
Abstract
As many as one third of children who reunify from child welfare systems reenter care because of continued child maltreatment. This can have long-term deleterious effects on mental health. Yet, few studies have examined interventions that have been effective in promoting successful reunification or reunification that does not result in recidivism. This study presents findings from a systematic review of interventions that target successful reunification. We searched five academic databases, governmental and educational websites to identify prior literature. Three researchers extracted data from N = 216 studies retrieved and screened in 10 that met all inclusion criteria. However, small sample sizes, lack of replication of studies, and small effect sizes limit the generalizability of findings. As such, the findings from this review highlight a need for more rigorous studies to build the evidence base of post-permanence interventions for families that reunify.
Reunification with a biological parent is the priority in child welfare systems, yet approximately 20% (Kids Count Data Center, 2019) of children who reunify with birth parents reenter foster care. The hazards of reentry have been found to be highest (0.059) during the first few months of reunification, dropping to 0.004 after 19 months post-reunification (Lee et al., 2012); thus, there is a higher risk of reentry during the first 18 months of reunification. Child maltreatment and caregiver instability can be particularly harmful for infants and toddlers given the critical stage of brain development during the first few years of life (Frame et al., 2000; Perry, 2009, 2014). The instability of attachment relationships during childhood, for example, has been linked to maladaptive adult mental health (Perry, 2014; Schore, 2016). Moreover, inconsistent caregiving via multiple removals from the birth family, coupled with exposure to child maltreatment, can impact long-term mental health outcomes for children in foster care (Kimberlin et al., 2009). The vulnerability and complex needs of young children in foster care systems have led professionals to a call for better coordination and improved interventions with biological families (Vig et al., 2005). For these reasons, young children in foster care systems need better coordination and interventions aimed at improving their reunification with biological families as well as interventions that support them post-reunification (Vig et al., 2005).
The need for effective reunification interventions is suggested in child welfare policy going back into the 1990s. The Adoption and Safe Families Act of 1997 (ASFA; Public Law 105-89) set guidelines to establish time constraints on reunification of children in foster care with biological parents to avoid children languishing in care (O’Neill Murray & Gesiriech, 2004). ASFA requires state agencies to make reasonable efforts to provide biological families with services that are individualized, accessible, and timely (Mallon & McCartt Hess, 2005). Critics have worried, however, that these stricter time constraints might lead to rushed reunifications (Streff, 2016) or, alternatively, not give families who require longer term supports the opportunity to reunify, thus not resulting in improved interventions (Rockhill et al., 2007; Moye & Rinker, 2002). Instead, it has been proposed that one way to improve reunification success would be to conceptualize reunification as an ongoing process instead of the end destination or goal (Wulczyn, 2004). This shift toward successful reunification is evidenced in a recent brief from the Child Welfare Information Gateway (CWIG, 2017) that focused on ways to support post-reunification success for families involved in child welfare systems. Supports such as collaboration with courts, community providers, and families have been suggested to provide ongoing support for families post-permanence, though in practice, literature has suggested that many interventions still focus on reunification as a final outcome with few or no services provided after families have physically reunified. Yet, reentries can occur up to 5 years or more after reunification (Font et al., 2018), evidencing a need for long-term, ongoing support that families can access as stressors arise.
Research on Successful Reunification of Families
Despite the importance of reunification in child welfare policy and practice, reviews that examined effective interventions in this area are rather nonexistent. Most of literature instead examined risk factors associated with reunification instead of reentry or recidivism after reunification. White and colleagues (2015) conducted a systematic review to examine risk factors for recurrences of child maltreatment among reunified families, including any level of substantiation; however, this review only identified risk factors, such as parental substance use and mental health problems, without assessing interventions that could help mitigate risk of future child maltreatment. White and colleagues (2015) found little evidence that child-level characteristics such as gender or ethnicity were associated with recurrences of child maltreatment. In contrast, parental risk factors such as drug use, alcohol misuse, and mental health problems were consistently linked with recurrences of child maltreatment (White et al., 2015). Another systematic review focused on factors that impacted reunification rates among mothers with histories of substance use; this review concluded that mothers who used heroin had lower rates of reunification and that many had mental health issues co-occurring with their substance use disorders (Doab et al., 2015) but did not specifically address effective interventions.
Although little has been systematically reviewed about recidivism and reentry after reunification, two recent reviews examined the effects of interventions on physical reunification rates. A recent meta-analysis examined the effectiveness of interventions to increase parental engagement and physical reunification rates (Maltais et al., 2019). This review concluded that family-focused interventions increased parental engagement and physical reunification rates. Another recent review of cross-system collaboration and reunification outcomes found that Family Drug Treatment Courts may increase the odds of physical reunification for families from child welfare systems (Ogbonnaya & Keeney, 2018). These reviews can help identify interventions for families and agencies that help families reunify from foster care. However, there is a lack of understanding of what helps families stay together after reunification and prevent reentries into foster care systems. Thus, there is a need to expand on these prior studies to not only understand factors and interventions to increase physical reunification rates but also interventions that can support families to achieve successful reunifications and decrease reentry rates.
Aims of the Study
The current study addresses the gap in literature on how best to intervene with families as they reunify from child welfare systems by systematically reviewing evidence from prior studies on the effectiveness of interventions in increasing successful reunification. For this review, successful reunification is defined as lack of reentry into care or lack of re-referral for recurrences of child abuse or neglect. The objective of this systematic review is to review prior evidence on interventions that have decreased reentry and re-referral rates of children who have reunified with a biological parent from foster care.
Method
Search Procedures
The Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols checklist (PRISMA-P; Moher et al., 2009) for conducting and reporting systematic reviews guided the process from question development to eligibility criteria, data collection procedures, data analysis procedures, risk bias assessment, and presenting and interpreting results. We developed a specific search strategy, and the following search terms were used: (reunification) AND (foster care) AND (intervention OR service* OR therapy OR program OR strateg*) and (famil*). Searches were initially conducted in April, 2018, repeated in July, 2018, and repeated for a final time in September, 2019. The following search terms were used in the Google searches: (reunification) AND (foster care) AND (intervention OR service* OR therapy OR program OR strategy) AND (famil*) site: gov; and (reunification) AND (foster care) AND (intervention OR service* OR therapy OR program OR strategy) AND (famil*) site: edu. There were three main strategies used to search available literature: (a) academic search engines, including dissertation and abstract indexes; (b) searches of government and educational institutions using Google; and (c) direct contact with professionals at child welfare systems and experts in the field of child welfare to identify reports and other program evaluations that met the inclusion criteria. The second two strategies were included to increase potential gray literature that could meet inclusion criteria.
A total of five academic search engines, including PsycINFO, academic search complete, SocINDEX, family studies abstracts, and ERIC, were searched to identify articles that might meet eligibility criteria. For the Google searches, literature published on university websites and government agencies such as the CWIG were searched. Finally, emails were sent to contact people at all 50 state child welfare agencies to identify any other program evaluations. To improve upon the searches and increase potential gray literature, a librarian who specializes in social sciences and social work was consulted about the selection of search terms, and two experts in the field of child welfare were also consulted.
Inclusion and Exclusion Criteria
Following the PRISMA-P guidelines, studies were included if they met these criteria: (a) population: biological parents of children in foster care in the United States after 1997; (b) intervention: any intervention that targeted the population of interest and met the other inclusion criteria; (c) comparison: any study that included an intervention group and comparison, be it matched or randomly assigned; (d) outcome: subsequent contact with child protective services after reunification, either via re-referral for child maltreatment or reentry into foster care; and (e) study design: quasi-experimental or experimental so that the study included an intervention and comparison group. Any intervention was eligible for inclusion as long as it reported at least one outcome related to reunification success (e.g., reentry or referral rates) and targeted biological parents of children who reunified from foster care. Given the importance of the time constraints placed on case plans with the ASFA (1997), only studies that were conducted after the implementation of ASFA were included. Finally, given the previous geographic eligibility criterion, only studies in English were included.
The exclusion criteria included (a) studies in which the sample included participants outside of the United States, (b) studies that did not specifically test an intervention, (c) studies that tested an intervention that had been implemented prior to 1997, (d) studies that did not report on measures for a comparison and intervention group, (e) studies that did not use an experimental or quasi-experimental design, and (f) studies that did not report on a measure of successful reunification (e.g., reentry or re-referral to child protective services).
Data Extraction
A group of three social work researchers developed a codebook and utilized a data extraction sheet to collect data for this systematic review. Ten studies from the initial searches were coded as a pilot, and the three researchers met after to discuss protocol and refine inclusion and exclusion criteria. These studies were the first 10 retrieved from the academic searches. Each individual study was coded for study bibliographic information (e.g., author, year, geographic location of sample), study design (e.g., experimental, quasi-experimental, or other), sample characteristics (e.g., biological parents or foster parents, sample size, age of participants), and intervention. The team grouped outcomes into two main types: reentries into foster care and re-referrals to child protective services.
Inter-rater and inter-coder reliability
All literature that was initially retrieved was screened by two review authors and then a random 10% sample of all initial articles was assigned to a third coder to increase rigor and improve inter-coder reliability. Following a similar protocol, two coders read the full-texts of all articles screened in after the initial round of titles and abstracts and a random 10% sample of these articles were assigned to a third coder. Inter-coder reliability was assessed after each round of coding, ranged from 91% to 98%, and discrepancies were addressed as a team. A standardized coding sheet was used by each coder to examine specific variables relevant to the inclusion criteria and outcomes of interest.
Risk of Bias in Individual Studies and Across Studies
In accordance with the PRISMA-P systematic review guidelines, the authors of this study assessed the risk of bias in each individual study and across studies to help interpret findings and identify the strength of the included studies (Viswanathan et al., 2017). The studies that met all eligibility criteria were assessed for risk of bias guided by the Cochrane Collaboration’s tool for assessing risk of bias (Higgins & Green, 2011). This included an assessment of the following six domains: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other bias. A coding sheet was developed by the first author to assess each domain within each individual study. Two coders used this sheet to assess bias and met to discuss any discrepancies. As studies were screened, they were assessed as either having a low risk of bias, unclear risk of bias, or high risk of bias, in accordance with the Cochrane Collaboration tool for assessing risk of bias (Higgins & Green, 2011).
Results
Study Selection
Figure 1 presents the PRISMA flow diagram which detailed our search procedure. Databases were searched simultaneously using the tool to simultaneously search the five academic databases and thus automatically deleted any duplicate articles across databases. The initial searches of databases from all three points in time (March 2018, July 2018, September 2019) resulted in a total n = 178 articles. A screening of reference lists from these articles, the Google searches, and consultation with professionals at state agencies yielded an additional 38 reports for initial review, resulting in a total N = 216 articles.

PRISMA flow diagram of articles screened at each stage.
In the first round of screening, titles and abstracts were read by two readers to determine initial eligibility criteria. Articles were only excluded in this stage if the title or abstract contained information that clearly did not match eligibility criteria; if eligibility criteria were not clear from the title or abstract, the article was included for Round 2 screening. In Round 1 of title and abstract screening, a total of 49 articles were screened in for full-text reading and the remaining 167 were screened out. Of those screened out, the majority did not evaluate a specific intervention, did not use the population of interest, or were conducted outside of the United States.
In Round 2 of screening, full texts were read and articles were coded using a standardized coding sheet that included all eligibility criteria, outcomes measured, main findings, and any study limitations identified. Of the 49 articles screened in this stage, 39 were excluded. Articles were screened out for multiple reasons and some articles met multiple criteria for exclusion.
Removal reason
In Round 1 of screening, the research team read the titles and abstracts of 216 studies. In this round of screening, a total of 167 articles were screened out; n = 116 were screened out because they lacked an intervention, n = 26 were screened out because they did not take place in the United States, n = 19 were screened out because they did not include a measure of reentry or recidivism, and n = 6 were screened out because the population of the study did not include biological parents of children in care. Studies in Round 2 of screening were excluded because of the study design (e.g., the outcomes did not capture measures of reunification success; n = 18); population (e.g., data from before the ASFA of 1997, intervention with foster parents instead of biological parents, or population outside of the United States; n = 25); or lack of intervention (n = 8). The remaining n = 10 articles met all inclusion criteria and were included for synthesis in this review. These 10 articles present findings from 10 distinct studies.
Assessment of Risk of Bias
In accordance with the Cochrane guidelines for systematic reviews (Furlan et al., 2015), an assessment of risk of bias was conducted to systematically examine the methodological rigor and overall quality of the studies that met inclusion criteria (Higgins & Green, 2011; Moher, et al., 2009). Table 1 displays the results of the assessment of risk of bias in each individual study.
Risk of Bias Across Individual Studies.
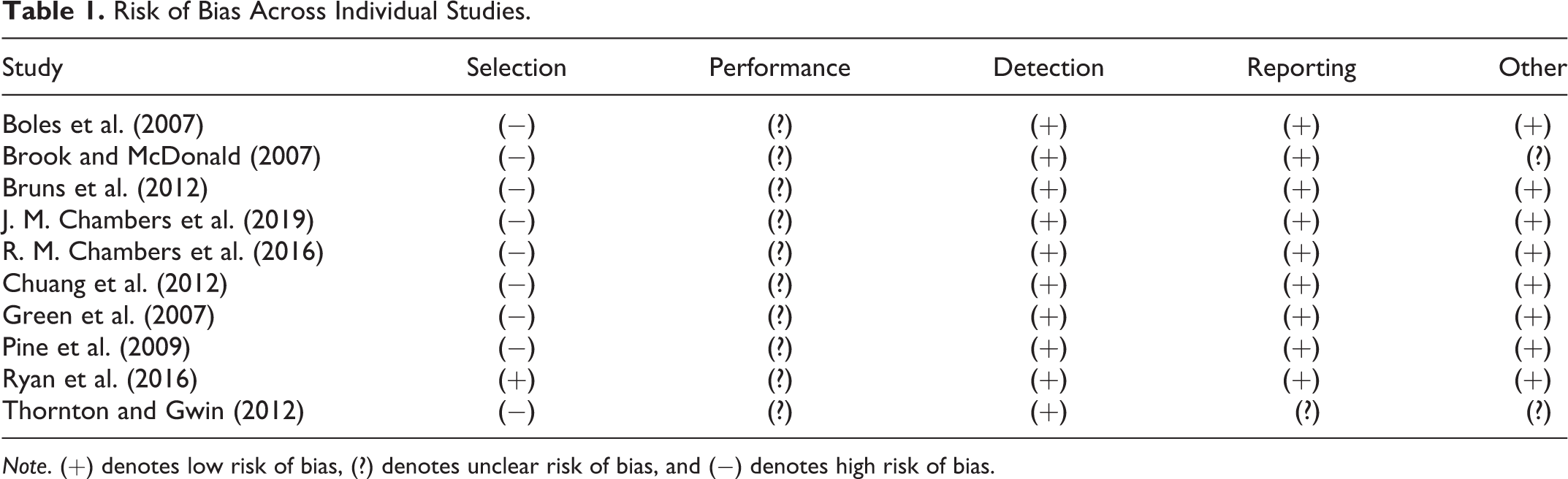
Note. (+) denotes low risk of bias, (?) denotes unclear risk of bias, and (−) denotes high risk of bias.
Nine of the articles had a high risk of selection bias since they used a quasi-experimental design instead of randomized methods. The remaining study had a low risk of bias because of the experimental design that randomized participants into the intervention and control groups. Participants in all 10 studies were aware that they were receiving the intervention; however, the use of administrative data to track results reduced the risk of bias in reporting outcomes in these studies.
Analysis of Studies
Table 2 displays the authors, design, sample, outcome measure(s), and results for each of the 10 final studies included in this review. The 10 studies involved a total of 7,278 parents. Eight of the 10 studies reported the number of children that these parents had, which resulted in a total of 8,742 children, with two studies (Chuang et al., 2012; Ryan et al., 2016) not reporting specific child demographics or characteristics. Overall, the results showed that there were mixed results for the effectiveness of the reunification interventions studied. Six of the studies showed at least one positive outcome based on the outcomes measured (Bruns et al., 2012; J. M. Chambers et al., 2019; R. M. Chambers et al., 2016; Chuang et al., 2012; Ryan et al., 2016; Thornton & Gwin, 2012), while three studies did not find a difference in outcomes between the intervention and comparison groups (Boles et al., 2007; Green et al., 2007; Pine et al., 2009), and one study found that intervention families had worse outcomes than the comparison group (Brook & McDonald, 2007). Effect sizes were not reported in the studies demonstrating a weakness in the report of findings across the studies. The research team utilized the Campbell Collaboration Effect Size calculator (Wilson, n.d.) to calculate effect sizes for eight of the 10 studies; the remaining two studies did not list enough information to provide estimates of effect size. In the eight studies that provided enough information to calculate effect size, risk ratios (RRs) were calculated that ranged from 0.16 to 3.28.
Participant Characteristics
Of the 7,278 parents included in the 10 studies, there was varying information about sociodemographic characteristics. Five of the 10 studies reported caregiver gender (Boles et al., 2007; Chuang et al., 2012; Green et al., 2007; Ryan et al., 2016; Thornton & Gwin, 2012); of the 4,980 parents who received services in these five studies, 4,108 (82.49%) were female. Studies varied in their conceptualization and operationalization of race/ethnicity. One study only reported child race (J. M. Chambers et al., 2019); two studies only reported parent race (Chuang et al., 2012; Green et al., 2007); one study reported race as a “family characteristic” (Ryan et al., 2016); five studies reported both parent and child race (Boles et al., 2007; Brook & McDonald, 2007; Bruns et al., 2012; R. M. Chambers et al., 2016; Pine et al., 2009); and one study reported only the proportion of “families of color” in the sample (Thornton & Gwin, 2012). Studies also varied in the number of racial/ethnic categories included. Two studies compared White to any non-White participants (J. M. Chambers et al., 2019; Thornton & Gwin, 2012), while other studies separated out non-White racial categories.
Six of the 10 studies reported parental risk factors such as mental health issues, substance use, or neglect of children (Boles et al., 2007; Bruns et al., 2012; J. M. Chambers et al., 2019; R. M. Chambers et al., 2016; Pine et al., 2009; Ryan et al., 2016). A further three studies did not specify parental risk factors or removal causes but listed parental substance use as an inclusion criterion to receive the intervention (Brook & McDonald, 2007; Chuang et al., 2012; Green et al., 2007). Of the nine studies that reported parental substance use (either as a risk factor or inclusion criterion), 2,552 of 2,849 parents that received interventions (89.58%) had an issue with substance use. Three studies (Boles et al., 2007; J. M. Chambers et al., 2019; R. M. Chambers et al., 2016) reported the proportion of parents receiving the intervention that had an underlying mental health issue; of 756 parents that received interventions in these three studies, 221 (29.23%) had a mental health issue, although none of these were specified. Of 759 parents that received services in four studies (Bruns et al., 2012; J. M. Chambers et al., 2019; R. M. Chambers et al., 2016; Pine et al., 2009) that examined removal causes, 416 (54.80%) had neglect listed as a removal cause. Two studies (Boles et al., 2007; Ryan et al., 2016) reported rates of homelessness among parent participants; of the 1,685 parents who received services in these studies, 439 (26.05%) had experienced homelessness. Another two studies reported domestic violence as a risk factor among parent participants (R. M. Chambers et al., 2016; Pine et al., 2009) and found that of the 183 parents who received services, 54 (29.51%) had experienced domestic violence.
Outcomes
Studies measured three distinct child welfare outcomes related to successful reunification: reentry, recidivism (e.g., subsequent investigations, substantiated re-referrals), and stability after reunification. Table 2 presents the main findings, sample characteristics, interventions, and study design for the 10 studies that met eligibility criteria.
Characteristics of Prior Studies on Interventions to Increase Reunification Success.
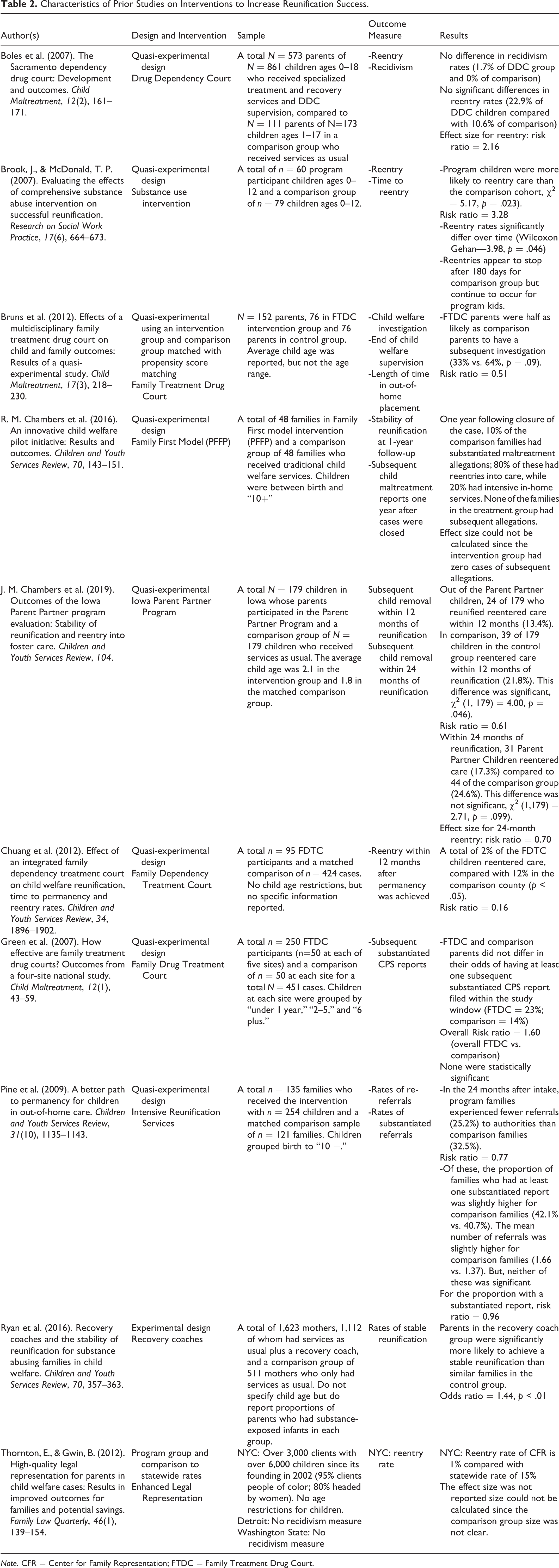
Note. CFR = Center for Family Representation; FTDC = Family Treatment Drug Court.
Reentries
Five studies measured entries into care after reunification; four measured reentries after case closure (reentry), and one measured both recidivism (reentries before case closure) and reentry. Of the five studies that had a measure or reentry, two studies found that families in the intervention group were less likely to reenter care (Chuang et al., 2012; Thornton & Gwin, 2012). However, of these two studies, only one listed the size of the comparison group; therefore, only one effect size could be calculated, resulting in an RR of 0.16 for Chuang and colleagues’ (2012) study of Family Drug Treatment Courts.
One study found no difference in reentry rates between the intervention and comparison group (Boles et al., 2007). In this study, 22.9% of the Drug Dependency Court intervention group reentered care compared to 10.6% of the comparison group, with an RR of 2.16. A different study found that program families were less likely to reenter care within 12 months but that the difference in reentry rates was not significant at 24 months post-discharge (J. M. Chambers et al., 2019). Within 12 months, 13.4% of the Parent Partner intervention families reentered care, compared to 21.8% of the comparison group, χ2 (1, 179 = 4.00, p = .046, resulting in an effect size of RR = 0.61. Yet, at 24 months post-reunification, 17.3% of the Parent Partner families had reentered care compared to 24.6% of the comparison group, χ2 (1, 179) = 2.71, p = .099, resulting in an effect size of RR = 0.70.
The last study that measured reentries found that families in the intervention group were more likely to reenter care than the comparison (χ2 = 5.17, p = .023; Brook & McDonald, 2007). This study had an effect size of RR = 3.28.
Only one of the studies measured recidivism and found that a slightly higher proportion of families in the Drug Dependency Court reentered care before case closure (1.7%) than those in the comparison group (0.0%; Boles et al., 2007). However, the difference was not significant. The effect size could not be calculated for recidivism because the comparison group had 0.0% of families that reentered.
Recidivism
One study (Bruns et al., 2012) examined any re-referral to child protective services after reunification as an outcome. One study (Pine et al., 2009) examined both substantiated and unsubstantiated re-referrals to child protective services after reunification. Two studies (Chambers et al., 2019; Green et al., 2007) only examined substantiated re-referrals to child protective services. Of these four studies that examined re-referrals to child protective services, none found significant differences between the intervention and comparison groups.
The two studies that examined any re-referral to child protective services had a combined total of 211 parents in the intervention group and 197 parents in the comparison groups. The effect sizes for these studies ranged from RR = 0.51 to RR = 0.77. Bruns and colleagues (2012) found that 33% of the Family Treatment Drug Court group had a subsequent investigation with child protective services compared to 64% of the comparison group (p = .09). Pine and colleagues found that 25.2% of the intervention group experienced a subsequent referral compared to 32.5% of the comparison group.
Of the three studies that examined substantiated re-referrals to child protective services, there was a combined total of 433 families in the intervention groups and 370 families in the comparison groups. None of these three studies found significant differences in substantiated re-referrals. Two of the three studies reported enough information to calculate effect sizes; the effect sizes for these two studies ranged from RR = 0.96 (Pine et al., 2009) to RR = 1.60 (Green et al., 2007). Proportions ranged from 0% substantiated re-referrals among intervention families (R. M. Chambers et al., 2016) to 23% (Green et al., 2007) and 40.7% (Pine et al., 2009). In contrast, proportions of substantiated referrals among the comparison groups ranged from 10% (R. M. Chambers et al., 2016) to 14% (Green et al., 2007) to 35.2% (Pine et al., 2009).
Stability after reunification
Another measure of successful reunification was stable reunification. One study measured stable reunification, conceptualized as no reentries into foster care or other placement changes after reunification. Ryan and colleagues (2016) found that parents in the recovery coach intervention group were significantly more likely to achieve a stable reunification than those in the services-as-usual group, Exp(B) = 1.43, p < .01.
Intervention Characteristics
Of the 10 studies, 4 focused on Family Drug Treatment Courts (Boles et al., 2007; Bruns et al., 2012; Chuang et al., 2012; Green et al., 2007), while the other studies each evaluated a different intervention (e.g., intensive reunification services, recovery coaches). Nonetheless, given different models of Family Drug Treatment Courts, such as integrated and parallel, and different services provided in each, it is difficult to directly compare these studies. However, it is important to note that studies used a variety of interventions including inpatient and outpatient that could be examined further in future studies. Another two studies focused on substance abusing families in child welfare systems and included interventions such as recovery coaches (Brook & McDonald, 2007; Ryan et al., 2016). One study evaluated an intervention that provided enhanced legal representation for biological parents (Thornton & Gwin, 2012), one study evaluated a parent partner approach to provide mentorship to recently reunified families (J. M. Chambers et al., 2019), and the remaining two studies evaluated interventions that offered intensive reunification services and support for families (R. M. Chambers et al., 2016; Pine et al., 2009). The weak study designs and outcomes that showed only small effect sizes limits conclusions about the efficacy of specific interventions.
Family Drug Treatment Courts
The four studies that evaluated Family Drug Treatment Courts had a combined total of 994 parents that received the intervention and a combined total of 812 parents in comparison groups. Parent age ranged from 28 years old at one of the sites in Green and colleagues’ (2007) study to 34 years old at another site in Green and colleagues’ (2007) study. Two of the four studies reported average child age, and this ranged from 2.9 years old (Bruns et al., 2012) to 6.2 years old (Boles et al., 2007). In Green and colleagues’ (2007) study, between 45% and 63% of parents in the family treatment drug court had children under 2 years of age. Three of the four studies had a sample that was predominantly non-Hispanic White (Boles et al., 2007; Bruns et al., 2012; Chuang et al., 2012).
Of the four studies that evaluated Family Drug Treatment Courts, one evaluated a parallel model (Boles et al., 2007), two evaluated an integrated model (Bruns et al., 2012; Chuang et al., 2012), and one evaluated four slightly different models across sites (Green et al., 2007). The parallel Drug Dependency Courts continued to review child welfare aspects of cases in family courts but offered a specialized court officer who helps coordinate and oversees the recovery aspects of the case. Parents involved in child protective services had their cases flagged by an early intervention specialist if they met criteria and were then offered an opportunity to participate in the Drug Dependency Court. The parallel Drug Dependency Court provided parents with substance abuse treatment and a recovery specialist, as well as rewards to incentivize treatment compliance (Boles et al., 2007).
In contrast to the parallel Drug Dependency Court, the integrated Family Drug Treatment Court provided one judge who could oversee both the child protection and substance use components of a case. In addition to only having one judge, integrated models provided families with interdisciplinary teams including attorneys and social workers to provide wraparound and identify and refer families with complex needs to services (Bruns et al., 2012). Furthermore, the integrated Family Drug Treatment Court in Chuang and colleagues’ (2012) study provided biweekly court appearances, parenting classes, group counseling, individual counseling, and psychiatric and educational support as needed, in addition to the outpatient substance use rehabilitation services.
The final study that evaluated Family Drug Treatment Courts did not specify whether they were integrated or parallel models. Instead, Green and colleagues (2007) described the differences among the Family Drug Treatment Courts across the four sites selected in their study. At the Family Drug Treatment Court at Site A, parents tended to receive substance use rehabilitation services outside of the court and only received court-ordered referrals and services in cases of noncompliance. In addition, the Family Drug Treatment Court provided parents with a specialized case manager. At Site B, the Family Drug Treatment Court offered transitional housing services, a Head Start program with parenting classes, and short-term, long-term, and outpatient substance use services. The Family Drug Treatment Court at Site C included court-appointed special advocates and more integration of child welfare workers into team meetings, as well as assessment and referral for substance use treatment. The final Family Drug Treatment Court at Site D offered foster grandparents as mentors, weekly team meetings, and both residential and outpatient substance use treatment with diverse providers that contracted with the court (Green et al., 2007).
Other substance use interventions
An additional two studies (Brook & McDonald, 2007; Ryan et al., 2016) evaluated the impact of other interventions for substance-abusing families on child welfare outcomes. Given the differences in the core components of these interventions and samples, the studies are detailed individually below.
The intervention in Brook and McDonald’s (2007) study was developed in response to the growing needs of families with alcohol and drug abuse disorders and provided intensive services. A lead agency served as a coordinator for child welfare services, temporary assistance, domestic violence shelters, family courts, and housing services. Monthly meetings were held with the child welfare workers, substance abuse treatment providers, mental health workers, court representatives, and other relevant professionals involved with the case. Substance abuse services were provided by one center that focused primarily on intensive outpatient treatment (Brook & McDonald, 2007).
The intervention in Ryan and colleagues’ (2016) study consisted of assignation of professional recovery coaches who worked as intensive case managers for parents with substance abuse issues whose children were involved in child welfare systems. The recovery coach conducted assessments, advocated for the parent, assisted with service planning, outreach, and case management, as well as doing home visits, coordinating with the substance abuse treatment providers, and continuing home visits with child welfare workers and substance abuse treatment workers. Recovery coaches also continued to provide services until the case was closed, which gave them time to do home visits after children had reunified with the parents before the case was discharged from the child welfare system (Ryan et al., 2016).
Enhanced legal representation
One study evaluated the impact of enhanced legal representation on child welfare outcomes (Thornton & Gwin, 2012). The Center for Family Representation (CFR) provided enhanced legal services to families with child welfare contact. This included legal representation and assistance outside of court settings to help families understand and engage in the judicial processes, as well as advocating for referrals to services as needed (Thornton & Gwin, 2012). This specific CFR was founded in 2002 to respond to a crisis in representation of child welfare–involved families in New York. Families who participated in CFR were provided with interdisciplinary representation, including a social worker, parent advocate who has successfully reunified from child protective services with their children, and attorney.
Parent partner approach
One study evaluated the impact of the Iowa Parent Partner approach on successful reunification (J. M. Chambers et al., 2019). This intervention targeted families who had recently reunified from child welfare systems. Parents were matched with a mentor who provided support, guidance, and motivation. In addition, parents were provided opportunities to work with social workers, lawyers, and other community partners to receive additional services as needed. Parent mentors were selected by matching veteran parents who had been successful in reunifying and navigating child welfare systems and had similar characteristics, such as mental health problems, or substance use, as the parent in need (J. M. Chambers et al., 2019).
Intensive reunification services
The final two studies (R. M. Chambers et al., 2016; Pine et al., 2009) examined the impact of intensive reunification services on child welfare outcomes. As with the other studies presented earlier, given the different core components and target samples, these two studies are detailed individually instead of combined.
The Families First Model (PFFP) was implemented as part of the Pomona Family First project and consisted of four strategies to improve child welfare outcomes. PFFP consisted of a strengths-based model that focused on child safety, family well-being, and community partnerships (R. M. Chambers et al., 2016). The strategies in PFFP included finding foster and kinship families in children’s own neighborhoods, building community partnerships to link families with services, facilitated team meetings, and created tools to examine family outcome data (R. M. Chambers et al., 2016).
The intervention in Pine et al.’s (2009) study provided intensive, home-based services that were adapted to each individual family’s needs, including parent–child visitation, group classes, and family therapy. Each family was assigned an Masters-level social worker, a family support worker, a caseworker from the state agency, and a team leader from the program (Pine et al., 2009).
Study Designs and Comparison Groups
Nine of the 10 studies utilized a quasi-experimental design by comparing families that received the intervention to a matched comparison group (Boles et al., 2007; Brook & McDonald, 2007; Bruns et al., 2012; J. M. Chambers et al., 2019; R. M. Chambers et al., 2016; Chuang et al., 2012; Green et al., 2007; Pine et al., 2009; Thornton & Gwin, 2012). Only one study (Ryan et al., 2016) utilized an experimental design. Six studies (Brook & McDonald, 2007; Bruns et al., 2012; Chuang et al., 2012; Green et al., 2007; Pine et al., 2009; Thornton & Gwin, 2012) utilized a matched sample from the same jurisdiction—either by state or county, along with other matched characteristics. Cases in each of the quasi-experimental studies except one (Thornton & Gwin, 2012) were selected based on child age, race and ethnicity, parental substance use, and time of placement in foster care. The comparison group in Thornton and Gwin’s (2012) study consisted of statewide average reentry rates for families that had reunified during the same time frame as their study. However, in this study, cases were not matched to reduce selection bias, and no other characteristics of the comparison group were reported.
Only one study (Ryan et al., 2016) randomly assigned families to the intervention or comparison group. In their study, a total of 511 mothers were randomly assigned to the control group, while 1,112 families were randomly assigned to the recovery coach intervention.
Risk of Bias Across Studies
In accordance with the PRISMA-P checklist, the results from the risk of bias assessment are presented in Figure 2. This assessment examined different domains of risk that could potentially impact the quality of the findings as well as the interpretability and generalizability of them.
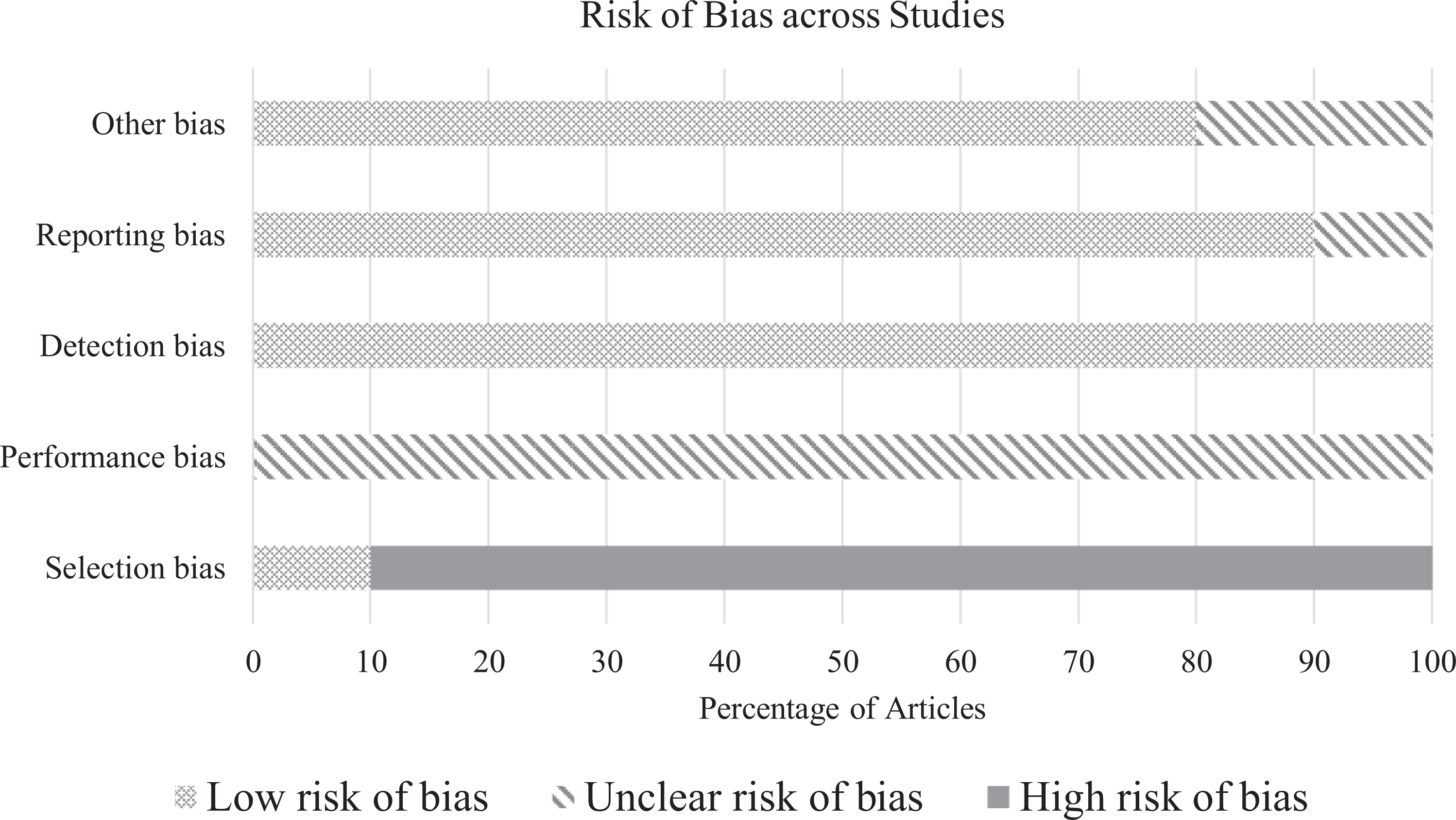
Risk of bias across studies.
Overall, the articles included had the highest levels of risk of bias in the domains of selection and performance. Randomized control trials have been difficult to execute in child welfare, and there are difficulties in carrying out research designs that satisfactorily examine the efficacy of interventions (Dixon et al., 2014; Mezey et al., 2015). The lack of controlled designs within the studies examined in this review is certainly evident in this review.
Discussion
This article systematically reviewed studies on interventions that could increase successful reunification of families involved in child welfare systems. Through the screening processes, a total of 10 studies that evaluated an intervention targeting successful reunification met all inclusion criteria and were coded and synthesized. Consistent with prior literature that has highlighted the need to view reunification as an ongoing, long-term process (Wulczyn, 2004), the majority of the studies included an intervention focused on reunification as the final outcome instead of targeting successful reunification via long-term work with the families. Four of the 10 studies showed consistently higher rates of successful reunification among participants than the comparison groups. Notably, all of these studies provided coordination or partnerships with other systems, such as the legal system (Chuang et al., 2012; Thornton & Gwin, 2012), substance use rehabilitation (Chuang et al., 2012; Ryan et al., 2016), or community partnerships (R. M. Chambers et al., 2016). Therefore, there are multiple interventions that focus on collaboration among community partners to increase family support post-reunification. This coincides with prior literature that highlighted the need to integrate service systems (Marsh et al., 2006), build community and interagency partnerships (Spath et al., 2008), and engage interdisciplinary professionals (Rolock et al., 2015).
For social work practitioners, the positive statistical findings in some of these articles, such as the increased rates of successful reunification with recovery coaches (Ryan et al., 2016) and with specific models of Family Drug Treatment Courts (Chuang et al., 2012), could help guide practitioners to implement interventions supported by evidence. Furthermore, these findings highlight the importance of cross-system collaboration and engaging key system partners, such as judges, lawyers, and other service providers, such as the Family Drug Treatment Courts (Chuang et al., 2012).
Furthermore, as the Families First Prevention Services Act of 2018 is implemented, local child welfare systems will need to adopt agency policies that prioritize evidence-based services. In fact, child welfare agencies can utilize some funding through the Families First Prevention Services Act for services that reduce the likelihood of entry or reentry into foster care. Therefore, based on the findings from this review, interventions such as Recovery Coaches or Family Drug Treatment Courts might facilitate successful reunification and prevent recurrences of child maltreatment.
Yet, of the 10 studies, none evaluated the same type of intervention or implementation of the intervention. The variation in interventions and the fact that the effect sizes of individual studies were extremely small limits our confidence in the efficacy of the interventions studied. Four studies evaluated Family Drug Treatment Courts (Boles et al., 2007; Burns et al., 2012; Chuang et al., 2012; Green et al., 2007); the Family Drug Treatment Courts assessed were diverse in core components and implementation. For example, one assessed a parallel model, two assessed integrated models but each one offered varying services, and one did not specify what type of model was used. Therefore, it is difficult to synthesize or generalize the results of these studies. Overall, families in five of the interventions: the PFFP model (R. M. Chambers et al., 2016); an integrated Family Drug Treatment Court (Chuang et al., 2012); an intensive reunification intervention (Pine et al., 2009); the recovery coach intervention (Ryan et al., 2016); and enhanced legal representation (Thornton & Gwin, 2012), rates of subsequent contact with child protective services were lower than the comparison groups. In contrast, for families in the other three Family Drug Treatment Court models (Boles et al., 2007; Bruns et al., 2012; Green et al., 2007), rates of subsequent contact with child protective services were the same among intervention and comparison groups. In a study of the Parent Partner Approach, reentry rates were lower among the intervention group for the first 12 months post-reunification, but these differences disappeared by 24 months post-reunification (J. M. Chambers et al., 2019). The final study (Brook & McDonald, 2007) found that families in the intervention group had higher rates of subsequent contact with child protective services than families in the comparison group.
Nonetheless, given the lack of replication of studies and overall small sample sizes, it is necessary to repeat these studies and compare findings across larger, more heterogeneous samples. Furthermore, selection bias in 9 of the 10 studies highlights a need for continued randomized controlled trials and more research to increase the evidence base for interventions in child welfare settings. Also important to the findings is the fact that none of the research studies included families with infants and young children. Given the increase in the proportion of infants and young children entering child welfare systems across the United States, the particular vulnerability of this age-group (Perry, 2009) and the added challenges families might face when reunifying with children who have never lived with them before, there is a need for evaluations of interventions that target these families.
In addition to child age, diverse populations are limited in these studies. All four studies that evaluated family drug courts were predominantly White and female, highlighting the need to further study these interventions to determine how best to target and adapt interventions based on the sociodemographic characteristics and needs of families that they serve. Only one study, for example, the enhanced legal representation study, served urban families who were almost entirely single female-headed African American households (Thornton & Gwin, 2012). Therefore, it is important in future studies to examine the impact of this program on other populations, such as rural families, or other families of color.
In addition, none of the interventions from the included studies have been truly replicated, which limits our ability to generalize findings. Despite four different studies that evaluated Family Drug Treatment Courts, for example, each one used a different model and diverse sample. Furthermore, the studies included did not mention model fidelity, which could help researchers identify the core components of the intervention to replicate and evaluate in other settings. In addition, only one of the studies (Ryan et al., 2016) utilized an experimental design. Moreover, lack of detail about the sample involved or the use of nonequivalent groups further limits the generalizability of these findings.
Limitations
Although this study adds to our understanding of how to support families to foster successful reunification, there are several limitations that should be acknowledged. First, the relative lack of randomized controlled trials in child welfare settings has limited our ability to attribute positive outcomes solely to participation in the intervention. Second, our conceptualization of successful reunification was based on re-referrals or reentries into care. Since administrative data were used in most studies, it is possible that re-referrals or reentries were underreported, either because children reentered care in a different county or state from where they were discharged originally, or because the follow-up time was not enough to capture subsequent contact with child protective services that might occur 12 months, 18 months, or even further after the physical reunification. Furthermore, there could be other measures that could capture well-being for reunified families; the lack of referrals or reentries into foster care does not necessarily mean that children and families are not experiencing challenges or stressors that impact well-being. In parallel, some of the outcomes in the studies included in this systematic review, such as placement changes after reunification, may be due to factors unrelated to the family risk factors targeted by the intervention. In addition to these limitations, our decision to include only studies that utilized an experimental or quasi-experimental design may limit the type of findings and measures reported and the overall number of available articles, given the overall lack of utilization of experimental designs in child welfare. Furthermore, only one of the studies included in this review (R. M. Chambers et al., 2016) assessed fidelity measures; therefore, future studies could include measures of fidelity in addition to outcome measures. Finally, given the differences among samples and interventions, it is difficult to generalize results to larger child welfare populations. Despite the limitations noted above, this review can help guide future directions in practice, policy, and research based on the findings, overview, and critique of the prior empirical evidence.
Conclusion
The results of this systematic review fill a gap concerning a review of intervention studies on family reunification within child welfare practice. The limitations in studies preclude any definite conclusions about the effectiveness of interventions that have been studied. This review also sheds light on gaps and dimensions of successful reunification that remain understudied. There are several implications for future research from this study. First, there is a need to design, implement, and evaluate interventions that are developmentally sensitive. Prior studies on reunification have argued that families with young children and this age-group have specific vulnerabilities to inconsistent care. Yet, none of the interventions in this review targeted families with infants and young children. Furthermore, with the Families First Prevention Services Act, it is necessary to replicate studies and utilize more rigorous designs, such as randomized controlled trials, to build evidence-based practice in child welfare. Notably, of the 10 studies that measured successful reunification in this systematic review, only one utilized an experimental design. Indeed, child welfare agencies will have to evaluate the interventions they implement more rigorously to comply with the Families First Prevention Services Act. Finally, as interventions are implemented, fidelity should also be assessed so that interventions that have positive findings, such as recovery coaches, can be implemented similarly in other agencies. As we continue to build our evidence base in child welfare, the findings from this systematic review can help us target interventions based on what has worked in the past, while adapting the interventions to family needs as those change over time.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.