
Abstract
Purpose:
Bivariate and logistics regression analyses were conducted to examine the effectiveness of child welfare agencies’ Family Group Decision-Making (FGDM) practices focused on strengthening families and positive outcomes for children. This study evaluates one mid-Atlantic state’s implementation of a FGDM called family involvement meetings (FIMs) to improve family strengths and their active engagement in the service planning process.
Methods:
Through use of a FIM Feedback Survey, participants provided satisfaction feedback on the general FIM process and what factors are associated with their satisfaction and decision-making at the meeting.
Results:
Multiple factors of participant’s engagement, incorporating family strengths, and the FIM facilitator’s knowledge and skills had significant impacts on the participant’s decision-making and overall FIM satisfaction score.
Discussion:
This study will contribute to examining FGDM facilitators’ practices and effective outcomes of FIMs to improve the well-being, safety, and permanency outcomes for children and their families.
Under the Children and Family Services Review conducted by the Children’s Bureau, the outcomes of safety, permanency, and well-being are intended to increase states’ child welfare systems ability to help children and families and to shift practices toward a family-centered practice (FCP) approach (U.S. Department of Health and Human Services [USDHHS], 2010). FCP is a framework that prioritizes family strengths, perspectives, and input to guide successful change and treatment (Allen & Petr, 1998; Craft-Rosenberg, Kelley, & Schnoll, 2006), and the Children’s Bureau has identified the Family Group Decision-Making (FGDM) practice as a key principal of the FCP model (USDHHS, 2010). The purpose of the FGDM meeting is to gather all family members and professionals involved with the case together to have an open conversation about the child and family’s current situation and to make decisions of the steps needed to reach their well-being, permanency, and safety goals (Berzin et al., 2008). Many states have implemented the FGDM model, or similar models, in order to shift the focus of the services from the individual child to incorporate the whole family (Berzin, 2006), and to empower the youth, family members, and other community partners to work together on the family’s service plans to promote a healthy family unit. Through this process, the family’s needs and strengths are identified and are used to help decide the best treatment and placement options for the child and family (Crea & Berzin, 2009). In order to examine the positive impact that the FGDM model has on both the child and family’s needs and outcomes, it is important to examine both the family and nonfamily members’ level of engagement (Rockhill & Rogers, 1999). In addition, examining the participant’s perspective of the overall process can contribute to examining the effects of the family’s FGDM involvement and satisfaction on both the child and family’s outcomes.
The purpose of this study is to examine all participants’ overall satisfaction with the FGDM and what characteristics are associated with their satisfaction and decision-making at the meeting in one mid-Atlantic state. This study is the first to use a statewide large participant sample to examine participants’ satisfaction with the meeting, facilitator, and the decision-making process since the state implemented the FGDM process. This study also examines the FGDM facilitator’s role in the participant’s experience of the FGDM. Results from the study will contribute to providing important implications for social work practice and policy related to the FCP model and FGDM practice. This study will also provide implications for training and involvement of facilitators in the FGDM process.
Contexts of FGDM and Its Impacts on Child Welfare Practices and Outcomes
Framework of the FGDM model
In 1989, New Zealand passed the New Zealand Children, Young Person and their Families Act, which required family group conferencing be used as an inclusive, decision-making process for juvenile delinquents and child welfare cases (Levine, 2000). During that same time frame, in the United States, the FGDM practice first began in the 1990s and similarly was implemented to address the disparities and disproportionality needs of family being provided child welfare services (American Humane Association, 2010). Currently being implemented throughout multiple states using a variety of names, the FDGM model incorporates the same core aspects in order to achieve a family-centered approached to identifying and addressing the child and family’s needs.
The FGDM process examines three different aspects of the family and child dynamics during the course of the meeting. The first topic discussed is the reasons or issues that brought the child and family to work with the child welfare agency. After looking at the leading concerns of the family and child, the FGDM group looks to examine the strengths of the family and child. By identifying the family and child’s strengths, the group is able to determine the level of need of supports and services for the child and family to help ensure safety and well-being of both (Berzin et al., 2008). These FDGM characteristics follow the recent child welfare practice trends that child welfare agencies are increasing their FCP and strength-based approaches when working with the families and children they serve (Weigensberg, Barth, & Guo, 2009).
Along with these pertinent characteristics of the FGDM process, there are also several different principles which must be taken into consideration during the FGDM process. These principles include careful consideration and respect toward the family and child’s culture and community (Maluccio & Daly, 2000; McDonald & Associates, 2000; Moore & Mc-Donald, 2000; Pennell & Burford, 1994; Ryburn, 1993); allowing the child’s opinion and thoughts to be heard (Doolan & Phillips, 2000; Hassall, 1996; Immarigeon, 1996; Maluccio & Daly, 2000; Moore & McDonald, 2000; Pennell & Burford, 1994); empowerment of the family and child (Ban, 1996; Maluccio & Daly, 2000; McDonald & Associates, 2000; Moore & McDonald, 2000; Ryburn, 1993); partnership of the families, community members, and child welfare agencies working together to formulate a service plan (Ban, 1996; Graber, Keys, & White, 1996; Hassall, 1996; Maluccio & Daly, 2000; Pennell & Burford, 1994); and exploring and expanding family and community resources and supports (Ban, 1996; Graber et al., 1996; Maluccio & Daly, 2000; McDonald & Associates, 2000). While many agencies have used variations of the FGDM process, the same core characteristics and principles remain constant in order to help empower and strengthen the families and children served (Berzin et al., 2008). Therefore, a thorough evaluation of the FGDM practice is important in order to examine the effectiveness of these core components and characteristics on the participants’ satisfaction, engagement, and outcomes.
Based on the FGDM framework, a trained facilitator has various roles and responsibilities throughout the FGDM process. One main role is to coordinate the participation of all of the case’s participants and to ensure that a service plan is accurately developed and is assessing the family’s progress toward their goals. The facilitator also builds relationships and trust among the FGDM participants so that information can be shared honestly and openly in order to help develop a service plan to meet the family’s identified needs (American Humane Association, 2010). As an advocate for the family, the facilitator must also ensure that the family’s strengths and culture are acknowledged and respected (American Humane Association, 2010). When challenges and issues do arise during the meeting, the facilitator acts as a mediator to share the identified needs and brainstorm possible solutions. Another responsibility of the FGDM’s facilitator is to verify that all of the case’s information is shared between the child welfare agency, the family, and other stakeholders and that all participants clearly understand their roles in the service plan (American Humane Association, 2010). Lastly, the facilitator must ensure the integrity of the FGDM process to the FCP model to ensure that every family is receiving the appropriate child welfare services needed to reach their goals (American Humane Association, 2010).
Implementation of the FGDM model
In 2006, one mid-Atlantic state shifted their child welfare practices toward the FCP framework. During this process, the state’s child welfare agency implemented the FGDM practice, known as family involvement meetings (FIMs) across all of the state’s jurisdictions. The state’s FIM policy proposed that FIMs should be conducted at important decision-making points in the family and child’s case in order to assess the needs and develop a service plan for the family that provides the safest and least restrictive placement for the child(ren) involved (Maryland Department of Human Resources [MD DHR], 2009b). These significant points are known as “trigger events” and are identified by the child welfare worker managing the case. The state’s FIM triggers include when a child is removed from the family (removal FIM), a change in the permanency plan (permanency plan FIM), changes occur to a child’s placement (placement change FIM), a youth begins the transition to adulthood (youth transition FIM), when a youth is voluntarily placed in care (Voluntary Placement Agreement [VPA] FIM), and other types of FIMs which occur occasionally based on the specific needs of the case. For all trigger events, all members of the case should be invited to participate in the FIM process. Along with this collaboration, the FIM process looks to engage the family through a strengths-based approach which focuses on the family’s core unit of strengths and supports to lead to successful treatment and change (Department of Human Resources, 2009a). In cases that transportation is a barrier for family members, many jurisdictions are using technology to help involve family participants so that all available family resources and supports can be identified and provide input as possible placements if needed to prevent a child’s removal from their family. Since the FIM has recently been implemented in the state, in an effort to understand outcomes and impacts of the FIM process, it is important to examine certain aspects of participants’ experiences during the FIM process. It is also necessary to examine all participants including families, caseworkers, supervisors, and service professionals’ feedback of the meeting and facilitators, to assess what factors have impacts on a participant’s decision-making ability and their agreement to the plan developed at the FIM. This study is the first to examine the outcomes and impacts of the FIMs in the state.
Previous Studies Regarding the Effects of FGDM on Child Welfare Practices and Outcomes
After a review of the research on the benefits of implementing the FGDM process, the results are very promising to revitalizing the child welfare programs and services. Results of a study conducted by Pennell (2006), analyzing 27 FGDM and 336 participants, indicated that mothers and maternal family members had a higher rate of participation in the FGDM meetings than fathers (Pennell, 2006). Since one of the crucial aspects of the FGDM process is family collaboration, this study shows that one side of the family is not as involved as it could be, therefore, the FGDM model could be leaving out valuable input, resources, and supports from the child and family’s service plan. Another finding was that over half of the sample were able to voice their opinions during the meeting which shows that this process is giving an opportunity to have not only professionals but the families and children voice their opinion as well (Pennell, 2006). This is a shift in practice for many child welfare agencies and is beneficial for empowering families and children to reach their service plan objectives.
Other research studies conducted on the FGDM process examine the process’s effectiveness based on the participant’s satisfaction and evaluations. In Oregon, an exploratory study of a mixed sampling of 26 family unity meetings held between January 1998 and March 1999 collected 163 different participant’s perspectives and experiences using qualitative methods (Rockhill & Rodgers, 1999). The results showed that family’s satisfaction and involvement in the FGDM process was higher when there was sufficient preparation of the meeting, a greater number of family members in attendance, a clear goal and meeting purpose, a conversation about the family’s strengths, adequate time, efficient time management, good facilitation, and use of the meeting (Rockhill & Rodgers, 1999). Based on these results, the FGDM process can in fact have a positive influence on the family’s engagement with the service plan which could potentially lead to better child’s well-being, safety, and permanency outcomes but more research needs to be done on a larger sampling of participants and over a longer period of time to determine what level of participation and support needs to be given by the participants in order for positive effects on their engagement to occur.
Child welfare agencies are also looking to help keep children in a family environment and divert them from entering the foster care system altogether. Through the FGDM process, family, community, and professional participants discuss the best placement options for the child (Crea, Crampton, Abramson-Madden, & Usher, 2008). A study conducted by Crampton and Jackson (2007), a multiple, nonequivalent comparison group design was used to examine the FGDM model’s implementation effect on 257 family cases with the intention that the FGDM process would help to reduce the racial disproportionality among families’ experience with the child welfare system. The results indicated that the children who had a FGDM meeting remained outside of the child welfare system more often than those who did not have a FGDM meeting at all. Those who were not placed in the child welfare system were most likely placed with a relative resource. This study indicates the shift of child welfare agencies’ focus from child to family and the practice to use all resources and supports to prevent the child from entering into out of home care. In addition to diversions, multiple outcome-based research studies conducted have also found other benefits of FGDM meetings to include: reduction of reoccurrence of maltreatment, decreased involvement with child protective services, and an increase in placements with relatives (Crampton, 2003; Crampton & Jackson, 2007; Pennell & Burford, 2000; Sundell & Vinnerljung, 2004).
Since the positive outcomes and effects of the FGDM process can be influenced by various factors in the overall process, it would be imperative to examine the methods of implementing the FGDM model within the literature. One study investigated a northern Atlantic state’s implementation process of the FGDM model (Rauktis, Mcarthy, Krackhardt, & Cahalane, 2010). The results of the study showed that an agency’s culture and administration can place challenges on how effective new practices are when being implemented (Rauktis et al., 2010). Location, financial support, committed staff, and the agency’s practice approach are all factors which can influence the FGDM process (Rauktis et al., 2010). Leadership is necessary throughout the entire implementation process of FGDM since caseworker’s attitudes can be one of the most significant challenges an agency has when implementing this new practice (Rauktis et al., 2010). Since the FGDM process can be beneficial to the agency’s child and family outcomes, it is imperative to examine the implementation process to ensure that the practice has fidelity to the FGDM model and that the positive benefits can be seen by the child welfare agency as well as the children and families in the community.
After examining the research of the FGDM process, there are still research gaps which need to be investigated in order to receive a comprehensive understanding of the implications of the FGDM process on the children and families receiving child welfare services. The long-term outcomes of the child and families who were a part of the FGDM process is one area lacking appropriate research (Wang et al., 2012). While there is limited research on the long-term outcomes, some research studies have used the participant’s perspectives or experiences about the FGDM process in both qualitative and quantitative methods in order to see the impact of the FGDM model on the child and family (Rockhill & Rodgers, 1999). Multiple research studies have surveyed the participant’s satisfaction of the FGDM process but only on very small samples of the populations. There is also a research gap in evaluating the facilitator’s role on the participant’s level of satisfaction and engagement in the FGDM process. Therefore, there is a need to conduct research using larger sampling of the participant population in addition to examining the participant’s satisfaction of the FGDM facilitator. To develop a more comprehensive understanding of the FGDM process in the literature, this study will analyze both the level of satisfaction of the FIM (state’s FGDM process) participant on the overall process and also on the FIM’s facilitator among a large sampling of participants.
The contribution of this study is that it addresses these research gaps in the FGDM practice. First, unlike in previous studies, this study examines satisfaction level of a larger size sample which includes a variety of participants using feedback survey data collected for the FIMs. Through a statewide analysis of the FGDM survey, this study provides a unique insight on how effective the State is in implementing the FGDM practice for various families and children with a variety of needs and goals. Secondly, unlike previous FGDM research, this study’s sample includes not just family and youth, but all participants including social workers and other professionals to provide comprehensive feedback. The participants in this study includes family members, youth, child welfare agency caseworkers, child welfare agency supervisors, community services providers, legal representatives, educational professionals, and other service professionals. Lastly, this study also examines a large spectrum of participants’ perspectives of the FIM facilitators so that the impacts of facilitators’ practice on overall satisfaction with the meeting and decision-making outcomes can be determined unlike in previous research. This study is the first to examine the effects of FIM in the state so it can contribute to the implementation of more effective FDGM practices and provide significant implications and suggestions for policies and training of FGDM facilitators and social work professionals.
Method
Data Collection Process and Sample
This study examined participant’s satisfaction and outcomes of FIM through the use of the Feedback Survey. This study’s sample consists of a total of 78 FIMs with 618 participants across 9 different jurisdictions in one mid-Atlantic state from May 2013 until April 2014. The 78 FIMs surveyed included: 21 placement change FIMs, 16 other FIMs, 13 removal FIMs, 12 youth transition FIMs, 10 permanency change FIMs, 5 VPA FIMs, and 1 unidentified FIM type. The study’s entire sample was made up of participants who had attended the meeting and then were prompted to voluntarily complete a survey. The survey was also translated and available in Spanish for a portion of the surveying population who spoke Spanish. Of the 618 total FIM participants, 461 participants completed the Feedback Survey. This yielded a response rate of 75%. The sample included 461 participants of all ages whose role in the FIM included: the youth/child, parents including step or foster parents, other relatives, Department of Social Services (DSS) caseworker or supervisor, and other agency and community professionals (i.e., attorney, school representatives, etc.). Table 1 shows the survey participants’ relationship to the child. Nine participants did not identify their relationship to the child. Out of the 618 total participants, 157 chose not to respond to the survey.
Relationship of FIM Participants to Youth.
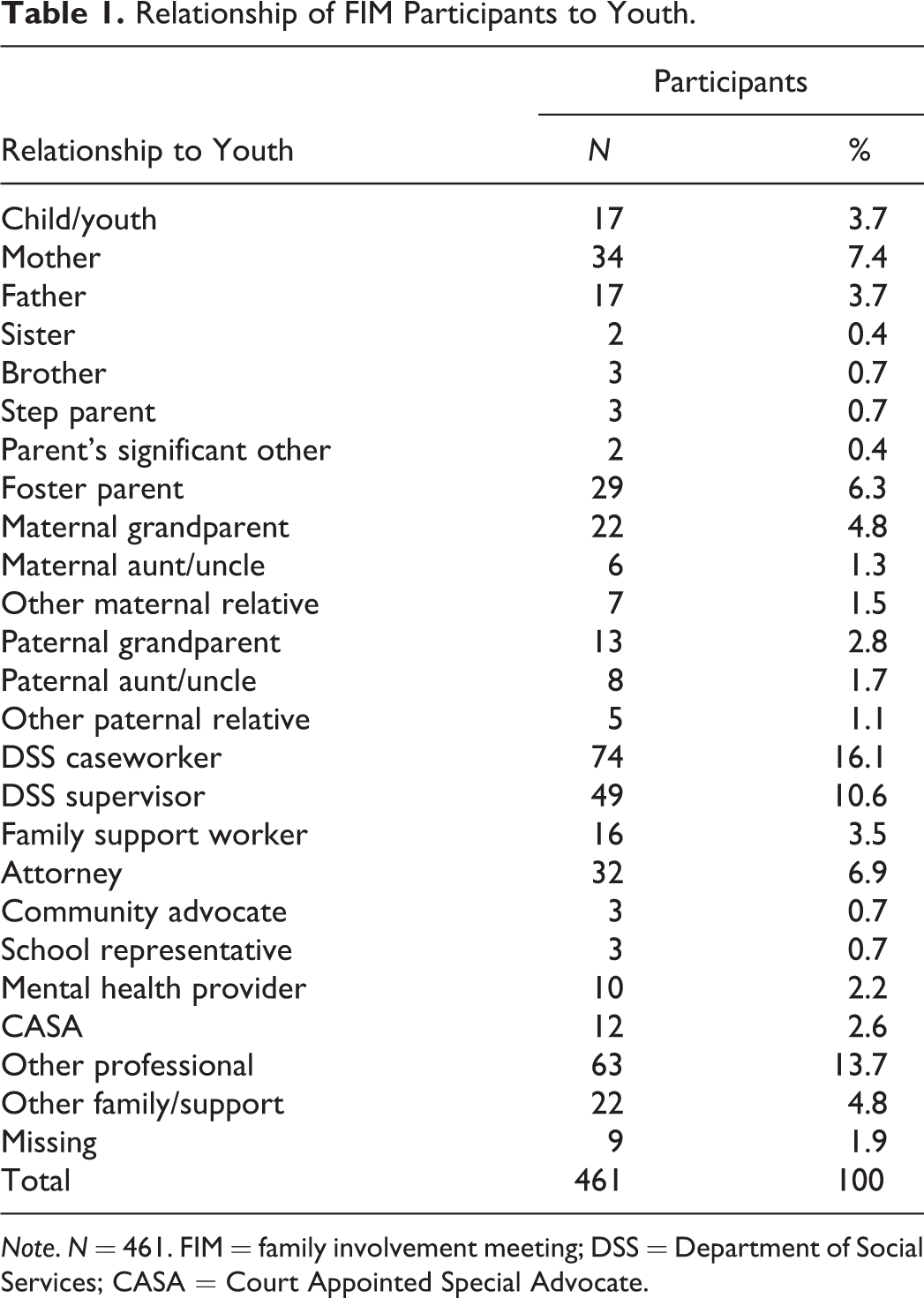
Note. N = 461. FIM = family involvement meeting; DSS = Department of Social Services; CASA = Court Appointed Special Advocate.
The study’s survey instrument was developed by collaboration between the state’s public child welfare agency and researchers from a university (University of Pittsburgh, School of Social Work Pennsylvania Child Welfare Training Program, 2008). This study and survey instrument was approved by the University’s Internal Review Board.
The state’s jurisdictions were requested to implement the FIM Feedback Survey for a certain period of time based on the state’s Quality Assurance Review schedule. Researchers implemented and trained local DSS’ FIM staff on the purpose, implementation, and collection of the FIM Feedback Survey and the FIM cover sheet.
Facilitators were asked to complete the FIM cover sheet to provide demographic information, purpose, and outcome questions about the case for which the FIM was held. On this cover sheet, the facilitator created a unique identification number so that the child’s name and identifying information would remain anonymous. This unique identification number was then placed on each survey distributed in order for the researcher to link the survey to the reason and outcome of the FIM.
All family members (youth, foster parents, family relatives, family supports, etc.) and all professional, nonfamily members (caseworkers, supervisors, community professionals, school representatives, attorneys, community advocates, etc.) are asked to complete the FIM Feedback Survey, in person at the conclusion of the FIM before leaving the meeting room. In order to remain anonymous, the participants placed their completed surveys in the standard envelope and sealed it before returning it to the facilitator. The participant’s completion of the survey was done voluntarily and anonymously. Once all surveys were collected, the facilitator placed them in an envelope and returned them to the university’s researchers.
Measurement and Analysis Model
The survey asked a series of questions eliciting participant’s feedback on different aspects of the FIM, including facilitator’s competency and professionalism, family or professional specific questions, and child welfare outcomes of safety, permanency, and well-being. Ratings were based on a Likert-type rating scale with 1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree.
Dependent variables
There are two dependent variables: (1) overall meeting satisfaction; it was measured by the sum of five variables that include children’s safety, agreement with the plan, plan’s effectiveness in helping the family to achieve goals, the plan addressing participants’ concerns, and the plan helping the family members address their issues that brought them to the meeting. The overall satisfaction is regarded as a continuous variable (ranging from 5 to 20), with high scores indicating the high satisfaction with the meeting; (2) decision-making at the meeting; it measured whether a decision was made at the meeting regarding the plan for the family and/or child receiving services, which is dichotomous, with 1 = yes, and 0 = no. Participants in this study were identified as everyone who participated in the FIM including youth, family members, welfare agency caseworkers, welfare agency supervisors, community service providers, educational providers, legal representatives, mental health providers, and other community service partners and providers.
Independent variables
To understand the determinants of the overall satisfaction with the meeting and whether a decision can be made at the meeting, we included three types of independent variables: (1) participants characteristics, which include gender and race; (2) meeting characteristics that includes participants’ understanding the purpose of the meeting, participants’ preparation for the meeting, everyone’s involvement in the meeting, being comfortable to express their ideas and opinions, having enough time to talk, feeling like part of the team, and building on the family’s strength; and (3) feedback on the facilitator’s skills that includes measuring their knowledge, respecting participants, remaining neutral, making participants feel comfortable, and managing time well. All the independent variables except gender and race are coded as dichotomous variables, with 1 = agree and 0 = disagree. For gender, male is coded as 1 and female as 0. For race, white is coded as 1 and other races as 0.
Bivariate analyses were conducted to examine differences between dependent variables and independent variables. Given multiple comparisons of the same indicators over a series of indicators for bivariate analysis, the α level was adjusted using Bonferroni. Multiple regression and logistic regression were conducted separately to examine factors associated with overall plan satisfaction and whether a decision was made at the meeting. Adjusted R 2 and pseudo R 2 were reported for these regressions. All the analyses were conducted using Stata 12.
Results
Characteristics of Participants
Based on the analysis of the sample population, 461 participants surveyed consisted of 17 youth, 173 family members, 262 professionals, and 9 participants did not identify their relationship to the youth. Table 2 summarizes the demographic information of all of the FIM participants who completed the survey. Of all the FIM participants who responded, 50% of participants were female and had a professional relationship to the FIM target child. For all family participants, about 66% were female, while 34% were male and 61% were White, followed by 31% of participants were African Americans and 0.6% identified as “Other” races. Out of the 17 youth participants, about 65% were female and 35% were male with 53% identified as White, 35% as African American, and 6% as Native American or Other. About 64% of all professional participants were White followed by 29% African American, 2% Other, and 1% Asian/Pacific Islander. Nearly 88% of professional participants were female while only 12% were male (1 (0.3%) professional participant identified themselves as transgender). The survey results showed that for all youth participants, only one participant (5.9%) had attended another FIM that month and the majority (64.7%) had not. For family participants, the majority (69.9%) had not attended another FIM that month, and about 3% had attended another FIM during that same month. In contrast to both the youth and family participants, 45.8% of professional participants had attended another FIM that month and 41.2% had not. The survey was designed to only ask professionals about their level of education and their years of practice in the field. Of all of the 262 professional participants, 15% had 2 or less years of experience and 16% had 25 or more years of experience in their professional career. For the professional participants in this sample, more than half had a graduate degree (54.2%).
Characteristics of the FIM Participants.
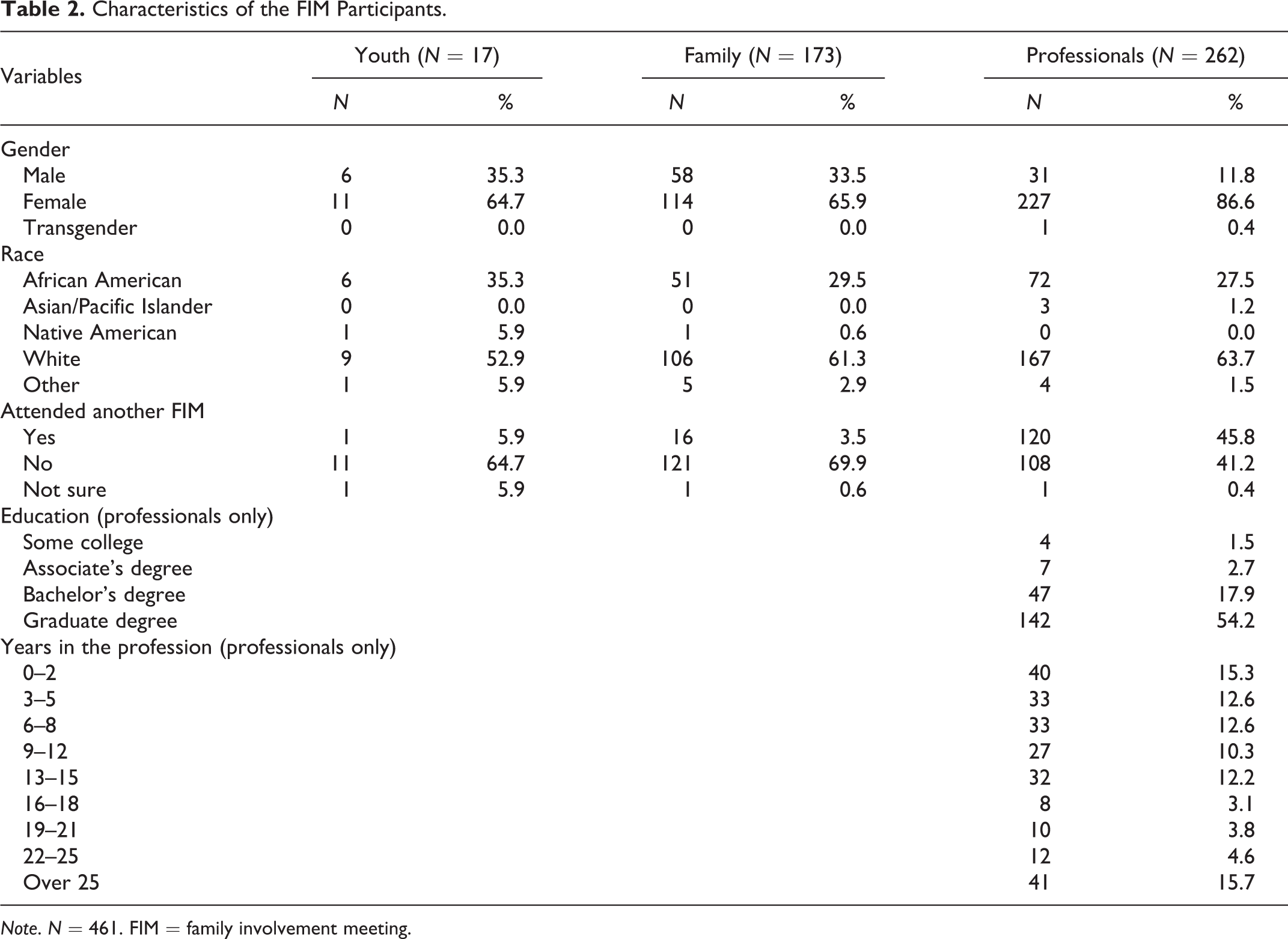
Note. N = 461. FIM = family involvement meeting.
For all of the FIMs surveyed more professionals participants were surveyed than family and youth participants. This trend could be present in the results due to the FIM location and agency’s involvement in the case. At some jurisdictions, one case could be involved in multiple service programs. Therefore in order to share information and be consistent in service planning, multiple agency and community professionals could be present to share updates and information on the services they are providing to the family. Also since transportation is often a common barrier for families, some of the family members may decide to participate in the FIM process over the phone. Because of the limitations of the survey tool, those participants who participate in the meeting over the phone are unable to take part in the FIM survey.
The results in Table 3 display the brief characteristics of the target child who were identified. Because there is missing information, the target child’s characteristics were not included in the analysis. The target child is the child for whom the FIM was being held, is the primary focus of the service plan, and can participate in the FIM if he or she is of appropriate age and maturity.
Characteristics of the Target Child for FIM.

Note. N = 93. FIM = family involvement meeting.
The information of the target child was collected from the FIM cover sheet which was completed by the FIM facilitator. Of the 78 FIMs that were conducted, 93 different children were identified as target children. Multiple FIMs conducted referenced more than 1 target child. While 93 target children were identified through the survey, only 17 youth actually participated in the survey. Youth participation in the FIM and survey depends on the youth’s age, maturity, and willingness to complete the survey after the FIM. These factors could account for the low participation rate of youth in the survey. Based on the overall target children population, the majority of the children were female (51.3%) and White (44.9%). Although for the majority of the target children their ethnicity was not identified, for those which were about one-quarter (25.6%) of the target child sample population consisted of children of non-Hispanic ethnicity. About 31% of the target child’s sample was older (between the ages of 16–20 years old) which is similar when compared to the 25% of the sample who were young (between the ages of infancy to 5 yearsold). Almost three-quarters (71.8%) of the target children involved in the FIM had had a prior report of abuse and neglect to the local department of social services.
Factors Associated With Overall Plan Satisfaction and Decision-Making
Bivariate analyses were conducted to examine differences between dependent variables and independent variables. Table 4 shows the results from the bivariate analysis. Bonferroni tests were conducted to adjust the α levels for t-tests and χ2. All the factors except gender and race were positively associated with both overall satisfaction with the meeting and decision-making at the meeting. For example, when participants understood the purpose of the meeting, their satisfaction scores were 4 points higher than those who did not understand, t = 3.81, df = 3.97, p < .01, and if participants understood the purpose of the meeting, 90% of them made a decision regarding the plan for the family and child receiving services, 40% higher than those who did not understand, χ2 = 13.48, df = 0.4, p < .01. When participants answered that they had enough time to talk, their satisfaction scores were 8.26 points higher than those who did not, t = 15.80, df = 8.26, p < .01, and 93% of them made a decision regarding the plan, 61% higher than those who did not, χ2 = 94.07, df = 0.61, p < .01. The rest of the factors associated with overall satisfaction were the meeting built on family’s strength, t = 14.52, df = 6.31, p < .01, being part of the team, t = 11.83, df = 5.50, p < .01, and were comfortable to express their opinions, t = 10.95, df = 5.62, p < .01.
Overall Satisfaction of Plan and Decision-Making at the Meeting Broken Down by Characteristics.

*p < .10. **p < .05. ***p < .01.
Table 5 shows the results from multiple regression analysis conducted to examine factors associated with the overall satisfaction with the meeting. The results show that all members’ participation in the meeting, β = 1.83, p < .01, 95% CI [1.15, 2.50], participants had enough time to talk, β = 3.62, p < .01, 95% CI [2.14, 5.10], participants felt like part of the team, β = 2.86, p < .01, 95% CI [1.57, 4.16], the meeting built on the family’s strengths, β = 2.97, p < .01, 95% CI [1.89. 4.06], the facilitator is knowledgeable, β = 2.73, p < .10, 95% CI [−0.12, 5.58], and the facilitator made participants comfortable, β = 1.82, p < .10, 95% CI [−0.27, 3.91], had positive association with participants’ overall satisfaction with the FIM. Among them, a variable that participants had enough time to talk had the highest impact on the overall satisfaction score, and it increased the score by 3.62 points. The next important factors were family’s strength, being part of the team, and the facilitator’s knowledge. Surprisingly, the facilitator’s management of the meeting’s time is negatively associated with overall plan satisfaction, β = −3.09, p < .10, 95% CI [−6.31, 0.14].
Factors Associated With Overall Satisfaction With the Meeting.

Note. R 2 = 0.58 and adjusted R 2 = 0.56.
*p < .10. **p < .05. ***p < .01.
Table 6 shows the results from the logistic regression used to understand the factors associated with decision-making. Model 1, without including overall satisfaction scores on plan, shows that being White, β = 1.05, p < .05, 95% CI [0.03, 2.08], engaging family members in the meeting, β = 1.14, p < .05, 95% CI [0.01, 2.26], having enough time to talk, β = 1.51, p < .10, 95% CI [−0.32, 3.34], feeling as being part of the team, β = 2.74, p < .01, 95% CI [1.08, 4.40], the meeting built on family’s strengths, β = 1.60, p < .05, 95% CI [0.17, 3.03], and facilitator’s attitude of respecting participants, β = 4.42, p < .10, 95% CI [−0.19, 9.02], had positive association with high probability of making a decision during the meeting. Taking feeling as being part of the team as an example, the odds to make a decision was 14.5 times [exp(2.74) − 1] higher for those who felt as part of the team than those who did not. Interestingly, the facilitator’s ability to make participants comfortable reduced the probability of decision making, β = −3.23, p < .10, 95% CI [−6.53, 0.06].
Factors Associated With Decision-Making.
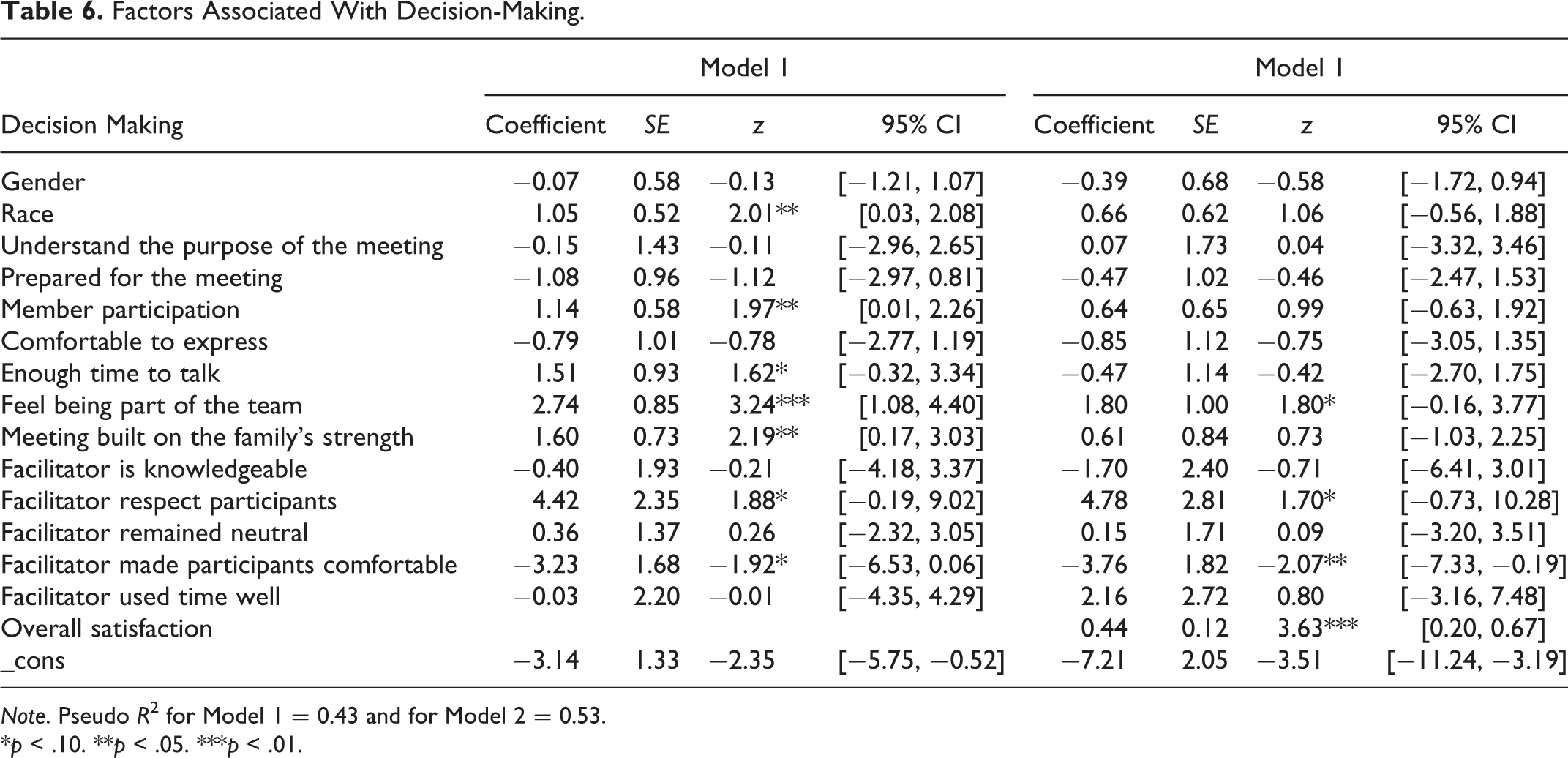
Note. Pseudo R 2 for Model 1 = 0.43 and for Model 2 = 0.53.
*p < .10. **p < .05. ***p < .01.
After including the overall satisfaction scores on plans in Model 2, the variables of involving members in the meeting and facilitator’s attitude of respecting participants remained statistically significant, and facilitator’s ability to make participants feel comfortable had still negative associate with the decision-making. The overall satisfaction with the meeting was associated with higher probability of decision-making at the meeting, β = 0.44, p < .01, 95% CI [0.20, 0.67]. One point increase in overall satisfaction with the meeting was associated with 55% [exp(0.44) − 1] higher odds of making a decision during the meeting.
Summary of Results
When comparing the results of the analysis, it can be seen that there are many significant factors which can influence a participant’s overall satisfaction and decision of a plan for the child and family. The results of the study show that participants were more likely to be found satisfied with the meeting when they were engaged in the process, able to express their own thoughts, able to be part of the planning team, able to build the plan on the family’s strengths, the facilitator was highly knowledgeable, and the facilitator made them feel comfortable. The logistic regression results showed that when it comes to making a decision regarding the plan, if the overall plan score was excluded, White participants, those who were engaged in the meeting process, given the opportunity to speak, and felt that the plan was built on the family’s strengths were more likely than other participants to make a decision regarding the future plan for the child and family. Consequently, the results displayed that unlike the participant’s satisfaction of the plan, the facilitator’s ability to make the participant feel comfortable had a negative impact on whether a decision was made at the meeting. Further analysis of the logistic regression including participant’s overall satisfaction scores showed that overall satisfaction with the meeting increased probability of making a decision regarding the next plan for the family and child.
Discussion and Applications to Social Work Practice
The goal of this study was to examine what characteristics of one mid-Atlantic state’s FGDM process, named FIM, influence on a participant’s overall satisfaction and decision-making regarding the plan for the family and child receiving services. The results of the study demonstrate the importance of the FGDM model and other similar models like FIM on the practices of effectively involving participants in planning and decision-making for child welfare services. Through implementation of the FGDM process, child welfare agencies have shifted their practices to support the involvement of family, community members, and professionals in the planning and decision-making process for families receiving services. The findings of this study are similar to the previous research that shows that for child welfare practices, the FGDM process builds on the strengths of families, engages the participants in the development of the family’s plan, and allows them to feel empowered by the process (Michalopoulos, Ahn, Shaw, & O’Connor, 2012; Weigensberg et al., 2009). By having the participant’s engagement and support in the process, decisions can be made to ensure that families and children are receiving the services and support which are necessary to keep them safe and healthy.
Another key aspect of the results shown in this study is when the participant is satisfied with the FGDM meeting, it is associated with a higher probability of the team making a decision on the service plan. This satisfaction can be positively influenced by elements of the FGDM process including participants having enough time to talk, development of the plan based on the family’s strengths, participants feel like part of the team, and participants are comfortable to express their thoughts and ideas about the plan. With all of these aspects affecting the outcomes of the FDGM meeting is it vital that participants engage in the FDGM process to help empower the family to reach their goals and strengthen their families.
Along with the engagement of the participant, the FGDM facilitator also plays an important role in the FGDM process. The facilitator’s role of assisting the participants in a productive discussion while enabling the participants to feel comfortable is crucial for the participants to be overall satisfied and make the appropriate decisions for the plan. Based on the study’s findings in order to help increase participant satisfaction of the overall plan, the facilitator should make the participant feel comfortable within the dynamics of the team. Through this comfortability, participants can unite together as a team and focus to address the issues and concerns that the family is facing. The results show further implications on the facilitator’s skills and education. In order to increase the participant’ s level of comfortability, FGDM facilitators should be educated to increase their knowledge of resources, interventions, and effective practices as well as trained in skills of group engagement, dynamics, and environment in order to positively effect a participant’s satisfaction level of the FGDM and the case’s plan.
The results of this study demonstrate that the fidelity of the FGDM process to the FCP model is key in order to be effective in making decisions and developing a successful service plan. In order to ensure the fidelity of the FDGM to the FCP framework, Rauktis, Bishop-Fitzpatrick, Jung, and Pennell (2013) developed a three-factor tool. This tool examines the three aspects of the FGDM to include: (1) productive decision-making, (2) family group inclusion, and (3) professional supportiveness (Rauktis, Bishop-Fitzpatrick, Jung, & Pennell, 2013). This study supports how influential these three factors can be on the satisfaction and the overall decisions made for the families and children involved. Continued evaluation of the fidelity and effective implementation of the FGDM process can lead to potentially more positive and successful family and child outcomes.
This study also supports that multiple factors including family’s engagement, strengths, comfortability, and the facilitators’ practice all play a vital role in the FGDM process. The facilitator acts as the mediator, the active listener, the leader, and the resource and practice expert. Therefore, it is imperative that child welfare agencies train facilitators with the appropriate mediation and skills necessary to empower all participants in the FGDM process. This mid-Atlantic state, used a 3-day initial training of the FGDM framework, process, and skills for each practicing FIM facilitators, followed by annual refresher trainings provided by the partnering university. The initial training provided an in-depth examination of the FGDM model, practices, and skills in order to implement the FIM process across a variety of children and families involved with child welfare services. In the facilitator’s training, mediation and active listening skills should be learned in order for the participants to have their input heard and clearly expressed to the group. Facilitators will also learn to be cognizant of the need to fully engage all of the participants appropriately in order to ensure that all participants have a voice in the final plan. The facilitators should be trained in the overall FGDM model, its principles, and effective communication and mediation skills so that they will be able to remain neutral throughout the meeting and help facilitate the group to developing a plan. Based on this study’s findings, if the facilitator is able to properly engage and effectively lead a FGDM meeting, the probability of a successful outcome for that family and child also increases.
Although this study provided valuable insights on the FGDM process, as in all research studies, there are some limitations. The implementation of the FIM Feedback Survey was such that the survey tool was only used by participants who are physically present at the FIM which excludes those participants who are on the phone. In order to account for this limitation, an electronic form of the survey is being examined to allow phone participants’ feedback to be given. Additionally, during Phase 1 of the FIM evaluation research, nine of the state’s jurisdictions participated in the research and conducted the survey. When conducting Phase 2, all jurisdictions in the state will implement the feedback survey, and results of that evaluation will be included in a future study.
After examining the results, another limitation was found in that there were a low percentage of youth participants who provided their feedback on the FIM process. This limitation could be due to the youth’s age, maturity, and willingness to participate in the survey. Recently, a new state policy implemented increases the number of FIMs for older youth so an increase in youth participants should occur during Phase 2 of the FIM implementation evaluation process. In addition to this limitation, service providers had a higher response rate to the survey when compared to the youth and family member participants. While it is important to note that not all the service providers are employed by the child welfare agency, this limitation can significantly bias the results of this study. The professional participants are more educated because of their training on the model and practices of the FGDM process and therefore could be biased when evaluating the FGDM process. Also the large number of professional participants could be seen due to the fact that some children and families work with multiple community service providers or have other supports in the community. These professional providers may not have any expertise in the FGDM practice or framework. Lastly, it is important to identify that another limitation for this study is that its outcome measure was of unknown validity and reliability.
Building off of the results of this study, further research could be conducted to examine the longitudinal effects of the FGDM process on the child’s permanency outcomes. An evaluation of the consistency and impact of the FGDM practices over time could display the most beneficial FGDM practices for long-term permanency outcomes. In addition, to help improve the current child welfare policies and practices, an evaluation of the practice should be conducted to ensure that proper support and consistent implementation of the FGDM principles and guidelines are available according to fidelity of the FCP model. Likewise, to help grow the potential of the FGDM practice, a future study could examine the effects of the FGDM process of certain case types on the outcomes of the cases for the children involved. Similarly, a longitudinal evaluation could lead to a more in-depth assessment of the delivery of services and supports through the FIM process. This research could help social work practice identify the most effective ways of assessing what the needs of the family are and what resources would help strengthen the family unit, ultimately leading to a decrease of the reoccurrence of maltreatment. This analysis could similarly lead to improving the resources found in each jurisdiction, a family’s access to those resources, establishing an appropriate time frame for which the services and supports are provided, and identifying what services are most effective in supporting families and promoting a child’s safety, well-being, and permanency.
Footnotes
Authors’ Note
We are currently in a confidentiality agreement with this state that requires no identification of the state within this article.
Acknowledgments
We extend our gratitude to the supervisors and workers who contributed to this study by providing valuable information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a contract with a mid-Atlantic state’s child welfare agency.