
Abstract
Purpose:
It is critical to assess hospice professionals’ discrimination between adaptive and maladaptive reactions to terminal illness in persons at the end-of-life to assure targeted intervention aimed at maintaining quality of life. The proposed measure, the Hospice Professionals Understanding of Preparatory Grief scale (HPPG), contains affective, behavioral, and cognitive reactions to terminal illness and asks respondents to identify which reflect adaptive and maladaptive responses.
Methods:
Hospice professionals across three states (n = 196) completed the novel HPPG via online survey.
Results:
Initial evidence via expert panel review, confirmatory factor analysis, and domain restructuring suggests good content and factorial validity. Final reliability (α stratified = .861) indicates good internal consistency.
Discussion:
The HPPG is the first measure to assess hospice professionals’ understanding of reactions to terminal illness and serves as an initial examination of this critical skill in hospice professionals including social workers. The HPPG can be used as a self-assessment or measure of continuing education.
Over one million deaths occurred under the care of hospice in the United States in 2012 (National Hospice and Palliative Care Organization [NHPCO], 2013a). The American health-care system will face a dramatic increase in the use of hospice and palliative end-of-life services as a result of longer life expectancies, technological advances, and aging baby boomers (Prost, 2014). In hospice and many other settings, patient assessments are used to guide care. However, the progressive nature of many end-of-life conditions and subsequent cognitive decline predicates the use of proxy-assessed ratings completed by persons other than the patient receiving care. Previous research indicates that the validity of proxy ratings is modest at best, including those completed by hospice professional proxies. Studies have revealed proxy-assessed ratings are most often aligned with patient ratings when the symptom is concrete and observable (Lobchuk & Denger, 2002; Pickard & Knight, 2005). It is clear, however, that many signs and symptoms at the end of life may not be readily visible.
Inaccurate proxy ratings may be grounded in hospice professionals’ lack of understanding related to patient reactions to terminal illness. As a result, an instrument capable of examining how hospice professionals differentiate adaptive and maladaptive reactions in persons at the end of life is warranted. Accurate differentiation between adaptive and maladaptive responses enhances hospice professionals’ capacity to provide accurate proxy assessments—therefore increasing the likelihood of providing timely, targeted interventions aimed at maintaining patient quality of life (QoL). The Hospice Professionals’ Understanding of Preparatory Grief (HPPG) Scale is a novel measure designed to assess hospice professionals’ ability to distinguish between adaptive and maladaptive reactions to terminal reactions in persons at the end of life.
Hospice and Persons With Terminal Illness
The specially trained hospice interdisciplinary team provides individualized, compassionate end-of-life care for both patients and their loved ones. The foremost goals of the hospice team are managing patient pain, assistance with the cognitive processes of dying, and offering education to family and loved ones regarding proper patient care to enhance care outcomes and maintain patient and family members’ QoL at the end of life (NHPCO, 2013b).
Social workers, specifically, are integral members of the hospice team and serve as resources for patients, families, and clinical staff, as they offer a systemic and holistic perspective when it comes to meeting patient needs. The utilization of social workers in hospice care has been associated with reduced operational costs, increased patient QoL, improved clinical team satisfaction, and a reduction in team turnover (Reese & Raymer, 2004).
Reactions to Terminal Illness
Patients report a wide variety of affective, behavioral, and cognitive responses to terminal illness at the end of life that impacts QoL (Tsilika et al., 2009). These reactions include, but are not limited to, pleasurable experiences with friends and family, increased spirituality, thoughts of satisfaction and contentment, feelings of self-worth, in addition to increased sensitivity to pain, fatigue, appetite disturbances, insomnia, constipation and nausea, pharmaceutical side effects, difficulty concentrating, anxiety, depression, and fear (Griffin, Koch, Nelson, & Cooley, 2007; Mystakidou, Tsilika, Parpa, Galanos, & Vlahos, 2008; Periyakoil & Hallenbeck, 2002; Tsilika et al., 2009). Previous research has demonstrated that these domains (i.e., cognitive, affective, and behavioral) are interrelated. For instance, anxiety has been shown to shape patient behaviors (Lehto & Stein, 2009), and somatic symptoms, such as increased pain, have been closely associated with depression and anxiety (Mystakidou et al., 2005).
These responses to terminal illness are best thought of as a continuum with poles being considered either adaptive or maladaptive. At one end of the spectrum are adaptive reactions (e.g., preparatory grief). In contrast, some responses to terminal illness are potentially more problematic, or maladaptive, for patients and/or loved ones, and may pave the way for sustained psychological distress and, subsequently, reduced QoL (Mystakidou et al., 2005, 2008; Periyakoil & Hallenbeck, 2002; Periyakoil et al., 2005). Between these two poles exists a wide range of reactions that are highly individualized and subject to the patient’s primary diagnosis.
Adaptive reactions to terminal illness
“Anticipatory grief” describes grief reactions that occur in absence of actual death, but instead to the “threat of death” (Lindemann, 1944, p. 200). Some scholars have associated anticipatory grief and anticipatory mourning with the processes incurred by the loved ones of the dying—these individuals anticipate the death of the patient and experience bereavement prior to the patient’s passing (Kacel, Gao, & Prigerson, 2011; Walker & Pomeroy, 1997). Preparatory grief, in contrast, occurs in the dying (Periyakoil & Hallenbeck, 2002). The primary difference between these two constructs, then, is who is experiencing the grief.
Some scholars have noted that patients effectively “die” psychosocially prior to their physical death—their past, present, and future losses penetrating every element of their person (Freeman & Ward, 1998; Mystakidou et al., 2005). That is, during this unique developmental stage, persons with terminal illness experience preparatory grief, an adaptive response to terminal illness. For the current study, preparatory grief will be defined as the common, acute responses to terminal illness experienced across individual domains (i.e., affective, behavioral, and cognitive) that may temporarily reduce QoL.
Maladaptive responses to terminal illness
Some consensus exists regarding what types of responses to terminal illness are considered maladaptive. These more problematic reactions in persons with terminal illness include ongoing depressed mood, persistent feelings of emptiness, and suicidal behaviors resulting in reduced QoL (Mystakidou et al., 2009; Periyakoil et al., 2005; Pessin, Rosenfeld, & Brietbart, 2002). These reactions have also been shown to increase the perception of pain that often results in the overuse of unnecessary pharmacological interventions. It must also be noted that sustained, severe psychological distress and feelings of hopelessness have been found to increase the risk of suicidal thoughts and behaviors in persons at the end of life (Mystakidou et al., 2009; Periyakoil et al., 2005; Pessin et al., 2002). In this study, maladaptive responses to terminal illness will be defined as those chronic, reactions resulting in a significant, sustained decrease in QoL experienced across individual domains (i.e., affective, behavioral, and cognitive; Mystakidou et al., 2005, 2008; Periyakoil & Hallenbeck, 2002; Periyakoil et al., 2005).
Cognitive domain
The cognitive domain of reactions to terminal illness for the current study includes thoughts, attitudes, beliefs, or understandings about death and dying a person experiences while facing terminal illness. This can be related to future uncertainty, meaning found in life and in dying, and perceived ability to change one’s dying process (Cicirelli, 2003; Vess, Landau, Routledge, & Arndt, 2009). Maladaptive cognitive reactions to terminal illness include increased thoughts of suicide or beliefs that the patient is completely alone.
Affective domain
Individuals with terminal illness may demonstrate a variety of emotions or moods while navigating the end-of-life process. For the current study, the affective domain of reactions to terminal illness includes expressed or withheld emotions or moods regarding the dying process a person experiences while terminally ill. Persons with terminal illness may worry, experience anxiety and depression, or perhaps fear. Apprehension, for example, has been said to exist as a matter of growing death awareness (Lehto & Stein, 2009). Maladaptive affective reactions, in contrast, include feelings of prolonged hopelessness and helplessness or ongoing bouts of depression.
Behavioral domain
Persons with terminal illness must also contend with somatic manifestations of grief and other behaviors at the end of life. For the current study, the behavioral domain of reactions to terminal illness includes physical grief reactions and/or somatic complaints in persons with terminal illness that are unrelated to the terminal disease process a person experiences while terminally ill. Mystakidou et al. (2005) indicated that patients noting poor performance status had significantly higher scores related to physical complaints when compared to their high performance status counterparts. These reactions may include, but are not limited to, changes in sleeping habits, disordered eating, and physiological responses such as difficulty swallowing, breathing, or changes in heart rate. Maladaptive behavioral reactions, including suicidal acts, may indicate severe psychological distress and a significant decrease in patient QoL.
Assessing Reactions to Terminal Illness
Self-reports are often considered the most accurate assessment, or “gold standard,” of a patient’s end-of-life experience (Lobchuk & Denger, 2002; Pickard & Knight, 2005; Prost, 2014; Tang & McCorkle, 2002). However, barriers to self-assessment validity are numerous. For instance, medical complications or delirium may cloud accurate assessment for both patients and caregivers (Pessin et al., 2002), or patients may find the assessment process physically or emotionally burdensome (Pickard & Knight, 2005; Sneeuw, Sprangers, & Aaronson, 2002). As a result, proxy ratings may be completed by hospice professionals to guide care.
Research in oncology, long-term care, and end-of-life care has highlighted incongruence exists between proxy and patient-assessed ratings across a variety of conditions including pain, psychological distress, and QoL (Cohen, Boston, Mount, & Porterfield, 2001; Hill, 2002; Lobchuk & Denger, 2002; Sneeuw et al., 2002; Tang & McCorkle, 2002). Proxy ratings are generally most aligned with patient assessments (i.e., more accurate) when the symptom is easily observable (e.g., nausea and suicidal behaviors; Lobchuk & Denger, 2002; Pickard & Knight, 2005). When matched head-to-head, proxies are more likely to overestimate symptom distress and underestimate QoL than their patients Sneeuw et al., 2002.
It has been suggested that this “perception gap,” the disparity that emerges when comparing matched, self-assessed ratings to assessments completed by proxies may be rooted in several correlates, namely, proxy professional characteristics. For instance, proxies’ lack of training or education related to the assessment of psychosocial stressors in persons at the end of life has been cited as a possible precursor of the perception gap (Pessin et al., 2002). It is further possible that interrater disparities emerge as a result of low palliative care self-efficacy. Palliative care self-efficacy is a measure of how well professionals who provide palliative care services perceive their capability to answer questions and respond to end-of-life care needs in their patients (Phillips, Salamonson, & Davidson, 2011). Though related to training and education regarding psychosocial stressors and reactions to terminal illness, palliative care self-efficacy more closely reflects capabilities and confidence in palliative care service provision.
The current study is aimed at developing and validating an instrument capable of examining how hospice professionals differentiate adaptive and maladaptive reactions in persons at the end of life. It is believed that the accurate differentiation of these reactions will support accurate assessment, subsequent intervention (Chochinov, Wilson, Enns, & Lander, 1997; Pessin et al., 2002; Shuster, Breitbart, & Chochinov, 1999), and the maintenance of QoL in persons with terminal illness (McKiernan, Spreadbury, Carr, & Waller, 2013; Pickard & Knight, 2005).
Patient-Assessed Measures
As previously noted, self-reports are often considered the most accurate representation of how a hospice patient truly “is”(Prost, 2014) despite the frequent use of proxy-assessed measures in end-of-life care and limitations associated with self-report bias. Several self-assessed measures have been developed and validated with samples of persons with terminal illness in an attempt to capture reactions, both adaptive and maladaptive, to one’s impeding death.
Preparatory grief in advanced cancer (PGAC)
Mystakidou et al. (2005) provided the first self-report inventory aimed at identifying preparatory grief in persons with cancer. The PGAC contained 36 items with a 4-point Likert-type scale response option scheme ranging from 0 (disagree) to 3 (agree) taking less than 10 minutes to complete. Patients indicated how much they agreed or disagreed with a variety of statements describing possible reactions to having cancer with higher scores indicating greater levels of preparatory grief. Seven factors were extracted via exploratory factor analysis, yielding a total variance explained of 65.84%. The subscales retrieved were later named self-consciousness, disease adjustment, sadness, anger, religious comfort, somatic symptoms, and perceived social support (Mystakidou et al., 2005). The initial validation with a sample of cancer patients (n = 200) demonstrated adequate internal consistency (α = .838).
Terminally Ill Grief or Depression Scale (TIGDS)
Recent research has also focused on delineating adaptive and maladaptive responses to terminal illness (Irwin et al., 2008; Periyakoil & Hallenbeck, 2002; Periyakoil et al., 2005). Depression can occur in up to 45% of those who are terminally ill and has been shown to reduce QoL in the dying. The TIGDS contained 42 items across two subscales: preparatory grief and depression with true/false response options. The TIGDS was administered with a small sample (n = 55) of patients with terminal illness. Results revealed an intraclass coefficient for the two domains (.86, preparatory grief; .97, depression) demonstrating good reliability. A receiver operating characteristic (ROC) curve analysis was utilized to determine the validity of the TIGDS alongside established clinical criterion (i.e., depression average score ≥ 2.5). The depression score provided an isolated cut point highlighting that 62% of the patients (n = 8) were also identified by clinicians as depressed (i.e., scored ≥2.5). Of those with scores less than 3, only one was incorrectly classified by clinicians as depressed (7%). Findings from the ROC curve analyses indicated the TIGDS demonstrated an ability to differentiate adaptive and maladaptive responses in patients. The depression subscale also illustrated a strong, positive correlation with the Hospital Anxiety and Depression Scale total score as hypothesized, indicating good convergent construct validity (Periyakoil et al., 2005).
The HPPG Scale
The previous literature review has highlighted several themes. First, hospice agencies are charged with assuring that patient QoL is maintained throughout the dying process. Research also indicates that some reactions to one’s impending death can be considered adaptive (preparatory grief) and others more so maladaptive (Kacel et al., 2011; Mystakidou et al., 2005, 2008; Periyakoil & Hallenbeck, 2002; Periyakoil et al., 2005; Rando, 1984). Literature from a variety of disciplines has further indicated matched comparisons between patient and proxy ratings are often incongruent—resulting in an interrater or perception gap (Mittal et al., 2007; Pickard & Knight, 2005). This disparity poses far-reaching implications, as the inability to differentiate adaptive from maladaptive reactions to terminal illness precipitates an inability to intervene, further risking patient’s QoL. These concerns predicate an investigation regarding hospice professionals understanding such reactions; however, no such measure exists.
The previous self-assessed measures demonstrate unique strengths and contributions to the end-of-life care literature. The proposed measure, however, shifts the perspective to that of the hospice professional and, as with the TIGDS (Periyakoil et al., 2005), aims to highlight both adaptive and maladaptive responses to terminal illness. Considering these themes, the research question for the current study is, Can hospice professionals’ understanding of adaptive and maladaptive responses to terminal illness be usefully modeled and scaled? It is hypothesized that a three-factor structure paralleling the affective, behavioral, and cognitive domains of reactions to terminal illness will be found.
Methods
Instrument Development
Items for the HPPG were constructed based on items from the TIGDS (Periyakoil et al., 2005) and PGAC (Mystakidou et al., 2005) measures, as well as end-of-life care literature highlighting various responses to terminal illness (Kacel et al., 2011; Mystakidou et al., 2008; Periyakoil & Hallenbeck, 2002; Rando, 1984). The HPPG, however, shifts the assessment perspective to that of the hospice professional working with persons with terminal illness. An initial pool of 52 questions was constructed utilizing a domain sampling plan of both adaptive and maladaptive reactions across affective, behavioral, and cognitive domains. Each domain included a stem listed above the group of respective items (i.e., cognitive: “terminal patients may think … ”; affective: “terminal patients may feel … ”; behavioral: “terminal patients may … ”). Hospice professionals were asked to “please take a moment to consider each statement and indicate how closely you think the reaction reflects typical, preparatory grief in terminal patients by selecting the appropriate response option ranging from 1 = mostly false to 5 = mostly true.” The instructions further clarified that those reactions that were given higher scores would reflect reactions considered more normative and those reactions that were given lower scores, in turn, would reflect pathological reactions.
Questions in the affective domain included items such as terminal patients may feel “fear of the unknown,” “satisfied when reflecting on their past,” and “a persistent sense of emptiness.” Questions appearing within the behavioral domain asked about patient preferences of isolation and ongoing fits of crying that do not respond to consolation. Items within the cognitive domain included queries regarding a patient’s thoughts about suicide, worries about the responsibility of their terminal diagnosis, and beliefs of having lived “a good life.”
HPPG subscales are scored by taking the mean of item responses after reverse scoring maladaptive items with the following recoding scheme: 1 = 5, 2 = 4, 3 = 3, 4 = 2, and 5 = 1. As a result, hospice professionals who indicated they believe what previous literature indicates is a maladaptive reaction to be adaptive will score a “1.” Subscale scores range from 1 to 5 with higher scores indicating increased accuracy of differentiating adaptive and maladaptive reactions in persons with terminal illness within each domain. The global HPPG score is obtained by computing a mean of subscale scores. Global scores also range from 1 to 5 with higher scores indicating increased accuracy of differentiating adaptive and maladaptive reactions in persons with terminal illness.
Content Validity
The initial 52-item HPPG Scale was provided to six expert panelists consisting of three hospice professionals and three PhD-level social work faculty members. The hospice professionals (two social workers and one administrator; all female) were currently employed with two different local hospice providers in a small, southeastern community. Faculty panelists (all female) were familiar with literature in hospice and end-of-life care, as well as instrument validation. Panelists were provided a content validity exercise with the original items (n = 52) and domain structure of the HPPG and associated global and domain (i.e., cognitive, affective, and behavioral) definitions. The content validity exercise asked that experts rate each item based on its accurate representation of the construct domain definition presented. Response options ranged from 1 (not at all) to 5 (very well). Items constructed as maladaptive were clearly identified by the author using an asterisk to assure expert assessment was accurate.
Of the six experts approached, three panelists provided feedback regarding item modification, item–domain fit, and possible item removal. Results of the content validity exercise can be found in Table 1 (n = 3; one faculty member and two hospice professionals). Mean scores and standard deviations across cognitive domain (n = 13), affective domain (n = 25), and behavioral domain (n = 14) items were calculated. Items with mean responses lower than 3 (n = 13; 25%) were flagged for further inspection though these items were not removed at this stage. Items on the HPPG scale scored an average of 3.43 (SD = 1.04), which demonstrated slightly greater than average item–domain fit. Two items were shifted from one domain to another (i.e., affective to cognitive; cognitive to affective), and two items were removed based on language biases (“terminal patients may think they should try to commit suicide;” “terminal patients may think they can ‘beat’ their diagnosis”) resulting in the 50-item HPPG.
52-Item Hospice Professionals’ Understanding of Preparatory Grief Scale: Content Validity Ratings.
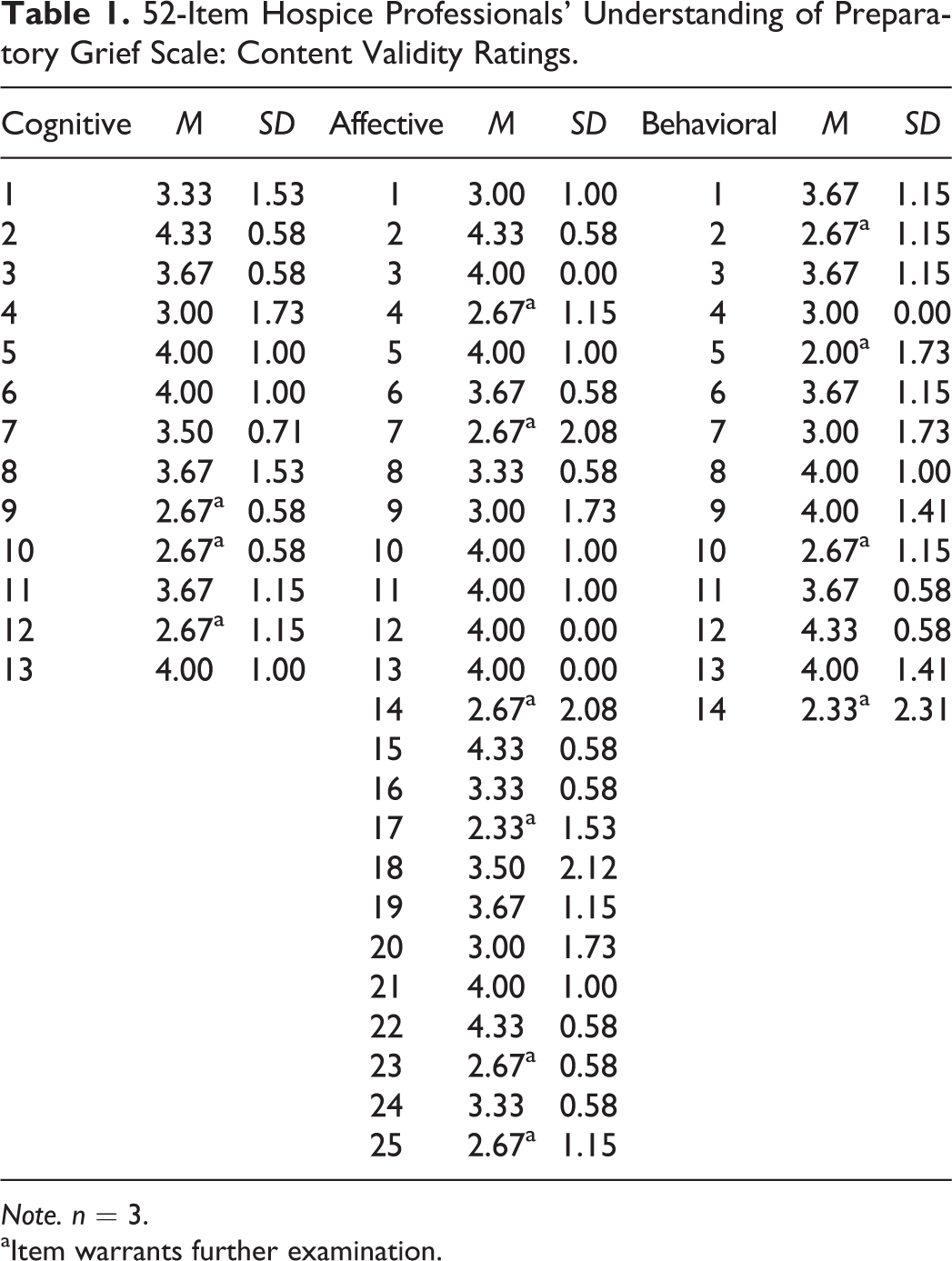
Note. n = 3.
aItem warrants further examination.
Data Collection Instrument
The data collection instrument included the 50-item HPPG, a standardized measure and single-item indicator (SII) to assess convergent construct validity, and several additional demographic questions to assess discriminant construct validity and to characterize the responding sample. The instrument was estimated to take less than 15 minutes to complete. The Palliative Care Self-Efficacy Scale (PCSES; Phillips et al., 2011), a standardized self-assessment, was used to assess convergent construct validity. The PCSES is aimed at determining how well professionals who provide palliative care services perceive their capability to (1) answer questions related to end-of-life care and (2) respond to end-of-life reactions in patients (Phillips et al., 2011). Twelve items are divided evenly across the two subscales. Respondents were asked to rate their perceived capability to perform each of the associated palliative care tasks including items related to supporting patients and families at the end of life, coping with and reacting to reports of nausea and vomiting, and answering questions regarding medication management. Response options provided ranged from 1 (need further basic instruction) to 4 (confident to perform independently).
Initial validation with over 400 aging care professionals revealed a two-factor solution with Cronbach’s α for global and subscales ranging from .87–.92 demonstrating good reliability and alignment with the a priori factor structure. It was hypothesized that global scores on the HPPG will be positively correlated with global scores on the PCSES (Phillips et al., 2011), demonstrating evidence of convergent construct validity. As hospice professional’s perceived capacity to answer patient questions and respond to patient symptoms increases, it is likely that their accurate differentiation of adaptive and maladaptive reactions in persons with terminal illness will also increase. It was further hypothesized that individual global scores on the HPPG would be positively correlated with individual respondent scores on the SII. The SII asked respondents to rate their perceived ability “to differentiate normative, preparatory grief from atypical responses to terminal illness in the persons who are dying.” Response options ranged from 1 (very poor) to 5 (very good).
Eight additional items were included in the data collection instrument such as queries regarding demographic characteristics (e.g., age, sex, and race), as well as professional characteristics (e.g., primary role within the hospice agency; number of years working in hospice or palliative end-of-life care). Responses to these questions were used to characterize the responding sample. Discriminant construct validity evidence was examined by inspecting correlations between the demographic characteristics of sex and race and individual global HPPG scores. It was hypothesized that no statistically significant relationship would emerge between individual global scores on the HPPG and respondents’ sex and race.
Sampling and Data Collection
Institutional review board (IRB) approval was obtained after expert panel content validation and prior to data collection. The current study utilized two primary sources to obtain participants: Agency ListServs and Facebook. First, the author obtained permission from respective agency directors to utilize ListServs for the Florida Hospice and Palliative Care Association (FHPCA) and the Louisiana-Mississippi Hospice and Palliative Care Organization (LMHPCO) to e-mail the data collection instrument to individual hospice professionals currently registered with each organization (2,890 and 1,027, respectively). Additionally, the author utilized Facebook to post a brief description of the study to gain additional responses once every other day for 14 days. Persons currently employed with hospice or palliative end-of-life care agencies that were over the age of 18 were asked to participate.
A series of four e-mails were utilized to recruit potential participants from the FHPCA and LMHPCO ListServs. An initial e-mail provided detailed information regarding study background, associated risks and benefits, and consent information, as well as the anonymous survey link. Three additional e-mails were sent 7, 10, and 14 days after the initial e-mail to increase the response rate. Respondents were asked to affirm their understanding of the purpose of the study, their awareness of the associated risks and benefits of participation, and the voluntary nature of their anonymous responses. Only after providing affirmative responses to each of these queries were respondents provided access to the data collection instrument.
Analysis
SPSS Version 20 (IBM Corp., 2011, Armonk, NY) was utilized to examine univariate and bivariate descriptive statistics, item-by-item correlation matrixes, and internal consistency. LISREL 8.80 (Jöreskog & Sörbom, 2006) was utilized to examine factor structure of the HPPG. Composite variables were created to represent subscale and global scales for the HPPG upon examining missingness. Convergent and discriminant construct validity of the global HPPG were examined using bivariate correlations in SPSS Version 20 (IBM Corp., 2011), as well. Items were retained based on several forms of statistical and psychometric evidence including internal consistency and model–data fit indexes. Last, readability analyses were performed using Microsoft Word for the global HPPG to assure ease of use.
Results
Approximately 5% of registered contacts on both the FHPCA and LMHPCO ListServs initiated the online survey between January 28, 2014, and March 13, 2014 (n = 316). Of these, 241 completed the data collection instrument. Data from these respondents were combined and exported from the Qualtrics Research Suite into SPSS Version 20 (IBM Corp., 2011) for further cleaning and analyses. Cases where respondents did not complete the novel HPPG Scale (n = 45; Items 4–13 in the online survey) were excluded from analyses leaving 196 cases for subsequent analyses.
Demographics
Descriptive statistics (e.g., mean, range, skewness, and kurtosis) were examined to assure univariate normality among demographic characteristics and items contained within the HPPG. All HPPG items fell within the acceptable ranges (i.e., skewness ≤ 3 and kurtosis ≤ 10), indicating subsequent analyses were appropriate.
Respondent characteristics can be found in Table 2. Demographic characteristics indicate that over 80% (n = 161) of the respondents were female. Frequencies were examined for respondent race, and only 9.7% of respondents indicated a racial makeup other than White/Caucasian indicating racial homogeneity. For this reason, respondent race was dichotomized to include White (n = 177) and non-White groups (n = 17; human, n = 2). The average age of respondents was approximately 50 years with responses ranging from 22 to 71.
50-Item Hospice Professionals’ Understanding of Preparatory Grief Scale Respondent Characteristics.

Note. PCSES = Palliative Care Self-Efficacy Scale, range = 12–48, α = .89.
Professional characteristics were also examined. The majority of respondents self-reported the highest level of education obtained was a bachelor’s degree (35.7%). The majority of respondents indicated their primary role within the hospice or palliative end-of-life care agency was social work (25.5%), followed closely by administration (21.4%), and other roles such as bereavement and community education (20.9%). Respondents reported a wide range of direct patient contact each week (0–60 hr) with an average of 17 hours. Respondents also self-reported an average of 9.1 years working in hospice with responses ranging from 0 to 39 years. The average score on the PCSES (Phillips et al., 2011) was 42.3 with possible scores ranging from 12 to 48. This can be considered a moderate-high average level of palliative care self-efficacy for these respondents. Internal consistency for the global PCSES (α = .89) demonstrated good internal consistency for this sample, closely paralleling results from the measure’s initial validation.
Missing Data
Of the 196 cases, only three of the novel scale items demonstrated missingness, and of these, none exceed 2% missing. Little’s Missing Completely at Random (MCAR) test revealed χ2 = 83.27(97) and a nonsignificant p value (.839). This indicated the use of imputation for these values was appropriate. Mean value imputation was used, and 196 cases were retained for the following analyses.
Internal Consistency
Item-by-item correlations were examined within subscales to reduce redundancy prior to examining internal consistency. The largest item-by-item correlations did not exceed the suggested cutoff .8 for any HPPG subscales (cognitive = .592, affective = .705, and behavioral = .767). Cronbach’s α was used to determine internal consistency within subscales. Results of initial reliabilities for subscales can be found in Table 3. Initial αs (cognitive = .234, affective = .599, behavioral = .383) fell far below the suggested .70 threshold which indicated poor internal consistency.
50-Item Hospice Professionals’ Understanding of Preparatory Grief Scale Reliability: Internal Consistency.
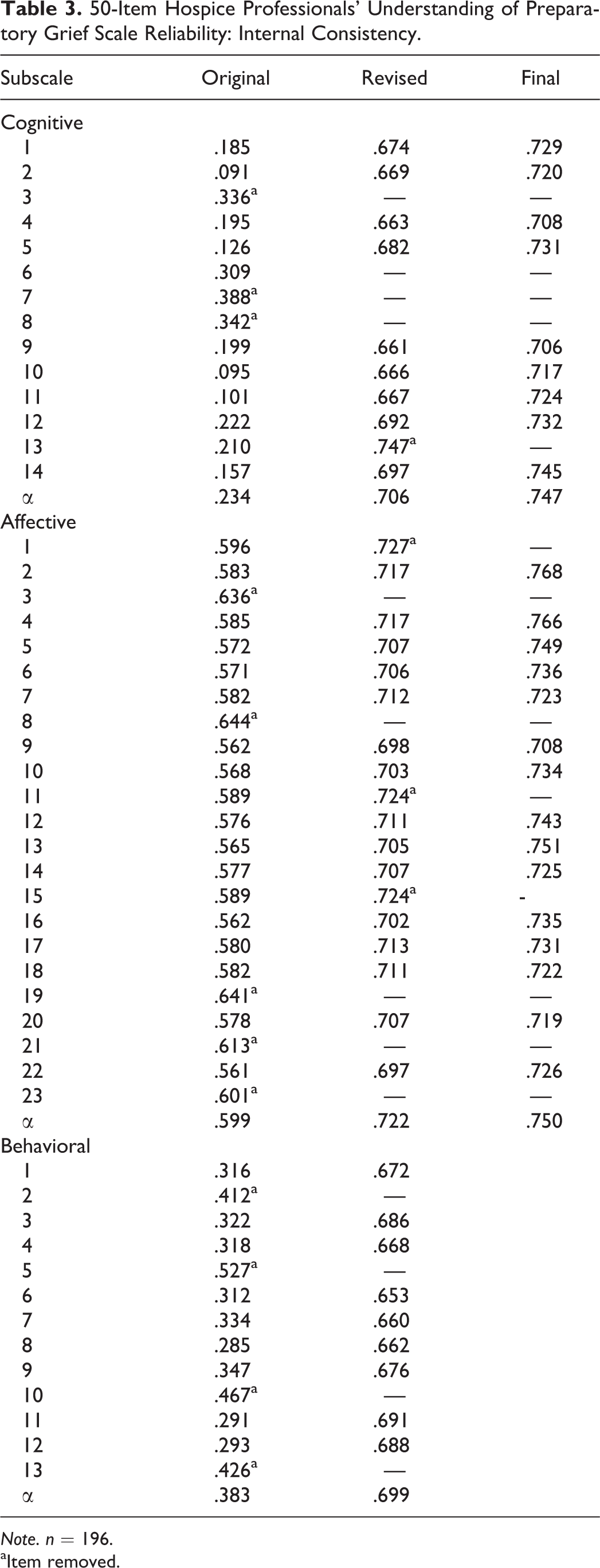
Note. n = 196.
aItem removed.
Alpha-if-item deleted values were examined to determine whether items warranted removal. Four items with alpha-if-item deleted values ranging from .309 to .388 were removed (e.g., “terminal patients may think they have lost their dignity”) from the cognitive domain yielding a revised α of .706. Similarly, 5 items with high alpha-if-item deleted values (range: .601–.644) were removed (e.g., “terminal patients may feel guilty about past wrongdoing”) from the affective domain subscale producing an α of .722. Four items with alpha-if-item deleted values ranging from .412 to .527 were also removed from the behavioral domain (e.g., “terminal patients may cry uncontrollably”) yielding a revised α of .699. Subsequent item removals for the cognitive (1 item) and affective domains (3 items) allowed αs to further surpass the minimally acceptable value of .70 (.747 and .750, respectively; Abell, Springer, & Kamata, 2009). Figure 1 depicts these and subsequent item attrition. The remaining items (n = 33) were retained for subsequent confirmatory factor analysis (CFA).
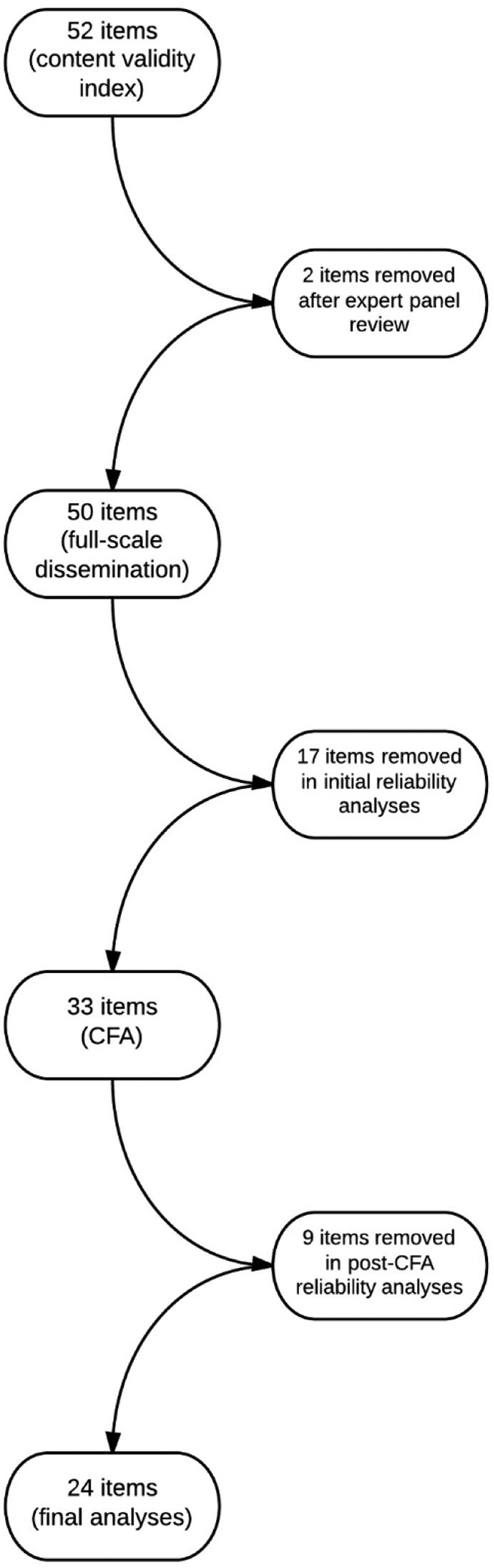
Flow chart depicting item attrition.
CFAs
LISREL 8.80 (Jöreskog & Sörbom, 2006) was utilized to examine the accuracy of the hypothesized factor structure of the revised 33-item HPPG via CFA. Goodness of fit was determined based on several indexes including root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), comparative fix index (CFI), Tucker–Lewis index (TLI), and the ratio of degrees of freedom to χ2. Acceptable values for RMSEA range from <.05 to <.08 with smaller values indicating better model fit. Values of SRMR are expected to fall below .10. Values of CFI and TLI above .90 indicate acceptable fit with values above .95 illustrating excellent fit. Desirable χ2/df ratios are less than 2 or 3. Values larger than 3 suggest poor fit (Abell et al., 2009). A summary of CFA model results can be found in Table 4. Initial results indicated poor model fit with all values outside acceptable ranges.
33-Item Hospice Professionals’ Understanding of Preparatory Grief Scale Confirmatory Factor Analyses: Initial and Respecified Models.
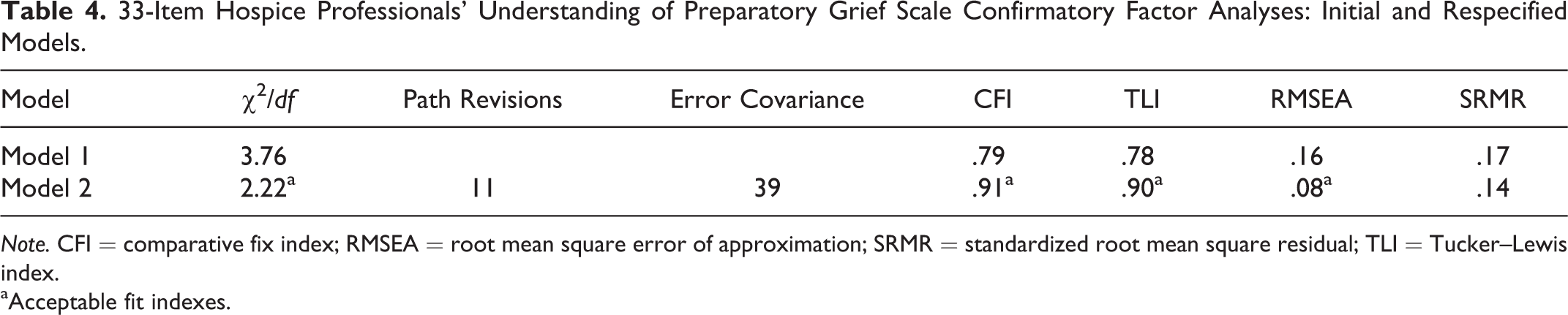
Note. CFI = comparative fix index; RMSEA = root mean square error of approximation; SRMR = standardized root mean square residual; TLI = Tucker–Lewis index.
aAcceptable fit indexes.
LISREL provides two primary forms of modification: path revision and correlations among error covariance terms. Revised paths (i.e., item moved from initially hypothesized domain to a different domain) were considered if two conditions were met: (1) the resulting difference in model χ2 was 10 or greater and (2) items demonstrated appropriate conceptual fit within the new domain. Correlations of error covariances were considered when items were related conceptually (i.e., both items are from the same domain). For example, the affective domain item “terminal patients may feel pleasure when loved ones visit” was moved to the cognitive domain as the reduction in χ2 was greater than 10 and feeling pleasure could be closely conceptualized as thinking pleasant thoughts about loved ones.
Based on modification indexes provided by the first CFA model, a second CFA model incorporated 11 revised paths between observed and latent variables and 39 error covariances.
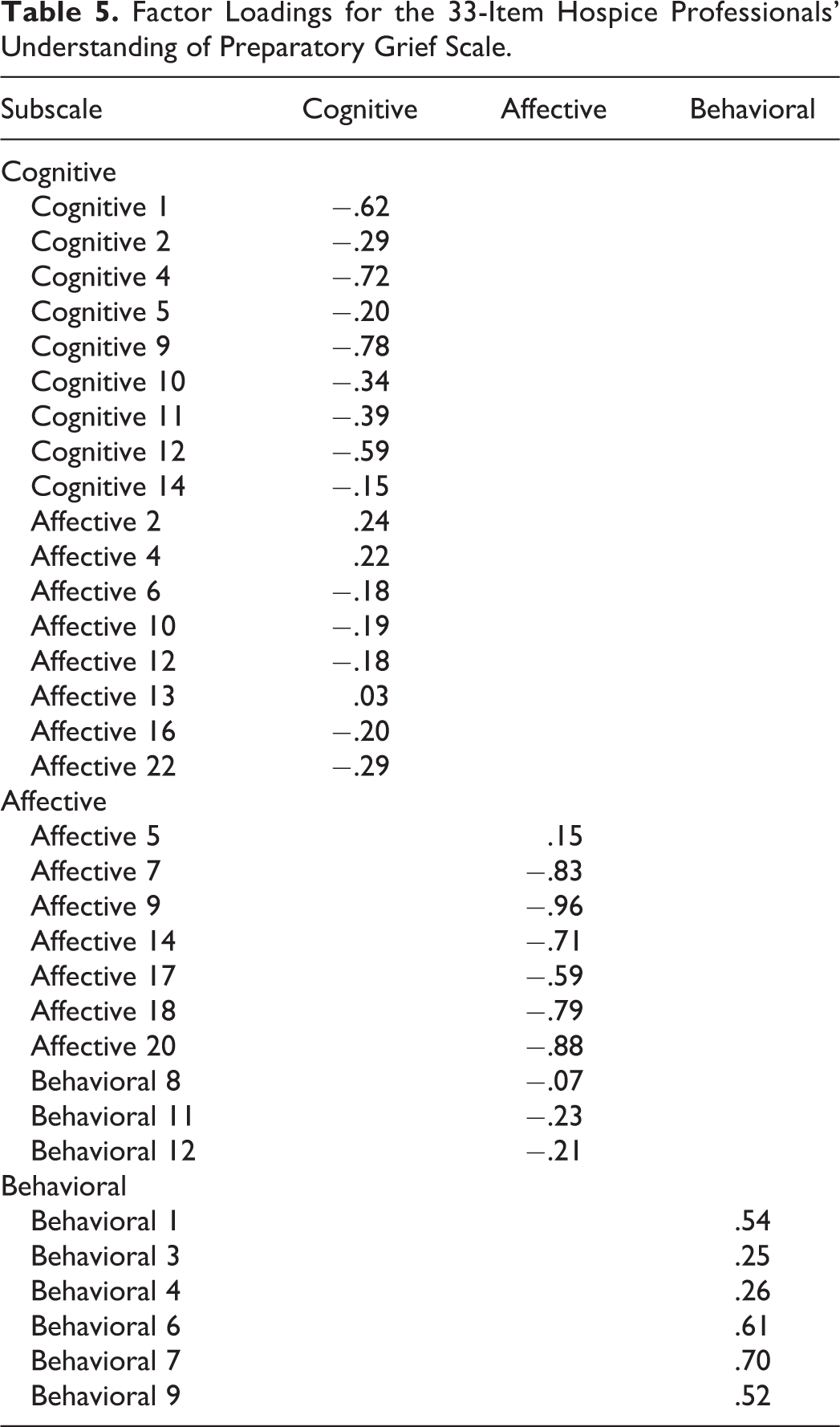
This second model yielded improved model fit with a χ2/df ratio of 2.22, CFI = .91, TLI = .90, RMSEA = .08, and SRMR = .14. Four of the five resulting fit indexes were considered acceptable where the value of SRMR (.14) lies just outside the acceptable target range. Factor loadings for 33-item HPPG Scale can be found in Table 5.
Factor Loadings for the 33-Item Hospice Professionals’ Understanding of Preparatory Grief Scale.
Internal Consistency: Revisited
Suggested path revisions resulted in domain restructuring of the 33-item HPPG. These revisions required subsequent reliability analyses to assure adequate internal consistency (i.e., α ≥ .70). Findings are presented in Table 6. The post-CFA cognitive domain (n = 17) included original items from affective and cognitive domains that could be understood as either thoughts or moods contingent upon question stem. The initial α was .783. Two alpha-if-item deleted values exceeded the initial reliability coefficient and were removed (e.g., “terminal patients may feel fearful about the unknown”). Subsequent revision included removal of one additional item and a final α of .820 (n = 14). Items contained within the final cognitive domain included both adaptive and maladaptive reactions to terminal illness across the initial affective (n = 5) and cognitive domains (n = 9).
33-Item Hospice Professionals’ Understanding of Preparatory Grief (HPPG) Scale Reliability: Internal Consistency.
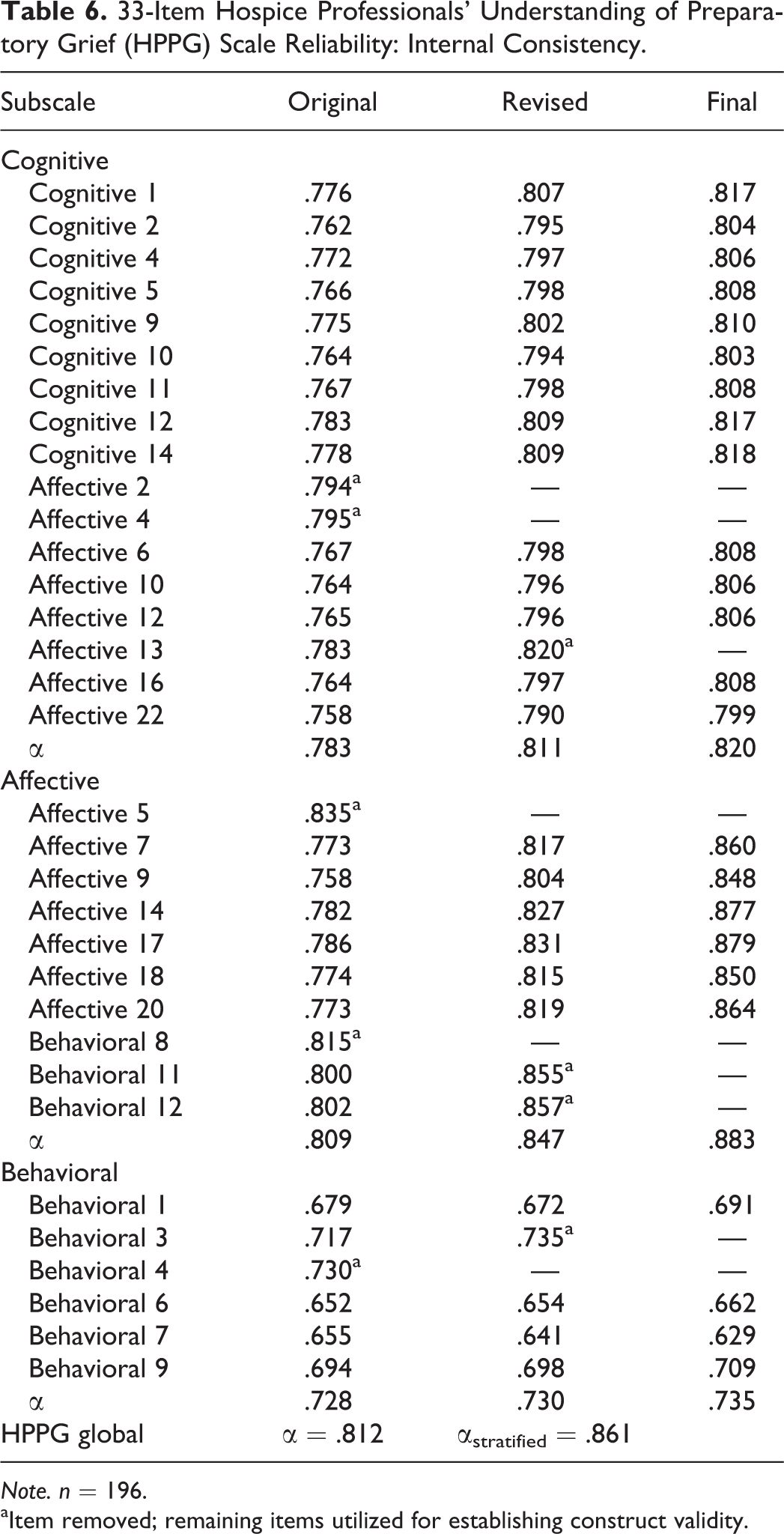
Note. n = 196.
aItem removed; remaining items utilized for establishing construct validity.
The post-CFA affective domain (n = 10) included items from both the previously hypothesized affective and behavioral domains with an initial α of .809. Those items from the behavioral scale were all reverse scored (i.e., reflecting maladaptive responses to terminal illness) and were constructed with similar language (e.g., “persistent,” “prolonged”). Two items were removed based on alpha-if-item deleted values. This revision revealed two additional problematic items (e.g., “terminal patients often appear happy when surrounded by friends and family”). These items were removed, and the final α was .883 (n = 6). The final affective domain contained only items from the initially hypothesized affective domain.
Finally, the post-CFA behavioral domain (n = 6) demonstrated an initial reliability of .728. One item provided an alpha-if-item deleted value greater than the initial α and was consequently removed. One final revision included the removal of one additional item. The final post-CFA behavioral domain yielded a reliability of .735 (n = 4) and contained only items from the initially hypothesized behavioral domain. The final instrument, along with participant instructions, can be seen in Figure 2 and includes 24 items across the three previously hypothesized domains (cognitive, n = 14; affective, n = 6; behavioral, n = 4).
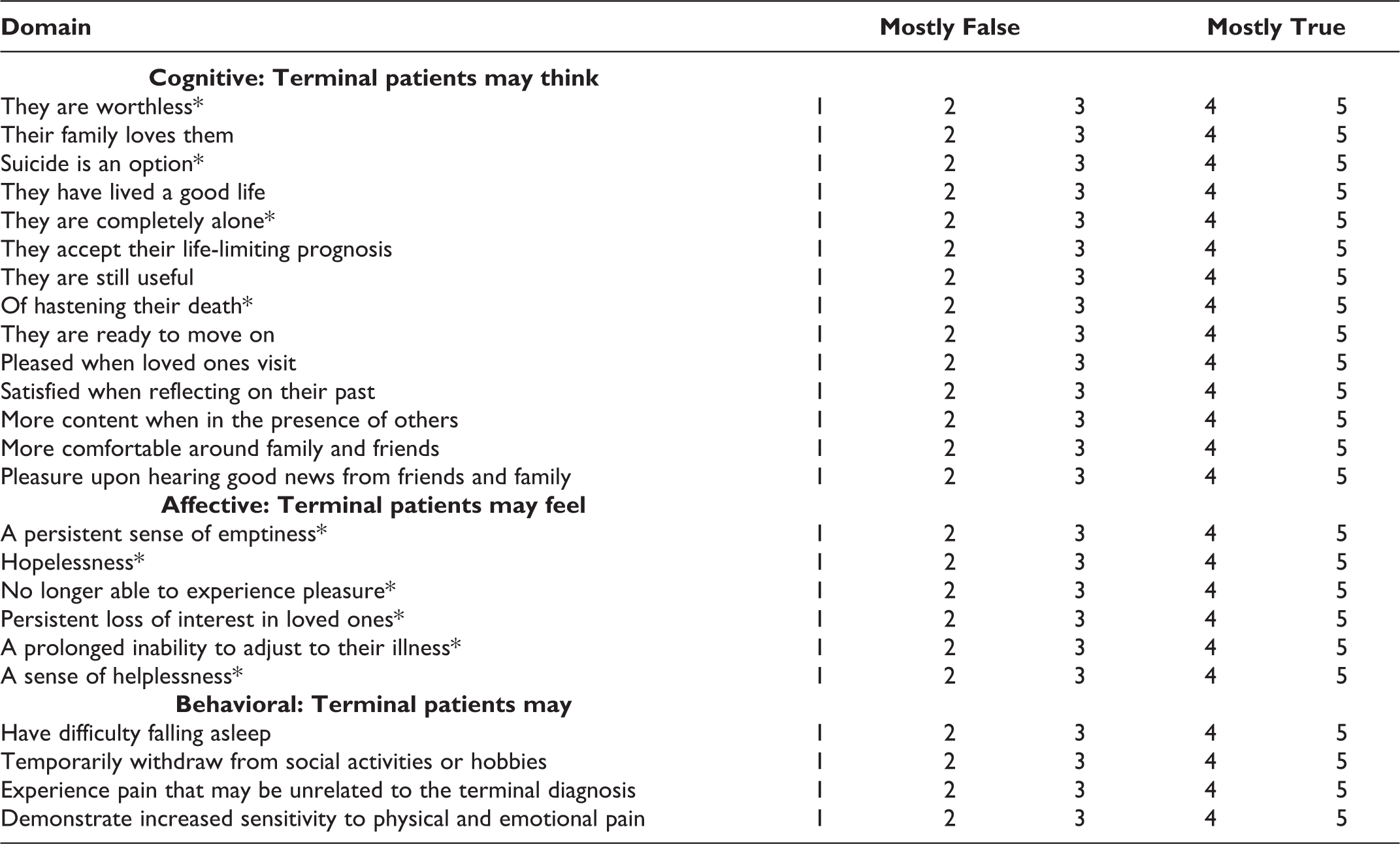
Final instrument: Hospice Professionals’ Understanding of Preparatory Grief Scale.
Construct Validity
Results of analyses examining convergent and discriminant construct validity can be found in Table 7 and reflect minor revisions in item–domain composition. As previously indicated, the final cognitive domain construction included items drawn from the initial affective domain. It was hypothesized that correlations between individual global HPPG scores and two other measures (i.e., individual global PCSES scores; SII) would be positive and statistically significant. However, no significant correlation emerged among respondent global HPPG scores, global PCSES scores (r = .053; p > .05), or the SII (r = .119; p > .05). As a result, the hypothesized convergent construct relationship was not supported.
24-Item Hospice Professionals’ Understanding of Preparatory Grief (HPPG) Scale Construct Validity.
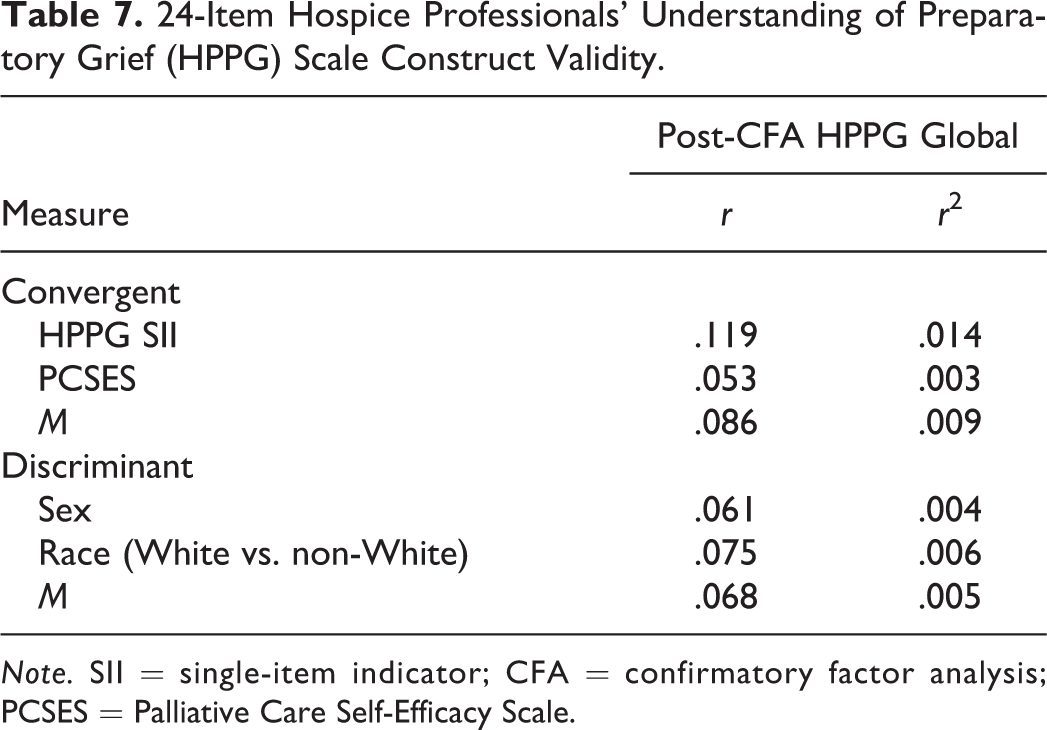
Note. SII = single-item indicator; CFA = confirmatory factor analysis; PCSES = Palliative Care Self-Efficacy Scale.
It was further hypothesized that the HPPG would not be correlated with respondent sex and race, two variables used to establish discriminant construct validity. Bivariate correlations support the discriminant construct validity hypotheses demonstrating no statistically significant relationships between respondent global HPPG scores, sex (r = .061; p > .05), and race (r = .075; p > .05).
Global Statistics
Cronbach’s alpha indicated good reliability (α = .812) for the HPPG. Previous research has indicated, however, that Cronbach’s alpha for multidimensional scales may be underestimated due to correlations between subscales or domains (Abell et al., 2009). The reliability coefficient of stratified alpha, in contrast, acknowledges subscale correlations and provides a more accurate measure of internal consistency. The stratified alpha for the HPPG (α = .861) indicated increased reliability when compared to Cronbach’s alpha.
The standard error of measurement (SEM) for the HPPG subscales was also examined. This estimate can be used to predict possible scores based on a respondent’s observed score. Lower values of SEM, with suggested scores less than or equal to 5% of the response range, are preferred (Abell et al., 2009). Desired subscale SEM values for the HPPG should fall at or below .20. Results indicated that subscale SEM values for both the affective (.29) and behavioral (.35) domains fell above the desired 5% cutoff. The SEM for the HPPG cognitive domain emerged just outside the suggested value (.21).
Subscale and global HPPG correlations were also examined, and findings from these bivariate analyses can be found in Table 8. The resulting statistics indicated strong positive correlations between the affective subscale and the global HPPG (r = .744, p < .01) and cognitive subscale (r = .534, p < .01). It must also be noted that the behavioral subscale demonstrates a weak-to-moderate, negative relationship across all other subscales and the global HPPG. Further, Pearson’s r between the cognitive subscale and global HPPG (.927, p < .01) indicated a very strong, positive relationship unlikely to have occurred by chance.
24-Item Hospice Professionals’ Understanding of Preparatory Grief (HPPG) Subscale and Global Scale Correlations.
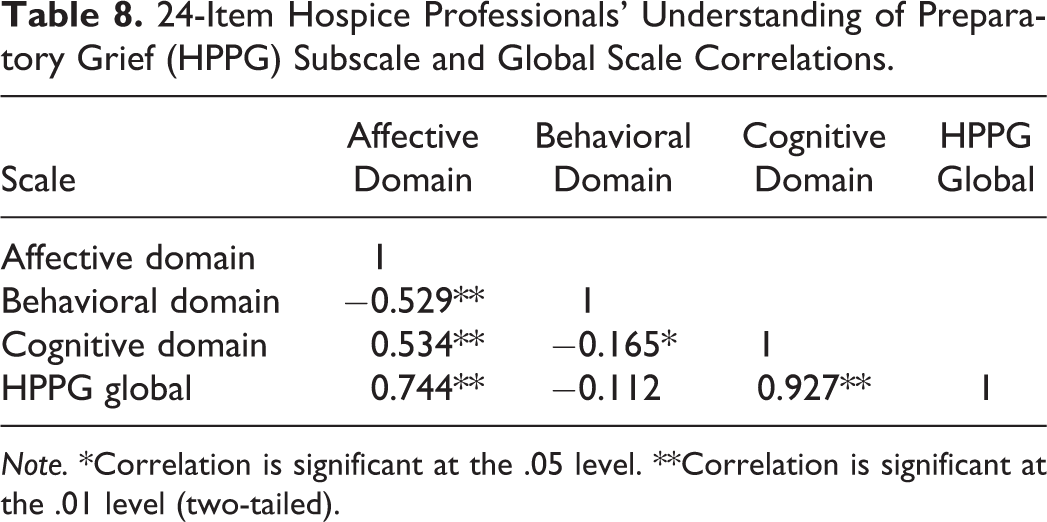
Note. *Correlation is significant at the .05 level. **Correlation is significant at the .01 level (two-tailed).
Final readability analyses on the HPPG were used to assure ease of use with hospice professionals. The resulting Flesch–Kincaid reading level was 7.2. This reading level is appropriate, as hospice professionals have completed high school and are unlikely to have concerns understanding the content presented in the HPPG instructions or items.
The HPPG global score is meant to capture a hospice professional’s ability to differentiate between persons’ adaptive and maladaptive reactions to terminal illness. Global scores are computed by obtaining an average of subscale scores with higher scores indicating increased ability to accurately differentiate responses to terminal illness (range = 1–5) based on items constructed from previously validated scales (i.e., PGAC, TIGDS). The mean global HPPG score was 3.64 (SD = .249), indicating a slightly greater than average self-assessed ability to differentiate between adaptive and maladaptive responses to terminal illness. This and other subscale and global scale statistics can be found in Table 9.
24-Item Hospice Professionals’ Understanding of Preparatory Grief (HPPG) Subscale and Global Scale Descriptive Statistics.
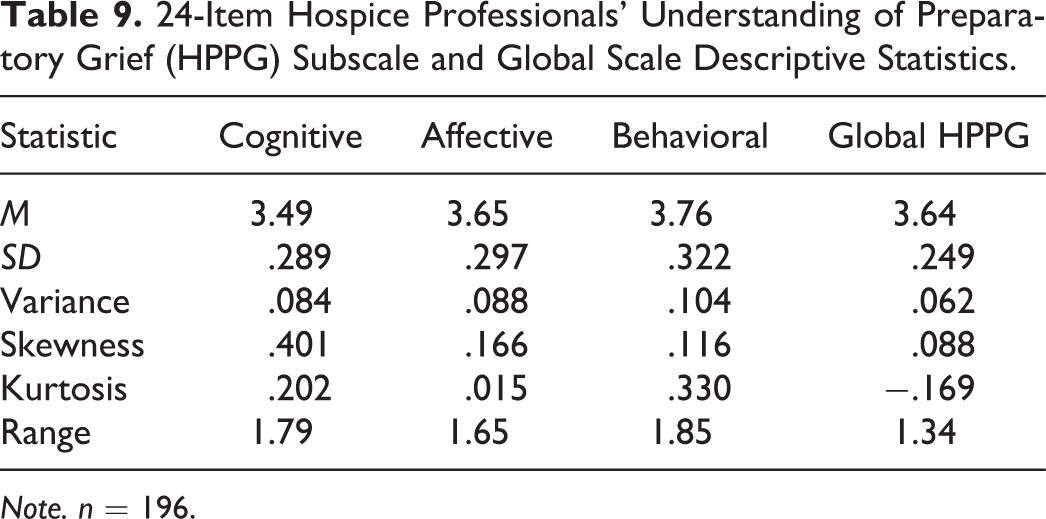
Note. n = 196.
Discussion and Applications to Practice
The results of the current study detailed the first attempt to develop and validate a measure of hospice professionals’ understanding of adaptive and maladaptive reactions in persons with terminal illness. Initial findings indicated support for item–domain content validity via use of an expert panel and good internal consistency (α = .812; αstratified = .861) of the hypothesized three-factor model of adaptive and maladaptive responses to terminal illness. Several limitations must be noted, however.
Only three of the six expert panelists provided responses to the content validity exercise. However, experts provided qualitative feedback that helped shape final item revisions and initial domain restructuring. Suboptimal purposive sampling via agency ListServs led to reduced response rates. It is possible that respondents who completed the survey, therefore, may be different than those who declined to participate. Nearly 13% (n = 51) potential participants were lost by the final screening of the consent process indicating concerns with the stringency of language. The IRB indicated strong support of the specific wording used in the application because of its thorough assessment of informed consent. However, this assurance of participant informed consent and awareness of risks and benefits resulted in a large loss of potential participants. As a result, only 196 of the 396 potential respondents who clicked on the survey link completed the novel HPPG.
Subscale and global HPPG alphas remained strong throughout initial reliability analyses and item removal, CFA, and subsequent reliability analyses. Despite final revisions yielding desired results for 4 of 5 goodness-of-fit indexes, 11 path revisions and nearly 40 error covariances were used to modify the first CFA model. This may indicate correlation with an additional latent variable that was not contained within the model (Abell et al., 2009) or may point toward the use of a higher order CFA in future studies. Capitalizing on parametrization can be understood as enhancing statistical fit at the potential cost of substantive fit. However, path revisions and error covariance were allowed only upon assuring conceptual alignment with domain definitions (i.e., item–domain fit).
The post-CFA domain restructuring created concerns related to stem and item alignment. For instance, the initial affective item, “terminal patients may feel pleased when loved ones visit” appeared as “terminal patients may think pleased when loved ones visit.” Necessary grammatical revisions would need to be made prior to a subsequent validation. Importantly, many of these interdomain revisions were recommended by expert panelists in early stages of content validity, thus reinforcing the ongoing debate of subscale and subsequent item correlation. It must also be mentioned that items contained within the affective domain of the final HPPG scale included only reverse-scored items as a result of post-CFA domain restructuring. This may be as a result of the similar descriptors contained within these items (e.g., “persistent,” “prolonged”).
Variability in respondents’ true scores is a concern, as confidence intervals established by SEM values were larger than the acceptable value. In particular, the affective and behavioral domains had high SEM values as a result of the increased variability associated with responses to these items. This further reinforces the challenges noted by previous researchers and practitioners regarding the ease of differentiating persons’ reactions to terminal illness. This may prove problematic if administrators of the HPPG are seeking smaller ranges of true scores for assessment and training purposes. An additional psychometric limitation emerged upon examining the correlation between the cognitive domain subscale and global HPPG (r = .927, p < .01). This very strong, positive relationship may indicate that the cognitive subscale and global HPPG are measuring the same construct.
Indicators of convergent construct validity failed to support the a priori hypothesis. However, variables chosen to examine discriminant construct validity (i.e., race, sex) proved successful as neither emerged as significant correlates with respondent global HPPG scores. Additional efforts will need to be made to establish convergent construct validity, as palliative care self-efficacy did not correlate with global HPPG scores as hypothesized. This result may be sample-driven, a reflection of proposed relationships among the constructs in question, or a product of the post-CFA item–domain restructuring.
The HPPG is a self-assessment tool aimed at highlighting hospice professionals’ ability to differentiate among persons’ adaptive and maladaptive reactions to terminal illness. The measure can provide a framework for both practice and research. Use of the HPPG in hospice and palliative end-of-life care agencies can enhance practitioner awareness of various responses to terminal illness and set the stage for increased thanatological education for professionals and, subsequently, the reduction of the interrater perception gap. As previously noted, wide variability in grief reactions ought to be explored to assure adequate assessment and subsequent patient intervention (McKiernan et al., 2013; Pickard & Knight, 2005). Hospice professionals’ appropriate intervention, in turn, increases the ability to maintain patient QoL. Further, the HPPG is the first measure aimed at examining professionals’ ability to differentiate between persons’ adaptive and maladaptive reactions to terminal illness. Respondent scores closest to 5 reflect an increased ability to distinguish responses to terminal illness accurately. Lower scores, in contrast, indicate a decreased ability to distinguish responses to terminal illness accurately. As a result, the measure can be used to establish a knowledge base regarding the potential relationship between the professional characteristic of understanding preparatory grief, adaptive, and maladaptive reactions to terminal illness and the interrater perception gap in end-of-life care.
Findings from the initial validation of the HPPG predicate the need for subsequent validation with a larger, more representative sample of hospice professionals using the final instrument. Revisions to consent language will also assure increased response rates. Increased efforts to identify appropriate measures to establish convergent construct validity will also be necessary as will future factor analyses that examine the influence of additional latent constructs.
Footnotes
Acknowledgments
The author would like to thank the teams at the Florida Hospice and Palliative Care Association and the Louisiana-Mississippi Hospice and Palliative Care Organization and Neil Abell, PhD for their support and helpful feedback throughout the study process.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.