
Abstract
Purpose:
This study investigated process and outcomes of the Parenting for Lifelong Health (PLH) for Young Children and for Adolescents programs implemented as part of routine service delivery in postconflict settings.
Methods:
These group-based programs were delivered by trained facilitators to 97 caregivers (PLH for Young Children) and 108 caregiver–adolescent dyads (PLH for Adolescents) over 12 or 14 (respectively) weekly sessions. Routine monitoring data were collected by the implementing partners using standardized self-report measures. Reducing harsh discipline was specified as the primary outcome, with secondary outcomes including improvements in positive parenting and reductions in poor parental supervision and parental inefficacy.
Results:
Analyses were intention to treat. Both PLH programs retained effectiveness in routine conditions in a postwar setting, with moderate to large effect sizes. The programs also had high enrollment and attendance rates, indicating high acceptability.
Conclusions:
Findings suggest promising viability for the implementation of evidence-based parenting programs in challenging postconflict contexts.
Keywords
Worldwide, over one billion children experience violence each year (Hillis et al., 2016). However, children in low- and middle-income countries (LMICs) experience a disproportionate burden of violence and abuse (Hillis et al., 2016), with rates presumed to be even higher in conflict-affected settings (Stark & Landis, 2016). The impacts of violence against children—defined as the physical, psychological, and sexual abuse of children (World Health Organization [WHO], 1999)—on physical and mental health and social functioning are severe and long lasting, with significant economic and social costs (Fang et al., 2017; Knox et al., 2011; Peterson et al., 2018). These consequences for health, social development, and the economy call for the urgent implementation of prevention strategies. As part of the 2030 Sustainable Development Goals, the WHO and partners’ INSPIRE: Seven Strategies for Ending Violence Against Children recognizes parenting programs as a key strategy for preventing violence against children (WHO, 2016).
Nurturing and responsive care from parents and caregivers serves as an essential protective resource in promoting children’s resilience and is especially important in contexts of crisis (Betancourt & Khan, 2008; Tol et al., 2013). In settings affected by armed conflict, as in other challenging contexts of chronic poverty and stress, caregivers’ abilities to provide these critical resources can be affected by a range of factors, including the breakdown of extended support systems (Betancourt et al., 2013), forced displacement and/or separation from primary caregivers (Stark & Landis, 2016), and decreased access to basic needs such as food, shelter, and education (Hart, 2015). As a result, children exposed to armed conflict and political violence may also experience heightened rates of violence and abuse within the home and community (Rubenstein, Lu, MacFarlane, & Stark, 2017). Parenting programs that enhance caregiver–child relationships through positive parenting and provide age-appropriate, nonviolent discipline strategies offer a promising approach to preventing violence against children (Barlow et al., 2006; Chen & Chan, 2016).
Given the higher risk of violence against children in LMICs, the need for parenting interventions may be greatest here. Nevertheless, most parenting programs have been developed and tested in stable high-income countries (HICs; Chen & Chan, 2016; Knerr et al., 2013). These interventions are typically delivered on a small scale and administered under tightly controlled conditions for the purposes of a study; often programs are not widely disseminated after study completion (Gottfredson et al., 2015). Although the evidence is growing, only few parenting programs have been tested in LMICs (Knerr et al., 2013; Mejia et al., 2012) and even fewer have been tested in conflict-affected settings (Jordans et al., 2016). Thus, despite parenting programs’ established effectiveness in reducing violence against children (Barlow et al., 2006; Chen & Chan, 2016; Furlong et al., 2012), questions remain about how to implement them after trial, especially under conditions of routine service delivery in humanitarian contexts.
The few parenting programs in HICs that have been run at scale or as part of routine service delivery show varying results (Forgatch & DeGarmo, 2011; Hutchings et al., 2007; Little et al., 2012; Malti et al., 2011), demonstrating that despite the high-quality service settings, training, and technical assistance typically available, many barriers to successful implementation still exist. It may, therefore, be even harder to adopt, implement, or sustain such interventions if local capacity is absent (Gottfredson et al., 2015).
Obstacles to implementing parenting programs in LMICs, and particularly those affected by conflict, include weak and unstable service delivery systems into which to integrate interventions, limited funding to maintain services, and lack of human resources to deliver services (Knerr et al., 2013; Mejia et al., 2012). Another challenge facing the successful implementation of parenting programs is their transferability. Programs developed and tested in one context may need to be adapted for provision by a range of different service delivery systems and settings when disseminated elsewhere (Kumpfer et al., 2012; Richter et al., 2017). While a review of evidence-based parenting programs found promise of transportability, only one study identified was from a LMIC (Gardner et al., 2016). Promisingly, the International Rescue Committee has successfully replicated adapted versions of a parenting program among displaced Burmese families in Thailand (Annan et al., 2017; Sim, Annan et al., 2014) as well as in postconflict Liberia (Puffer et al., 2015; Sim, Puffer, et al., 2014), suggesting the feasibility of transferability from one humanitarian context to another. Nonetheless, further research is needed to inform whether programs developed in relatively low-conflict settings such as South Africa are transferable to a high-conflict, post-war setting such as South Sudan.
South Sudan has experienced decades of recurrent humanitarian crises that have escalated since 2013. Approximately 2.6 million people in South Sudan have fled their homes since the conflict began, with more than 50% estimated to be children (WHO, 2018b). This crisis has had devastating effects on the economy, food security, child survival, and access to health services (WHO, 2018b), increasing risks of violence against children both in the home and community (Rubenstein et al., 2017). In line with the South Sudan National Health Policy, Catholic Relief Services received funding to deliver the Parenting for Lifelong Health (PLH) programs for Young Children and for Adolescents to address violence against children in the home and the community.
The PLH Programs
PLH is a collaborative research initiative that was formed to address the need for culturally relevant, affordable, and effective parenting programs in LMICs (Ward et al., 2014). It involves the development, testing, and large-scale dissemination of a suite of low-cost, evidence-informed parenting programs, covering the age range from 0–18 years. The programs are designed for resource-poor contexts, require little or no equipment, and are typically implemented by community workers.
PLH for Young Children is a 12-session group-based intervention for caregivers of children aged 2–9 (Ward et al., 2020). PLH for Adolescents is delivered as a 14-session group-based intervention for caregivers and their 10- to 18-year-olds (Cluver et al., 2018). For both programs, sessions last approximately 2–3 hr. The programs are based on social learning theory (Bandura, 1977) and focus on reducing harsh discipline practices, increasing positive caregiver–child relationships, developing socioemotional regulation, and learning authoritative limit setting. Additional focus in the PLH for Adolescent program is on shared family budgeting and protecting adolescents from violence outside the home. Table 1 shows the content and structure of each program.
Overview of Program Content and Structure.
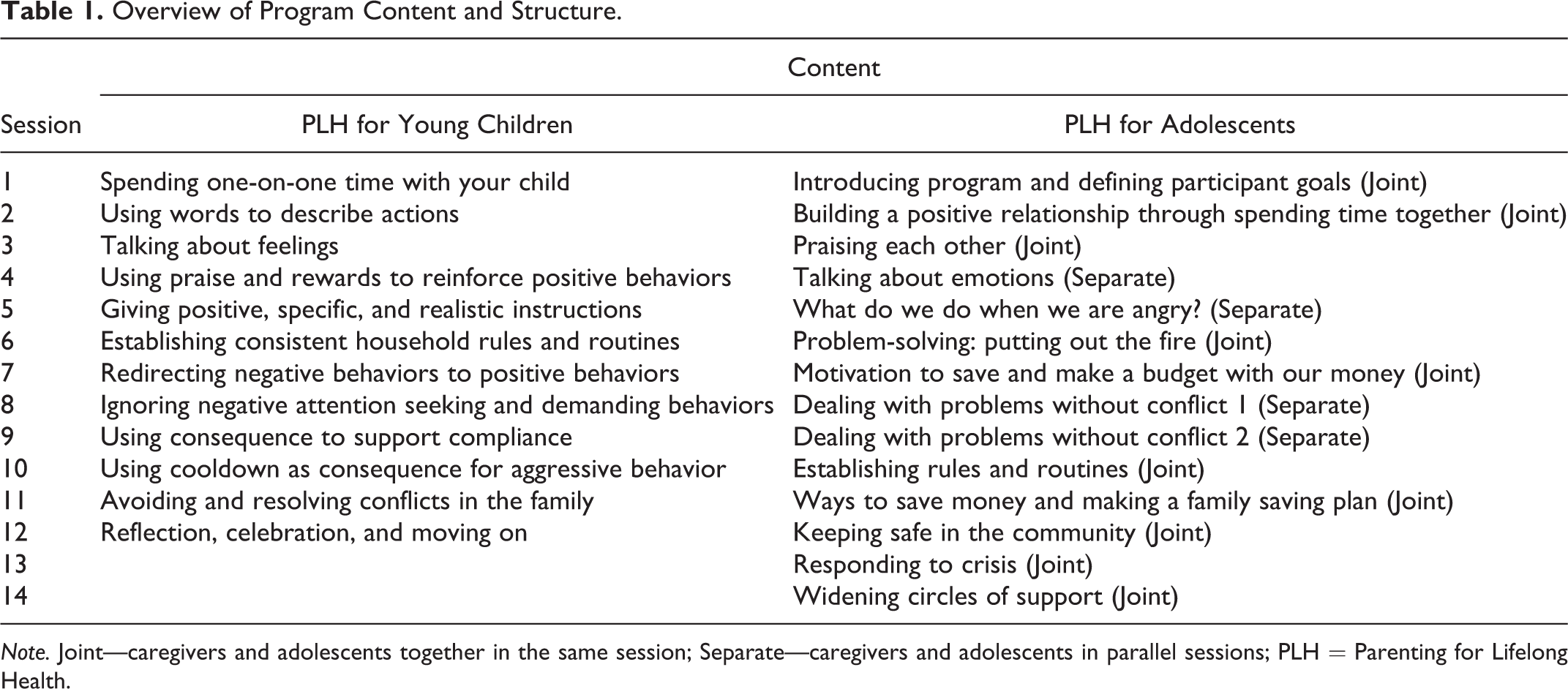
Note. Joint—caregivers and adolescents together in the same session; Separate—caregivers and adolescents in parallel sessions; PLH = Parenting for Lifelong Health.
PLH for Young Children and PLH for Adolescents provide some of the most promising evidence of parenting program effectiveness in LMICs (Cluver et al., 2018; Cluver et al., 2016; Lachman et al., 2017; Lachman et al., 2018a; Ward et al., 2020). One of the first countries implementing these programs as part of routine service delivery is South Sudan. Coordinating Comprehensive Care for Children, or 4Children, is a 5-year United States President’s Emergency Plan for AIDS Relief–funded project led by Catholic Relief Services. The project selected both PLH programs to be part of a suite of services offered to households of orphans and vulnerable children in Juba, South Sudan. In addition to parenting support, these services included case management and referrals for health services and household economic strengthening. Minor adaptations were made to the PLH for Adolescents program, to include more emphasis on fathers, as 4Children specifically aimed to target male caregivers. The programs were also renamed “Beit Salaam” or “House of Peace” by local implementers to reflect the aim to model peace-building behaviors for future generations at the family level. The adaptation process was supported by Clowns Without Borders South Africa, a nongovernmental organization that supports the dissemination and capacity building of the PLH programs.
Research Aims
The aims of this study were to use routine monitoring and evaluation data to investigate the process and intervention outcomes of both PLH programs implemented in a postconflict setting in South Sudan to inform the feasibility of transporting the programs from low-conflict- to high-conflict-affect settings. Reducing harsh discipline was specified as the primary outcome, with secondary outcomes including improvements in positive parenting and reductions in poor parental supervision and parental inefficacy. The following research questions were examined: Do caregivers and adolescents who participate in the PLH programs report reduced harsh discipline and improved positive behaviors? How is program attendance associated with primary and secondary outcomes? Which demographic characteristics are associated with higher or lower program attendance?
Methods
Participants
Families were screened into 4Children’s orphans and vulnerable children program using the Household Vulnerability Prioritization Tool, developed by the Palladium Group for Catholic Relief Services in Uganda and adapted for use in South Sudan for identifying families in need of services. This tool asks families to report on child abuse issues in the home (repeated physical abuse; child labor; neglect; early marriage, pregnancy, or parenthood; and sexual abuse) and high vulnerability indicators (child-headed households, no food in a day in the last 30 days, a member of household who is HIV positive, and a child not enrolled at school) to determine which households are in need of an intervention in economic strengthening; food security and nutrition; health, water, sanitation, and shelter; education; psychosocial support and basic care; and child protection. Families in need of child protection and psychosocial support and basic care qualified to participate in the PLH programs.
4Children recruited participants for the PLH programs from six sites within Juba, South Sudan. The majority (75%) of recruitment was done at health-care facilities through clinic staff, while the rest (25%) was done within communities by community workers. Ninety-seven caregivers were recruited for PLH for Young Children, and 107 caregivers and 108 adolescents were recruited for PLH for Adolescents. Prior to the first session, facilitators conducted a preprogram home visit with each family to introduce the program. Parents were asked to identify one child between the ages of 2–9 and 10–18 (depending on which program they were recruited for) with whom to practice what they learnt during the program.
Given that this study had no control over sample size, post hoc sensitivity power analyses were conducted using G*Power, version 3.1.92 (Faul et al., 2007) for multiple linear regression. The recommended effect sizes used were as follows: small ( f 2 = .02), medium ( f 2 = .15), and large ( f 2 = .35; Cohen, 1988). With a five-predictor variable equation and an alpha level of p < .05, an effect size of f 2 = .14 was detectable at 80% power for a sample of 97 and an effect size f 2 = .13 was detectable for a sample of 108. Thus, there was adequate power to detect small to large effect sizes.
Ethical Procedures
The study protocol was approved by the ethics review boards of the South Sudan Ministry of Health (MOH/ERB5/2018) and at the Universities of Cape Town (PSY2017-040) and Oxford (R48876/RE002). Informed consent procedures were conducted by the implementing partners. Catholic Relief Services South Sudan anonymized the data by removing any identifying information, including names, contact details, birth dates, and any additional unique characteristics that may enable identification. Anonymized data were then shared with the research team for analysis.
Training, Delivery, and Data Collection
Clowns Without Borders South Africa provided training in program delivery to community volunteers and supervisors employed by 4Children, as well as clinic community volunteers and social workers from the Ministry of Gender, Child, and Social Welfare and from six health facilities including Juba Teaching Hospital, Juba Military Referral Hospital, Al-Sabah Children Hospital, Kator, Munuki, and Nyakuron Primary Healthcare Centers. Thirty-three facilitators were trained in PLH for Young Children in October 2016 (4 days, totaling 24 hr). In August 2017, an additional 32 facilitators were trained in PLH for Adolescents. Clowns Without Borders South Africa also trained 13 supervisors (1 day, 6 hr) who provided weekly supportive supervision via Skype throughout implementation. All facilitators underwent a certification process that provided assurance of quality of delivery.
Delivery ran from March to July 2017 for PLH for Young Children and from November 2017 to May 2018 for PLH for Adolescents. Group sessions were conducted on a weekly basis in various community facilities including churches, schools, and community health centers. If participants were unable to attend group sessions, facilitators conducted individual family consultations at participants’ homes after the group session. Home visit consultations covered the same material in an individualized format as the group session. The programs concluded with a community celebration and certificate ceremony. Some participants received incentives based on individual and household needs as suggested by the Household Vulnerability Prioritization Tool. These included the provision of school materials and tuition for school-age children throughout program delivery, short-term food support in 2017, and transport refunds in 2018.
To strengthen local capacity, and in line with routine monitoring of services, data collection was integrated into the community partners’ monitoring and evaluation systems instead of employing independent data assessors. As such, facilitators collected data on participant enrollment and attendance, as well as the baseline and postassessment data. Questionnaires were not translated into local languages as the official language in South Sudan is English. However, facilitators were bilingual both in Juba Arabic (the dominant language spoken in Juba) and English and were thus able to administer the questionnaires by translating them in the moment during data collection where participants needed translation. While this may have introduced bias into the data, it is the most feasible approach for community-based organizations delivering services.
Measures
Process outcomes
Enrollment
Catholic Relief Services collected data on beneficiary enrollment and attendance via registers completed by the facilitators. Enrollment referred to whether participants attended at least one group session out of the total number of sessions (either 12 or 14 depending on the program; Baker et al., 2011). Participants who missed all the group sessions but received home visit consultations were considered nonenrollees, given that facilitators, rather than participants, initiated home visits.
Attendance
Attendance referred to the percentage of total sessions attended once enrolled (Baker et al., 2011; Chacko et al., 2016). If the full session content was delivered via a home visit, participants were considered as having attended that session (Lachman et al., 2018a).
Demographics
Family demographic variables included caregiver gender and child gender and child age at baseline.
Primary outcomes
For both PLH programs, harsh parenting was measured using 8 items from the International Society for the Prevention of Child Abuse and Neglect Child Abuse Screening Tool for Trials (ICAST-Trial; Meinck et al., 2018). This tool requires caregivers and adolescents to indicate the frequency of different forms of abuse over the past month (0 = never, 8 = 8 or more times). Items are summed, with higher scores indicating greater frequency of harsh discipline, as well as subscales for physical and emotional abuse. The ICAST-Trial has good internal consistency (α = .77–.88) and has successfully been used in other studies of PLH programs in South Africa, Tanzania, the Philippines, and Southeastern Europe (Frantz et al., 2018; Lachman et al., 2018b; Lachman et al., forthcoming; Ward et al., 2020).
Secondary outcomes
For the PLH for Young Children program, positive parenting was measured using the Supporting Positive Behavior and Setting Limits subscales from the Parenting Young Children scale (7 items each; McEachern et al., 2012). Caregivers respond to items on a 7-point Likert-type scale (1 = never; 7 = always). Items sum to generate a total frequency score and total scores for each subscale—higher scores indicate greater use of positive parenting practices. The subscales were found in the original validation study to have high construct validity (α = .78, .79, respectively), high convergent validity with other similar tests (McEachern et al., 2012), and have successfully been used in South Africa and the Philippines (Alampay et al., 2018; Ward et al., 2020).
The Positive Parenting (6 items) and Poor Monitoring and Supervision (10 items) subscales of the Alabama Parenting Questionnaire (APQ; Essau et al., 2006) were included to assess positive parenting in the PLH for Adolescent program. The APQ measures the rate of specific behaviors toward children in the past month on a 5-point Likert-type scale (1 = never; 5 = always). Items sum to create a frequency score—higher scores indicate greater regular use of positive parenting. The APQ has good reliability (α > .70; Essau et al., 2006) and has successfully been validated in low-resource community settings in Australia (Elgar et al., 2007).
To capture parental inefficacy, two additional items from the ICAST-Trial (Meinck et al., 2018), which do not pertain to abuse but rather to sense of inefficacy, were included in the PLH for Adolescent questionnaire. These items have successfully been used in South Africa and the Philippines (Cluver et al., 2018; Lachman et al., 2018b).
Data Analysis
Analyses were conducted in SPSS Version 25 (IBM Corporation, 2017) and R Version 3.5.1 (R Core Team, 2018). Internal consistency of each measure was assessed using coefficients such as Cronbach’s alpha, omega, and greatest lower bound along with bootstrapping to obtain 95% confidence intervals (CIs; Revelle & Zinbarg, 2009). Principal component analyses were conducted for scales demonstrating poor reliability (Peters, 2014). Where principal component analyses indicated divergence of unidimensionality, the scale was split into subscales and the internal consistency was calculated for each subscale (Dunn et al., 2014).
The assumption that data were missing at random was confirmed using Little’s Missing Completely at Random Test (Little, 1988). Multiple imputation of missing data was performed using multivariate imputation by chained equations (MICE) via the mice package in R (van Buuren & Groothuis-Oudshoorn, 2011). Missing data were imputed at item level using predictive mean matching. Convergence was confirmed visually by plotting the chains (five chains, five iterations).
Multivariate linear mixed models were employed, accounting for random effects such as nesting within parenting groups (Finch et al., 2014), to estimate the effectiveness of the intervention in an intention-to-treat analysis. Time, attendance, caregiver gender, and child age and gender were treated as fixed factors. Random effects included individual participants and parenting groups, which provided a more accurate estimation of variance explained by the model (Finch et al., 2014). The models were fitted using the R package lme4 (Bates et al., 2015). Standardized beta coefficients and 95% CIs were obtained via the sjPlot package in R (Lüdecke, 2019). Observed p values were examined as a means of assessing strength of association rather than using it to determine statistical significance. Effect sizes and 95% CIs for each outcome were described by Cohen’s f 2, where f 2 ≥ 0.02, f 2 ≥ 0.15, and f 2 ≥ 0.35 represent small, medium, and large effect sizes, respectively (Cohen, 1988).
Results
Internal Consistency
Tables 2 and 3 present the results of the reliability measures for each program. All of the scales for PLH for Young Children had one or more reliability measure .70 or greater (Peters, 2014). All but two of the scales for PLH for Adolescents had acceptable reliability with one or more reliability measure .70 or greater (Peters, 2014). The ICAST Physical Abuse subscale for adolescents and the ICAST Emotional Abuse subscale for caregivers both had reliability below .70 at baseline and postassessment. Principal component analyses indicated that one component was underlying adolescents’ (ICAST Physical Abuse) and caregivers’ (ICAST Emotional Abuse) responses. Since these scales showed reliability approaching .70, unidimensionality, and only had few items (Cortina, 1993), they were retained for the outcome analyses.
PLH for Young Children: Reliability Analyses of Imputed Data at Baseline and Postassessment.
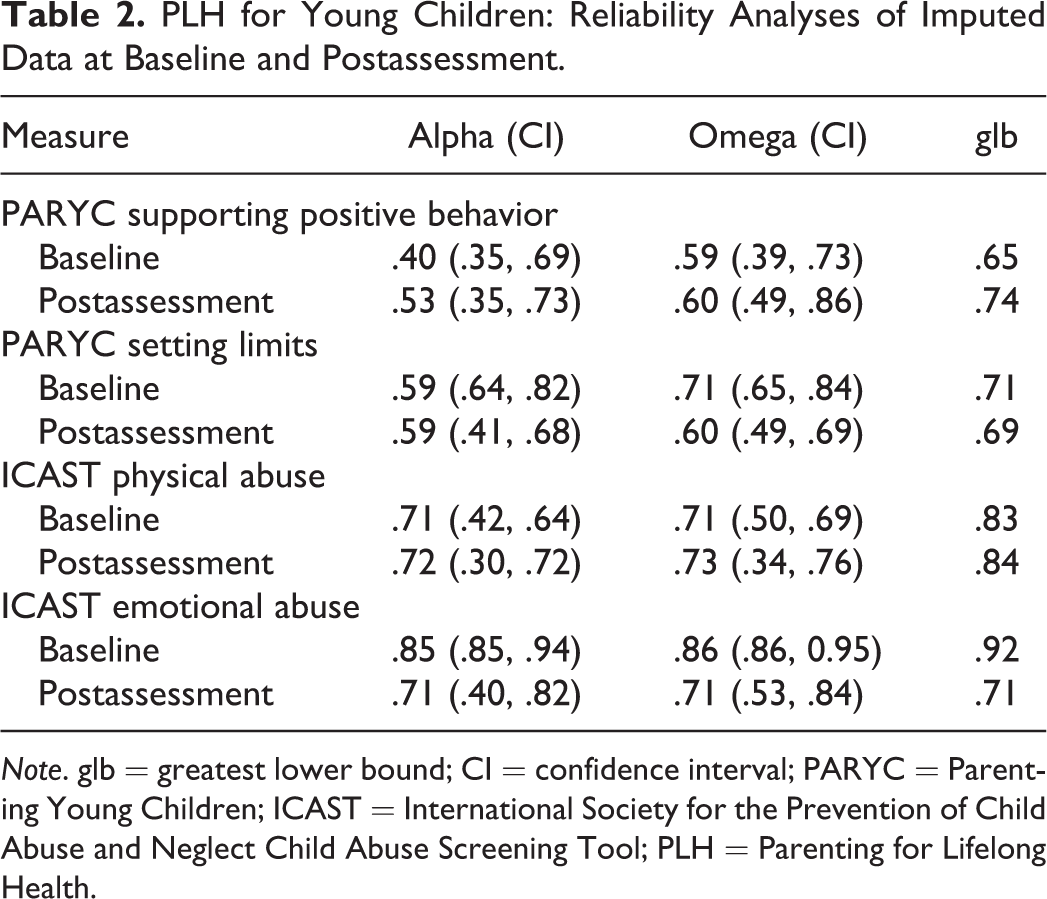
Note. glb = greatest lower bound; CI = confidence interval; PARYC = Parenting Young Children; ICAST = International Society for the Prevention of Child Abuse and Neglect Child Abuse Screening Tool; PLH = Parenting for Lifelong Health.
PLH for Adolescents: Reliability Analyses of Imputed Data at Baseline and Postassessment.
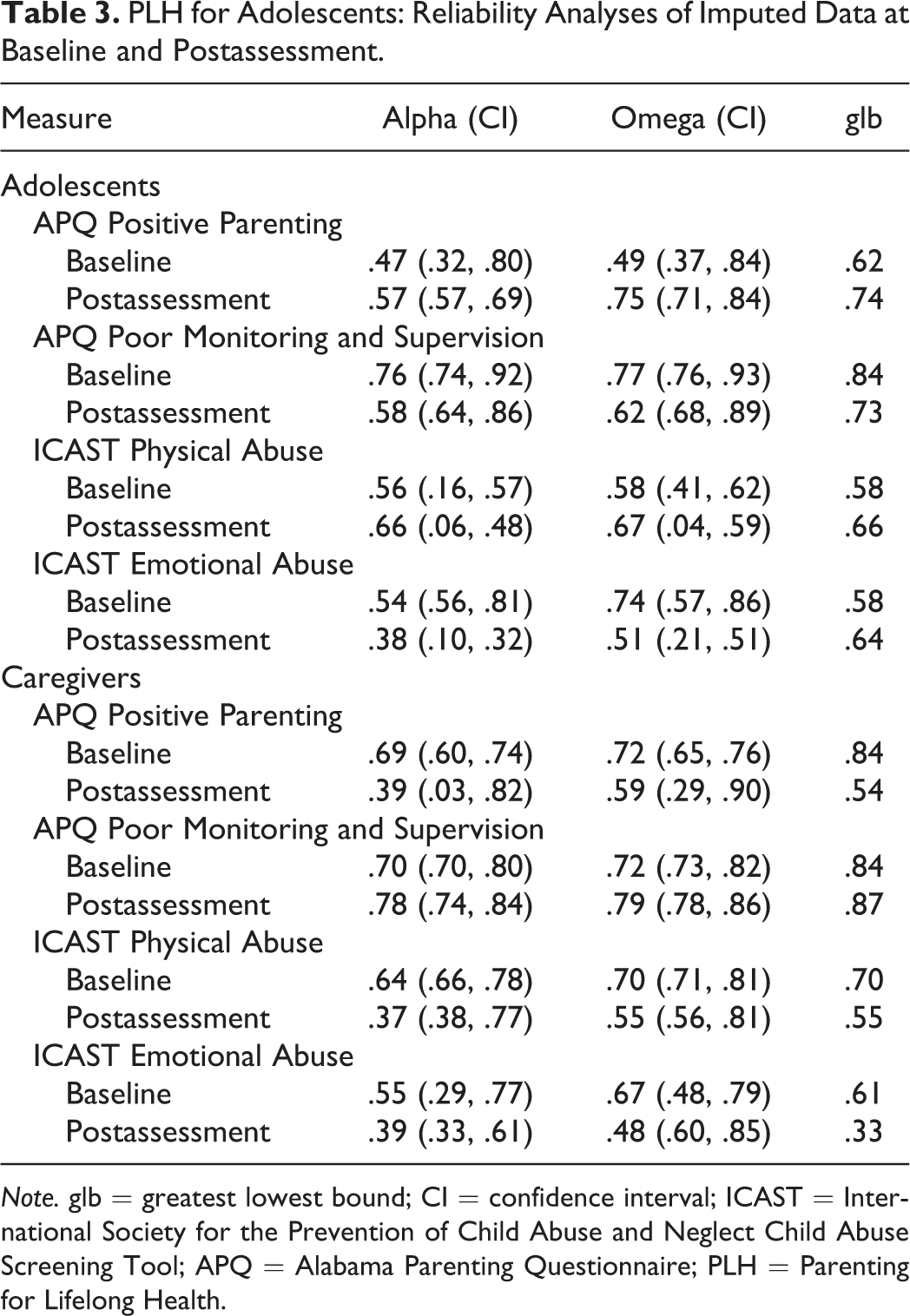
Note. glb = greatest lowest bound; CI = confidence interval; ICAST = International Society for the Prevention of Child Abuse and Neglect Child Abuse Screening Tool; APQ = Alabama Parenting Questionnaire; PLH = Parenting for Lifelong Health.
Sample Characteristics
PLH for young children
Seventy-four female and 24 male (23.7%) caregivers completed the baseline assessment. While the program was intended to be delivered to caregivers with children between the ages of 2 and 9 years, facilitators recruited some participants with children above 9 years (n = 4; ranging from 10 to 14 years). The mean age for all of the children was 7.10 years (n = 73, SD = 2.15). Just over half (n = 51, 52.6%) of the children were male.
PLH for adolescents
Fifty-nine female (55.1%) and 48 (44.4%) male adolescents and 81 (75.7%) female and 26 (24.3%) male caregivers completed the baseline assessment. Adolescents’ ages ranged from 10 to 17 years, with a mean age of 14.45 years (n = 105, SD = 2.10).
Program Participation
PLH for young children
Of the 97 caregivers who were recruited for the program, 96 (99%) attended at least one group session and 94 (97%) attended at least half (six group sessions or home visits) of the program. No caregivers were lost at the postintervention assessment; thus, all 97 participants were included in an intent-to-treat analysis. The average overall attendance rate was 10.71 (SD = 2.13) of 12 sessions, or 89.25% of the program. Analyses found differences in attendance patterns between female and male caregivers (standardized [std.] β = 28, 95% CI [.15, .41], p < .001), where female caregivers were more likely to attend the program. Caregivers with older children were also more likely to attend (std. β = 0.15, 95% CI [.02, .28], p = .025). Child gender was not related to caregiver attendance. Higher attendance was not related to greater effects on primary or secondary outcomes.
PLH for adolescents
Of the 107 caregivers who were recruited, 86 (80.4%) attended at least one group session and 64 (60%) attended at least half (seven group sessions or home visits) of the program. Just under half (53 caregivers, 49%) of the recruited caregivers completed the postintervention questionnaire. Of the 108 adolescents who were recruited for the program, 69 (63.89%) attended at least one group session and 60 (55.6%) attended at least half (seven group sessions or home visits) of the program. Fifty-two (48.15%) of the recruited adolescents completed the postintervention assessment. Tables 4 and 5 summarize baseline comparisons of caregivers and adolescents lost to the postintervention assessment and those retained.
Baseline Comparisons of Adolescents Lost to Postassessment and Those Retained.
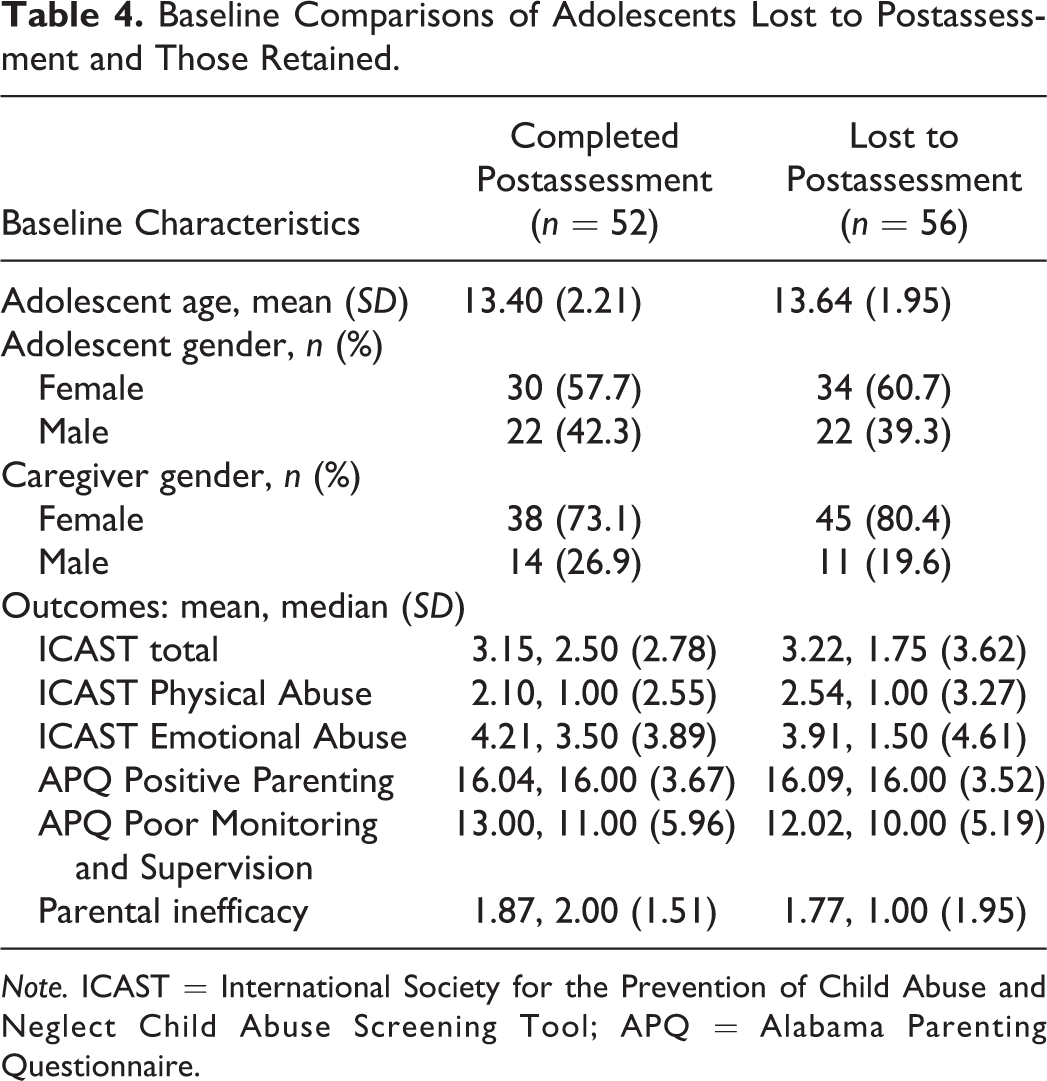
Note. ICAST = International Society for the Prevention of Child Abuse and Neglect Child Abuse Screening Tool; APQ = Alabama Parenting Questionnaire.
Baseline Comparisons of Caregivers Lost to Postassessment and Those Retained.
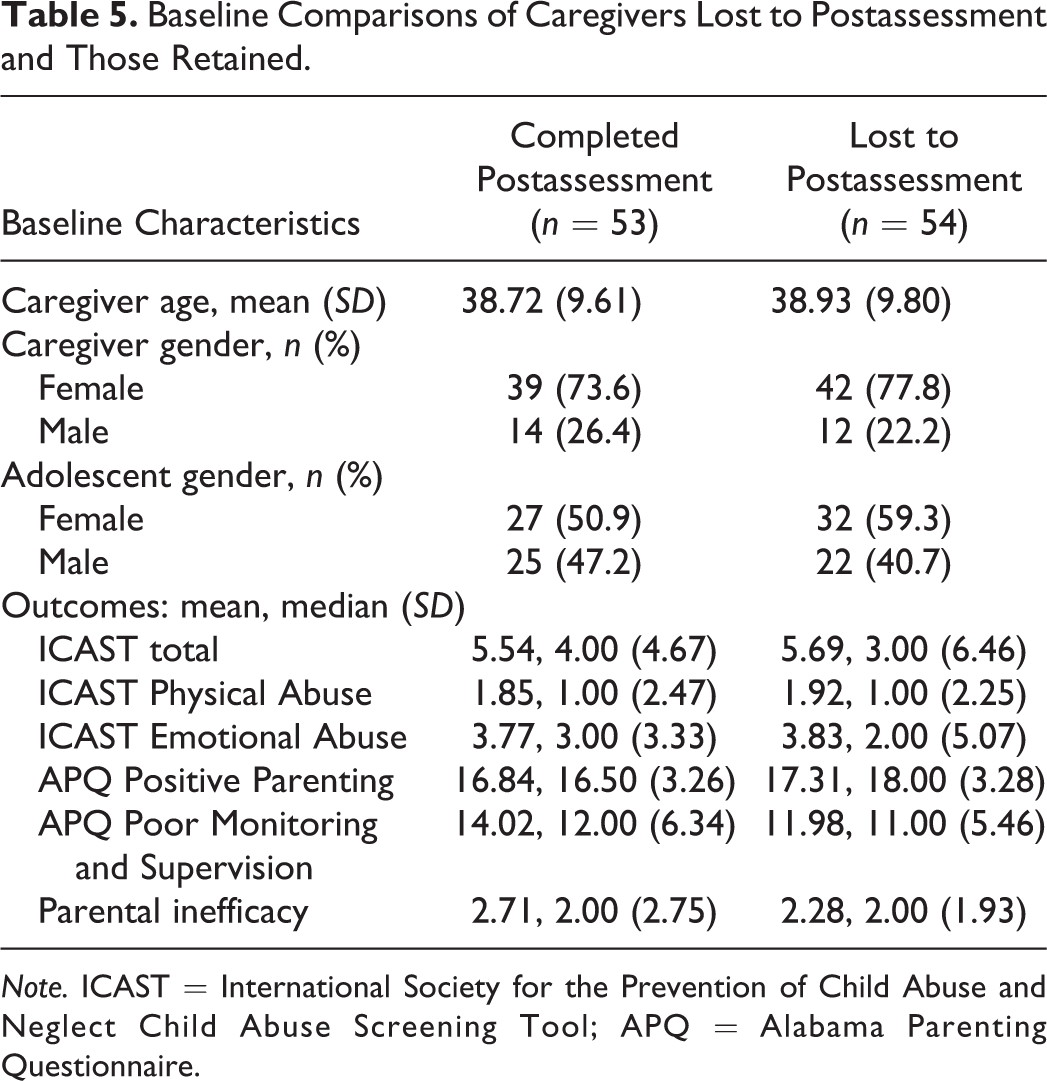
Note. ICAST = International Society for the Prevention of Child Abuse and Neglect Child Abuse Screening Tool; APQ = Alabama Parenting Questionnaire.
An intent-to-treat analysis was conducted, that is, all 107 caregivers and 108 adolescents were included in the analyses. The mean overall attendance rate was 6.81 (SD = 5.88) sessions, or 48.64% of the program for adolescents and 7.40 (SD = 5.63) sessions, or 52.86% of the program for caregivers. There were no differences between female and male attendance patterns, both for caregivers (std. β = 0.01, 95% CI [−.12, .14], p = .836) and for adolescents (std. β = 0.09, 95% CI [−.03, .21], p = .136). Adolescent age was also not associated with caregiver (std. β = −0.09, 95% CI [−.22, .04], p = .159) or adolescent (std. β = 0.10, 95% CI [−.23, .30], p = .168) attendance. Higher attendance was associated with increased positive parenting reported by adolescents (std. β = 0.18, 95% CI [.03, .32], p = .022); no other associations were found between attendance and outcomes.
Outcomes
Tables 6 and 7 summarize outcomes comparing baseline and postintervention scores.
PLH for Young Children: Outcomes Using MLMM and an Intention-to-Treat Analysis.

Note. std. β = standardized beta estimates; CI = standardized confidence intervals; R 2 = conditional R 2; f 2 = Cohen’s f-squared effect size; MLMM = multivariate linear mixed modeling; ICAST = International Society for the Prevention of Child Abuse and Neglect Child Abuse Screening Tool; PARYC = Parenting Young Children.
PLH for Adolescents: Outcomes Using MLMM and an Intention-to-Treat Analysis.
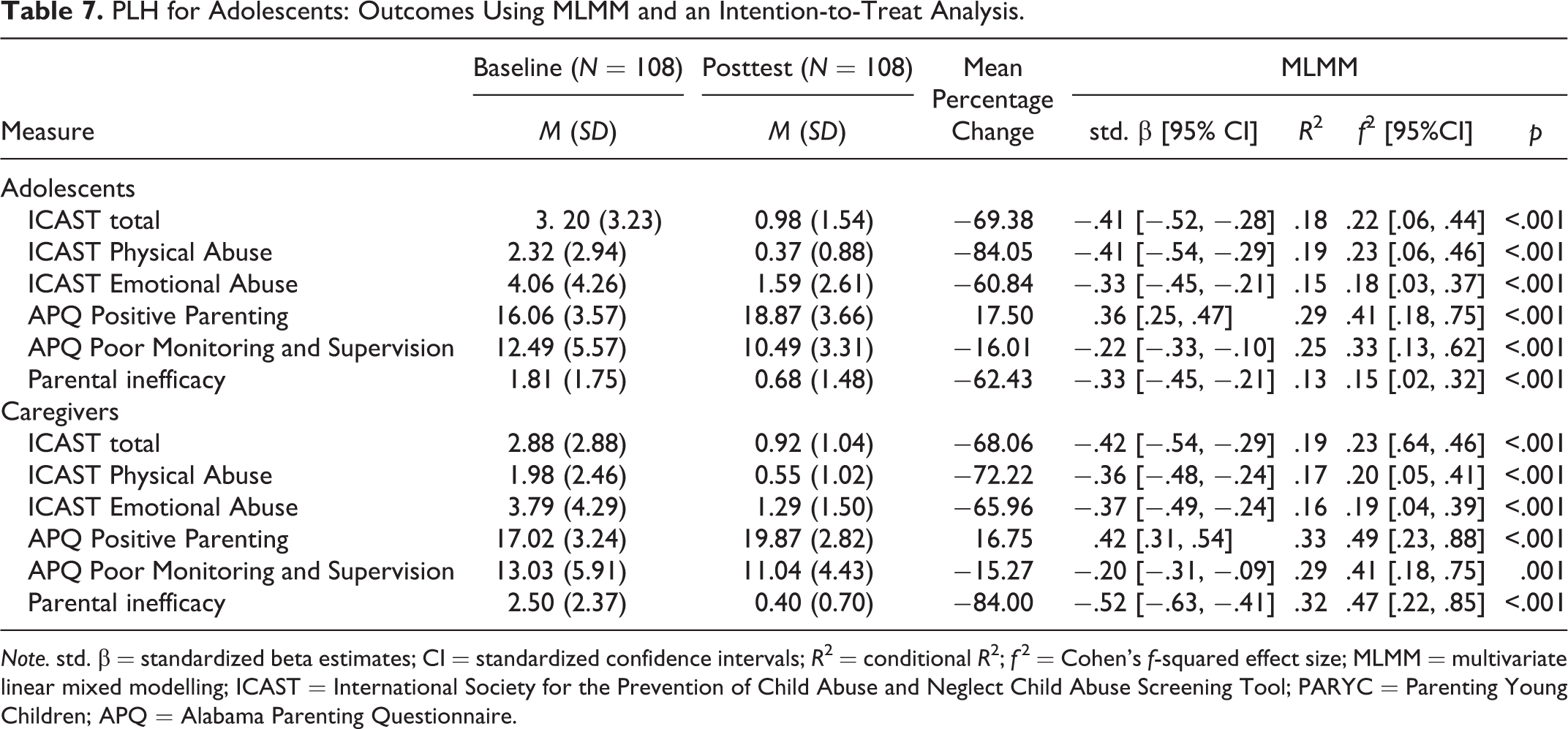
Note. std. β = standardized beta estimates; CI = standardized confidence intervals; R 2 = conditional R 2; f 2 = Cohen’s f-squared effect size; MLMM = multivariate linear mixed modelling; ICAST = International Society for the Prevention of Child Abuse and Neglect Child Abuse Screening Tool; PARYC = Parenting Young Children; APQ = Alabama Parenting Questionnaire.
PLH for young children
There were large reductions in overall harsh discipline based on the ICAST total scale ( f 2 = 0.89, 95% CI [0.51, 1.54], p < .001). There were also large reduced treatment effects for the ICAST Physical Abuse and Emotional Abuse subscales ( f 2 = 0.82, 95% CI [0.46, 1.42], p < .001; and f 2 = 0.45, 95% CI [0.20, 0.82], p < .001, respectively). Caregivers also reported moderate treatment effects for supporting positive behavior ( f 2 = 0.33, 95% CI [0.12, 0.63], p < .001) and large effects for Parental Limit Setting subscale ( f 2 = 0.45, 95% CI [0.20, 0.82], p < .001). No adverse events were noted.
PLH for adolescents
There were moderate reductions in overall harsh discipline, as reported by both caregivers ( f 2 = 0.27, 95% CI [0.09, 0.52], p < .001) and adolescents ( f 2 = 0.22, 95% CI [0.06, 0.44], p < .001). There were moderate reductions for Physical Abuse and Emotional Abuse subscales, as reported by caregivers (Physical Abuse: f 2 = 0.22, 95% CI [0.06, 0.44], p < .001; Emotional Abuse: f 2 = 0.22, 95% CI [0.06, 0.44], p < .001) and adolescents (Physical Abuse: f 2 = 0.23, 95% CI [0.06, 0.46], p < .001; Emotional Abuse: f 2 = 0.18, 95% CI [0.03, 0.37], p < .001).
Caregivers and adolescents reported large treatment effects for increased positive parenting (caregivers: f 2 = 0.56, 95% CI [0.29, 0.98], p < .001; adolescents: f 2 = 0.45, 95% CI [0.21, 0.81], p < .001) and moderate to large effects for reduced poor monitoring and supervision (caregivers: f 2 = 0.41, 95% CI [0.18, 0.75], p = .001; adolescents: f 2 = 0.33, 95% CI [0.13, 0.62], p < .001). Additionally, there were moderate to large decreases for parental self-inefficacy following the intervention (caregivers: f 2 = 0.52, 95% CI [0.26, 0.92], p < .001; adolescents: f 2 = 0.16, 95% CI [0.02, 0.34], p < .001). No adverse events were noted.
Discussion and Application to Practice
Results indicate that the PLH programs for Young Children and Adolescents in South Sudan appear to be a successful example of implementation of evidence-based parenting programs within routine service delivery, suggesting that these interventions can be transported across cultural settings as well as from a relatively low-intensity conflict area to a high-intensity conflict setting.
The enrollment and attendance rates for PLH for Young Children were higher than those achieved in the PLH for Young Children trials in South Africa (Lachman et al., 2017; Wessels, 2017), the recent Filipino trial (Lachman et al., 2018b), and were greater than parenting programs of similar length in HICs (Chacko et al., 2016; Hutchings et al., 2007). Even under ideal trial conditions, high level of enrollment and attendance is challenging; real-world delivery is typically even very lower, often less than 10% (Fagen et al., 2009). Nevertheless, high enrollment and attendance rates in this study were achieved despite delivery under highly stressful postwar circumstances, including curfews and poor infrastructure. Potential reasons may be that programs were nested within other services instead of a stand-alone program like in South Africa or that programs were delivered as part of preexisting health services. This may be particularly important in conflict-affected settings where families are affected by adversities on multiple levels (Inter-Agency Standing Committee, 2007; Jordans et al., 2016).
Enrollment and attendance for PLH for Adolescents was considerably lower than PLH for Young Children. Caregivers and adolescents who did not complete the postintervention questionnaire reported slightly higher abuse at baseline compared to those who were retained at postintervention (see Tables 4 and 5). Families with higher abuse levels may therefore require additional support to encourage higher engagement in the program. Anecdotally, facilitators also reported that a chief reason for poor attendance was that program schedules conflicted with caregivers’ working hours, also found to be an issue in the South African trial (Ward et al., 2020). Moreover, many caregivers worked on farms, which affected their ability to attend, especially since PLH for Adolescents took place during the wet season (November 2017–May 2018) when crops are typically planted. Additionally, public infrastructure such as roads and bridges is lacking in most parts of the country due to the devastation from the internecine conflict (WHO, 2018b), compromising access to urban areas for a large proportion of the population during rainy season. These barriers to program attendance highlight the need to roll out interventions in rural communities to reduce traveling long distances and to find creative ways to reach employed caregivers, perhaps through workplace delivery (Sanders et al., 2011), or to ensure sessions take place outside of working hours.
The difficulty of recruiting male participants in parenting programs has been well documented, even in HICs (Panter-Brick et al., 2014). Encouragingly, almost one quarter of the participants in PLH for Young Children comprised of male caregivers, although male caregivers appeared to be slightly less likely to attend, possibly because female caregivers are generally considered the primary caregiver for younger children. Similarly, almost one quarter of the participants in PLH for Adolescents comprised of male caregivers. For this program, male and female caregivers were equally likely to attend, perhaps because both female and male caregivers are equally engaged with childcare as children get older. Moreover, the high rate of male caregivers recruited into the program for PLH for Adolescents may be due to program adaptations by Catholic Relief Services South Sudan specifically aimed at male caregivers. Future research should explore this particular aspect of 4Children South Sudan’s success.
Despite the challenges in program attendance for PLH for Adolescents, both interventions reduced harsh discipline with moderate to large effect sizes. Reduction in abuse was exceptionally high for both PLH programs, reducing between 68% and 77% from baseline. Positive parenting behavior also improved following both programs, with moderate to large effect sizes. For PLH for Adolescents, adolescents and caregivers independently reported reductions in parental inefficacy with moderate to large effect sizes. Overall, the interventions showed no evidence of harmful effects. The results from both PLH programs are encouraging as they indicate that retained effectiveness is possible in routine service delivery despite the conditions that prevail in challenging contexts.
Contrary to existing literature that shows a positive relationship between attendance rates and program outcomes (Baydar et al., 2003; Reyno & McGrath, 2006), higher program attendance was not significantly associated with greater effects on primary or secondary outcomes in either intervention (except for adolescent reported positive parenting). This may be due to limited variation in dosage (Shenderovich et al., 2019), especially for PLH for Young Children. Alternatively, participants may have learnt missed program material from facilitators and peers in home visits and later sessions, consequently still improving despite overall lower dosage. However, this cannot be identified without a control group, thus requiring further research.
Many evidence-based parenting interventions developed in HICs require program delivery by highly skilled professionals such as psychologists and nurses, often not available in high-need settings (Knerr et al., 2013). Results from South Sudan illustrate that it may be possible to deliver parenting programs using trained and supervised paraprofessionals. This has important implications for scalability as it reduces the overall cost and increased feasibility of implementation in low-resource conflict settings.
To ensure that programs can be delivered with effectiveness across different settings, feasible and cost-effective monitoring strategies are also required (WHO, 2018a). This study demonstrates that it is feasible for local implementing organizations to collect monitoring data during routine delivery, an encouraging finding as it can help implementers improve future delivery. It may, therefore, be beneficial for donors to encourage the organizations they fund to collect this type of data. Nevertheless, this would require support to learn how to collect and analyze such data.
These findings should be interpreted in the light of several of limitations. First, findings from routine pre–post data are only suggestive of potential intervention results and should be considered with caution as the programs were not studied in the context of randomized controlled trials (Rossi et al., 2004). Second, outcomes were only measured using self-reports collected by facilitators who had also delivered the program to participants, which may have increased reporting biases due to social desirability (van de Mortel, 2008). Future research could consider independent investigators for postassessment data collection or observational methods to evaluate program effects from multiple perspectives (Gardner, 2000). However, both these methods may be less feasible in routine settings due to additional costs. Thirdly, measures were in English but were administered by facilitators who translated them verbally for participants in the moment during data collection. While this may introduce bias into the data, it is the approach most feasible for community-based organizations delivering services with limited financial resources to implement more robust evaluation procedures. Lastly, outcome measures were collected immediately after the programs, and thus, whether the effects will endure remains unknown.
Despite these limitations, findings indicate that both PLH programs appear to retain effectiveness in routine service delivery under highly stressful postconflict circumstances. Despite many potential barriers to implementation, including poor infrastructure and curfews, the programs had high enrollment and attendance rates, suggesting that these programs can be delivered to very vulnerable families. Furthermore, the results show that collecting routine monitoring data, even under the difficult conditions of postconflict, low-income contexts with staff who were not trained in monitoring and evaluation, is possible. Given the small sample size, more research into what improves and inhibits effectiveness in routine delivery is needed (Loening-Voysey et al., 2018). Nevertheless, these findings suggest promising program viability and may carry potential to reach families who are in the greatest need of intervention.
Footnotes
Acknowledgments
The authors are grateful to the following: the implementing partners, program facilitators, and families who participated in this study; the United States President’s Emergency Plan for AIDS Relief (PEPFAR) and the United States Agency for International Development (USAID) under cooperative agreement AID-OAA-A-14-00061; the European Research Council under the European Union’s Horizon 2020 research and innovation programme (Grant Agreement No. 737476 and Grant Agreement No. 771468), the UKRI GCRF Accelerating Achievement for Africa’s Adolescents Hub (Grant Ref: ES/S008101/1), Research England, the John Fell Fund, the Leverhulme Trust (PLP-2014-095), the Cambridge Trust, and the University of Oxford’s ESRC Impact Acceleration Account (1311-KEA-004 and 1602-KEA-189); Clowns Without Borders South Africa for providing training and supervision; Prof. Colin Tredoux (University of Cape Town) for assistance with the statistical analyses.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C. W., J. M. L., and L. C. are codevelopers of the PLH for Young Children and PLH for Adolescents programs, which are licensed under a Creative Commons 4.0 Non-commercial No Derivatives license, and cofounders of the PLH initiative. J. M. L. is also the Executive Director of Clowns Without Borders South Africa, a nonprofit institution responsible for the dissemination of the program. J. M. L. also receives occasional fees for providing training and supervision to facilitators and coaches. J. M. L. and C. W. have participated (and are participating) in a number of research studies involving the program, as investigators, and the Universities of Oxford, Glasgow, and Cape Town receive research funding for these. Conflict is avoided by declaring this potential conflict of interests and by conducting and disseminating rigorous, transparent, and impartial evaluation research on both this and other similar parenting programs. S. B., F. M., K. M., and D. O. work for Catholic Relief Services, which was the implementing partner.
Funding
The authors received no addtional financial support for the research, authorship, and/or publication of this article.