
Abstract
Effectively responding to the problem of suicide requires an accurate understanding of which interventions are most helpful in given circumstances. This systematic review examined research on the degree to which motivational interviewing (MI; Miller & Rollnick, 2013) is effective in helping individuals suffering from suicidal ideation.
Individuals contemplating suicide struggle with painful emotions such as hopelessness, depression, anxiety, stigma, worthlessness, isolation, disappointment, and frustration (Ali & Gibson, 2019; Mok et al., 2016). Those considering suicide often view it as a method to end suffering, an escape from seemingly insurmountable life problems. Suffering brings people to contemplate suicide, and suicidal behavior results in agony for families, friends, and surrounding communities (Cerel et al., 2008). Suicide and suicidal ideation (SI) are far too common. Death by suicide is the 10th overall cause of death within the United States, the second leading cause of death among people ages 10–34, and the fourth among people ages 35–44 years (Centers for Disease Control [CDC], 2022). According to the CDC (2022) “In 2020, an estimated 12.2 million American adults seriously thought about suicide, 3.2 million planned a suicide attempt, and 1.2 million attempted suicide” (para. 3).
Considerable efforts have been made to understand suicide and its prevention. Strategies to prevent suicide include teaching coping and problem-solving skills, social outreach, psychotherapy, pharmacotherapy, hospitalization, means restriction, promoting social connections, shifting media communications about suicide, creating protective environments, increasing financial and housing stability, and others (CDC, 2022; Fox et al., 2020). Although suicide prevention and response efforts can theoretically take place in many contexts (e.g., schools, military, public announcements), short-term or triage care settings such as emergency departments or hospitals often encounter individuals at high risk for suicide. In response, short-term interventions have developed to both reduce immediate risk and promote follow-up with ongoing mental health care. Often, such strategies focus on helping individuals develop safety plans which may include ideas on what they can do to recognize warning signs, improve coping, reduce stress, improve social connection, reduce lethal means, and improve connections to mental health counselors (Doupnik et al., 2020).
A meta-analysis spanning 50 years of research on the treatment of self-injurious thoughts and behaviors (SITB) examined a wide range of SI interventions, including psychopharmacology, cognitive therapy, cognitive behavioral therapy, dialectical behavioral therapy, and other psychotherapies, safety planning, and inpatient hospitalization (Fox et al., 2020). The authors reported that across 1,125 unique randomized control trials (RCT), effects were small with no identified moderators across outcomes, participant characteristics, or intervention characteristics. They estimated that the advantage of intentional SITB interventions resulted in 9% advantage over control conditions (Fox et al., 2020). These authors noted that intervention effects did not increase across time despite increasing numbers of studies across time.
In a more nuanced meta-analysis of short-term interventions to prevent future suicide, Doupnik and colleagues (2020) found that such approaches were helpful in decreasing suicide risk and depression, but they did not reach the level of statistical significance—results similar to Fox and colleagues (2020). However, these short-term interventions did significantly increase the likelihood of follow-up mental health care which, based on the previously mentioned meta-analysis (Fox et al., 2020), may only be expected to create small effects.
MI (Miller & Rollnick, 2013) is both a treatment philosophy and a set of methods employed to help people increase their intrinsic motivation by exploring and resolving ambivalence about behavioral change (Lundahl & Burke, 2009). In the past few decades, MI has become a well-recognized brand that has been used in psychotherapy, medicine, addictions, public health, and beyond (Lundahl & Burke, 2009). Many healthcare providers who want to assist people to make important behavioral changes—such as reducing their alcohol intake or giving their suicide means (e.g., weapons) to someone else temporarily—assume that giving them knowledge is sufficient. In this vein, professionals may simply advise high-risk drinkers to lower their consumption or avoid situations in which they tend to drink, or they may direct a suicidal patient to call a hotline instead of acting on their thoughts when they are in crisis. However, more “seasoned practitioners realize that even superb advice often fails to yield behavior change” (Lundahl & Burke, 2009, p. 1233). Why? Because even clearly knowing what should be done is often not sufficient motivation to actually change. MI identifies four key processes to change: engagement with the provider, focusing on specific health behaviors to change, evoking a client's motivation for change, and evoking the client's plan for successfully realizing the change (Miller & Rollnick, 2013). That is, in addition to working to develop rapport, there is a focus on what to change, why change is important, and how to actualize change. In each process, a key MI tenet is to encourage the client to provide their own thoughts, known as evoking, along with ample amounts of reflecting and affirming clients’ thoughts to strengthen the client's resolve and commitment to change (Miller & Rollnick, 2013). A key assumption of MI is that knowledge and skill alone cannot overcome low motivation in producing behavioral change.
Motivation is thus essential to the change process, and such motivation is influenced by the therapist's interpersonal style (Norcross, 2002). In one classic study, the more the therapist confronted (e.g., “you’re an alcoholic”), the more the client drank a year later (Miller et al., 2001). MI instead views clients as the experts on their own life who can choose their own behavioral goals and reasons for such goals. MI therapists strive to promote a collaborative relationship with their clients based on empathy, which is part of what makes the treatment work (Miller & Rose, 2009).
In addition to this supportive relationship, MI adds a guiding component in which the therapist works toward specific goals of directly increasing individuals’ motivation to reduce an unhealthy behavior or increase healthy behavior. To do so, MI asks probing questions to encourage clients to discuss the gap between their unhealthy behaviors (e.g., binge drinking, parasuicidal actions) and their own short- and long-term goals (e.g., be a good partner or student, graduate from college, live a long life, etc.) in the hope that focusing on the discrepancy will motivate change. Similarly, MI encourages client speech that favors change—what is termed change talk (Amrhein et al., 2003)—which has emerged as a significant predictor of outcome (Magill et al., 2014). In other words, if you can help individuals verbalize why and how they might like to change their behavior, rather than nagging or telling them to do so, the probability of them changing is enhanced (Burke & Wrona, 2023).
A large and expanding number of controlled research studies (300+) of MI have demonstrated that, despite its typically brief duration (one or two sessions), it is significantly (10–20%) more effective than no treatment and at least as effective as other viable treatments for a wide variety of problems, ranging from substance use to reducing risky behaviors and increasing client engagement in treatment (Lundahl et al., 2010). MI works in a variety of formats, although it may work best as a prelude to other treatments, the way it was initially designed—to be followed typically by other behavioral interventions (Lundahl et al., 2010).
In this vein, MI has increasingly been recognized as a short-term intervention that may help in one-on-one suicide prevention efforts. Although not specifically designed to help individuals contemplating suicide, MI’s attention to value clarification, mobilizing motivation to change, lifting confidence, and promoting client engagement align with suicide prevention efforts such as asking individuals to shift behaviors contribute to suicide risk (Britton et al., 2020; Miller & Rollnick, 2013). For example, MI strategies might help motivate a person who is contemplating suicide to seek mental health counseling where they can work through issues related to the suicide risk. Alternatively, MI might prompt a person to examine the advantages of life, thereby strengthening their commitment to live. MI also focuses on helping people develop credible plans, such as a safety plan, that may lessen the risk of suicide. MI’s commitment to promoting engagement (e.g., nonjudgmental attitudes, emphasizing connection, highlighting autonomy) between the healthcare provider and the client can also be seen as a strength considering the stigma surrounding suicidality and mental illness.
Attempts to shift a person’s relationship to seeing their life as a life worth living differs from more ordinarily studied behavioral change efforts such as alcohol consumption, tobacco use, or the like (Britton et al., 2016). The question then becomes how well strategies and philosophies from MI transfer to the problem of suicide. A review of the literature on MI’s application to suicide prevention reveals three noteworthy trends. First, MI was often used to motivate individuals to pursue mental health treatment after being discharged from an emergency medical setting. Second, MI was seen as an approach that could respond to an individual's ambivalence about living. Here, the assumption is a person contemplating death by suicide is also contemplating living. Britton and colleagues (2008, 2011), borrowing from both MI and self-determination theory (SDT; Deci & Ryan, 2000), note the importance of how a professional engages ambivalence. Too much emphasis on one side of the ambivalent position, such as arguing for the client to choose life, may inadvertently encourage the individual to “balance” the ambivalence scale by arguing for death, which may inadvertently motivate the client to believe death by suicide is sensible.
The third notable trend was that MI was always connected to another intervention more proximally related to suicide prevention. For example, Britton and colleagues (2016) connected Means Restriction and MI. Means restriction involves removing easy access to lethal means, such as firearms, that could be used in a suicide effort. The rationale is that moments of suicide risk are often temporary and restricting access to a lethal means might prevent an impulsive lethal act. Britton and colleagues note that the decision to attempt suicide occurred within 1 hr in 75% of cases. Also, the preferred method to attempt suicide is connected to access convenience. Removing a lethal means or making accessibility more challenging would theoretically lower suicide attempts (Gvion et al., 2015). However, encouraging an adult to voluntarily shift their access to lethal means, such as their own firearm, requires motivation. Hence, MI is considered an approach that can help lift a person's motivation to voluntarily remove or restrict access to lethal means.
A key idea of annexing MI to other suicide prevention efforts is that, without motivation, clients are unlikely to engage in such efforts. Britton and colleagues (2008, 2011) argue that proven psychological interventions for reducing suicide risks, such as cognitive therapy and dialectical behavioral therapy, will not help clients if they do not attend treatment. MI has been put forth as an approach to increase the client's efficacy and motivation to actively utilize safety plans (e.g., Micol et al., 2022).
Several systematic reviews and meta-analyses have examined MI's impact in areas such as addiction, medicine, and mental health (e.g., Lundahl & Burke, 2009; Lundahl, Kunz, et al., 2010; Lundahl, Moleni, et al., 2013). Results from these studies suggest that MI is a valuable resource to healthcare providers because of its consistency in improving client or patient outcomes through promoting clients’ motivation to make behavioral changes. However, no known systematic review has been applied to understanding how MI may prevent suicide. Our study fills this gap. Specifically, this study reports on two research questions. First, What is the nature of MI-infused interventions applied to suicide prevention? Second, to what degree are such interventions effective?
Method
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) throughout. Meta-analysis statistics were computed using Comprehensive Meta-Analysis (Biostat, Inc, 2006–2022).
Inclusion Criteria
To be included, a study must have (a) applied some aspect of MI in isolation or with another intervention, (b) been directed toward a person currently identified as at risk for suicide (i.e., SI or suicidal behavior), (c) been published in a peer-reviewed journal or dissertation to promote study rigor homogeneity, (d) supplied sufficient data to calculate effect sizes, and (e) been published in English. Given the dearth of empirical studies in this area, no requirement was made for a study to include a comparison group.
Search Strategy
The search was conducted on September 9, 2021, and allowed for any study prior to this time. The following terms were inputted through EBSCOHOST: “suicide” AND TI (motivational interviewing or mi or motivational interview) OR AB (motivational interviewing or mi or motivational interview). TI = Title and AB = Abstract. The following databases were searched: APA PsycArticles, APA PsycINFO, CINAHL, CINAHL Complete, MEDLINE, MEDLINE Complete, Psychology and Behavioral Sciences Collection, and Social Work Abstracts. Reference lists of studies advanced to the full-text review were individually searched for relevant studies.
Covidence (2022) software was used to screen studies. In total, 147 studies were initially identified, though four were duplicates. Of these, 109 were screened out based on the title and abstract review. Thirty-four studies were submitted to a full-text review, of which nine were included (see Figure 1). All decisions to include or exclude an article were made by two coders; interrater reliability, proportionate agreement, was .86. Disagreements were resolved through reviewing decisions with the first author until consensus was achieved.
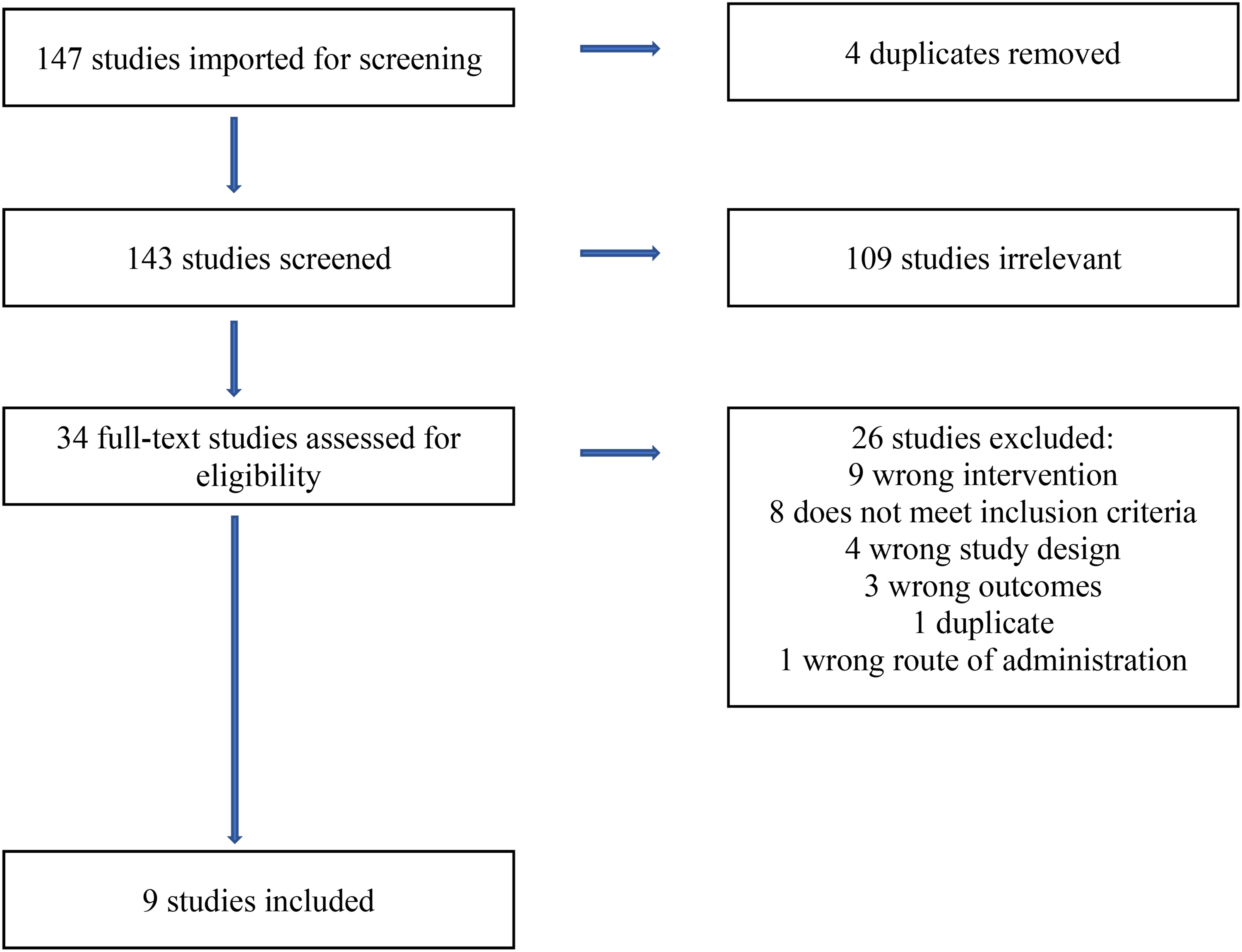
Covidence PRISMA.
Studies that had a similar focus that did not meet our exact criteria were excluded. For example, studies that measured the effect of brief interventions on suicide but did not explicitly mention the use of a MI protocol (e.g., Fleischmann et al., 2008) were excluded, as were studies of related outcomes such as overdose prevention or firearm safety that did not directly target SI (e.g., Anestis et al., 2021; Bohnert et al., 2016).
Coding Studies
Studies were coded for the following information: publication year, intervention setting (e.g., hospital, school), MI's role (i.e., stand-alone, integrated with another treatment), nature of control group, supervision provided, total time with provider, number of sessions with provider, provider's qualifications, delivery method (e.g., group, individual), number of participants, participants age, racial composition, location, and whether the study was a pilot or demonstration study. A common tension in syntheses research is deciding which outcomes to include given the research question of the systematic review crossed by both the variance in outcomes reported and the availability of information needed to calculate effect sizes in primary studies. This study examined how MI-infused interventions impacted the degree to which clients sought mental health care and other variables proximal to suicide. Not all variables reported in primary studies met these criteria. Interrater reliability across these studies and participant characteristics was .94.
A brief narrative overview of the nine included studies is provided prior to presenting meta-analytic findings.
Five of the nine studies were designed by the investigators as pilot studies, which often means that they are underpowered and not intended to provide high-quality data for significance testing. That said, consistent with the intent of systematic reviews to collect all available evidence, Thabane et al. (2010) recommend the inclusion of pilot studies in meta-analysis as long as methodologies are similar to other included studies, which is the case in our study.
Meta-Analysis
Comprehensive meta-analysis (CMA, Biostat, Inc, 2006–2022) was used to calculate and integrate effect sizes using a random effects model. Hedges’ g with confidence intervals are reported. Given the limited number of studies, only pooled effect sizes from three classes of dependent variables are reported (i.e., those with more than seven indicators): suicide attempts, suicide ideation, and follow-up with mental health care after treatment.
Results
The earliest identified study employing MI to prevent suicide was published in 2012 by Britton et al. Six of the remaining studies were published in 2018 or later, suggesting an emerging interest in MI's potential role in preventing suicide. Of the nine included quantitative studies, two were co-authored by P. Britton (Britton, Chapmam, et al., 2020; Britton, Maisto, et al., 2012) and four were co-authored by C. King or E. Czyz (Czyz et al., 2019; King, Eisenberg et al., 2015; King, Gipson, et al., 2015; Pfeiffer et al., 2019). All studies blended MI with some other form of suicide prevention intervention and were delivered individually. Eight of the nine studies took place within a hospital setting, whereas one was conducted on a college campus (King, Eisenberg, et al., 2015). Three studies (King, Gipson, et al., 2015; McManama O’Brien et al., 2018; Sedghy et al., 2020) did not supply information about the use of a MI training manual, whereas six reported that a manual was used. Of the studies that used a manual, all reported utilizing some form of monitoring or supervision to promote adherence. On average, the amount of time spent with a client was 141 min (SD = 106) across an average of 2.64 (SD = 1,54 sessions, once an outlier (six meetings; Pfeiffer et al., 2019) was removed. Seven of the nine studies utilized a mental health professional to deliver MI; one utilized a nurse (Sedghy et al., 2020), and one utilized paraprofessionals (Pfeiffer et al., 2019). These studies measured a range of outcomes related to suicidality, such as SI, suicide attempts, and treatment-seeking behavior.
With the exception of one study that did not use a control group (Britton et al., 2012), all others used some form of randomized assignment to an MI-infused treatment or a treatment as usual (TAU) condition. On average, there were 31.33 (SD = 20.1) participants per study within treatment groups and 35.45 (SD = 19.2) in control conditions. Overall, there were 282 participants in MI-infused conditions. Across all studies, the average percentage of females was 55.37 (SD = 31.1) in the treatment groups and 59.4 (SD = 24.2) in the control groups. The average age was 26.7 (SD = 12.8) for those in the treatment conditions and 23.1 (SD = 8.5) in the control conditions. All but one study (Sedghy et al., 2020) reported on the ethnicity of participants, although uneven in their specificity. On average, 68.4% of participants were White (SD = 15.9), 19.2% were Black (SD = 21.5), 14.5% were Latin/Hispanic (SD = 1.9), 9.8% were Asian (SD = 12.6), 2.3% were Pacific Islander (SD = 0.6), and 2.0% were Native American/Alaskan Native (SD = 0.8). All studies originated within the United States, except for one (Sedghy et al., 2020), which was conducted in Iran. See Table 1 for information on the exact number of participants per condition.
Effect Sizes (Hedges’ g, Random Effect Model) at Short- and Longer-Term Follow-Up Periods.

Notes. *p < .05 **p < .01.
Combined immediate and 60 day follow-up. 2Suicide Ideation and Free of Suicide ideation. 3Combined 3- and 6-month follow-up. 4Present, duration, and frequency of SI. 5Readiness to seek treatment. 6Efficacy, Use, Readiness, Intention. 7Depression. 8PH-9. 9(Increased: Hope, emotional support, friendship. Decreased: loneliness, stigma). 10No control group, pre–post effects only.
Narrative Overviews of Included Studies
Given the limited number of studies examining this important topic, brief narrative overviews of each study are provided prior to presenting meta-analytic findings.
Britton et al. (2012). Designated as a pilot study. Participants. Military veterans in a psychiatric care hospital are admitted due to SI or attempts. MI's Role + Intervention. Authors developed “MI-SI,” which is motivational interviewing for suicidal ideation. The authors hypothesized that suicide represents an internal struggle to live or die, a form of ambivalence. MI was used to “resolve” ambivalence toward choosing to live and engage in life-enhancing activities. That is, Change Talk (MI's term for motivational speech) was named “Living Talk” and included reasons the client wanted to live, whereas “sustain talk” would be the client's reasons to die. Clinicians also engaged in problem-solving and safety planning. In addition to routine care, participants in the intervention group received two 50-min MI sessions prior to being discharged. Comparison Group. No comparison group was used. Measured Indicators of Suicide Risk. Suicidal ideation. Results. Across both time periods, results followed expectations where the risk for suicide went down significantly. Without the benefit of a comparison group, however, it is impossible to isolate the unique impact of MI relative to other treatment inputs.
King, Eisenberg et al. (2015). Designated as a pilot study. Participants. Compared to all other studies, participants in this study were not assessed at a hospital. Rather, university students were recruited if they reported elevated risk suicide factors from a broadly disseminated online mental health screening. MI's Role and Intervention. In an innovative program, ebridge, MI provided students with personal feedback related to online screening results regarding suicide risk. The feedback involved engaging common MI skills such as emphasizing choice about seeking counseling, use of permission questions, offering affirmations, gathering information through open-ended questions, and routinely offering reflections. A motivational ruler was utilized to both assess students’ readiness to change and to evoke change talk. Compared to the control group, those in the ebridge program had access to online counseling that was asynchronous and encouraged students to follow up with counseling. Comparison Group. After completing the online screening, those in the control group could receive feedback on their relative risk for harm and information about mental health resources through an online portal; however, there was no option to connect with a human. Measured Indicators of Suicide Risk. Information on student's mental health, SI, readiness to seek help, perceived need for help, and meeting with a mental health professional. Results. Consistent with the study authors’ stated goal, at the 2-month follow-up, the students randomized to the eBridge group reported significantly higher readiness scores, particularly readiness to talk to family and friends about seeing a mental health professional, and readiness to see a mental health professional, and were more likely to have received mental health treatment during the 2-month study period. However, there was no discernible advantage for the intervention group in terms of mental health outcomes such as depression or alcohol use measures.
King, Gipson, et al. (2015). Participants. Forty-nine adolescents seen in an emergency department for nonpsychiatric problems who also screened positive for suicide risk or mental health problems. MI's Role and Intervention. The intervention group received MI-based (similar to motivational enhancement therapy, MET) feedback on screening tools that detected mental health risks. Further, they received a 35–45 min MI interview that encouraged an action plan that would help them overcome their mental health concerns. Comparison Group. After completing the screenings, these adolescents received information pamphlets about mental health concerns and phone numbers for crisis lines and community support. Measured Indicators of Suicide Risk. Depression, hopelessness, SI, and alcohol consumption. Results. While none of the results reached statistical significance, the authors noted that all measured outcomes had effect sizes that were at least in the small range with moderate effects for hope and large effects for depression.
McManama O’Brien et al. (2018). Designated as a pilot study. Participants. Adolescents receiving care at an inpatient psychiatric setting who reported both suicidal risk and alcohol consumption. MI's Role and Intervention. MI was used to promote a “teachable moment” by applying MI to both alcohol consumption and suicidality through the authors’ ASIST program (Alcohol and Suicide Intervention for Suicidal Teens). ASIST consists of a 60–90 min individual session and a 20–30 min session with the adolescent's family. Change talk efforts centered on reducing alcohol consumption and preventing suicide. Consistent with MET, adolescents were given personalized feedback on their relative alcohol consumption and risk to self-harm. Comparison Group. The comparison group received TAU. Measured Indicators of Suicide Risk. Alcohol consumption (not reported here), suicide ideation, and suicide attempts were assessed. Results. Suicide risk factors were not significantly different between the two groups at follow-up. Of interest, the authors reported no significant difference in SI after controlling for baseline levels of suicide. However, their data showed that, on some indicators, those in the treatment group benefited less than those in the TAU group of this pilot study.
Czyz et al. (2019). Designated as a pilot study. Sample. Teenagers psychiatrically hospitalized due to suicide risk. MI's Role and Intervention. The authors developed MI-SafeCope where MI was used to enhance safety planning (e.g., use of coping strategies during a crisis, recognizing suicide warning signs, connecting to support, reducing access to lethal means). Further, MI was used to increase teenagers’ motivation and efficacy in engaging safety planning strategies to prevent suicidal risk once outside of the psychiatric hospital. Treatment included sessions with teenagers, family members, and a post-discharge booster call. Comparison Group. Hospitalized teens received standard care including developing a safety plan. Measured Indicators of Suicide Risk. Nonstandardized indicators of self-efficacy to refrain from suicidal behavior, safety planning (use, readiness, intention), use of coping strategies, parents’ readiness to support their teenagers, and standardized measures of suicide ideation and attempts. Results. There were no statistically significant effects overall, except for parents reporting that they were more supportive toward their children in the MI-infused group versus the comparison group.
Grupp-Phelan et al. (2019). Participants. Adolescents taken to an emergency department who scored high on risk for suicide (i.e., they were not necessarily taken to the hospital due to suicidal behavior). MI's Role + Intervention. The authors developed the Suicidal Teens Accessing Treatment After an Emergency Department Visit (STAT-ED), which included aspects of MI, problem-solving, referral assistance, and case management. The target of MI was encouraging follow-up mental health care and problem-solving around reducing barriers to such care. Change Talk might have included language where the adolescent discussed the advantages of seeking care and how to overcome challenges to seeking mental health care. The protocol began after the adolescent was discharged from the hospital. Comparison Group. Adolescents in the TAU received a mental health evaluation and referral to a mental health provider. Measured Indicators of Suicide Risk. The authors examined the rate at which youth initially followed up with mental health care, the number of mental health appointments attended, time to mental health treatment post discharge, suicide attempts, SI, and a measure of depression. (Note: In our analyses below, we utilized parent reports only and not agency reports given the more proximal nature of such data). Results. In alignment with their goal of encouraging youth to attend mental health care, there was a statistically significant advantage for those in the treatment condition in the percentage of youth who attended therapy at 6 months and the number of sessions attended. No other variable was statistically significant.
Pfeiffer et al. (2019). Designated as a pilot study. Participants. Adults admitted to an inpatient psychiatric unit due to SI or a suicide attempt. MI's Role and Intervention. Peer specialists, individuals who had experienced mental illness previously, were trained in the PREVAIL program, which included several mental health modalities including MI. For up to 12 weeks post discharge, peer specialists met regularly (i.e., 2× per week for 2 weeks, then 1× per week for 6 weeks, then every other week) to promote hope, a sense of connection, and safety. The average number of sessions with a peer specialist was around six appointments of approximately 1 hr each. The aim was to reduce loneliness and promote engagement in life activities while assessing for suicide risk. MI principles were incorporated throughout to encourage positive engagement in life. Comparison Group. Participants in the treatment as the usual condition were discharged according to regular procedures. Measured Indicators of Suicide Risk. This was an open trial, so many instruments examined the acceptability of PREVAIL (none of which are reported in the present systematic review). Information was also gathered on suicide attempts, ideation, seeking mental health treatment, and reducing risk factors linked to suicide. Results. There were no statistically significant results.
Britton et al. (2020). Participants. Military veterans within an inpatient psychiatric unit due to SI or suicidal behavior. MI's Role and Intervention. Authors developed “MI-SI” (see above). Of interest, the authors reported that their study began before Miller and Rollnick’s (2013) book on MI was released, which suggested focusing more on the “health positive” side of ambivalence rather than a more neutral position wherein both sides of ambivalence are equally explored using techniques such as the decisional balance. Britton et al. revised their protocol so that therapists only focused on clients’ reasons to live, not their reasons to die through the decisional balance technique. They named this approach MI-SIR (revised). The authors used an RCT with a TAU and two treatment groups: MI-SI where the decisional balance was used and MI-SIR where the decisional balance was not used. Intervention participants received 1–2 MI sessions with a booster phone call approximately 1 month after discharge in addition to TAU. Comparison Group. TAU included psychiatric care and a safety plan at discharge. Measured Indicators of Suicide Risk. Three indicators of suicide risk were assessed: suicide attempts and suicidal ideation (strength of SI and being free of SI). Results. Across all indicators and all times, the overall effectiveness was not statistically significant though some statistically significant findings were reported.
Sedghy et al. (2020). Participants. The report from Sedghy and colleagues (2020) represents the only identified study from outside of the United States. Adults admitted to a hospital secondary to a suicide attempt participated in a MI enhanced discharge. MI's Role and Intervention. One week after discharge, participants received two MI sessions that focused on safety planning and seeking mental health services. Change talk targeted the impact of the suicidal attempt and reasons for living, as well as strengthening efficacy around utilizing a safety plan. Comparison Group. Those in the comparison group received TAU. Measured Indicators of Suicide Risk. Suicidal ideation, attempts, and engagement in mental health counseling were assessed. Results. All assessed indicators of risk were in the desired (MI) direction and statistically significant.
Meta-Analytic Findings
We now turn to the meta-analytic findings, with combined effect sizes when at least four studies contributed to an outcome. Note, effect sizes are reported such that those with positive values represent movement in a desired direction, whereas those with negative values represent an advantage for the control group. For example, a positive effect size in seeking treatment suggests more treatment-seeking behavior and a positive value in suicide attempt indicates fewer suicide attempts. Convention holds that an effect size around the “0.2” range is small, yet statistically significant, whereas effect sizes in the “0.5” and “0.8” are moderate and large, respectively (Cohen, 1988).
For suicide attempts across all time measurements and all studies, there was no statistically significant advantage for MI-infused programs, Hedges’ g = 0.1 (−0.2, 0.4), k = 7, z = 0.6, p = .5. Heterogeneity analysis suggested that this value was stable, I-squared = 7.3, p = .4. For SI, there was a nonsignificant overall effect for MI-infused programs, Hedges’ g = 0.2 (−0.1, 0.5), k = 18, z = 1.3, p = .2. Heterogeneity analysis suggested that this value was not stable, I-squared = 88.3, p < .001. However, moderator analyses were not pursued given the limited number of studies. Consistent with the other meta-analytic review on brief interventions targeting suicide (Doupnik et al., 2020), our analysis revealed that MI-infused interventions did significantly improve the likelihood that participants would follow up with mental health care, Hedges’ g = .4 (0.1, 0.6) k = 12, z = 3.0, p = .002. Heterogeneity analysis, however, suggested that this value was not stable, I-squared = 59.8, p < .01, but moderator analyses were not pursued given the limited number of studies. Table 1 provides the effect sizes grouped into related outcomes at two time points (0–2 months and 3–6 months). Only Czyz et al. (2019) reported on death by suicide post intervention; in this pilot study, none of the 17 youth in the TAU group died by suicide, whereas one of the 17 in the MI-infused intervention died by suicide.
We did conduct one moderator analysis across all studies and outcomes because over half of the studies were pilot studies, which could influence outcomes given their trial nature and tendency to be underpowered (see above narrative review). Across all 73 outcomes, there was no statistically significant difference between the 42 outcomes from pilot studies g = 0.2 (CI = 0.0, 0.4) and the 31 outcomes from non-pilot studies, g = 0.2 (CI = 0.1, 0.4), Qb = 0.0, p = .8.
In addition to quantitative results, a brief overview of authors’ reports is provided on how MI was included (see Table 2). Note that a deep understanding of what aspects of MI were used, emphasized, or omitted is necessarily limited given the nature of reporting in peer-reviewed journals and clinical work. That said, all studies reported efforts to enhance client motivation toward change through evoking change talk and most discussed the importance of developing plans. All studies noted the importance of engaging clients through identification of the “Spirit of MI” (e.g., acceptance, non-possessiveness). There was less clarity on how often efforts focused on lifting client's efficacy toward safety or how client ambivalence was addressed.
Aspects of Motivational Interviewing Present in Treatment.

Discussion
MI is being increasingly integrated into brief interventions designed to lower suicide risk, whether through attempting to shift a person's relationship to a life worth living, seeking mental healthcare, or utilizing safety planning strategies. For several reasons, the contribution of MI's ability to respond to the problem of suicide cannot yet be confidently understood given the current development of the literature. In part, because there was significant heterogeneity in the findings suggesting third variables may be important though not enough studies exist to conduct such moderator analysis. Further, MI was always infused with other interventions limiting an understanding of MI's unique impact on SI and related variables. That said, findings from our study are consistent with those of Doupnik et al. (2020), which could not yield definitive results regarding the benefits of brief interventions on proximal indicators of risk, namely suicide attempts and SI, whereas such interventions did result in increased connection to other providers. The MI-infused interventions did result in consistent improvements in increasing the likelihood of individuals seeking follow-up treatment. It is thus possible that the MI-infused interventions “did their job” in terms of connecting individuals to mental health providers who would then be in a better position to work on reducing suicide risk more systematically than via brief intervention.
MI has generally been applied to problems of behavioral excess (e.g., drinking too much alcohol, illicit drug use) or behavioral deficits (e.g., sedentary lifestyle, not following through with medical recommendations), with small to moderate effect sizes (mean d's around 0.3; Lundahl & Burke, 2009; Lundahl et al., 2013). Directing MI to the problem of suicide may require adjustments. A meta-analysis of suicide interventions that did not specify if MI was used showed a small effect in reducing SITB (Fox et al., 2020), which suggests that interventions can help those struggling with SI. All but one of the identified studies took place in a hospital setting where the duration of treatment is generally short-term, even though the individual is experiencing a mental health or existential crisis. The mindset of an individual in a hospital setting, such as an emergency room, may not be the ideal place to contemplate larger questions of living and dying given the constrictions of time providers are allowed to engage with patients. Even most safety planning efforts adopt a short-term focus on managing immediate risk factors rather than excavating reasons linked to a person's contemplation of suicide (e.g., depression, stress, loss).
The small and mainly pilot-based literature to date of MI-infused interventions for suicidality leaves us with much to investigate in future studies. For example, some studies herein reported on earlier versions of MI (pre-2013) that, based on current knowledge, would not be expected to work and were modified with a heavier focus on eliciting and amplifying change talk rather than providing equal attention to examining reasons for contemplating suicide. Furthermore, the target of the MI-infused treatments most often focused on seeking follow-up mental health care rather than addressing factors linked to SI which is problematic both theoretically and empirically in terms of understanding the degree to which MI can address suicide risk properly. For comparison, meta-analyses of cognitive behavioral thearpy (CBT) for suicide prevention found that interventions that do not focus on suicide do not reduce indicators of risk (Tarrier et al., 2008). Context heavily influences treatment goals and intervention delivery. Most of the included studies took place in short-term and triage-oriented settings, such as emergency departments and psychiatric hospitals, where a primary goal is to address immediate concerns and, where needed, refer to other providers to address non-emergency concerns. The literature on MI applied to the problem of suicide is still in its infancy and has not yet been designed to generate significant testing.
Accordingly, the most convincing outcome for the efficacy of a specific suicide prevention strategy would be a significant reduction in completed suicides within a certain follow-up period. However, given the low probability of future suicide even in high-risk groups, much larger samples than those reported herein would be required to obtain interpretable differences in suicide rates (Möller, 1989). As a result, researchers employ other outcome criteria, such as the frequency of suicidal attempts or ratings of mental health at follow-up (Möller, 1989). Future research must, therefore, clearly theorize on and elucidate the specific targets on which MI-infused strategies might operate, ranging from ambivalence about living or dying, SI, and suicidal intentions/attempts, to mental health status, readiness to seek help, and the likelihood of following up with a mental health visit.
Authors of the most CMA of interventions designed to reduce suicide risk hypothesized that “an intervention might employ persuasive techniques to convince the individual that the consequences of suicidal behavior are likely to be extremely negative rather than beneficial (e.g., surviving but being maimed or disabled; terrible effects on family and friends” (Fox et al., 2020, p. 1141). This hypothesis is consistent with the main goal of MI—promote motivation to change through helping clients become aware of discrepancies between deeply held values and certain behaviors, such as suicide. While results from our study do not empirically support this hypothesis, more research is certainly needed.
Several limitations need to be considered in interpreting our findings. First, only a few studies were identified, largely pilot studies, limiting both generalization of findings and the ability to detect nuances through moderator analyses. Second, the unique contribution of MI could not be isolated because all studies blended MI and other clinical approaches, such as safety planning or cognitive therapies. Combining therapeutic approaches is a common evolution in treatment, and efforts to analyze the cost–benefit ratio of deliberately engaging MI techniques require further investigation. From our findings, all questions about the utility of MI in relation to the problem of suicide must account for the integration of other interventions. Relatedly, it is impossible to ascertain the relative influence of MI in such intervention combinations or which aspects of MI were most helpful. Given the limited number of studies, risk of bias analyses wās not deemed appropriate leaving open the question of the generalizability of these findings. Lastly, the results from our study cannot be generalized to nonhospital settings, such as how MI-infused interventions function in routine health and mental healthcare settings.
In conclusion, MI-infused interventions promote follow-up mental health care for those identified to be at risk of suicide outside of existing mental health care. However, the positive benefits of such interventions did not reach to the important goal of reducing suicidal ideation or behavior. Given the high importance of this work, refinements of MI-infused approaches and further investigations are therefore strongly warranted.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.