
Abstract
Purpose:
The study assessed the effectiveness of computerized brief interventions (CBIs) for youth (aged 15–25) defined as risky alcohol users.
Methods:
We searched 10 electronic databases. Eligible studies were randomized and quasi-randomized controlled trials examining the effect of CBIs for youth.
Results:
Fifty-three studies with 33,316 participants were included. Moderate quality evidence showed CBIs to reduce risky alcohol use compared to single-dose assessment. Short-term (<6 months) effects were overall larger than long-term (≥6 months) effects. None of the studies reported adverse effects.
Conclusions:
The positive effects, easy administration, and lack of adverse effects of CBIs indicate that such brief interventions are a feasible way to reduce risky alcohol use in youth.
Risky alcohol use among youth remains a substantial public health issue (United Nations, 2003; United Nations Office on Drugs and Crime, 2010), and harmful use of alcohol is the leading risk factor for death and disability for persons aged 15–49 years (World Health Organization, 2014). Alcohol misuse represents a societal burden due to costs related to health and social care, law enforcement, and welfare assistance, as well as costs resulting from reduced productivity and increased mortality (Thavorncharoensap, Teerawattananon, Yothasamut, Lertpitakpong, & Chaikledkaew, 2009). High consumption of alcohol is directly related to risky behaviors such as intoxicated driving, unprotected sexual intercourse, and interpersonal violence (Cherpitel, Ye, Bond, & Borges, 2003; Foran & O’Leary, 2008; Jennison, 2004; Karam, Kypri, & Salamoun, 2007; Miller, Naimi, Brewer, & Jones, 2007). In addition, youth binge drinking can have both short- and long-term negative impacts on an individual’s health, cognitive functions (Lopez-Caneda et al., 2013), and increases the risk of developing alcohol (Jennison, 2004) and other substance use disorders (Odgers et al., 2008). Thus, there is a need for early interventions to reduce or eliminate risky alcohol use among youth.
Many countries have made prominent efforts ranging from government policy initiatives to primary health-care services to minimize the long-term consequences of alcohol use. Implementing screening and brief interventions for youth at risk of alcohol problems might have several advantages (Roche & Freeman, 2004). However, the effects of brief interventions for reducing risky alcohol use are still unclear and should be examined with systematic methods.
Computerized Brief Interventions
Brief interventions primarily work through two main mechanisms: (1) by making the clients think differently about their risky use and (2) by providing them with competence to change their behavior if they are motivated to change. It has been suggested that the assessment component of brief interventions alone might lead to behavioral change (Kaner et al., 2013), particularly in primary care settings (O’Donnell et al., 2014). In addition, studies indicate that computerized interventions with feedback elements can lead to some reductions in the use of alcohol and other substances over time (LaBrie, Hummer, Neighbors, & Pedersen, 2008; Suffoletto, Callaway, Kristan, Kraemer, & Clark, 2012).
The rapid advancement of technology and increasing digitalization of health-care services have introduced a new type of interventions, namely computerized brief interventions (CBIs). CBIs include both online and offline interventions (e.g., software, websites, and downloadable applications (i.e., “apps”) delivered via electronic devices such as personal computers, tablets, and smartphones. The majority of CBIs include three components: assessment, feedback, and decision-making. The computerized algorithm first assesses the user’s risk profile (e.g., low, medium, or high). This is followed by the feedback session, which often includes the assessment results and delivery of a psychoeducation component suited according to the user’s risk profile through interactive computer programming. Lastly, the decision-making module helps to identify the user’s readiness for change. CBI can help promote a sense of anonymity and may allow users to provide honest alcohol use information (Moyer & Finney, 2004).
The main benefit of CBI is its large reach, low cost, and simulation of an “interpersonal therapeutic component” by targeting recipients’ feedback and its appeal to youth used to digital media (Fox, 2006; Fox & Duggan, 2013). The underrepresentation of youth among users of standard face-to-face alcohol and other drug specialist services warrants the use of more effective media, such as computerized interventions, to reach this population.
Previous reviews and meta-analyses examining Internet-based interventions (Tait & Christensen, 2010) and online alcohol interventions (White et al., 2010) have studied the effects of CBI delivered as stand-alone or in combination with face-to-face interventions. Tait and Christensen (2010) limited their review to studies targeting youth younger than 25 years with problematic substance use. Moreover, they did not explicitly differentiate between specific substances and focused solely on CBI. White et al. (2010) included studies on the effect of online-alcohol interventions more generally, without limitation to age and time range. These reviews have focused either on the universal prevention of problematic substance use or on the treatment and rehabilitation of individuals who have established substance dependency. Most focus solely on computerized interventions are limited to college students and thus exclude groups of youth who are not attending college.
The aim of this review is to assess the effectiveness of CBIs to prevent the development of alcohol use in risky youth users (aged 15–25), by synthesizing data from randomized and quasi-randomized controlled trials. The review is an abridged version of a Campbell systematic review (Smedslund et al., 2017).
Differences Between the Campbell Systematic Review and This Article
In addition to alcohol, the Campbell review included studies about cannabis. As we found few studies targeting cannabis, and no studies found significant effects on cannabis consumption, we focus exclusively on alcohol outcomes in the present review. In order to make the article more readable, we removed some of the comparisons in the original Campbell review: feedback plus moderation skills versus feedback only, gender-specific feedback versus gender-neutral feedback, and multidose assessment and feedback versus single-dose assessment and feedback. Few studies we reviewed provided information on these three comparisons, and the results did not add much to the overall findings.
Method
Search for Literature
In May 2016, we searched a selection of bibliographic and gray literature databases covering the research fields of medicine/health care, psychology, education, and social studies. We also searched registries of ongoing and unpublished studies. Our search strategies are detailed in the Campbell review (Smedslund et al., 2017). Individual search strategies combining text words and database-specific subject headings were adapted to each database. The search strategy combined two search blocks with the Boolean operator “AND.” The first search block are terms related to risky alcohol or cannabis intake, and the second block are related to computers, apps, social media, and so on. The subject headings and text words in each block were combined with the Boolean operator “OR.” To restrict the retrieval of references to the study types defined in the protocol, we added a filter for study design. We screened reference lists of included studies and relevant systematic reviews.
The complete search strategy for one of the databases (Ovid MEDLINE) and a list of the names of databases used are given in Online Appendix 1. We searched for both alcohol and cannabis, but this article only presents the alcohol studies.
Eligibility Criteria
We included all randomized or quasi-randomized controlled trials of any CBI used as a stand-alone treatment aimed at reducing alcohol consumption (see Table 1). Eligible comparators included no intervention, waiting list control, or an alternative brief intervention (computerized or noncomputerized). Participants were young people between 15 and 25 years of age defined as risky consumers of alcohol. Males were considered as at risk if they consumed five or more drinks in a single occasion or if they consumed 14 or more drinks a week. Females were considered risky consumers if they consumed four or more in a single occasion or if they had seven or more drinks a week.
Eligibility Criteria.

Data Collection
Two reviewers independently screened abstracts and read full texts according to inclusion criteria. A third reviewer resolved disagreements. The reviewers used a predefined data extraction form to extract data (e.g., participants, design, sample size, outcomes, and results) and independently rated each selected study on the risk of bias (RoB) domains developed by Cochrane (Higgins & Green, 2011). A third reviewer resolved disagreements. The quality of evidence was assessed and rated using Grading of Recommendations Assessment, Development and Evaluation (GRADE, 2015).
Data Analysis and Synthesis
Results of the syntheses are reported for short- and long-term follow-up time points by primary outcome of interest. We used risk ratios or rate ratios for dichotomous outcomes, and standardized mean differences for continuous outcomes. Effect sizes were reported along with their 95% confidence intervals (CIs). We calculated effect sizes with Review Manager 5.3 (2014) or from past published meta-analyses, when we did not manage to obtain effect sizes from primary study authors.
We investigated the following factors, with the aim of explaining any observed heterogeneity: characteristics of the control condition (no intervention, assessment only, other active intervention, etc.). We assessed the heterogeneity between studies using I 2 and τ2 statistics (Higgins & Green, 2011). We conducted sensitivity analysis to assess whether selection bias and attrition bias affected the overall effect size, 95% CI, and I 2. The sensitivity analyses were executed when there were 10 or more studies included in the meta-analysis. To examine reporting bias, we compared the published report with the pretrial protocols when the protocols were available. When there were 10 or more studies, we used funnel plots to assess publication bias.
Results
The searches (including searches for cannabis use) identified 7,553 records, with 7,111 resulting from the search of the electronic databases and 442 from gray literature searches (see Figure 1). We retrieved 197 references in full text after excluding duplicates, of which 53 studies with alcohol users met criteria for inclusion after reading full texts. Main reasons for exclusion after full text readings were (i) participants were not high-risk drinkers (n = 81), (ii) the intervention did not meet inclusion criteria (n = 31), (iii) the study design did not meet inclusion criteria (n = 8), (iv) authors did not report included outcomes (n = 8), or (v) an effect size was not reported and could not be computed (n = 16). We excluded 144 studies after reviewing the full text. For detailed information on excluded studies, see the full Campbell review (Smedslund et al., 2017).
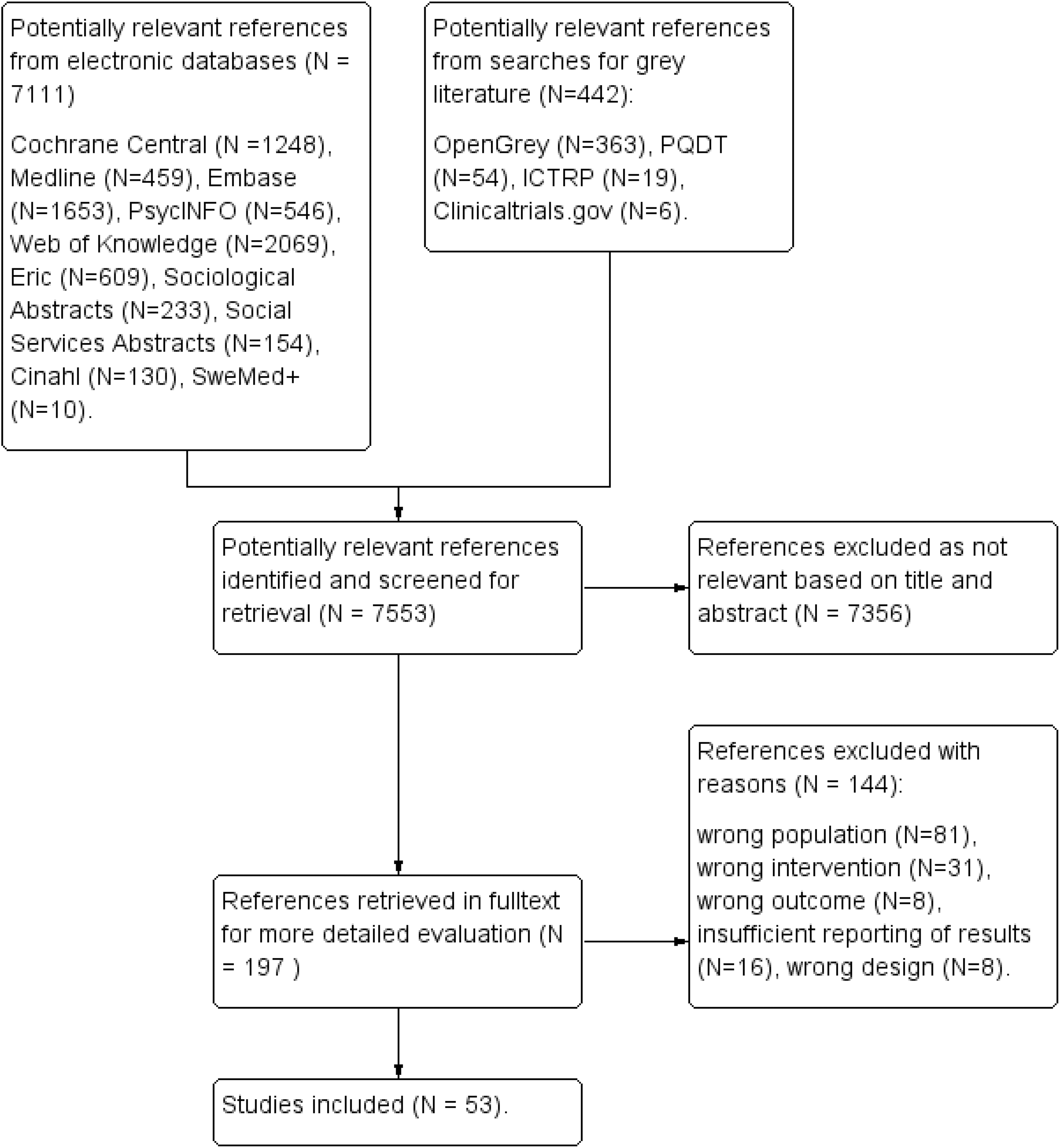
Flow chart for study flow.
The included studies (n = 53) were published between 2004 and 2016 (see Table 2 for characteristics of included studies). Most of the studies (n = 39) were conducted in the United States. The number of participants varied between 18 and 3,422, and the percent females ranged from 0 to 82. Most interventions involved some kind of assessment, followed by personalized feedback compared to average values among peers. The duration of intervention was poorly reported, probably because the participants were free to visit the program webpage as often and as long as they wanted. Most interventions were delivered on the Internet, but some studies only reported that they were delivered using a computer. A few interventions were designed as e-mails. The comparison groups received no intervention (e.g., waitlist), attention control, assessment only, usual care, or education (e.g., a leaflet). A few computerized interventions were compared with face-to-face interventions. The follow-up durations ranged between 1 week and 1 year. Almost all studies estimated some combination of quantity and frequency of alcohol consumption. Some of the studies tried to assess heavy episodic drinking, peak exposure, and consequences of alcohol use. The most common assessment instruments used were the Daily Drinking Questionnaire and Alcohol Use Disorders Identification Test.
Characteristics of Included Studies.
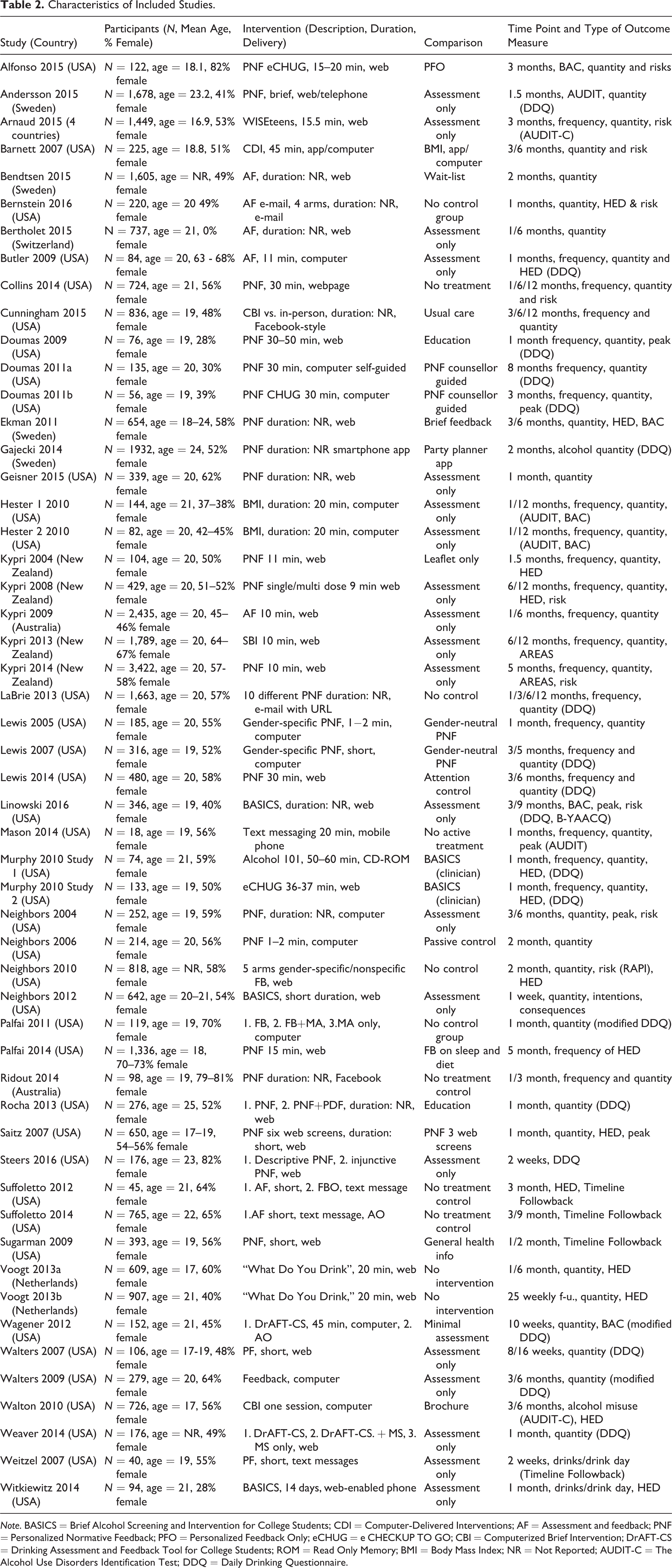
Note. BASICS = Brief Alcohol Screening and Intervention for College Students; CDI = Computer-Delivered Interventions; AF = Assessment and feedback; PNF = Personalized Normative Feedback; PFO = Personalized Feedback Only; eCHUG = e CHECKUP TO GO; CBI = Computerized Brief Intervention; DrAFT-CS = Drinking Assessment and Feedback Tool for College Students; ROM = Read Only Memory; BMI = Body Mass Index; NR = Not Reported; AUDIT-C = The Alcohol Use Disorders Identification Test; DDQ = Daily Drinking Questionnaire.
Approximately two thirds (66%) of the studies were considered to have a high risk of bias on one of the bias domains. The domains with largest proportion of high risk were “blinding of participants and personnel” and “incomplete outcome data.” The largest proportion of unclear risk being recorded was for “selective reporting” and “allocation concealment.” The domains with the lowest risk of bias were “blinding of outcome assessment” and “random sequence generation” (Figure 2).
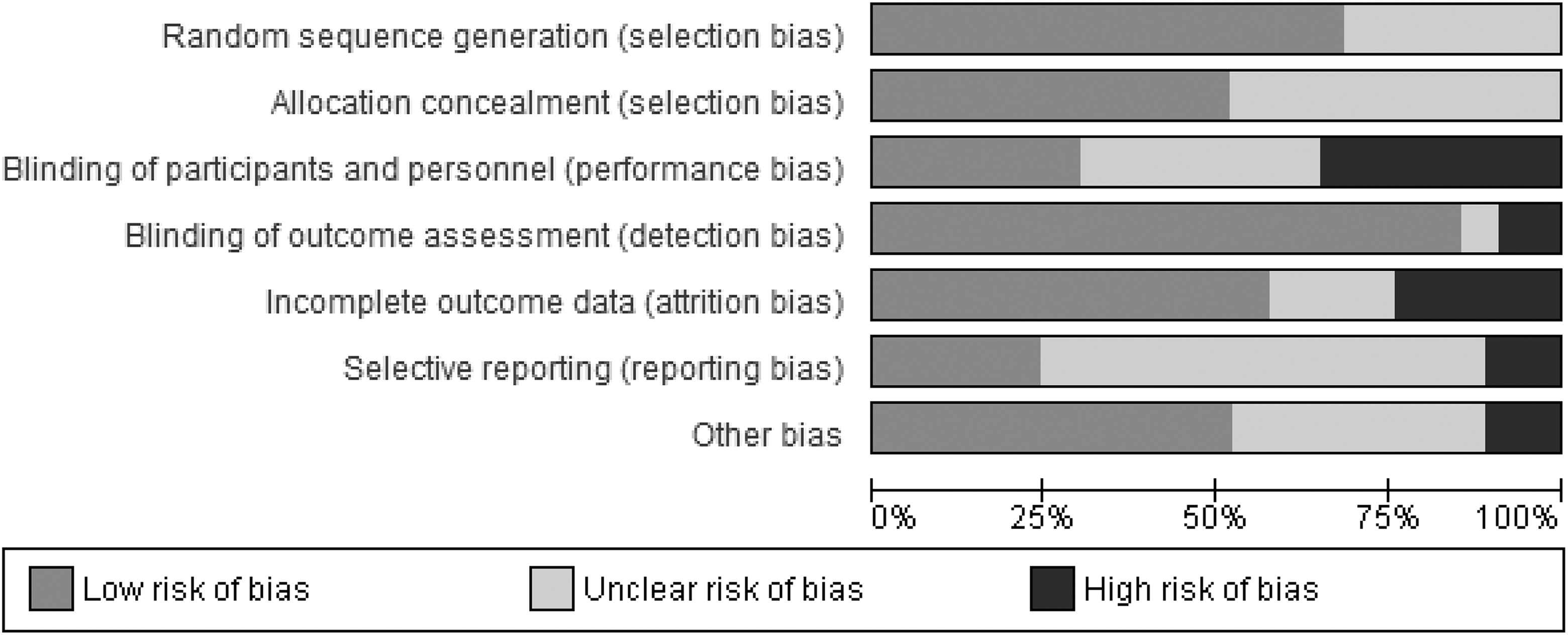
Risk of bias in the included studies.
Assessment and Feedback Versus No Intervention—Short- and Long-Term Effects
A meta-analysis of 15 studies found that assessment and feedback gave a small reduction in short-term alcohol consumption compared to nointervention (see Table 3; SMD: −0.17, 95% CI [−0.27, −0.08], I 2: 52%), while the effect size for the three studies looking at long-term alcohol consumption were standardized mean difference (SMD): −0.17, 95% CI [−0.30, −0.04]; Table 3). The quality of the evidence was low (Table 3).
Assessment and Feedback Compared to No Intervention—Short and Long Term.
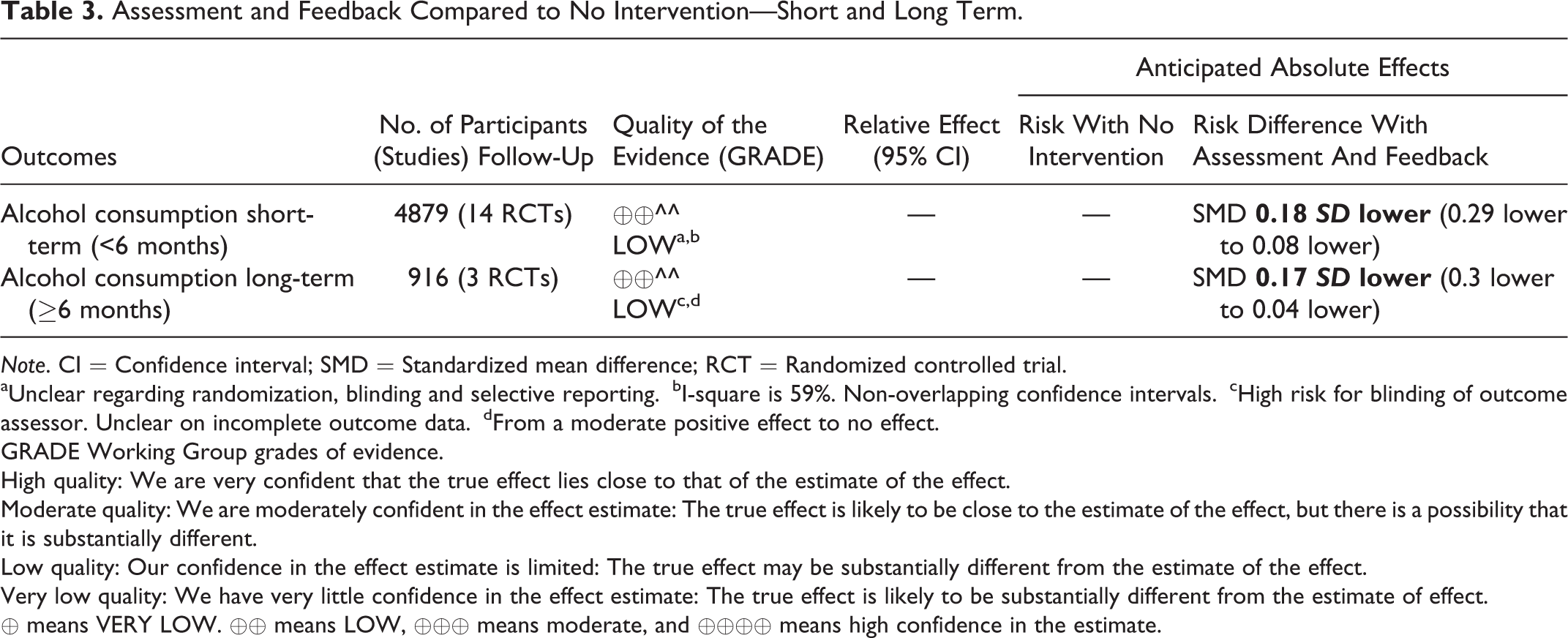
Note. CI = Confidence interval; SMD = Standardized mean difference; RCT = Randomized controlled trial.
aUnclear regarding randomization, blinding and selective reporting.
bI-square is 59%. Non-overlapping confidence intervals.
cHigh risk for blinding of outcome assessor. Unclear on incomplete outcome data.
dFrom a moderate positive effect to no effect.
GRADE Working Group grades of evidence.
High quality: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect.
Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
⊕ means VERY LOW. ⊕⊕ means LOW, ⊕⊕⊕ means moderate, and ⊕⊕⊕⊕ means high confidence in the estimate.
Assessment and Feedback Versus Assessment Only—Short and Long Term
A meta-analysis of 24 studies with 25 independent samples showed a similar effect size as in the comparison of computerized assessment and feedback versus assessment only (SMD: −0.15, 95% CI [−0.25, −0.06) at short term. For the long-term follow-up, there were only three studies, and there was no significant effect (SMD: −0.03, 95% CI: [−0.19, 0.12]). The evidence was of low quality (Table 4).
Assessment and Feedback Compared to Assessment Only- Short and Long Term.
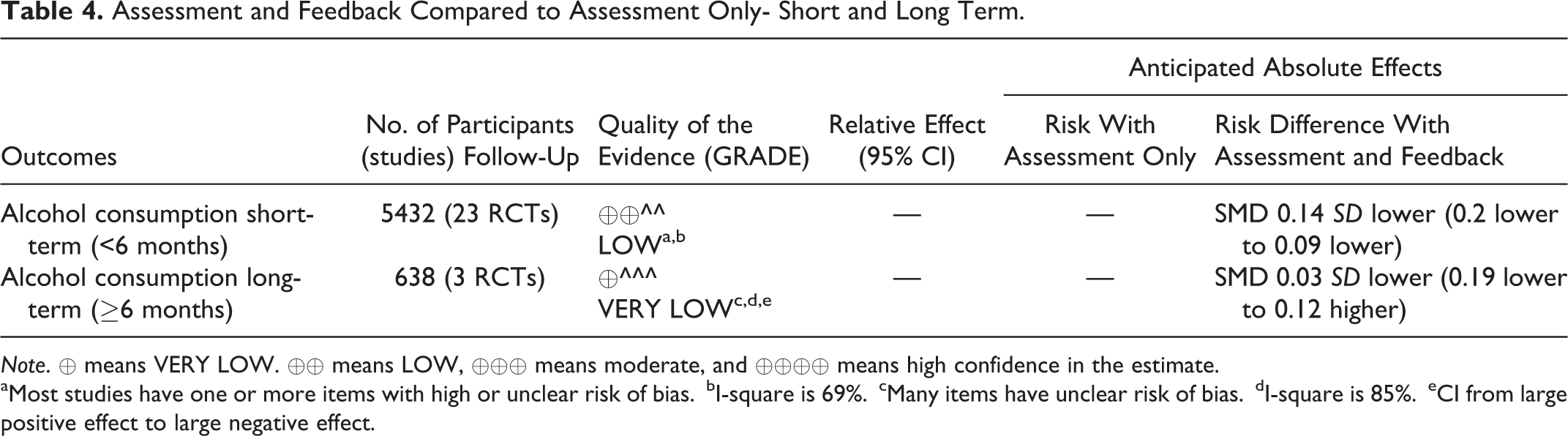
Note. ⊕ means VERY LOW. ⊕⊕ means LOW, ⊕⊕⊕ means moderate, and ⊕⊕⊕⊕ means high confidence in the estimate.
aMost studies have one or more items with high or unclear risk of bias.
bI-square is 69%.
cMany items have unclear risk of bias.
dI-square is 85%.
eCI from large positive effect to large negative effect.
Assessment and Feedback Versus Education—Short and Long Term
A meta-analysis of seven studies showed no significant short-term effect of assessment and feedback compared to education (SMD: −0.02, 95% CI [−0.21, 0.17]). One study (Walton 2013) did not find a significant long-term effect but the effect size (SMD: −0.23, 95% CI [−0.51, 0.04]) was in favor of assessment and feedback over education. The evidence was of very low quality (Table 5).
Assessment and Feedback Compared to Education, Short and Long Term.
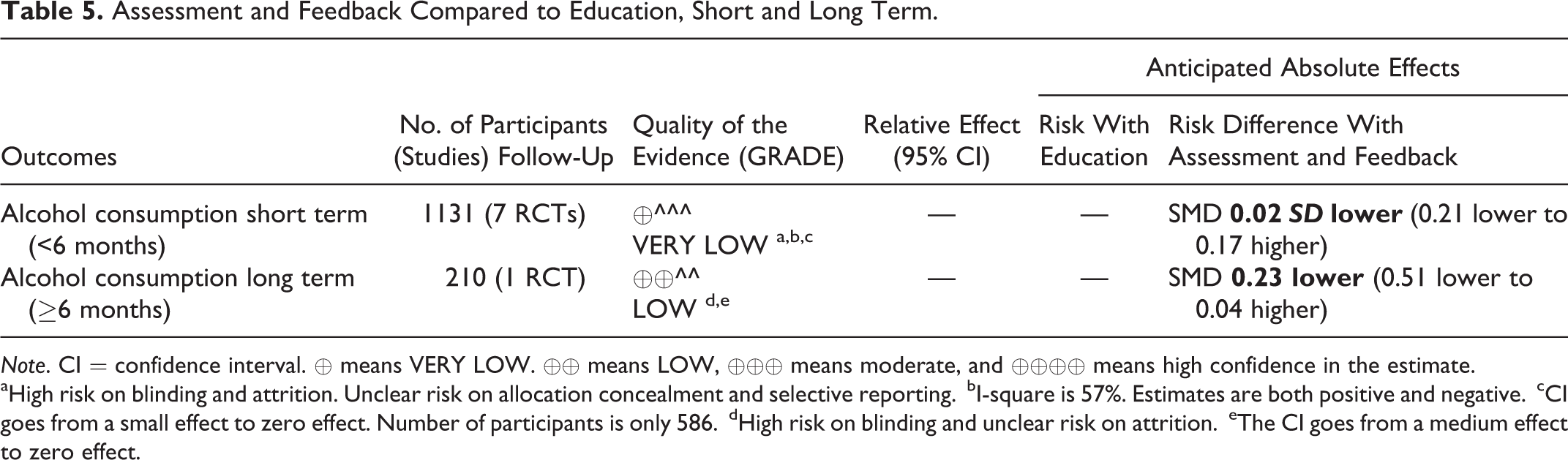
Note. CI = confidence interval. ⊕ means VERY LOW. ⊕⊕ means LOW, ⊕⊕⊕ means moderate, and ⊕⊕⊕⊕ means high confidence in the estimate.
aHigh risk on blinding and attrition. Unclear risk on allocation concealment and selective reporting.
bI-square is 57%. Estimates are both positive and negative.
cCI goes from a small effect to zero effect. Number of participants is only 586.
dHigh risk on blinding and unclear risk on attrition.
eThe CI goes from a medium effect to zero effect.
Comprehensive Feedback Compared to Brief Feedback—Short and Long Term
A meta-analysis of four studies reported no added short-term effect (SMD: −0.01, 95% CI [−0.18, 0.19]) while one study that reported long-term effect (SMD: −0.06, 95% CI [−0.28, 0.16]) found little difference between the groups. The evidence was of low quality (Smedslund et al., 2017).
Computer Assessment and Feedback Versus Counselor Assessment and Feedback—Short and Long Term
A meta-analysis of six studies did not find that the short-term effect of CBI is different from a brief intervention delivered by a counselor (SMD: −0.10, 95% CI [−0.30, 0.11]). In addition, one study (Cunningham et al., 2015) reported incidence ratios (IRs), which could not be entered in the meta-analysis. The IR for computer intervention versus control was 0.88 (95% CI [0.78, 0.99]) and for therapist feedback versus control was 0.86 (95% CI [0.77, 0.98]). The two studies with long-term effects also showed no difference (SMD: −0.11, 95% CI [−0.53, 0.32]). The quality of the evidence for all comparisons were very low (Smedslund et al., 2017).
Comparisons Between Two Types of CBIs
Six studies compared two types of CBI. Brief Alcohol Screening and Intervention for College Students (BASICS) did not have a different short-term effect than either alcohol 101 (SMD: 0.21, 95% CI [−0.25, 0.67]) or Check-Up to Go (eCHUG) (SMD: 0.21, 95% CI [−0.20, 0.63]). A web chat based on motivational interviewing principles (MI chat) had no different effect from a technical chat (SMD: −0.01, 95% CI [−0.31, 0.29]). Adding a personalized drinking feedback (PDF) to a personalized normative feedback (PNF) had no short-term effect on drinking (SMD: 0.23, 95% CI [−0.17, 0.63]). A web-based intervention had a small, significant short-term effect compared to an interactive voice-based intervention (SMD: −0.18, 95% CI [−0.35, −0.01]). There was no difference between a gain-focused and a loss-focused message (SMD: 0.06, 95% CI [−0.20, 0.33]) or between a message focusing on long-term consequences and a message focusing on short-term consequences (SMD: 0.09, 95% CI [−0.17, 0.36]; Smedslund et al., 2017).
Adverse Outcomes and Sensitivity Analysis
We did not find any evidence of adverse effects of CBI in this review. Sensitivity analyses did not show any specific trends (Smedslund et al., 2017).
Discussion
We assessed the effectiveness of brief computerized interventions on reducing risky alcohol consumption for youth aged 15–25 years. We found a small reduction in alcohol consumption short term (<6 months) when BCI was compared to no intervention or assessment only: The quality of the evidence was low. The effect was in general not sustained for long-term measurement (>6 months).
These results are in line with a meta-analysis from 2012 concluding that computerized interventions were effective compared to a control group, but that face-to-face interventions were more effective than computerized interventions (Carey, Carey, Henson, Maisto, & DeMartini, 2011). Tait and Christensen (2010) found an overall effect of Internet-based interventions of d = −.22, but it is difficult to discern if this supports our findings as this was a composite outcome. Six reviews claim to find effects of CBI (Cadigan et al., 2015; Laging, 2012; Portnoy, Scott-Sheldon, Johnson, & Carey, 2008; Rooke, Thorsteinsson, Karpin, Copeland, & Allsop, 2010; Tait & Christensen, 2010; White et al., 2010). This review cannot make such a clear conclusion as most of the comparisons have low quality of evidence. This could be due to our population (i.e., youth at risk of alcohol abuse with no diagnosed substance use disorder), and the robust quality assessment of the studies using GRADE. Still the effect sizes found in our review are not very different from those found in other reviews. In addition, almost all effect sizes in our review are in favor of computerized interventions, when compared to control.
Strengths and Limitations
The current review applied a rigorous and transparent systematic approach of searching, screening, and quality assessing the studies according to predefined criteria with no time or language restrictions. The review is more thorough than previous reviews. We are confident that we found most of the randomized controlled studies relevant to the study objective.
Participants in most of the studies were U.S. university or college students in North America. Thus, the results cannot necessarily be applied to populations outside the United States, North American context or to youth who are not university or college students. While most of the studies used more current technologies, such as application software (i.e., “app”) for smartphones and tablet computers, a small number of earlier studies used older technologies such as CD-ROMs on a desktop computer. Using smartphones or tablets compared to stationary computers makes the intervention more mobile and accessible. Thus, the results cannot be generalized to digital platforms other than those examined.
A great number of the studies were considered high risk on at least one of the risk of bias domains, such as the participants were not adequately blinded, the assessors were not blinded, the attrition was high, unbalanced or unexplained, or selective reporting was suspected. We also downgraded most of the evidence due to imprecision (small sample sizes). Exceptions were three large studies by Kypri et al. (2009, 2013, 2014), which included more than 7,000 participants.
Implications
CBIs are fast and easy to administer, able to reach many people, are at low cost, and have no known adverse effects. The effects are, however, probably small to moderate, at least in this highly selective group of youth at risk of alcohol abuse. Practitioners who want to reach many people and have limited resources might consider administering such interventions. However, if it is of greater importance to use a more evidence-based method and more resources and clinical skills are available, practitioners might want to use interventions that have proven efficacy for risky substance use behaviors.
Based on the included studies in the current review, CBIs might reduce alcohol consumption with a small effect size, although it is difficult to be certain because of the overall low methodological standard. The research community should develop a list of standard outcome criteria, which can help compare results between studies.
Supplemental Material
Supplemental_Material - Effects of Computerized Interventions on Risky Alcohol Use Among Youth: Systematic Review
Supplemental_Material for Effects of Computerized Interventions on Risky Alcohol Use Among Youth: Systematic Review by Geir Smedslund, Wendy Nilsen, Sabine Wollscheid, Asbjørn Steiro, Lin Fang and Lillebeth Larun in Research on Social Work Practice
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.