
Abstract
The World Health Organization reports reveal that the average risk of dying from pregnancy-related causes in sub-Saharan Africa is about 1 in 45 compared to 1 in 5,400 in high-income countries. In Ethiopia, maternal mortality remains a tremendous problem. Several studies associate the high maternal mortality ratio to the widespread practice of home birth, household income, and lack of transportation. Absent from the findings of these studies is any discussion of the sociocultural contexts that might influence maternal health service utilization. Birthing bears cultural significance accompanied by rituals. Thus, any solution to maternal health problems must consider the sociocultural and grassroots context. It is important to learn the needs and priorities of the mothers who are targets of maternal health policies. Using Indigenous approaches, this study examines the gaps in Ethiopian maternal health policies and programs. The study also identifies culturally relevant solutions that address the needs of communities.
A child’s well-being begins with the health of the child’s mother. Women as mothers are life-givers as well as pillars of society and bearers of cultures (Tinker, 1991; Walker, 1995). Hence, a mother’s health and well-being become significant to the development and maintenance of the community and the development of prospective future generations (Akujobi, 2011; Walker, 1995).
Maternal and child health appeared at the forefront of public health concerns in 1987 when the World Bank, the World Health Organization (WHO), and the United Nations (UN) Population Fund jointly launched the Safe Motherhood Initiative (Mahler, 1987; Potts & Hemmerling, 2006). The Initiative’s goal was to reduce maternal mortality and morbidity by at least half by the year 2000. The goal was not met (Potts & Hemmerling, 2006), and so, improving maternal health was incorporated in Millennium Development Goals (MDGs) as MDG 5, where the target became a 75% reduction in maternal mortality by the end of 2015. Again, the target was missed (Easterly, 2005; Midgley, 2008). Data from WHO (2019) showed that the global maternal mortality ratio (MMR, number of maternal deaths per 100,000 live births) dropped by about 38% between 2000 and 2017. Currently, maternal health is part of Sustainable Development Goals (SDGs) 3—good health and well-being along with child health, malaria, and HIV/AIDS, among others. This goal aims to reduce the global MMR to less than 70 per 100,000 live births by 2030.
Despite international efforts to reduce maternal mortality, the risk of dying from a maternal-related cause for women in developing low-income countries remains high. Reports of the WHO (2019) reveal that the average risk of dying from pregnancy-related causes in sub-Saharan Africa is about 1 in 45 compared to 1 in 5,400 in high-income countries.
This study examines the gaps in maternal health policies and their implementation at the grassroots. The study also sets forth workable strategies and recommendations that might be used to establish culturally relevant maternal health policies and programs that address the needs of communities using Indigenous approaches.
Maternal Mortality in Ethiopia: A Brief Background
Maternal mortality remains one of the biggest challenges in Ethiopia. The WHO defined maternal mortality as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of pregnancy, from any cause related to or aggravated by pregnancy or its management, but not from accidental or incidental causes.
Several studies (Amin et al., 2010; Chandrasekhar et al., 2011; Karim et al., 2010; Osubor et al., 2006) associate the high MMR to the widespread practice of home birth without skilled birth attendants. These studies analyzed the geographic, socioeconomic, and contextual factors impacting the utilization of maternal health services. Among these factors, women’s autonomy (Woldemicael & Tenkorang, 2010), household income (Amin et al., 2010; Chandrasekhar et al., 2011), distance from health facilities and transportation (Karim et al., 2010; Okojie, 1994), residence in rural versus urban settings (Nigussie et al., 2004), cost of maternal health services (Osubor et al., 2006), and access to radio (Karim et al., 2010) appeared to have the largest impact. Woldemicael and Tenkorang (2010) measured women’s autonomy using women’s freedom of mobility, control over household resources, ability to make decisions on household purchases, freedom from domestic violence, and participation in child-related decisions. But absent from the findings of these studies is any discussion of the sociocultural contexts that might influence health service utilization.
As part of MDG 5, the Ethiopian Ministry of Health trained and deployed female Health Extension Workers (HEWs) to reduce maternal mortality through increasing the prevalence of facility-based delivery. While HEWs have succeeded in providing preventive health services (Datiko & Lindtjørn, 2009; Teklehaimanot & Teklehaimanot, 2013; Wakabi, 2008, 2010), their efficacy in promoting facility-based delivery remains questionable. To date, only 10% of births occur in health facilities assisted by trained professionals (Demographic Health Survey, 2010, 2011). Critics of international policies (Midgley, 2008; Muchhala & Sengupta, 2014; Saith, 2006; Sumner & Tiwari, 2009) argue that the MDGs and SDGs cannot sustainably eradicate maternal health challenges. They reject the policies as prohibitively expensive and imposed on countries by the UN without adequate contextual analysis.
Any solution to current maternal health problems must take into account the social context in which the care is rendered. For most, if not all, ethnic groups in Ethiopia, the process of birthing (i.e., pregnancy, birth, and postpartum) bears cultural significance accompanied by rituals and traditional practices. To fully understand these practices, it is important to go back to the individual communities and learn the needs and priorities of the mothers who are targets of maternal health policies (Gray & Coates, 2010; Gray et al., 2008; Sheehan, 2011). These women, rather than policy experts, are best suited to explain their sociocultural and economic contexts and clearly identify the gaps in maternal health care to bring about change.
Method
Indigenous research approaches were utilized to explore gaps in maternal health services in Ethiopia from the grassroots perspective. Indigenous approaches require participant-level engagement and acceptance of autonomy of the grassroots as research collaborators (Denzin & Lincoln, 2000; Ibrahima & Mattaini, 2019; Matsinhe, 2007; Nicholls, 2009; Sheehan, 2011, Smith, 2012). Indigenous approaches informed the research questions, recruitment of research participants, data collection and analysis, and member checks.
Study Setting
The study occurred in North Wollo Zone, Ethiopia. North Wollo is one of the 67 zones in Ethiopia and one of the 10 zones of the Amhara Region located in Northern Ethiopia. The researcher picked North Wollo due to her prior relationship with the community and the culture. Having a personal connection and work experience in these communities provided an opportunity to acknowledge Indigenous knowledge and apply Indigenous approaches in the research (Denzin & Lincoln, 2000).
The Health Sector Development Plan (HSDP IV—2010/11—2014/15) of Ethiopia introduced a three-tier health care delivery system that provides coordinated service using a referral system. Level 1 includes primary hospitals in woredas—district that covers from 60,000–100,000 people. The second level includes health centers that are serving from 15,000–25,000 people. The third level consists of health stations and health posts that are considered satellite health facilities serving 3,000–5,000 people. Accordingly, an assessment report by the WHO (2000) indicated that there are two hospitals, eight health centers, sixty-two health stations, and thirty-three health posts in North Wollo Zone. This zone is administratively divided into eight woredas (i.e., districts) with an estimated population of 1,500,303. Of the eight woredas, the interviews were carried out in six—Habru, Gubalafto, Meket, Gidan, Raya Kobo, and Lasta—due to time and budget constraint.
Recruitment
Gatekeepers were used to identify potential research participants. In qualitative research, gatekeepers assist the researcher to gain access and develop trust with the community of study (Hatch, 2002; Kovach, 2010; Sheehan, 2011; Smith, 2012). Gatekeepers with different backgrounds—elders and community leaders, religious leaders, local government administrators, and community-based service providers—were used to ensure sufficient variation among research participants. Gatekeepers identified 30 women above age 18 residing in North Wollo Zone as potential research participants.
Data Collection
Interviews
Data were collected using in-depth, semistructured individual interviews. The interviews were audiotaped and lasted from 40 to 90 min. The interviews were conducted in Amharic, the native language used in North Wollo Zone. They took place at a convenient place and time based on the preference of the research collaborators. Interview settings included the participants’ homes, their yards, a classroom, an office, and under the shadow of a tree in a school compound. These locations ensured that interview settings were natural, safe, and comfortable for the participants.
Visual dialogue
Visual dialogue was used during the interview. Visual dialogue is a visual and interactive process used to investigate cultural, social, and environmental practices (Sheehan, 2011). Research participants were asked to express certain concepts through drawings or using natural settings as a metaphor or a symbol. The visual expressions were then photographed and documented. Using visual dialogues afforded more richness to the data and enhanced the research participants’ collaboration. It also gave research participants the space to create their own meanings in a relatable way that is natural to them.
Observation
Observation was used to understand research participants’ interpersonal relationships, their relationships with their environment, and how their environment affects their access and utilization of maternal health services. The observation was guided by an ‘observation log’ where the researcher marked the presence or absence of accessible roads, transportation (public transportation, cars, bicycles, motorbikes, animals), household energy supply and access to clean water (electricity, solar, gas, and/or biogas), means of communication (mobile phones, landlines, internet, fax, post offices), and public or private facilities (schools, hospitals, open market places, grocery stores, places of worship and rituals). The criteria were selected because they have direct or indirect impact on maternal health.
Data Analysis
All of the qualitative interview data were de-identified and transcribed verbatim in Amharic, their original language. The transcribed data were then imported into computer-based qualitative analysis software, ATLAS.ti (Version 7.5.11), to manage, sort, and code the data. Next, Miles et al. (2013) interactive model for analysis was employed. This model involves three concurrent flows of activities—data condensation, data display, and conclusion drawing/verification.
The first flow of data analysis started with coding the transcribed materials. A research assistant was involved in the coding process. The research assistant was from North Wollo Zone and knew the cultural contexts and nuances in the community. He also had an MA degree in economics and worked as a program director for an Indigenous nongovernmental organization (NGO). Before the research started, he completed the necessary training in human subject research, Indigenous methodologies, and qualitative research analysis, with emphasis on coding and the overall process.
The research assistant and the researcher discussed coding procedures and coded the first five interviews together. They separately coded the remaining data and compared their codes for purposes of uniformity. When coding differences arose, they discussed them and noted the difference. The codes were modified several times as interviews continued and common themes emerged. Similar codes and phrases were sorted under different families in ATLAS.ti, which were patterns and recurring themes in the narratives (Corbin & Strauss, 1990; Miles et al., 2013).
The second flow of activity is data display. Miles et al. (2013) proposed using matrices, graphs, charts, and networks. Therefore, in addition to the thick text descriptions, photographs were used to display the data.
The third stream of data analysis is drawing and verifying conclusions. The data analysis was grounded in the research questions and Indigenous Methodologies (Smith, 2012), while remaining open to unexpected results. Notes from the guided observation were used as a memo to enrich the analysis and capture visual nuances. Member check was used to verify the analysis, prevent misrepresentation, and increase local validity.
Sharing the analyzed data with the participants and having their input ensure that the researcher has accurately translated their viewpoints into data (Krefting, 1991). Circles were used for member checks. Circles are conducted under the simple rules that each person speaks in turn, holds authority for the time they speak, and reciprocates by speaking responsibly from self and not about others (Boyes-Watson, 2013; Sheehan, 2011). The primary data analysis was shared with eight research participants to ensure equity, accuracy, and accountability. Every participant commented on content as well as the presentation of the findings, influencing the (re)structuring of findings.
Results
Background of Research Collaborators—Demography
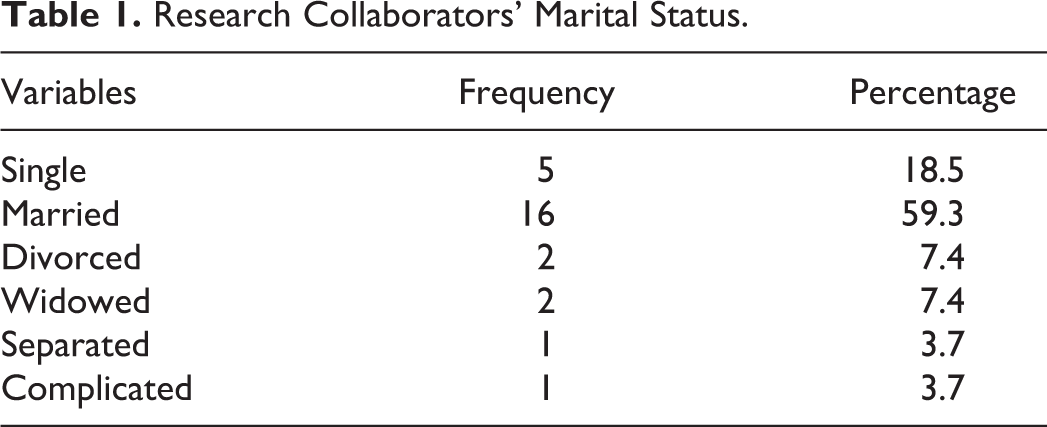
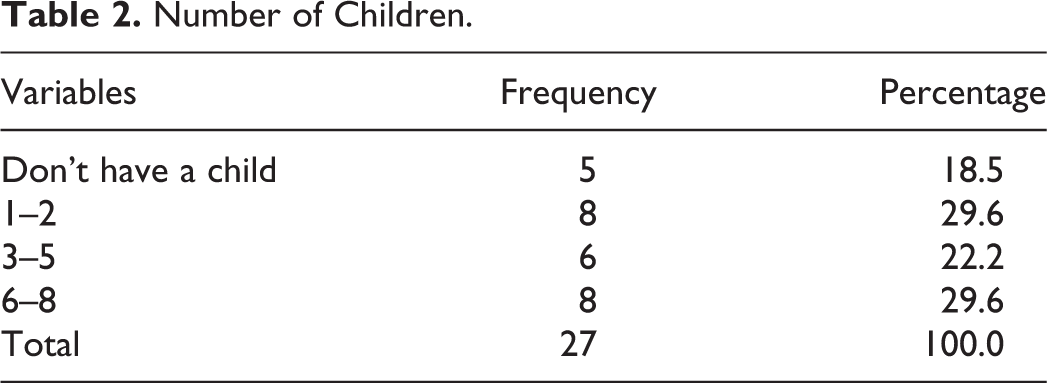
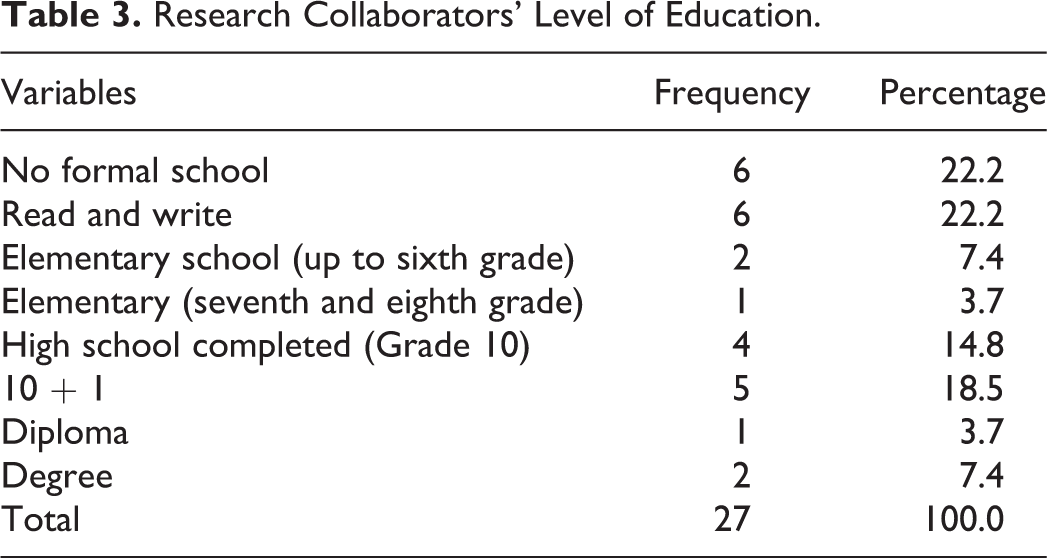
Twenty-seven of the 30 potential participants from diverse socioeconomic and educational backgrounds consented to take part in the research as research collaborators. Twenty-one of 27 (78%) were married once in their lifetime (see Table 1), and 22 had children (see Table 2). Twelve (44%) completed high school (Grade 10 in Ethiopian curriculum). Five were HEWs, one possessed a bachelor of science in nursing, two had management degrees, three only completed elementary school (sixth–eighth grade), and six had never been to school and could not read or write (see Table 3). Research participants took part in a variety of livelihood or professional backgrounds including farmers, small business owners, HEWs, community-based volunteers, traditional birth attendants (TBAs), Women’s Affairs Office representatives, and NGO program coordinators.
Research Collaborators’ Marital Status.
Number of Children.
Research Collaborators’ Level of Education.
Gaps in Maternal Health Care
Research collaborators discussed different services that are available within their communities. These services include traditional community–based care and policy-led, facility-based services. Community-based traditional services provide well-rounded support for mothers from pregnancy to delivery and postpartum (Aras) rendered by families and neighbors, TBAs, and community-based associations (including Kere or Idir, and Mahiber and Senbete). These services include minimizing the work expectations of expectant mothers during pregnancy, providing emotional and spiritual support during delivery, accompanying new mothers during birth, caring for newborn children, preparing food, and cleaning and managing households after delivery. The services are free, voluntary, and grounded in the traditional and spiritual values of the community rather than formal medical expertise. Describing her 36 years of service to mothers in her community as a TBA, one of the research collaborator said: I have delivered countless babies…. I helped deliver four twins, and 3 breeched babies. But thank God the mothers and the babies were ok. There was a day I helped four mothers in one day.…I even helped mothers deliver in hospitals. The doctor told the mother that she had more time and left. I was in the hospital accompanying my other neighbor. That girl [who was told its not time yet] begged me not to leave her there. So I stayed with her and she was in full labor—I helped her deliver in the waiting room! The baby was born before the doctor returned back from the delivery room.…Another time, my neighbor was going to church when she heard a noise and she found out that a woman is in labor so she called me. I went there and helped the woman who delivered on the side road. I used plastic bags instead of gloves because gloves are difficult to get. Then we took the mother and the baby to the hospital.…I never charged those mothers a nickel. Those who can afford to buy things will bring me gifts to show their gratitude.
After identifying maternal health services, research collaborators identified various gaps. These gaps can be categorized into five themes: (1) lack of resources in home delivery, (2) perception of birth and death, (3) spiritual indications, (4) access to health facilities, and (5) obstructions in health facilities and service delivery. Visual dialogues were also used to capture these gaps in maternal health services.
Lack of resources in home delivery
Most of the gaps identified in community-based care are related to TBAs’ lack of medical training, knowledge, and skill regarding identification and management of complications during delivery, such as eclampsia, hemorrhage, breeched birth, retained placenta, and/or prolapsed uterus. If these complications occur, TBAs are only capable of providing emotional and spiritual support. As a participant stated: I don’t like homebirth. I have experienced it. I have a bleeding problem and it is not easy to clean up after delivery…. But in health centers, it is clean. Moreover, mothers could face complications if they give birth at home. The baby could be breeched, they may suffer from hemorrhaging, fistula could happen, and the child could be suffocated. Motherhood is loaded with the unexpected.
Perception of birth and death
Research participants generally believed that God would protect them during home birth and that, if they died, their deaths were predetermined as opposed to preventable: Mothers strongly believe that they can give birth at home without any complication, with the support of God. And for most mothers, homebirth has no consequence. So nobody attributes harm or death to homebirth. And, if death is to happen, no one can stop it. Therefore, mothers prefer homebirth and the help of traditional birth attendants. “If you are meant to die, doctors cannot rescue you from death no matter how hard they try.”
Spiritual indications
Traditional beliefs and spirituality factored into mothers’ health service–seeking behavior and utilization. Some of the research collaborators stated that mothers reject routine care because such care would displease spirits that they believe possess them, as one collaborator said: “Some mothers do not want to get vaccination when they are pregnant because they assume injections are opposed to their ‘spirit’.” These beliefs were particularly prevalent in women from rural neighborhoods.
Access to health facilities
Research participants raised lack of routine access to health facilities as a major gap in maternal health care. Health posts in rural villages lack the resources to provide maternal health services, so they refer patients to the nearest health center. But health centers are located in major towns far from rural villages. Lack of access to transportation compounds this problem: The problem is that we don’t have health centers nearby. There is no place to go when we are sick. The health posts are doing their best but it is not enough. It is also very difficult to carry mothers who are in labor and walk on these hills [pointing at the hills] for 3-4 hours.
Obstructions in health facilities and service delivery
Research collaborators frequently expressed the lack of trust in the quality of service at health facilities because they perceived health care professionals to be incompetent and unprofessional. They frequently associated delivery at health facilities and hospitals with medical negligence and unnecessary C sections. Availability of care is also an obstacle to receiving facility-based care as 24/365 care is not expected from the medical community. Health posts and health centers are often closed during public holidays. And even when they are open, research participants confirmed there exists a shortage of medical supplies and skilled professionals.
Moreover, health facilities have stringent rules and regulations that conflict with the culture and traditions of the community. For instance, most health care professionals assisting with delivery in hospitals and health facilities are men. Nearly all of the research participants expressed fear of being nude in front of a man based on a culturally rooted belief that doing so is shameful: “nobody likes to be exposed in front of men, hence they prefer women.” Health facilities could be scary for mothers since women are afraid of being naked in front of stranger men [midwife and interns]. In addition, they always want their sister or mother to be with them in the labor room, but it is not allowed. Traditionally women never be left alone in a room while in labor, as it is believed they would be exposed to evil spirit. Moreover, birth is natural.
Supply Versus Demand: Visual Expressions
Research participants were asked to visually represent and compare the available supply of maternal health care services with the demand for such services using visual expressions—visual dialogue. Their expressions, set forth using various-sized rocks, stone beads, bottle caps, and household and farm tools, demonstrated a substantial discrepancy. Several research participants used rocks to represent supply and demand, with larger rocks representing demand and smaller ones representing supply. They explained that the smaller rocks represent that their needs were only partially met.
Conclusion: Recommendations and Implication to Social Work
The influence of cultural norms, traditions, and rituals on health service–seeking behavior in North Wollo Zone was evident in this study. However, as research collaborators identified, the national maternal health program does not account for cultural and traditional norms inextricably linked to birthing in the region. A primary example is that the overwhelming majority (more than 95%) of midwives and doctors in health facilities are male whereas, in traditional community practice, women serve as prayer leaders, birth attendants, and caregivers. Another traditional practice absent from facility-based care is the presence of family members in the delivery room.
The gender discrepancy among medical professionals is a reflection of nationwide shortcomings regarding women’s access to formal education. Free and universal access to primary school education is a recent phenomenon in Ethiopia. Increased access should eventually lead to increased numbers of women in health care professions and, in turn, alleviate some of the issues referenced above. The other major hurdle to access facility-based care is access and obstructions in health facilities and services. Lack of basic infrastructures such as roads, electricity, telephone, transportation, and clean water supplies has left many expecting mothers with a Hobson’s choice.
Recommendations
Maternal health requires holistic and culturally relevant interventions that focus on the economic, social, physical, mental, emotional, and spiritual well-being of mothers. In North Wollo, it is important to address basic structural needs including access to education, clean water, energy sources, and women’s economic independence as well as pre- and postnatal care and support. Accomplishing these goals requires addressing poverty, including TBAs in maternal health policies and enhancing resources and the quality of care at medical facilities.
Address poverty
The unspeakable impact of poverty was observed in every sector of development in the region, including health, education, and agriculture. While solutions to poverty are largely beyond the scope of this research, there is no doubt that poverty has a profound impact on maternal health in North Wollo. All research participants suggested providing economic support for mothers in the community by engaging them in income-generating activities, building their technical skills and financial literacy, augmenting women’s financial contribution to their households, and increasing women’s autonomy. Improvements in these areas would certainly lead to improvements in women’s lives as a whole, including maternal health.
Include TBAs
Research collaborators recommended training and building the traditional scientific and medical knowledge of TBAs because, aside from medical knowledge, TBAs have the requisite trust of mothers and skill set required to bring about change. Providing training to TBAs would be more efficacious than the current policy of attempting to replace them altogether with new “professionals” or “paraprofessionals” who lack the trust that TBAs have acquired through years of traditional practice. Indeed, encouraging medical professionals and TBAs to work together stands to benefit the mother, TBAs, and medical professionals alike. TBAs would benefit from the knowledge of medical professionals, medical professionals would benefit from the cultural and experiential knowledge of the TBAs as well as their relationships to mothers, and mothers would receive well-rounded, holistic care more consistent with their cultural beliefs.
Enhance resources
It is beyond debate that home birth is risky to mothers, particularly given the unpredictability of complications. But facility-based care has its own problems that must be addressed to become a more appealing option for expecting mothers. Facilities frequently have medical staff shortages as well as a lack of basic supplies like gloves, cleaning supplies, and medications. The research participants relayed a number of “horror stories,” well-known in their communities, that serve as cautionary tales against electing facility-based delivery. Accordingly, the community is unlikely to trust and abide by government mandates designed to force mothers to deliver in facilities, particularly when death is culturally perceived as an inescapable condition that women would rather face with their families at home.
Enhance quality of care
Research participants confirmed that enhancing the quality of care at health care facilities to increase utilization requires the creation of a welcoming environment capable of providing culturally component services. Any improvements to the availability of medical supplies and access to medical professionals must be accompanied by corresponding innovations driven by Indigenous practices, values, and cultural contexts. For example, developing birthing centers would likely be more attractive to mothers seeking to experience birth as a natural, rather than medical, phenomena. Such birthing centers should foster the role of TBAs as partners and invite family members to accompany mothers during delivery.
Limitations of the Study
This research is a qualitative study using observation and in-depth interview techniques for data collection informed and shaped by Indigenous research methodologies. Indigenous methodologies are culture and context specific. As noted at the outset, due to budgetary and time concerns, the research was not conducted in every possible location in the region. In addition, this study focused exclusively on North Wollo, which was purposefully selected due to the researcher’s prior relationship and familiarity with the area. The limited geographic region may limit the transferability of these findings to other contexts and/or participants.
Implications of the Study
This study has implications for social policy, social work research, and practice as it challenges the current top-down approach in policy development and program design through recognizing Indigenous knowledge and using Indigenous approaches. Indigenous approaches acknowledge that there is no standard policy and/or intervention program, which can be replicated everywhere and yield similar results (Smith, 2012). Hence, secular approaches that ignore these facts will not effectively address social problems that require culturally relevant interventions.
For countries like Ethiopia, it is important to reflect on the trends of policies, national strategies, and development programs that have been carried out under the UN framework. These global goals set the directions of development policies and provide monetary contributions to implement those policies. However, examining the socioeconomic and political dimensions in the development, ratification, and adaptation of international health and development policies and the power imbalance between the “developed” nations that provide loans and grants and the “developing” nations that need loans and grants to carry out health and development programs is obvious. In this structural reality, countries ratifying and/or adopting these policies, especially grassroots, have minimal or no say on the development of policies that influence their day-to-day livelihood. Understanding this context is the basis for understanding systemic oppressions and why barriers exist in the implementation of policies and programs.
Social work as a practice-based profession needs to challenge tailor-made Western theories and practice approaches. In postcolonial Africa, the struggle for ethnic, sociocultural, and political autonomy is real. Even if one can argue that Ethiopia was not colonized, the nation is highly influenced by Western neoliberal policies manifested through its economic and social policies. Therefore, decolonizing the formulation of socioeconomic policies, research processes, and intervention programs is important (Chilisa & Ntseane, 2010; Escárcega, 2010; Matsinhe, 2007). Decolonization is a process of decentering colonial discourse and power structures (Gray & Coats, 2010), which requires ethically and culturally acceptable approaches to the study of issues involving grassroots and criticizing the underlying assumptions, motivation, and values that are enacted with imperialism and colonialism (McCleland, 2011; Smith, 2012). This study reveals gaps in maternal health program planning, service provision, and service utilization. Thus, it can also be used to start conversations on reconciling maternal health needs in the community with international programs and interventions that are tailor-made to fit all.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.