
Abstract
This article reports a systematic review of the effectiveness of individual child play therapy with children aged 4–12 on several different presenting concerns. From over 5,000 citations, 180 studies were reviewed in detail and 17 met the inclusion criteria. A wide range of results on different concerns were revealed, with effect sizes ranging from d = –0.04 to g = 3.63, though most ranged from .35 to .80. Across most concerns, play therapy was affirmed as an empirically supported therapy.
Play therapy is a widely publicized and frequently employed form of therapy for children (Boyd Webb, 1996, 2019). This is because children may be developmentally unready or unable to express and explore their feelings, thoughts, and social behaviors in words as adults do. For children, play and activity serve as key means of communication about needs, fears, and anxieties. Play is also a means of self-expression, enjoyment, and self-actualization. Used in therapy, play provides a means for children to express what concerns them without requiring predominantly verbal expression of their thoughts and feelings (Axline, 1969; Boyd Webb, 1996, 2011, 2019; Cutler & Timberlake, 2000; Gil, 1991).
Play therapy is a structured, theoretically based, approach to therapy that builds on the normal communicative and learning processes of children (O’Connor & Schaefer, 1983). The U.S.-based Association for Play Therapy (2016, para. 7) defines play therapy as “the systematic use of a theoretical model to establish an interpersonal process wherein trained play therapists use the therapeutic powers of play to help clients prevent or resolve psychosocial difficulties and achieve optimal growth and development.” Play therapy is an important and growing approach to intervention for childhood disorders and difficulties (Getz, 2011; Mueller, 1994).
There are many different forms of play therapy. Play therapies are often categorized as either nondirective (Lebo, 1953) or directive (Leggett & Boswell, 2017) in approach, though some models employ both nondirective and direct components (Efron, 1981; Kenney-Noziska, Schaefer, & Homeyer, 2012). There are many named models of play therapy, including child-centered play therapy (CCPT), Theraplay, cognitive behavioral play therapy, sandtray, and others. For the purposes of this systematic review, play therapy is defined as an interpersonal process between a trained clinician and an individual child client used to prevent or resolve child (aged 4–12) mental health and behavioral difficulties. This definition excludes models that heavily involve parents, such as parent–child interaction therapy, models that may include play components, group models, and play models not delivered by a trained clinician. Notably, our definition also purposefully excludes a growing body of “child life” play interventions (Association of Child Life Professionals, 2017). Child life services include a range of play-based interventions to prepare and support children for medical procedures and services. However, our focus is on play therapy as used clinically to address mental health and behavioral concerns.
As early as the 1930s, social workers were involved in the development and delivery of play therapies (Allen, 1934; Taft, 1933). Aiello (1999), Boyd Webb (1996, 2019), Carroll (2000), Dripchak (2007), Levy (2008), McDonald et al. (1997), Timberlake and Cutler (2001), Swainson (1995) and other social workers have studied play therapies. Yet play therapy is not widely taught in social work programs despite calls from students working with children for more extensive education in it (Weil, 2012). Some programs do, however, offer dedicated courses on play therapy (i.e., University at Buffalo, NYU). Other programs include play therapy education in child and/or family practice courses (Gil, 2015). This raises the questions, “Is individual child play therapy effective?” and “Can play therapy be considered a research supported therapy?” This systematic review seeks to answer these two questions which may help guide social work practice, education, and research.
Review of the Literature: Prior Studies on Play Therapy
As early as 1953, Lebo questioned the lack of research documenting the effectiveness of play therapy. Phillips (1985) also challenged the effectiveness of play therapy, noting the small samples sizes utilized and the omission of control or comparison groups in published studies. Carroll (2000) argued that research assessing the effectiveness of play therapy is needed in social work. LeBlanc and Ritchie (2001) completed a meta-analysis of play therapy outcomes with children with a mean age of 7.8 years, reporting overall a 0.66 standard deviation (SD) improvement. LeBlanc and Ritchie also found that parent involvement was linked to better outcomes, as was longer duration play therapy with the child. Bratton, Ray, Rhine, and Jones (2005) completed another meta-analysis of play therapy outcomes. They included 93 studies with children of a mean age of 7 years, reporting overall 0.80 SD improvement. Bratton and colleagues further reported that humanistic and nondirective play therapies had better results (d = 0.93) than did behavioral approaches (d = 0.73) and that involvement of parents was linked to better outcomes. Further, they reported that “play therapy appeared equally effective across age, gender, and presenting issue” (p. 376). These early reviews found play therapy to be quite effective.
Later, Ray, Armstrong, Balkin, and Jayne (2015) published a review and meta-analysis of 23 CCPT studies provided in elementary schools. They report smaller but statistically significant effects, ranging from d = 0.34 for externalizing problems, 0.21 for internalizing problems, and 0.34 for total problems. Lin and Bratton (2015) completed another meta-analysis of 52 controlled studies completed from 1995 to 2010. They report an overall effect size of d = 0.47 for CCPT, as well as “statistically significant relationships between effect size and…child’s age, child’s ethnicity, caregiver involvement, treatment integrity, publication status, and presenting issue” (p. 45). CCPT appeared effective but with smaller effect sizes than had been previously reported. No 95% confidence intervals (CI) were reported. These publications, however, mixed several different models and modalities of play therapy.
From a methodological perspective, Bratton and Swan (2017) reviewed 26 studies including both individual and group CCPT, filial therapy, group sandtray therapy, and Adlerian play therapy. Experimental, quasi-experimental, and one group pre–post designs were included. Twelve studies included active treatment comparisons while 14 employed wait-list controls; with a mean of 42 participants per study. Manualized treatment approaches were few but appeared in some recent studies. Bratton and Swan argue that play therapy is an empirically supported treatment (EST) or research-supported treatment (RST), demonstrating effectiveness with diverse populations and in a variety of real-world settings. However, they did not perform a meta-analysis of the studies they summarized due to variation in outcomes studied nor did they provide 95% CI for their effect size results. While play therapy studies have improved in methodological quality, issues including research design, attribution bias, validity of measures, full reporting of statistics, and definitions of the treatments may warrant further examination.
The Cochrane Collaboration has established international standards for systematic reviews of treatment outcomes Higgins and Green (2011). A Cochrane Collaboration search revealed no reviews on play therapy. However, it was noted in Gillies and colleagues (2016) systematic review that, for reduction of [childhood] PTSD symptoms in the short term, there was a small effect favoring cognitive behavioral therapy (CBT) over eye movement desensitization and reprocessing (EMDR), play therapy, and supportive therapies (SMD = 0.24, 95% CI [0.42, −0.05]; 7 studies; 466 participants). The quality of evidence for this outcome was rated as moderate. (Main Results)
A systematic review of the effectiveness of play therapy appears warranted based on the varied results and limitations of prior work. This study seeks to examine the effectiveness of individual play therapy. “Is individual child play therapy effective for child mental health and behavior concerns?” and “Can play therapy be considered a research supported therapy?”
Method
This systematic review (SR) was guided by Cochrane Handbook 5.1 standards (Higgins & Green, 2011) as possible. Meta-analytic aggregation of results was not undertaken as our purpose was to examine the effectiveness of play therapy as a treatment for many childhood concerns, not just one single concern or disorder as done in Cochrane reviews. We included 17 experimental studies. A team of four clinical social workers completed this SR. None of the team were authors of included publications. The team searched for the terms “play therapy,” “play psychotherapy,” and “experiment*,” “RCT*,” “child*,” “effectiveness,” “outcomes,” and “efficacy”—both separately and in combination using Boolean AND and OR operators. Between 1980 and 2018, the PubMed data base yielded 2,257 citations, PsycInfo yielded 2,209 citations, CINAHL Plus yielded 914 citations, and Social Work Abstracts yielded 105 citations. From these 5,485 publications, we reviewed abstracts to determine whether publications met the SR criteria or were irrelevant or duplicate publications. In addition, a “pearl growing” technique was applied to identify additional literature using citations from relevant articles and books of play therapy from the past 10 years, yielding three more publications for inclusion. In the end, 96 publications were reviewed by at least two team members, along with 14 recent books on play therapy. A total of 17 publications proved relevant and met quality and inclusion standards. A Quorum chart summarizes the search results (see Figure 1).

Quorum chart for the play therapy systematic review.
Inclusion criteria for this SR were the following: (1) Individual outpatient play therapy for children, though caregiving adults may have been involved conjointly as well (but not family or group therapy); (2) children between the ages of 4 and 12 years, with no intellectual impairment; (3) the primary treatment goals were clearly identified in the publication; (4) the play therapy model was clearly identified, though a treatment manual was not required; (5) a detailed description of the sample (size, ages, and ideally ethnicities) was provided; (6) outcome measures were clearly identified; (7) outcome evaluations were sought including; (8) stated means and SDs for both pre- and posttreatment measures; and (9) published in English language between 1990 and 2018. Finally, (10) only experimental designs with a control group were sought following Cochrane standards.
Effect sizes were calculated based on reported pretest and posttest results using Ellis’s (2009) online calculator. This calculator uses an unbiased estimator of combined SDs. The Cohen’s d statistic was used where both treated or control groups included 25 or more participants; Hedges’s g was used where groups included 24 or fewer participants. This was done to avoid inflated results (Hedges & Olkin, 1985). In practice, the calculated differences between d and g values were very small. The 95% CI for the effect sizes were calculated using Hedges’ formula (Hedges & Olkin, 1985). Because the play therapy models and samples differed, and addressed different concerns, results are reported for each publication and are not statistically aggregated.
There was risk of bias within these studies. While random assignment appeared well-documented (low risk), few studies used any form of blinding (medium risk). Attrition rates were low overall (low risk). However, the outcome measures used varied widely. While most studies stated that the measures had “good” psychometric properties they were normed on small samples and often with little diversity. Attribution bias was potentially a high risk as study authors were often providers and/or creators of the tested therapies. Among the included studies, CCPT was the most frequently employed model. However, there was little discussion in these studies regarding treatment fidelity (medium risk). Duration and frequency of the delivered therapy also varied widely, even within the CCPT model.
As noted, we have chosen not to perform an aggregative analysis of these findings as our goal was to assess the efficacy of play therapy on several very different disorders. This would make aggregation misleading. In this way, the present study intentionally differs from Cochrane systematic review standards and Forest plots which include such aggregation for a single target disorder or outcome.
Overall, individual play therapy had effect sizes ranged from a low of d = –0.04 to a high of g = 3.63, though most ranged from .35 to .80 (see Table 1). In summary, play therapy effect sizes ranged from d = 0.22 to 2.27 for aggression, 0.33 to 1.94 for attention or ADHD symptoms, .18 to 2.73 for anxiety, and 0.26 to 0.98 for externalizing behaviors. Cohen (1988) states that effect sizes of 0.20 are small, 0.50 medium, and 0.80 or greater are large effect sizes. Cohen also states that effect sizes can also be interpreted as the extent of nonoverlap (difference) between the distributions of pre- and postscores. That is, if there is no difference in pre- to postscores an effect size of .00 results. An effect size of 0.5 indicates a nonoverlap of 33% in the two distributions of scores; an effect size of 0.8 indicates a nonoverlap of 47.4% in the two distributions. An effect size of 1.7 indicates a nonoverlap of 75.4% in the two distributions (Cohen, 1988). In general, small effect sizes are not statistically significant, while medium to large effect sizes are linked to statistically significant results. Overall, play therapy effect sizes below a value of .30 were few but present. On the other hand, several extremely large effect sizes (over 1.00) were also reported.
Summary of Studies Included in This Review, Effect Sizes, and 95% Confidence Intervals.

Note. ACAT = Ahwaz Children’s Anxiety Test; ADDES = Attention Deficit Disorder Evaluation Scales; ADHD = attention deficit hyperactivity disorder; ADPT = adlerian play therapy; BASC = Behavioral Assessment System for Children; BASC-C/P Parent = behavioral assessment system for children, child-parent rating scale; CBADS = Child’s Beliefs About Divorce Scale; CBCL = Child Behavior Checklist; CCPT = child centered play therapy; CDI = children’s depression inventory; CSEI = Coopersmith Self-Esteem Inventory; CTRS = Conners’s Teacher Rating Scale, revised; DOF = direct observation form; IRS = Impairment Rating Scale; PT = Play Therapy; PTSD = post-traumatic stress disorder; PROPS = parent report of post-traumatic stress symptoms; RCMAS = Revised Children’s Manifest Anxiety Scale; RCT = experimental research design; SCBE = Social Competence and Behavior Evaluation Scale; STAI = State-Trait Anxiety Scale; TBA = total brief achievement; TRF = teacher report form; VSMS = vineland social maturity scale; YCAT = Young Child’s Achievement Test; WJIII = Woodcock–Johnson Total Brief Achievement Scale.
a95% confidence interval crosses the zero line (no difference in the population).
Most of the 95% CI calculated on these 17 studies based solely on pretest to posttest results did not include a 0.00 value (45 of 57). CIs that do not include a zero value indicate a statistically significant results at the p < .05 level. However, 12 of 57 comparisons, including all 6 of Ritzi, Ray, and Schumann’s (2017) results, did include (or crossed) the zero value in the 95% CI calculated here. These 95% CI results indicate a different, nonsignificant, result in contrast to some of the initially published results for these 12 studies.
Complied descriptively by problem type, results included in this review show considerable variation (see Table 2). Both small (.20 to .40) and extremely large effect sizes (>1.0) were found. In several instances, a single study might report two different results based on the perspective of the rater: parents and teachers often differed in their ratings. For aggression, attention issue or ADHD symptoms, anxiety, and externalizing behaviors at least half of the results demonstrated effect sizes of .50 or larger–medium to large effect sizes. A few effect sizes were extremely large. Variation in results was notable.
Effect Sizes and Study Numbers for Select Child Concerns.
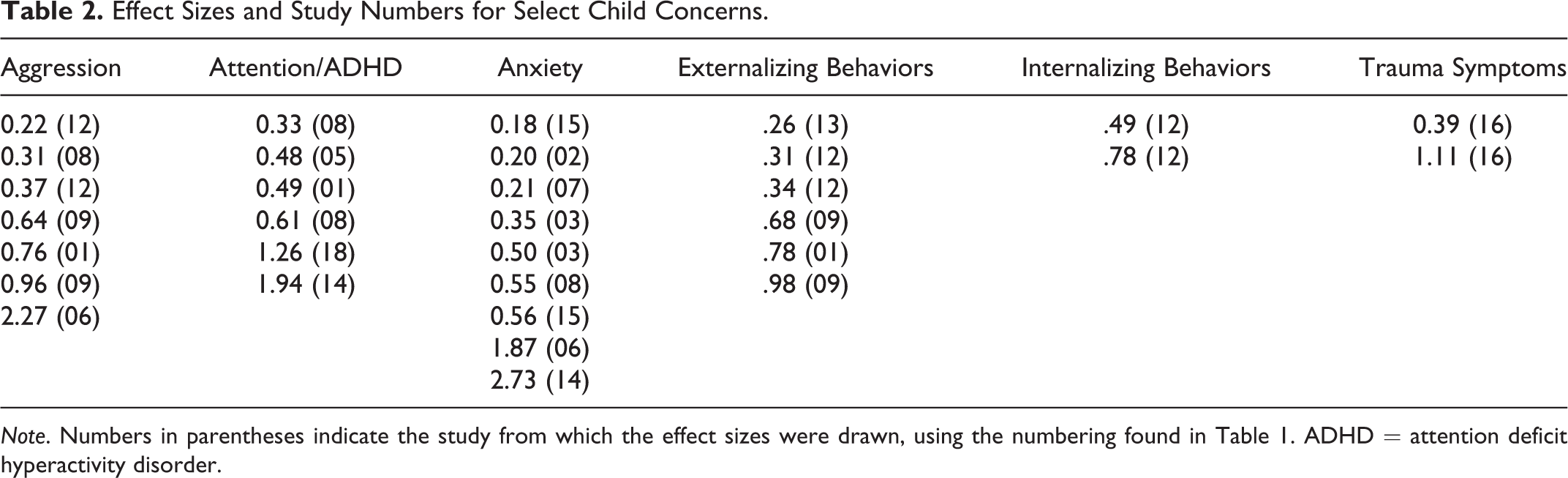
Note. Numbers in parentheses indicate the study from which the effect sizes were drawn, using the numbering found in Table 1. ADHD = attention deficit hyperactivity disorder.
Discussion
Overall, individual child play therapy is often effective as documented by this systematic review. As always, not all treatments will prove beneficial for all clients, settings, and needs. Differences in outcomes across settings, providers, and models of play therapy were found in this review. Nonetheless, individual child play therapy appears to meet criteria as an EST or RST. That is, there are two or more studies, at least one completed by researchers who were not the creators of the treatment model, using appropriate methods and measures, demonstrating play therapy’s effectiveness. A few of these models had treatment manuals, though play therapy is purposefully highly individualized. Most studies cited specific authors and play therapy models as guides for their interventions.
A wide range of concerns, and a wide range of measures, were used to assess the effectiveness of play therapy. Many concerns centred on classroom behaviors and readiness for classroom learning, though with likely broader life impact. Teacher and parent ratings predominated. Almost all of the standardized outcome measures were reported to have reasonable psychometric properties in the original publications, though a few were researcher-created. Some measures, such as the Child Behavior Checklist (Achenbach, 1999), may lack sensitivity to detecting small changes made over a few days or weeks. While costly, use of both symptom specific and more wide-ranging omnibus measures on many symptoms would be useful in future research. This would allow determination of change on target concerns as well as assessment of unintended effects of treatment (Ogles, Lambert, & Masters, 1996). Development of a consensus set of outcome measures would also be useful to guide future research on play therapy.
The duration of each play therapy session, their frequency (weekly, twice weekly, biweekly, etc.), and the overall duration of the treatment varied considerably among these studies. Authors often noted this was function of funding or fitting into school schedules. The question of whether or not the pacing and length of play therapy interventions has differential impact on outcomes is not clear and warrants further research. Further research is also needed to determine whether the pacing and duration of play therapy leads to lasting change: Very few publications included any follow-up measures of effectiveness. Play therapy is effective at its ending but if, and how long, its beneficial impact endures has not been well examined. This should be a future focus of research.
Some play therapy models specifically addressed symptoms such as sexualized behaviors, attention deficits, or anxiety. How to include emphasis on these and similar concerns into an intentionally flexible treatment model warrants further conceptualization and research. More work to blend play therapy with psychoeducation and to focus on specific concerns is also indicated.
Several studies included racially/ethnically varied samples. Many studies were done in Texas and included Hispanic, African American, European American, and bi- or multiracial participants. Future research should continue to incorporate such diversity, with greater attention to Native American and Asian populations as well. Most studies included both boys and girls. Attention to nonbinary genders should also be part of future play therapy research. Overall, samples were small: Larger and more diverse samples should be included in future research.
Currently, the overall quality of outcome research on play therapy may be characterized as low to moderate. Future research should include more true RCTs, greater detail of the play therapy provided including attention to treatment fidelity, use of standardized measures with strong psychometric properties, and larger and more socially diverse samples. CI should be reported for all statistics but were absent from the publications included in this review. Power analyses should also be completed and reported. Outcome studies should be completed by persons who are not creators of the models under study to avoid potential attribution bias. Finally, funding sources should be fully documented in future play therapy outcome studies.
Play therapy continues to warrant a place in clinical practice for a range of childhood concerns. This and prior work demonstrate that play therapy meets American Psychological Association criteria as an EST. It fits very well with children’s styles of communication and growth. Still, additional research is needed to refine these results. Play therapy also merits continued, and expanded, inclusion in the social work curriculum and that of allied professions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.