
Abstract
Objective:
To describe the quantitative validation of a unique questionnaire to measure moral distress among social workers in long-term care facilities in Israel.
Method:
Overall, 216 long-term care facilities’ social workers took part in the pilot study that included psychometric evaluation and construct validation. Moral distress was examined by two scales, measuring the frequency and the intensity of morally loaded events. A third scale was created, representing the product of the frequency and intensity scores for each item separately.
Results:
Two items with high floor effect were removed. The internal reliability of each of the three Moral Distress Scales was .92. An exploratory factor analysis suggested a single-factor solution. The construct validity was approved. In its final version, the questionnaire consisted of 15 items.
Conclusions:
We believe that the questionnaire can contribute by broadening and deepening ethics discourse and research with regard to social workers’ moral conflicts and moral distress.
Keywords
A prominent ethical dilemma in the theoretical literature on social work deals with the conflictual obligations of social workers, when their primary obligation to their clients is challenged by their obligation to the organization for which they work (Dogloff, Harrington, & Loewenberg, 2012; Linzer, 1999). This dilemma has emerged in qualitative studies which describe the difficulties of social workers to act in accordance with their primary obligation to the clients due to rules, regulations, and bureaucratic considerations (Hyde, 2012; Papadaki & Papadaki, 2008; Wilson, 2004) as well as due to commercial and reputational interests (Lev & Ayalon, 2016; (Lonne, McDonald, & Fox, 2004).
A theoretical and empirical concept, which is taken from the nursing literature and relates to these dilemmas, is called “moral distress.” Accordingly, moral distress occurs in situations where a nurse has difficulty acting in accordance with professional moral due to institutional constraints and restrictions (Jameton, 1984). This concept has been widely discussed and explored in the nursing literature and was more recently expanded in relation to other health professions (Corley, Elswick, Gorman, & Clor, 2001; Hamric & Blackhall, 2007). Nevertheless, very few studies have explored moral distress among social workers as a unique group (Houston et al., 2013; Mänttäri-van der Kuip, 2016).
Because it is expected that the experiences of social workers are quite different from those of nurses with regard to moral distress, it is important to develop a measure to assess moral distress among social workers. Such a measure is expected to increase awareness of the topic and potentially result in insights concerning those workers who experience the highest levels of moral distress and require further assistance in the form of educational interventions or additional supervision. The purpose of the present article is to describe the quantitative validation of a unique questionnaire which examines moral distress among social workers in long-term care facilities (LTCFs) in Israel. The description of the qualitative validation of the measure is detailed elsewhere (Lev & Ayalon, 2018).
Moral Distress
The definition of moral distress includes two essential elements: the existence of a moral phenomenon and an inconvenient psychological response to this phenomenon (Fourie, 2015). A significant conceptual extension emerged in a study by Kalvemark et al. (2004), which explored moral distress among health-care professionals. They suggested that moral distress occurs not only in situations where the health-care professional acts against his or her professional judgment but also in situations when he or she acts in accordance with it, but, in doing so, clashes with regulations. This implies that moral distress could be a result of any situation in which the actions of the health-care professional lead to a violation of an obligation either to the management or to the clients (Kälvemark, Höglund, Hansson, Westerholm, & Arnetz, 2004).
The most widely used instrument to measure moral distress is the Moral Distress Scale (MDS). This scale explores the frequency and intensity of 38 items, which reflect moral problems faced by nurses (Corley et al., 2001; Corley, Minick, Elswick, & Jacobs, 2005). The MDS has been the basis for many studies and was shortened or modified for use with different health-care professions (Hamric & Blackhall, 2007). These studies have indicated that moral distress was associated with organizational–environmental characteristics, such as perceived poor ethical climate (Corley et al., 2005; Hamric & Blackhall, 2007; Pauly, Varcoe, Storch, & Newton, 2009; Sauerland, Marotta, Peinemann, Berndt, & Robichaux, 2014, 2015), low levels of support and leadership, low satisfaction with the possibility to consult with colleagues, high instrumental leadership, and low supportive leadership (de Veer, Francke, Struijs, & Willems, 2013; McAndrew, Leske, & Garcia, 2011). In addition, positive associations have been found between moral distress and professional characteristics like dimensions of burnout (Meltzer & Huckabay, 2004) and intention to leave the job (Karanikola et al., 2014; Papathanassoglou et al., 2012; Piers et al., 2012). Finally, moral distress has been found to be negatively associated with psychological factors like empowerment (Browning, 2013; Ganz et al., 2013) and autonomy (Karanikola et al., 2014; Papathanassoglou et al., 2012).
Moral Distress and Social Work
Only very few studies have identified social workers as a unique group which requires its own scale for the purpose of assessing moral distress (Houston et al., 2013; Mänttäri-van der Kuip, 2016). The limited research on moral distress among social workers is unexpected due to the significant ethical component inherent in the social work profession (Openshaw, 2011; Weinberg, 2009). Unlike the nursing profession and other health professions which usually tend to involve life-and-death dilemmas, the ethical dilemmas faced by social workers tend to be less dramatic, tangible, or concrete (Weinberg, 2009). Therefore, ethical dilemmas that relate to the work experience of social workers are not reflected in the existing scales which are mostly intended to measure moral distress among nursing and other health-care professionals (Corley et al., 2001, 2005; Hamric & Blackhall, 2007).
A wider view of ethical dilemmas among social workers and the emotional reactions to them can be found in scales that examine stress and distress reactions to ethical issues. An empirical concept which has a similar meaning to moral distress and has emerged in the nursing literature is “ethical stress” which is experienced when the health-care professional is coping with ethical dilemmas (Raines, 2000). Similarly to moral distress, the measure has been examined among social workers, adapted from a scale developed for nurses (O’Donnell et al., 2008; Ulrich et al., 2007). In another study, a unique scale was developed to assess ethical stress among criminal justice social workers (Fenton, 2015). An additional empirical concept, which was examined among social workers and is unique to this profession, is termed “disjuncture.” This concept describes a dilemma that results in distress when there is a discrepancy between the social worker’s beliefs and behaviors (DiFranks, 2008).
LTCFs
LTCFs for the older adults in Israel are part of a spectrum of long-term care services for older adults (Brodsky, Shnoor, & Be’er, 2012). In Israel, LTCFs can be divided into two main categories: nursing homes for either individuals who require nursing care or older adults with mental impairments and old-age homes for functionally independent and semidependent frail older adults (Iecovich, 2001). Nursing homes and old-age homes serve about 3% of the individuals aged 65 and older in Israel. A third type of LTCF is the continuing care retirement community (CCRC). CCRCs provide housing and services for mostly functionally independent older adults (Ayalon & Green, 2012).
These three types of LTCFs have been portrayed on a continuum of autonomy versus control, with nursing homes being the most controlled institutions, where older adults have very limited autonomy, whereas CCRCs represent the other side of the spectrum as institutions which provide older adults with choice and self-determination. Nonetheless, LTCFs, especially nursing homes, have been described in the literature as possessing characteristics of total institutions (Lang, Löger, & Amann, 2007). These total features are often expressed by the desire for conformity and obedience (Solomon, 2004) and by a drive toward functional efficiency, which is reflected in a rigid daily routine, a lack of privacy and autonomy, and limited choice opportunities (Angelelli, 2006; Harnett, 2010). These features could potentially weaken the power of the residents when facing the management and staff (Nelson, 2000).
The imbalance in resources between the residents and the management/staff can make it difficult for social workers to act in accordance with their primary obligation to the residents (Allen, Nelson, & Netting, 2007; Fogler, 2009; Lev & Ayalon, 2015, 2016). The total features of LTCFs, on the one hand, and the role of social workers as advocates for the residents, on the other hand, could intensify the difficulties of social workers to act in accordance with their obligation to the residents and could lead to moral distress (Jameton, 1984).
A Questionnaire to Assess Moral Distress Among LTCF Social Workers
The construction of the present questionnaire was based on a secondary analysis of a qualitative study that addressed moral dilemmas of social workers in nursing homes in Israel (Lev & Ayalon, 2015, 2016). The data were analyzed on the basis of a predetermined typology (Given, 2008), which was derived from the theoretical and empirical definitions of moral distress (Fourie, 2015; Jameton, 1984; Kälvemark et al., 2004). Based on these definitions, three themes were identified and determined as the organizing framework of the questionnaire. The first theme encompassed respondents’ perceptions of the ethical behavior of the management or staff and how this related to their perceived inability to act in accordance with their obligation to the residents. The second theme addressed perceived actions in accordance with the obligation to the management and staff when respondents felt conflicting obligations toward the management versus residents, whereas the third theme addressed perceived actions in accordance with the obligation to the residents in these situations.
Following the definition of moral distress, which emphasizes the existence of a moral phenomenon and a psychological response to this phenomenon (Fourie, 2015; Jameton, 1984), the questionnaire included two scales. The first scale assessed the occurrence of a moral phenomenon and its frequency, and the second scale assessed the occurrence of distress in response to the phenomenon and its intensity.
Content validation included review and evaluation by two experts, a cognitive interview with nursing home social workers and three focus groups with experts and the target population. In its final version, the questionnaire consisted of 17 items which describe perceptions or actions related to possible conflictual situations for social workers in LTCFs. Participants were asked to rate the perceived frequency of moral dilemmas during the past year and to evaluate the intensity of the distress that followed these events. The frequency scale ranged between 0 = never, 1 = seldom, and 5 = often. The intensity scale ranged between 0 = not at all, 1 = low intensity, and 5 = high intensity. The construction and the content validation of the questionnaire are described in detail by Lev and Ayalon (2018). The Hebrew version of this scale is available from the corresponding author upon request.
The Present Study
The purpose of the present study is to describe a second stage of validation of the questionnaire designed to examine moral distress among LTCF social workers in Israel. This stage relied on a pilot study of LTCF social workers in Israel in order to establish the psychometric evaluation and construct validation of the questionnaire.
Method
Study Sample
To ensure a high participation rate, phone calls were placed by the first author to all LTCFs in Israel: 215 nursing homes, 94 integrated old-age homes (which include nursing departments), 75 old-age homes, and 185 CCRCs (Brodsky et al., 2012). Nursing homes and old-age homes were identified through Israel’s Ministries of Health and Social Affairs websites. The CCRCs were located through different private and public websites. The first author introduced herself and the study and asked for permission to contact the social workers employed in the facility for the purpose of conducting the study. After permission was obtained, the questionnaires were sent via e-mail or post and collected through a Google Drive application, e-mail, fax, or post based on the preference of the participants. In some occasions, the first author came to the facility and provided a lecture on the research topic after the social workers in the facility answered the questionnaire. Additionally, some participants were located through conferences and courses targeting this population. In summary, 216 questionnaires were collected.
No official information was available regarding the exact number of social workers in LTCFs in Israel. However, it can be assumed that there are around 250–300 social workers employed in nursing homes and old-age homes in Israel based on the standard of one social worker to 100 beds (Brodsky et al., 2012). This does not represent an exact number because some of the social workers are employed in more than one facility or work part time. Because there are no standards for social work services in CCRCs, we have no appraisal of the exact number of social workers in these facilities. We do know, however, that of the 343 institutes that were approached, 302 agreed to participate in the study.
The study population included 216 social workers employed in nursing homes (37.7%), old-age homes (12.7%), integrated old-age homes (32.5%), and CCRCs (17%). The majority (91%) were women, 58% of them had a bachelor’s degree, 41% had a master’s degree, and 1% (two participants) had a PhD. Their ages ranged between 23 and 77.
Study Procedure and Analysis
The study was approved by the ethics committee of the authors’ university. All participants received a comprehensive explanation about the study prior to giving their informed consent to participate in the study. Three scales were assessed. Scales consisted of the frequency with which the event occurred, the intensity of the moral distress associated with it, and a multiplication of these two scales, which reflects the overall moral distress.
The psychometric evaluation of the three scales was established by obtaining floor and ceiling effects, internal reliability, a frequency distribution, and exploratory factor analysis. A floor effect refers to a high percentage of respondents who gave the lowest possible score (never or not at all), whereas a ceiling effect refers to a high percentage of respondents who marked the highest possible score (often or high intensity; Alexander et al., 2005). Recent studies have distinguished between “significance effect,” which indicates a percentage above 20 at floor or at ceiling, and “high effect,” which indicates a percentage above 70 at floor or at ceiling. These studies recommended the removal of items with high effects (above 70%) because these items are likely limited in their responsiveness to clinical change (Alexander et al., 2005; Cheng et al., 2007).
The construct validity of the questionnaire was established by examining both convergent validity (strong correlations of the scales with variables that theoretically were expected to be significantly related to it) and discriminant validity, which corresponds to low correlations of the scales with variables that theoretically were predicted to be less related with moral distress (Collins, Onwuegbuzie, & Sutton, 2006).
Convergent validity was established in relation to two environmental variables which were found to be negatively correlated with moral distress: ethical climate (Hamric & Blackhall, 2007; Pauly et al., 2009) and support in the workplace (de Veer et al., 2013; McAndrew et al., 2011) and two variables, that related to professional attitudes, which were found to be positively correlated with moral distress: emotional exhaustion and depersonalization as part of the burnout scale (Meltzer & Huckabay, 2004; Ohnishi et al., 2010) and intention to leave the job (Karanikola et al., 2014; Papathanassoglou et al., 2012; Piers et al., 2012).
Discriminant validity was established against constructs which were predicted not to be strongly correlated with moral distress. These constructs relate to the “personal accomplishment” factor in the burnout scale (Maslach, Jackson, & Leiter, 1986), which was found in previous studies to have only a weak correlation or no correlation whatsoever with moral distress (Meltzer & Huckabay, 2004; Ohnishi et al., 2010). An additional construct was the “support from friends and relatives” factor in the support scale (Lindström et al., 2000), which was not tested in previous studies due to the absence of a theoretical rationale for such a relationship.
Measures
In addition to the moral distress questionnaire, social workers were asked to provide sociodemographic information including gender, age, marital status, religion, strength of religious beliefs, country of origin, education, and seniority as social workers. Additionally, social workers were asked about the type of institution and population they work with. In order to establish convergent validity, the following questionnaires were included in the pilot study.
Ethical environment
Ethical environment was measured by the Ethical Environment Questionnaire. The scale consists of 20 items (e.g., “The administration of this organization is concerned with ethical practice”). Participants are asked to rate their level of agreement on a 5-point scale that ranges between “strongly disagree (1) and strongly agree (5; McDaniel, 1997). The scale was translated to Hebrew and then back translated to English by independent translators. Internal consistency in the present study was .95.
Support
The support questionnaire was taken from the General Nordic Questionnaire for psychological and social factors at work. The questionnaire consists of 8 items that encompass three sources of support from superiors (3 items, e.g., “If needed, is your immediate superior willing to listen to your work-related problems?”), coworkers (2 items, e.g., “If needed, can you get support and help with your work from your coworkers?”), and friends and relatives (3 items, e.g., “If needed, can you talk with your friends about your work-related problems?”). Participants were asked to rate their level of support on a 5-point scale, which ranges between very seldom or never (1) and very often or always (5; Lindström et al., 2000). The scale was translated to Hebrew and then back translated to English by independent translators. Internal consistency in the present study was .85, .82, and .76, respectively.
Burnout
Burnout was measured using the Hebrew version of the Maslach Burden Inventory. The inventory consists of 22 items that encompass three aspects of the job experience: emotional exhaustion (9 items, e.g., “I feel emotionally drained from work”), depersonalization (5 items, e.g., “I become more callous toward people”), and personal accomplishment (8 items, e.g., “I can easily understand patients’ feelings”). Participants were asked to rate each statement on a 7-point scale. More burnout is indicated by a higher score on the emotional exhaustion and depersonalization scales and a lower score on the personal accomplishment scale (Maslach & Jackson, 1986). A Hebrew translation of the scale was used (Ayalon, 2008). Internal consistencies in the present study were .90, .76, and .81, respectively.
Intention to leave the job
Intention to leave was measured by the turnover intentions questionnaire. The scale consists of 3 items. Participants are asked to rate their level of agreement with several statements on a 5-point scale (e.g., “I think a lot about leaving the organization”) with a higher score, indicating greater agreement (Cohen, 1998). The scale was translated to Hebrew and then back translated to English by independent translators. Internal consistency in this study was .90.
Results
The data were analyzed using SPSS, Version 23, for Windows. Due to the nature of the questionnaire and in accordance with the instructions provided to respondents, we treated items that were ignored with regard to the frequency and intensity scales as irrelevant to the respondent’s work experience. Therefore, 43 missing values on the frequency scale and 322 values on the intensity scale were replaced by a 0 score.
Of the 17 items, 14 items on the frequency scale and 15 items on the intensity scale had a significant floor effect (see Table 1). A high floor effect was evident for Item 12 (I felt that there has been an expectation of me to conceal or to give false information in situations where there is suspicion of abuse) and 13 (I acted in a way which was in contradiction with my professional beliefs due to concerns of losing my job) with regard to both the frequency and intensity scales (see Table 1). The high floor effects imply that the phenomenon described by these items can be considered as extreme and do not represent the work experience of LTCF social workers. Therefore, these 2 items were removed. A ceiling effect was not observed for any of the items.
Frequencies and Floor and Ceiling Effects.

After the removal of the 2 items, a third scale was created consisting of the multiplication of frequency and intensity items. The means and standard deviations of the items on the three scales are detailed in Table 2. With the possible range of scores between 0 and 6 for each scale, the mean score for the frequency scale was 1.36 ± 92 (range 0.62–2.19) and 169
Means and Standard Deviations.
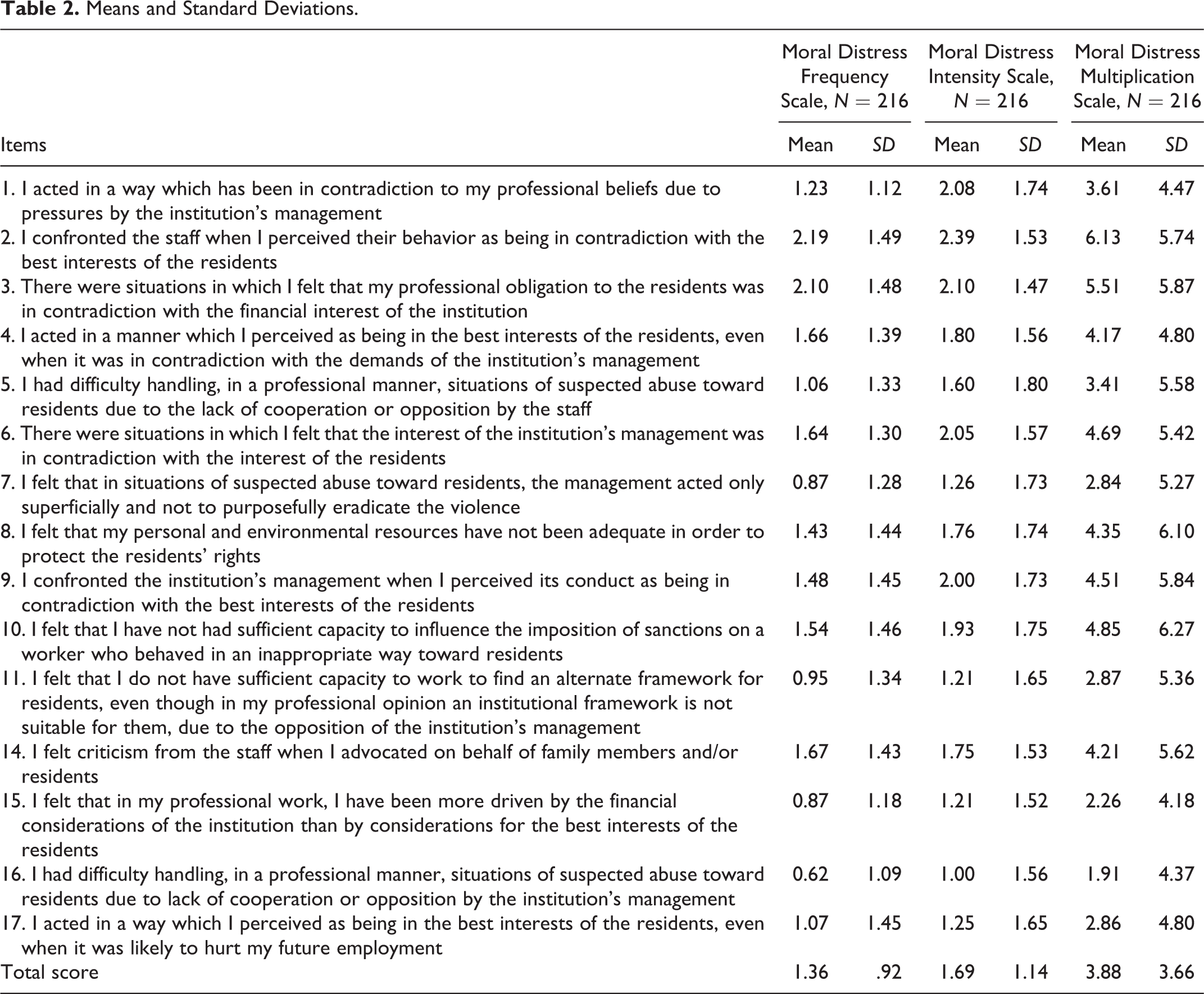
The items which received the lowest mean score on the frequency scale were Items 16 and 7, which correspond to perceived inadequate response of the management to suspected abuse. Similarly to the frequency scale, the items which received the lowest mean score on the intensity scale were Item 16, followed by Items 11 and 15, which had the same mean score. Item 11 addresses the perceived difficulties of the social worker to find an alternate framework for residents due to the opposition of the management, and Item 15 describes the social worker’s feelings that his or her professional work has been driven by the financial considerations of the institution more than by considerations for the best interests of the residents.
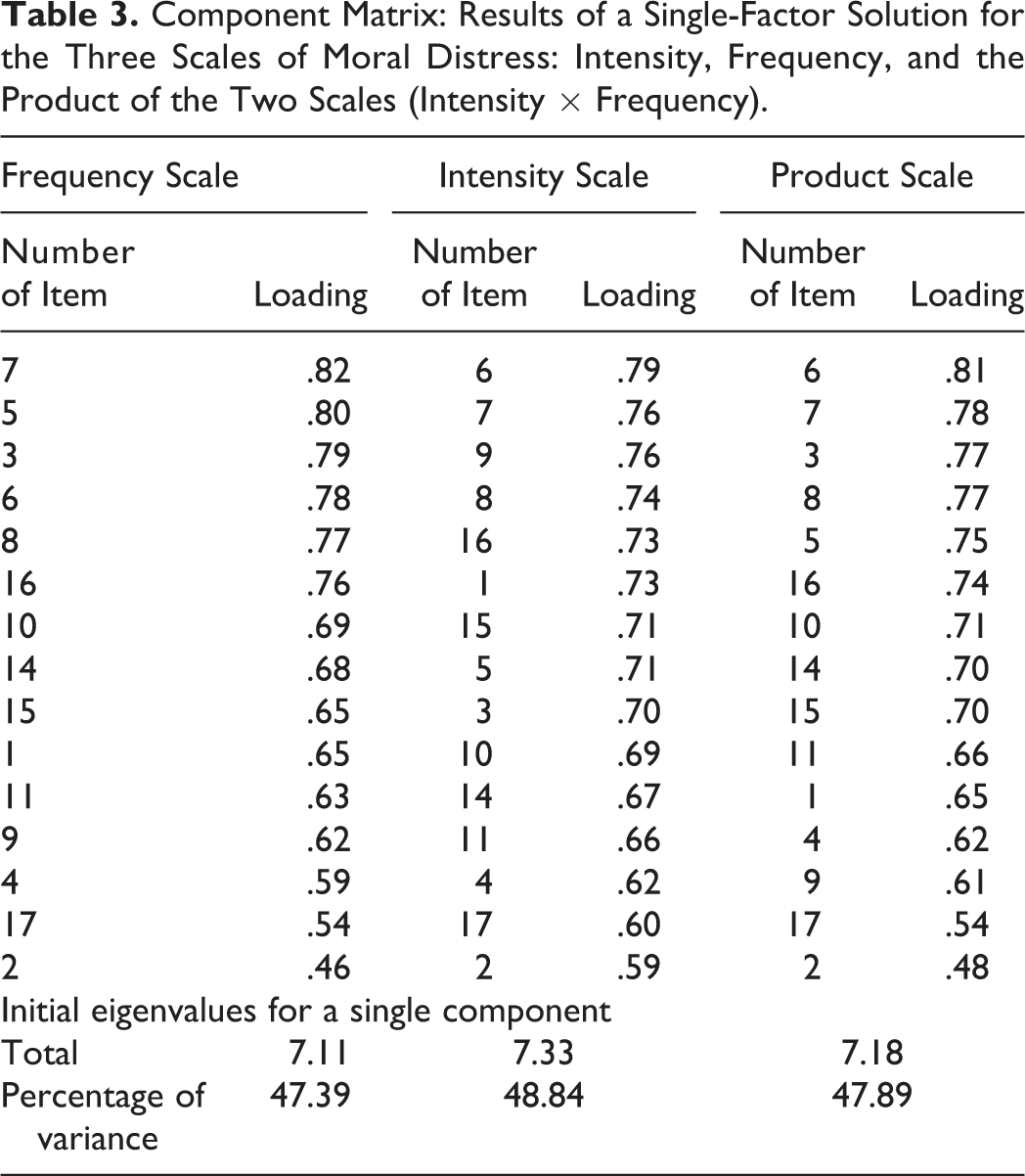
An exploratory factor analysis was separately established for each scale. For all three scales, the scree tests indicated that the break between a steep slope and leveling off occurred after a single factor (reflected in the drop of the total eigenvalues from 7.11–7.33 for a single component to 1.3–1.5 for two components). This suggests that each scale can be explained by a single factor that accounts for more than 47% of the variance (see Table 3). All item loadings were greater than .40 (see Table 3) and, therefore, indicated their adequate association with the respective factor (Costello & Osborne, 2005).
Component Matrix: Results of a Single-Factor Solution for the Three Scales of Moral Distress: Intensity, Frequency, and the Product of the Two Scales (Intensity × Frequency).
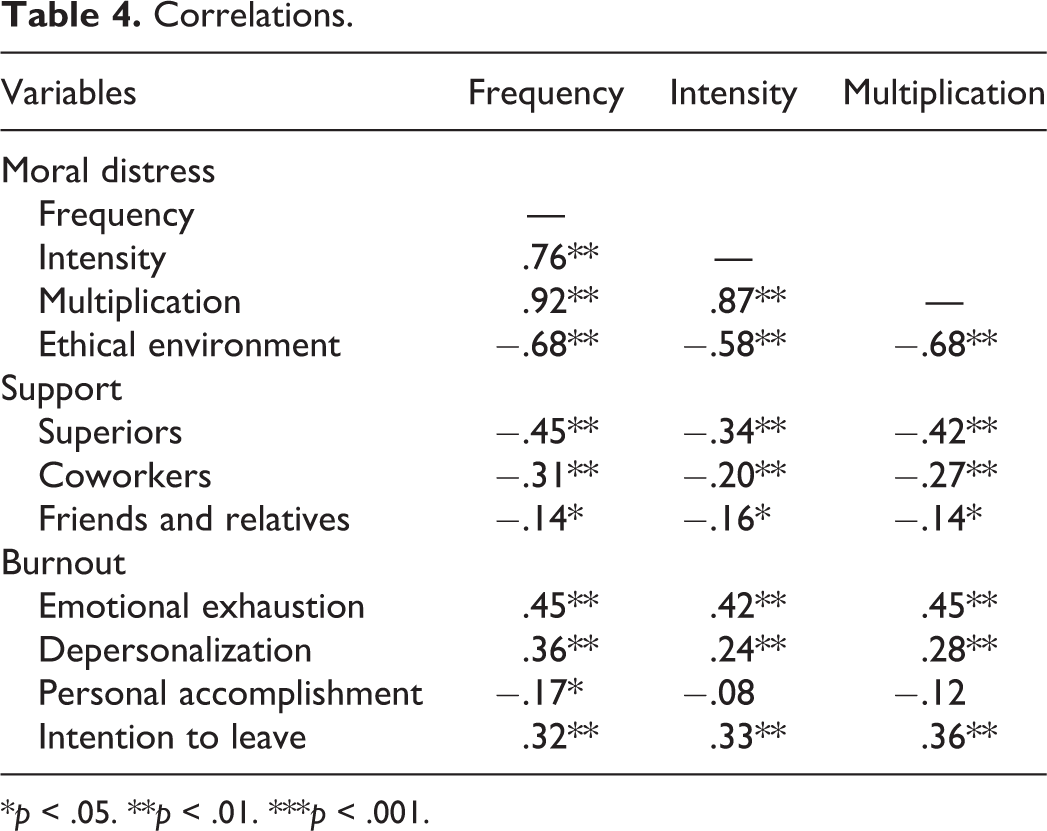
Reliability was assessed by determining Cronbach’s α coefficient for each of the three MDSs. The Cronbach’s α coefficients were .92 for all the three scales. The correlations between the three scales resulted in strong positive correlations (see Table 4), which indicating a potential for multicollinearity (Pallant, 2013).
Correlations.
*p < .05. **p < .01. ***p < .001.
Pearson correlations were computed to assess the construct validity of the questionnaire (see Table 4). The convergent validity indicated high negative correlations of the three MDSs with ethical environment and moderate negative correlations with superior support. The three MDSs had positive moderate correlations with emotional exhaustion and intention to leave the job. Moral distress frequency had a moderate negative correlation with coworker support and a moderate positive correlation with depersonalization, whereas the two other MDSs had weak negative correlations with coworker support and weak positive correlations with depersonalization.
The discriminant validity resulted in weak negative correlations of the three scales with support from friends and relatives. In addition, personal accomplishment had a weak negative correlation with moral distress frequency and no significant correlation with the two other MDSs.
Discussion and Applications to Practice
The present article describes the second stage of validation of a questionnaire to assess moral distress among social workers in LTFCs. The term moral distress includes both a moral phenomenon and an inconvenient psychological response to this phenomenon (Fourie, 2015; Jameton, 1984). Following this definition, for each item separately, we assessed the frequency of the perceived moral phenomenon and the intensity of the distress that followed it (Corley et al., 2005; Hamric & Blackhall, 2007). In order to assess the level of moral distress, we created a third scale that represents the product of the frequency and intensity scores for each item separately (Hamric & Blackhall, 2007). The strong positive correlation between the three MDSs indicates a potential for multicollinearity (Pallant, 2013). Because of this multicollinearity, the multiplication scale, which is based on the frequency and intensity scales, is recommended for use in future studies.
The findings indicate that the moral phenomena, described by several different items, were relevant to the work experience of most participants and were accompanied by some distress. However, an examination of the distribution of the items with regard to the frequency and intensity scales indicated significant floor effects for most of the items in both scales (above 20% of respondents had the lowest possible score). These significant floor effects could be explained by the unique nature of the present questionnaire. The questionnaire was expected to be positively skewed because the items described negative and even extreme moral phenomena, such as not reporting abuse of older adults.
The moderately low levels of moral distress frequency and intensity in the present questionnaire are consistent with other studies that explored moral distress among nurses. Oh and Gastmans (2013) found in their review of studies exploring moral distress among nurses that seven of the eight studies reported low frequency of moral distress events. However, unlike the present study, most of the studies found moderately high levels of moral distress intensity among nurses, whereas only two studies of nine reported low levels of moral distress intensity (Oh & Gastmans, 2013).
A notable finding is that of the 4 items, which had the greatest floor effect and the lowest mean with regard to frequency, three addressed the perceived inadequate response of the management to suspected abuse (Items 12, 16, and 7, respectively). The low frequency can be explained by the extreme nature of the events that were described by these items. Although most of the respondents reported not experiencing these events, we decided to remove only Item 12 (due to its high floor effect) and to leave the remaining items. The reason for this is embedded in the severe potential implications of abuse to the residents’ confidence and well-being (Castle, Ferguson-Rome, & Teresi, 2015; Lindbloom, Brandt, Hough, & Meadows, 2007). Hence, we believe these events should be addressed even if they occur at a low frequency.
The exploratory factor analysis indicated that each of the three MDSs could be explained by a single factor. These findings are notable due to the different and even opposing themes that were included in the questionnaire. The themes were created based on the moral distress definition by Kalvemark et al. (2004) and included items which described the difficulty of the social worker to act in accordance with his or her moral and professional obligation to the residents due to institutional restrictions and also items which described actions of the social worker in accordance with his or her moral and professional obligation to the residents, despite institutional restrictions. Thus, the findings of the exploratory analysis support the qualitative findings of Kalvemark et al. (2004) that moral distress could be a result of any situation in which the actions of the health-care professional lead to a violation of an obligation either to the management or to the clients. Although all of the items belonged to a single factor (Costello & Osborne, 2005), the 4 items with the lowest loadings in the frequency and product scales described actions of the social worker in accordance with his or her obligation to the residents, which could represent somewhat different qualities of moral distress.
Finally, we provided evidence for the construct validity of the present questionnaire. The strong negative correlations of the three scales of moral distress with the ethical environment scale imply that the moral distress questionnaire addresses the environmental aspects present in the LTCF. This is reflected by items that contain explicit and implicit descriptions of the perceived behavior of the management concerning ethical issues. However, unlike scales which measure the ethical environment, most of the items in the moral distress questionnaire also assessed the passive or active reactions of the social worker to that environment.
As noted, the moral distress questionnaire is based on a secondary analysis of a qualitative study that addressed moral dilemmas of social workers in nursing homes in Israel (Lev & Ayalon, 2015, 2016). Based on qualitative content validation (Lev & Ayalon, 2018), psychometric evaluation, and construct validation, the questionnaire has expanded its relevance to LTCFs social workers in Israel. Nevertheless, because the questionnaire was developed and validated in Israel, its adjustment to other cultures or countries requires sensitivity to possible cultural or contextual differences. These differences can be reflected in the structure of the LTCFs, the target population, or the supervision and the role definition of the social workers in these facilities. Hence, future research will benefit from examining the psychometric properties of this measure in different sociocultural contexts.
Another limitation of the present questionnaire is reflected in the fact that all items are long and unidirectional. This might cause a response bias, when early items trigger the response pattern (Tourangeau & Rasinski, 1988). Furthermore, the significant moral component that is embedded in the questionnaire might elicit a social desirability bias, as the respondents might respond in a manner that is viewed favorably by others (Paulhus, 1991). However, because of the nature of the questionnaire, which examines moral phenomena and the distress that followed them, we could not formulate items in a positive direction. It is important to note that this is similar to other MDSs (Corley et al., 2001; Hamric & Blackhall, 2007). Future research might use social desirability scales for control purposes (Paulhus, 1991).
Finally, the present moral distress questionnaire is based on a self-report, monomethod approach. Exploring the perceptions and attitudes of other professionals in LTCFs or the residents themselves as well as adding other measurement tools, like observations, could enrich our understanding of moral distress among LTCFs social workers.
We believe that the importance of the current questionnaire stems from the fact that distress not only impacts the well-being of social workers in LTCFs but also has severe implications to the well-being and safety of LTCFs’ residents (Castle et al., 2015; Lindbloom et al., 2007). The implications of moral distress to the well-being of the residents could be due to the difficulties of the social worker to protect the residents’ rights and safety because of institutional constraints and restrictions. The implications could also be indirect, due to emotional exhaustion and depersonalization, which are reflected in negative and cynical attitudes and feelings of the social worker toward the clients (Maslach et al., 1986).
We believe that the questionnaire will contribute by broadening and deepening ethical discourse and research with regard to social workers’ obligational dilemmas and conflicts, in an era in which rules, regulations, and bureaucratic considerations as well as commercial and reputation interests of the organization, make it increasingly more challenging for social workers to act in accordance with their obligations to their clients (Abramovitz, 2005; Lev & Ayalon, 2015, 2016; Lonne et al., 2004; Papadaki & Papadaki, 2008; Wilson, 2004). Ethical discourse and research are particularly important in an era where neoliberalism and privatization have spread worldwide and are responsible for a transition of social services from governmental ownership to public and private ownership (Carey, 2008; Liljegren, Dellgran, & Höjer, 2008). Although the questionnaire was built and validated for assessing moral distress among LTCF social workers, it could be adjusted and extended to social workers who work in other institutions characterized by “total” features like boarding schools and institutions for people who suffer from cognitive, physical, or mental disabilities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.