
Abstract
Objective:
This study evaluated the effectiveness of the Healthy Start Home Visiting Program—School-Based Model (HSS), using a cluster randomized controlled trial design.
Methods:
Participants included 224 parents from 20 preschools randomized into intervention and wait-list control groups at the preschool level. Furthermore, 105 parents from the participating preschools were trained as parent ambassadors to assist in program delivery. They were randomized into intervention and control groups at the preschool level. Outcome measures included parent and teacher reports on children’s learning, parent report on children’s behavior and health, their own parenting, and direct assessment of children. Parent ambassadors completed measures on parenting and their children’s behavior before training and after program delivery.
Results:
There was significant improvement at postintervention in parenting, children’s behavior, and learning and health in the intervention group, compared with the control group.
Conclusions:
The results provided evidence on the effectiveness of the HSS program.
Children develop at a very rapid rate during the first few years of their lives (Knudsen, Heckman, Cameron, & Shonkoff, 2006). The greatest plasticity is found in the early years, and the best opportunity for intervention to promote optimal development is during the early years (World Health Organization, 2013). The best returns to a society’s investment is to invest in programs targeting the early years (Heckman, 2000). The acquisition of early foundational skills is critical for the development of higher cognitive capacities at a later age, and the acquisition of these skills is greatly influenced by caregivers (Knudsen et al., 2006).
Many early childhood intervention programs have been developed for children from challenged families in western countries, to help them overcome their challenges and to promote their optimal development. Programs such as Nurse Family Partnership, Perry Preschool Program, and Abecedarian Program have been shown to be effective in producing cognitive gains in children and other long-term gains such as increased high school completion rate, tertiary education admission rate, and employment rate (F. A. Campbell, Ramey, Pungello, Sparling, & Miller-Johnson, 2002; Magnuson & Shager, 2010; Olds, 1988; Schweinhart & Weikart, 1990). These programs have also been found to be cost-effective in producing US$4.00–US$12.90 return per dollar spent (Masse & Barnett, 2002; Schweinhart & Weikart, 1990).
Effective intervention programs should be comprehensive, covering physical, cognitive, and psychosocial development, and should target young children and their families from challenged backgrounds (Engle et al., 2007). Families should be supported to promote early child development through parent training programs (Marmot, 2010). There should be parent training to improve parenting skills, enhance parent’s social support, and their knowledge on child development (Mersky, Topitzes, & Reynolds, 2011). Parent training programs have been found to be effective in producing gains in parental psychosocial health and reduction in child behavior problems (Barlow, Smailagic, Huband, Roloff, & Bennett, 2012; Piquero, Farrington, Welsh, Tremblay, & Jennings, 2008). Furthermore, program effectiveness of early intervention programs is positively associated with program duration, intensity, and quality (Engle et al., 2007).
In Hong Kong, there are a number of early intervention programs for parents with preschool children from challenged families. The Parent and Child Enhancement (PACE) program was designed for parents with 2-year-old children from challenged families who were not attending preschools (C. Leung, Tsang, & Lo, 2017), and the content included child cognitive and psychosocial development. The program was delivered in social service centers. The Hands-On Parent Empowerment (HOPE) program was a preschool-based program which targeted new immigrant families and the content included child cognitive and psychosocial development (C. Leung, Tsang, & Dean, 2011). The Healthy Start Home Visit Program was a home visiting program for parents with preschool children from challenged families, and the content included physical, cognitive, and psychosocial areas (C. Leung, Tsang, & Heung, 2015). A group of parents were trained to become parent ambassadors who then delivered the program to challenged families through 20 home visiting sessions, under the supervision of a coordinator, who was a registered social worker.
The Healthy Start Home Visiting Program—School-Based Model (HSS)
The context of delivery is an important factor in the delivery of parenting programs (Shriver & Allen, 2008), as contextual variables might affect program delivery and effectiveness. Gross and Grady (2002) argued for the delivery of parent training programs in preschools. Preschools have the greatest potential to access parents and they are also accessible to parents. Preschools share the same goal of promoting child development with parent training programs, and parent training could be perceived as enhancing the goals of the preschool. The support and encouragement from preschool teachers and principals are important motivating factors for parent participation and attendance. In terms of program sustainability, the staff could be encouraged to be involved in the parent training and the trained parents could provide peer support for other parents. It is also a useful strategy to encourage home–school co-operation.
The Healthy Start Home Visit Program is a comprehensive program targeting child physical, cognitive, and psychosocial development, and it has been found to be effective with Hong Kong Chinese parents (C. Leung et al., 2015) in terms of child learning, behavior and health, parenting stress, social support, and self-efficacy. However, some Hong Kong parents are reluctant about home visits due to the crowded living environment in Hong Kong. On the other hand, many parents find it convenient to attend a parenting program in their children’s preschools while their children are attending preschool classes. A school-based parent training program could also serve to enhance the sustainability of the program and to promote home–school co-operation. It was thus decided to adapt the Healthy Start Home Visit Program into a preschool-based program, the HSS. The HSS program was delivered by social workers from the project team in the participating preschools in a group format. A preschool representative (preschool teacher or school social worker or religious teacher) and a number of parents (parent ambassadors) in each participating preschool would receive a six-session training program provided by the project team. The parent ambassadors would assist the social workers of the project team in the delivery of the program. The school representative served as the bridge between the preschool and the project team and was responsible for the logistic arrangement of the school-based program.
The target participants were parents with preschool children from challenged families and/or parents with noncompliant and/or aggressive children. The expected outcomes were a decrease in child behavior problems and an improvement in child learning and child physical health (oral health, physical activity, home safety, and healthy feeding practice). The choice of these outcomes was guided by research. Poverty is associated with academic difficulties and psychological difficulties such as behavior problems (Flouri, Midouhas, & Joshi, 2014; Ip et al., 2013). Parents of noncompliant children are at higher risk of physical maltreatment when disciplining their children (Hurlburt, Nguyen, Reid, Webster-Stratton, & Zhang, 2013). Dental caries of preschool children is negatively associated with family income, parent education, and parent dental knowledge (Chu, Ho, & Lo, 2012). Home injury and sedentary activities are negatively associated with family socioeconomic status (Drenowatz et al., 2010; Kelishadi et al., 2016). Parent education level is positively associated with their nutrition knowledge (Räsänen et al., 2003).
The content of the HSS program was based on the Healthy Start Home Visit Program but was reduced to 12 sessions, to make it less demanding on the commitment of parents. The content focused on positive parenting strategies as these strategies were found to be the driving force for changes in child behavior (Gardner, Burton, & Klimes, 2006). The strategies included strategies to enhance parent–child relationship (e.g., spending quality time with children, use of reflection), strategies to increase positive behavior such as use of praise and rewards, and strategies to decrease undesirable behavior such as ignoring and time-out. For learning, the strategies included paired reading (S. F. Lam, Chow-Yeung, Wong, Lau, & Tse, 2013) and the use of prompts and demonstrations in teaching preschool concepts. For oral health, the content included healthy food and drinks and tooth brushing (Rogers, 2011). For nutrition, the content included healthy feeding practices such as balanced diet. There was also a session on the importance of physical activities, with examples of physical activities suitable for preschool children. For home safety, the content included home safety measures (e.g., safety guards for windows) and the identification and removal of home safety hazards (e.g., blind cord loops).
In terms of the strategies to achieve the outcomes, a group approach was used as there is research evidence to demonstrate the effectiveness of group parent training programs in producing positive changes in child and parent outcomes such as child behavior problems, parenting stress, and confidence (Barlow et al., 2012; Piquero et al., 2008). The program consisted of 12 weekly group sessions on the management of child behavior, as well as strategies to promote child learning, which were delivered in the participating preschools by the social workers from the project team. In addition to these school-based group sessions, there were three mass lectures for all the intervention group participants on nutrition, oral health, and physical exercise conducted by the respective health professionals. These lectures were delivered in the participating preschools or community service centers. Finally, there was one home visiting session delivered by a social worker from the project team and the parent ambassadors on home safety measures. The program details are in Table 1.
Program Outline of Healthy Start Home Visiting Program—School-Based Model.

The Present Study
This study aimed to evaluate the effectiveness of the HSS program using a cluster randomized controlled trial design. The primary outcomes were child behavior and child learning. The secondary outcomes were parenting stress, social support, self-efficacy, and child health indicators such as feeding practices, sedentary activities, home injury, and child oral health practices. The hypotheses were: The intervention group parents would report lower child behavior problems than the control group parents at postintervention. The intervention group children would achieve better child learning than the control group children at postintervention. The intervention group parents and teachers would report better child learning than the control group parents and teachers at postintervention. The intervention group parents would report better child health in terms of higher frequency of tooth brushing, healthier feeding practices, less sedentary activities, and fewer incidents of home injury than the control group parents at postintervention. The intervention group parents would report lower parenting stress and higher social support and self-efficacy than the control group parents at postintervention.
Method
Design
This study adopted a cluster randomized controlled trial design. There was no blinding of participants. Allocation ratio was 1:1. As parents within the same preschool might exchange information, the unit of randomization was at the preschool level, to avoid contamination.
Participants
HSS participants
The inclusion criteria were parents of preschool children (i) from socially challenged backgrounds (new immigrants, single parents, and low-income families) and/or (ii) identified by the participating preschools to have parenting needs (parents whose children were noncompliant and/or aggressive) and (iii) the parent and the child should normally reside in Hong Kong. The exclusion criteria included children with major developmental problems, history of domestic violence, drug abuse, or mental illness in the family.
The participants included 224 parents recruited from 20 preschools. Ten preschools (n = 102) were randomized into the intervention group and 10 preschools (n = 122) were randomized into the wait-list control group.
For sample size calculation, based on the medium effect size in the Healthy Start Home Visit Program (C. Leung et al., 2015), the sample size for an individual-level randomized controlled trial would be 64 per group (power = .8, α = .05; Cohen, 1992). For cluster randomized controlled trials, a design effect should be considered due to intracluster correlation (ρ). The formula for adjustment is 1 + (n − 1) ρ, with n as the average cluster size (M. K. Campbell, Mollison, Steen, Grimshaw, & Eccles, 2000). With an average cluster size of 11.2 and an average ρ for parent and child measures of 0.07 in the Healthy Start Home Visit Program (C. Leung et al., 2015), the design effect was 1.714 and a sample size of 220 would be required. The present sample size was considered adequate.
Parent ambassadors
The parent ambassadors included 105 parents with children attending the intervention (n = 51) and wait-list control (n = 54) preschools.
Measures for HSS Participants
The following measures were administered to the intervention and wait-list control group participants before (pre) and after program completion (post). Intervention group participants were also administered the same set of questionnaires 4 months after program completion (follow-up).
Child learning and behavior outcome measures
The Cognition Scale of the Hong Kong Comprehensive Assessment Scale for Preschool Children (HKCAS-P) version (C. Leung, Mak, Lau, Cheung, & Lam, 2013)
This scale is developed and normed for Hong Kong children aged 3–6 years and is individually administered to children. It consists of 40 items on preschool concepts such as color, shape, and categorization. It correlated with the Wechsler Preschool and Primary Scale of Intelligence–Revised and it could differentiate children with developmental delay from children with typical development. The reliability was .93 (C. Leung et al., 2013).
Eyberg Child Behavior Inventory (ECBI; Eyberg & Ross, 1978)
This is a multidimensional measure of parental perception of disruptive behavior in children, with 36 items to be completed by parents. It consists of two scales. The Intensity Scale measures the frequency of problem behavior and is rated on a 7-point scale. The Problem Scale measures the extent to which parents are concerned about their children’s behavior and is rated as 1 (yes) or 0 (no). The Chinese version of the inventory was validated by C. M. Leung, Chan, Pang and Cheng (2003). The Chinese version correlated with child behavior problem and parenting stress measures. The reliability estimates of the Intensity Scale and Problem Scale were .94 and .93, respectively.
Gumpel School Readiness Scale (Gumpel, 1999)
This is a 6-item measure on child learning behavior and preschool concepts. The teachers and parents rate their students/children on each statement on a 4-point scale (1 = never, 2 = seldom, 3 = sometimes, and 4 = always). A Chinese version was developed and validated (Ho, Leung, & Lo, 2013). The scale correlated with child cognitive development and child behavior, and it could differentiate children of different age groups. The reliability estimates of the teacher and parent versions were .81 and .70, respectively (Ho et al., 2013).
Behavior Rating Scale for Presented Academic Self-Esteem in Young Children (Fuchs-Beauchamp, 1996)
A Chinese version was developed and validated (C. Leung, Lo, & Leung, 2012). The Chinese version consists of 15 items and covers areas such as a sense of competence, persistence, initiative, and coping. There are teacher and parent versions in the validated Chinese version (C. Leung et al., 2012), where the teachers and parents rate their students/children on each statement on a 4-point scale (1 = never, 2 = seldom, 3 = sometimes, and 4 = always). The Chinese version correlated with child cognitive development and child behavior, and it could differentiate children with developmental disabilities from children with typical development. The reliability estimates of the teacher and parent versions were .95 and .89, respectively (C. Leung et al., 2012).
Inventory of School Motivation (McInerney & Ali, 2006)
A Chinese version of the Effort subscale (a measure of effort attribution and effort-focused motivation) and Task subscale (a measure of task orientation and involvement) was developed and validated (C. Leung & Lo, 2013). In the validated Chinese version, the teachers and parents rate their students/children on each statement on a 4-point scale (1 = never, 2 = seldom, 3 = sometimes, and 4 = always). Both subscales correlated with child behavior and child cognitive skills, and they could differentiate children with developmental disabilities from children with typical development. The reliability estimates of the Effort subscale were .89 and .92 for the parent and teacher versions, respectively. For the Task subscale, the reliability estimates of the parent and teacher versions were .77 and .85 (C. Leung & Lo, 2013).
Health status
This consists of questions on the frequency of sedentary activities, number of home injuries, and hospital casualty department visits.
Hong Kong Parent Feeding Questionnaire (Department of Health, 2012)
This is a 35-item measure on parent knowledge, attitude, and practices on child feeding, to be rated on a 3-point scale. A high score indicates healthier feeding practices. This scale has been used in the Healthy Start Home Visit Program with reliability estimates of .79 and .80 for preintervention and postintervention assessment (C. Leung et al., 2015).
Frequency of tooth brushing
This is a questionnaire on oral health practice in preschool children developed by the Oral Health Education Unit of the Department of Health, HKSAR. The parents rate each item on a 5-point scale. A higher score indicates more frequent tooth brushing.
Parent outcome measures
Parenting Stress Index (PSI; Abidin, 1990)
This is a 36-item questionnaire on parenting stress. The Chinese version of the scale was validated by D. Lam (1999). The scale correlated with anger expression with an overall reliability of .89.
General Self-Efficacy Scale (Schwarzer, 1993)
This scale is used as a measure of parent confidence. It consists of 10 items measured on a 4-point Likert-type scale ranging from not at all true (1) to exactly true (4). A validated Chinese version is available with a reliability of .91 (Zhang & Schwarzer, 1995).
Duke-UNC Functional Social Support Questionnaire (Broadhead, Gehlbach, de Gruy & Kaplan, 1988)
This is used as a measure of parent social network. It consists of 8 items on perceived social support in various areas. The Chinese version of the questionnaire has been used with parents with preschool children with satisfactory reliability (.92) in the Healthy Start Home Visit Program (C. Leung et al., 2015).
Demographic information
Parents were requested to supply basic demographic information.
Measures for Parent Ambassadors
The intervention and wait-list control group parent ambassadors were requested to complete the ECBI (Eyberg & Ross, 1978), PSI (Abidin, 1990), General Self-Efficacy Scale (Schwarzer, 1993), and Duke-UNC Functional Social Support Questionnaire (Broadhead et al., 1988) before intervention group parent ambassadors started their six-session training and after intervention group parent ambassadors had completed the program delivery. Furthermore, the intervention group parent ambassadors completed the same set of questionnaires again 4 months after the completion of program delivery. The parent ambassadors were also requested to supply basic demographic information.
Procedures
This study was approved by the ethics committee of The Hong Kong Polytechnic University. This study was registered with ISRCTN Registry (ISRCTN16238864).
HSS participants
The service was delivered through a nongovernmental organization (NGO) with a team of registered social workers and an educational psychologist. The NGO recruited the participating preschools. The parent participants were then recruited by the participating preschools. Recruitment of the parent participants commenced in September 2016.
Upon confirmation of the participation of the participating preschools, the preschool list was sent to the first author, who was not involved in the preschool recruitment. The first author used a random number table to randomly allocate the participating preschools to either the intervention or wait-list control groups.
In September/October 2016, the intervention and wait-list control group parents completed their questionnaires in the participating preschools, after briefing by the research assistants and signing the consent forms. Teacher questionnaires were sent to the participating preschools, and the completed questionnaires were returned to the project team through the participating preschools. The children in both groups were individually assessed in their own preschools by qualified users of the HKCAS-P or psychology graduates under the supervision of qualified users of the HKCAS-P, who were not informed of the group status of the children. The parents and teachers of both the intervention and wait-list control groups completed these questionnaires after the intervention group had completed the intervention in the target children’s preschools in February/March 2017. The children in both the intervention and wait-list control groups were being administered the HKCAS-P at about the same period in their preschools. The parents, teachers, and children in the intervention group were administered the same set of questionnaires in the children’s preschools approximately 4 months (June/July 2017) after they had completed the program.
Upon the completion of the intervention program by the intervention group, the wait-list control group participants were offered the intervention program.
Parent ambassadors
The parent ambassadors were recruited by the NGO through the participating preschools (90%) or recommended by the preschool principals (10%) in September 2016. All of them completed the pretraining measures on parenting and child behavior in their children’s preschools before the commencement of the training of the intervention group parent ambassadors (September/October 2016). They were requested to complete postintervention measures after the intervention group parent ambassadors had delivered the HSS program (February/March 2017). The intervention group parent ambassadors were also requested to complete the same set of questionnaires 4 months after program delivery (June/July 2017).
The Intervention
The HSS program consisted of 12 school-based group sessions on strategies to promote parent–child relationship, strategies to increase positive behavior, and strategies to manage inappropriate behavior, as well as strategies to promote learning such as paired reading and learning of preschool concepts. These sessions were delivered by qualified social workers from the project team in the participating preschools. Parent ambassadors assisted in the course, as leaders in small group discussions, making buddy-calls to HSS participants, leading role-play in the group sessions, pairing with social workers to conduct home visits, and providing supplementary classes to the HSS participants who were absent for classes. Three talks on health-related topics (oral health, nutrition, and physical exercises) were delivered by the health professionals in the respective fields. One home visiting session on home safety was conducted by the social workers and parent ambassadors. The program was adapted from the Healthy Start Home Visit Program by an educational psychologist, under the supervision of the first, second, and third authors. A program manual (which could be obtained by contacting the third author) was developed and the facilitators were required to follow the session plan in the manual. There were supervision meetings and irregular site visits and on-site supervision provided by the third author and her supervisory staff including the educational psychologist.
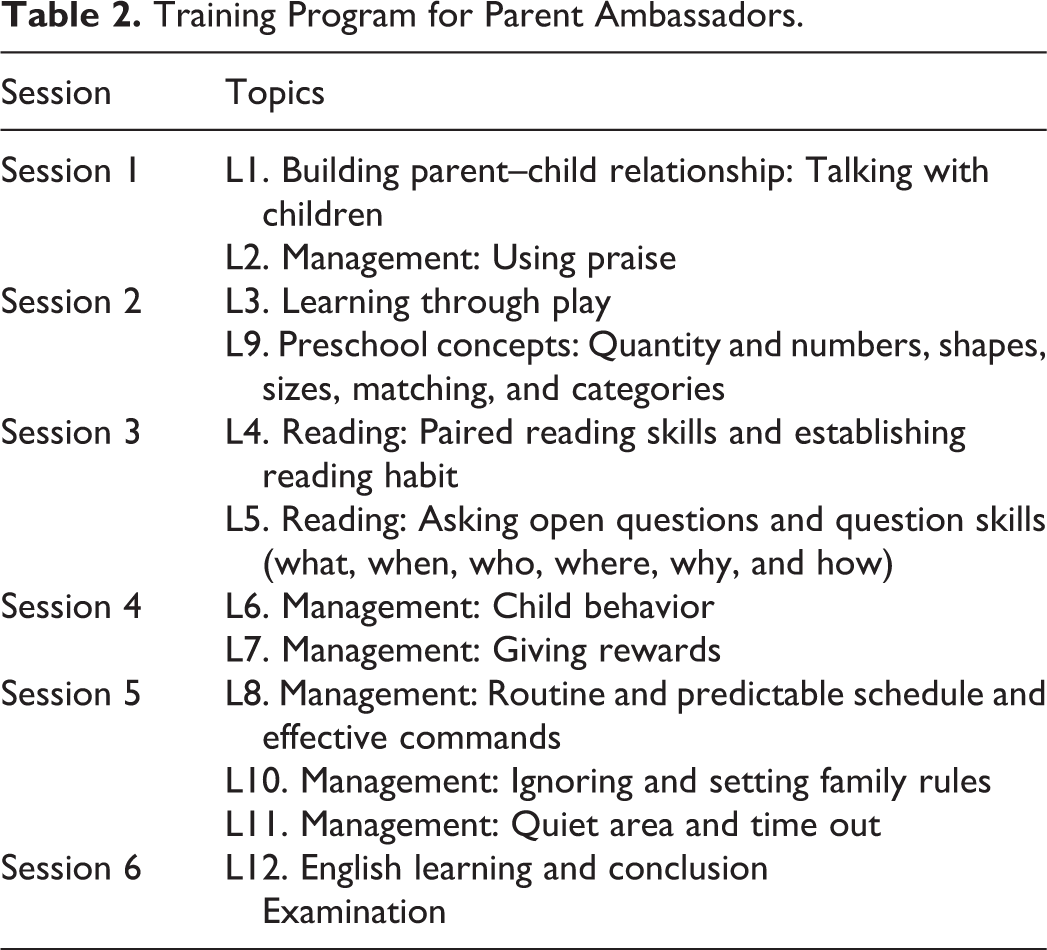
For the training of the parent ambassadors, they attended a six-session training program on the topics to be covered in the HSS program. The training was delivered by the social workers and the educational psychologist from the project team. The details are in Table 2. No service was provided to the parent ambassadors in the wait-list control group while the intervention group parent ambassadors were receiving training.
Training Program for Parent Ambassadors.
Data Analysis
Analysis of postintervention results was by intention-to-treat. Missing data were estimated using multiple imputation (five imputations). Preintervention measures were used as predictors for missing postintervention measures. The main analysis strategy was linear mixed method regression with group status, preintervention scores, and confounding variables as fixed factors, with the preschool as a random factor and postintervention scores as dependent variables. Independent t test and χ2 test were used to examine baseline differences. Effect sizes were reported as Cohen’s d (with 95% confidence interval [CI]). Effect sizes provide information on the magnitude of the treatment effect and its CI provides information on the precision of the estimate (Lee, 2016). According to Cohen (1992), the effect sizes of .20, .50, and .80 are regarded as small, medium, and large effect sizes.
For the 4-month follow-up results, only the intervention group members were included. Missing data were estimated using multiple imputation (five imputations). Preintervention and postintervention measures were used to predict missing 4-month follow-up data. Repeated measures analysis of variance (ANOVA) was used to analyze the data. 1
Results
The Sample
Among the intervention group participants, six dropped out because of health, work, family issues, or lack of time. In the intervention group, there were 98 parents with complete pre- and postdata, 96 children with complete pre- and postdata, and 98 teachers with complete pre- and postdata. At 4-month follow-up, there were 94 parents and teachers with complete data and 93 children with complete data. For the wait-list control group participants, 12 left the project because of personal, health, work issues, and lack of time. Due to administrative difficulties, one wait-list control school (n = 4) failed to provide postintervention teacher questionnaires and child assessment results. In the wait-list control group, there were 117 parents with complete pre- and postdata, 112 children with complete pre- and postdata, and 113 teachers with complete pre- and postdata. The overall attendance rate of the intervention group participants was 87.57%. The flow of participants is shown in Figure 1.
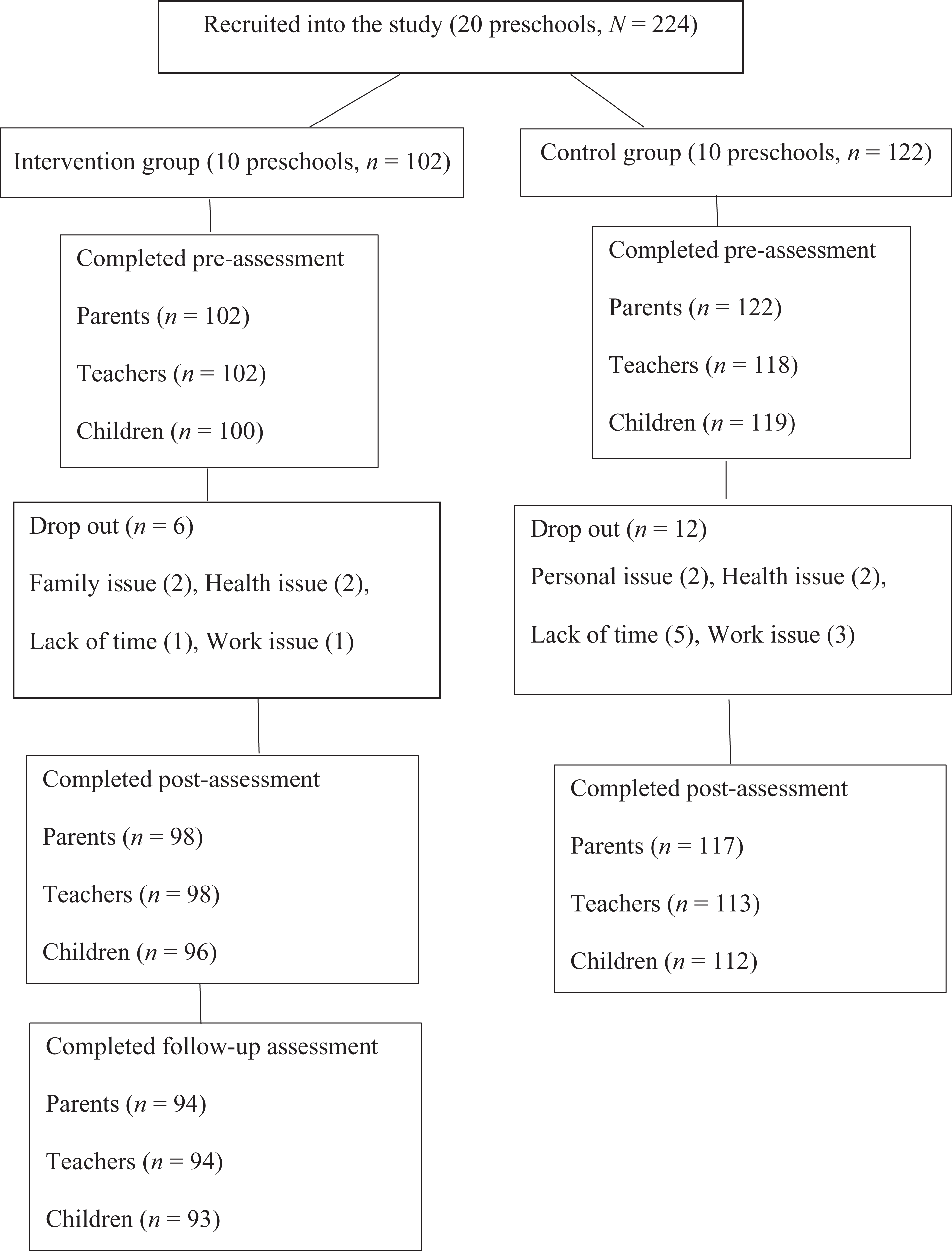
Flow of Healthy Start Home Visiting Program—School-Based Model participants.
For parent ambassadors, two intervention group parent ambassadors dropped out from the program because of family and work issues. For the wait-list control arm, three dropped out because of change of preschools and lack of time. There were 100 with complete pre- and postdata (intervention = 49, wait-list control = 51). At 4-month follow-up, there were 48 intervention group parent ambassadors with complete data. The overall attendance rate for the six-session training was 99.02%, and the overall attendance rate for program delivery was 87.21%. The flow of parent ambassadors is shown in Figure 2.
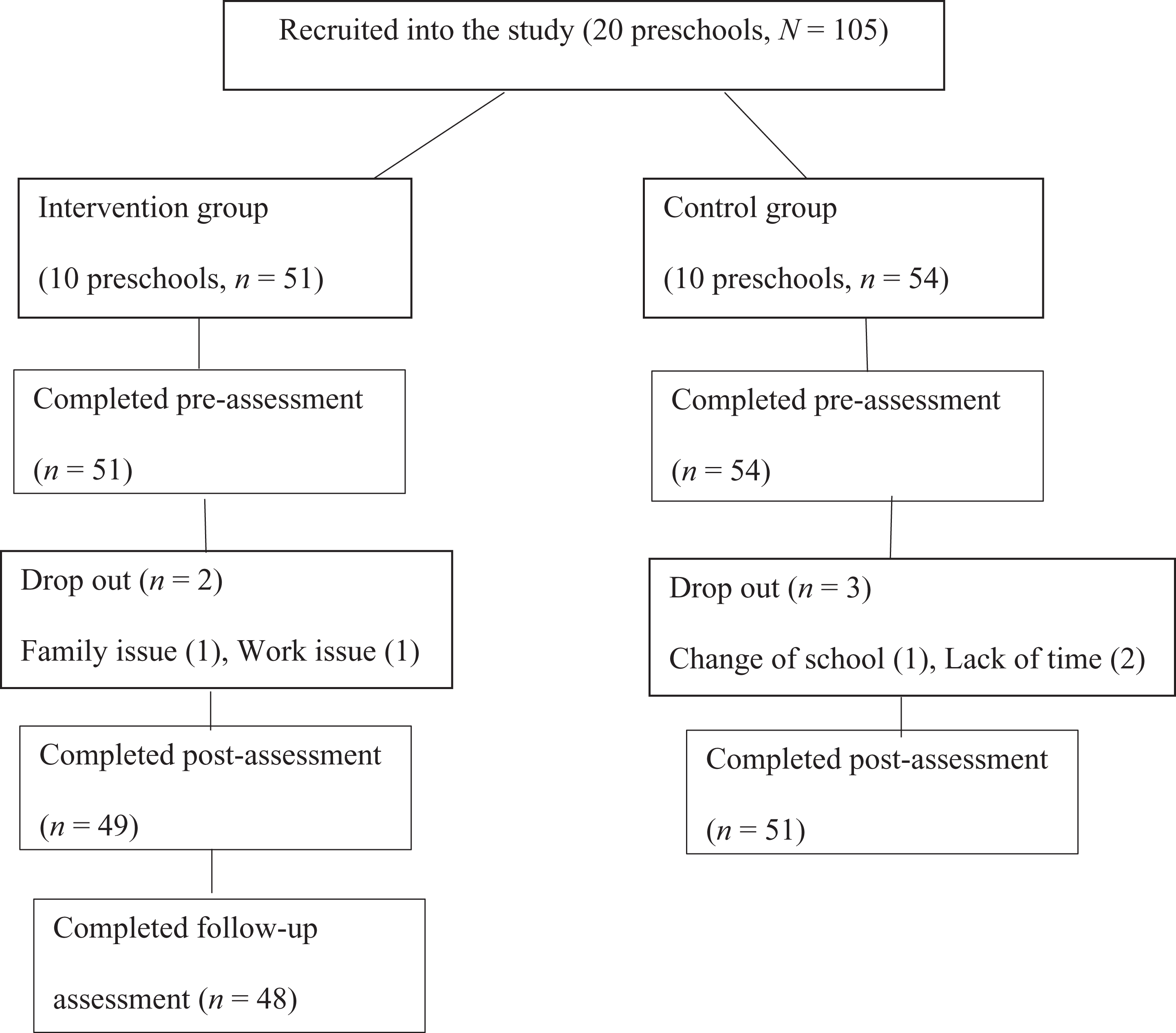
Flow of parent ambassador participants.
HSS Participants
There were significant differences between the intervention and wait-list control group participants in terms of mother’s employment status, mother’s length of residence in Hong Kong, children’s length of residence in Hong Kong, preintervention teacher report of school readiness, preintervention teacher report of effort motivation, and preintervention sedentary activities. The demographic details are in Table 3. The mean and standard deviation of the pre, post, and follow-up scores are in Table 4. The reliability estimates of most measures were above .70.
Demographic Characteristics of Healthy Start Home Visiting Program—School-Based Model Parent Participants.

Preintervention, Postintervention, and Follow-Up Scores of Healthy Start Home Visiting Program—School-Based Model Parent Participants.
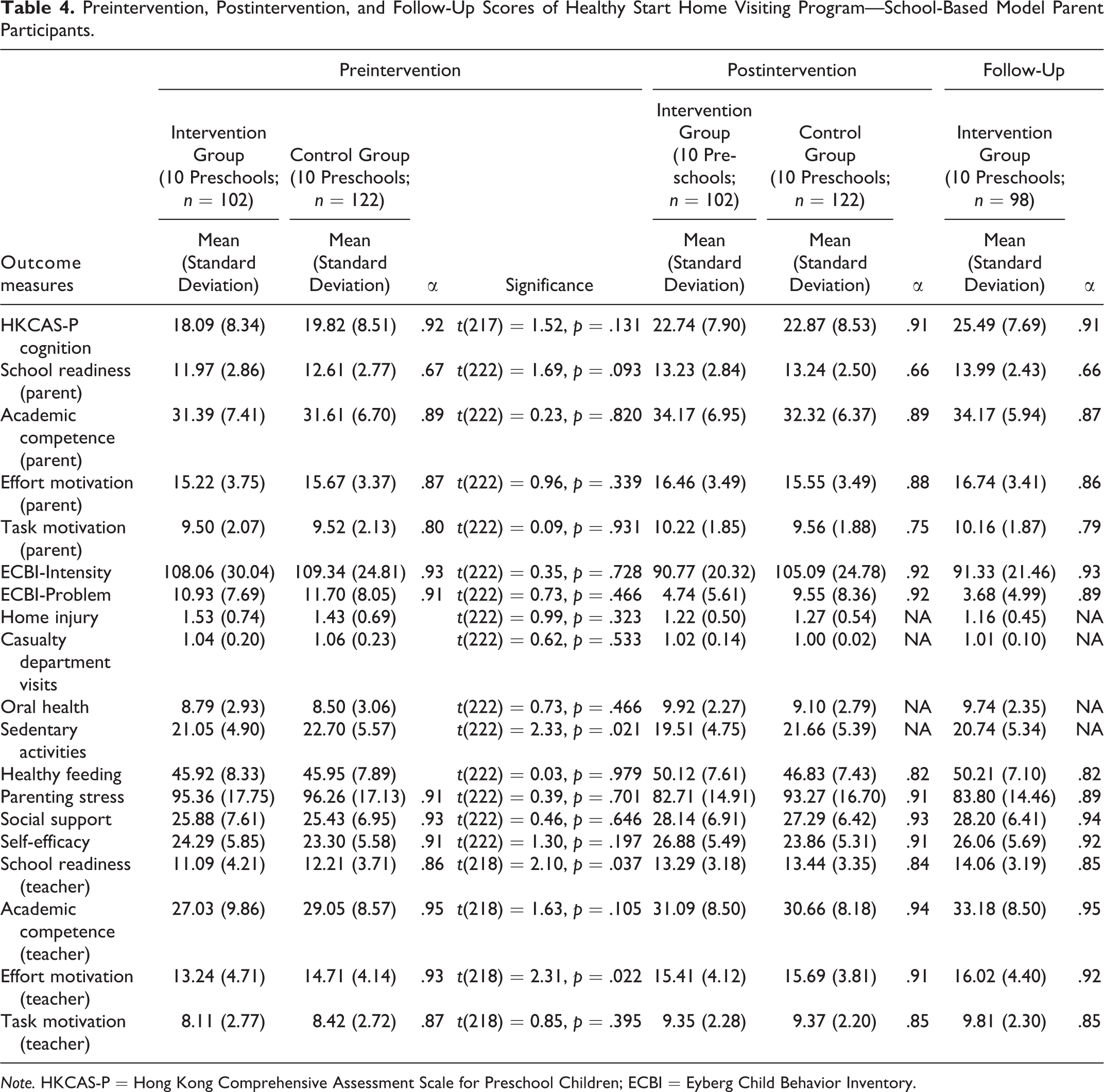
Note. HKCAS-P = Hong Kong Comprehensive Assessment Scale for Preschool Children; ECBI = Eyberg Child Behavior Inventory.
Intention-to-Treat Analysis of Postintervention Outcomes
Little’s missing completely at random (MCAR) test was significant, χ2(32) = 48.43, p = .031, indicating that the data were not missing completely at random. As the missing data were related to missing teacher and student measures from one wait-list control preschool, rather than the missing data itself, it could be regarded as missing at random and multiple imputation can be valid in this case (Scheffer, 2002). In the analysis reported below, multiple imputation (five imputations) was used to estimate missing data. In the linear mixed method regression analyses reported below, the fixed factors were group status, preintervention scores, mother’s employment status, mother’s length of residence in Hong Kong, children’s length of residence in Hong Kong, preintervention teacher report of school readiness, preintervention teacher report of effort motivation, and preintervention sedentary activities. The dependent variables were postintervention scores, with the preschool as a random factor.
In terms of Hypothesis 1 on the reduction in child behavior problems, linear mixed method regression results were significant for ECBI-Intensity, t = 3.81, p < .001, d = 0.63, 95% CI [0.35, 0.89], and ECBI-Problem, t = 4.81, p < .001, d = 0.66, 95% CI [0.39, 0.93]. Intervention group participants reported lower child behavior problem scores at postintervention than the wait-list control group participants.
In terms of Hypothesis 2 on the improvement in child learning, linear mixed method regression results were not significant for HKCAS-P cognition scores, t = 1.18, p = .238, d = −0.02, 95% CI [−0.28, 0.25].
In terms of Hypothesis 3 on the improvement in parent and teacher report of child learning, linear mixed method regression results were significant for parent report of academic competence, t = 2.05, p = .041, d = 0.28, 95% CI [0.01, 0.54], task motivation, t = 3.03, p = .002, d = 0.36, 95% CI [0.09, 0.62], effort motivation t = 2.87, p = .004, d = 0.26, 95% CI [−0.01, 0.52], and teacher report of academic competence, t = 1.96, p = .050, d = 0.05, 95% CI [−0.21, 0.31]. The intervention group participants reported higher scores on these measures at postintervention, compared with the wait-list control group participants. However, the results were not significant for parent report of school readiness, t = 0.26, p = .796, d = 0.00, 95% CI [−0.26, 0.26], teacher report of school readiness, t = 1.49, p = .137, d = −0.05, 95% CI [−0.31, 0.22], task motivation, t = 0.86, p = .389, d = −0.01, 95% CI [−0.27, 0.26], and effort motivation, t = 1.42, p = .155, d = −0.07, 95% CI [−0.33, 0.19].
In terms of Hypothesis 4 on the improvement in child health outcomes, linear mixed method regression results were significant for frequency of tooth brushing, t = 2.89, p = .004, d = 0.32, 95% CI [0.05, 0.58], and healthy feeding practice, t = 3.17, p =.002, d = 0.44, 95% CI [0.17, 0.70], with the intervention group participants reporting higher frequency of tooth brushing and healthier feeding practice at postintervention than the wait-list control group participants. The results were not significant for sedentary activities, t = 1.32, p = .191, d = 0.42, 95% CI [0.15, 0.68], home injury, t = 0.05, p = .960, d = 0.09, 95% CI [−0.17, 0.35], and casualty department visits, t = 1.27, p = .204, d = −0.18, 95% CI [−0.45, 0.08].
For Hypothesis 5 on the improvement in parenting outcomes, linear mixed method regression results were significant for parenting stress, t = 5.26, p < .001, d = 0.66, 95% CI [0.39, 0.93], and self-efficacy, t = 4.59, p < .001, d = 0.56, 95% CI [0.29, 0.82]. The intervention group participants reported lower parenting stress and higher self-efficacy at postintervention, compared with the wait-list control group participants. Linear mixed method regression results were not significant for social support, t = 0.57, p = .572, d = 0.13, 95% CI [−0.14, 0.39].
Intention-to-Treat Analysis of Follow-Up Data
In terms of Hypothesis 1 on the reduction in child behavior problems, at 4-month-follow-up, repeated measures ANOVA results were significant for ECBI-Intensity, F(2, 194) = 48.45–52.81, p < .001, partial η2 = .33–.35, and ECBI-Problem, F(2, 194) = 91.98–98.34, p < .001, partial η2 = .49–.50. Post hoc analyses (Bonferroni adjustment) indicated that for ECBI-Intensity, the postintervention and follow-up scores were significantly lower than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. For ECBI-Problem, the scores at all three time points differed significantly from one another, with steady decreases at each time point. The results indicated that the participants could maintain their program gains in terms of child behavior.
In terms of Hypothesis 2 on the improvement in child learning, at 4-month follow-up, repeated measures ANOVA results were significant for HKCAS-P cognition scores, F(2, 188) = 162.49–171.57, p < .001, partial η2 = .63–.65. Post hoc analyses (Bonferroni adjustment) indicated that the HKCAS-P cognition scores at all three time points differed significantly from one another, with steady increases at each time point. The results indicated that the participants could maintain their program gains at 4-month follow-up.
For Hypothesis 3 on the improvement in parent and teacher report on child learning, repeated measures ANOVA results were significant for parent report of school readiness, F(2, 194) = 29.92–32.77, p < .001, partial η2 = .24–.25, academic competence, F(2, 194) = 18.14–18.87, p < .001, partial η2 = .16–.16, effort motivation, F(2, 194) = 9.83–11.30, p < .001, partial η2 = .09–.10, and task motivation, F(2, 194) = 9.32–10.51, p < .001, partial η2 = .09–.10. Furthermore, repeated measures ANOVA results were significant for teacher report of school readiness, F(2, 194) = 60.43–62.52, p < .001, partial η2 = .38–.39, academic competence, F(2, 194) = 53.23–54.92, p < .001, partial η2 = .35–.36, effort motivation, F(2, 194) = 30.23–32.42, p < .001, partial η2 = .24–.25, and task motivation, F(2, 194) = 28.83–31.19, p < .001, partial η2 = .23–.24. Post hoc analyses (Bonferroni adjustment) indicated that for parent report of school readiness, teacher report of school readiness, and academic competence, the scores at all three time points differed significantly from one another, with steady increases at each time point. For parent report of academic competence, effort motivation, and task motivation, teacher report of effort and task motivation, the postintervention and follow-up scores were significantly higher than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. The results indicated that the participants could maintain their program gains at 4-month follow-up.
With regard to Hypothesis 4 on the improvement in child health outcomes, at 4-month follow-up, repeated measures ANOVA results were significant for frequency of tooth brushing, F(2, 194) = 11.77–13.08, p < .001, partial η2 = .11–.12, home injury, F(2, 194) = 12.53–13.46, p < .001, partial η2 = .11–.12, sedentary activities, F(2, 194) = 6.75–7.29, p = .002–.001, partial η2 = .07–.07, and healthy feeding practice, F(2, 194) = 36.89–39.47, p < .001, partial η2 = .28–.30. The results were not significant for casualty department visits, F(2, 194) = 0.50–0.84, p = .539–.391, partial η2 = .01–.01. Post hoc analyses (Bonferroni adjustment) indicated that for frequency of tooth brushing and healthy feeding practice, the postintervention and follow-up scores were significantly higher than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. Post hoc analyses (Bonferroni adjustment) indicated that for home injury, the postintervention and follow-up scores were significantly lower than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. For sedentary activities, the postintervention scores were significantly lower than the preintervention scores. The results indicated that the participants could maintain their program gains at 4-month follow-up.
For Hypothesis 5 on the improvement in parenting outcomes, at 4-month follow-up, repeated measures ANOVA results were significant for parenting stress, F(2, 194) = 42.37–46.81, p < .001, partial η2 = .30–.33, self-efficacy, F(2, 194) = 14.84–16.59, p < .001, partial η2 = .13–.15, and social support, F(2, 194) = 9.35–10.63, p < .001, partial η2 = .09–.10. For parenting stress, post hoc analyses (Bonferroni adjustment) indicated that the postintervention and follow-up scores were significantly lower than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. For social support and self-efficacy, the postintervention and follow-up scores were significantly higher than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. The results indicated that the participants could maintain their program gains in terms of parenting outcomes.
Analysis of postintervention outcomes based on complete data
In terms of Hypothesis 1 on the reduction in child behavior problems, linear mixed method regression results were significant for ECBI-Intensity, z = 4.22, p < .001, d = 0.64, 95% CI [0.36, 0.91], and ECBI-Problem, z = 5.03, p < .001, d = 0.68, 95% CI [0.40, 0.95]. Intervention group participants reported lower child behavior problem scores at postintervention than wait-list control group participants.
In terms of Hypothesis 2 on the improvement in child learning, linear mixed method regression results were not significant for HKCAS-P cognition scores, z = 1.20, p = .229, d = 0.00, 95% CI [−0.27, 0.27].
In terms of Hypothesis 3 on the improvement in parent and teacher report on child learning, linear mixed method regression results were significant for parent report of academic competence, z = 2.37, p = .018, d = 0.26, 95% CI [−0.01, 0.53], task motivation, z = 3.25, p = .001, d = 0.38, 95% CI [0.11, 0.65], and effort motivation, z = 2.95, p = .003, d = 0.26, 95% CI [−0.01, 0.52]. The intervention group participants reported higher scores on these measures at postintervention than the wait-list control group participants. However, the results were not significant for parent report of school readiness, z = 0.23, p = .821, d = −0.03, 95% CI [−0.30, 0.24], teacher report of school readiness, z = 1.46, p = .143, d = −0.04, 95% CI [−0.31, 0.23], academic competence, z = 1.61, p = .107, d = 0.05, 95% CI [−0.22, 0.31], task motivation, z = 0.91, p = .361, d = 0.00, 95% CI [−0.26, 0.27], and effort motivation, z = 1.30, p = .194, d = −0.07, 95% CI [−0.34, 0.20].
In terms of Hypothesis 4 on the improvement in child health outcomes, linear mixed method regression results were significant for frequency of tooth brushing, z = 3.32, p = .001, d = 0.32, 95% CI [0.05, 0.59], and healthy feeding practice, z = 2.95, p = .003, d = 0.45, 95% CI [0.17, 0.72], with the intervention group participants reporting higher frequency of tooth brushing and healthier feeding practice at postintervention than the wait-list control group participants. The results were not significant for sedentary activities, z = 1.84, p = .066, d = 0.45, 95% CI [0.18, 0.72], home injury, z = 0.25, p = .802, d = 0.11, 95% CI [−0.15, 0.38], and casualty department visits, z = 1.42, p = .155, d = −0.21, 95% CI [−0.48, 0.06].
For Hypothesis 5 on the improvement in parenting outcomes, linear mixed method regression results were significant for parenting stress, z = 5.04, p < .001, d = 0.66, 95% CI [0.38, 0.93], and self-efficacy, z = 5.17, p < .001, d = 0.58, 95% CI [0.30, 0.84]. The intervention group participants reported lower parenting stress and higher self-efficacy at postintervention, compared with the wait-list control group participants. Linear mixed method regression results were not significant for social support, t = 0.31, p = .758, d = 0.10, 95% CI [−0.17, 0.37].
Analysis of 4-month follow-up results based on complete data
For Hypothesis 1 on the reduction in child behavior problems, repeated measures ANOVA results were significant for ECBI-Intensity, F(2, 186) = 51.23, p < .001, partial η2 = .36, and ECBI-Problem, F(2, 186) = 92.18, p < .001, partial η2 = .50. Post hoc analyses (Bonferroni adjustment) indicated that for ECBI-Intensity, the postintervention and follow-up scores were significantly lower than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. For ECBI-Problem, scores at all three time points differed significantly from one another, with steady decreases at each time point.
In terms of Hypothesis 2 on the improvement in child learning, at 4-month follow-up, repeated measures ANOVA results were also significant for HKCAS-P cognition scores, F(2, 178) = 160.74, p < .001, partial η2 = .64. Post hoc analyses (Bonferroni adjustment) indicated that the HKCAS-P cognition scores at all three time points differed significantly from one another, with steady increases at each time point.
In terms of Hypothesis 3 on the improvement in parent and teacher report on child learning, repeated measures ANOVA results were significant for parent report of school readiness, F(2, 186) = 30.60, p < .001, partial η2 = .25, academic competence, F(2, 186) = 18.68, p < .001, partial η2 = .17, effort motivation, F(2, 186) = 11.24, p < .001, partial η2 = .11, and task motivation, F(2, 186) = 10.64, p < .001, partial η2 = .10. Furthermore, repeated measures ANOVA results were significant for teacher report of school readiness, F(2, 186) = 57.25, p < .001, partial η2 = .38, academic competence, F(2, 186) = 49.55, p < .001, partial η2 = .35, effort motivation, F(2, 186) = 29.34, p < .001, partial η2 = .24, and task motivation, F(2, 186) = 28.96, p < .001, partial η2 = .24. Post hoc analyses (Bonferroni adjustment) indicated that for parent report of school readiness, teacher report of school readiness, academic competence, and task motivation, scores at all three time points differed significantly from one another, with steady increases at each time point. For parent report of academic competence, effort motivation, and task motivation, and teacher report of effort motivation, the postintervention and follow-up scores were significantly higher than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores.
With regard to Hypothesis 4 on the improvement in child health outcomes, at 4-month follow-up, repeated measures ANOVA results were significant for frequency of tooth brushing, F(2, 186) = 13.44, p < .001, partial η2 = .13, home injury, F(2, 186) = 12.62, p < .001, partial η2 = .12, sedentary activities, F(2, 186) = 5.63, p = .004, partial η2 = .06, and healthy feeding practice, F(2, 186) = 37.27, p < .001, partial η2 = .29. The results were not significant for casualty department visits, F(2, 186) = 0.60, p = .484, partial η2 = .01. Post hoc analyses (Bonferroni adjustment) indicated that for frequency of tooth brushing and healthy feeding practice, the postintervention and follow-up scores were significantly higher than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. Post hoc analyses (Bonferroni adjustment) indicated that for home injury, the postintervention and follow-up scores were significantly lower than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. For sedentary activities, the postintervention scores were significantly lower than the preintervention scores.
For Hypothesis 5 on the improvement in parenting outcomes, at 4-month follow-up, repeated measures ANOVA results were significant for parenting stress, F(2, 186) = 43.45, p < .001, partial η2 = .32, self-efficacy, F(2, 186) = 17.38, p < .001, partial η2 = .16, and social support, F(2, 186) = 8.75, p < .001, partial η2 = .09. For parenting stress, post hoc analyses (Bonferroni adjustment) indicated that the postintervention and follow-up scores were significantly lower than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. For social support and self-efficacy, the postintervention and follow-up scores were significantly higher than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores.
Parent Ambassadors
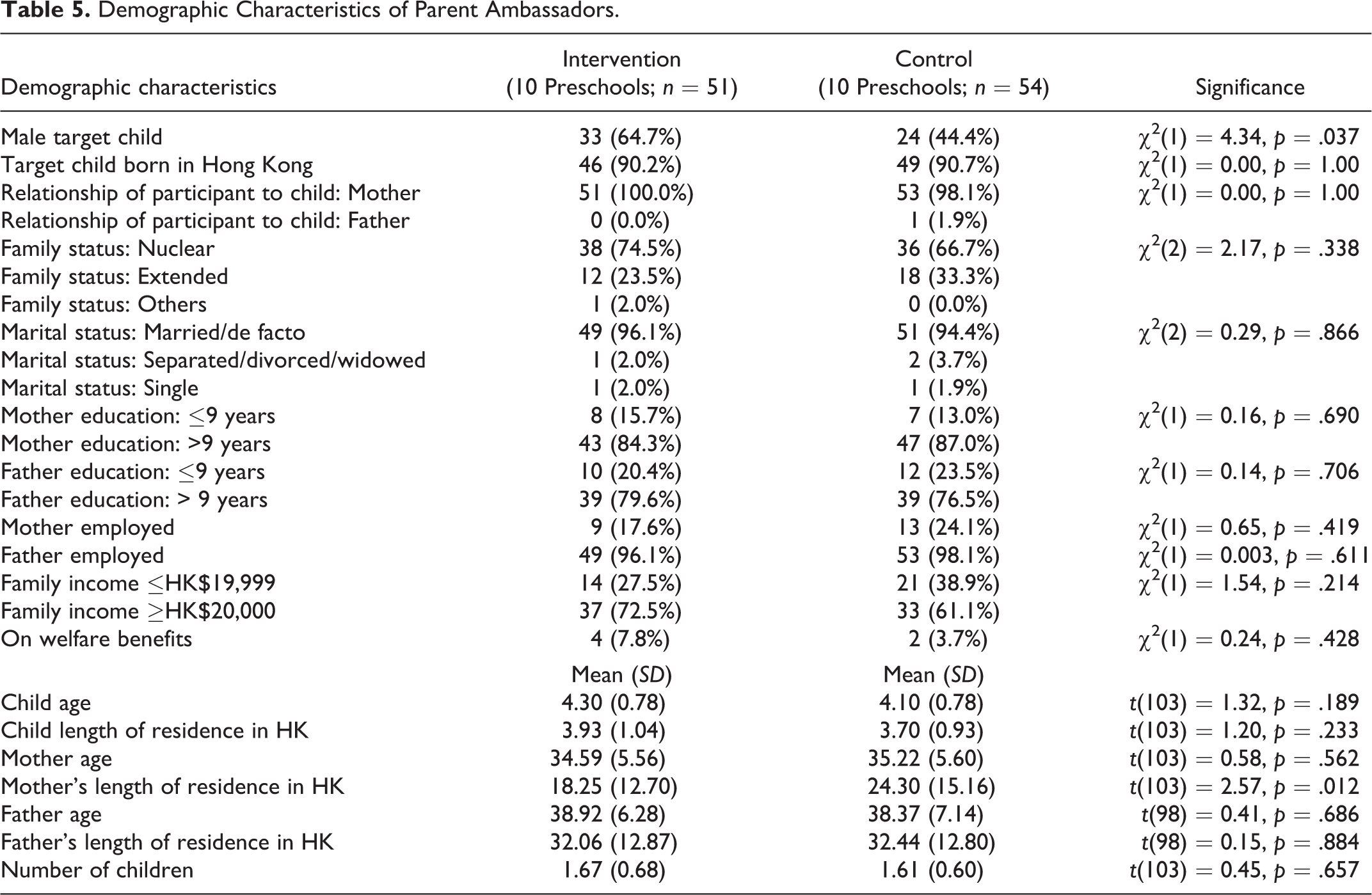
Little’s MCAR test was not significant, indicating that the data were missing completely at random. The intervention and wait-list control group parent ambassadors differed in terms of mother’s length of residence in Hong Kong and child sex. In the linear mixed method regression analyses reported below, the fixed factors were group status, preintervention scores, child sex, and mother’s length of residence in Hong Kong. The dependent variables were the postintervention scores, with the preschool as a random factor. The demographic characteristics of the parent ambassadors are in Table 5. The mean and standard deviation of the pre, post, and follow-up scores are in Table 6.
Demographic Characteristics of Parent Ambassadors.
Preintervention, Postintervention, and Follow-Up Scores of Parent Ambassadors.

Note. ECBI = Eyberg Child Behavior Inventory.
Intention-to-treat results
At postintervention, linear mixed method regression results were significant for ECBI-Intensity, t = 6.70, p < .001, d = 1.11, 95% CI [0.69, 1.51], ECBI-Problem, t = 6.32, p < .001, d = 1.00, 95% CI [0.59, 1.40], parenting stress, t = 3.57, p < .001, d = 0.73, 95% CI [0.33, 1.12], self-efficacy, t = 3.30, p = .001, d = 0.61, 95% CI [0.21, 0.99], and social support, t = 2.31, p = .022, d = 0.42, 95% CI [0.03, 0.80]. The intervention group parent ambassadors reported lower child behavior problems and parenting stress, higher social support, and self-efficacy at post-intervention, compared with the wait-list control group parent ambassadors.
At 4-month-follow-up, repeated measures ANOVA results were significant for ECBI-Intensity, F(2, 96) = 48.98–50.85, p < .001, partial η2 = .51–.51, ECBI-Problem, F(2, 96) = 47.38–48.49, p < .001, partial η2 = .50–.50, parenting stress, F(2, 96) = 42.29–44.09, p < .001, partial η2 = .47–.48, self-efficacy, F(2, 96) = 8.42–9.59, p = .002–.001, partial η2 = .15–.17, and social support, F(2, 96) = 7.74–8.25, p = .003–.002, partial η2 = .14–.15. Post hoc analyses (Bonferroni adjustment) indicated that for ECBI-Intensity, ECBI-Problem, and parenting stress, the postintervention and follow-up scores were significantly lower than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. For social support and self-efficacy, the postintervention and follow-up scores were significantly higher than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. The results indicated that the parent ambassadors could maintain their program gains.
Analysis based on complete data
Linear mixed method regression results were significant for ECBI-Intensity, z = 7.46, p < .001, d = 1.17, 95% CI [0.73, 1.58], ECBI-Problem, z = 7.09, p < .001, d = 1.04, 95% CI [0.62, 1.45], parenting stress, z = 3.94, p < .001, d = 0.78, 95% CI [0.37, 1.18], social support, z = 2.61, p = .009, d = 0.45, 95% CI [0.05, 0.85], and self-efficacy, z = 3.48, p < .001, d = 0.66, 95% CI [0.25, 1.05]. The intervention group parent ambassadors reported lower child behavior problems and parenting stress, higher social support and self-efficacy at postintervention, compared with the wait-list control group parent ambassadors.
At 4-month-follow-up, repeated measures ANOVA results were significant for ECBI-Intensity, F(2, 94) = 47.87, p < .001, partial η2 = .51, ECBI-Problem, F(2, 94) = 45.58, p < .001, partial η2 = .49, parenting stress, F(2, 94) = 41.71, p < .001, partial η2 = .47, self-efficacy, F(2, 94) = 9.12, p = .001, partial η2 = .16, and social support, F(2, 94) = 8.40, p = .002, partial η2 = .15. Post hoc analyses (Bonferroni adjustment) indicated that for ECBI-Intensity, ECBI-Problem, and parenting stress, the postintervention and follow-up scores were significantly lower than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. For social support and self-efficacy, the postintervention and follow-up scores were significantly higher than the preintervention scores, but there was no significant difference between the postintervention and follow-up scores. The results indicated that the parent ambassadors could maintain their program gains.
Discussion and Applications to Practice
Hypothesis 1 on the reduction in child behavior problems was supported. At postintervention, the intervention group participants reported lower child behavior problems than the wait-list control group participants. They could also maintain their program gains at 4-month follow-up. The results were consistent with that of the Healthy Start Home Visit Program (C. Leung et al., 2015), as well as other group-based parent training programs such as PACE and HOPE (C. Leung et al., 2011; C. Leung et al., 2017).
Hypothesis 2 on the improvement in child learning was not supported. There was no significant difference in terms of individual child assessment results on cognitive skills. In the present school-based program, the sessions on child learning were reduced, compared with the original home visiting program (C. Leung et al., 2015), and this might have explained the results.
Hypothesis 3 on the improvement in parent and teacher report of child learning was partially supported. At postintervention, the intervention group participants reported higher parent report of academic competence, task, and effort motivation, as well as teacher report of academic competence than the wait-list control group participants. The participants were also able to maintain their program gains at 4-month follow-up. The results were consistent with that of the Healthy Start Home Visit Program (C. Leung et al., 2015), as well as other group-based parent training programs such as PACE (C. Leung et al., 2017). However, there was no significant difference in terms of most teacher reports of child learning. In a group of children, it might be more difficult for the teachers to observe changes in learning motivation as the changes might be more subtle. Parents might notice the changes in their children more easily.
Hypothesis 4 on the improvement in child health outcomes was partially supported. At postintervention, there was an increase in frequency of tooth brushing and healthy feeding practice in the intervention group, compared with the wait-list control group. However, there was no significant difference in terms of sedentary activities and home injury. The results were consistent with that of the Healthy Start Home Visit Program (C. Leung et al., 2015). The incidence of home injury was relatively low at preintervention and this might be a possible explanation for the lack of improvement.
Hypothesis 5 on the improvement in parenting outcomes was partially supported. At postintervention, there was a significant decrease in parenting stress and an increase in self-efficacy in the intervention group, compared with the wait-list control group. However, the results were not significant for social support. The results were consistent with that of the Healthy Start Home Visit Program (C. Leung et al., 2015), except for social support. In a home visiting program where the program was delivered to the parents on an individual basis, there were more opportunities for personal sharing and relationship building. In a group setting, participants might be less willing or had less chance to share personal or family difficulties with other group members, and they perceived no significant enhancement in social support. The sensitivity of the scale might have affected the usefulness of the scale in different contexts. It is also possible that those parents who were willing to join educational programs might already enjoy reasonable social support, thus making it hard to show further significant gains.
With a home visiting program, program attendance could be flexibly arranged according to the parent’s schedule, and the parents would not have to travel to attend the program. This arrangement made a 20-session program less demanding to the parents. In a school-based program where parents have to attend 20 sessions, it could be perceived as rather demanding. In order to make it appear less demanding to parents, and to minimize inconvenience to the participating preschools, the program was reduced to 12 sessions, with sessions on child learning reduced, and sessions on child health topics covered in the form of mass lectures. The reduction in learning sessions might explain the present child learning outcomes. Although the children were attending preschools, parents might still need tailored support to equip them to facilitate the learning of their children.
For the parent ambassadors, they reported significant decrease in child behavior problems and parenting stress and significant increase in social support and self-efficacy after completion of training and program delivery. The results are consistent with that in the Healthy Start Home Visit Program (C. Leung et al., 2015). However, in the C. Leung et al. (2015) study, there was no control group of parent ambassadors and the results could be due to test or practice effect. In the present study, with a control group, the effectiveness of the parent ambassador program could be more clearly ascertained. The parent ambassadors would be a potential social capital for the preschools because with their enhanced identity as “parent ambassadors”, tailored training and regular supervision by the project team, as well as hands-on practice to deliver their support to families assigned under their care, they own the relevant knowledge, attitude, and skills to perform.
There were some limitations in this study. First, the 4-month follow-up results involved only the intervention group participants, as the wait-list control group participants were offered the program after the intervention group participants had completed the intervention. The follow-up results could not be entirely attributed to the intervention. Second, the parenting and child behavior outcome measures were based on parent report only. Third, though the facilitators delivered the program according to a manual, there was only irregular independent fidelity check. Fourth, the sample size might be inadequate for teacher measures and the sample size for parent ambassadors was less than that required, thus affecting the power of the study. Finally, our design did not control for placebo effect, social desirability, and the wish to please the researchers. These should be taken into consideration in the interpretation of results.
This study, which involved community partners and large sample sizes, also brought fruitful insights on research and practice. In terms of research, the experience showed that even in the preschool context, good understanding and support for rigorous research could be implemented if the research team could clearly articulate the importance of such studies and provide needed support (e.g., designated social worker coordinating the whole project, regular team meetings with the project team, and participating partners for direct communication). In this case, bringing randomized controlled trial studies into more preschools was made possible through the fruitful track record of the project team and convincing witnessing by former participating preschools in the Healthy Start Home Visit Program. When more community partners embrace the need for evidence-based practice, future studies can strive for larger samples, longer follow-up studies, and including control group in the follow-up evaluation.
In terms of practice, the project identified some good practices in the engagement of community partners to join the project and parents to join as ambassadors or beneficiaries. The personal recommendations among preschool principals and key teachers engaged the participating preschools to join a randomized controlled trial study, while the personal recommendations among parents engaged more parents to enroll to help or to learn. Face-to-face briefing meetings also facilitated firsthand understanding of the project and allowed direct communication to clarify questions and sort out logistic hurdles. With the growing critical mass that enjoyed the benefits of the project, it will help to foster the proper culture to develop and subscribe to evidence-based services.
In this project, some adjustments were made to transform the original home visitation–based program into a school-based one, including reducing the number of sessions to 12, pairing social workers and parent ambassadors to make home visits to participant families, and giving new duties to the parent ambassadors. They had to facilitate in role-play demonstrations and group discussions in the parent training sessions. Their work was facilitated by school representatives who provided logistic support. This service model facilitated a transdisciplinary approach to get different professionals to work seamlessly with parents and young children. This is a step forward in fostering early identification and intervention should young families encounter issues and need to seek help. Having peers, social workers, and teachers with the right mind-set to empathize and encourage should have extended and strengthened the support safety net, and quantitative evidence on this should be collected in future studies.
The other successful strategic program adjustment was to maintain a compulsory home visit within the program even when the whole project shifted from home- to school-based. It relieved the hesitation of some families to open their residences for multiple visits by “strangers” but maintained the compulsory home visit as a “safety check” to ensure participant families do not harbor child safety hazards. Such home visits helped the visiting social worker and parent ambassador to better understand the family in context, fine-tune their team work, and ascertain the safety standard of the homes according to the checklists developed in the Healthy Start Home Visit Program. If the home environment is adversarial, further support could be rendered by the NGO providing social services. These are reasonable measures to ensure home safety while making the program more cost-efficient and sustainable, as well as less threatening to parents new to such services.
Overall, the present results provided initial evidence on the effectiveness of the HSS. There were encouraging benefits for the participating parents, target children, and the parent ambassadors.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by The Quality Education Fund, Education Bureau, Hong Kong SAR Government.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.