family or moving to an adoptive or preadoptive home, foster home, or discharging to the home of a relative or legal guardian. Institutional placements included discharging to a group care facility, residential treatment, a hospital, a juvenile detention center, or a state training academy.
Covariates
Participant characteristics including age, race, gender, and trauma histories are recorded as part of the intake process. Due to low representation of certain racial/ethnic groups (see Table 2), race was collapsed into White and non-White categories for inferential analyses. Five dichotomously coded trauma measures included confirmed and suspected incidents of physical abuse, sexual abuse, emotional abuse, neglect, and exposure to domestic violence.
Data Analysis
A series of analyses using SPSS version 22 were performed to examine differences in treatment outcomes between groups. Repeated measures analysis of variance (RMANOVA) was used to examine differences between groups on average change in functional impairment from admission to discharge. The difference in average length of time in treatment was examined using multivariate regression and a logistic regression was used to determine whether there were differences in the probability of discharging to a community-based placement versus an institutional placement.
Using Mplus version 7, a zero-inflated Poisson (ZIP) regression was used to examine group differences in physical restraints and seclusion room incidents. ZIP is an appropriate method when count variables serve as the outcome and when the distribution of the outcome variable includes excessive zeros (Lambert, 1992). The number of physical restraints for the sample ranged from 0 to 130. About 37.1% of youth experienced no restraints and the measure of skewness was 4.16, indicative of a highly and positively skewed distribution. Seclusion incidents ranged from 0 to 128 with 64.9% of the sample having experienced no incidents (skewness = 3.72). For ZIP models, maximum likelihood is the default estimator using robust standard errors. Two regression models are estimated, a count model predicts the probability of experiencing the event (i.e., restraint or seclusion) and the other, a logit model, predicts the probability of not experiencing the event (i.e., restraint or seclusion).
Results
The results of the RMANOVA showed a statistically significant effect for Time, F(1, 200) = 31.035, p = .000, η2 = .133. There was a significant interaction for Time × Condition, F(1, 200) = 36.288, p = .000, η2 = .154, indicating a difference in the average change in functional impairment over time between TI-PRT and traditional PRT. The η2 value indicates an effect size in the moderate range, indicating that approximately 15% of the difference in effect was attributable to the treatment condition. Interactions for Time × Age, F(1, 200) = .739, p = .391; Time × Gender, F(1, 200) = .011, p = .916; and Time × Race, F(1, 200) = .190, p = .663, were not statistically significant.
ZIP: Restraints and Seclusion Incidents
The average number of restraints in TI-PRT facilities (M = 9.13, SD = 17.38; Median = 3) was higher compared with traditional PRT (M = 6.13, SD = 6.13; Median = 1). Conversely, the average number of seclusion room placements in traditional PRT (M = 10.90, SD = 25.96; Median = 0) was higher than TI-PRT (M = 4.19, SD = 9.82, Median = 0). It should be noted that the median is likely to be more representative of the frequency of occurrences across the population of youth in both PRT conditions. Table 3 provides a summary of results of the ZIP models for restraints and seclusion room placements. The upper right-hand side of the table shows that the count portion of the model revealed that with each additional year of age, the expected number of physical restraints increased by 15% (p = .002). The logit portion of the model revealed that as CAFAS scores increased, the odds of experiencing no restraints decreased slightly (odds ratio [OR] = .98, p = .007). Neither the count nor logit portion of the model showed differences in restraints between groups or revealed relations with any of the other covariates.
Zero-Inflated Poisson Predicting Restraint and Seclusion Room Incidents.
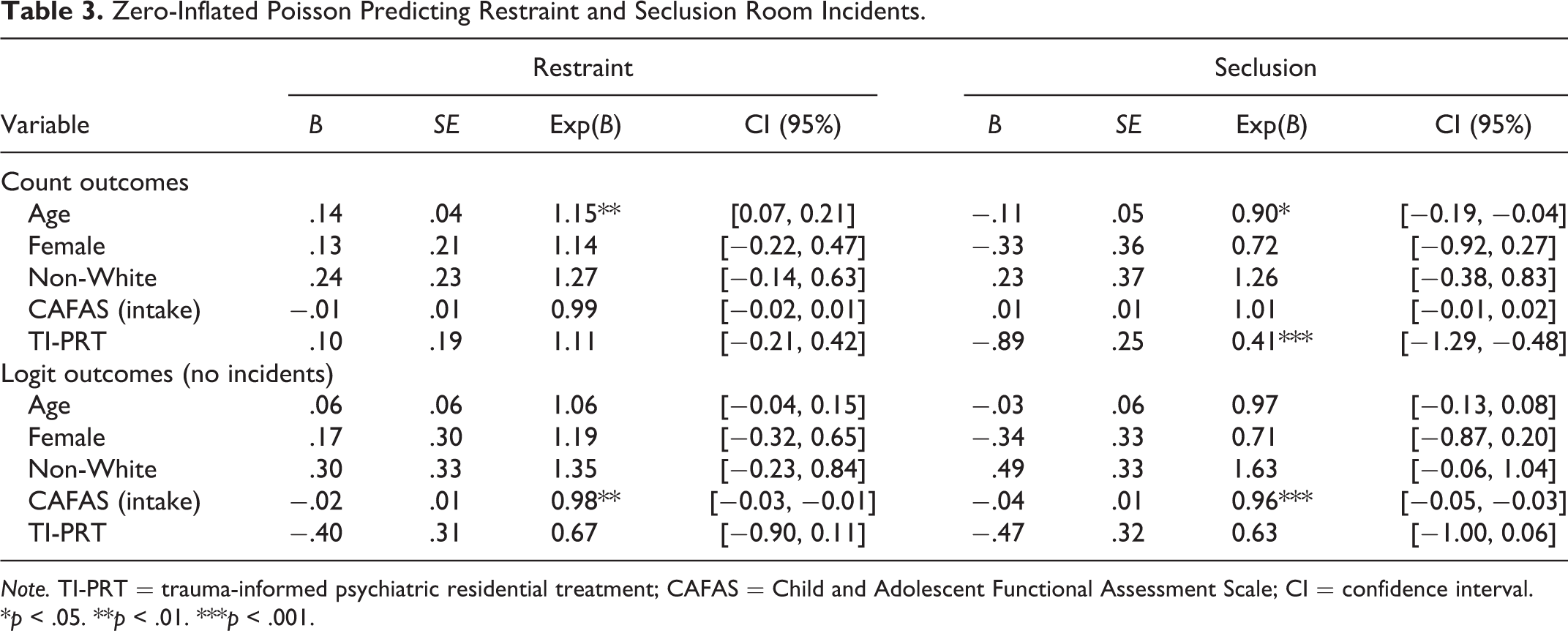
Note. TI-PRT = trauma-informed psychiatric residential treatment; CAFAS = Child and Adolescent Functional Assessment Scale; CI = confidence interval.
*p < .05. **p < .01. ***p < .001.
The count portion of the ZIP model, presented on the upper left-hand side of Table 3, revealed statistically significant associations between age and treatment condition and seclusion room incidents. For each additional year of age, the expected number of seclusion room incidents decreased (OR = .90, p = .014). The expected number of seclusion room incidents for youth in the TI-PRT condition was less compared with youth in the traditional PRT condition (OR = .41, p = .000). The logit portion of the model showed that as CAFAS scores increased, the probability of experiencing no seclusion room incidents decreased (OR = .96, p = .000). No other covariates were statistically significant.
Multivariate Regression: Length of Time in Treatment
Youth receiving TI-PRT spent fewer months in treatment (M = 6.45, SD = 3.07) compared with those in the traditional PRT (M = 10.78, SD = 4.71) on average. Table 4 presents results from a multivariate regression on length of time in treatment. The results show that, controlling for age, gender, race, and CAFAS scores at intake, there was a statistically significant association between treatment condition and length of stay, F(5, 204) = 13.07, p = .000, R 2 = .247. Receiving TI-PRT versus traditional PRT accounted for approximately 25% of the variance in length of stay between groups.
Multivariate Regression on Length of Stay in Treatment.
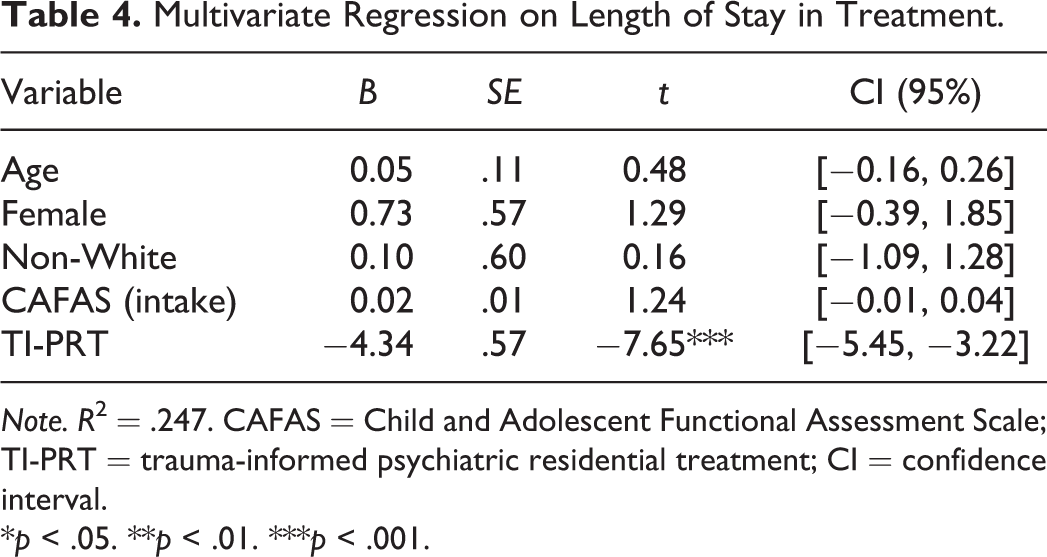
Note. R 2 = .247. CAFAS = Child and Adolescent Functional Assessment Scale; TI-PRT = trauma-informed psychiatric residential treatment; CI = confidence interval.
*p < .05. **p < .01. ***p < .001.
Logistic Regression: Discharge Placement
Approximately 93% of youth in TI-PRT discharged to community-based placements compared with 82% in the traditional PRT. The Hosmer and Lemeshow test, a frequently used test of goodness of fit for logistic regression models, yielded a p value that was higher than the established cutoff of .05, χ2(8) = 3.74, p = .880, indicating adequate model fit. Results from the logistic regression (presented in Table 5) showed a statistically significant association between CAFAS scores at discharge and discharge placement. Specifically, a one unit increase (10 points) in CAFAS scores was associated with a .97 decreased odds of discharging to a community-based placement controlling for age, race, gender, and treatment condition. Despite a higher percentage of TI-PRT youth discharging to community-based settings, statistically, treatment group was not associated with differences in discharge placement.
Logistic Regression on Discharge Placement Type (Community-Based Placement).
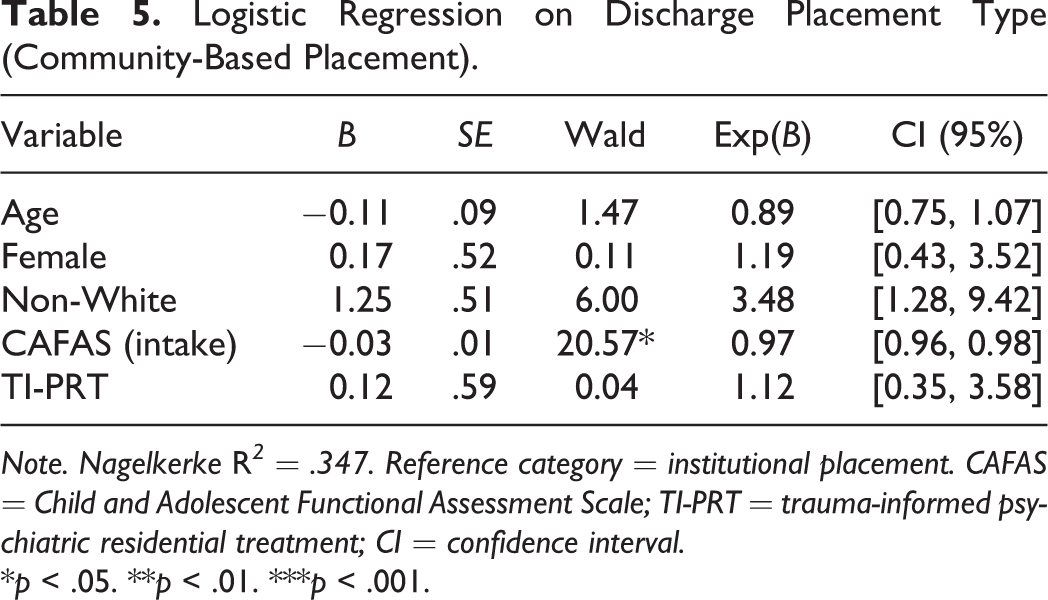
Note. Nagelkerke R 2 = .347. Reference category = institutional placement. CAFAS = Child and Adolescent Functional Assessment Scale; TI-PRT = trauma-informed psychiatric residential treatment; CI = confidence interval.
*p < .05. **p < .01. ***p < .001.
Discussion and Application to Practice
The purpose of this study was to examine the effectiveness of a trauma-informed model of PRT compared with a traditional approach. Specifically, it was expected that youth receiving TI-PRT would experience greater reductions in functional impairment, fewer physical restraints and seclusion room placements, and shorter lengths of stay and would be more likely to discharge to a community-based placement compared with those who received traditional PRT.
The hypothesis that TI-PRT would result in greater reductions in impairment was supported. These results are consistent with findings from previous investigations also supporting trauma-informed approaches as effective in reducing functional impairment in samples of youth in residential treatment (A. D. Brown et al., 2013; Greenwald et al., 2012; Hodgdon et al., 2013). The results from the current study showed that both groups were admitted with CAFAS scores indicating severe levels of functional impairment requiring intensive inpatient treatment (Hodges, 2003). CAFAS scores at the time of discharge indicated that, on average, youth in both groups experienced significant improvements in impairment over the course of treatment. Yet, the TI-PRT group experienced greater decreases in impairment, beyond what was observed in the traditional PRT. Based on suggested interpretations of the CAFAS (Hodges, 2003), scores that fall in the 50–90 range are indicative of impairment that may warrant services beyond outpatient. Substantively, youth discharging from traditional PRT, with average scores of 87.17 were at the higher end of this score range, whereas those discharging from TI-PRT, with average scores of 53.81, were near the lower end, closer to functional levels that are considered to be manageable with community-based care.
The second hypothesis that youth in TI-PRT would experience fewer restraints and seclusion room placements was partially supported. Unlike the findings from previous evaluations (A. D. Brown et al., 2013; Greenwald et al., 2012; Hodgdon et al., 2013), receiving TI-PRT did not appear to have an impact on incidents of physical restraints. This may be partially attributable to differences in samples or modeling methods across studies. In the current study, many youth in both groups were never restrained or placed in a seclusion room and most of those who were had few repeat incidents. The results would likely vary for a sample of youth for whom physical behavioral management methods were more frequently required or in programs where such approaches are more frequently utilized to manage behaviors.
Despite limited incidents, there were differences between groups in the use of seclusion room placements. The TI-PRT group experienced fewer incidents than those in the traditional PRT. This outcome, limited to seclusion room placements, suggests that trauma-informed care applied in PRT under similar conditions may hold promise for helping agencies support efforts to reduce the use of this form of behavior management. However, these results should be viewed as suggestive and warrant further investigation prior to drawing firm conclusions.
Consistent with the findings of Greenwald et al. (2012), the third hypothesis proposing that TI-PRT would be associated with fewer months in treatment was also supported. Time spent in treatment was around 4 months less for the TI-PRT group. The design of this study does not account for external factors that may have contributed to the shorter amount of time in treatment. Changes in policy corresponding with increased efforts to reduce the length of time children spend in out-of-home care that coincided with the study time frame are likely to have played a role in accounting for a portion of the difference in time between groups. An observation worthy of noting and warranting further exploration is the combined finding that youth in TI-PRT achieved greater improvements while spending less time in treatment. Effective treatment models that expedite the treatment process have potential to facilitate current child welfare initiatives to provide evidence-based services that reduce the amount of time children spend in out-of-home care, particularly in placements that are considered more restrictive.
The final hypothesis that youth in TI-PRT would be more likely to discharge to community-based placements versus institutional placements was not supported. Not surprisingly, CAFAS scores at the time of discharge were the strongest predictor of discharge placement. This finding is also likely to have been impacted by policy emphasizing placement in family- and community-based settings whenever possible. Another contributing factor related to the study sample was that nearly 75% of permanency goals were for family reunification in both groups. Future analyses of these data will consider differences in meeting permanency goals of reunification accounting for family involvement in treatment, family contacts, and other relevant treatment factors.
These findings should be considered in light of a number of limitations related to the study design. The use of a nonrandomized, quasi-experimental design does not control for the many factors that could influence the results. For example, there may be systematic differences between groups that impact response to treatment or influences that are external to the treatment setting such as policy decisions and changes in practices that overlapped with the study period. Given that the sample was drawn from psychiatric residential facilities within one agency in the Midwest, generalizability to other settings is limited. Further, the lack of representation of non-White youth limits the generalizability of treatment effects to other racial/ethnic groups.
The approach taken by the agency to implementing trauma-informed programming was a likely key factor contributing to positive outcomes. The agency not only integrated a trauma-informed approach in the PRT facilities but was actively integrating trauma-informed programming throughout the entire agency at the same time. As part of the process of converting to a trauma-informed organization, the agency hired and designated personnel to lead the process. All staff received initial and ongoing training, regular consultation, and supervision throughout the process. Having strong leadership and staff buy-in is a critical factor that promotes continuity in the implementation process, improved model fidelity, and ultimately, more successful results. Developing a clear-cut implementation strategy and monitoring process is essential to successfully integrating trauma-informed approaches. Follow-up analyses of these data will focus more closely on examining factors associated with implementation such as the consistency between staff’s attitudes and perceptions with trauma-informed principles and how these and other environmental factors impact youth outcomes.
The current study is among the first independent outcomes studies of an agency-adapted model of trauma-informed care in PRT that utilizes a comparison group design and that includes both children and adolescents in the sample. The results from this study build upon existing evidence supporting trauma-informed residential services as a promising approach for reducing functional impairment and that may result in helping youth achieve greater outcomes in a shorter amount of time than traditional approaches. Additionally, the findings suggest that trauma-informed approaches in PRT may help reduce the use of locked seclusion room placements, a behavioral management practice that has raised concerns in the past (Hodas, 2006; Huckshorn, 2004).
Nationally, child welfare providers are increasingly adopting principles of trauma-informed care and integrating trauma-informed approaches into practice. Given the growing momentum toward the use of trauma-informed care, the need for research that examines the impact of such approaches is needed, particularly in the area of residential treatment where there is a lack of research, yet research findings show that a high percentage of the youth served in residential programs are trauma affected (Briggs et al., 2012; Zelechoski et al., 2013). Finally, in addition to future research that utilizes well-controlled designs, subgroup analyses are needed to determine for which types of youth and trauma-related impairments are trauma-informed approaches more or less effective and in what residential contexts.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.