
Abstract
Objectives:
This study aims to investigate the effects of the Thank you–Sorry–Love (TSL®) program on posttraumatic growth (PTG) and cortisol level in parents of children with cancer.
Methods:
A total of 15 mothers of children with cancer were randomly assigned to the experimental group (n = 7) with the TSL intervention or a control group (n = 8) without any intervention. PTG and cortisol level were checked 3 times at the pretest, posttest, and 10-week follow-up.
Results:
PTG scores were significantly different between the two groups at the posttest and the follow-up test. Cortisol level was only significantly different between the two groups at the posttest.
Conclusions:
The TSL program may be a possible intervention for parents of children with cancer.
The 5-year survival rate of childhood cancer in South Korea has rapidly increased from 54.6% in the 1990s to 76.9% in the 2010s (Korea Central Cancer Registry, 2012). This rate is not appreciably lower than the 5-year survival rate in the United States, which is 83.1% (Howlader et al., 2012). Due to the recent increase in this survival rate, childhood cancer is considered a chronic illness requiring long-term support from family members (M. A. Kim & Yi, 2012).
Childhood cancer is a life-threatening illness that influences posttraumatic stress reactions not only in children with cancer but also in their parents (Pai et al., 2007). However, results of studies on the effects of childhood cancer on families are not consistent. Some studies focused on the negative influences of childhood cancer such as more conflicts between parents and a higher rate of divorce compared to healthy groups (Madan-Swain, Brown, Sexson, & Baldwin, 1994; Morris et al., 1997). In contrast, some studies have demonstrated that the psychological functions and family interactions of childhood cancer families are not significantly inferior compared to healthy controls (Greenberg, Kazak, & Meadows, 1989; Radcliffe, Bennett, Kazak, Foley, & Phillips, 1996).
Of particular interest, some studies have focused on paradoxical changes in families related to childhood cancer experiences, that is, posttraumatic growth (PTG; Barakat, Alderfer, & Kazak, 2006). PTG is defined as “the experience of positive change that occurs as a result of the struggle with highly challenging life crises” (Tedeschi & Calhoun, 2004, p. 1), which includes changes in self-perception, interpersonal relationships, and spiritual aspects (Tedeschi & Calhoun, 1995). Families facing childhood cancer find meaning and benefits from adverse experiences of cancer (Calhoun & Tedeschi, 1998). Some also find a sense of spiritual completeness regardless of their religiosity (Eiser & Havermans, 1994; Kupst et al., 1995). Childhood cancer possibly has a “silver lining” for families (Kazak et al., 2007, p. 1106), which means paradoxical growth in spite of challenges of cancer experiences.
A positive perspective on traumatic experiences is criticized for several reasons, including the possibility of victim blaming and the poor effectiveness of interventions based on adopting a positive perspective toward severe trauma (Peterson, 2006). For instance, people who experience problems after adverse life experiences may be considered to be “losers.” A positive perspective does not ascribe maladaptation to individuals facing suffering. Rather, a positive perspective is based on humanistic trust in the growth and changes in people (Seligman, Steen, Park, & Peterson, 2005). Moreover, interventions with a positive approach are effective in people with nonclinical problems as well as those with clinical depression (Sin, Porta, & Lyubomirsky, 2011). Recently, positive approaches have been shown to be effective in people with childhood cancer (Kazak et al., 1999; Pai & Kazak, 2006).
The Thank you–Sorry–Love (TSL®) family program is based on employing positive assumptions against challenges in life (H. J. Kim, 2012). The TSL family program was developed in Korea and aims to promote basic and essential positive interactions between family members, such as “Thank you,” “Sorry,” and “Love.” Culturally, Korean people are reluctant to express deep emotions to their family members. In spite of the usefulness of family interventions introduced from Western countries, changes begin with the expression of emotions. According to recent studies, the TSL family program is effective not only in terms of psychosocial adjustment but also in physiological reactions such as total antioxidant capacity and cortisol level (J. Y. Kim, Kim, & Nam, 2012). The TSL family program has been found to be effective in retired elderly men (J. Y. Kim et al., 2012), middle-aged women (H. J. Song, 2012), North Korean refugee women in South Korea (H. J. Kim, 2012), and adolescent victims of parental intimate partner violence (K. Y. Lee, 2013).
We believe that the TSL family program may possibly promote PTG. Interventions that aim to promote the expression of positive emotions, such as appreciation or blessings, have been shown to be effective (Jim & Jacobsen, 2008; Stanton et al., 2002). The first part of TSL, Thank you, is closely connected to flourish training in applied positive psychology (Peterson, 2006). The experimental group, who wrote down blessings in their daily life, exhibited more improvement in their quality of life than the comparison group, who wrote down problems or the control group, without any intervention (Emmons & McCullough, 2003). The second part of TSL, Sorry, originates from the intention to care and sympathize with others and evidence that sincere apologies can reduce suffering (Zechmeister, Garcia, Romero, & Vas, 2004). The last part of TSL, Love, is defined by “the expansion of the self” (Aron & Aron, 1996, p. 56). Love, and the concept of self-expansion, has a thread of connection with the PTG experience. Relational changes with others in PTG experiences can be interpreted as self-expansion.
Furthermore, the TSL intervention may alter the client’s cortisol level. The TSL intervention to improve PTG may be beneficial to improve hypothalamic–pituitary–adrenal (HPA) axis functioning. Traumatic events, such as receiving a cancer diagnosis, are mediated by the limbic system, which has a close relationship with the autonomic nervous system (ANS) in coping with traumatic stress. The ANS responds to stress by altering the hypothalamus to stimulate the pituitary gland to excrete adrenocorticotropic hormone (ACTH). The ACTH stimulates the adrenal glands to excrete cortisol (Rothschild, 2000). Hypersecretion of cortisol has immunosuppressive effects, resulting in the downregulation of the immune system (Andersen, Kiecolt-Glaser, & Glaser, 1994). The hypersecretion of cortisol is commonly observed among people with chronic stress exposures such as caregiving of children with chronic illness (Bella, Garcia, & Spadari-Bratfisch, 2011) or cancer diagnosis and treatment (Cruess et al., 2000). The relations between psychosocial intervention and biological changes have been studied during recent decades. Exposure therapy for people with phobic anxiety has been shown to affect endocrine and cardiovascular responses including cortisol level (Nesse et al., 1985). Recently, studies found that interventions for PTG are beneficial for HPA axis functioning. A cognitive–behavioral stress management intervention, which aims to improve the PTG of women being treated for breast cancer, has been shown to reduce serum cortisol (Cruess et al., 2000). A mindfulness-based stress reduction program has also been shown to significantly decrease the cortisol levels of women with breast cancer (Carlson, Speca, Patel, & Goodey, 2004).
Method
Participant Characteristics
Eligible participants were mothers who had experience caring for children diagnosed with cancer in the previous 5 years. We selectively recruited mothers due to the concentration of child care among women in Korea, which is one of the highest ranked countries with regard to gender gap in time spent in unpaid work, such as child care among Organization for Economic Cooperation and Development (OECD) countries (OECD, 2015). Mothers tend to spend more time to care for their children with cancer than do their spouses, which means that the experiences of caring for children with cancer are not gender neutral in Korea (J. Y. Song & Lee, 2010). PTG is experienced not only at the time of off-treatment as well as at the time of diagnosis (McFarland & Alvaro, 2000); we included mothers of children during the on-treatment period of cancer treatment.
Regarding the demographic characteristics of the participants, all participants were mothers of children with cancer. The age of participants ranged from 33 to 42 years (M = 37.28 years, SD = 3.99 years) in the experimental group and from 32 to 45 years (M = 38.63 years, SD = 3.85 years) in the control group. There were two (28.57%) male and five (71.43%) female children with cancer in the experimental group. There were three (37.50%) male and five (62.50%) female children with cancer in the control group. In the experimental group, six (85.71%) children were diagnosed with leukemia and one (14.29%) child was diagnosed with another type of cancer. Likewise, in the control group, five (62.50%) children were diagnosed with leukemia, one (12.50%) was diagnosed with a CNS tumor, and two (25.00%) were diagnosed with another type of cancer. A total of four (57.1%) children in the experimental group and four (50.0%) children in the control group were in treatment at the start of the program (Table 1).
Demographic Characteristics of Participants.

aNon-Hodgkin’s lymphoma, Langerhans cell histiocytosis, and Ewing’s sarcoma.
Sampling Procedures
Due to the negative stigma related to cancer in Korea (M. A. Kim & Yi, 2012), it was difficult to recruit study participants. The TSL program requires relatively self-initiated attitudes among participants in performing tasks such as expressing gratitude toward their family. Therefore, we recruited voluntary participants through a nationwide childhood cancer advocacy organization and self-help groups through posting a recruitment announcement on an Internet website from January to February 2014. We obtained written informed consent from eligible participants. All participants were provided KRW 150,000 in cash, approximately valued at $150, as a reward for participation. The study was approved by the institutional review board of Yonsei University (201310-SB-126-03).
Sample Size
Prior to recruiting participants, we conducted a power analysis to estimate sample size in consideration of the F tests with a medium-to-large estimated effect size (ES), based on the previous TSL intervention studies (e.g., H. J. Kim, 2012; J. Y. Kim et al., 2012; K. Y. Lee, 2013; H. J. Song, 2013), statistical significance, 80% power, and the number of groups. The estimated total sample size ranged from 12 to 22. Sample size was determined based on comprehensive consideration of the estimated sample size as well as the relations of group size and dynamics and the possibility of dropout.
Measures
In order to identify the effects of the TSL family program for parents of children with cancer, we used self-reported measurement as well as a biological marker. The effects on PTG and cortisol were measured. In order to determine the effects of the TSL family program on PTG, we used the Korean version of the Posttraumatic Growth Inventory (K-PTGI; S.-H. Song, Lee, Park, & Kim, 2009). The PTGI (Tedeschi & Calhoun, 1996) was previously translated to Korean as well as validated and reliability tested with a Korean population (S.-H. Song et al., 2009). The K-PTGI contains 21 items and employs a 5-point scale. Higher scores suggest a higher level of PTG; therefore, higher scores on post- and follow-up tests suggest the effectiveness of intervention. The K-PTGI includes five subscales: relating to others, new possibilities, personal strength, appreciation of life (AL), and spiritual change. The internal consistency was excellent in this study, with a Cronbach’s α of .89. Participant cortisol level was examined with blood samples taken at the pre-, post-, and follow-up tests. The recommended test time is within an hour of awakening (Chida & Steptoe, 2009). It was difficult to follow this recommendation; thus, we collected blood samples at 10:00 a.m. In order to control for other extraneous factors, such as diet or health supplements, participants fasted for 12 hours. The reference blood cortisol level used was 6.2–19.4 ml/dl (Chida & Steptoe, 2009).
Research Design
We conducted a two-group randomized experimental design with preintervention, postintervention, and follow-up testing on all participants. Participants were assigned to two groups with matching and randomization methods to promote the internal validity of the study. At the first step, we used a quota matrix by three cancer types (leukemia, CNS tumor, and other) due to the importance of the effects of cancer types on psychosocial outcomes (Zebrack et al., 2004). At the second step, we randomly assigned participants to two groups in each quota. The assignment process was conducted with the informed consent of all participants. Participants in the experimental group underwent the TSL family program intervention. Participants in the control group received no intervention. We included a randomly assigned nonintervention control group in order to minimize threats to internal validity due to the maturation of participants or testing effects. Participants of both groups were exposed to their social environment, such as contact with peers or physicians, without any manipulation. We only added the TSL intervention to the experimental group. The TSL family program was provided over 12 sessions from April 1 to June 24, 2014. The TSL intervention sessions were held in a group program room provided by a childhood cancer support organization accessible to participants and led by a trained social worker with more than 7 years of practical experience with people facing childhood cancer. Each session was about 90 min in length. The effects of the TSL program were tested with self-reported questionnaires and blood tests on three occasions: pretest (1 week before the start of the group program), posttest (1 week after the end of the group program), and follow-up test (10 weeks after the end of the group program).
Intervention: TSL Family Program for Parents of Children With Cancer
The TSL family program promotes positive expression, including appreciation (Thank you), sympathetic and empathetic feeling (Sorry), and love between family members (Love; J. Y. Kim et al., 2012). Originally, the TSL family program consisted of 14 sessions, including 6 sessions on the Thank you section, 4 sessions on the Sorry section, and 4 sessions on the Love section. However, the TSL family program for improving PTG of parents of children with cancer required revised to be appropriate. We revised the TSL from 14 sessions into 12 sessions because of concerns regarding child health status. Due to the importance of finding appreciation for life and family and expressing emotions, the 12 sessions included 6 sessions of Thank you, 3 sessions of Sorry, and 3 sessions of Love.
The Thank you section, the first part of the TSL family program for parents of children with cancer, was intensified. One half of the sessions were focused on dealing with the emotions of AL among in children and their families. The emotion of gratitude is defined as “a warm sense of appreciation for somebody or something, a sense of goodwill toward that person or thing, and a disposition to act that flows from appreciation and good will” (Fitzgerald, 1998, p. 120). In order to promote PTG, gratitude for life and family members is essential. Finding meaning and thriving during suffering can lead to personal growth and positive perceptions of one’s self (A. Lee Duckworth, Steen, & Seligman, 2005).
The Sorry section, the second part of the TSL program for parents of children with cancer, was revised in consideration of participants’ excessive guilt over their children’s disease. The original TSL program was designed to promote expression of regret for others’ pain in order to improve empathy. However, parents of children with cancer tend to consider their children’s disease their fault. Guilt is a natural defense mechanism used to cope with challenges in the face of traumatic events such as a child’s diagnosis of life-threatening illness (Li, Stroebe, Chan, & Chow, 2014); however, it may lead to psychopathologies (Tangney, Wagner, & Gramzow, 1992). Therefore, the second part of the TSL aims to relieve guilt.
The Love section, the last part of the TSL program for parents of children with cancer, was not modified. Due to the expansiveness of the concept of love from sexuality to spirituality, it is hard to study in behavioral science (Hendrick & Hendrick, 1986). The original TSL program considers love as a natural flowing process toward achieving appreciation (Thank you) and empathy (Sorry; J. Y. Kim, 2014). Loving is defined as expanding oneself (Aron & Aron, 1996). If we love others, we are able to see their difficulties through their perspective, not our perspective. Participants are encouraged to view life from their children’s perspective in the Love sessions. For example, some participants shared their experiences that they were reluctant to hang out with their children for appearance changes such as hair loss in order to protect their children through avoiding strangers’ eyes. Such protection may be less empathetic behavior, though it is based on love (Nam & Choi, 2013).
Statistical Methods
Independent sample t-tests between experimental and control groups and analysis of covariances (ANCOVAs) were used to check the homogeneity between groups. The pretest of PTG scores was not significantly different between the two groups, t(14) = −1.34, p >. 05. Additionally, the pretest levels of cortisol were not significantly different between the two groups, t(14) = .057, p > .05.
An ANCOVA was used to control for pretest scores in order to promote internal validity. Since it was found that the pretest scores of each participant were closely related to their posttest and follow-up test scores, pretest scores were used as control variables in posttest and follow-up test group comparisons. An ANCOVA was needed in the experimental design to satisfy two assumptions (Wickens & Keppel, 2004). First, the posttest and follow-up test scores should be linearly related to pretest scores. We examined the linearity in pretest–posttest and pretest–follow-up test scores of PTG and cortisol with scatter plots. Second, the regression slope of the interaction term between pretest scores and the group variable should be statistically equal. The interaction term of the pretest PTG score and group variable was not significant at the posttest, F(1, 10) = .01, p > .05, or the follow-up test, F(1, 8) = 1.31, p > .05. Additionally, the interaction term of the pretest cortisol level and group variable was not significant at the posttest, F(1, 8) = 2.58, p > .05, or the follow-up test, F(1, 6) = .73, p > .05. Therefore, two assumptions of ANCOVA were satisfied.
Results
Participant Flow
We recruited 19 voluntary participants and excluded 4 participants who did not meet the inclusion criteria. Therefore, 15 participants were enrolled. We assigned seven participants to the experimental group and eight participants to the control group. At the posttest, one participant in the experimental group declined to complete self-report survey, and two participants in the experimental group declined the blood test due to their children’s poor medical status. At the follow-up test, one participant in the experimental group and two participants in the control group declined to complete self-report survey, and two participants in the experimental group and three participants in the control group declined the blood test due to their children’s medical status and participants’ returning to work. The flow of participants is depicted in Figure 1.
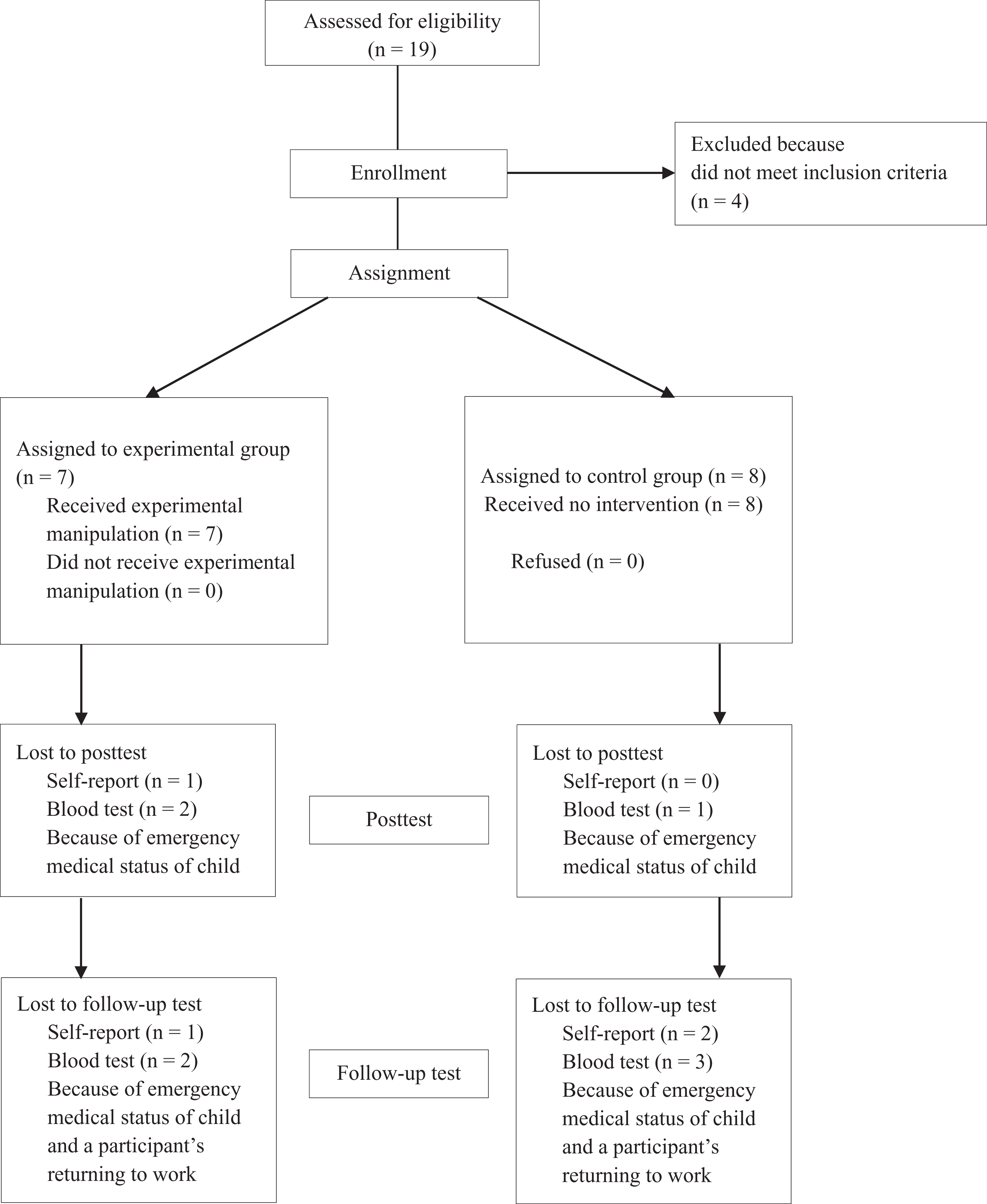
Flow of participants through each stage of the study.
PTG
The TSL program significantly improved PTG at the posttest and follow-up test. The group variable was significant in the ANCOVA model at the posttest, F(1, 11) = 9.39, p < .05, ES = .81, and the follow-up test, F(1, 9) = 7.39, p < .05, ES = 1.13, when controlling for pretest scores, which indicates significant between group differences at the posttest and follow-up test. In other words, the TSL intervention may improve the PTG level in the experimental group at the posttest and follow-up test (see Figure 2).
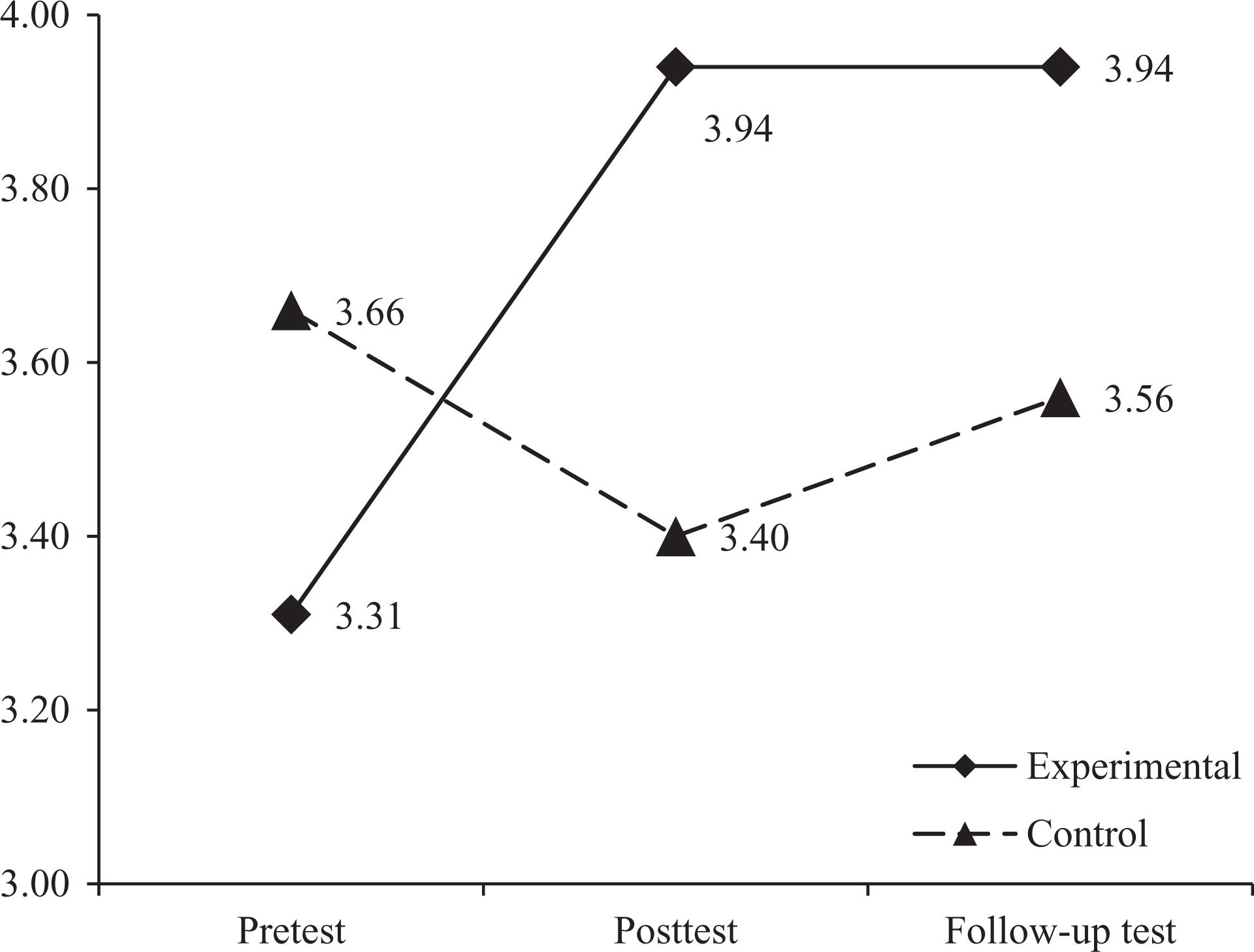
Changes in posttraumatic growth (PTG) scores.
Cortisol
The TSL program only affected cortisol level at the posttest, F (1, 9) = 3.50, p < .1, ES = .38; the effects of intervention were not maintained at the follow-up test, F(1, 7) = .49, p > .05, ES = .50. Cortisol level was marginally lower in the experimental group than in the control group at the posttest at a significance level of p < .10 when controlling for the pretest level of cortisol. The gap between the two groups narrowed at the follow-up test (see Figure 3). While the cortisol level of the experimental group was lower than that of the control group at the follow-up test, this difference was not statistically significant.

Changes in cortisol level (ml/dl).
Discussion and Applications to Practice
Several possible applications for social work practices for families experiencing childhood cancer are suggested in this study. The TSL program assumes that positive emotional interaction between family members allows them to find benefits and meanings in spite of the difficulties and challenges of cancer. This is consistent with the results of previous studies, which supported the effectiveness of positive emotional expression for PTG (Jim & Jacobsen, 2008; Stanton et al., 2002). Furthermore, the TSL program may influence the level of cortisol, a stress hormone. Biomarkers, including cortisol level, are less affected by extraneous validity threats such as social desirability or placebo effects (J. Y. Kim et al., 2012). The observed cortisol level changes may be explained by the positive correlation between physical and mental health improvement.
Intervention to find and express gratitude between family members is important to promote PTG for people affected by childhood cancer and may be a benchmark for social work programs for people affected by other types of cancer. Gratitude not only refers to the reactive feeling of receiving benefits but also the proactive feeling of finding benefits from one’s family. Despite the fact that parents of children with cancer suffer from enduring difficulties in cancer-related treatment and experiences, they paradoxically find gratitude for their children’s existence and support from family members. The TSL program begins with existential questions such as “Who am I?” (J. Y. Kim, 2014, p. 35) and “What do you suffer if your family does not exist?” (J. Y. Kim, 2014, p. 50). These methods aim to achieve the emotional disclosure of suffering from their children’s cancer experiences as well as reevaluation of their existence. The concept of PTG includes existential reevaluation (Hefferon, Grealy, & Mutrie, 2009). Interventions to promote PTG include emotional disclosure (Jim & Jacobsen, 2008). Finding and expressing gratitude do not exhaust emotional resources but reciprocally share energy to cope with difficulties and help to build the solid foundations of a durable family (J. Y. Kim, 2014). The TSL program may be a potential intervention to promote PTG in the setting of advocacy or self-help groups of people with childhood cancer—as well as social work in health care—due to the simplicity of the TSL program, which requires relatively little complicated knowledge or skill to apply.
Social work interventions that result in positive psychosocial changes could potentially lead to improvement in physical health, based on the results of this study. Similar to previous studies on the effectiveness of the TSL program for other populations (H. J. Kim, 2012; J. Y. Kim et al., 2012; K. Y. Lee, 2013), the TSL program may have positive effects on PTG as well as cortisol level for parents of children with cancer. The mechanisms of HPA axis responses to stress experiences have been studied, and results suggest that interventions for PTG are beneficial to HPA axis functioning (Carlson, Speca, Patel & Goodey, 2004; Cruess et al., 2000); the results of this study may also indicate a correlation between PTG and physical health improvement. Similarly, positive emotional changes have been shown to improve immunity and survival rates of patients with hepatocellular carcinoma (Dunigan, Carr, & Steel, 2007; Rasmussen, Scheier, & Greenhouse, 2009). Psychosocial interventions to improve PTG, such as the TSL program, might possibly improve physical health as well, based on this study.
Small sample size due to the negative stigma attached to cancer in Korea (M. A. Kim & Yi, 2012), high rates of dropout due to inevitable medical emergencies, and difficulties in obtaining the cortisol at the recommended test time may be possible limitations with regard to external and internal validities, which should be remedied in future studies. Although similar events, such as recurrence of cancer or emergency room visits, occurred in the experimental group as well as in the control group, it is difficult to determine whether these events equally affected outcomes in the two groups.
Despite the limitations of this study, psychosocial intervention that emphasizes family-based and positive reappraisal of cancer experiences, such as the TSL program, is a possible approach for improving the quality of life of families affected by cancer. Cancer experiences are shared and appraised collectively by family members; therefore cancer is considered a family affair (Ben-Zur, Gilbar, & Lev, 2001). Collective reappraisal of stress events in family members may possibly be a key to stress coping (Berg, Meegan, & Deviney, 1998). Therefore, the TSL program can be an effective social work program to improve PTG in those with a similar family cultural background. The TSL program is based on the Korean cultural context, in which emotional disclosure between family members is uncommon. Furthermore, the target population of this study was parents of children with cancer; however, the TSL program may be a valid benchmark for people of other ages with cancer.
Footnotes
Author’s Note
This study was recomposed by using a part of Kwonho Choi's doctoral dissertation in 2015.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the financial support of Yonsei University Future-leading Research Initiative of 2014 (RMS2 2014-22-0119) and the Brain Korea 21 Plus (BK21plus) Program (Social Welfare Education with Glocalization, Creativity, and Convergence against New Social Risks) from the School of Social Welfare, Yonsei University.