
Abstract
Keywords
Adolescence is a crucial phase of human life and is one of the most rapidly changing stages of human development and lays an essential foundation for adult health (Sawyer et al., 2012). Depression is a key factor affecting the mental health of adolescents across the world. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM–5), or International Classification of Diseases, 10th Revision (ICD-10), depressive disorder was seen in 2.6% (95% CI 1.7–3.9) of adolescents globally (Polanczyk et al., 2015). A series of social and psychological risk factors were found to be related to adolescent depression (Tang et al., 2020a, 2020b). In addition, depression was found to be closely linked to severe consequences such as suicide ideation, attempts, and completion (Pagliaro, 1996; Prager, 2009).
On a continuum of severity, depressive symptoms were even more common. The existing studies using Center for Epidemiologic Studies-Depression Scale (CES-D) as a measurement tool and 20 as cutoff, the prevalence of depressive symptoms has varied between 18.6% and 23.7% for Chinese adolescents (Huang et al., 2011; Yang et al., 2013; Zhang et al., 2001; Zhou et al., 2009). A meta-analysis screening the literature from 2010 to 2020 reveals that 28% of the Chinese adolescents in secondary schools experienced significant depressive symptoms (Yu et al., 2022). Middle and late adolescence seems to be a more vulnerable period. Research revealed that the prevalence of major depressive disorder (MDD) is significantly higher in adolescents both aged from 14 to 15 years (2.89%) and from 16 to 19 years (3.45%) than adolescents aged from 11 to 13 years (1.00%). The age of 14 was a turning point after which the prevalence of depressive disorder increased sharply (Yang et al., 2013). Therefore, it is necessary to provide professional service for adolescents, especially those in secondary schools, to cope with emotional difficulties.
Although there is a great need for depressive symptoms prevention, there is a lack of professional resources to deal with this mental health issue. China's community-based mental health care is not yet mature and is subject to poor conditions, professionals reluctant to work in community agencies, as well as other limitations (Hedman et al., 2012; Wong et al., 2014). School counseling centers are the most accessible resources for adolescents in secondary schools. In 2012, China stipulated that primary and secondary schools must carry out mental health education for its students, including group counseling, psychological training, seminars, etc. Furthermore, a counseling room should be established to help students solve issues with learning, life, and growth. However, many challenges exist in depression prevention in school settings. One key challenge is a lack of effective prevention programs, making it difficult for schools to address the increasing prevalence of depressive symptoms among secondary school students. Therefore, an essential task would involve developing an evidence-based depression prevention program for students.
During the past three decades, programs that were designed for preventing depressive symptoms has been conducted and disseminated worldwide. Researchers used randomized controlled trials (RCTs) to assess the effectiveness of these programs in schools and communities (Hetrick et al., 2015). Most prevention programs for adolescent depressive symptoms in schools are based on cognitive behavior therapy (CBT) (Werner-Seidler et al., 2021). There also exist prevention programs based on interpersonal psychotherapy (Mufson et al., 2011; Weissman & Markowitz, 2007). A small number of programs have used mindfulness-based cognitive therapy, acceptance and commitment therapy, psychoeducational contents, or a combination of these treatments. There has been much research on the efficacy of prevention programs for adolescent depressive symptoms.
According to Gordon Jr (1983), there were three types of prevention: universal, selective, and indicated prevention. Selective prevention is aimed at those who have certain risk factors, which may prevent them from developing into a disorder, such as a prevention program specifically for students with parents with an MDD history. Indicated prevention targets those who have not yet reached the diagnostic criteria for disease (e.g., DSM-5 diagnostic criteria for MDDs) but have shown early symptoms. Universal prevention is offered to the entire population, regardless of whether participants have depressive symptoms or certain risk factor. A meta-analysis comparing the three types of prevention shows that all of them could effectively reduce depressive symptoms (Stockings et al., 2016). Universal prevention resulted in a small but significant reduction in depressive symptoms in post-intervention (d = 0.11, 95% CI 0.05–0.16); this effect remained in 12-month follow-up (d = 0.09, 95% CI 0.01 to 0.17). Selective prevention has a slightly larger effect size in the posttest (d = 0.23, 95% CI 0.09–0.36) but decayed during other follow-up assessments. Indicated prevention significantly reduced depressive symptoms in the posttest (d = 0.33, 95% CI 0.20 to 0.46) and in 6–9 months (d = 0.26, 95% CI 0.12 to 0.39) but were not retained after 12 months.
Compared to the other two prevention approaches (i.e., selective prevention and indicated prevention), universal prevention has numerous benefits for the general public. It is offered to the entire population, regardless of whether participants have depressive symptoms or certain risk factor, which has a broad target population that can obtain therapeutic knowledge and skills simultaneously. Also, this approach has the potential to avoid stigma which is common in China (Yang et al., 2020). Third, universal prevention is cost-effective, and requires less training than selective or indicated prevention and is suitable for large-scale dissemination. Fourth, if universal prevention is used in schools, it can be carried out by the school's mental health staff (such as school counselors, nurses, or social workers) who are familiar with their students and can modify the prevention protocols for a more effective delivery (Ahlen et al., 2015).
However, high-quality prevention programs on Chinese adolescent depression are scarce. Zhao et al. (2019) developed a prevention program based on positive psychology for Chinese junior secondary school students. The program included three modules and a total of 10 sessions. Data were collected in a baseline and posttest. An ANOVA analysis showed that the effect of time condition was significant (p = .019, η2 = 0.032). Specifically, there were no significant differences between the control and intervention groups in the baseline. Following the intervention, the depressive symptoms in the control group increased significantly, whereas depression levels in the intervention group did not change. Depressive symptoms in the control group were significantly more prevalent than that in the intervention group, indicating that the program may be able to effectively prevent the increase of depressive symptoms. The study provided evidence on the effectiveness of a universal prevention for adolescent depressive symptoms in mainland China. However, there was no follow-up data collection in this study, meaning that the long-term effects of this prevention program could not be determined.
Due to the prevalence of depressive symptoms among Chinese adolescents and its negative consequences, it is necessary to develop an effective universal prevention program. Therefore, we designed a universal prevention program mainly based on the techniques in cognitive behavioral therapy, in order to reducing adolescents’ depressive symptoms. The aim of this study is to investigate the efficacy of this universal prevention program for adolescent depressive symptoms in senior secondary schools. Therefore, we hold the follow study hypotheses: The intervention group demonstrated a greater reduction in the levels of depressive symptoms (primary outcome variable) following the prevention program than the control group (Hypothesis 1); The intervention group demonstrated a greater reduction in the levels of anxiety and stress (secondary outcome variables) following the prevention program than the control group (Hypothesis 2); The intervention group demonstrated a greater improvement in quality of life, attitudes towards mental illness, and help-seeking intentions following the prevention program than the control group (Hypothesis 3).
Method
Location and Participants
The trial was conducted at a senior secondary school in Dongguan, Guangdong, China. Dongguan is a city with a highly developed economy; its GDP in 2019 ranked fourth in the province and 19th in the country. This school has an excellent reputation for teaching in Dongguan. Weekly psychological courses are provided for second-year students. Therefore, the program was conducted with Year 2 students. A total of six classes were willing to participate in the study, namely three classes randomly assigned to the intervention group (including 148 students) and three as control groups (including 131 students). A research assistant who did not play a role in implementing the program used a computerized block randomization with a 1:1 allocation ratio to the two conditions. This study obtained ethical approval from the Human Research Ethics Committee at the University of Hong Kong. The trial was also registered in the Chinese Clinical Trial Registry (ID: ChiCTR1900023145).
The trial was conducted based on the CONSORT-SPI (Consolidated Standards of Reporting Trials statement extended to social and psychological intervention trials; Grant et al., 2018). Informed consent was obtained after randomization, which is different from individual randomized controlled trials, in which informed consent is often granted before randomization. However, in cluster RCTs, individuals who participate in the study are generally only approached after randomization (McRae et al., 2011). Informed consent in this study included a written personal assent form for students and written passive consent form for the guardians. The passive consent was issued because many students lived in school dormitories and did not live with the guardians, meaning that it was difficult to obtain the guardian's active consent. Thus, students were encouraged to communicate with guardians using phones or messages to make them fully aware of the content and purpose of the program. Moreover, the program itself, as it aimed to provide mental health services to students, would not adversely affect their rights or welfare. Therefore, passive consent could be used under this condition (Chartier et al., 2008; Littenberg & MacLean, 2006).
The trial was conducted from May to June 2019. Data collection was conducted before the start of the program (baseline), after the program (posttest), and 6 months after the end of the program (follow-up).
Sample Size
Based on the findings of a meta-analysis (Stockings et al., 2016), universal prevention has a small effect size of d = 0.11 (95% CI 0.05, 0.16) in post-intervention. To a power of 0.80, Cohen's d of 0.11 and α of 0.05, each study condition required at least 1,299 participants, resulting in a total of 2,598 participants. Therefore, the sample size of the formal RCT was large, and conducting a formal trial may incur risks early in the development of new prevention programs, the effect of which is uncertain.
Therefore, a pilot RCT was more appropriate for this study. Researchers have suggested that the sample size of the pilot study must represent 10% of the formal trial (Connelly, 2008). Recently, scholars have provided a more reliable estimate of the sample size of a pilot study based on the effect size that an intervention program may produce. For a formal trial designed with 90% power and two-sided 5% significance, each intervention arm of a pilot trial should have sample sizes of 75, 25, 15, and 10 for extra small effect sizes (0.1), small (0.2), medium (0.5), or large (0.8), respectively (Bell et al., 2018; Whitehead et al., 2016).
According to the first sample size calculation method (10% of the sample size in the full trial), this study required 130 participants per arm and 260 participants in total (2598
Interventions
Based on the results of a systematic review and meta-analysis, negative cognitions, rumination, and negative life stressors have a strong correlation with depressive symptoms (Tang et al., 2020a, 2020b). Therefore, the three risk factors were identified as risk factors for depressive symptoms among Chinese adolescents and became the targets of this prevention program. The prevention program was designed by a research team, including the authors and a group of experienced clinical psychologists and secondary school counselors. The program consisted of six sessions. Session 1 to 4 focused on cognitive restructuring to aid students in modifying their negative cognitions. Session 5 taught students to practice mindfulness breathing to reduce rumination. In Session 6, students were taught communication techniques to reduce interpersonal distress (see Table 1 for session description in detail).
Program Contents.
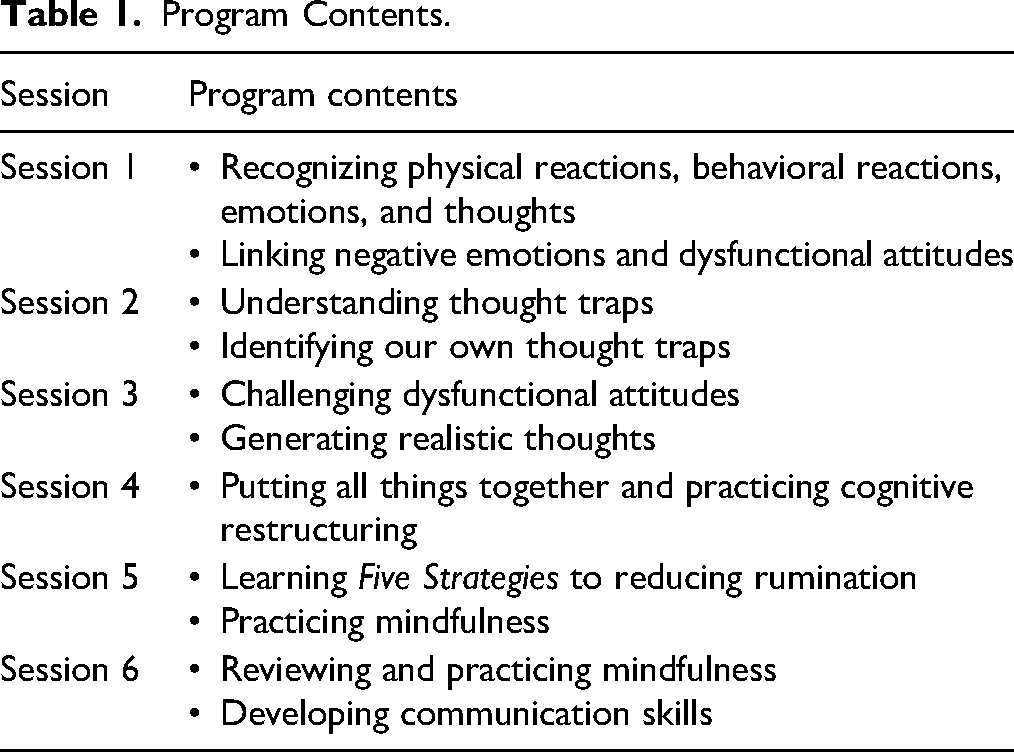
Participants in the intervention group received six sessions, each of which lasted for approximately 40 min. The contents were delivered in many formats, such as didactic teaching, activities, role play, multimedia presentations, and group discussions. The intervention group was delivered by the first author (XT). Participants in the control group also received a 6-week course, which delivered by one school counselor. The content of the course in the control group focused on career exploration, including exploring individual's abilities, personality, personal values, majors, and university choices. The control groups did not receive contents similar to the intervention condition or other active components aimed at addressing mental health issues.
Intervention Fidelity
All of the sessions were video recorded. However, the recordings of Session 2 were damaged due to malfunctions with the recorder. The videos of the other five sessions were properly stored. For each session, there were three videos from three classes in the intervention group. One video was randomly selected from the three classes for further assessment, which resulted in a total of five videos. The two school counselors with a master's degree that were independent from the program were asked to evaluate the leader's adherence to the manual that was developed using an 18-item checklist created based on the contents of the manual. Overall mean adherence to the manual was high at 92%.
Measures
Short Mood and Feelings Questionnaire (SMFQ)
SMFQ (Angold et al., 1995) was a 13-item self-report questionnaire that assessed the presence and severity of depressive symptoms in children and adolescents. Respondents had to report their emotions and behaviors within the past 2 weeks, such as “I felt miserable or unhappy,” “I did not enjoy anything at all.” Respondents were asked to rate each item on a 3-point scale of not true (0), sometimes true (1), or true (2). Scores were summed, ranging from 0 to 26, with higher scores indicating more severe symptoms. The overall factorability of SMFQ demonstrated a robust one-factor measure of depressive symptoms (Costello et al., 1991; Messer et al., 1995). The scale has high test/retest reliability, internal consistency, criterion validity, and convergent validity with other measures for depressive symptoms in children and adolescents (Kent et al., 1997; Rhew et al., 2010; Thapar & McGuffin, 1998). High internal consistency (Cronbach's alpha = 0.88) and retest reliability (r = .84) were also found in Chinese adolescents (Cheng et al., 2009). In this study, the Cronbach's alpha was excellent (0.84 at baseline, 0.88 at posttest, 0.90 at follow-up).
Depression Anxiety and Stress Scale (DASS-21)
DASS-21 (Lovibond & Lovibond, 1995) uses three subscales to measure depression, anxiety, and stress, respectively. Participants had to rate how much they experienced emotions described in the item in the past week from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). When calculating the total score, each item had to be added and multiplied by two to compare with the full version of DASS. Therefore, the total score range of each subscale was 0 to 42, in which a higher score meant more severe symptoms. DASS-21 has been widely used in clinical and community samples (Antony et al., 1998) and positive internal consistency reliability, and validity in the youth group (Szabo, 2010; Tully et al., 2009; Willemsen et al., 2011). This measure also has good psychometric properties (internal consistency reliability of depression subscale is higher than 0.75) in Chinese adolescents (Gong et al., 2010; Mellor et al., 2015; Zhang et al., 2016). The three measurements of Cronbach's alpha in this study were greater than 0.80.
The World Health Organization Quality of Life-Brief Form (WHOQOL-BREF)
WHOQOL-BREF is used to measure the quality of life (Whoqol Group, 1998). This measure is a shortened version of the longer questionnaire WHOQOL-100. The shortened version is convenient for screening the general population. The questionnaire contains a total of 26 items; the first two of these items are global questions about the overall quality of life and satisfaction with health, which were not used for analysis in this study. The remaining 24 questions measure four domains, namely physical health, psychological health, social relationships, and environmental contexts. Question 21, “How satisfied are you with your sex life?” was deleted from this study because it was not appropriate for Chinese secondary school students. All questions were scored on a 5-point scale. The scores of each domain were summarized separately and converted into a score of 0–100 compared to the original 100-item WHOQOL. WHOQOL-BREF is widely used in many cultures and has been translated into 19 languages, including Chinese. A cross-cultural comparative study found that WHOQOL-BREF has the same factor structure and equivalence in all 13 countries, and the Cronbach's alpha in various fields in the Chinese group was 0.72–0.85 (Hao et al., 2006). In this study, internal consistency was poor in physical health (α = 0.43 to 0.57) and psychological health (α = 0.49 to 0.58) but acceptable for social relationship (α = 0.76 to 0.83) and environmental context (α = 0.76 to 0.81).
Attitudes towards mental illness were assessed with two statements. The first statement assessed adolescents’ attitudes towards the efficacy of intervention: “intervention can help people with mental illness lead normal lives.” The second statement assesses these individuals’ perceptions of the general public's attitudes towards people with mental illness: “People are generally caring and sympathetic to people with mental illness.” These two items were used in a large-scale survey conducted by the US Centers for Disease Control and Prevention (CDC) and the Substance Abuse and Mental Health Services Administration (SAMHSA) to track state-level attitudes towards mental illness (The US Centers for Disease Control and Prevention, 2012). Similar to the CDAS, back-translation was also used to validate the two items in Chinese.
Help-seeking intention was assessed by question: “If you had a serious mental health problem right now, to what extent would you like to seek help from the following people?” This item was developed by Yap et al. (2013), and the categories included general practitioner (GP)/doctor, psychologist, psychiatrist, mental health specialist/service, counselor, helpline, etc. These categories were modified to include resources from which Chinese adolescents in a school setting could seek help. Categories included parents and relatives, classmates and friends, teachers at school, and professional personnel (e.g., school counselors). In each category, respondents were asked to rate their intentions on a 5-point scale.
Knowledge was measured by a self-developed scale including seven items on depression, cognitive restructuring, mindfulness, and communication strategies were created to measure knowledge relevant to the content of the prevention program. These items included the distinction between depressive symptoms and disorder, the difference between thoughts and feelings, appropriate ways of challenging distorted thoughts, the contents of mindfulness, and communication strategies. Six questions were single-choice questions, and one question was a multiple-choice question. Participants were asked to choose the correct answer from the given answers. If the single-choice questions were answered correctly, 1 point would be scored; if the multiple-choice question is answered correctly, 2 points would be scored. The total score ranged from 0 to 8, with a higher score being indicative of a more accurate understanding of the program.
Statistical Analysis
The effect of the intervention on primary outcomes, secondary outcomes, and process variables was analyzed with the intention-to-treat (ITT) principle. Data analysis was performed in SPSS 26. The demographic characteristics of the two groups at baseline were tested using t-tests and chi-square tests. The correlation between all variables at the baseline was also analyzed by linear mixed models (LMMs).
The standardized mean difference, which is also known as Cohen's d, was calculated for the effect of intervention condition on each outcome. As the scores of the variables differed at baseline, a formula adjusted for the baseline values proposed by Morris (2008) to calculate Cohen's d was used in this study. The effect size was based on mean pre-post change (Mpost, T−Mpre, T) in the intervention group minus the mean pre-post change (Mpost, C−Mpre, C) in the control group, divided by the pooled baseline standard deviation (SDpre)

Results
Demographics of Participants
Figure 1 illustrates the process of this study. There were six classes in total, three of which were randomly assigned to the intervention group, and three randomly assigned to the control group. There were 155 students in the intervention group and 146 students in the control group. Informed consent was obtained after randomization. Seven students in the intervention group did not participate in data collection, and 11 students in the control group did not participate in data collection. Furthermore, four students lacked baseline data. In the intervention group, 148 participants were involved in the prevention program and data collection at baseline, posttest, and 6-month follow-up. In the control group, 131 participants participated in the control condition. The data of four participants were not available at posttest but available at follow-up. According to the ITT principles, respondents who participated in data collection in the baseline (148 in the intervention group, 131 in the control group) were included in the data analysis.
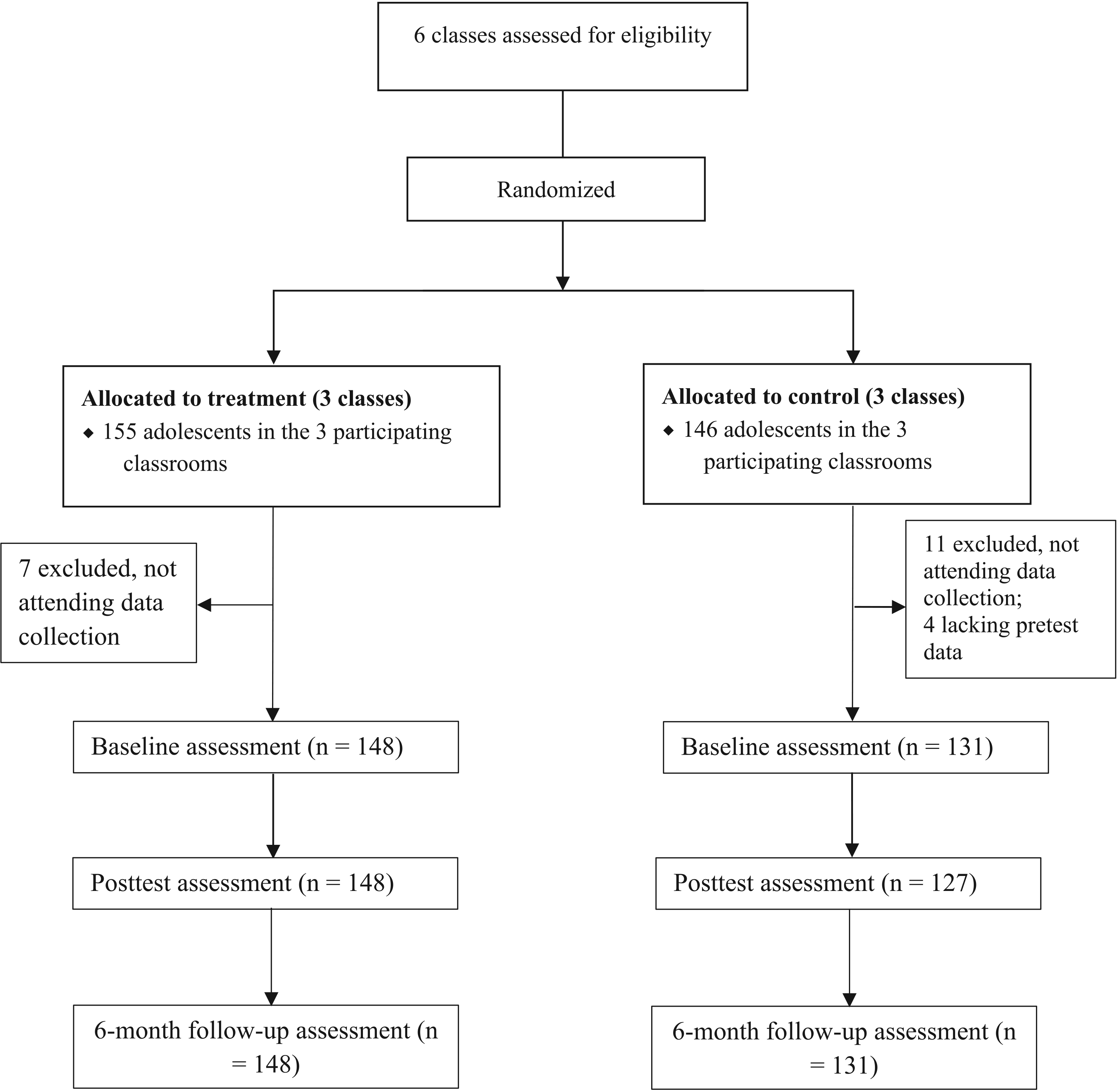
CONSORT flow diagram.
The demographic characteristics of the participants at the baseline are presented in Table 2. There was no significant difference between the control and intervention groups in all demographic variables. The average age of the subjects was 16.7 years (control group, M = 16.7, SD = 0.51; intervention group, M = 16.67, SD = 0.50). The percentage of male students in both groups was slightly higher than that of female students.
Demographics of Participants.

Intervention Effects
Table 3 shows the findings of the LMM, which examined the main effects of group, time, and the group
Linear Mixed Models of Intervention Effects.
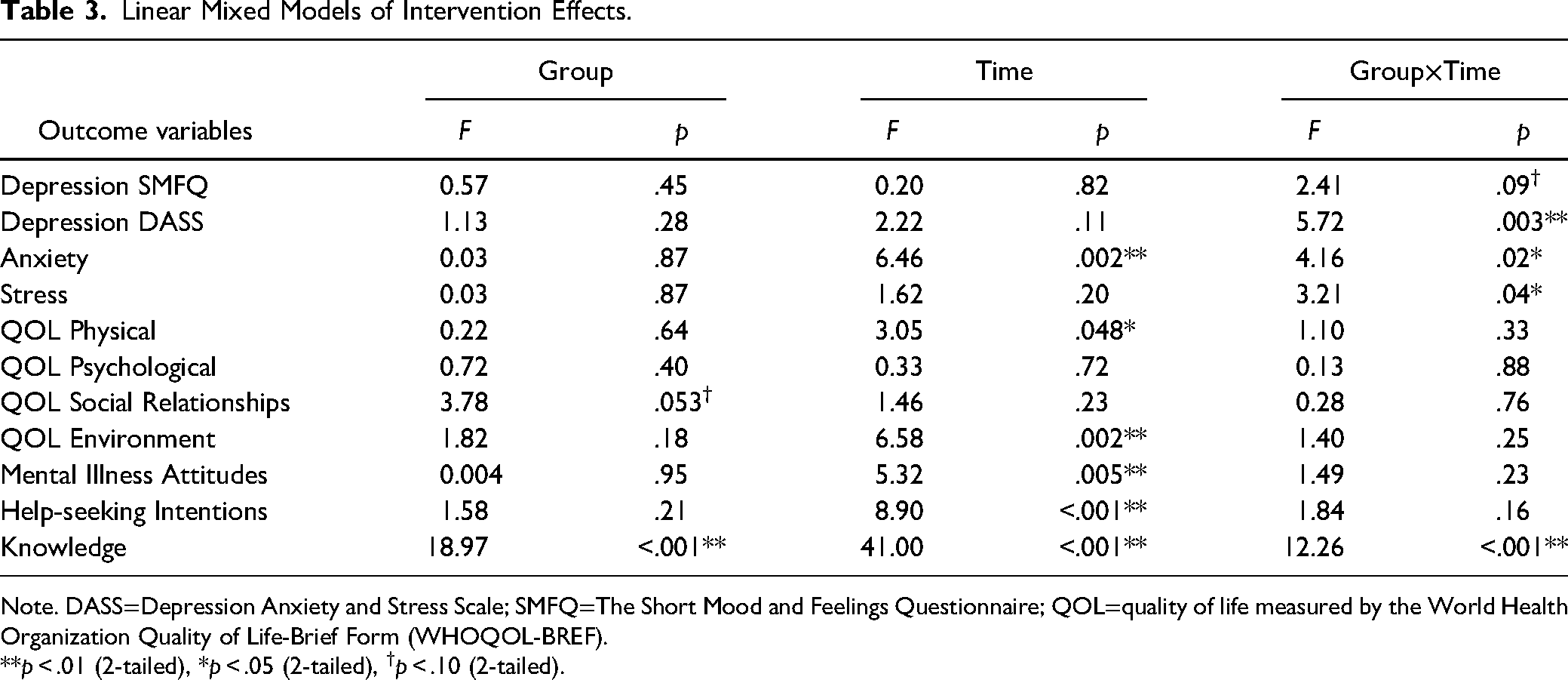
Note. DASS=Depression Anxiety and Stress Scale; SMFQ=The Short Mood and Feelings Questionnaire; QOL=quality of life measured by the World Health Organization Quality of Life-Brief Form (WHOQOL-BREF).
**p < .01 (2-tailed), *p < .05 (2-tailed), †p < .10 (2-tailed).
Effect Size Between Intervention and Control Group for Outcome Variables.
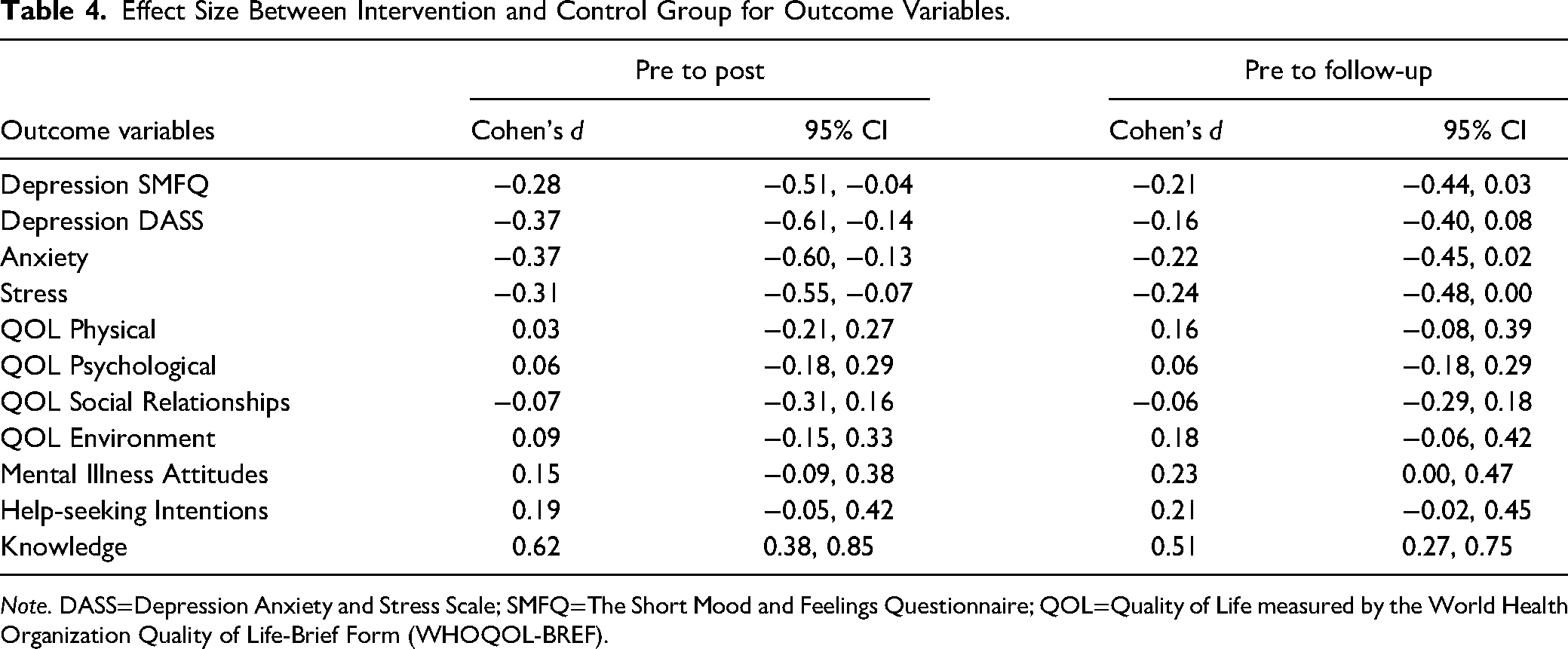
Note. DASS=Depression Anxiety and Stress Scale; SMFQ=The Short Mood and Feelings Questionnaire; QOL=Quality of Life measured by the World Health Organization Quality of Life-Brief Form (WHOQOL-BREF).
Depression
Depression shows significant in the study. On the SMFQ scale, the results of the LMM suggest that the group
In addition, The group
Anxiety
The interaction between group and time was significant (F(2, 550) = 4.16, p = .02). The main effect of time was also significant (F(2, 550) = 6.46, p = .002). Post-hoc comparisons found that the anxiety score of participants in the control group increased slightly from baseline to posttest, though this change was not significant (Mdiff = 0.68, p = .73). Furthermore, there was a significant decrease from posttest to follow-up (Mdiff = 1.38, p = .057). However, the score change from baseline to follow-up was insignificant (Mdiff = 0.69, p = .70). The anxiety score had a different pattern in the intervention group, which was characterized by a significant decrease from baseline to post (Mdiff = 1.60, p = .01) and a continuous but nonsignificant decline from posttest to follow-up (Mdiff = 0.52, p > .99). The intervention group achieved a larger reduction in anxiety scores than the control group at posttest (d = 0.37, 95% CI 0.60, 0.13); however, the intervention effect decayed in the 6-month follow-up (d = 0.22, 95% CI 0.45, 0.02). These results support our second hypothesis.
Stress
The change of mean scores of the two groups at three time points was similar to those on the trend of anxiety. LMM shows that the group
Other Outcomes
The third hypothesis was partially supported. The group × time interaction was insignificant for all dimensions of quality of life and mental illness attitudes. In terms of knowledge of depression and psychological techniques, the main effect of time (F(2, 548) = 41, p < .001) and group (F(1, 279) = 18.97, p < .001) and the interaction between the two (F(2, 548) = 11.26, p < .001) were significant. At posttest, the knowledge level of the intervention group was significantly higher than that of the control group (Mdiff = 0.92, p < .001), representing a moderate to large effect size (d = 0.62, 95% CI 0.38, 0.85). In the 6-month follow-up, the intervention group continued to maintain a high level of knowledge (Mdiff = 0.75, p < .001), showing a moderate effect size (d = 0.51, 95% CI 0.27, 0.75).
Discussion
This pilot RCT found that universal prevention significantly reduced depression, anxiety, and stress in Chinese adolescents. The results added new supporting evidence to the effectiveness of universal prevention.
According to Cohen's (1988), effect sizes are categorized as small (d = 0.2), medium (d = 0.5), and large (d = 0.8). Therefore, the effect sizes for depression, anxiety, and stress in this study are considered to be small to medium. In the broader literature, studies have shown inconsistent findings on the effect of universal prevention for depressive symptoms in adolescents. Although the previous meta-analysis showed that the pooled effect of universal prevention was significant with an effect size of d = 0.11 (Stockings et al., 2016), this finding should be interpreted with caution because the reviewed studies were heterogeneous; there were considerable differences in prevention contents, session numbers, group size, cultural background, research design, etc.
Many studies supported the effectiveness of universal prevention in the adolescent population. For example, Pössel et al. (2013) implemented a universal prevention program for depressive symptoms in adolescents (mean age = 15.1). The program adopted a cognitive-behavioral approach and consisted of two components, namely cognitive and social components. Cognitive components included recognition of emotions and cognition and the identification of and challenges with negative cognitions. Social components taught students skills about assertiveness and social competence. Five hundred eighteen participants were randomly assigned to one of three groups, namely the intervention group, nonspecific control, or the no-intervention control condition. The results showed that the depressive symptoms in the cognitive-behavioral group improved more than in the other two groups at a 4-month follow-up. In another New Zealand-based study of the prevention of depressive symptoms in adolescents (mean age = 14.2), the intervention group (n = 192) used techniques based on the cognitive-behavioral approach (cognitive restructuring) and interpersonal therapy approach (problem resolution and conflict resolution). The control group was a placebo group with a focus on having fun but without active elements. The results showed that, after the 11-session intervention, the intervention group had significantly improved depressive symptoms more than the control group. However, the effect was not maintained in the 18-month follow-up (Merry et al., 2004). A third study used mindfulness-based programs to guide adolescents (M = 16.8) in 8-week experiential mindfulness exercises (e.g., mindfulness of breathing, body scan), psycho-education, and sharing and discussion in small groups. The participants in the control group took regular school courses. The results suggest that the mindfulness group had a significantly lower level of depressive symptoms than the control group in the 6-month follow-up (Raes et al., 2014).
However, a number of studies failed to support that universal prevention could effectively reduce depressive symptoms. For example, in the universal prevention by Stallard et al. (2012), 392 adolescents aged 12–16 received classroom-based cognitive behavioral therapy, including nine main sessions and two booster sessions. The content of these sessions included cultivating emotion-regulation capacities, coping mechanisms, and thinking styles. There were two control conditions, namely 374 participants being assigned to the attention control and 298 being in the usual school provision arm. The study only measured depressive symptoms at baseline and after 12 months, finding that the CBT group did not perform more effectively than the other two groups. Another study with a larger sample size was carried out in Chile, a developing country, and published in JAMA Pediatrics (Araya et al., 2013). The researchers designed a prevention program based on cognitive-behavioral therapy. This program consisted of 11 weekly and two booster sessions and involved thought restructuring, emotions, and problem-solving strategies. 1,221 adolescents received the intervention, and 1,291 received standard curriculum as a control. The results suggest no significant difference in depressive symptoms scores between the prevention and control groups at the three- and 12-month follow-up. A third study was conducted by Lai et al. 2016 on Hong Kong adolescents (mean age = 15.1). The prevention manual was also based on CBT, mainly focusing on teaching students to identify thought traps and improve practical communication and problem-solving skills. The study used two intervention groups and a control group, of which 1,480 students participated in a group led by professionals, 935 in the groups were led by the teachers, and 976 acted as control group. Compared to the control group, the depressive symptoms in participants in a professional-led group and teacher-led group did not significantly reduce.
The former three effective and latter three ineffective prevention programs were similar in many aspects. In terms of the contents, these programs mainly included cognitive restructuring, problem-solving, and communication skills. Most of the universal prevention done so far had been based on the cognitive-behavioral approach. Despite the similarities, some programs were effective, whereas others were not. In complex psychosocial interventions, there may be various factors affecting the intervention effect. Studies have found that the intervention effect tends to be larger in trials with a small sample size (Slavin & Smith, 2009; Zhang et al., 2013). Trials with a large sample size may encounter circumstances that reduce its effectiveness. For example, in the Chilean study discussed, the booster sessions were not performed due to unanticipated events in schools (Araya et al., 2013). In the Hong Kong study, full prevention was covered in 12 sessions, though some students only took 6–8 sessions (Lai et al. 2016). Extensive clinical trials also involved several group leaders. It is challenging to ensure that all leaders have adequate adherence and competence during the implementation of the intervention. It was shown that the experience of the leaders significantly affected the effectiveness of the intervention. The programs led by professionals (such as experienced trainers and psychologists) were more effective than those led by school teachers with limited training (Ahlen et al., 2018; Essau et al., 2012; Roberts et al., 2010; Stallard et al., 2014). In addition, the severity of the symptoms, gender, age, and other factors may have impact on the effectiveness of the intervention (Stice et al., 2009).
Like those effective programs, the present study was also able to significantly reduce depressive symptoms among adolescents. This may be because the prevention program was designed to focus on the causal risk factors that have the strongest relationship with depression, that is, negative cognition, rumination, and negative life events (see Tang et al., 2020a, 2020b). Also, the program was led by professionals, which ensured the fidelity of the intervention implementation.
The study also found that the program may significantly reduce anxiety and stress, which is consistent with research that has found that universal prevention based on the cognitive-behavioral approach can alleviate depressive and anxiety symptoms simultaneously (Ahlen et al., 2018; Johnstone et al., 2014; Johnstone et al., 2020).
This study also has the following limitations. First, as this was a pilot study, the sample size was small and the sample was only taken from one grade in the same school. The sample representation and generalization of the results were also poor. Secondly, the study had a small cluster during the random assignment, resulting in a significant difference in outcome variables between the intervention and control groups at baseline level.
In conclusion, the results of the pilot trial indicated that this prevention program can significantly reduce depressive symptoms. In addition, the program significantly reduced anxiety and stress. Knowledge related to depression and intervention techniques was also improved after the intervention. This study adds supporting evidence for the effect of universal prevention for depressive symptoms in adolescents. A full RCT is warranted to provide a more reliable evaluation of its effect. Given the importance of universal prevention to the general population, it is worth continuing to explore this type of prevention for depressive symptoms in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Major Innovation & Planning Interdisciplinary Platform for the “Double-First Class” Initiative, Renmin University of China; New Faculty Start-Up Grant (22XNKJ27), Renmin University of China.