
Abstract
This exploratory netnographic study is among the first to investigate military video blogs (milvlogs) posted by Iraq and Afghanistan veterans who self-published stories on military-related trauma to YouTube. Studies have shown that self-published milvlogs provide benefits such as education, social support, and self-management of chronic physical and psychological illness. The aim of this study was to explore combat veterans’ milvlogs and to determine themes that emerged across the videos. We transcribed and analyzed content from 17 milvlogs. Our analysis yielded seven themes: motivation, loss, managing symptoms, help-seeking, guilt and shame, suicide, and connecting to other veterans. We concluded that veterans were initially drawn to vlogging to connect to others. Vlogging also served as a medium for combat veterans to tell their stories, position these stories against others’ experiences, and engage in outreach and advocacy. Finally, milvlogs may provide an easily accessible resource for developing preventive and/or mental health treatment/support links.
Introduction
Posttraumatic stress disorder (PTSD) is the most common mental health diagnosis for men who served in Operation Enduring Freedom (OEF), Operation Iraqi Freedom (OIF), and Operation New Dawn (OND), and the second most common for women who served in these operations (Koo, Hebenstreit, Madden, & Maguen, 2016). Recounting war experiences in a safe, supportive environment is vital for traumatized veterans’ readjustment and recovery (Usbeck, 2014). “Soldiers and warriors have always related their combat experience to an audience; be it in songs, memoirs, or letters from the front” (Usbeck, 2012, p. 271). In fact, some evidence-based therapies for PTSD (e.g., exposure therapy, cognitive processing therapy) facilitate the sharing of trauma stories and provide social support (Foa, Hembree, & Rothbaum, 2007; Monson et al., 2006).
For individuals with military-related trauma, treatment seeking, therapeutic engagement, and learning new coping skills can present particular challenges. Due to the avoidance behaviors and social impairment that can accompany traumatic military experiences (Cukor, Spitalnick, Difede, Rizzo, & Rothbaum, 2009), service members and veterans may struggle with telling their stories in traditional mental health settings. Some recent studies suggest that Internet video blogs (vlogs) may provide a relatively comfortable outlet for sharing a variety of traumatic experiences (Huh, Liu, Neogi, Inkpen, & Pratt, 2014; Liu, Huh, Neogi, Inkpen, & Pratt, 2013; Raun, 2012). Molyneaux, O’Donnell, Gibson, and Singer (2008) define vlogs as “blogs created in video rather than textual form” (p. 2). While oral history projects with veterans (e.g., Natick Veterans Oral History Project) have often included narrations of combat-related experiences as well as subsequent life experience, the context of vlogging differs. Oral history projects are planned and involve a formal interview between two people in which the subject responds to specific questions (Baylor University Institute for Oral History, 2016). In contrast, a vlog is completely self-published and self-motivated, focusing exclusively on topics most salient to the individual in that moment in time.
Military-related vlogs, or “milvlogs,” may provide novel context to aid our understanding of veterans’ combat-related trauma. The purpose of the present study is to describe how socially disconnected Iraq and Afghanistan combat veterans communicate narratives of their combat-related experiences via military video web blogs, referred to here as “milvlogs.” Milvlogs are a recent technological development in personal accounts of war trauma. To our knowledge, this is the first study to investigate self-published vlogs posted by Iraq and Afghanistan veterans.
Review of the Literature
PTSD, a chronic, disabling stress disorder, results from direct or indirect exposure to actual or threatened death, serious injury, or sexual violence (American Psychiatric Association [APA], 2013). Up to 15% of U.S. military members who served in OEF/OIF/OND will develop PTSD (Yarvis, 2011). According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; APA, 2013), persons with PTSD experience symptoms that fall into four main categories: reexperiencing, avoidance, hyperarousal, and (emotional) numbing. Symptoms of numbing (e.g., social detachment, disinterest, and disconnection), subsumed under the DSM-5 category of Negative Alterations in Cognitions and Mood, are particularly salient in understanding why some combat veterans turn to YouTube to tell their PTSD stories because this symptom subcluster limits social functioning (Hassija, Jakupcak, & Gray, 2012; Kerig, Bennett, Chaplo, Modrowski, & McGee, 2016). A number of service members and veterans experience partial or subsyndromal PTSD, yet demonstrate significant psychosocial impairment (Maguen et al., 2013; Pietrzak, Russo, Ling, & Southwick, 2011; Pietrzak & Southwick, 2009).
Many Iraq and Afghanistan veterans who would benefit from mental health services face challenges such as seeking and engaging in mental health services. One national study of OEF/OIF veterans revealed that nearly half who had screened positive for PTSD or depression reported no use of mental health care within the previous year (Tanielian & Jaycox, 2008). In addition, PTSD treatment dropout rates are high, ranging from 28% to 30% (Chard, Schumm, Owens, & Cottingham, 2010; Eftekhari et al., 2013). Barriers to treatment engagement among current and former military personnel include negative treatment beliefs (Spoont et al., 2014; Valenstein et al., 2014; Vogt, Fox, & Di Leone, 2014), trauma-related avoidance, system-level barriers (Sayer et al., 2009), and stigma (Kim, Thomas, Wilk, Castro, & Hoge, 2010; Sayer et al., 2009; Vogt et al., 2014). Social networks have been found to help service members and veterans overcome their concerns and begin treatment (Sayer et al., 2009; Spoont et al., 2014).
Receiving social support and telling one’s story are important needs of many trauma survivors (Caddick, Phoenix, & Smith, 2015; Hundt, Robinson, Arney, Stanley, & Cully, 2015), though the precise reason for this is still under debate. According to Bamberg’s (2004) positioning theory, narrators construct identities by positioning themselves against “master narratives” (p. 335) or dominant social discourses. Constructing narratives is viewed as a reflexive process that helps resolve issues of continuity and change in the self over time by giving a fixed meaning to shared experience (Bamberg, 2010). In traditional therapy, facilitators affirm, challenge, and reinterpret client’s stories to propel them toward a master narrative, which is an agreed-upon set of explanations for troubling thoughts and emotions. Structured social support groups, such as Alcoholics Anonymous, can function in a similar way. Online posting of nontextual videos, stories, or other forms of personal narrative may function likewise. Posts are created and then distributed for the purposes of inviting and collecting commentary through which the self is further evaluated against the dominant narrative of viewers. Online posting differs from traditional narrative sharing in a therapeutic context in that it is often leaderless; affirmation, challenge, and reinterpretation are the venues of all those who share an interest or concern, not just an expert facilitator.
Many military veterans are turning to the Internet for online support options (Salzmann-Erikson & Hiçdurmaz, 2017) in ways that are similar to others experiencing mental health-related conditions. Research shows that receiving online support from persons with a similarly stigmatized condition can challenge shame and promote empowerment (van Uden-Kraan et al., 2008). Online interaction confers particular benefits to persons with stigmatizing conditions whose need for social connection is often harder to meet in offline interactions (Pendry & Salvatore, 2015).
The past decade has witnessed the emergence of Internet-based technologies that enable users to engage in nonwritten forms of storytelling. One of the most popular forms is the vlog. Vlog is a portmanteau for video weblog and can be used as a noun or a verb (i.e., “the act of creating a vlog”; Holtgrave, 2015, p. 190). Although researchers have investigated the use of text-based blogs as a form of social support in chronic disease management (Huh et al., 2014), vlogging is a newer trend and investigations of its use in health management are nascent, with even fewer studies focusing specifically on vlogging for mental health purposes. Vlogging can provide a rich source of information on the experiences of persons with psychological illness that are otherwise difficult to access (Anthony, Kim, & Findlater, 2013). Moreover, for individuals with chronic physical and psychological illnesses, the sense of social connection embedded within the participatory culture of Internet vlogging might create an environment wherein they can share their experiences with others who share similar concerns (Jenkins, Purushotma, Weigel, Clinton, & Robison, 2009).
Reflecting Bamberg’s positioning theory, Raun (2015) describes a vlog as “a kind of diary with constant and continuous updates” (p. 366, emphasis added). In his research with transsexual persons, he viewed vlogs “as a site for autobiographical storytelling” (Raun, 2015, p. 366). Kaminsky (2010) distinguishes a vlog from a video journal in that vlogs are generated for widespread viewing online, while a video journal is created for the sole purpose of self-exploration and can either remain private or become a video blog.
In a qualitative study of vlogs posted to YouTube by persons with diabetes, HIV, and cancer, Huh et al. (2014) found primary motivations for vlogging were to help oneself via self-journaling; to help others by providing encouragement, education, and inspiration; and that these purposes were often intertwined. Though less often observed, other motivations included feeling a need to respond to others and entertaining. Huh and colleagues (2014) also identify several advantages unique to health vlogs in comparison with health blogs (written weblogs) for providing support to chronically ill persons with stigmatizing illnesses. Specifically, the video medium facilitated “intense personal disclosure” (Huh et al., 2014, p. 29) among vloggers. Vloggers often revealed far more personal details about their real identities, with some providing personal email addresses and phone numbers. Also, vloggers with chronic illness were more likely to intentionally disclose their stigmatized status, show their faces, and use their real names. In contrast to blogs, vlogs promoted self-disclosure that led to greater intimacy and connection with viewers, suggesting unique opportunities for social support through visual venues. Huh and colleagues (2014) suggest that the ability to see faces provided credibility and relatability not found in text-based blogs, resulting in strong community-building as reflected in the intimacy of viewer comments.
Only a few recent studies have examined the use of vlogging for mental illness management. In an onto-epistemological analysis, Fletcher (2016) theorized that vlogs of persons with schizophrenia are unique expressions of illness that privilege the accounts of the diagnosed, thereby transforming static understandings of schizophrenia as an isolating illness to one that can be shared. In a qualitative case study, Betton and Tomlinson (2013) explored the lived experience of one YouTube vlogger with schizoaffective disorder and concluded that social media can aid persons with mental illness in their recoveries by reducing social isolation and stigma. In a netnographic qualitative study of vloggers with PTSD arising from sexual harassment, motor vehicle accidents, childhood trauma, crime, and war, Salzmann-Erikson and Hiçdurmaz (2017) found that vlogging not only enabled individuals with PTSD to share narratives about their life conditions, but also functioned as a form of self-care. More recently, in a narrative analysis of YouTube videos, blogs, and discussion forums among persons with PTSD, Salzmann-Erikson and Hiçdurmaz (2017) observed the emergence of therapeutic factors identified by Yalom and Leszcz (2005), most notably, universality (“you are not alone”) and instillation of hope (“if there are people who cope with this, I can too”; p. 292).
Because vlogs are often publicly accessible, they can be used to increase awareness and provide information about mental illness to the viewing community. Liu and colleagues (2013) found individuals with chronic illness used vlogging not only to seek out connection and interaction with viewers, but to also educate them about the strategies they used to manage their chronic health illnesses. In an exploratory study of vlogs posted by people with bipolar disorder, Holtgrave (2015) suggests that the asynchronous nature of the medium is particularly appealing to vloggers with stigmatized mental health conditions. Holtgrave concluded that people with stigmatized conditions can choose what aspects of their identities they wish to disclose and when they wish to disclose them. Power over editing and the enable/disable comments function provide a sense of control and empowerment.
In this exploratory study, we were interested in what motivated OEF/OIF/OND combat veterans to vlog their PTSD stories. Specifically, for what purposes are milvlogs being used, what types of information is being shared, and what can be learned from them?
Method
The purpose of the present study was to describe how OEF/OIF/OND combat veterans communicate narratives of their PTSD experiences via military video web blogs, or “milvlogs,” on YouTube. Officially launched in 2005 and bought by Google a year later (Burgess & Green, 2009), YouTube is a free online digital technology streaming platform that allows registered amateur videographers to upload short videos taken with a cell phone or small camera and unregistered users to view them. Although YouTube is not the only video-sharing platform, it is the largest, boasting close to one third of the universe of Internet users (YouTube, n.d.). YouTube tracks how often a video is viewed, features a box for comments, offers “thumbs up” and “thumbs down” buttons to indicate viewer reactions, and provides a continuously updated tally of viewer votes shown below the video; this feature is useful to researchers who wish to assess the reach of video content.
To achieve the study purpose, we utilized netnography, or “Internet ethnography,”—a “qualitative research methodology that adapts ethnographic research techniques to the study of cultures and communities emerging through computer-mediated communications” (Kozinets, 2002, p. 2). Netnography is particularly useful for studying social media communications in difficult to access study populations (Kozinets, 2010), such as combat veterans experiencing military-related trauma. In this study, we used Kozinets’ (2015) six-step netnographic method (research planning, entrée, data collection, data analysis, ethical standards, and representation). A narrative lens was also used, given our focus on how socially disconnected combat veterans use Internet vlogging to communicate their PTSD stories.
Sample
We selected a sample using critical case sampling, a type of purposive sampling that involves choosing a small number of the most illustrative cases to “yield the most information and have the greatest impact on the development of knowledge” (Patton, 2002, p. 276). Our intention was also do obtain a heterogeneous group of veterans in terms of age, race, gender, and branch of service. We searched vlogs of Iraq/Afghanistan veterans’ self-reported posttraumatic stress stories published on YouTube (i.e., a credible self-proclamation of having PTSD or military-related trauma found either in the milvlog title, description on the YouTube page, or contained corpus of the text of the milvlog). Combat veteran was defined as anyone who deployed (active duty, National Guard, Reserves) to Iraq and/or Afghanistan from the outset of the war in Afghanistan in 2001 to the conclusion of the study at the end of February 2017. To better understand why veterans turned to the Internet to share their military-related trauma stories, we chose a sample of milvlogs featuring elements of the socially impairing nature of trauma, including PTSD. We defined social disconnection/impairment as expressions of feeling lonely, misunderstood, isolated, detached from others, or experiencing relationship difficulties, expressed either in the milvlog or on the poster’s YouTube page. Illustrative cases were those vloggers who featured the richest descriptions of the PTSD experience (i.e., description of at least one of the 20 PTSD symptoms listed in the DSM-5 (APA, 2013), combined with details about the associated relationship distress or social impairment experienced by the vlogger as a result. Milvlogs that did not feature both a description of a PTSD symptom and its accompanying social impairment were not considered as illustrative cases. This study retrospectively examined previously published milvlogs and relied on observation of 17 publicly available milvlogs published by 17 unique vloggers.
Data Collection
We chose YouTube as a source of rich data via audiovisual, narrative, and interactive content. To locate potential milvlogs, we used YouTube’s relevance-based search mechanism and the advanced features of Google search, inputting keywords to retrieve results. The search terms were PTSD, posttraumatic stress, post-traumatic stress, soldier, veteran, Marine, military, combat, National Guard, reserves, Airman, Navy, Army, and Air Force. Inclusion criteria included (a) audible quality, (b) English language, (c) military vlogger, (d) description of at least one or more posttraumatic stress symptoms related to OIF/OEF/OND deployment, and (e) description of how the symptom(s) impaired social functioning. Exclusion criteria were (a) videos uploaded by government, professional, educational, veteran groups, or news organizations; (b) stories about someone else with posttraumatic stress; and (c) product or commercial endorsements.
The lead researcher conducted an initial search resulting in 12,800 total results; she then scanned the results until PTSD or “posttraumatic stress” was no longer included in the title. From the resulting 600 vlogs, she eliminated 401 irrelevant results (i.e., search hits that were not PTSD stories posted by military veterans) and excluded another 125 milvlogs that did not meet inclusion criteria. Of the remaining 25 milvlogs, 17 contained enough information to fully answer the research question (i.e., milvlogs of a PTSD story that met inclusion criteria, contained a description of at least one DSM-5 PTSD symptom, and included a description of how that symptom affected social functioning). The research team unanimously assessed the selected milvlogs to be authentic accounts of war trauma. For vlog attributes, we captured vlog title, date, vlogger name, length, numbers of views, comments, likes, and dislikes. For descriptive information, we recorded observed and/or self-reported vlogger gender, race (i.e., White, Non-White), and if provided, branch of service, and deployment location. In most all cases, marital status and age were not obtainable through the milvlog posts. This information is summarized in Table 1. PTSD diagnoses were self-reported by the vloggers.
Demographic Variables of Vloggers Included in the Qualitative Analysis.

Note. OIF = Operation Iraqi Freedom; OEF = Operation Enduring Freedom; OND = Operation New Dawn.
Data Analysis
We used an inductive approach to examine the visual elements and the corpus of the transcribed text of milvlogs posted by U.S. combat veterans about their personal narratives of military-related trauma. Over a 6-month period, the 17 milvlogs selected for analysis (totaling almost 3 hours of video) were viewed multiple times each, both separately and together by the lead researcher and a research associate. The audio from the milvogs was professionally transcribed and verified for accuracy by the researcher. The research associate assisted with the content analysis and with coding the audiovisual elements and text of the milvlogs, as well as recording and coding scene-by-scene descriptions for the two unnarrated milvlogs. QDA Miner 4.1.29, a mixed-methods qualitative software program, was used to assist with data management and analysis.
We conducted a qualitative thematic analysis of transcribed texts from milvlogs combined with a quantitative content analysis strategy to evaluate milvlog analytics and attributes. Using an open coding process to develop the codebook, we separately identified preliminary codes relevant to the research purpose. Coding involved clustering significant statements (i.e., phrase or sentence-length statements that conveyed vloggers’ military-related trauma experiences) into units of meanings and synthesizing them into themes to create an integrative description portrayed in the 17 milvlogs. Moving from tentative codes to final codes was an iterative process where we continuously revised, refined, and merged codes to generate a subset of themes, as recommended by Creswell (2013). Initially, we identified 555 significant statements from the milvlogs. We met on several occasions to collapse these into 31 clusters of meaning, and distilled these meaning clusters into 18 themes, which were further reduced to seven themes.
Evaluation Criteria
The research team consisted of five individuals: a licensed clinical social worker in the dissertation phase of a doctoral program with 10 years of experience treating combat trauma in military populations, and four research associates—a military family member in the dissertation phase of a doctoral program, two social work professors with extensive qualitative research experience, and a PhD-level Licensed Clinical Social Worker with almost 20 years of experience treating PTSD and comorbid mental health problems in combat veterans.
According to Lincoln and Guba (1985), rigor in qualitative research can be demonstrated through credibility (i.e., confidence in the veracity of findings), confirmability (i.e., degree to which findings result from participants and are unbiased by researcher), dependability (consistency and repeatability of findings), and transferability (i.e., applicability of findings to other settings). To increase credibility of study findings, the research team triangulated methods by conducting both a thematic analysis of vlog texts and a content analysis of vlog attributes. Multiple sources of data were used, including both the text of the vlogs and the vlog descriptions from the YouTube page. Finally, credibility was enhanced by inviting vloggers who left contact information in their YouTube “About” pages to participate in member checks. Two vloggers indicated the findings accurately reflected their experiences; additional details were added in response to feedback from a third participant.
To establish dependability, we consulted a PhD-level expert on combat PTSD, who assessed that the study’s conclusions were supported by the data. To ensure transferability, thick and rich descriptions of combat veterans’ posttraumatic stress stories are presented. We ensured confirmability through reflexivity—continuously checking for any evidence of bias or distortion throughout the study. Field notes were also maintained during the data collection and analysis processes, which facilitated thoughtful reflection before and during all phases of this study.
Ethical Considerations
Before beginning this research, we obtained University Institutional Review Board approval for this study. Although publicly available data were used, we engaged with participants and sought their consent. Of the 17 vlogs selected for inclusion, only 12 vloggers provided contact information. To gain entrée (Kozinets, 2015) to the vlogger community, the lead researcher sent an email describing her qualifications and interest in the military vlogger community. Ten of the 12 vloggers responded to an email explaining the purpose of the study and gave permission for the use of their vlogs in the study. Quotes from vlog transcripts were used only with the permission of the vlogger or (for those vloggers who were unable to be contacted) if the quote did not appear in the first 20 results of the YouTube search engine to ensure quotes were not readily identifiable through a reverse search. Member names and vlog URLs were concealed to ensure participant privacy.
Results
A first step in analysis was to conduct a content analysis of the milvlogs to present a description of the audiovisual elements and features of the milvogs. Following a report on the milvlog characteristics and analytics, we present data on how OEF/OIF/OND combat veterans communicated narratives of their military-related trauma experiences through milvlogs.
Audiovisual Elements and Analytics
We analyzed each of the 17 milvlogs for setting elements, themes, and the overall emotional presentation of the vlogger. In every case, vloggers revealed their faces, although in one vlog, the veteran only showed a still photo throughout, accompanied by narration. In another, only the vlogger’s upper face and eyes were visible. In 12 of the 17 milvlogs, vloggers identified themselves using both first and last names. In each milvlog, the veteran was seated or standing in front of a camera with a relatively bare, sterile background, although one vlogger, an Afghanistan veteran, narrated his story on his walk home from work late one evening. Another vlogger, who served in Iraq, filmed his video in a hotel room. Two milvlogs displayed personal photos in the background, blurred out in one and indiscernible in the other. Two vloggers had division flags in the background. A few displayed tattoos with military themes. One vlogger shook his bottle of medicine in front of the camera. In another, a vlogger displayed a large plastic medicine planner filled with his weekly supply of pills. Two milvlogs were filmed without narration, instead using a series of scenes set to music that depicted a typical life in the day of a person with PTSD. For milvlogs without narration, the research team coded scene-by-scene descriptions recorded by two members of the research team during independent viewings. Military themes (e.g., medals, maps) were much more prominent in the unnarrated milvlogs.
For most vlogs, the overall emotional tone was sadness. One vlogger appeared quite angry and identified his milvlog as a “rant.” Several milvlogs devolved to despair and anguish over the course of the video. The vloggers had varying levels of videography skill; about half used advanced editing techniques (e.g., transitions, text overlays, music, sound effects, overhead scenes). Two vloggers indicated they had some degree of professional videography training.
Milvlog features were identified by examining the content and analytics of the YouTube milvlog page and the vlogger’s YouTube site. Milvlog characteristics are summarized in Table 2. The 17 milvlogs included in the study were published between 2008 and 2017. Milvlog lengths ranged from just over 1 minute to almost 26 minutes (M = 10:21). Ten milvlogs contained social media links, with Google Plus, Facebook, and Twitter being the most popular. Other social media sites included Instagram, Pinterest, Reddit, Tumblr, Twitch, and Vine. Two milvlog sites provided links to the National Suicide Hotline and the Veterans Crisis Line. One of these also included links to PTSDchat.org and Military OneSource. Three milvlogs had donation buttons where viewers could provide financial support to these vloggers’ YouTube sites. Seven vloggers interacted with commenters on the vlog site (see Table 2 for number of comments). It is unknown how many communicated using other forms of social media.
Milvlog Characteristics.
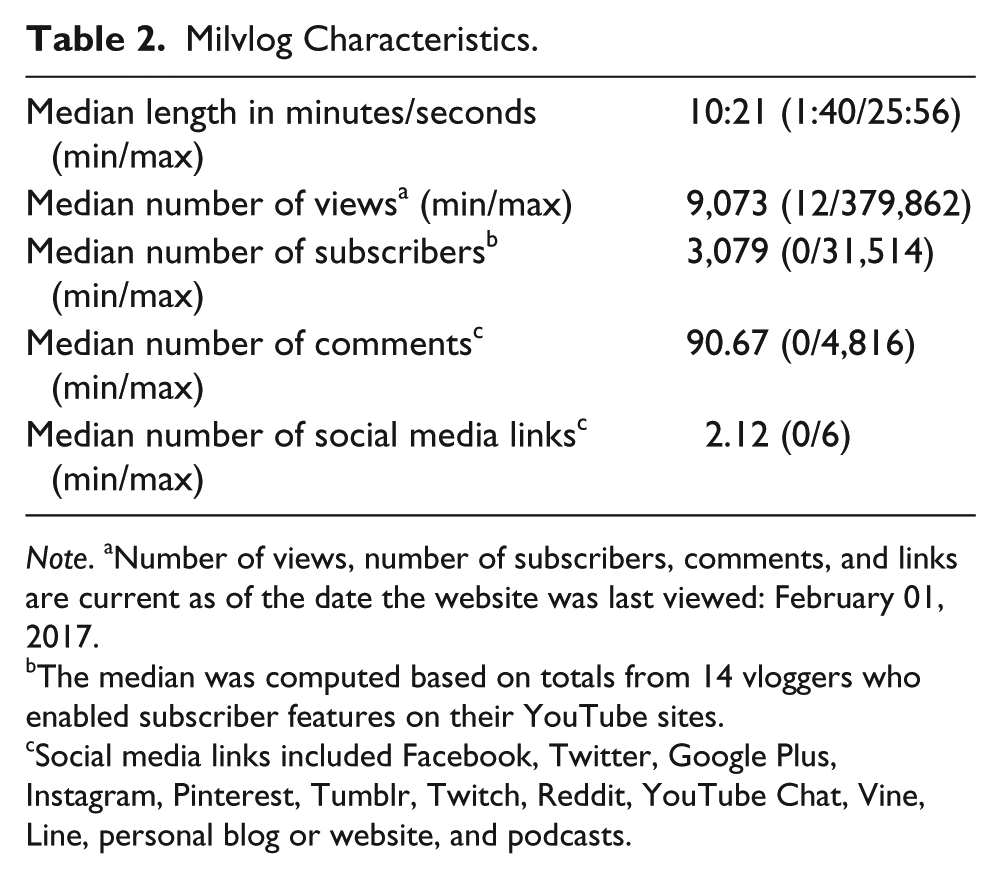
Note. aNumber of views, number of subscribers, comments, and links are current as of the date the website was last viewed: February 01, 2017.
The median was computed based on totals from 14 vloggers who enabled subscriber features on their YouTube sites.
Social media links included Facebook, Twitter, Google Plus, Instagram, Pinterest, Tumblr, Twitch, Reddit, YouTube Chat, Vine, Line, personal blog or website, and podcasts.
Themes Related to Narratives of PTSD Experiences
Motivation: “I make these videos because . . .”
A central theme of these vlogs was an explicitly stated motivation by veterans for self-publishing their stories to YouTube, either in their milvlog description or in the milvlog itself. Most wanted to help others better understand the experience of having PTSD. A vlogger who identified himself as an Army combat infantryman said, “I really want to help a lot of people out there that may not understand us.” Others wanted to assist fellow survivors, as seen in this quote by a former Army ranger: “This is it. PTSD in a nutshell. Maybe you laughed. Maybe you learned something. But hey, if it helped one guy out there, it’s well worth it.” Reflecting the therapeutic aspect of universality, several vloggers used the video medium to reassure others they were not alone, as illustrated in this quote: “I realized I wasn’t by myself. I met people who suffer from PTSD just like I did . . . This is not something to try to deal with on your own.”
Based on milvlog descriptions and data from the corpus of the texts, most vloggers posted their milvlogs to help others, while reaping self-therapeutic benefits, as expressed by an Iraq combat veteran: “I’m doing these to help my treatment and shed some insight on what PTSD is.” Two vloggers wished to combat the stigmatized perception of veterans with PTSD. “I can talk what I think to myself . . . alone,” stated a veteran of Afghanistan, alluding to the unique therapeutic benefits of the medium for veterans with PTSD who want to process their experiences, but struggle with expressing themselves in therapeutic settings.
Loss: “One of the hardest things.”
Loss was a second theme found in the PTSD stories told via milvlogs. One type of loss was the permanent psychological change that came from experiences in war. Addressing friends and relatives of veterans with PTSD, a former Army infantryman expressed, “They notice there’s something very different about them. Of course, everybody changes, especially after deployment. They’re in survival mode . . . in reality, they’re not the same.” Likewise, a vlogger serving as a combat infantryman shared, “There have been several events in my life, over this past tour, that I feel have changed me forever.”
Some veterans described experiencing major losses of those close to them. One recalled watching a friend die as the “hardest thing” he experienced during combat. A vlogger in his early 20s reflected, “I returned from my year-long tour in Afghanistan . . . By that time in my life, I had already lost seven close friends.” Another expressed profound grief over losing friends and battle buddies in combat. A grieving combat infantryman described the sudden loss of a friend who died in an improvised explosive device (IED) attack: “His vehicle got blown up and he died before I even got overseas.”
Some vloggers shared an overwhelming sense of frustration and sadness over how their PTSD had damaged relationships. An Iraq veteran, alone in a hotel room and anguished over not having seen his infant son for months, stated, “He was my hope for the future, he was my support . . . Now my ex wants to gain full custody or have me waive my rights. She’s using my PTSD, my TBI [Traumatic Brain Injury] against me.”
Managing symptoms: “I’m losing my fricking mind.”
All the vloggers expressed concerns about symptoms associated with PTSD, notably hypervigilance, numbing, sleep disturbances, anger, and substance misuse. Hypervigilance was the most frequently acknowledged symptom and was depicted in the two unnarrated vlogs. Others struggled with feeling numb. An Army ranger with multiple deployments to Iraq described how the compartmentalization required to survive in war manifests as emotional numbing upon return: “You get used to shutting off your emotions. You come back—it’s real hard to turn them back on.” Sleep was elusive for most vloggers.
Anger was another common complaint among vloggers in this sample. This was best illustrated by a combat infantryman who said, “You become blinded by anger . . . it was either holes in the wall or dishes were broken, or, you know, my knuckles were bloody or something was broken or torn up.” Addressing family members, one veteran described how anger is often a secondary emotion for underlying emotional torment: “When we’re angry we’re not yelling at you, we’re yelling at ourselves and the pain we feel.”
Another concern illustrated in milvlogs was drug and alcohol use to cope. When discussing her experience with PTSD, a former Marine simply stated, “I drank my face off.” Another former Marine shared, “I got into drugs. I started out with prescription pills and then when that got too expensive, I went into harder things like heroin. It was basically just to quiet my mind and to relax, to forget.”
Help-seeking: “Help me!”
For some, stigma associated with PTSD interfered with seeking mental health services. Referring to the movie, First Blood (Kotcheff, 1985), in which a Vietnam veteran with PTSD engages in combat with law enforcement in a small U.S. town, one veteran of Iraq spoke out against the negative societal perception of veterans with PTSD, proclaiming, “I ain’t no John Rambo, I ain’t no psychopath.” A combat infantryman shared how stigma interfered with his help: “It was like something was wrong with you, so I waited a good four years before I finally asked for help.”
Over half of the participants expressed concerns about seeking care through the Veterans Administration (U.S. Department of Veterans Affairs [VA]) or Department of Defense (DOD). Vloggers relied heavily on VA care but believed the VA was not meeting their needs. Specific concerns included long waiting periods to see someone, a lack of providers who could prescribe medication, inexperienced practitioners, providers with no combat experience, and providers without proper credentials to provide specialized care.
One veteran stated, “In some cases it takes two to three weeks to see a therapist.” Another indicated his doctor prescribed medication for him without ever having seen him. Some vloggers expressed concerns over the quantity of medication they were being prescribed, with one Iraq veteran stating, “I take about 12 pills a day, I don’t want to take 12 pills a day.” Another stated, “They just loaded me up with meds.”
A Marine who served in Iraq shared his frustration with mental health providers naive to war. Another veteran shared a dissenting view on the helpfulness of mental health providers who had not seen war, stating, “she’s not a combat vet, but . . . she’s a great listener and she’s very honest. She tells it to you like it is.”
Despite any issues with help-seeking, veterans still felt that it was important to get help to cope with symptoms. Emphasizing the importance of seeking help, an Afghanistan veteran proclaimed, “A person with PTSD that wants to be better will seek treatment. He will do what he can to keep his demons at bay.” Even though they saw PTSD as lifelong struggle, vloggers overwhelmingly believed symptoms could improve, as shown in this statement by a veteran who spent 48 months in Iraq: “You can fight this . . . if you’re dealing with PTSD . . . It can get better.”
Some vloggers held out hope that needed improvements in the VA, including the Veterans Health Administration, would manifest. A former military policeman sent out a call to action to veterans to spearhead needed changes in the VA: “Just because the VA is not what you want it to be, it doesn’t mean that you can’t make it what you want it to be . . . We have to make our VA better!”
Guilt and shame: “Don’t thank me for my service.”
About half of the participants expressed feelings of guilt in their vlogs, even in the ones not narrated. Reflecting on his own survival, a combat veteran in his late 20s wondered why five others were killed instantly by an IED but his life was spared. Like him, many vloggers were wracked with feelings of guilt and shame because they survived, but fellow warriors did not. One noted, “Samurais used to kill themselves over shame.” He went on to describe the connection between guilt and shame as “Soul cancer. This is the one where people kill themselves over all the time. It’s where you have to do something that conflicts directly with your ethics, morals, or values.” An Iraq veteran captured the moral complexities of combat believed by some experts to contribute to PTSD due to moral injury: I didn’t want to kill people; I wanted to kill monsters and I saw terrorists as a monster . . . but I didn’t see monsters, I saw people. There were kids that were used as bombs by terrorists and we couldn’t save them you know.
Suicide: “PTSD won’t take my life.”
Most of the vloggers struggled with past thoughts of suicide and memories of comrades who had died by suicide. One combat veteran observed that not everyone with PTSD survives it: “During my 4 years of intensive treatment, I met countless people who were going through the same thing I was. Some of those people are no longer here due to suicide.” Several vloggers referenced worrisome suicide statistics, as in the words of this Army combat infantryman: “Recent years have shown us that there are more veterans that are committing suicide than the 22 [per day] that was reported earlier by the Department of Veterans Affairs.”
For suicidal veterans with PTSD, getting needed help can be lifesaving. An Afghanistan veteran in his early 20s expressed the importance of finding support to survive PTSD: “I would go in and out of wanting to kill myself. Luckily, I went and got help.” Another vlogger who had served in Afghanistan cautioned, “Don’t wait until it’s too late. Your family loves you.”
Connecting to other veterans: “Other vets can talk to other vets because they’ve been through it.”
Most vloggers described a profound loss of connection to others after returning home—to a country that seemed to no longer understand them. A Marine veteran disclosed, “You can’t really relate to anyone else in the world [because] of what you’ve done . . .” One veteran of Afghanistan questioned, “What could I tell you to help you understand?” With a sigh, he answered himself, “Some things should be bottled up for a reason and never be shared with anyone . . . or only with people as messed up as you are.” He went on to describe his experience speaking to a veteran of a previous war era who told him, “I served in Vietnam. I had a very similar . . . experience to you.” Another vlogger recalled, “I talk to World War II vets that they still have Normandy in their mind or they may have North Africa in their mind. I’ve talked to Vietnam vets who [say] Vietnam is still fresh in their mind.”
Discussion
This study is the first to focus on OIF/OEF/OND veterans who self-published their stories about military-related trauma to YouTube. The research adds to the nascent literature on how combat veterans use vlogging to tell others about their war trauma experiences. Through analysis, we found seven overarching themes that related to how combat veterans communicate narratives of their PTSD stories through milvlogs. In essence, vloggers expressed feelings of alienation as they struggled with coping and self-management in a social environment that offered little understanding. As a positive response, they turned to YouTube as a way to tell their stories, connect with others, combat stigma, address issues of paramount concern to veterans—mental health care and military suicide—and engage in advocacy efforts.
Our findings suggest that vlogging served as a medium that facilitated connection with others, in individuals whose illness otherwise increases the likelihood of social isolation. Vlogging may, therefore, be a vehicle for telling stories that might not otherwise be told. Veterans who share their military-related trauma narratives via vlogging have control over their stories—how much to tell and when, and the ability to edit comments. Many vloggers were motivated by a desire to provide support to others as well as to receive support. Survey research conducted by Foster (2013) of people who used YouTube for mental health reasons found that providing support to others was ranked higher than any other motivation. Regarding our theme of motivations, most veterans in our sample had a variety of reasons for choosing to tell their stories on YouTube. These reasons included some combination of the functions of vlogging found by Holtgrave (2015) in her study of individuals with bipolar disorder, most notably providing information, forming community, and mitigating stigma. However, unlike people with bipolar disorder, the vloggers in this study also engaged in grassroots advocacy efforts, such as providing weblinks on their vlog pages to PTSD and military suicide prevention resources. One vlogger even issued a call to action to all veterans to take responsibility for spearheading improvements in the VA health care system. Our findings were consistent with those of Pendry and Salvatore (2015), who suggested that online forum users with stigmatized conditions who have positive experiences online likely experience improved well-being, and thus become “empowered and galvanized” to participate in civic engagement activities (p. 217).
Vloggers struggled with managing symptoms, particularly hypervigilance, numbing, anger, sleep disturbances, and substance misuse, which persisted many years after combat (Solomon & Mikulincer, 2006). Using in-depth interviews, Lee, Vaillant, Torrey, and Elder (1995) observed the intractability of PTSD symptoms in combat veterans as late as 50 years after the end of World War II (WWII). Another theme central to these veterans’ PTSD stories was loss. Vloggers experienced a loss of self and important relationships and the loss of friends and battle buddies through death. Vloggers in this sample turned to YouTube to process feelings of alienation and grief. According to Westphal and Convoy (2015), the traumatic death of a military buddy can be akin to the loss of a spouse, parent, or sibling. Vloggers also noted the persistence of feelings of loss. Harvey, Stein, and Scott (1995) who interviewed Normandy Invasion veterans 50 years after D-Day, found that unresolved grief over deaths of friends persisted many years later.
With regard to help-seeking, subthemes included stigma and issues with care. For some participants, perceptions of stigma interfered with seeking needed mental health services. The impact of stigma as a barrier to help-seeking in veterans with PTSD is supported by evidence from multiple studies (Blais & Renshaw, 2013; Kim, Britt, Klocko, Riviere, & Adler, 2011; Ouimette et al., 2011).
Statements from some vloggers seemed to indicate ambivalence about seeking care. On one hand, veterans acknowledged that seeking help is necessary; yet, some also described a mistrust of service providers. Previous research has also found that negative treatment beliefs act as a barrier to seeking treatment for PTSD for veterans (Spoont et al., 2014; Valenstein et al., 2014; Vogt et al., 2014). Likewise, vloggers in this study expressed concerns about counselors who lacked understanding of the combat experience, though some had positive beliefs about the potential benefits of treatment even if they were not accessing it. Other previously identified barriers to help-seeking were found in our data, including long wait-times for care, problems accessing appropriate qualified providers, and the avoidant and socially isolating nature of trauma symptoms.
Vloggers in our sample also expressed guilt and shame about what they perceived as morally injurious actions they took during their combat experiences. Moral injury, defined as “perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held moral beliefs and expectations,” is a recent construct useful in describing the profound spiritual changes observed in many combat veterans (Litz et al., 2009, p. 695). One vlogger, in particular, shared his feelings of guilt and shame over seeing enemy soldiers as people and not monsters. In fact, combat veterans’ struggle with the humanity of the enemy puts them at risk for moral injury (Currier, McCormick, & Drescher, 2015). PTSD experts have identified guilt and shame associated with moral injury as important emotions to address when treating PTSD in combat veterans (Bryan, Morrow, Etienne, & Ray-Sannerud, 2013; Litz et al., 2009).
Suicide was also evident in the military-related trauma narratives, with some vloggers struggling with their own suicidal feelings, yet, the majority being personally affected by suicide deaths of fellow veterans. Feelings of social isolation and loneliness are often related to depression (Hawkley & Cacioppo, 2010) and risk factors for suicide (Van Orden et al., 2010). In general, vloggers were deeply concerned about the problem of military suicide and wished the VA to do more for veterans dealing with suicidality. Given that military suicide has received considerable public attention over the past few years (Kang & Bullman, 2009), it is perhaps unsurprising that this issue was prominent in the vlogs.
Finally, most vloggers felt the only people who could really understand them were fellow veterans. Anecdotally, it is common for those with a nonnormative experience to report being better understood by another person who had a similar experience. There are a number of ways to understand this phenomenon. From a clinical perspective, we believe this finding supports Bamberg’s (2010) assertion that narrative is a reflexive process. Stories, diaries, and weblogs are not single events, but invitations to commentary that will be used to reinterpret narrative. In traditional therapy, the therapist facilitates reinterpretation of client narratives to create change. Self-help groups often have the same effect. Vlogging appears to be an extension of these processes, though the particular benefits and risks associated with vlogging are still largely unknown.
Implications
OEF, OIF, and OND veterans are the first large-scale veteran cohort to return to civilian life during the period of rapid technological development that began in the late 1990s. They are the first group of veterans to use Internet technology on a large scale to tell their stories. This research is among the first to investigate the uses and potential impact of military video blogs (milvlogs) among veterans who have experienced combat-related trauma. We thought it was important for researchers to document the content and usage of milvlogs for this population as a foundation for additional research. This descriptive study can help behavioral health providers gain insight into service members’ and veterans’ experiences with PTSD.
Previous research has shown that telling one’s story is often important to trauma survivors (Hundt et al., 2015). Telling one’s story serves to break the isolation that often accompanies stigmatized health and mental health conditions (Caddick et al., 2015). Positioning theory (Bamberg, 2004) suggests that narrators construct a counternarrative to what is perceived as a master narrative, or dominant social story, on various events; however, stories are, by nature, social events. Counternarratives, to be credible, must be shared and affirmed by others. Many of the milvloggers commented on the guilt, shame, anxiety, or deep confusion that arose when social norms that are appropriate in noncombat settings, such as sacrificing oneself for a friend or seeing children as having good intentions, are unachievable or violated in combat. As posited by Bamberg (2004, 2010), milvlogs appear to be a means of reaching others with similar experience who can affirm the counternarrative, that is, place the norm violation in its appropriate context. Milvlogs are created and distributed in the hopes of finding other veterans for whom the counternarrative is relevant and can be affirmed.
Military veterans are turning to the Internet for online support in ways that are similar to others experiencing mental health–related conditions (Salzmann-Erikson & Hiçdurmaz, 2017). Research so far suggests that online interaction confers particular benefits to persons with stigmatizing conditions whose need for social connection is often harder to meet in offline interactions (see Pendry & Salvatore, 2015). However, the current literature is insufficient to draw firm conclusions. Positioning theory is likely to be useful in addressing the long-term therapeutic benefits and risks associated with publicly presenting one’s personal counternarratives. For example, do counternarratives serve to reisolate narrators by drawing negative reactions from people who cannot identify with the combat context? On a related note, what happens when fellow veterans disaffirm, contradict, or deny the legitimacy of the milvlogger’s counternarrative? Both of these questions will require longitudinal study.
Mental health researchers and providers should be aware of technological innovation in storytelling among those with trauma-related concerns, including veterans. Milvlogs can serve as a resource and educational tool for learning about their combat-related trauma, including how veterans struggle with traditional mental health treatment programs. Vlogs can help providers identify psychological and structural barriers that hinder care, as well as provide insight into combat veterans’ perceptions of existing service gaps. In this study, one perceived gap was a lack of behavioral health providers who can treat combat-related PTSD. Another was a concern that military suicide is not being adequately addressed.
Evidence about the role of vlogging for veterans with PTSD and combat-related trauma is only now emerging, but it is important for clinicians to discuss the benefits and risks of participating in online activities related to their trauma. This study supports the idea that milvlogs function much like textual storytelling. Many of the veteran participants found therapeutic benefit in telling their stories via video. While the vlogs were publicly available, they were clearly produced with the needs of other veterans who might be having similar experiences in mind. Vloggers formed a comradery with others that tended to help normalize their experiences. Vlogging might also serve as a way for people who are not ready or able to manage their trauma-related problems to become more comfortable with the idea of attending therapy.
While there are benefits to vlogging, there are potential risks that have not been adequately explored. For example, vloggers risk unintended consequences for their current or future employment, litigation, and family relationships due to the public but highly intimate and personal nature of their self-disclosures (Rodewig, 2012). Vlogs and other online commentary can be accessed indefinitely and shared indiscriminately over the Internet, in some cases even after individuals have taken steps to take them offline. Furthermore, in the online environment, any public disclosure or comment invites potentially damaging “hate” comments that disapprove of the vlogger’s lifestyle or elements of the video content (Huh et al., 2014). Such disapproval might be damaging to individuals who are in a vulnerable state. To the extent possible, mental health professionals should be aware of these risks and be prepared to discuss the risks with those who have submitted vlogs or have plans to do so.
Not only did vloggers in this sample create informal support communities, but also some bridged service gaps by engaging in grassroots efforts to improve outreach, education, and support to service members and veterans struggling with PTSD and suicidality. This was done by including web links to professional treatment and military suicide prevention resources on their milvlogs. Mental health interventionists will need to be aware of the potential of vlogs to provide social support and links to helpful services. At the same time, they will need to be in a position to help clients evaluate the value, need, and effectiveness of services.
Some of the milvlogs in this study garnered thousands of views and hundreds of comments. Another issue this presents for mental health professionals involves how they should link to these types of web-enabled support groups, if at all. Encouraging more vloggers to add PTSD treatment and suicide prevention links on their video sites could aid existing treatment and military suicide prevention efforts by reaching vulnerable service members, veterans, and military family members who were motivated to seek out PTSD milvlogs because of their own struggles coping with personal or loved ones’ symptoms. At the same time, one of the reasons milvlogs are effective is that they are perceived as exclusive to “people like us.” Even though they are publicly available for viewing, too much comment or interference from people who are “outside” the group might be viewed with mistrust.
Study Limitations
This study had three limitations that readers should consider. First, although vloggers self-reported having posttraumatic symptoms and/or having been diagnosed with PTSD, the authors did not perform clinical interviews with participants and were therefore unable to confirm participants’ reported diagnosis. Furthermore, because self-report was used to ascertain diagnoses rather than clinical interviews, we were unable to assess the degree to which comorbidity may have played a role in vloggers’ preference for a web-based interaction format. Second, YouTube is the most popular video-sharing medium; however, there are others. For example, we did not look at milvlogs published using other video-sharing platforms such as Vimeo. Future research efforts might focus on PTSD milvlogs published using multiple video-sharing platforms. These two limitations affect transferability of findings to veterans with a confirmed PTSD diagnosis and to those who use less popular or alternate video platforms. A third limitation is that we did not explore how viewing another’s military-related trauma story affected viewers and if messages about suicide and suicide prevention resources provided through this medium are effective. Addressing this information in future research will help researchers and clinicians better evaluate the extent to which milvlogs are helpful and useful to veterans.
Conclusion
Milvlogs are emerging as a form of education, social expression, and social support for war veterans with PTSD. Vlogging offers war veterans an alternative platform for telling their stories, potentially decreasing social isolation and stigma, and encouraging social action. PTSD often includes discomfort with the live social interaction required in more traditional therapy settings. Vlogging offers an alternative means of sharing one’s PTSD story with others as vloggers can tell their stories without being overwhelmed by the presence of others, yet still be able to connect with viewers and commenters attracted to their milvlog pages. This mode of sharing stories has the potential to facilitate therapeutic engagement because it gives veterans a way to feel safe sharing their concerns. In this study, our results suggest that some veterans are using vlogging to speak out on issues of paramount concern to the greater military and veteran community, such as suicide prevention and problems accessing VA services; thus, vlogs might also serve as a means for veterans to advocate for their health and mental health needs.
Footnotes
Acknowledgements
The lead author wishes to thank her dissertation committee, particularly Dr. Donelle Barnes and Dr. Regina Praetorius, for their assistance with the original study. In addition, we wish to thank Dr. Rosalind Evans for assistance with coding and Dr. Donald Schuman, LCSW, SGM, USA-Ret, for sharing his expertise on combat-related PTSD.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.