
Abstract
Objective:
The feasibility and acceptability of CHOICES-TEEN—a three-session intervention to reduce overlapping risks of alcohol-exposed pregnancy (AEP), tobacco-exposed pregnancy (TEP), and HIV—was assessed among females in the juvenile justice system.
Method:
Females aged 14–17 years on community probation in Houston, TX, were eligible if presenting with aforementioned health risks. Outcome measures—obtained at 1- and 3-months postbaseline—included the Timeline Followback, Client Satisfaction Questionnaire-8, session completion/checklists, Working Alliance Inventory–Short, and open-ended questions. Twenty-two participants enrolled (82% Hispanic/Latina; mean age = 16).
Results:
The results suggest strong acceptability and feasibility with high client satisfaction and client/therapist ratings, 91% session completion, and positive open-ended responses. All youth were at risk at baseline, with the following proportions at reduced risk at follow-up: AEP (90% at 1 month, 71.4% at 3 months), TEP (77% of smokers [n = 17] at reduced risk at 1 month, 50% at 3 months), and HIV (52.4% at 1 month, 28.6% at 3 months).
Adolescent females detained or on probation in juvenile justice settings often engage in multiple health behaviors that place them at risk of HIV and substance-exposed pregnancies (Lawrence, Snodgrass, Robertson, & Baird-Thomas, 2008; Rosengard et al., 2006). Specifically, they engage in frequent sexual behaviors that put them at risk of unplanned pregnancy, sexually transmitted infections (STIs; Belenko et al., 2008), and HIV (Committee on Pedatric AIDS, 2006) while also smoking (Helstrom, Bryan, Hutchison, Riggs, & Blechman, 2004) and engaging in alcohol use (Lawrence et al., 2008), which further place them at risk of both tobacco-exposed pregnancy (TEP) and alcohol-exposed pregnancy (AEP; Delpisheh, Attia, Drammond, & Brabin, 2006; Helstrom et al., 2004).
There are well-documented health consequences of smoking and drinking during pregnancy for both female youth and the fetus (Delpisheh et al., 2006; Kulig, 2005; Wiemann & Berenson, 1998). While many cease alcohol or cigarette use after discovering they are pregnant (Forray, Merry, Lin, Ruger, & Yonkers, 2015), nearly half of the U.S. pregnancies are unplanned (Finer & Zolna, 2016) with females unaware of their pregnancy continuing to drink or smoke during the early and critical weeks of gestation. Compared with adult women, adolescents are more likely to have an unplanned pregnancy, take longer to recognize they are pregnant (De Genna, Larkby, & Cornelius, 2007), and are less likely to reduce alcohol or tobacco consumption once they find out they are pregnant (Cornelius et al., 1994), putting them at higher risk of TEP or AEP. These pregnancies are also at risk for mother-to-child HIV or STI, as many of these youth may not seek early or regular prenatal care (CDC, 2018a).
The association between substance use and STI/HIV sexual risk behavior among youth is well-documented, with younger, female, and racially/ethnic minority populations at highest risk of HIV infection through heterosexual contact (CDC, 2018b; Howard & Wang, 2004). Co-occurring substance use and sexual risk behaviors are more pronounced among juvenile justice populations, with females in these settings presenting with a unique, multirisk profile (Rosengard et al., 2006; Teplin, Mericle, McClelland, & Abram, 2003). While nationally representative samples are generally lacking for this population, several trends have been identified in the literature. Alcohol use and smoking are more prevalent and comorbid among females in criminal justice settings (Helstrom et al., 2004; Parrish et al., 2011), with delinquent adolescent females reporting more frequent smoking than males and nearly a third meeting clinical criteria for a substance use disorder (Cropsey, Linker, & Waite, 2008; Domalanta, Risser, Roberts, & Risser, 2003; Helstrom et al., 2004; Lederman, Dakof, Larrea, & Li, 2004). In addition, most (90%) are sexually active and less than half use condoms or contraception (Crosby et al., 2004; Kingree, Braithwaite, & Woodring, 2000; Lawrence et al., 2008; Teplin et al., 2003). Approximately a third of female youth in these settings have previously been pregnant one or more times (Lawrence et al., 2008; Lederman et al., 2004; Schmiege, Broaddaus, Levin, & Bryan, 2009). Compared with community female youth samples, this population engages in earlier and more frequent sexual risk behavior with multiple partners (Lederman et al., 2004).
Females in juvenile justice settings are also consistently at high risk of STIs and sexually transmitted HIV compared to their noninvolved peers and at an even higher risk than their male involved counterparts (Belenko et al., 2008), reporting less frequent condom use (Belzer et al., 2001; Broaddus & Bryan, 2008; Committee on Pedatric AIDS, 2006; Kelly, Lesser, & Paper, 2008; Robertson, Stein, & Baird-Thomas, 2006) and more frequent acquisition of STIs placing them at further risk of HIV infection (CDC, 2018a).
Despite this population’s unique, multirisk health profile and the critical opportunity to intervene while youth are on community probation, there is a paucity of gender-specific prevention programming to reduce these risks (DiClemente et al., 2014; Lawrence et al., 2008). This presents a challenge for prevention and highlights an urgent need to develop efficacious, gender-specific, multirisk “bundled” (targeting more than one behavior) prevention approaches for this vulnerable population (Belenko et al., 2008; Committee on Pediatric AIDS, 2006; Ickovics, 2008). Bundling efficiently aggregates services to promote synergistic gain when intervening with high-risk populations that do not routinely seek services (Ickovics, 2008) and is increasingly being used in medical or other opportunistic settings. While not yet tested with adolescents, a bundling (Ickovics, 2008; Parrish et al., 2011) or multiple-behavior approach (Geller, Lippke, & Nigg, 2017; Nigg, Allegrante, & Ory, 2002) has shown promise in more efficiently reducing health risk behavior (Werch, 2007). There is a need, however, to conduct research to better understand which and how many behaviors can be bundled and for which target populations (Werch, 2007).
The CHOICES Line of Research and CHOICES-TEEN
One possibility to meet these overlapping needs among the female juvenile justice population is to adapt an existing empirically supported prevention intervention for adult women called the CHOICES preconception intervention. This intervention utilizes the transtheoretical model of behavior change, motivational interviewing (MI), and content aimed to increase participants’ motivation to change risky alcohol use, smoking, and contraception use, along with a referral for contraception education and services (Velasquez, von Sternberg, & Parrish, 2013). The need for the CHOICES intervention and its efficacy has been demonstrated through a line of epidemiological and intervention research funded by the Centers for Disease Control and Prevention (CDC; Floyd et al., 2007; Project CHOICES Intervention Research Group, 2003; Velasquez et al., 2017). In the first multisite randomized controlled trial testing the efficacy of a four-session version of CHOICES among high-risk women of childbearing age (18–44), the CHOICES intervention group, relative to a brief advice group, significantly reduced their risk of AEP (69.1% vs. 54.3%) and had 2-fold greater odds of being at reduced risk of AEP at 9 months (Floyd et al., 2007). This intervention has been broadly disseminated to the public, with the original manual and related training materials available on the CDC website (https://www.cdc.gov/ncbddd/fasd/choices-implementing-choices.html). This first aforementioned efficacy study highlighted the need (and opportunity) to also prevent nicotine-exposed pregnancies, as more than 70% of those at risk of AEP were also smoking (Floyd et al., 2007). Analysis of study data also indicated that women receiving two sessions were as likely to reduce their risk of AEP as those receiving four. Consequently, a second efficacy trial was funded by the CDC to test a two-session version of CHOICES, called CHOICES Plus, that would also focus on reducing the overlapping risk of TEP within a large, public medical setting (Velasquez et al., 2017). This study also supported the efficacy of CHOICES Plus in significantly reducing the risk of both AEP and TEP among women aged 18–44 years compared to a brief advice group (Velasquez et al., 2017).
CHOICES-TEEN was adapted from the original CHOICES and CHOICES Plus preconception interventions to be developmentally appropriate for adolescent females and reduced HIV/STI risk in addition to reducing risks of AEP and TEP (Floyd et al., 2007; Project CHOICES Intervention Research Group, 2003; Velasquez et al., 2010; Velasquez et al., 2017). CHOICES-TEEN builds upon the CHOICES line of research by expanding the reach of this intervention to high-risk adolescent females who are—compared to adult women—more likely to have an unplanned pregnancy, take longer to realize they are pregnant, and less likely to stop using substances once they realize they are pregnant (Cornelius et al., 1994; Cnattingius, 2004; De Genna et al., 2007). This intervention, which will be described in more detail in the Methods section, consists of two sessions with a master’s level counselor, a session with an adolescent medicine specialist to discuss HIV/STI and pregnancy prevention, possible referral for HIV/STI testing and contraceptive services, and a referral to a phone-based smoking cessation program called the Texas Quitline. The intervention was delivered to female youth on intensive juvenile community probation.
The aims of this one-arm pilot study were to further understand the feasibility of targeting multiple bundled health risks in high-risk adolescents as well as to evaluate the feasibility and potential promise of an adapted gender-specific prevention intervention—CHOICES-TEEN—in reducing the risks of HIV/STI, TEP, and AEP among adolescent females on community probation.
Materials and Method
Following Stage 1a/1b intervention development guidelines (Rounsaville, Carroll, & Onken, 2001), a one-arm design was used to assess the reductions of risk (among an all-risk sample at baseline) following the CHOICES-TEEN intervention at 1- and 3-month follow-up. Supplemental data were collected to assess client adherence, retention, acceptability, and the feasibility and quality of treatment delivery. Data were collected by research assistants trained in the study protocol. This study was approved by the Harris County Juvenile Justice, University of Houston and University of Texas Health Science Center at Houston Institutional Review Boards.
Female adolescents aged 14–17 years were recruited from three community probation programs in Houston, TX. Youth assent and the parent/guardian permission were obtained in person or by phone to conduct eligibility screenings. To be eligible, participants were at risk of HIV/STI, AEP, and TEP and had all of the following behaviors in the prior 3 months: (1) sexual intercourse with a male, (2) inconsistent/ineffective condom use, (3) inconsistent/ineffective contraception use, (4) drinking at risky levels (>3 drinks in 1 day or >7 drinks in a week), and (5) current smoking. Given that this was a feasibility study, and the initial recruitment numbers were lower than expected, the smoking inclusion criterion was relaxed after 6 months to ensure an adequate sample. Of the 150 females screened, 31 (21%) were at risk of both AEP and TEP and 37 (25%) at risk of AEP. If eligible, the voluntary nature and details of the study were described to the youth and guardian using IRB-approved assent and permission documents, questions were elicited and answered, and written informed consent was obtained from youth and parent/guardians prior to study participation. As shown in Figure 1, three (8.1%) declined participation and six (16.2%) did not return to the site for various reasons (e.g., additional criminal charges and noncompliance with the program). Of the 28 who returned for assent/parental permission and baseline assessment, 2 were identified as ineligible, leaving a pool of 26 from which 4 did not return for similar aforementioned reasons. Of the 22 participants who started the intervention, 20 completed all three sessions (91%) and 2 completed one session. One- and 3-month follow-up assessments were obtained for all 21 of the 22 (95%) youth who received the intervention. While two youth initiated the smoking Quitline fax referral, none of them completed this component of the program.
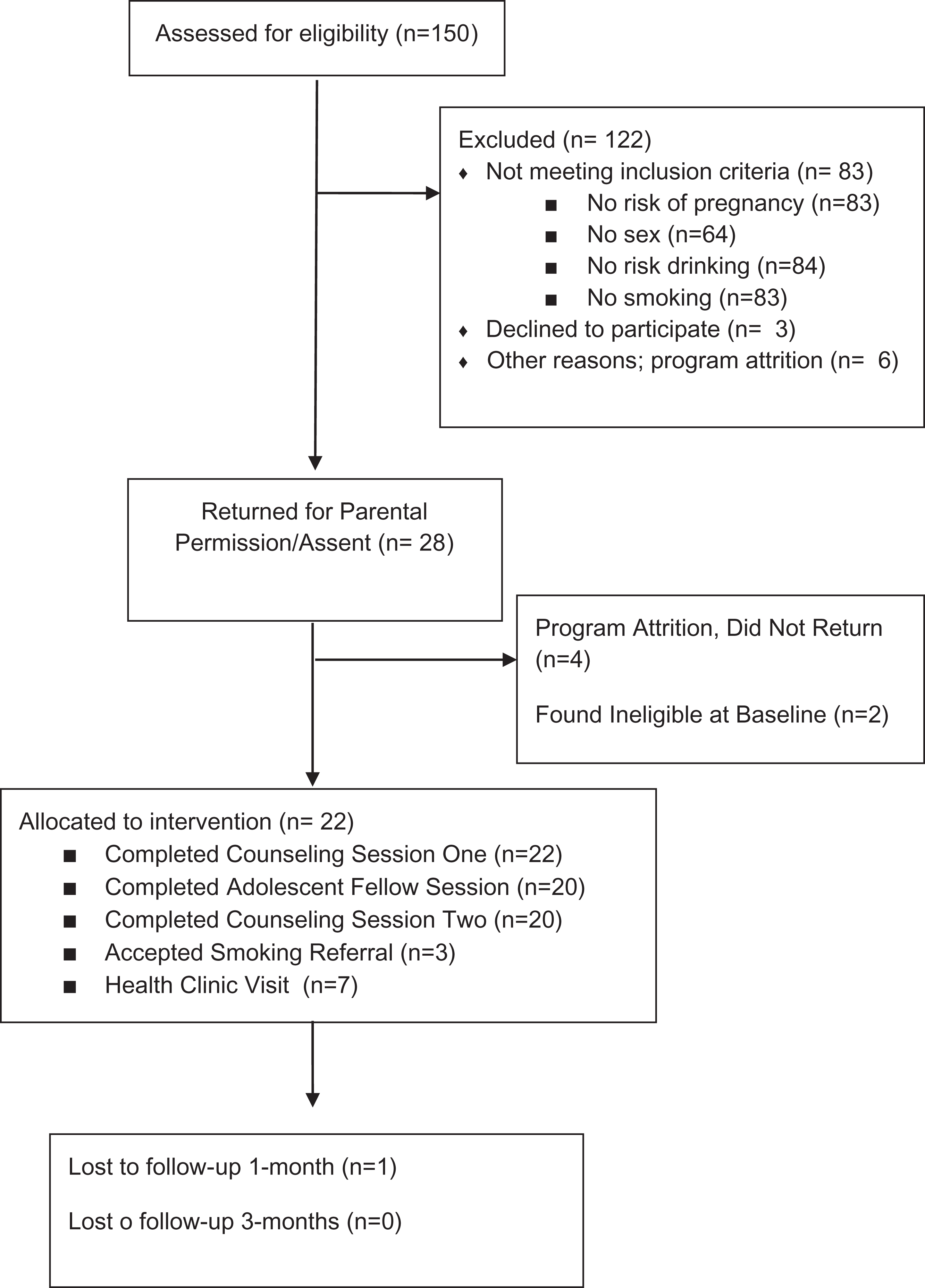
Study flow diagram.
CHOICES-TEEN Intervention
CHOICES-TEEN was adapted from the original CHOICES and CHOICES Plus preconception interventions to be developmentally appropriate for adolescent females and reduced HIV risk (Floyd et al., 2007; Project CHOICES Intervention Research Group, 2003; Velasquez et al., 2010, 2017). The efficacy of the CHOICES and CHOICES Plus bundled preconception interventions in reducing the risks of AEP and TEP among adult women in high-risk settings has been established through a series of CDC-funded studies (Floyd et al., 2007; Project CHOICES Intervention Research Group, 2003; Velasquez et al., 2017). CHOICES-TEEN builds upon this work by expanding the reach of this intervention to high-risk adolescent females. As shown in Table 1, CHOICES-TEEN includes two motivational counseling sessions with a master’s level counselor, one session with an adolescent medicine physician, and a referral to the Texas Tobacco Quitline. The Quitline accepts fax referrals from physicians of youth who are ready to quit smoking. A Quitline counselor then assesses the youth for one or more of the following referrals: telephone counseling, community-based cessation services, and youth friendly smoking cessation materials.
CHOICES-TEEN Intervention Session Components.
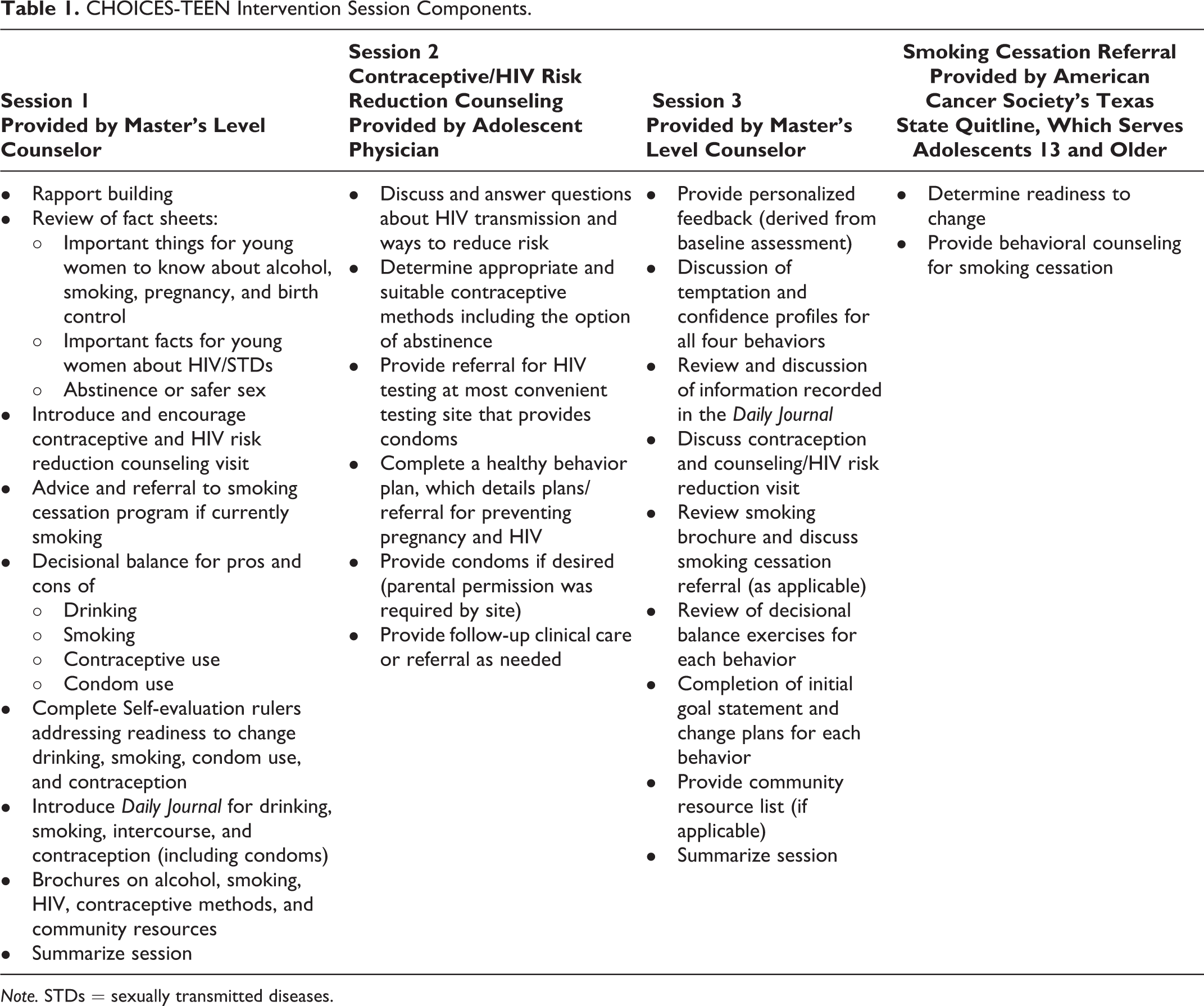
Note. STDs = sexually transmitted diseases.
Master’s level counselors, previously trained for prior CHOICES intervention studies, provided the counseling sessions and were supervised by experts in MI and the CHOICES-TEEN intervention. The majority of sessions (68.2%) were provided by one of the three master’s level counselors, and outcome did not differ by counselor at 3-month outcome. All sessions were audio-recorded, and 15% were reviewed for quality and fidelity using the Motivational Interviewing Integrity Scale 3.1.1 and CHOICES-TEEN protocol checklist. All counselors were deemed as proficient in the intervention by a CHOICES expert who is also a member of the Motivational Interviewing Network of Trainers. The adolescent medicine physicians, who provided the second session focused on HIV and pregnancy risk reduction education and the development of a healthy behavior plan, received a 3-hr training on the use of MI in a medical context and the CHOICES-TEEN protocol.
Measures
Demographic and background health variables
Demographic and background health variables, including sexual activity/risk behaviors and substance use history/frequency, were collected using an audio computer-assisted self-administered interview (ACASI). The AUDIT, a 10-item questionnaire used to measure alcohol use and problems, was also used to describe the sample with regard to harmful drinking (Babor, de la Fuente, Saunders, & Grant, 1992).
Timeline followback interview (TLFB)
The TLFB interview, which collected detailed self-report behavior data using a calendar recall method, was administered by a trained interviewer at baseline (i.e., 90 days prior), 1-month postbaseline follow-up, and 3-month postbaseline follow-up (Floyd et al., 2007; Sobell, Brown, Leo, & Sobell, 1996; Velasquez et al., 2017). Data collected included number of daily alcohol drinks, sexual activity, condom use, effective contraception, and smoking. These data were divided into 30-day increments to calculate the following: (1) risk drinking (>3 drinks in 1 day or >7 drinks in a week), (2) risk of pregnancy (any occurrence of vaginal intercourse without effective contraception including condoms), (3) HIV risk (any occurrence of vaginal or anal sex without a condom), (4) AEP risk (any occurrence of risk drinking plus any occurrence of vaginal intercourse without effective contraception during the same time period), and (5) TEP risk (any smoking plus any occurrence of vaginal intercourse without effective contraception during the same period).
Client Satisfaction Questionnaire–8 (CSQ-8)
Client satisfaction was measured using the CSQ-8 (Attkisson & Zwick, 1982). This standardized measure consists of eight questions followed by a 4-point Likert-type scale, with possible scores ranging between 8 and 32, and higher scores indicating higher levels of satisfaction. This questionnaire was administered, along with five open-ended questions about the intervention, using the ACASI in a private setting at the end of the 3-month follow-up. The five open-ended questions solicited comments/suggestions, what was liked about the intervention, what was liked least about the intervention, suggestions for improvement, and the most important aspects of the intervention.
Working-Alliance Inventory–Short (client/therapist)
This measure is used to assess three key aspects of the therapeutic alliance—agreement on the goals of therapy, tasks of therapy, and the development of an affective bond (Hatcher & Gillaspy, 2006). This scale consists of 12 items followed by a 7-point Likert-type scale, which ranges from never to always. This scale was administered to both the youth and the counselor at each of two counseling sessions.
Data Analysis
The Statistical Package for Social Sciences (SPSS Version 23) was used to conduct all analyses. Descriptive statistics were used to describe the sample, reductions in dichotomous risk of AEP, TEP, and HIV among an all risk sample at baseline, feasibility and acceptability measures, and responses to the CSQ-8 at 3-month follow-up. Inferential statistics were not used to assess behavior change, as all youth were considered to be at risk of AEP, TEP, and HIV at baseline. A simple thematic analysis was conducted of brief open-ended responses concerning the acceptability of the intervention provided by the youth when completing the CSQ-8 at 3-month follow up. These questions asked about what was liked most and least about the intervention and suggestions for improving the intervention.
Results
Participants ranged in age from 14 to 17, with a mean age of 16 years (SD = .89). Eighty-two percent were Hispanic/Latina, with 55% reporting Mexican origin. The sample was racially diverse with 18% Black, 18% White, 9% American Indian/native Hawaiian, 4.5% multiracial, and 27% reporting race as Hispanic/Mexican American. The youth were all English speaking. However, we did have a Spanish-speaking counselor available to provide the intervention in Spanish if needed and to communicate with Spanish-speaking parents/guardians. Prior arrests ranged from 1 to 10 or more, with 59% only having 1 or 2. Participants reported prior arrests for the following reasons: 45% assault, 41% petty theft, 27% truancy, 22% possession of marijuana or other drugs, 18% running away, and 14% trespassing. With regard to sexual orientation, 73% were heterosexual and 23% bisexual. All youth reported using drugs in the last 6 months, and among those who smoked, five were daily smokers. The mean AUDIT score was 2.5 (SD = 2.87).
Risk of AEP, TEP, and HIV/STI
Of the 22 participants who received the intervention, one did not complete the follow-up assessments. Reduction of AEP, TEP, and HIV risk was based on the frequency of youth in the at-risk or reduced risk category based on the TLFB at each follow-up period. Successful change was categorized as “reduced risk” instead of “no risk” because all contraception methods, including condoms, fail a certain percentage of the time even with perfect use. As noted previously, these data were divided into 30-day increments to calculate the presence of combined or single risk behaviors within each time frame over a continuous 7-month period: 3-month baseline (3 months prior to baseline), 1-month follow-up (from baseline to 1 month later), and 3-month follow-up (from 1 month to 3 months postbaseline). AEP risk was defined as the presence of risk drinking and risk of unplanned pregnancy during the same time period, TEP risk was defined as any smoking plus risk of unplanned pregnancy during the same period, and HIV/STI risk as any occurrence of vaginal or anal sex without a condom.
Ninety percent (n = 19) of participants were at reduced risk of AEP at 1 month, and 71.4% (n = 15) were at reduced risk at 3 months. Using an intent-to-treat analysis (treating the drop out as a failure), 86.4% were at reduced risk at 1 month and 68.2% were at reduced risk at 3 months.
Seventeen of the 22 (77%) participants were smokers and at risk of TEP at baseline. Of those at risk at baseline, 68.8% (n = 11) were at reduced risk at 1 month and 50% (n = 8) were at reduced risk at 3 months. With the intent-to-treat analysis, 64.7% were at reduced risk at 1 month and 47.1% were at reduced risk at 3 months. Of those who smoked at baseline, 71.4% reported currently smoking cigarettes at 1 month and 73.3% at 3 months.
All 22 participants who received the intervention were at HIV/STI risk at the baseline. Fifty-two percent were at reduced risk at 1 month, and 28.6% were at reduced risk at 3 months. Of the 11 who were not at risk of unplanned pregnancy at 3 months, only 2 were not using condoms while sexually active and using another contraceptive method. Using an intent-to-treat analysis, 50% were at reduced risk for HIV/STI at 1 month and 27.3% were at reduced risk at 3 months.
The route by which the youth reduced their AEP and TEP risk is provided in Figure 2.

Distribution of youth achieving reduced risk of alcohol-exposed pregnancy and tobacco-exposed pregnancy at 1 month and 3 months.
Feasibility
The CHOICES-TEEN intervention checklist indicated that all aspects of the intervention were delivered and that the sessions did not exceed the planned 45- to 60-min duration. The CHOICES-TEEN MI Scale, which assessed the degree to which counselors believed they emphasized various aspects of an MI approach, was rated as over a 4 on a 1–5 scale for all items. CHOICES-TEEN counselors indicated per structured session notes that all participants appeared to comprehend session tasks. The average per-item mean for youth on the task (M = 5.99, SD = .97), bond (M = 6.04, SD = .95), and goal (M = 5.56, SD = 1.12) subscales of the Working Alliance Inventory–Short ranged between 5 (often) and 7 (always) on a 1–7 scale.
Participant Acceptance/Satisfaction With Intervention
All except one of the 22 youth enrolled in the intervention completed all three sessions delivered on site at a weekly community-based probation program. In response to the anonymously administered CSQ-8 at 3-month follow-up, female youth (n = 20) reported high levels of satisfaction (M = 24, SD = .71; average per-item mean = 3) with the intervention, with scores ranging from 23 to 25. Specifically, 60% described the quality of services as “excellent” and 40% described the services as “good.” Despite being a nontreatment seeking population, fifty-five percent of youth indicated that they “definitely” received the service desired, with 45% indicating they “generally” did. Sixty percent indicated “most” of their needs have been met by the intervention, while 35% indicated “almost all” of their needs were met, and one youth indicated their needs were not met. All youth indicated they would refer a friend in need of similar help to the program. Ninety-five percent of youth reported being “mostly” or “very” happy with the amount of help they received. With regard to overall satisfaction, 65% reported being very satisfied, and 35% mostly satisfied. Ninety-five percent indicated they would return to the program if they were to seek help again. Twenty of the 22 participants provided anonymous written feedback to the open-ended questions that followed the CSQ-8. Responses indicated that youth valued the opportunity to be honest in a relational, confidential setting and that the counselors and doctors provided useful information that they did not know or had not considered. In particular, the youth appreciated the opportunity to have a conversation with a physician to obtain accurate information about their options for preventing unplanned pregnancy and HIV/STIs. Youth suggested the program may be more successful if assistance was provided for transportation and appointment setting with the health clinics. They also suggested that the program expand to reduce the health and pregnancy risks associated with marijuana and other drugs.
Discussion
This one-arm feasibility study suggests that the CHOICES-TEEN intervention is feasible, acceptable, and promising with regard to reducing the risk of AEP, TEP, and HIV/STI among female youth involved with the juvenile justice system. The retention of youth who began the intervention was 91% for all three sessions, and youth reported feeling positively about the intervention, suggesting that the intervention was acceptable. With regard to feasibility, all intervention components were completed with ease within the designated session time frames. Taken together, these findings suggest that it is feasible to target multiple health-risk behaviors (smoking, risk drinking, contraception use, and condom use) simultaneously with this high-risk population. However, future research with a control group will be necessary to test the efficacy of this intervention.
The reductions in risk of AEP were comparable to reductions of risk found in CHOICES intervention studies with women (Floyd et al., 2007; Velasquez et al., 2017). With regard to TEP, the reduction of risk was 50% in this study and 69.8% in the CHOICES Plus study (Velasquez et al., 2017). However, this sample only included five youth reporting daily smoking, suggesting many of these youth may be engaging in light and intermittent smoking which often mistakenly perceived by youth as less harmful or addictive (Amrock & Weitzman, 2015). This may be one of the reasons that few youth accepted and followed up with the smoking cessation referral. In addition, open-ended feedback from the youth suggested that smoking was a temporary replacement for marijuana, while they were being randomly drug tested by probation. This suggests a need to better understand the patterns of smoking and marijuana use among high-risk females in these settings for purposes of preventing substance-exposed pregnancy.
The proportions of youth reducing HIV/STI risk at 3-month follow-up were not as high compared to AEP and TEP, which is not surprising as there is only one way to reduce this risk—condom use. While it is most ideal that youth reduce their risk of pregnancy by either abstinence or using both condoms and other contraceptive methods, it is encouraging that the large majority of youth who reduced their risk of pregnancy in the study were using condoms, which protect against both unplanned pregnancy and HIV/STIs. In addition, HIV/STI prevention research with juvenile justice populations has generally resulted in more modest effect sizes for behavioral change (Tolou-Shams, Stewart, Fasciano, & Brown, 2010), highlighting a need to develop more robust interventions.
Despite encouraging findings, these results should be interpreted with some caution, given the small sample size and lack of a control group. Also, while self-report measures are a major data source for clinical and resource purposes, they have been criticized for potential bias. However, retrospective self-reports of behavior collected in settings which minimize these potential biases have been shown to be reliable and valid. Still, future research would benefit by incorporating biological measures that further substantiate self-report. Finally, given feedback from the youth and the providers, it may be useful to expand the CHOICES-TEEN model to incorporate marijuana and other drugs as well as to explore the utility of providing all of the aspects of the intervention in a postadjudication placement setting to reduce client transportation challenges and the time commitment for travel of providers.
Implications for Practice and/or Policy
Given the limited research on gender-sensitive interventions with female youth in juvenile justice settings, this research highlights several implications for practice and policy. First, this is the first study to report on the prevalence of substance-exposed pregnancy in a sample of female youth in the juvenile justice system. Of the 150 youth screened, 25% were at risk of AEP in this study, which is much higher than the 3.4% at risk in the general population (Cannon et al., 2015). This finding, combined with the aforementioned literature documenting these overlapping risks in multiple, larger samples of female youth, suggests an urgent need for interventions and/or policy to reduce these risks. Specifically, programming should be provided that informs female youth of these risks as well as efficient, prevention interventions that have promise for broad prevention impact. AEP is 100% preventable, has been recently estimated to be more prevalent than autism (May et al., 2018), and can lead to costly lifelong cognitive, behavioral, emotional, and adaptive functioning deficits. Smoking and HIV/STIs can also severely affect the health of both female youth and their children both during and after pregnancy (e.g., second-hand smoke; HHS, 2014; Delpisheh et al., 2006; Kulig, 2005; Wiemann & Berenson, 1998). As such, the development of and funding for early prevention programs for one of the society’s highest risk populations that rarely receives integrated health care are essential.
Second, this study suggests integrated, multirisk bundled motivational enhancement interventions provided at opportunistic times can be feasible, acceptable, and potentially promising for female youth in the juvenile justice system. As such, programs that focus on more than just one risk behavior during times of detention or community probation may be more efficient and cost-effective. Finally, youth appreciated the opportunity to receive individualized information about their sexual health and substance use in an accepting and supportive context. Such efforts can be further bolstered by ensuring better access to referrals by providing transportation to follow-up medical visits, as this can be a major service barrier for this population. Finally, none of the youth in this study accepted the incoming smoking cessation Quitline referral phone calls. As such, nontelephonic options, such as the U.S. Health and Human Service’s QuitSTART technology application, may be a better fit for some youth.
Conclusions
CHOICES-TEEN is acceptable and feasible and appears promising for reducing overlapping, bundled health risks—AEP, TEP, and HIV—among high-risk female youth in juvenile justice settings. Given the potential for impacting multiple, overlapping health risks in an opportunistic manner, future research should examine the efficacy of this intervention with a more robust sample.
Footnotes
Acknowledgments
Harris County Juvenile Probation provided essential support of this project by facilitating essential partnerships and space in the field. Robin Harris provided coordination of the project in the field, and Barbie Atkinson, Matiko Bivens and Lisa Connelly were the CHOICES-TEEN counselors. Rebecca Beyda, M.D. and Laura Grubb M.D., provided the Adolescent Medicine risk reduction counseling sessions. Alicia Kowalchuk, M.D. provided Motivational Interviewing training for the Adolescent Medicine Fellows, and Nanette Stephens provided fidelity monitoring and training for the CHOICES-TEEN counselors. Ralph DiClemente, Ph.D. and Carrie Randall, Ph.D. provided consultation to support the implementation of this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Grant Number 1R03DA034099 from the National Institute of Drug Abuse, National Institutes of Health.