
Abstract
The “DACAmented Voices in Healthcare” project examined the intersection of restrictive immigration policies and health care via photovoice, a participatory action research approach, with immigrant youth living in Arizona, who were recipients of the Deferred Action for Childhood Arrivals (DACA) program. These “DACAmented” youth took part in nine photovoice sessions exploring their health care experiences and accessibility to care using documentary photography and narratives. They poignantly illustrated their experiences through images identifying their main health concerns and strengths, facilitating the development of health policy recommendations. This article illustrates the thematic findings and discusses policy recommendations and lessons learned from presentations to policy makers and health care providers. Findings suggest that immigrant youth are knowledgeable of their family’s health care needs and hold a unique and important position within mixed-status households. Health care providers can benefit from the proposed recommendations by building bridges to care to address health equity in immigrant communities.
Keywords
Introduction
This article examines the health care experiences of undocumented youth with Deferred Action for Childhood Arrivals (DACA) status and their mixed-status family households 1 in the politically restrictive environment of the state of Arizona. The study design utilized a participatory approach (Coghlan & Brannick, 2003; Israel, Schulz, Parker, & Becker, 1998; Lewin, 1946, 1947), working collaboratively with immigrant youth and employing photovoice as a primary method (Wang, 1999; Wang & Burris, 1997). This allowed “DACAmented” 2 youth—an expression often used by DACA recipients as a play on the terms documented and undocumented—to be intimately involved in every stage of the project. This article illustrates their main health concerns and collective desires to engage in the delivery of care and development of health policies that directly affect their community. This study explored their shared concerns over the high costs of medical care, the complicated requirements to access care, limited options available, pervasive discrimination, and fear of being identified as undocumented, leading to the possibility of deportation and separation from family, while also emphasizing their community’s strength and resilience. Most importantly, they seek to be understood, asking that their humanity be acknowledged.
Background
Arizona Senate Bill 1070 (SB1070) was the harshest state-level immigration policy in the country at the time it was enacted in 2010. Although the law was contested through the courts, its impact is still felt throughout the state (Magaña, 2013; National Immigration Law Center [NILC], 2016; Sinha & Faithful, 2012). Arizona had previously adopted several restrictive state-level policies that superseded SB1070 and thus constructed a climate of fear in immigrant communities that persists to this day (Magaña, 2013; NILC, 2016; O’Leary & Sánchez, 2011). The daily anxiety of being detained and deported has created emotional distress for immigrant communities in the state (Carvajal et al., 2012; Hacker, 2011; O’Leary & Sánchez, 2011).
One major effect has been that many immigrant families from eligible households stopped enrolling in public health programs out of fear of interacting with authorities (Castañeda & Melo, 2014; O’Leary & Sánchez, 2011). The introduction and enactment of such exclusionary policies continue to have a negative impact on the well-being of many communities, particularly those with large numbers of immigrant households (Castañeda, 2014; Castañeda & Melo, 2014; Magaña, 2013; NILC, 2016; O’Leary & Sánchez, 2011). With the initiation of the 2017 Trump administration, further restrictive immigrant legislation emerged at the national level, which included increased deportation efforts, intensified militarization along the U.S.–Mexico border, and the rescission of Obama’s executive actions including the DACA program (Muzaffar & Pierce, 2016).
Enacted in 2012, the DACA program allowed youth who immigrated as children to receive a temporary reprieve from deportation and the ability to work through the issuance of a temporary work permit. Eligible youth had to meet age and residency criteria, educational requirements, and lack any felony convictions to qualify for the program. By 2015, DACA recipients were also able to obtain a drivers’ license in every state. These opportunities allowed them to pursue new jobs and higher education, and thus advance their careers and establish lives in the United States. 3 The program was rescinded by the Trump administration in September 2017. Nonetheless, during the 5 years of the DACA program, approximately 800,000 beneficiaries experienced a profound increase in educational and work opportunities (Gonzales, Roth, Brant, Lee, & Valdivia, 2016).
One area in which their lives remained the same, however, was in regard to access to health care. DACA recipients, like other undocumented immigrants, faced a number of barriers to accessing services. In addition, they were explicitly exempted from all provisions of the Affordable Care Act (ACA) and remained ineligible for Medicaid and the ability to purchase private insurance through the state-based health exchanges (Castañeda, 2017). Addressing health equity for the populations affected by these federal policy changes has thus become even more challenging, albeit critical, for public health professionals.
Theoretical Framework
Photovoice, a qualitative method that combines photography and community-based social action, was founded on the principles of empowerment education, feminist theory, and documentary photography. It seeks to address health as a vital social issue, engaging with topics ranging from youth substance abuse to environmental injustice (Catalani & Minkler, 2010; Graham et al., 2013; Thompson, 2016; Wang, 1999; Wang & Pies, 2004). According to Wang & Burris (1997), the three primary goals of photovoice are to enable community members to document and reflect on their own strengths and concerns, promote critical dialog through group discussion of photographs, and communicate important health messages to policy makers to advocate for needed resources and policy change (Wang & Burris, 1997; Wang, Morrel-Samuels, Hutchison, Bell, & Pestronk, 2004; Wang & Pies, 2004). Photovoice’s theoretical underpinnings of empowerment education draw from the Brazilian educator Paolo Freire’s work on critical consciousness (Carlson, Engebretson, & Chamberlain, 2006; Wang & Pies, 2004). Freire’s participatory learning approaches engaged teacher and student as “co-creators of knowledge,” hence, reversing the power dynamics of education from a dialectic to an egalitarian approach (Freire, 1973; McCarthy, Freire & Macedo 1986; Shor & Freire, 1987). This pedagogical framework emphasizes the importance of critical dialog as a way of addressing social issues affecting people’s lives (Freire, 1973; McCarthy, Freire, & Macedo, 1986; Shor & Freire, 1987). Complementary to this, feminist theory promotes empowerment by recognizing participants as experts of their own lived experience, appreciating and raising up their voices and subjective experience as coresearchers and advocates for their communities (Wang & Pies, 2004).
Method
Study Design
Photovoice: A participatory action research approach
The study design utilized a participatory action research approach employing photovoice as a primary method of engaging and working collaboratively with immigrant youth (Burnes, 2004; Coghlan & Brannick, 2003; Lewin, 1946; Wang, 1999; Wang & Burris, 1997). Participatory action research, a methodological strategy that is complementary with the theoretical underpinnings described above, goes beyond the contribution of new knowledge by creating a direct connection between knowledge and action that can affect directly the health of communities (Coghlan & Brannick, 2003; Israel et al., 1998; Lewin, 1946, 1947). Moreover, participatory action research methodologies like photovoice can promote social justice through the reversal of power structures inherent in the academic research paradigm by engaging marginalized community members as central to all stages of the research process (Carlson et al., 2006; Haque & Eng, 2011; Strack, Magill, & McDonagh, 2004; Wang & Burris, 1997). The “DACAmented Voices in Healthcare” project engaged immigrant youth in data collection, interpretation, and analysis of their own health concerns. Furthermore, the participants developed policy recommendations to address their identified health care needs. The institutional review board at the University of Arizona approved this research.
Recruitment and Sampling
Ten immigrant youth between the ages of 18 and 26 were recruited, although only seven were able to complete all sessions over the 3-month period (Table 1). Having gained a precarious and impermanent immigration status, DACAmented youth remain a “hidden population” among their peers. As such, they have had little opportunity to explore and express their health care experiences and concerns. To date, no study has utilized photovoice as a methodology to elicit DACAmented individuals’ health concerns. Recruitment of DACAmented youth occurred via outreach to immigrant-serving nonprofit organizations, social media, and promotoras (community health workers) at community health clinics and family resource centers. Word-of-mouth also helped identify eligible participants for snowball sampling. Study participants were screened, interviewed, and consented prior to attending the photovoice sessions. To defray travel costs to the photovoice sessions, participants were provided US$50 cash stipends, which were disbursed at two different points in the study.
Participant Demographic Characteristics.
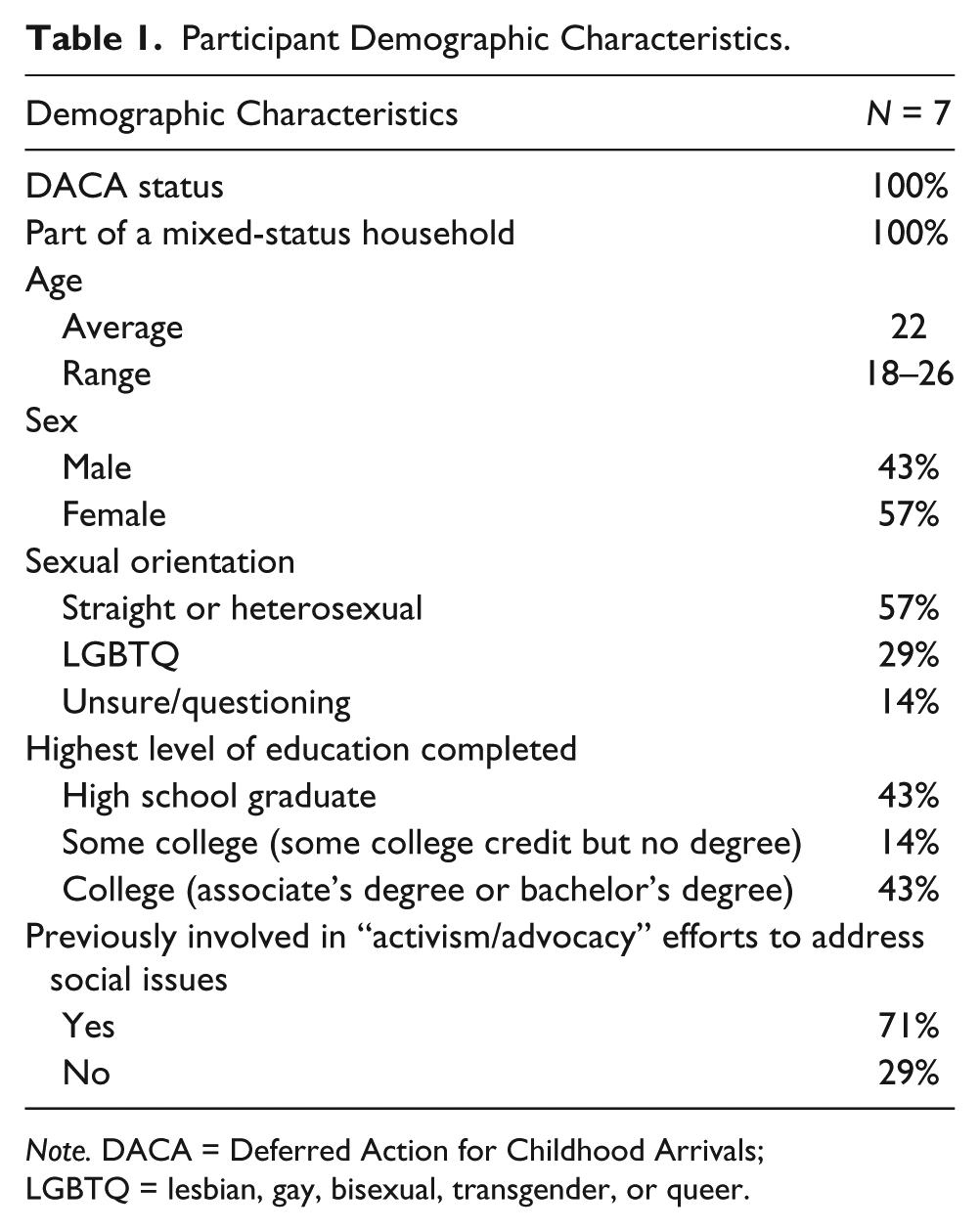
Note. DACA = Deferred Action for Childhood Arrivals; LGBTQ = lesbian, gay, bisexual, transgender, or queer.
DACAmented Voices for Health Care photovoice curriculum
Participants attended nine weekly sessions. Key elements of the curriculum were adapted from an existing photovoice manual, From Snapshot to Civic Action: A Photovoice Facilitator’s Manual (Powers, Freedman, & Pitner, 2012) and supplemented with photography training sessions facilitated by a guest instructor with experience in photovoice and community-based media processes. Through lectures and hands-on exercises, participants were provided an overview of photovoice, photocomposition, photography field ethics, and camera usage. An experienced writer and spoken-word poet also facilitated a creative writing workshop to assist the participants in developing their writing ideas. Both guests were selected because of their experience working with and sharing community voices. Participants were also offered an optional site visit to view photographic documentary archives at the University of Arizona Center for Creative Photography.
Throughout the 9 weeks, participants were asked to respond to three prompts (Table 2). One related to their specific health care barriers and concerns as DACAmented individuals, whereas another asked about their family’s main health care barriers and concerns. A third prompt addressed health promotion and available resources. After photographing in response to each prompt, participants selected and submitted their top three images to present and discuss as a group. The participants selected final images for display at a public photo exhibit, as well as for publication and dissemination. In keeping true to photovoice principles, the data collection, analysis, and interpretation of results were participant-driven, with the research team serving as facilitators (Evans-Agnew & Rosemberg, 2016; Hergenrather, 2009). Sessions were primarily conducted in English, although participants intermittently spoke in Spanish or code-switched between both languages to express their ideas and emotions.
Themes.
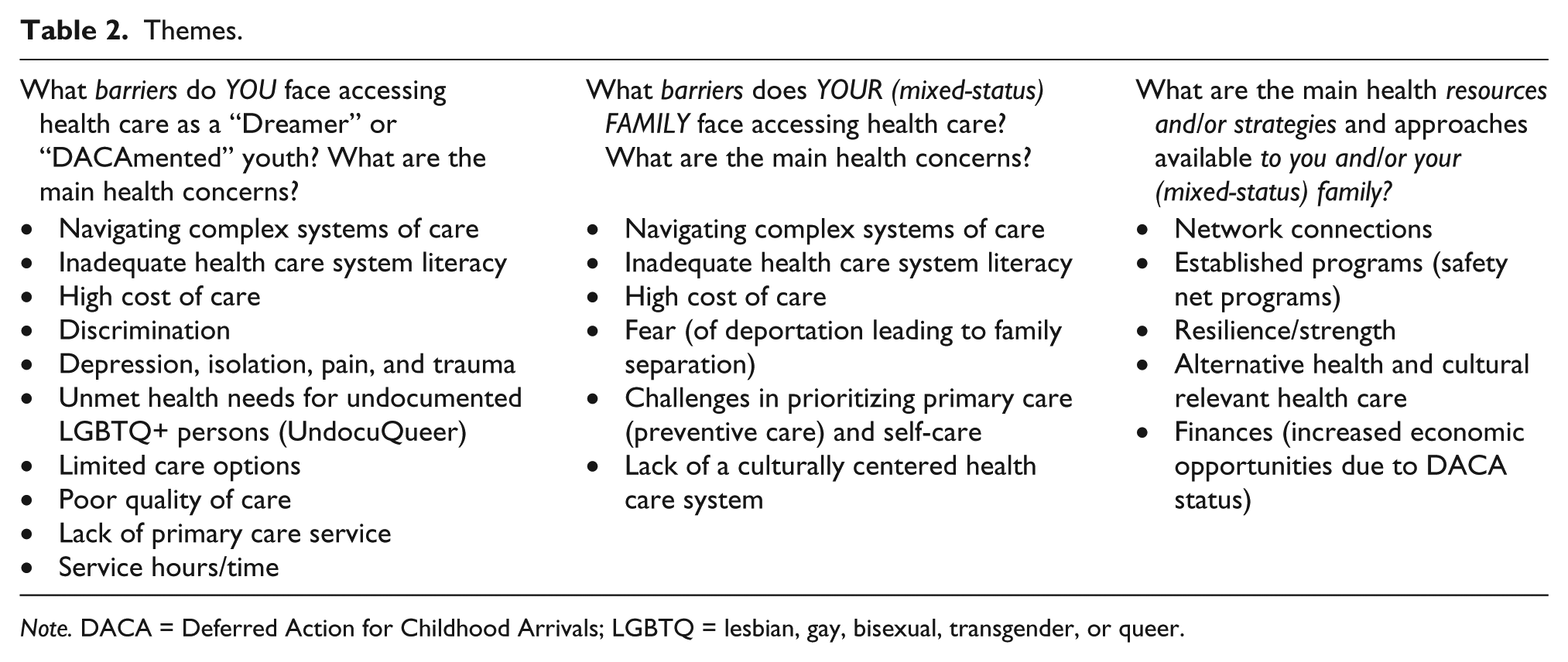
Note. DACA = Deferred Action for Childhood Arrivals; LGBTQ = lesbian, gay, bisexual, transgender, or queer.
Analysis and Documentation
During analysis and interpretation sessions, participants identified their main health concerns and strengths by using affinity diagrams, an inductive method for groups to visualize and organize their ideas and thoughts (Hanington & Martin, 2012; Kawakita, 1991). The use of affinity diagrams allowed them to brainstorm as a collective group to identify main themes and subthemes regarding their specific health concerns and strengths. Using the collection of images and narratives submitted for each assignment, participants worked in two small groups to identify main themes and subthemes subsequently seeking input from the larger group to finalize themes. Researchers only sought clarity from the participants if themes were unclear. Their shared and collective concerns led to draft solutions and policy recommendations. Researchers summarized their findings and presented them for final approval from the participant group at the last session. Recommendations were displayed at a public exhibit and shared at meetings with policy makers and health care providers.
Results
Thematic Analysis: Themes
Table 2 illustrates the main themes that participants identified for each assignment. Common themes regarding both their own and their households’ access barriers and concerns included difficulty navigating complex systems of care, incomplete health literacy, the high cost of care, fear of deportation and family separation, and discrimination. Although this study did not specifically seek to document the UndocuQueer experience—that is, the intersection of undocumentedness and lesbian, gay, bisexual, transgender, questioning and queer (LGBTQ+) identities—participants who identified as such discussed health concerns related to their gender identities; these main themes spoke about their specific concerns related to traumatic experiences and unique needs.
Furthermore, the concept of time resonated across the themes in various ways. Notably, participants stated that their immigration status, and hence their “legality,” was bound by a specific time frame, because their DACA status had to be renewed every 2 years. Within the theme of “high cost of care,” participants described having to save money over a period of time to afford the cost of medical expenses. Other examples related to time off work to seek health care when, in many cases, time equated loss of money. Because sick leave is generally not available to them, or their immigrant family members, they lose out on income when spending time seeking services. The concept of time is depicted below by Josué’s “Schedule of an Immigrant Life” (see Figure 1). In the following section, we elaborate on selected main themes.
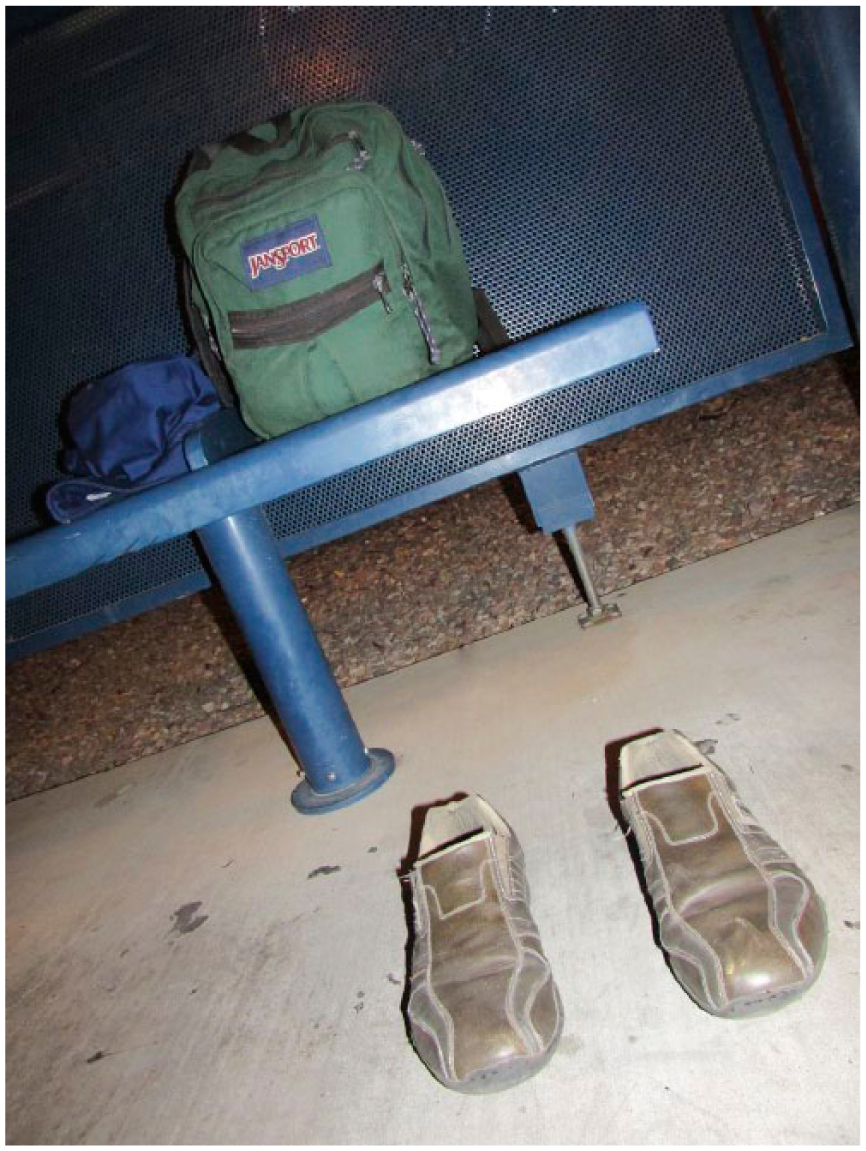
“Schedule of An Immigrant Life” by Josué.
Navigating complex systems of care and inadequate health care system literacy
Challenges to health care usage were linked to a lack of knowledge of available services, confusion over requirements, and complex application processes required to understand if services were indeed available to them, regardless of immigration status. Youth identified the ambiguous nature of clinics in extending services to immigrants, particularly undocumented immigrants, as a barrier to care. Through trial and error, they learned who is and who is not their ally in the health care community. As Miguel conveys in his photo submission, “¿Estan Abiertos?” [Are You Open?], “As a DACAmented individual I grew up undocumented most of my life and learned to use uncertainty about access to services because of my immigration status as a strength. I never knew until I tried” (Figure 2). Another participant compared navigating the health care landscape to a “foreign language,” a sense of not understanding all the rules, procedures, and requirements for accessing care for themselves and their household. This is due to the complexity of the application process and the number of requirements needed to apply for services that were cumbersome and too rigid to accommodate the family’s source of income, which is often unsteady and informal in nature.
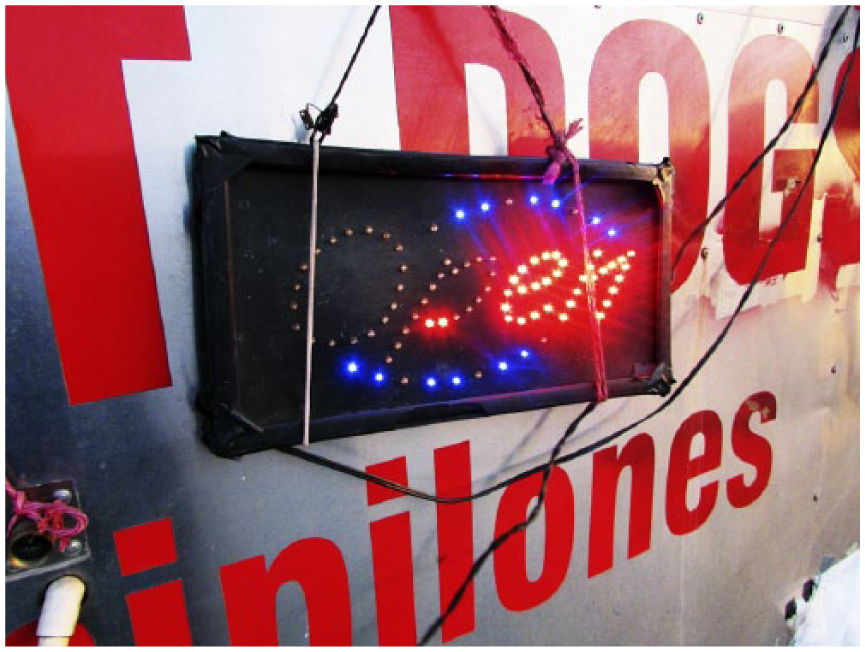
“¿Están abiertos?” [Are You Open?] by Miguel.
High cost of care
The high cost of health care services was a main shared concern among the group. Although a few participants had obtained employer-based coverage because of their DACA status, most were not employed full-time and thus not eligible for coverage. One participant was working five jobs at a time, but none included employee health benefits. Because participants, like their undocumented family members, do not qualify for health coverage under the ACA, they must pay for health services out of pocket. The cost for these services was often outside their ability to pay, even at the discounted rates offered by community clinics. Many times, they delayed preventive or basic care until health concerns developed into acute health problems, thus making treatment even more costly. Specialty care such as endocrinology is particularly expensive; discounted health plans only cover the cost associated with basic care.
Discrimination and fear
Discrimination and fear were referenced as barriers to care for many youth and their households. The fear of being identified as undocumented, leading to the possibility of being separated from family and potential deportation, persisted long after SB1070 was enacted, disputed, and appealed and increased again following the 2016 election. For their household members, youth stated that fear was the key reason for not seeking care. Most participants shared that it took time for them to feel safe, and that DACA allowed them the “legitimacy” to finally seek needed health services (see Figure 3), a privilege that their family members did not enjoy. Participants expressed feelings of being “undeserving” of care and services, and disclosed feeling discriminated against, not only because of their immigration status but also due to their ethnicity, skin color, language, and, for some participants, gender identity. Participants felt excluded from health services due to Arizona’s anti-immigrant climate, an underlying sentiment in society rather than by specific health care providers.

“Holding on to the Dream” by Alejandro.
Depression, isolation, pain, and trauma
Participants discussed their mental health needs as part of access to health services; in other words, “health” was not limited to primary care. They described mental health services as limited or nonexistent for undocumented populations. Cultural apprehension of mental health services was also discussed as an added barrier to seeking necessary services. A 2010 assessment report of behavioral health services at federally qualified health centers (FQHCs) noted that only 40% of the FQHCs provide mental health services at all of their sites (Lardiere, Jones, & Perez, 2011). And, although the majority of sites reportedly screen for depression, immigrant Latinos are less likely to seek mental health services when depressed (Martinez Tyson, Arriola, & Corvin, 2016). Depression, isolation, pain, and trauma were therefore central to group discussions regarding their shared experiences. At the end of the first discussion session, one participant stated that she felt “relieved.” When asked to clarify, she explained that she was relieved knowing she was not alone and among others that shared her experience as a DACAmented individual.
UndocuQueer unmet health needs
Participants who identified as LGBTQ+ expressed the heightened difficulties of their intersectional identities when seeking care, viewing this as both a strength and barrier. When asked to provide an example, one participant explained that when he seeks sexually transmitted disease testing, he strategically utilizes the services that are much more readily available as an LGBTQ+ person, as opposed to someone who is DACAmented. Participants also felt their “holistic” health needs were not being met at any clinic, and expressed having limited care options, including mental health as an UndocuQueer and person of color (see Figure 3). In Figure 3, Alejandro articulated his feelings of exclusion as a member of both the LGBTQ+ and immigrant community in his writings “Holding on to the Dream”: People constantly dismiss the many limitations we have in health care institutions. Refusing to acknowledge not only the physical pain but also the mental suffering one has or will endure as a Queer or Transgender Immigrant. Battling years of oppression, alienation, and criminalization.
In a separate example, another participant noted the lack of inclusive language of the health clinics’ intake forms, which they felt prevented health providers from understanding their health needs as part of both the LGBTQ+ and DACAmented community.
Mixed-status family resources and strategies
A reflection point among some participants, which is not listed as a priority but emerged as part of group discussion, was how their U.S.-born sibling(s) fared better than they do as DACAmented youth. In other words, their U.S.-born siblings’ health and educational opportunities are of higher quality and are more available when compared with their own. They felt that their younger siblings provide the family with an opportunity, despite some members’ ineligibility, to gain a better insight into various available public services and programs (e.g., educational and health programming). Additional resources and strategies identified included established community networks, safety net programs, self-care and advocacy, remedios caseros (home remedies), and increased economic opportunities due to their DACA status.
Resilience and strength
Participants identified their resilience, persistence, and unity as strengths, and this emerges and is expressed in several of their writings. Miguel’s “¿Estan Abiertos?” [Are You Open?] expresses ambiguity as an opportunity to seek clarification thus strength: “ . . . I grew up undocumented most of my life and learned to use uncertainty about access to services because of my immigration status as a strength” (Figure 2). We hear Perla’s resilience in the last stanza of her poem, “Yo Soy Un Humano” [I am Human], . . . Yo soy un humano [I am human], a human that has been stamped as unlawful in American soil, And I smile, smile como una niña esperando al paletero [like a girl waiting for the ice cream man] Because it has punctured me like an espina de nopal [cactus thorn] yet I have embraced it with prestige. (June 2016)
In another submission titled “Community Care,” Josué expresses the strength of unity found in his community (see Figure 4): “Hope for a better tomorrow, With a strong grip on faith . . . That’s OUR medicine, Because we don’t go through life alone, There is me and There is you . . . WE are OUR medicine.”

“Community Care” by Josué.
Youth’s Policy Recommendations
In line with the principles of participatory action research and photovoice’s commitment to social justice, participants developed a policy recommendation statement to advocate for change. The participants discussed their recommendations at presentations and meetings with policy makers and health care providers. The recommendations reflected many of the identified health care needs and concerns described earlier, and focused on creating inclusive spaces in health care to address their desire for “active” participation at institutional systems of care. They requested a “seat at the table” through the creation of a youth health task force that could work with health care providers and policy makers in addressing the health care needs of their community. Participants felt they are especially well qualified to contribute to the development of policy, because they personally understand what it is to be undocumented. Furthermore, their bicultural and bilingual aptitudes are useful for outreach to monolingual members in their communities. UndocuQueer participants requested tailored services to address health care in a more holistic manner. Finally, the group felt strongly that there was a vital need to acknowledge access to care as a fundamental human right, available to anyone despite migration status.
Discussion
Previous studies examining health issues for DACAmented youth have similarly reported that youth avoid health care systems due to fear of discrimination and deportation, particularly in regions where policies are more restrictive (Raymond-Flesch, Siemons, Pourat, Jacobs, & Brindis, 2014; Stacciarini et al., 2015; Talamantes & Aguilar-Gaxiola, 2017; Venkataramani, Shah, O’Brien, Kawachi, & Tsai, 2017). In one of the first studies examining DACAmented youth and health care needs, Raymond-Flesch et al. (2014) report that youth avoid health care systems due to cost of care, limited knowledge about the system, and mistrust of providers due to fear of discrimination and deportation. Moreover, mental health care was reported to be DACAmented youths’ greatest unmet health need. In a separate study, Venkataramani et al. (2017) report effects on mental health for DACAmented youth consistent with observational studies showing rising symptoms of anxiety and depression with policies that raise the risk of deportation.
The “DACAmented Voices in Healthcare” project provided a platform for immigrant youth to explore how Arizona’s restrictive political environment influenced their health care experiences. Youth participants were not only able to provide key insight into their own but also into their family’s main health concerns, and participants clearly framed these experiences within the distinctiveness of living in an anti-immigrant climate. The overall climate for undocumented persons in the United States—as well as formerly DACAmented youth—is becoming much more restrictive and hostile and will continue to exclude them in coming years. By using a participatory approach with a marginalized population, this study provides a window into the experiences of hostile environments and exclusionary policies, evident in the youth’s voices and photographs. The central message drawn from their body of work is the desire for inclusive spaces. Youth are also motivated to work collaboratively in the development and implementation of health care services in their communities, which have been heavily targeted and restricted from public benefits and programs.
DACAmented youth seek acknowledgment of their “deservingness” and moral worth in spaces that have been hostile and exclusionary. As Quesada (2012) explains in examining the impact of structural vulnerability on migrants’ health, “Such stigmatizing representations and the resultant social exclusion impact migrants’ sense of self worth as some convince themselves they are undeserving or unworthy of health care or are undesirable political subjects” (p. 896). The isolation, fear of deportation and family separation, and discrimination that participants face in Arizona—evident in their photographs, poems, and interviews—have led to trauma, stress, and anxiety that continue to be unaddressed, because mental health services are limited (Fortuna, Porche, & Alegria, 2008; Martinez Tyson et al., 2016; Raymond-Flesch et al., 2014).
As members of mixed-status households, participants also discussed how health care affects their family’s life. A study by Vargas and Pirog (2016) examines mixed-status households’ utilization rates of the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and concludes that the risk of deportation was negatively associated with WIC uptake (Vargas & Pirog, 2016). Our study similarly identified fear of deportation to be a major factor in accessing health care services. These findings have important implications not only in Arizona’s unique political climate but also more broadly across the United States, given the growing fear of family separation under the current Trump administration (Muzaffar & Pierce, 2016; Talamantes & Aguilar-Gaxiola, 2017).
Psychosocial Implications of “Veiled” Methods of Health Care Delivery
Public health officials often find themselves in a predicament when delivering care to undocumented persons, and this poses problems with outreach to immigrant communities and produces psychosocial implications. The ambiguity of services—that is, not knowing whether a health clinic, program, or service is available to them or their undocumented family members—is not only a major barrier to care but also reaffirmed youths’ feelings of invisibility and undeservingness. As Willen (2012) notes, notions of deservingness (and undeservingness) are “articulated in a vernacular moral register that is situationally specific and often context-dependent”; they are “shaped by political, economic, social and cultural context as well as personal values and commitments” (p. 814). As this study has shown, these exclusions are evident in mainstream systems of health promotion, prevention, and care in the United States. In the case of a highly restrictive policy environment like Arizona, immigrant youth receive unequivocal clues that they are unwanted and undeserving of medical assistance.
This feeling of invisibility was further underscored during a meeting with a public health official, who shared that the provision of health services to this population was a “non-issue” at his institution. He explained that they had worked hard to enact a “don’t ask, don’t tell” policy when providing services, and took strong measures to ensure that health providers did not ask for immigration status. Yet, when asked by a participant how they make this policy known to the undocumented community, he clarified that they do not specifically reach out to that population due to the potential negative political implications. After the meeting, the youth expressed disappointment with this approach to service delivery, which only made them feel more dejected and excluded. These “veiled” approaches of delivering care to undocumented populations produce distrust and further marginalize eligible mixed-status family members from available health care services, including U.S. citizens (Castañeda & Melo, 2014; O’Leary & Sánchez, 2011; Vargas, 2015; Vargas & Pirog, 2016). Furthermore, lack of clarity in identifying strategies to conduct outreach creates problems for sites that attempt to bridge services to individual members of mixed-status households that might be eligible for Medicaid or insurance plans under the ACA (Barry-Jester, 2015).
Limitations and Future Research
There are limitations to the study presented here. A purposive sample was utilized and may not be representative of other immigrant populations, particularly immigrant youth in different political environments. Second, with the exception of two participants, most participants had received prior advocacy training and worked on educational reform in Arizona; this political and institutional capital made this project uniquely feasible and successful. Finally, although this study did not seek to understand the UndocuQueer experience, three out of the seven participants identified as either “queer” or “unsure” of their sexual orientation (Table 1). Additional research is needed to further understand the unique health concerns that specifically pertain to this population.
Implications for Health Practitioners and Policy Makers
Include youth voices in health research and policy development
In a recent article, Lees et al. (2017) address the lack of inclusion of children and young people in health care research, specifically offering methods beyond interviewing that can promote their participation. The inclusion of immigrant youth in identifying their own health care needs was at the core of this project. The participatory nature of the study allowed youth voices to be heard, informing the analysis and assisting with policy proposals to improve health services for their communities. These young adults identified a need to develop a local task force to improve health care delivery in their community, and they expressed a strong desire to be part of the decision-making process. This requires health policy makers to work differently and to seek ways to engage and collaborate with youth. This requires more than just listening or providing them a “token” seat at the table; it requires commitment and an intentional desire for inclusiveness in the development process through, for instance, recruiting them as promotoras to enhance outreach efforts and provide input on policies.
There are many advantages to working with youth, particularly when seeking to improve health service delivery to communities with high numbers of mixed-status households: They are bilingual, bicultural, have a personal understanding of cultural barriers to seeking health services, and, perhaps most importantly, understand the community’s fears and apprehensions. They have the necessary skills to build bridges between communities and institutions of care (Raymond-Flesch, Siemons, & Brindis, 2016). Given the opportunity, they can assist health policy makers in addressing health equity in immigrant populations.
Expansion of safety net programs
The existence of safety net programs such as FQHCs, discount programs, and charitable clinics have been critical and will remain vital in the provision of care and health information to mixed-status households. In particular, community health centers are poised to play a critical role in the provision of services due to their model of care, which addresses cultural, language, and economic barriers. FQHCs include one-stop services that include primary care providers, behavioral health specialists, social workers, health educators, and many others. FQHCs often provide many services under one roof, facilitating care for households that have varied immigration status and limited care options for coverage. However, the capabilities of FQHCs to sustain and expand services will depend on the allocation of adequate resources for staffing and operations.
Training of health care professionals and frontline staff
Appropriate and adequate care for mixed-status households require that health professionals including frontline staff receive training to respond to their unique needs. Trainings should include not only instruction in cultural competency but also the ability to understand the unique structural challenges that mixed-status households face in obtaining care, particularly in restrictive policy environments that foster fear of family separation.
Increased outreach to immigrant households
Outreach efforts can increase health care access; thus, we recommend expanding application assistance to mixed-status households. In addition, health literacy programming and “know your health rights” workshops targeted to immigrant households can allow them to gain a better understanding of health care systems, facilitate usage, and assist in navigating available programs. Findings from Champlin, Mackert, Glowacki, and Donovan (2017) stress the importance of health information–seeking skills at a young age to improve health literacy. With the increase use of the Internet as a health resource, youth can benefit from interventions that instruct them on the identification of trustworthy health resources, credible content, and knowledge of health terminology (Champlin et al., 2017).
Local response and discretionary powers at the local level
How state and local governments respond to increased restrictive federal legislation can either widen the gap in the uninsured or improve health equity within communities. Just as states like Arizona and Texas have exercised local powers to further restrict public health benefits to immigrant communities, states and local governments can use their discretionary powers to expand services to them, as we have seen in the case of California. Recently, there has been increased opposition by sanctuary cities and localities to the current administration’s hardened immigration policies (Immigrant Legal Resource Center, 2017; Sanchez, 2017). Local authorities have a much more immediate impact on immigrant communities than do federal ones; they can choose to include immigrants as part of the fabric of their communities and construct them as deserving of benefits and services, thus recognizing their humanity.
Continued advocacy for immigration reform and health care for all
Health equity cannot be achieved without a commitment to inclusivity, including advocacy for immigration reform. The expansion of health care to all, regardless of status, would alleviate barriers to care. In the current national climate, we must respond to anti-immigrant rhetoric by underscoring the devastating health impacts of exclusion on individuals, families, and entire communities.
Conclusion
Photovoice findings suggest that immigrant youth, specifically DACAmented youth, are not only knowledgeable of their family’s health care needs but also hold a unique and important position within mixed-status households. Their positionality within their households and communities make them key collaborative health partners in the development and implementation of health care policies for immigrant populations. We argue that it is essential to include youth in the development of policies and programs that pertain to their communities to assist in the improvement of health service delivery to immigrant populations, especially in politically restrictive environments. The study took place in Arizona during a particularly hostile climate for immigrant communities; in the post-SB1070 era and under the current presidential administration, rhetoric against immigrants and refugees has been reignited. This study offers lessons and insights on how anti-immigrant and restrictive political environments affect health and how to engage immigrant youth in achieving health equity.
Footnotes
Acknowledgements
The authors gratefully acknowledge Josh Schachter and Sarita Gonzales for sharing their photography and creative writing expertise in support of this initiative. They also thank Alexandra Samarron Longorrio for her integral role in this project. They are grateful, inspired, and humbled by the DACAmented (Deferred Action for Childhood Arrivals) youth who took part in this photovoice project. Their courage to speak their truth gave the authors a deeper appreciation of their strength and resilience.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.