
Abstract
Keywords
Social work needs interventions that are sustainable and that bring about lasting positive change. In addition to criteria related to objectives, outcomes, theory, and design, achieving such interventions requires ensuring that they are meaningful for intervention agents, for example, social workers, and responsive to their organizational characteristics (Holosko, 2016). The aim of this article is to describe how we are developing an intervention in Danish municipalities aimed at enhancing parental monitoring as a protective factor in family foster care. We hope that our efforts can serve as a guide for those embarking on a similar endeavor. The article is a contribution to the special issue on “Program Theory in Social Interventions Developed in Practice Settings.” It falls in the category “Primary research investigating the application of theory in interventions developed and used in practice settings,” and responds to the emerging policy interest in identifying ways in which practitioners may be better assisted in developing and choosing interventions to use in practice.
Our description is structured around the first two steps in intervention development described by Fraser et al. (2009). Woven into it are examples of how we combined top-down and bottom-up approaches to intervention development, whereby input from researchers, social workers and other stakeholders before and during the development process informed choices made along the way (Fraser & Galinsky, 2010). We begin with our problem theory, which identified a serious problem and potentially malleable protective factors to deal with it.
Problem Theory: Children in Care Lag Behind
Generally, placement of children in out-of-home care (OHC) is an acknowledgement by social welfare authorities of these children's need for care and support, which their biological (or adoptive) parents are unable to provide. Thus, placement in care is expected to compensate for inadequate care in the biological (or adoptive) home. However, most studies have found worse long-term outcomes for young adults who were placed in care compared to peers (Doyle Jr, 2007, 2008; Lindquist & Santavirta, 2014; Olsen et al., 2011; Vinnerljung et al., 2010; Warburton et al., 2014) regardless of outcome, choice of comparison peer group, methodological approach, or location of study. The causal long-term developmental effects of out-of-home care seem to be neutral at best (Doyle Jr, 2007, 2008; Goemans et al., 2015). The much higher prevalence of psychological problems among children in OHC compared to their majority population peers is well documented (Egelund & Lausten, 2009; Vinnerljung & Hjern, 2018), and research indicates that it is imperative for social service authorities to have valid and reliable knowledge of the mental health problems of children in their care.
The same applies to monitoring the academic skills and learning difficulties among children in OHC. For decades, research from many countries has consistently reported that children placed in OHC perform poorly at school and are at greater risk (compared to majority population peers) of entering adulthood with only compulsory school completed (Brännström et al., 2017, 2020; Forsman, 2020; Kääriälä et al., 2018). One explanation for these results is insufficient knowledge, in particular, more actionable knowledge, of the problems in foster children's lives, which limits social workers’ ability to fulfill their obligation to support and supervise foster parents. Such an explanation points to the need for an intervention that would enable social workers to effectively monitor foster children's psychological wellbeing and learning difficulties, identifying any problems as they occurred.
It is well-documented that social service authorities commonly lack systematic routines for provision of health and developmental services to children in OHC, and have over-reliance on foster carer observations (Ashton-Key & Jorge, 2003; Butler & Payne, 1997; Kaltner & Rissel, 2011; Kling et al., 2016b, 2016a; Randsalu & Laurell, 2018; Ward et al., 2002). Another problem is the over-reliance on semistructured qualitative clinical interviews to assess the child's developmental needs, which can lead to unreliable results. For example, in a comparison of the screening ability of routine “service-as-usual” assessment to that of standardized psychometric instruments among children in foster care, the latter indicated at least twice as many children with severe mental health difficulties (Jee, Conn et al., 2010; Jee et al., 2010, 2011). Similarly, Andershed and Andershed (2016) compared social worker “service-as-usual” assessments of adolescents with conduct problems to those made using a structured assessment instrument and found that the latter identified a greater number of research-based risk and protective factors. These findings suggest that using standardized screening and assessment instruments can help to identify more accurately a child's needs, which is at the core of our theory of change. These two problems—children in foster care are lagging behind and this is partly owing to poor monitoring of their wellbeing and development in care—define our problem theory and provided the rationale for developing the intervention, Me and My Foster Family: Improving the Lives of Foster Children (MOMP).
Developing an Intervention Following a Stepwise Model
We devised and developed MOMP in close collaboration with social workers and other stakeholders to enhance parental monitoring in Danish municipalities using as a guide the Fraser et al. (2009) theoretical five-step model of how to develop interventions (Fraser et al., 2009, see p. 70, Figure 4.1). These steps are: (1) specify problem and develop program theory; (2) create and revise program materials; (3) refine and confirm program components; (4) assess effectiveness in variety of settings and circumstances; and (5) disseminate findings and program materials. In this study, we focus on the first two steps of which we provide an overview in Table 1 with some examples of how we have operationalized them. Elements in the first step were, for example, developing a problem theory of risk and protective factors (“lack of actionable knowledge about children's problems”) and a program theory of malleable mediators (“monitoring children's development using reliable and valid screening tools”). Those in the second step included, for example, developing the draft proposal and submitting it for expert review, and specifying core program elements (e.g., “registering children's background data” and “regularly conducting screening”) and fidelity criteria (e.g., “screening responses from a minimum number of respondent types” to obtain a holistic view of the child).
The First Two Steps in Intervention Development.

Note. Adapted from Fraser et al. (2009).
The elements of each step and the numbering of steps in the model suggest a neat and steady progression. The reality, of course, was marked by a mixing of steps, overlaps and frequently revisiting elements. For example, the problem theory described above, and an embryo of the program theory were already present in the application for funding, which is part of step 2. The former has not changed dramatically since funding was secured, but the program theory underwent further specification while the theory of change was still being developed. This was because of an (bottom) up and (top) down process, which meant that instead of the linear path suggested by the five-step model, we embarked on what in hindsight is better described as a vigorous tango, going back and forth and in circles as we danced with different intervention agents and stakeholders. Chen and Garbe's (2011) distinction between bottom-up and top-down approaches to evaluation captures well our need—also recommended in the Fraser et al. (2009) stepwise model—for combining research-based knowledge on intervention design and standardized screening instruments with the need to be responsive to intervention agents’ interests and needs.
For example, the crystallization of “parental monitoring” as a core concept in our theory of change was gradual, a case of practice informing theory, based on periodic workshops, and dialogue and consultation with intervention agents. It started with a seemingly straightforward, almost banal, observation of the pressing need to provide effective solutions to the problems of children in care in our research application. This led to an acknowledgment of a pre-condition for doing so: being able to identify problems more accurately. It culminated with the realization that what we were embarking on was very similar to a term we encountered in some of the literature, “parental monitoring” (more on this below). This left the task of assessing how the term needed to be adapted to fit the ideas driving intervention development. This included answering the question, “Who are the parents?” Our original idea in the funding application was that social workers would carry out screening, do a holistic assessment of the child's needs based on the responses of the foster parents and teachers, and use it in their counseling. However, as Fraser et al. (2009, p. 5) point out, even a focused intervention may require a set of complex substrategies. This meant in our case that, despite employing the same digital platform for screening in all municipalities, we ended with several different ways of implementing parental monitoring to account for the considerable differences in the way municipalities organized screening.
Theory of Change: The Constructs of Parental Monitoring and Tripartite Parenthood
Following our problem theory, we now present our theory of change, introducing the constructs of “parental monitoring” and “tripartite parenthood.” Several terms are used in the literature to describe theories in interventions (see Rogers, 2008). In this article, the term “theory of change” refers to a description of how and why a desired change is expected to happen in a particular context.
“Parental monitoring” is a central construct in development and prevention research owing to its potential as a malleable risk or protective factor that could be targeted for intervention. Within behaviorally oriented interventions, monitoring is considered central to the behavior change process. Several interventions include parental monitoring strategies as a part of the training, for example, Multidimensional Treatment Foster Care and Keeping Foster Parents Trained and Supported (Leve et al., 2012).
The construct has been described using different terms such as “supervision,” “tracking,” and “structuring,” and both the use of these terms and operationalizations of the construct by researchers have varied depending on the age or developmental phase of the children being studied and the outcomes of interest. For example, parental monitoring has been described as “a set of correlated parenting behaviors involving attention to and tracking of the child's whereabouts, activities, and adaptations,” including “both structuring the child's home, school, and community environments, and tracking the child's behavior in those environments” (Dishion & McMahon, 1998, pp. 61, 65) and as “a multidimensional construct measuring parents’ control, supervision and actively sought knowledge about youth's whereabouts, relationships and activities but also youth's disclosures to their parents about these factors” (Cooley et al., 2021, p. 630). “Tracking” can refer to an awareness of the child's location and activity at a particular moment.
Depending on the developmental phase being studied, parental monitoring has been linked to a wide range of outcomes, both positive, such as self-esteem and academic achievement, and negative, such as accident and injury resulting from risky behavior, delinquency and substance abuse. In the specific context of foster care, parental monitoring has been found to be positively associated with lower rates of internalizing and externalizing behaviors. Further, higher parental monitoring was also associated with a more positive relationship between the youth and caregiver, as perceived by the former (Cooley et al., 2021). “Monitoring” in the context of MOMP refers to awareness and tracking of foster children in two areas, their psychological wellbeing and academic skills. By “tracking,” we mean to follow or observe. The next question is, who is to do the monitoring? To answer it, we introduce the construct of “tripartite parenthood.”
Parental Monitoring Under Danish Laws: Tripartite Parenthood
The term “parent” generally refers to a person who “brings up,” “raises,” or “takes care of” a child and, more specifically, a person who has the authority to make decisions concerning and affecting the care, welfare, and proper development of a child (Bullock et al., 2006). This definition implies that a child in foster care has three sets of carers or “parents”: (1) the child's biological parents, (2) the foster parents, and the municipal child welfare service, represented by (3) the social worker (see also Christiansen, 2011; Swedish National Board of Health and Welfare, 2020. This implication is far from obvious—perhaps not even to all the designated “parents,” in particular social workers—and has serious implications because of the issue of duties, obligations, and responsibilities it raises.
Responsibility for parenting in this “tripartite parenthood” (Swedish National Board of Health and Welfare, 2020) is unequally shared: the foster parents have the greatest responsibility for the day-to-day life of the child while the biological (or adoptive) parents have the least. To explain the model of tripartite parenthood we draw on three sets of Danish laws that impinge on parental rights and responsibilities: the Parental Responsibility Act, Consolidation Act on Social Services and the Law on Adult Responsibility (Schultz et al., 2021). To simplify, we refer to these collectively as “the law.”
Figure 1 shows two contexts that move together through time: the foster child's daily context and the social worker's municipal context. Within the former, two sets of parents, biological parents and, in particular, foster parents, are supposed to conduct their monitoring, keeping an eye on the child's activities and behavior, as all parents would be expected to do. The term “social worker” in a Danish context covers at least two kinds of personnel, foster family counselors and statutory caseworkers because some municipalities have chosen a division of labor whereby the former deal with foster parents’ concerns while the latter attend to the needs of the foster child and its biological parents. We will use the umbrella term “social worker” unless otherwise necessary, but it is important to note that this is a gross simplification as the use of both statutory case workers and foster family counselors complicates the task of parenting.
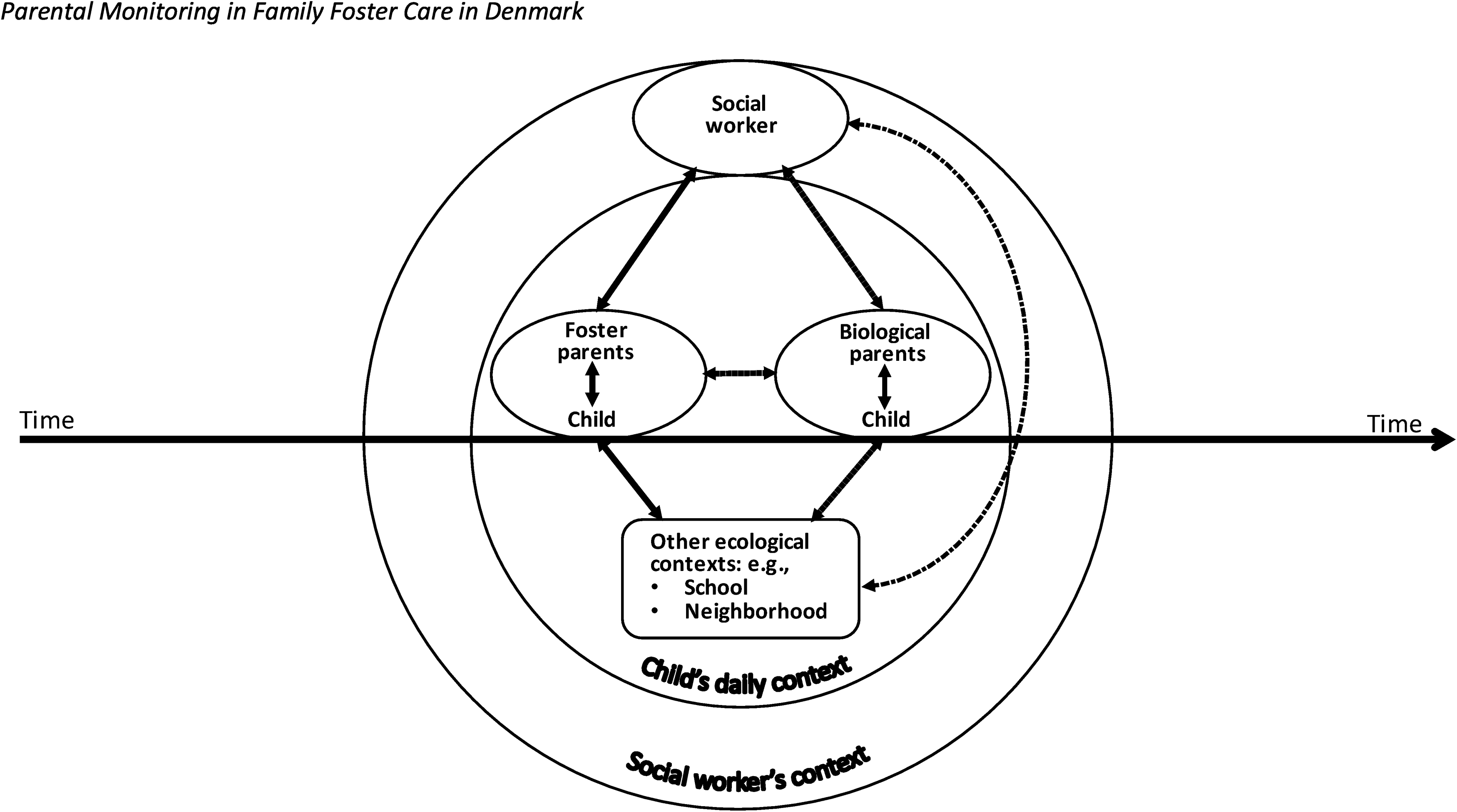
Parental monitoring in family foster care in Denmark.
Biological (or Adoptive) Parents
According to the law, the biological parents retain legal custody of the child and have right to supervized contact with their child and to be informed about their child's daily life by the municipality. Their relatively limited contact with the child and its ecological contexts (indicated by dashed arrows in Figure 1) limits the extent of their awareness of the child's development and needs.
Foster Parents
In contrast, the foster parents and municipality are responsible for all parental aspects of the child's daily life, including schooling and visits to the doctor. The discharge of these legal duties gives foster parents the greatest ability to observe the child by virtue of their greater contact with, and knowledge of, the child (indicated by bold, solid arrows in Figure 1). Yet, their ability to monitor the child's development can be inadequate for identifying the serious problems that foster children often have. This points to a need for improving the quality of monitoring, which in theory should be a logical way to effect a positive change for foster children.
Social Worker
The social worker, whom we designate as the third parent in the tripartite parenthood, is best placed to bring about this change by virtue of the authority and resources she commands as representative of the municipal child welfare authorities who have formal authority over, and responsibility for, the foster child, and who employ the foster parents to discharge this responsibility on their behalf (see also Bullock et al., 2006). We consider her a parent because her responsibilities include those of a parent, for example, speaking to the child about its needs, wishes, and wellbeing, assessing the child's developmental needs and documenting her professional assessments and decisions in the child's case book. In addition, she provides counseling to the foster parents and ensures that the two other parents in the tripartite model are discharging their duties in accordance with the law. Finally, any measures to help the child must be approved or sanctioned by her. It is, we argue, this responsibility as a parent that obligates the social worker to improve the monitoring of the child's development. Bullock et al. (2006) capture the essence of our point when they argue that the state has to parent children in care and that its major roles are to select substitute carers and coordinate the different aspects of the parenting and professional task.
At the same time, the social worker can perhaps best be described as a “superior standby parent” in the child's daily context. She is a “standby” parent because her contact with the child and foster parents is infrequent, typically every 6 months. The relative infrequency of the social worker's visits (e.g., in comparison it is ideally once a month in the United States) itself underscores the need for an intervention like MOMP. Further, anecdotal evidence suggested that the counseling provided by Danish social workers often suffered from a lack of reliable and actionable knowledge about the child's development and wellbeing (cf. Vinnerljung & Hjern, 2018). This knowledge gave impetus to the project in its infancy. MOMP transforms the twice-yearly visit into more of a structured observational period where the social worker is expected to collect standardized quantitative data on the child's wellbeing from multiple perspectives, interpret the results, use them to counsel the foster parents, and track change over time.
In Figure 1, the bold solid arrow from foster parents to the social worker indicates a relatively high monitoring interaction between them compared to that between social worker and the biological parents and the child's other contexts, for example, school, which are indicated with a dashed arrow. More generally, the law requires the municipal social authorities to continually undertake a systematic assessment of the child's development while the child is in care. However, the law does not use the term “parent,” with the moral and ethical obligations the term implies.
The foster parents are best placed to conduct parental monitoring in the everyday life of the foster child. However, of the three sets of parents, the social worker is the only one with the authority and resources to improve monitoring. The advice the social worker gives, concretely manifested in the child's care plan, is therefore based on mostly indirect monitoring, through the information provided by the adults caring for the child in different ecological contexts and periodic meetings with the child. Monitoring thus conceived works as a protective factor at the family level. In sum, building on the letter and spirit of the law, our theory of change conceptualizes the social worker as a member of the tripartite parenthood in family foster care, which obligates her to improve the monitoring of the child's development by harnessing her authority and resources to collect and analyze screening data, use it to counsel the foster parents and the foster child, and work with them to address any problems uncovered.
We operationalized the theory of change in collaboration with three municipalities, which varied widely in size and in geographical location. Mid-level managers, social workers, and family foster care consultants from the municipalities took part in discussions, interviews, observations, and workshops. Other stakeholders, organizations representing children in out of home care, parents of children in care, and foster parents, respectively, and state agencies such as the Danish National Board of Social Service participated in the latter as well.
While parental monitoring within tripartite parenthood is also conducted in treatment-as-usual, for the social worker it is typically plagued by the two problems noted above: over-reliance on foster carer observations and semistructured qualitative clinical interviews. Thus, our theory of change posits that change will occur through improved monitoring by the social worker using valid and reliable screening tools and drawing on responses not only from foster parents but also other carers and the child itself. This improved monitoring will increase the chances of appropriate measures to meet the child's needs.
Program Theory—Operationalizing the Theory of Change
Program theory operationalizes the theory of change into a theory of action. It is a way of developing an underlying model linking program inputs and activities to a chain of intended or observed outcomes (Rogers, 2008). The model specifies the malleable mediators as intermediate outcomes and then identifies the mechanisms of change needed to promote those outcomes (Fraser et al., 2009). As Table 2 shows, the direct target group in MOMP is social workers working with children in foster care. The indirect target group is the children in foster care fulfilling specific inclusion criteria and their foster parents. As a procedural intervention, MOMP enhances parental monitoring through two standardized measures for screening psychological wellbeing and academic skills that provide a brief and cost-effective way of determining if a foster child is in need of support or further assessment. Providing the social worker with valid and reliable measures enables the identification of problems as reported by the foster parents, biological parents, teachers or pedagogues, and the foster child (if above 11 years of age) or other carers if deemed necessary by the social worker. In this way the social worker can pinpoint where the problems lie, for example, in school but not in the foster home, and plan an intervention accordingly.
Overview of the MOMP Program Theory.
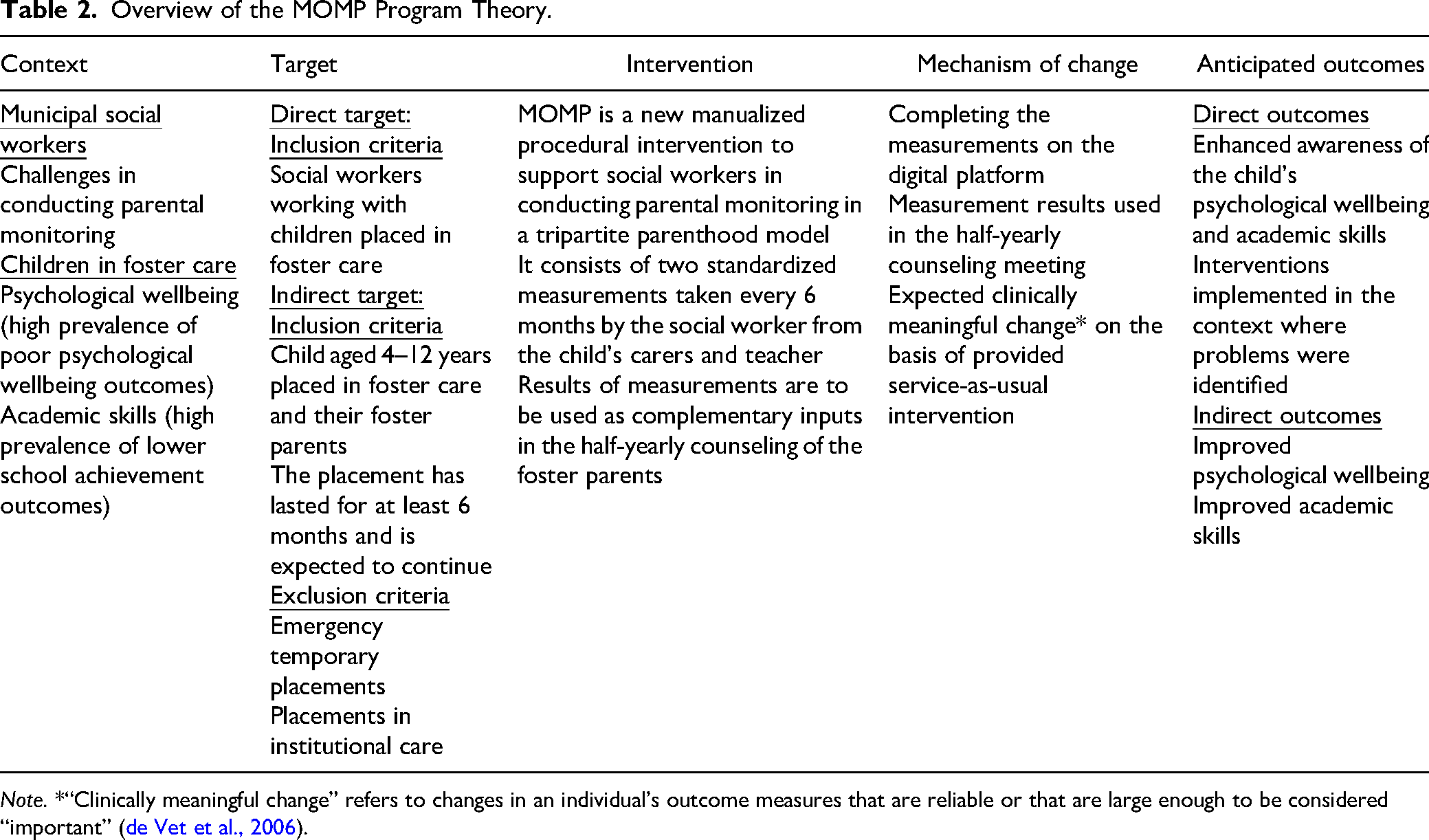
Note. *“Clinically meaningful change” refers to changes in an individual's outcome measures that are reliable or that are large enough to be considered “important” (de Vet et al., 2006).
The intended mechanism of change in a monitoring cycle is as follows: The child's carers answer the screening questionnaires about the child sent to them by the social worker via a digital platform→the social worker analyzes the data collected and discusses the results with the child's carers, leading to greater awareness of the child's wellbeing and its developmental needs→a service-as-usual intervention or further assessment is provided if necessary→the expected clinically meaningful change on each measure is assessed in the next round of monitoring and adjustments made accordingly. Planning MOMP activities around the half-yearly counseling meeting when the social worker in any case typically conducts her parental monitoring is a way to minimize increases in the social worker's workload. Next, we briefly describe the two standardized instruments used for monitoring, the digital platform for administering them, and how we trained social workers.
Standardized Instruments for Monitoring: SDQ and OBS-I
To monitor children's psychological wellbeing and academic skills and learning difficulties we searched for standardized measures that met the following requirements: They should have an official Danish version, be short, easy for a child's carers’ to self-administer and cheap, have a Danish reference group and ideally also have undergone relevant psychometric tests of reliability and validity in Denmark. For psychological wellbeing, the Strengths and Difficulties Questionnaire (SDQ) met these criteria, but the search for a corresponding measure of academic skills and learning difficulties proved fruitless. Therefore, we chose a subsection of a questionnaire with Danish norms, the Five-to-Fifteen (FTF) questionnaire (Lambek & Trillingsgaard, 2015) and named it “Attention to Learning” (OBS-I).
The SDQ (Goodman, 1997) is appropriate for 2-year-olds to 17-year-olds (though best validated for those 4 years old and above), so it is suitable for the children included in MOMP, who are in the age group from 4 to 12 years (http://sdq.dk/kort-om-sds/). Its psychometric properties have been tested (Baviskar et al., 2020; Niclasen et al., 2013; Niclasen et al., 2012), and Danish norm scores have been published (Arnfred et al., 2019).
Of the various SDQ versions available, we selected the double-sided version with impact supplement. All versions of the SDQ ask about 25 attributes, some positive and others negative, using a three-point response scale: not true, somewhat true, and certainly true. These 25 items are divided between five scales, each comprising five items: (1) emotional symptoms, (2) conduct problems, (3) hyperactivity/inattention, (4) peer relationship problems, and (5) prosocial behavior. The scores on the first four scales are summed to obtain a total difficulties score. The impact supplement has seven items measuring their impact on daily functioning and a slightly modified follow-up version with two additional questions for use after an intervention (www.sdqinfo.dk).
The same 25 items are included in questionnaires for completion by the parents or teachers of 4-year-olds to 16-year-olds. A slightly modified informant-rated version is used for the parents or nursery teachers. A self-report version is suitable for young people aged around 11 to 16 years, depending on their level of understanding and literacy. It asks about the same 25 traits, though the wording again is slightly different. The SDQ has generally been well-accepted by informants and is the only questionnaire of its kind that makes it possible to compare answers to the same questions across different respondents (http://sdq.dk/kort-om-sds/). This is a very useful property for social workers seeking to obtain a holistic view of the child. However, little was known about the clinical suitability of the instrument in social care, for example, whether all its subscales were equally reliable. Members of the project team addressed this lacuna via a systematic review (Bergström & Baviskar, 2021).
The OBS-I for 8-year-olds to 12-year-olds includes 29 items from the learning domain of the FTF questionnaire measuring reading/writing, math, general learning, and coping in learning with a three-point response scale very similar to that of the SDQ. The version for 5-year-olds to 7-year-olds includes 12 items from two domains, attention from the executive-functions domain and communication from the language domain. Further research needs to be conducted regarding the psychometric properties of the OBS-I.
Digital Platform for Data Collection and Analysis
A digital platform was needed to facilitate the administration of standardized instruments, collection and analysis of data, and registration of background information on the foster children, for example, whether they received special assistance in school or had undergone a psychiatric assessment. A privately operated digital platform was already in use in some Danish municipalities for collecting data on school pupils. While the extant infrastructure and developer's experience in collecting and storing data was an advantage for MOMP, the platform had to be adapted to the needs of the intervention. This required developing a new module to facilitate the integration of new screening questionnaires and enabling tracking the progress of each child using color-coded graphics. This was done in consultation with social workers, drawing on their input in workshops and think-aloud interviews.
The module facilitates data collection by providing a single user-friendly interface for registering each child and recording its background information, sending consent forms to biological parents, registering respondents for each foster child, sending them invitations, and information letters, receiving responses and displaying the results using, wherever possible, selected indicators of clinically meaningful change selected by the research team (Baviskar & Bergström, 2023). Step-by-step instructions were formulated for each of these procedures and improved through an iterative process drawing on experiences from training sessions and user feedback, and finally incorporated into the MOMP draft manual.
Several activities on the digital platform are used as program adherence criteria in the MOMP program theory and linked to direct and indirect outcomes (e.g., Collyer et al., 2020). These include registering the child's background information, collecting screening data before the half-yearly counseling meeting, and registering follow-up actions after the meeting.
In Denmark social workers usually do not use standardized screening instruments. Therefore, guidelines are provided in the MOMP manual on how to analyze and interpret the screening results and how to use them in counseling meetings with foster parents and child. The primary intent of the guidelines is to motivate the clinical curiosity of the social worker regarding the foster child's development and harness it to providing appropriate assistance to the child.
Training of Social Workers
As users of the digital platform, social workers in the three municipalities provided valuable input on adapting it to their needs. A general challenge in training social workers is that they are trained almost exclusively in the use of qualitative methods and have very limited experience with quantitative indicators or data (Taylor, 1990; Teater et al., 2017). Consequently, it was necessary to overcome unfamiliarity, and in some cases skepticism, among social workers regarding the use of the standardized measures in MOMP. To deal with these issues, several training sessions on how to collect and analyze screening data were conducted by the project leader and a psychologist from the MOMP team. Training was conducted using teaching material consisting of a step-by-step guide and worked-out examples developed for the purpose by the MOMP team. The training sessions were 4 to 7 h long depending on the municipalities’ needs. The number of social workers receiving training in each municipality also varied depending on how many worked as foster family consultants, for whom training was mandatory. In some municipalities these were joined by other social workers. The total number of trainees in a municipal session thus varied: five to seven in three municipalities, 13 to 15 in two municipalities, and 35 from one (the biggest). Social workers from the two smallest municipalities, with one to two social workers each, participated in joint sessions with neighboring municipalities. Feedback from participants was collected through questionnaires in the larger sessions and brief qualitative interviews in the smaller ones. In addition, 2 h sessions were held on average every eighth week over an 18-month period in each municipality for training social workers in how to use screening results to counsel foster parents. Furthermore, a plan for peer-to-peer supervision, telephone support, and additional on-demand training was developed.
On-demand training was also important owing to the generally high level of staff turnover observed in social work. Problems with turnover and retention in front-line staff working in child welfare are well-documented internationally (DePanfilis & Zlotnik, 2008; Katz et al., 2021; Mor Barak et al., 2001). However, there is surprisingly little research on this important topic in Denmark. Anecdotal evidence and statistics on some of the presumed causes of turnover such as stress suggest that it is a serious problem. For example, we were told by social workers in one of the municipalities that statutory caseworkers working with vulnerable children and youth did not last more than 18 months on average at their workplace. The high turnover has several negative effects, among them a steady loss of specialized knowledge, including that achieved through training and experience with MOMP. Combined with the hitherto voluntary nature of MOMP—social workers are not legally required to use it—this ultimately means a higher risk that the intervention will not be used in municipalities affected by changes among social workers.
The frequency and content of training sessions also varied by demand. The plan is to channel this demand, and the feedback received in courses, into obligatory courses that social workers will be expected to take to qualify as MOMP workers. Training content is prescriptive in the technical aspects of screening where the knowledge base is established, for example, how to determine whether a screening result indicates serious problems. In contrast, it is flexible when the knowledge base is incipient, taking the form of suggestions, for example, in what order to analyze the various scale scores from the SDQ or how to compare responses across respondents. Training sessions are at present in the order of the procedure leading up to the half-yearly counseling meeting, starting with the registration of a child on the digital platform and entering its background information (A in Figure 2) and ending with registering the follow-up actions agreed upon in the counseling meeting, for example, planning a service-as-usual intervention or doing nothing (D in Figure 2). For example, a child receives a high score based on the teacher's responses, but a low score based on the foster parents’ responses. The MOMP manual guides the social worker with questions for probing this apparent discrepancy in scores and helps her to decide if a service-as-usual intervention should be implemented for supporting the child in the school context.

Illustration of a MOMP cycle.
The result of the counseling meeting is ideally a plan for the anticipated outcome in relation to the expected change in scores by the next counseling meeting depending on the action taken. The screening result should enable different observable outcomes depending on the service-as-usual intervention used. For example, if the measurements indicate a high score either in the foster home or in school, a specific magnitude of positive change could be expected at the next counseling meeting based on the planned service-as-usual intervention. Actions planned in the counseling meeting should be documented according to mandatory procedure, which enables concrete and objective direct outcomes within MOMP.
At the next counseling meeting the new screening results are compared to those from the previous round. MOMP helps the social worker interpret score changes by using the concept of “clinically meaningful change,” which refers to changes in an individual's outcome measures that are reliable or that are large enough to be considered “important” (de Vet et al., 2006). Standardized instruments tend to manifest natural variation over time, often demonstrated by a test–retest calculation (e.g., Polit, 2014), and clinically meaningful change corrects for this. The manual provides the social worker with guidelines for interpreting change in scores or lack thereof by directing her clinical curiosity beyond the scores. For example, no change in scores could also indicate an intervention success if the child had experienced several major stressors in its social context between the planned half-yearly counseling meetings. This represents two complete cycles of parental monitoring (see Figure 2).
Discussion and Applications to Practice
The aim of this article was to describe the initial steps in developing MOMP, a procedural intervention as part of routine social work practice aimed at enhancing parental monitoring as a protective factor in family foster care. We have done so, using as a guide the first two steps of Fraser et al.'s (2009) model of intervention development.
Our contribution was two-fold. First, we adapted the construct of “parental monitoring,” hitherto used typically in the context of a single set of parents, to the context of family foster care in which parenting is the joint responsibility of social workers, foster parents, and biological parents. Such a conceptual adaptation was by no means self-evident. Combining the constructs of tripartite parenthood with monitoring in a family foster care context led to the hindsight that joint parental responsibility required the systematic generation and sharing of knowledge regarding the foster child's wellbeing and development—and that this, in turn, required the use of valid and reliable screening questionnaires that could be answered by those caring for the child in different life spheres, thereby promoting a holistic view of the child. It also underscored the social worker's role of lynchpin in facilitating such a holistic view.
Second, MOMP gives social workers the responsibility of screening for psychological problems. This is itself a significant innovation in that such activities would normally be undertaken by personnel trained in mental health. There is, to our knowledge, no precedence for standardized measures of mental health being administered and interpreted independently by social workers without assistance from mental health experts. In the United Kingdom, for example, where the use of the SDQ in child and youth welfare services is mandatory (Cox & Bentovim, 2000; Department for Education & Department of Health, 2015), social workers typically do not work independently with the SDQ; they are helped by Child and Adolescent Mental Health personnel to interpret results. Further, in most of the local authorities studied by Cocker (2019) the SDQ data collected were not used to assist social workers in identifying children's needs but were used to provide external performance information to the government. Thus, the use of SDQ independently by social workers to screen children in their care from multiple perspectives and interpret the resulting data to inform their decisions is, to the best of our knowledge, an international innovation.
Regarding practical lessons for social workers, findings from the MOMP project suggest that it is possible for social workers as part of routine practice to (a) measure the wellbeing and learning of children placed in foster care with standardized screening tools in a country without a tradition for using such tools, (b) use the measurement results in the counseling and supervision meeting with the foster parents, and (c) use input from this meeting to take appropriate actions. Further, our experience suggests that to maximize the benefits of screening, it is imperative that social workers set aside time to analyze screening results prior to discussing them with foster parents. Finally, the way internal administrative processes are organized matters. The data suggest that having an administrative secretary take care of screening procedures, thereby allowing social workers to focus on analyzing screening results and using them in their counseling, can lead to more effective screening.
For program developers, there are three lessons. First, the world of social work practice can often appear chaotic in contrast to the more structured world of research. This means that transferring neat models of intervention from paper to an often-messy reality requires continuous dialogue with project participants, especially intervention agents. Moving from a problem theory to specifying program elements throws up new challenges, situations of “not knowing what one does not know.” Avoiding such pitfalls requires frequent dialogue with, and observation of, intervention agents and knowing when to let them devise their own solutions, a case of combining top-down and bottom-up approaches (Chen & Garbe, 2011) to implementation. An example of this was when we thought we had a fully functional digital platform only to learn from interviews and on-site observations how frustrating it was for social workers to do ostensibly simple tasks such as administering questionnaires via the platform. Consequently, the municipalities adapted the functionality of the platform to their organizational set-up, which ultimately led to three broad ways of implementing the digital platform.
Second, apart from facilitating the adaptability of the intervention to organizational characteristics, dialogue with intervention agents, for example, discussing the strengths and weaknesses of screening instruments and being responsive to social workers’ concerns about using them, helps them to find meaning in the intervention. This contributes to ensuring its sustainability.
The theme of meaningfulness (e.g., Chalofsky, 2003; Chalofsky & Krishna, 2009) runs through the third point as well. Our experience has been that the most important bits of theory—our theory of change and program theory—did not come ready to “plug and play.” Indeed, the core idea of monitoring in a context of tripartite parenthood was clarified only when we were well into the pilot phase and sought to make sense of our actions. For example, at first glance the discussion of joint parental responsibility between the social worker, foster parents and biological (or adoptive) parents appeared unnecessary and irrelevant to implementation. But we realized that it was the theoretical proposition of joint parental responsibility, which was only implied by the legal text, which rendered meaningful the knowledge-sharing essential to monitoring and the screening tools facilitating it. In short, joint parental responsibility for the child's wellbeing was brought into relief by the construct of tripartite parenthood and rendered meaningful the act of knowledge-sharing to the benefit of the child and the use of screening tools facilitating this act. Such meaningfulness is an important source of motivation for social workers, who are not obligated to implement MOMP.
Our study of MOMP also has some limitations. First, it does not include any outcome measures since MOMP is still being developed. Thus, we do not know whether the intervention improves conditions for foster parents or foster children. The inclusion of appropriate outcome measures will be the focus of the next stage of development. Second, we did not investigate whether social workers failed to probe issues other than those suggested by the screening results or what they discussed in the absence of screening. Consequently, we have two suggestions to improve future social work research investigations. One is to include at least some appropriate outcome measures linked to the intervention, for example, sense of efficacy or stress among, foster parents, and the other, to include an analysis of potential strengths and weaknesses of the screening tools. So, we should perhaps have observed meetings between social workers and foster parents in the absence of MOMP—the counterfactual situation. Finally, it is important to remember that MOMP covers only part of the causal chain. Improving outcomes for foster children in MOMP depends mainly on the service-as-usual interventions provided, and over which MOMP has little influence. We hope that improved monitoring will instead give the social worker a better understanding of the child's needs and a stronger child perspective in their documentation of the child’s development in care. As Köhler et al. (2016) have pointed out, the child perspective is insufficiently incorporated in health care professionals’ case files and serious needs are unmet. We would argue that this finding applies just as much to social workers and the social care needs of vulnerable children. MOMP's main outcome will hopefully be a clearer documentation of the child's needs, which can better motivate targeted intervention.
MOMP is intended to be a low-cost intervention and we find it probable, based on the RE-AIM Framework (Glasgow et al., 1999), that MOMP will have high reach, adoption, implementation, and maintenance but low efficacy since it focuses on having an overall out-of-home population impact. Our next steps, following the Fraser et al. (2009) model, will be toward designing an experimental study to determine if parental monitoring in MOMP leads to better outcomes for the foster parents and the child.
Footnotes
Author Note
This work represents original and previously unpublished scholarship and is not under concurrent editorial review.
This paper was submitted as a contribution to the special issue of Research on Social Work Practice “Program Theory in Social Interventions Developed in Practice Settings”, guest edited by Tina M. Olsson and Therése Skoog.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was made possible through funding from TrygFonden (grant no. 30053) and the A. P. Møller Relief Foundation (grant no. 11619).