
Abstract
Purpose:
This study presents the development and initial validation of a Listening Scale (LS) that was used to assess the listening skills of a sample of Hong Kong counseling professionals and the potential penetration of psychoanalysis among this sample.
Method:
A total of 217 Hong Kong social workers, psychologists, and counselors were surveyed to develop and assess the scale’s internal psychometric properties.
Results:
Factor analysis confirmed a single factor structure for the LS, with 8 items. Internal reliability was good and discriminative validity was supported by comparisons with background information.
Discussion:
The LS shows promise as a meaningful, reliable, and valid measure. The LS could be useful to assess important dimensions of the practice of counseling professionals and to better assist their client-centered practice, and as a formative instrument for use by counseling professionals. Finally, the LS can assess the penetration of psychoanalysis where the psychoanalytic theory is not strong.
Counseling in Hong Kong is still at an early stage of development as well as its social recognition after more than 50 years from its emergence (Leung, 1999). In Hong Kong (differently than in mainland China and Taiwan), the term “counseling” is normally translated to 辅导 (Fu Dou), which emphasizes the attitude of “giving guidelines, advice.” Counseling in Hong Kong is provided mainly by social workers, then clinical psychologists and counselors (Leung, Chan, & Leahy, 2007). Previous studies found that counseling professionals in Hong Kong endorse and use mainly the behavioral/cognitive approach, followed by existential/humanistic (Chan & Lee, 1995), while psychoanalysis is rarely adopted (Cheung, 1997). In some cases, there could be interest in some psychoanalytical concepts; however, respondents revealed a rather eclectic approach and psychoanalysis is at best a tool to use in combination with other orientations/techniques. Recent studies have reported growing interest in psychoanalysis in mainland China and Taiwan (Gerlach, Hooke, & Varvin, 2013; Scharff & Varvin, 2014); however, the current penetration of psychoanalysis among Hong Kong counseling professionals is unclear, so further research is needed. This study aimed at understanding if psychoanalysis may be received among a sample of social workers, psychologists, and counselors who deliver counseling in Hong Kong. To do so, an operational definition of psychoanalysis was needed.
What Is Psychoanalysis?
Psychoanalytic theory is known for concepts like unconscious, transference, defense mechanisms, repression, and for the analysis of dreams. However, remarkable distinctions among various psychoanalytic schools exist, and previous attempts to describe common theoretical grounds among psychoanalysts have been unsuccessful (Blass, 2010; Green, 2005; Widlöcher, 2010). But psychoanalysis is more than just a sum of concepts—it is a practice. Some (e.g., Jiménez, 2009) argue that despite psychoanalysts tending to emphasize their theoretical divergences, in their practice, they tend to have more convergences. In line with this assumption, some tools have been developed for evaluating the “psychoanalytic process,” such as the Columbia Analytic Process Scale (Vaughan, Spitzer, Davies, & Roose, 1997) and the Analytic Process Scale (Waldron, Scharf, Hurst, Firestein, & Burton, 2004), which were developed to assess the presence and quality of the analytic process in a single therapy session; the Psychodynamic Intervention Rating Scale (Cooper & Bond, 1998), which was designed to assess therapists’ use of supportive and interpretative interventions in psychodynamic sessions; and the Therapist Verbal Intervention Inventory (Koenigsberg, Kernberg, Appelbaum, & Smith, 1993), designed specifically for use in the study of the treatment of patients with borderline personality disorders. However, despite the promising premises, already 20 years ago Vaughan, Spitzer, Davies, and Roose (1997) observed that “there is no meaningful consensual definition of the term AP (analytic process)” (p. 964), and more recently, Schachter, Schachter, and Kächele (2012) concluded that the concept of psychoanalytic process is “no longer a viable or useful construct and should be retired” (p. 19). Thus, a new perspective on defining the essence of psychoanalysis is needed. In addition, the aforementioned tools are made for use by external raters (who thus need to be trained), and they all serve to assess the quality and quantity of analytic work in a single session; however, they do not necessarily capture the therapist’s attitude toward clinical work.
In this study, listening was considered the most versatile and yet comprehensive concept, as it refers more to a practice than theories; then, listening can overcome the theoretical differences among various orientations and schools, allows cross-cultural research, and allows research in contexts where the psychoanalytic theory is not strong. Thus, psychoanalytic listening should be described and then viewed by the listening displayed by local counseling professionals.
Some instruments to assess the listening in counseling are the Active-Empathic Listening Scale (Bodie, 2011), the Active Listening Observation Scale (ALOS-global; Fassaert, van Dulmen, Schellevis, & Bensing, 2007), and the Jefferson Scale of Physician Empathy (Hojat et al., 2001). However, almost all of these counseling approaches rely on the traditional theory of communication (Shannon, 1948) but not psychoanalysis (Mounin, 1985). Thus, a definition and operationalization of psychoanalytic listening is needed.
Listening as a Key Concept of Psychoanalysis
Although Freud was a prolific author for almost 50 years, he expressly cited only a relatively limited number of technical rules for practicing psychoanalysis. For example, in 1912, he wrote Recommendations to Physicians Practicing Psychoanalysis; interestingly enough, such recommendations implicitly describe psychoanalytic listening. First, “not directing one’s notice to anything in particular and in maintaining the same ‘evenly-suspended attention’” (Freud, 1912, p. 110) is equivalent to the demand made to the client to obey the fundamental rule of the free association. Second, the analyst should do everything not to become a censor in selecting the patient’s material (metaphor of the receiver). Third, the analyst should patiently obey “the psycho-analytic rule, which enjoins the exclusion of all criticism of the unconscious or of its derivatives” (Freud, 1912, p. 118).
A number of psychoanalysts after Freud have written about psychoanalytic listening (for a review, see Sapisochin, 2013). Some have referred to it as a core concept of empathy (Greenson, 1960) and actually as empathic listening (see Jackson, 1992, for a review). Stewart (1983) criticized this empathy embeddedness as a way of listening, and instead he proposed what he termed interpretive listening. For Schafer (2005), listening itself is an interpretive action, so that there is no difference between listening and interpreting. Chodorow (2003) suggested distinguishing between listening for (i.e., listening driven by theory) and listening to (i.e., listening driven by individuality). Lacan (1977) stated, “we must listen to the speaker, when it is a question of a message that does not come from a subject beyond language, but from speech beyond the subject” (p. 214). Akhtar (2007) defined psychoanalysis as the “listening cure” building on the famous title of “talking cure.”
After a comprehensive literature review about psychoanalytic listening (Busiol, 2016), it can be said that “(a) while hearing is directed toward what is being said, listening is directed toward what is not being said; […] (b) the analyst listens what remains implicit and what is not being verbalized, including his/her feelings and reactions toward the client; (c) psychoanalytic listening is not intentional, the patient is required to free associate and say whatever comes to mind, while the analyst is required not to focus on anything in particular; […] (d) there is no dialogue in analysis, but instead, an asymmetrical conversation; (e) the aim of the psychoanalytic conversation is to reflect to the analysand his/her speech; […] (f) psychoanalysis is more effective when it sustains the formulation and the articulation of questions rather than the production of answers; and (g) the analyst’s engagement in the treatment is more important than the mastery of any techniques” (p. 60).
Psychoanalytic listening is not a unified construct; it cannot be, given that there is not only one version of psychoanalysis. Over the past century, the recommendations made by Freud have been challenged at various levels. Today, some might say that there are as many conceptualizations of psychoanalysis as psychoanalysts; thus, the above description should not be considered definitive and representative of all current psychoanalytic schools and/or orientations. Rather, the conceptualization of the psychoanalytic listening presented here is influenced by the European tradition of Sigmund Freud and Jacques Lacan, more than other authors and schools. Further, in this study, listening has been conceptualized as a style or a method (grounded primarily on the Freudian free floating attention and free associations), more than a hermeneutic or interpretive act. This means that listening has been conceptualized as answering the question “how to listen?” rather than “what to listen for?” As the psychoanalytic theory is not well received in Hong Kong, simply asking local counseling professionals if they know some psychoanalytic idiom or concept would not help to understand how they actually practice. Furthermore, it may be possible that Hong Kong counseling professionals have an attitude similar to psychoanalysis in their listening style, without being aware of it and without expressly referring to psychoanalysis. Then, examining their listening style was deemed to shed some light on how (local) counseling professionals practice, how similar or different from psychoanalysis their practice is, and eventually if psychoanalysis could be received by them.
Rationale and Study Purpose
The rationale to develop and validate a Listening Scale (LS) arose within the context of a previously conducted larger study which showed that the psychoanalytic theory was used infrequently among a sample of Hong Kong helping professionals, including psychologists, social workers, and counselors (Busiol, 2013). However, this study did not assume that psychoanalysis is completely missing from Hong Kong. As the earlier literature about its use/nonuse revealed, it may be that some features of psychoanalysis are already embedded in counseling professionals’ attitudes, even though they don’t expressly refer to psychoanalysis. Given the deep-seated culture mores, this study also sought to determine whether a cultural disposition of listening could be empirically determined by more precisely measuring the listening component. Thus, this study aimed to assess if local counselors share some similarities or differences with aspects of psychoanalysis related to this listening component. The development and validation of the LS was intended for assessing the penetration of psychoanalysis among counseling professionals in Hong Kong; however, the LS is not pan-theoretical and relevant to psychoanalysis regardless of school of thought or grouping. This study aimed to develop and validate a psychoanalytic informed LS for use by counseling professionals and to assess the degree to which social workers, counselors, and psychologists in Hong Kong may listen psychoanalytically, without being aware of it and without expressly referring to psychoanalysis.
Method
Participants
In Hong Kong, registration for social workers, psychologists, and counselors is not mandatory; so, it is simply not possible to know their exact number. Furthermore, since not all of them necessarily practice counseling as part of their profession, it is not possible to know how many of them actually deliver “counseling services.” For these reasons, a representative sample of this population was difficult to select, so purposive sampling was adopted. Potential participants were invited from the Social Welfare Department and some of the main local nongovernment organizations (NGOs). Further, a number of counseling professionals in private practice recruited by direct contact or snowball techniques became study participants. Targeted participants had to meet the following requirements: (a) hold a university degree in psychology, social work, or counseling; (b) deliver counseling as part of their routine practice; and (c) have at least 2 years of work experience in counseling.
It was assumed that all three of these disciplines (social work, psychology, and counseling) have differences in their education and their use and/or nonuse of psychoanalysis. As a consequence, a clustered sample representing these three cohorts was selected. A total of 550 questionnaires distributed by hand were conducted anonymously and the respondents understood that not even the researcher could identify them. This study was presented, in general terms, as a study on how local professionals conduct counseling (the complete questionnaire included many more items than those specifically presented here); psychoanalysis was never mentioned as the focus of the study, and nor was it mentioned that the researcher is a psychoanalyst. An information cover page assured respondents that this was not a test with right or wrong answers and that their personal opinion and experience were the only concern.
Eventually, 217 questionnaires were usable (a favorable response rate of 40%). Participants received no monetary rewards and their participation was on a voluntary basis. The majority of respondents were women (72%), between 31 and 40 years of age (43%), with a university degree primarily in social work (n = 156 or 72%, reflecting the higher percentage of social workers providing counseling in Hong Kong. Psychologists were n = 26 or 12%, and counselors were n = 35 or 16%), and were mostly Christians (53%). Almost all received their educational training in Hong Kong (98%). Less than one third (29%) had personally received counseling before or were personally receiving counseling themselves, at the time of the study. Of those, the majority (64%) underwent counseling for less than a year. The majority had less than 8 years of experience (63%) and worked in an NGO (76%). In most cases, their clients were adults (69%), and almost all of the samples (93%) reported using two or more counseling approaches. The most commonly endorsed counseling approaches reported by participants were cognitive–behavioral therapy (CBT) and/or cognitive therapy and/or behavioral therapy (72% of the respondents reported at least one of these approaches, with 56% reporting CBT, 28% cognitive therapy and 27% behavioral therapy), person-centered therapy (44%), narrative therapy (29%), positive psychology (27%), play therapy (27%), group therapy (24%), systemic therapy (23%), brief therapy (21%), art therapy (16%), task-centered therapy (15%), psychoanalysis (11% but more specifically, 8% among social workers and 17% among those with a degree in psychology or counseling), and gestalt therapy (10%). In 45% of these cases, psychoanalysis was reported to be used together with positive psychology and 40% with CBT. No counselor in the sample reported psychoanalysis as their only therapeutic approach.
Scale Development
Item generation
Following standard criteria for the development of valid and reliable questionnaires (Gillham, 2000; MacKenzie, Podsakoff, & Podsakoff, 2011; Worthington & Whittaker, 2006), a comprehensive list of 20 items was initially generated by the main researcher, who is a licensed clinical psychologist and psychotherapist (psychoanalytically oriented). This initial list of items was determined by reviewing: (a) existing literature describing the listening in psychoanalysis and (b) existing literature describing the listening in other psychotherapeutic/counseling approaches. Items were generated based on their satisfaction with two criteria: (1) they should be applicable to psychoanalysis in a broad sense, meaning that they should reflect the similarities and commonalities among different orientations and (2) ideally, they should help differentiate listening as in psychoanalysis from listening as in other psychotherapeutic or counseling approaches.
Stage 1: Item reduction and scale validation
The process of scale construction involved two stages of item reduction. In Stage 1 (prior to data collection), the aim was to reduce the number of items to include in the questionnaire. Thus, the initial list of 20 items was subjected to expert judgment for redundancy, face validity, content validity, and clarity. These eight experts were Western and Hong Kong clinical psychologists and psychotherapists (psychoanalytical orientation), all with strong backgrounds in psychoanalysis and an academic knowledge of counseling. The purpose of the list was explained to the experts, who were asked to simply answer agree/disagree to each item in the list. Further, they were asked to indicate those items that in their opinion did not draw a clear distinction between psychoanalysis and other counseling orientations and/or were not meaningful or confusing. Those items that did not score a great agreement among the experts were then removed. This round of item assessment resulted in the elimination of some irrelevant items, the addition of some others, and the collapsing of some related items into one. Other items underwent changes in wording. Whenever rephrasing was not possible and ambiguity remained, the item was also removed, as were items containing double questions. The wording of items was particularly challenging, both for the content addressed and for cultural context, which led in some cases to different interpretations. Items were translated from English into Chinese, to ensure that all the respondents (Hong Kong counselors) could easily understand the questions. Back-translation was not executed, because items were presented in both languages. After this process, the final list of items was reduced to 13.
The format of the questionnaire was designed following guidelines outlined by Gillham (2000) and Worthington and Whittaker (2006). All items were assessed on a 6-point Likert-type rating scale, comprising 1 = strongly disagree, 2 = moderately disagree, 3 = slightly disagree, 4 = slightly agree, 5 = moderately agree, 6 = strongly agree. The 6-point rating scale was preferred to a 5-point one, so that respondents could select a position rather than being “neutral,” and a 6-point scale tends to give better discrimination and reliability values than a 5-point one (Chomeya, 2010).
Stage 2: Scale construction
In line with Kline’s suggestion (2000), after collecting the questionnaires, the 13 items were analyzed and some were removed. Additional purification involved eliminating those items that did not clearly reflect a psychoanalytic construct, were too generic, and could apply to any counseling orientation (e.g., Items 90 “I ask the client his particular meaning of specific words” and 94 “I ask continuing questions like ‘Could you tell me more?’”). Further, some respondents argued that a few items were not appropriately translated or that the translation was open to different interpretations; these items were removed. Finally, items were also analyzed for very high interitem correlation (r ≥ .9), low or no item-total correlation (r < .3), and normal distribution (skewness of no more than |1| and kurtosis of no more than |3|). Items were then tested using exploratory factor analysis. The final LS items were reduced to 8.
Results
In order to establish the reliability of the 8-item LS, two reliability coefficients were determined. Nunnally and Bornstein (1994) have recommended that scales used in basic research should have reliability of about 0.70 or better. The Cronbach’s α of this scale was .73 and thus was regarded as satisfactory. Furthermore, the split-half reliability was r = .73.
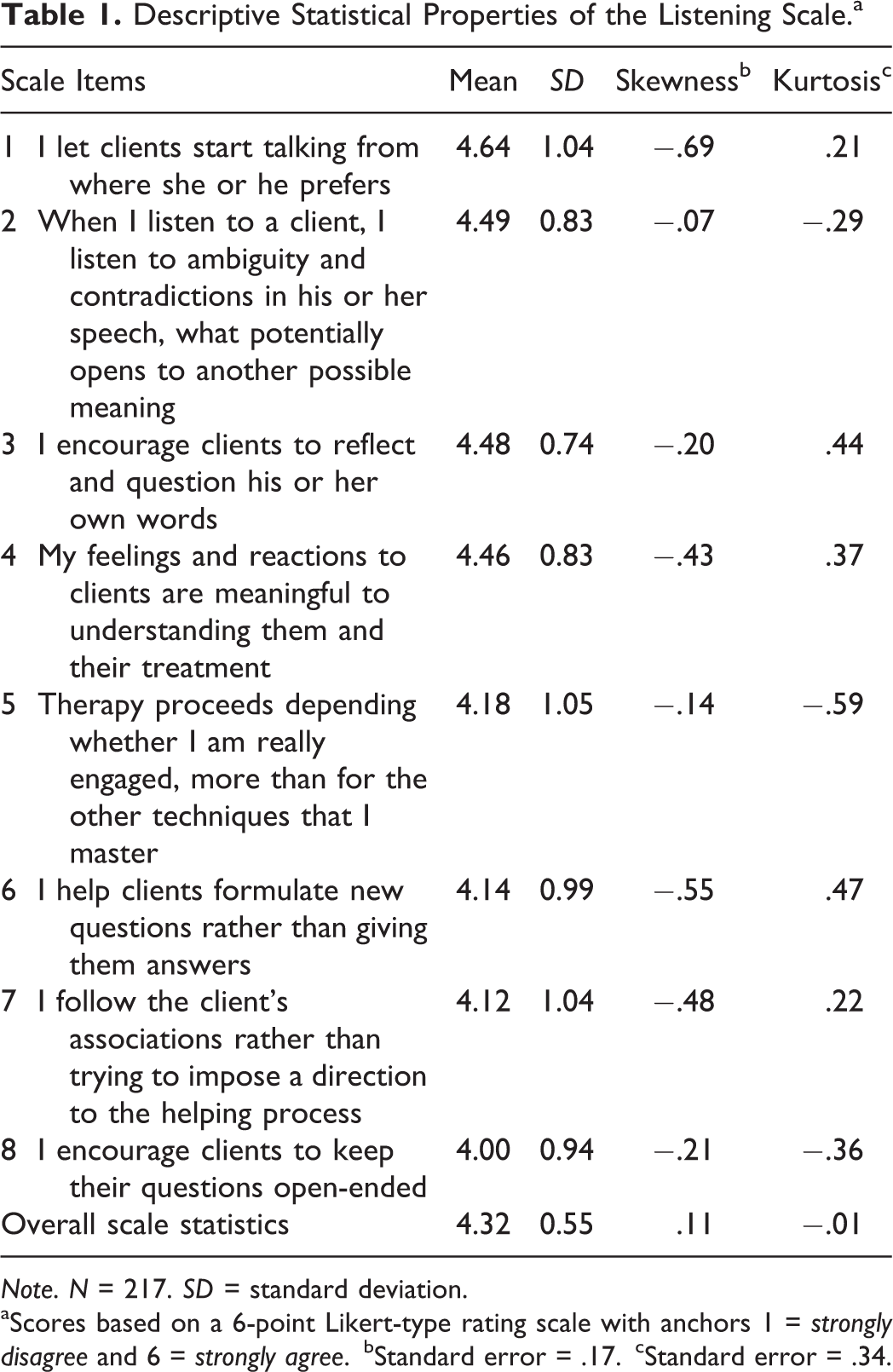
The descriptive statistics of the LS were then determined. Means, standard deviation, skewness, and kurtosis of all 8 items are reported in Table 1.
Descriptive Statistical Properties of the Listening Scale.a

Note. N = 217. SD = standard deviation.
aScores based on a 6-point Likert-type rating scale with anchors 1 = strongly disagree and 6 = strongly agree.
bStandard error = .17.
cStandard error = .34.
Confidence interval (CI) of the means ranged from a low of 4.24 to a high of 4.40 (95% CI [0.09, 0.42]). Considerable variation in means (R = .64) and standard deviation (R = .31) was noted. Also, the M of 4.32 was positioned between “slightly” and “moderately” agree on the 6-point rating scale. Participants utilized the full range of the scale (1–6) in their responses to these items. The distribution of the scores did not deviate substantially from normality. Data were also screened for multivariate outliers by using the “outlier labeling rule” (Hoaglin, Iglewicz, & Tukey, 1986) and by calculating the Mahalanobis distance at p < .001 (Cousineau & Chartier, 2015); in both cases, no outliers were found.
Exploratory Factor Analysis
First, Bartlett’s test of sphericity, χ2(28) = 240.30, p < .001, and the size of the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy (KMO = .83) ensured that the items of the LS had adequate common variance for factor analysis. Second, parallel analysis, minimum average partials (MAP) test, and scree plots were used to determine the number of factors to extract. In parallel analysis, 5,000 random permutations of the data to compute average eigenvalues were generated; results suggested retaining one factor as eigenvalue for this was higher in the actual data set (i.e., 2.03) than in the parallel analysis (i.e., 0.46). Subsequently, also the MAP test and scree plots indicated retention of one single factor. Therefore, a one-factor solution was extracted by Exploratory Factor Analysis (EFA) with principal axis factoring (PAF). Loadings of the items on this factor were all equal to or greater than .45 (Table 2). Factor 1 accounted for 35% of the total variance of the LS.
Factor Loadings of the Listening Scale.
Note. N = 217. Factors were extracted using principal axis factoring.
Discriminative Validity
Discriminative validity indicates if a scale differentiates (or does not differentiate) between groups that should differ (or not differ) based on theoretical reasons. To evaluate the discriminative validity of the LS, independent t-tests were performed among subgroups. The rationale was that if psychoanalytic listening is a structurally (i.e., qualitatively) different disposition toward listening, it should not be assessed simply depending on the demographic characteristics of the therapist, such as age, gender, years of working experience, and/or number of clients (as these measures express quantity but not necessarily qualitative changes). Further, it was assumed that all three cognate disciplines (social work, psychology, and counseling) have substantial theoretical differences from psychoanalysis; then, it was expected that scores of the LS would not exhibit statistically significant differences by academic degree. Instead, if the concept of listening can really describe a practice (and if the LS can really describe how respondents listen in practice, beyond theoretical differences), only those counseling professionals who have received personal therapy might report a different response than the rest of the group. Thus, the first hypothesis was that the LS would assess differences between counseling professionals who have received personal therapy and those who have not. Subsequently, the second hypothesis was that LS would not assess differences among other subgroups.
The main group of respondents was split by (a) age, (b) gender, (c) university major, (d) years of practice experience, (e) number of clients, and (f) history of therapy. For statistical purposes, the following continuous variables were dichotomized according to predefined cutoff points, so as to have subgroups with similar numbers of respondents: (1) age (≤40 vs. >41 years old); (2) years of practice experience (≤8 vs. >8 years); number of clients (≤100 vs.>100). Finally, the variable university major was dichotomized as social work versus nonsocial work.
Coherently with the assumptions, t-tests (with a Bonferroni adjustment for multiple statistical tests, p = .0083) showed that the only significant finding among the sociodemographics was related to history of therapy. Respondents who had been in therapy before (M = 4.50, SD = .57) reported significantly higher psychoanalytic listening than respondents who had not been in therapy (M = 4.24, SD = .53), t = −3.01, p = .003 (Cohen’s d measure of effect size was .47, 95% CI [0.18, 0.78]). Conversely, age, gender, university major, years of practice experience, and number of clients had no statistically significant influence on the psychoanalytic listening.
Discussion and Applications to Practice
The study presented herein describes the development and psychometric properties of the LS (see the complete scale in Appendix Table A1). Higher scores indicated that a therapist is able to suspend his or her attention and free his or her listening from any assumptions concerning the content and the meaning of the client’s speech and follow the talking of the client instead. The LS could be useful to assess important dimensions of the practice of psychoanalysts and counseling professionals and to better assist their client-centered practice. Second, here psychoanalysis has been reconsidered and operationalized in terms of a distinctive kind of listening, so the LS can assess the penetration of psychoanalysis where the psychoanalytic theory is not strong. Finally, listening is an essential component of any helping relation; thus, it allows comparison among different approaches. The LS can be a tool for dialogue between psychoanalysts of different orientations (as the operationalization of listening has the advantage that it may overcome several conceptual differences among psychoanalytic schools) as well as between psychoanalysts and other counseling professionals (e.g., to see how similar or different their practice really is).
Although listening is generally considered an essential component of any helping profession, little empirical work to assess it has been done, particularly in psychoanalysis. One of the merits of this study is the offering of a new perspective on defining an important component of the essence of psychoanalysis.
Evidence supporting the theoretical grounds of the LS was gathered from the reported independent t-tests. The LS demonstrated discriminative validity in detecting differences between six subgroups who were formulated according to background information. Professionals who had been counseled personally themselves had reported a higher listening disposition than professionals who had not received counseling. This is important as it emphasizes the importance of receiving therapy (particularly for a counselor), as a way of experiencing and improving one’s own listening skills. A personal analysis (or a training analysis) is essential in psychoanalysis in order to become a psychoanalyst (Masson, 1990). This is not always required by other psychotherapeutic/counseling schools. Instead, in regard to other sociodemographics analyzed, psychoanalytic listening was shown to be unrelated to years of experience, number of clients, or major, showing that it is not a merely cognitive skill that can be acquired as a result of longer practice or simply by training.
Findings from this study are relevant to social workers. First, according to the subgroup analyses, social workers may significantly benefit from receiving personal counseling, and subsequently this can be beneficial to their practice and to their clients. Social workers (particularly those who deliver counseling) are thus strongly encouraged to undergo their own personal psychotherapy; however, as undergoing personal psychotherapy appears to be particularly important for the quality of the counseling practice, it is this author’s opinion that professional bodies (e.g., social workers’ registration boards) should consider requiring social workers to undergo their own psychotherapeutic process as part of their training. Second, looking at the scores from this sample, it can be said that the respondents were inclined to listening what remains unsaid in the therapeutic process. However, previous research from Yip (2002) presents a different picture: Most social workers in psychiatric services in Hong Kong were described as being primarily focused on patients’ immediate problems and providing them concrete tasks: “[social workers] largely give advice and guidance to their patients rather than performing counseling” (p.39). Further, Yip (2002) found that they lacked specialized training and skills in in-depth counseling and received insufficient theoretical support from their colleagues and supervisors. Finally, Yip (2004) described the social workers as not having sufficient experience, knowledge, and understanding to carry out psychotherapy, which may cause poor or even negative outcomes. These results are not necessarily contrasting; instead, this may suggest that whereas social workers in Hong Kong are attentive and potentially know how to listen (as assessed by this scale), they do not always have the theoretical knowledge, or the framework, meaning that they do not know what to listen for. Further (psychoanalytic) training may lead to an effective improvement of the quality of their intervention, and more in general the quality of the profession in Hong Kong. The development of this LS allows highlighting strengths as well as identifying in more depth the criticalities of counseling professionals.
Another unique feature of LS is that it was entirely developed in Hong Kong, whereas most counseling assessment instruments originate in Europe or North America and are then imported/translated into other cultural contexts. The LS, while grounded in a local context, aims at assessing a “culture-up” perspective derived from Western theories. This potentially makes it culturally appropriate and valid in its place of origin as well as for international comparisons. However, the use of LS in other cultural contexts needs to be carried out to substantiate this contention and requires additional reliability and validity.
Further, these results show that local counselors score largely above the theoretical midpoint of the LS, showing a certain proclivity for psychoanalytic listening, although psychoanalytic theory and techniques were not used by this sample. This inclination to listen may be due to clinical and social work education, as the free-value, nonjudgment, and client-centered values are stressed throughout training in general. However, this may also suggest that Hong Kong Chinese culture may influence how local counselors listen. Previous studies indicated that in Hong Kong, people are more inclined toward listening rather than speaking (Busiol, 2013). For instance, Gao and Ting Toomey (1998) described Chinese communication as listening-centered (tinghua 听话). According to Dragan and Sherblom (2008), the very idea of communication, particularly in American and European societies, is often equated with talking rather than listening. In these contexts, effective communication normally relies on the speaker, whereas the role of the listener is often less emphasized (Janusik, 2004). Instead, Chinese culture encourages listening rather than speaking (Fang & Faure, 2010; Gao, 1998). For example, Chinese schools emphasize listening, reading, and writing skills, but rarely give importance to speaking skills (Lu, 2001). Additionally, Hong Kong Chinese culture emphasizes respect for hierarchies and humility, which is reflected in their attitude toward listening (i.e., parents, officials, elders, relevant others, etc.) rather than speaking. Thus, it may be that a listening orientation is already embedded in the Hong Kong Chinese culture, which might partially explain the listening profile reported by the local counselors in this study. However, without any other data and/or baseline statistics for comparison, it is not possible to come to a definitive conclusion, because it is not possible to know how therapists in general respond. Another unique feature of this study was that it was designed as quantitative research, which is rare in psychoanalytic literature.
Constructing the LS has been challenging, for a few reasons. First, the formulation of each item required deep rethinking of the assumptions about (and the specificities of) psychoanalysis as well as counseling methods, techniques, and theory. Second, as this scale intended to assess the inclination toward a practice that is not very popular in Hong Kong, items needed to be formulated avoiding any specific jargon and/or technical terms. As a result, now the LS can be an important tool for assessing the degree to which counseling professionals may listen psychoanalytically, without being aware of it and without expressly referring to psychoanalysis. The author recommends that future research on this instrument be conducted to determine its generalizability across different cultures.
This study had a few limitations. First, the LS represents a simple yet meaningful solution that has emerged from this study; however, there are many other ways to define psychoanalytic listening. Second, given its brevity, future research on psychoanalytic listening could consider the construction of longer multidimensional scales, as such scales are typically associated with higher reliability and more precise measurement. Third, professionals in this study may have found it socially desirable to report listening to a higher degree than they actually do in practice. In the process of scale construction, future research should consider adding more items that are negatively worded. Fourth, use of PAF implies a lack of generalizability of findings beyond the current sample. Finally, future research should also continue to evaluate the psychometric properties of the LS. Conducting confirmatory factor analysis is a recommended next step in this process, as this would assist with the stability of the factor structure that emerged in this study.
Footnotes
Appendix
The Listening Scale.

| Please Indicate the Response to the Right That Best Fits How Much You Agree or Disagree With the Following Statements Describing Your Counseling Practice | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Strongly Disagree | Moderately Disagree | Slightly Disagree | Slightly Agree | Moderately Agree | Strongly Agree | ||||
| 1 | 2 | 3 | 4 | 5 | 6 | ||||
| 1 I let clients start talking from where she or he prefers | 1 | 2 | 3 | 4 | 5 | 6 | |||
| 2 When I listen to a client, I listen to ambiguity and contradictions in his or her speech, what potentially opens to another possible meaning | 1 | 2 | 3 | 4 | 5 | 6 | |||
| 3 I encourage clients to reflect and question his or her own words | 1 | 2 | 3 | 4 | 5 | 6 | |||
| 4 My feelings and reactions to clients are meaningful to understanding them and their treatment | 1 | 2 | 3 | 4 | 5 | 6 | |||
| 5 Therapy proceeds depending whether I am really engaged, more than for the other techniques that I master | 1 | 2 | 3 | 4 | 5 | 6 | |||
| 6 I help clients formulate new questions, rather than giving them answers | 1 | 2 | 3 | 4 | 5 | 6 | |||
| 7 I follow the client’s associations rather than trying to impose a direction to the helping process | 1 | 2 | 3 | 4 | 5 | 6 | |||
| 8 I encourage clients to keep their questions open-ended | 1 | 2 | 3 | 4 | 5 | 6 | |||
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.