
Abstract
Fatal opioid overdoses can be prevented by opioid overdose prevention programs (OOPPs). The present study qualitatively examined the diffusion process of an OOPP among 30 persons who inject drugs (PWIDs) in an opioid-saturated community. Purposive sampling was used to recruit participants into three groups based on familiarity with the OOPP. Findings revealed that participants often adopted the OOPP, which was offered by a local harm reduction organization, if first exposed by staff hosting and implementing it. Barriers to adoption included belief that OOPP training was lengthy or unnecessary, lack of perceived relative advantage, nonengagement with the host organization, and trepidation of administering withdrawal-causing medication to fellow PWIDs. Participants outside of networks diffusing the OOPP were isolated from other PWIDs. Staff from the host organization were influential in encouraging OOPP adoption, which underscores their importance in the effort to reduce fatal overdoses.
Keywords
Introduction
The drastic uptick of fatal opioid overdoses in the United States throughout the past 15 years necessitates attention to ensuring effective public health programmatic responses (Rudd, Seth, David, & Scholl, 2016). A fatal opioid overdose is an acute condition occurring on the intake of an excessive amount of an opioid resulting in unconsciousness, respiratory depression, and ultimately death (World Health Organization [WHO], 2017). In 2017, over 72,000 persons died from a drug overdose in the United States (Centers for Disease Control and Prevention [CDC], 2018). In 2017, there were more than 1,200 overdose deaths in Philadelphia, a then city of 1.568 million (Philadelphia Department of Public Health [PDPH], 2018), which was the second highest in the nation in cities of more than 1 million persons, following Pittsburgh (CDC, 2017; as cited in PEW Charitable Trusts, 2018; U.S. States Census Bureau, 2018). In Philadelphia, the majority of opioid overdose deaths are attributed to heroin or fentanyl (PDPH, 2018; Philadelphia Medical Examiner’s Office [PMEO], 2016). Use of both heroin and fentanyl is on the rise in Philadelphia, which is often preceded by misusing opioid pain medication (OPM) (Lankenau, Teti, et al., 2012; Muhuri, Gfroerer, & Davies, 2013). Contributing factors to transitioning from OPMs to heroin and fentanyl include lower cost, better availability, and increased potency (Ciccarone, 2017, Cicero, Ellis, Surratt, & Kurtz, 2014; Lankenau, Teti, et al., 2012; Mars, Bourgois, Karandinos, Montero, & Ciccarone, 2014).
The most effective means of preventing an opioid overdose from becoming fatal is with the administration of naloxone, an opioid antagonist that was previously only available to emergency medical personnel (Wheeler, Jones, Gilbert, & Davidson, 2015). Prior to the development of opioid overdose prevention programs (OOPPs), overdose witnesses often had to rely on calling 911 for overdose victims to receive naloxone. However, most witnesses to drug overdoses are other drug users, for whom there are multiple known barriers to calling 911 (Tobin, Davey, & Latkin, 2005). Response to these barriers from the public health sector include the implementation of OOPPs into at-risk communities (Wheeler et al., 2015). OOPPs are training programs that teach laypersons effective rescue response to a witnessed overdose and equip them with naloxone. This program falls under the spectrum of harm reduction interventions, a framework used worldwide to reduce the harmful effects of illicit drug use including HIV and Hepatitis C (HCV) transmission, and other harms associated with drug-use stigma (Harm Reduction Coalition, 2018). Other programmatic examples include syringe access programs, which have demonstrated consistent effectiveness in reducing HIV transmission and typically offer access to drug-treatment services for interested persons (Bramson et al., 2015; Hall et al., 2008). OOPPs have shown much promise in curbing fatal opioid overdoses (Wheeler et al., 2015).
For public health programs like OOPPs to have impact, they must successfully diffuse among at-risk communities. To investigate the diffusion of OOPPs, a framework like the diffusion of innovation describes how new concepts, such as health programs, are circulated, adopted, and maintained within social systems (Rogers, 2002). Application of this framework offers insight into a program’s dissemination and adoption processes, which in turn offers opportunities for addressing potential programmatic barriers. Several studies (Clark, Wilder, & Winstanley, 2014; McDonald & Strang, 2016) have investigated the effectiveness, knowledge change, and barriers to OOPPs. However, none have investigated the diffusion process of an OOPP in an opioid-saturated community such as the study’s setting. To that end, the purpose of the present study was to assess the diffusion of an OOPP in a high opioid use setting, to identify ways that the program was disseminated and adopted among persons who inject drugs (PWIDs), and to identify barriers and gaps in the diffusion process.
Program
In 2006, an OOPP was established in Philadelphia, in an area characterized by open-air drug markets and the highest concentration of overdoses in the city (PDPH, 2018; PMEO, 2016). The OOPP’s host organization is the city’s only comprehensive harm reduction facility, which also operates the city’s only authorized syringe-exchange program. The OOPP is facilitated by trained host organization staff in which participants learn risk factors associated with overdose, signs and symptoms of an overdose, and how to effectively respond to an overdose including suggestions to call 911, administer rescue breathing, and administer naloxone. Participants are given a kit containing printed overdose response training instructions, two doses of naloxone (intranasal or intramuscular), nitrile gloves, and alcohol pads (Personal Correspondence, Project Coordinator, September, 2016). Since 2006, this OOPP had trained 4,779 persons.
Theoretical Framework
Developed in 1962 by E. M. Rogers, the diffusion of innovation theory describes how a new concept gains momentum over time within a social system and is subsequently adopted or rejected (Rogers, 2002). For public health research, the new concept might be a health program, like an OOPP. With any innovation, individuals first become exposed to it through certain communication channels, which could include peers, family, staff at attended organizations, or via intentional dissemination practices such as advertisements. The steps leading to adoption are referred to as the innovation-decision process and include (a) being exposed to the innovation, (b) developing an attitude toward it, (c) deciding whether to adopt or reject it, (d) subsequently seeking adoption, and last (e) confirming the adoption decision. Factors influencing adoption and rejection decisions are central in the present study.
The relative advantage concept, defined as the degree to which an innovation is perceived to be advantageous to existing options, is an important concept for the present study (Rogers, 2002). Preexistent beliefs regarding best practices for overdose response, coupled with prior success using these tactics, might affect OOPP adherence (Lankenau, Wagner, et al., 2012) and adoption. Last, barriers to diffusion are investigated, which refers to the disruption or obstruction in the flow of information (Rogers, 2002). Identifying such barriers is critical in overcoming them, and freeing the flow of diffusion.
Method
A qualitative methodology was employed as participant’s experiential narratives provide rich, contextualized accounts that could be analyzed to uncover themes associated with the diffusion of the OOPP (Tolley, Ulin, Mack, Robinson, & Succop, 2016). Qualitative research generally uses small sample sizes to uncover comprehensive understanding of complex issues, such as diffusion (Neale, Tompkins, & Sheard, 2008). In public health research, qualitative methods are appropriate for uncovering programmatic diffusion and impediments (Tolley et al., 2016). To that end, 30 in-depth qualitative interviews were collected from April 2015 to January 2016 in the study setting.
Setting
The location of the host organization was of prime importance as it is situated in a neighborhood of Philadelphia notorious for being an open-air hub of heroin, crack, prescription drug use, and sex work. The name of the setting is purposely omitted to not contribute to stigma. In 2015, Philadelphia Fire and Emergency Medical Services reported having administered naloxone in this area at a rate three times higher than other areas of the city (PDPH, 2016). The Philadelphia police captain whose district covers this area had stated, “We have a pretty robust heroin market. We’ve had it for quite a while” (Kilpatrick, 2016).
Sample
Inclusion criteria included ⩾ 18 years old, self-reported heroin injection in the past 30 days, witnessed an overdose in the last 2 years, and lived within the study setting parameters. Recruitment occurred via street-based engagement and chain referrals in specific locations known for high drug activity. Potential participants were asked whether they were interested in participating in a research study regarding opioid overdose, and a screener was used to assure potential participants met inclusion criteria, for example, “Have you ever injected drugs? When was the last time you injected any drug? What drug?” and “Have you ever witnessed an opioid overdose?” Purposive sampling was used based on categories of (a) those trained in the OOPP (trained), (b) those aware of the OOPP but not trained (untrained), and (c) those unaware of the existence of the OOPP (unaware). This was assessed in the screener by asking, “Have you heard of the Narcan program at Prevention Point? If so, are you trained?”
Data Collection
Interviews were recorded using a digital recorder and were collected by the first author of the present study, who has more than 10 years of experience working with persons who use drugs in various capacities. All interviews were conducted in semiprivate or private locations that were determined by the participant’s comfort level; most of the interviews were held at a nearby donut shop (n = 22), others at the host organization (n = 4), in participants’ homes (n = 3), and an alleyway (n = 1). Participants interviewed at the donut shop were offered coffee and donuts. Participants were given US$25 cash for their participation, information about local social and health services, and, if not already trained, were given resources for becoming trained in overdose prevention and obtaining naloxone. The informed consent process included discussing participant’s rights to withdraw from the study at any time, to not answer any questions that they did not want to, and to be informed of the purpose of the study, risks and benefits, and assurances of data security. Each participant was provided with a copy of the informed consent document as well as how to reach the principle investigator, research assistant, and Institutional Review Board (IRB) committee for any questions or concerns pertaining to the study. Participant names were never collected, and all demographic information is participant identified. The study’s ethical protocol was reviewed and approved by Drexel University’s IRB.
Measures
A semistructured interview guide was developed with respect to the diffusion of innovation theory. The interview guide comprised four modules: drug use history and current use, witnessed overdose experiences, experiences and perceptions of the study setting neighborhood, and demographics. The beginning module about witnessed overdose experiences included questions and probes regarding first exposure to the OOPP and adoption decisions designed to uncover diffusion, which were only asked to trained and untrained participants. For example, open-ended questions included, “Why did you choose to become trained (or not)? What was the training like?” The interview guide also included close-ended questions including, “How did you first hear about the Narcan program? Do you keep naloxone on you? Do you know other drug users who carry naloxone?” All participants were asked about their social networks and interactions with drug users in the neighborhood, which were especially important for the unaware group as they represent those to which the program has not diffused. The semistructured guide allowed for probes to further explore applicable narratives. The interview guide was piloted with the first three participants and adjusted accordingly; for example, participants were initially confused when asked about the OOPP but were familiar with it being called the “Narcan program.”
Analysis
Data consisted of transcripts and field notes. Each digitally recorded interview was transcribed verbatim. Field notes were kept following each interview to record themes and observations made throughout the data collection process. Transcripts were uploaded into qualitative analysis software ATLAS.ti 1.6.0 (484). Open coding was performed to separate data into broad topics including “awareness of OOPP” and “barriers to adoption.” From the broader topics, more nuanced coding emerged such as “diffusion source” and “motivating factors.” Descriptive demographic information was uploaded into Microsoft Excel and analyzed for averages and ranges.
Emergent themes were peer-debriefed and member-checked with study team members—including academics, host organization staff, and three participants—to ensure credibility of the analysis (Connelly, 2016; Tolley et al., 2016). The first author also had prolonged engagement with participants and kept detailed field notes. The authors conducted reflexivity efforts to consider biases and were subsequently discussed with contributing academics to promote data and analysis trustworthiness. Participants’ names were never known or collected as the one-time interview did not require personal information for follow-up.
Results
All demographics (Table 1) were based on participant self-report. Participants were typically male, white, and heterosexual, although a sizable portion of the sample identified as Latino/Latina (30.0%) compared with the general population (18.1%; U.S. Census Bureau, 2017). Participants generally had long drug-using histories (average 26.3 years). Participants mostly identified heroin as their drug of choice (86.6%). Notably, fentanyl was not mentioned as a drug of choice, which became more commonplace in Philadelphia in the years following data collection. Most participants had graduated from high school or higher (64.3%) and most were stably housed (63.3%). However, the trained group more frequently experienced homelessness at the time of interview than other groups. Positive HCV status was reported by 19 participants, which was highest among the trained group, and two participants reported being HIV positive. Participants mostly make money “hustling,” which entailed panhandling, odd jobs, favors, stealing, and sex work.
Sample Demographics (n=30)
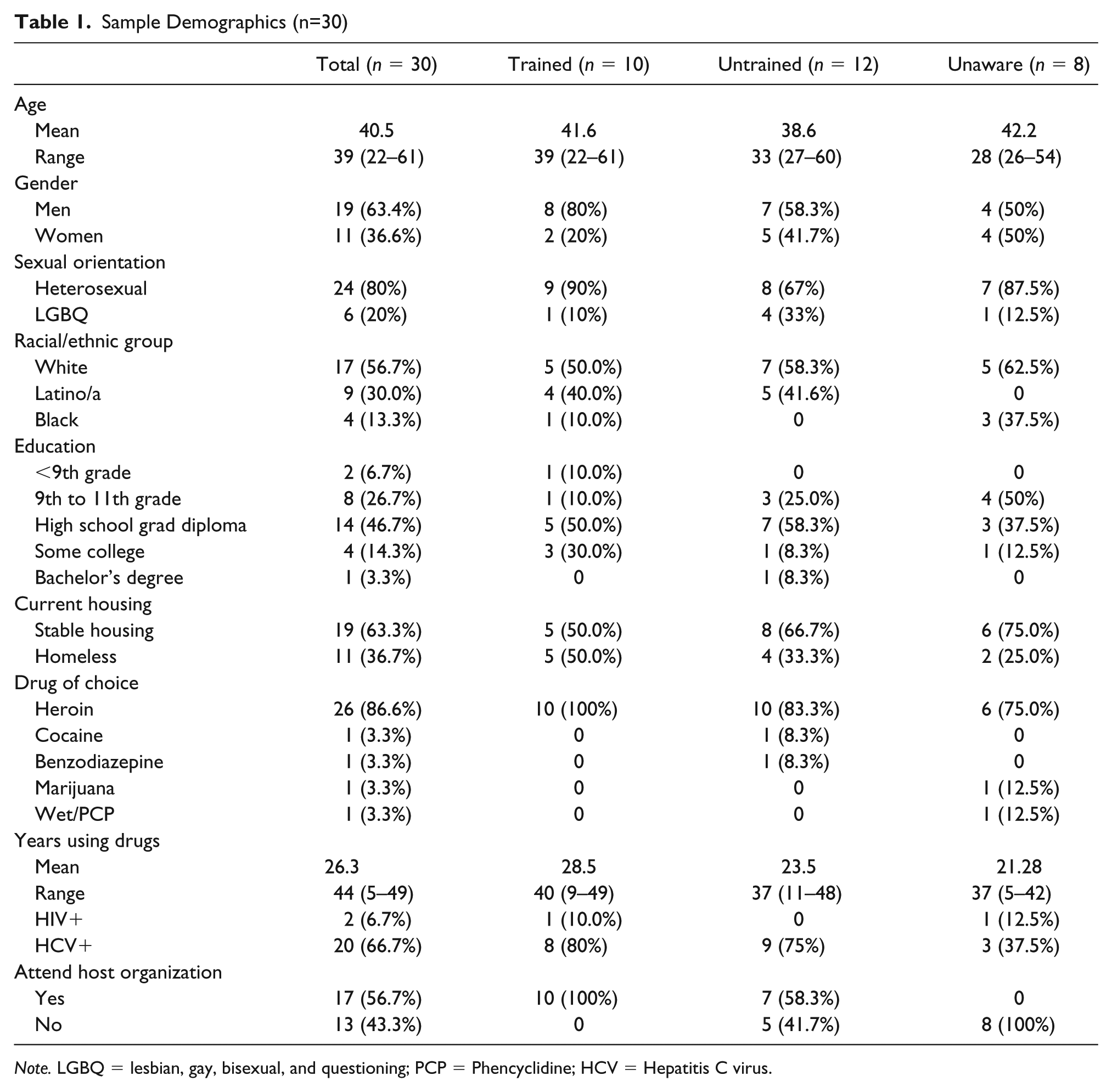
Note. LGBQ = lesbian, gay, bisexual, and questioning; PCP = Phencyclidine; HCV = Hepatitis C virus.
The Innovation-Decision Process
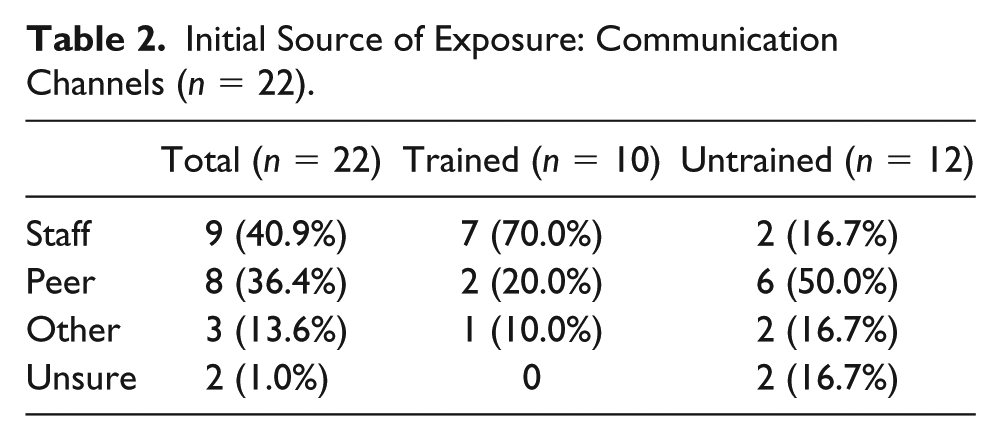
Identifying the source of a participants’ first exposure to the OOPP can reveal the communication channels through which the program was being diffused, and are summarized in Table 2. Participants were mostly exposed to the OOPP by staff at the host organization or by a peer, and adoption decisions varied accordingly.
Initial Source of Exposure: Communication Channels (n = 22).
Host organization staff exposure and adoption decision
Trained participants were most often introduced to the OOPP by staff. Adoption decisions were especially successful when coupled with immediate training offering. To illustrate, one participant (trained) confirmed this, “So umm well they (staff) just happened to ask me, “Hey you want to take the training?” “I said ‘sure I’ll take it.’ And I took it.” Another (trained) stated he learned about the OOPP “just from going there [host organization]” and was subsequently offered the training by staff and obliged. One participant (trained) stated she first heard about the OOPP from a staff member, but this did not lead to immediate adoption. Rather, she was exposed to the program and later approached a different staff member to request training.
Persistence from staff resulted in adoption for some, for example, “when I went down there to get needles they were calling for classes. The one guy kept bugging me and so finally I said, ‘yeah.’” He continued, “Yeah, once they get to see you’re a regular and stuff like that, you know, and they think you’re a little responsible . . . so they’ve seen me; they’re not just gonna train anybody cause it’s not a joke.” Another participant (trained) found out about the OOPP because “somebody in [the host organization] told me” and he “was coming to get needles anyway,” and thought to himself, “if I see somebody fall out I may as well have Narcan [naloxone].”
Nonetheless, not everyone first exposed to the OOPP by staff adopted the program. One participant (untrained) stated his awareness of the program was because, “Oh, I know a few people that work there [host organization] so they told me.” He was offered training and declined, but stated he does plan to get trained during a subsequent visit to the host organization. Another participant (untrained) stated, “Yeah, they [staff] mentioned it to me; I didn’t do no classes . . . I don’t think the heroin is good enough for me to overdose no more, it’s really bad out there.”
Peer exposure and adoption decisions
Exposure to the OOPP by peers less often resulted in OOPP adoption. To demonstrate, one participant (untrained) stated that his initial awareness of the OOPP resulted from observing a person with OOPP supplies in a drug-using context: I heard about it actually, I was under the bridge shooting dope and dude pulled out a Narcan bottle and I was like “damn what’s that bro?” And he’s like, “It’s Narcan,” or whatever and it had the needles and shit and I’m like, “How’d you get that?” And he’s like, “At [host organization], they give you a class and teach you how to do it, they give you the needles and all,” . . . cause a lot of people don’t want to call the ambulance cause they think they’re gonna get arrested. So he was like, “They’re giving out the bottles or whatever so you can save somebody,” which I was like “damn, that’s cool.” When he told me about it, I thought that was awesome because I know a lot of people that OD’ed and died and people just left them.
In spite of his enthusiasm for the OOPP, he did not seek training. He stated that he did not receive any services from the host organization, although he was familiar with it. One participant (untrained) casually stated he learned of the OOPP, “Just on the street,” while another (untrained) learned of it, “Through a friend.” Neither subsequently adopted the OOPP. One participant (untrained) first became aware of the OOPP “Just from people down in this area I guess.” When probed, she stated persons were discussing the OOPP in context of supplies available at the host organization, “Um it’s normally like if I asked somebody where they get their works from, and they say [host organization]. Then they’ll say like ‘they have this, that, and the third’ there pretty much—shit like that.” Her narrative suggested that the OOPP was becoming established among drug-using networks in the area. However, these discussions do not result in these participants seeking adoption. Another participant (untrained) stated, I didn’t take the class but um the person I—I worked for a pimp—the guy I was living with, he did it [OOPP training] so he always had Narcan on hand just in case something happened to one of us.
Although most participants exposed to the OOPP via peers did not adopt, some did. For instance, a participant (trained) recalled first seeing a peer with overdose prevention supplies and seeking out adoption information, Because this kid I seen he had vials of the Narcan and I was like, “How did you get that?” He’s like, “You go there [host organization], they give you a quick little course, they teach you what to do.” So, I went in and I asked them about that and they gave me a little quick course of it and they gave me one vial [of naloxone] and like four syringes full with it to show me how much you need to use.
He stated that he was not a regular at the host organization having only received services there two or three times prior. However, exposure to the OOPP spurred his interest and led to his seeking adoption of the program. A trained participant, who operated a “hack cab” [an underground taxi service], stated he first heard of the OOPP from a friend and subsequently adopted the program after being directly asked by staff, Actually, I was there and I was doing needle exchange or whatever and a guy came by and asked me “do you wanna Narcan kit? You know we can train you in how to use it and everything.” So me being the person I am I chose to, you know cause I deal with a lot of people in my car that I take them to cop, you know to get drugs, you know it’s better to help somebody than just to see them overdosing.
Alternative exposure sources and adoption decision
Two untrained participants could not recall how they first became aware of the program, whereas two others learned about it in different ways. For instance, one untrained participant stated she first heard about the OOPP by seeing flyers promoting it, while another said she learned about it through an another harm reduction group. One participant (trained) first heard about the OOPP from a seminar held at an intensive-outpatient treatment group he was attending, I was in outpatient and it was recently . . . One of the ladies came in . . . and she has the first half to like teach us a lesson . . . and she wanted to share with us about her experience with the Narcan training and she told us what she knew, and she brought the kit and her’s was actually like a nasal one, like it goes in the nose and whatever. Then yesterday, I met a friend here [host organization] and he let me stay with him and he showed me his [kit] last night and he was telling me you know, “You really need to get Narcan or whatever,” and I was like, “oh yeah.” I probably almost did the other day when I was here Tuesday. I signed up to see a doctor and on the checklist, it said, “Are you interested in that [OOPP training]?” And I was gonna do it, but they gave haircuts and I needed my haircut, and I left after the haircut. I didn’t stay for the doctor.
He was subsequently trained later the same week. His narrative of first exposure to the program via a treatment program is noteworthy. Subsequent encouragement from a peer resulted in his seeking program adoption, which occurred by staff announcing a training while he was exchanging syringes, “Umm, I just got here [host organization], I picked up my baggie and he announced it, ‘does anyone else want Narcan training?’ I was like yup, yup, me.”
Barriers to adoption
Many untrained participants showed enthusiasm for the OOPP but did not elect to adopt it. Various adoption barriers were explicitly and implicitly stated by participants and are presented in Table 3.
Barriers to Adoption Summary.

Note. OOPP = opioid overdose prevention program.
Lack of relative advantage
For adoption of the OOPP to occur, an individual must perceive it to be advantageous compared to preexisting strategies. Participants discussed various preexistent techniques for rescuing an overdose victim including smacking the victim, administering CPR, calling 911, placing ice on the victim’s genitals, injecting the victim with salt or milk, hitting the victim’s feet with a 2×4, or laying them in certain positions believed to stop an overdose. For some participants, preexistent techniques were believed to have been effective in the past, which rendered the OOPP redundant and unnecessary. For example, a participant (untrained) stated, “I heard about it [the OOPP] but I don’t know . . . I bring a lot of people back without Narcan.” Another (untrained) stated his experience injecting salt into victims works “right away,” even when other techniques fail. One participant (untrained) had injected salt to revive an overdose victim recently, and felt a sense of pride as no other witnesses knew how to intervene; “they didn’t know what to do, I was the only one . . . I’m from the old school.” He stated that he knew many tricks from the “streets” to reverse overdoses that in his experience are effective. The relative advantage of the OOPP was not perceived to be strong among these untrained participants.
Street availability of naloxone
One participant (untrained) stated he is “so used to pulling them [overdose victims] out myself” using street-based tactics but preferred to use naloxone as, “I gotta go with modern technology, so I’m gonna give em the Narcan.” He perceived naloxone to have a relative advantage over preexistent techniques but had been able to obtain naloxone on the street therefore bypassing the need to acquire training and naloxone at the host organization. He regularly carried naloxone that he received from a friend, saying, “well, I ain’t really trained but I know what to do.” He stated his friend trained him secondarily and that he has also observed overdose reversals with naloxone. Another untrained participant, who reported obtaining naloxone on the street, said that while she was never formally trained, she felt confident in her ability to rescue with naloxone, “I pretty much know like you just either put it in their [vein] or if it’s really bad you go for their chest.” Her statement represents concern that untrained participants do not believe the training will teach them new material. Notably, her belief of administering naloxone into a person’s chest was incorrect and intramuscular injection of naloxone is recommended over an intravenous injection.
Host organization nonparticipation
Some untrained participants discussed an interest in OOPP training but stated that they do not attend the host organization, which impeded the possibility of OOPP adoption. For example, one participant (untrained) stated he “definitely thought about” getting trained, but, “My whole thing is just I never went to [the host organization] or nothing, you know? That’s the only thing that stopped me from getting trained.” Not receiving services from the host organization was influenced by two participants’ desire to abstain from using drugs, as receiving services at a harm reduction agency was viewed as a symbolic commitment to continuing drug use. On inquiry of one untrained participant’s interest of OOPP training, he stated, “Well actually, yeah, but I ultimately want to get clean,” indicating a conflict between program adoption and desire to abstain from drug use. Another participant (untrained) similarly viewed using services at the host organization as a means of becoming trapped in a drug-using lifestyle, “Like, if I get the works and the water it will just get me stuck in this neighborhood. I don’t want to get stuck down here. I’m doing my hardest to get out of here.”
Time deterrent
Perceived length of OOPP training time was a factor reported to impede program adoption, which often related to aspects of using drugs. When questioned about program adoption barriers, an untrained participant stated, “time, my time, I can’t be sick in there, I have to be high.” Further inquiry into another untrained participant’s justifications for not adopting the OOPP led to her explanation that she perceived that it could “take out of my get high time.” Many discussed wanting to be in and out of the host organization as quickly as possible. Another (untrained) stated, “I go there to get my needles and then I leave.”
Causing withdrawal
Another barrier to OOPP adoption is that naloxone, while widely known as a life-saving medication, was known among participants for causing opioid withdrawal. Participants mentioned trepidation of administering naloxone due to fear of social or physical consequences. An untrained participant stated she was nervous to respond to an overdose with naloxone as the victim, “would be mad cause his high was blown,” while a trained participant stated his theory that persons avoid OOPP adoption because naloxone is “their worst nightmare.” Depriving a fellow drug user of euphoria by administering naloxone is cause for concern as the overdose victim might awaken angry. He continued, Cause nobody wants that [naloxone], you know? It makes you really sick cause you’re in automatic withdrawal and you’re mad you know? Really mad. People get really mad, I heard all these horror stories about what it’s like to get hit with Narcan.
One trained participant, who described himself as an old-timer, told a story of administering a six-bag neck shot to a peer who immediately overdosed; he then revived him with a large dose of naloxone, however, He started coming to then he started cursing me out cause it killed his high. I said, “well, I told you not to die, I told you to just do two bags.” But he did six . . . he was pissed off . . . he was like “what the fuck are you doing? I would have been alright.”
Another participant reported that anger coming from overdose victims is a result of an overdose occurring unbeknownst to the victim, “Well, you probably just saved their life but they’ll like be in denial that they were gonna die, and that you just fucked up their high.” An untrained participant revived a friend who overdosed in her home but the victim denied the overdose happened, And [afterward] he’s all pissed off and I’m like “dude you just OD’ed,” and he was like “no, I didn’t,” and I’m like “then why are you laying in the floor?” [He said], “I was just tired, I was taking a nap.” Like he swore he didn’t overdose but he was done for and he overdoses all the time.
Another participant [trained], who has previously overdosed, further confirmed this concern, “The thing with overdose is you don’t even know it happened it’s just . . . your brain doesn’t register the overdose.”
Disruption in Diffusion
The unaware group, participants who had never heard of the OOPP, indicated a disruption in diffusion among PWIDs in the study setting. Unaware participants were more typically women, Black, and stably housed, and less frequently reported being HCV positive (Table 1). No participants in this group reported ever receiving services from the host organization; most had never heard of it. Unaware participants also differed from trained and untrained participants in their engagement and sense of camaraderie with street-based drug-using networks.
Whereas most trained and untrained participants believed camaraderie existed among PWIDs in this area, unaware participants felt differently. To demonstrate, one participant (unaware) stated the camaraderie is insincere: “No, no, they pretend like they do [have camaraderie] but they don’t, no they don’t.” He also stated that he consumed drugs mostly alone, and knew no one in the area who was trained in the OOPP or carried naloxone. Another unaware participant stated that PWIDs did not have camaraderie, did not look out for one another, and knew no one who carried naloxone. A different participant stated, “I don’t really associate with them [other PWIDs] - just like on a ‘hi’ and ‘bye’ basis. I only see them in the neighborhood but I don’t really I don’t hang out with anyone like that.” An unaware participant, who had recently moved to the area following release from jail, had a small network she shared drugs with and stated, “I shoot up by myself or with people—it don’t matter.” She stated her network never discussed overdose, she knew no one who had naloxone, and when asked if she has interaction with other PWIDs in the area, she stated, “I don’t really talk to the people out here.”
Trained and untrained participants often participated in street-based drug-using social networks as a means of meeting various needs and resource sharing. To illustrate, when asked whether he ever shared drugs, a young trained participant described himself as a “loner . . . until recently like out of necessity hoping to find a place to stay I’ve used with about three people in the last 2 weeks.” His participation in drug-using networks was not due to sociability; rather, it was a means of obtaining his basic need of housing, which he accomplished through drug sharing. Similarly, another trained participant, who was also homeless, said he banded together with other PWIDs “just, like, on a survival basis.” Of the trained participants, 50% were currently homeless, compared with 33.3% of the untrained group and 25% of the unaware group (Table 1). Stably housed participants less frequently engaged in drug-using networks, which decreased the frequency of being exposed to the OOPP through this communication channel.
For untrained participants, lack of participation in drug-sharing and other forms of camaraderie among street-based drug-using networks may have disrupted diffusion of OOPP. Intentional or unintentional isolation led to not only being unexposed to the OOPP but also to the host organization, which resulted in exclusion from multiple types of harm reduction services.
Discussion
This theory-based analysis of the diffusion of an OOPP provides insight into the various determinants of program exposure, adoption decisions and influencing factors, and disruptions in the diffusion process among PWIDs. The present study is the first to our knowledge to recruit participants based on their familiarity with an OOPP. We followed the steps of the innovation-decision process and found that exposure via the host organization staff, coupled with training offering, appeared to facilitate adoption. Within the diffusion of innovation framework, mid-level organizational staff and officials who direct their influence to upping program adoption are regarded as “champions” (Rogers, 2002). Staff demonstrated their champion status as they were successful in promoting program adoption via one-on-one interactions and persistent training offering. Among participants familiar with the OOPP, many had a positive attitude regarding it, which is an important step in the innovation-decision process.
The champion effort was supported by PWIDs being exposed to the OOPP by peers. Peer communication is critical especially among “hidden” social networks, such as PWIDs, due to mistrust of outsiders (Dickson-Gomez, Weeks, Martinez, & Convey, 2006; Rogers, 2002). Furthermore, results indicate that OOPP training status was associated with having at least one peer who was trained (Wagner et al., 2013). In the present study, most participants exposed to the OOPP by peers showed interest in the program, but not all adopted it. However, those who were exposed by peers and later offered training by staff did adopt, suggesting that peer exposure leading to adoption might be facilitated by champions. However, this requires increasing host organization participation.
The underlying causes of resistance to harm reduction organizations by some PWIDs is important to consider. To start, purchasing syringes on the street might be preferred for a variety of reasons related to accessibility and stigma. Naloxone is likewise available on the street indicating that the host organization is not viewed as the only source. However, OOPP training is important as it significantly increases knowledge of overdose prevention (Wagner et al., 2010). Participants interested in stopping their drug use reported believing that receiving services at the host organization represented a symbolic commitment to drug use, which contradicted their desire to abstain. However, these participants have been unsuccessful in abstaining from drugs. Similarly, another study found that drug users who had abstained from drug use also ceased participation in a peer-led HIV-risk-reduction program due to avoidance of persons and places reminiscent of their drug use, suggesting that the act of abstaining may be a barrier to harm reduction programming altogether (Convey, Dickson-Gomez, Weeks, & Li, 2010). Moreover, in all public health programming, there will be a subset of the intended audience who are resistant to participation due to mistrust of health services and stigmatization, and therefore, will not seek out services at the host organization irrespective of potential benefit (Ahern, Stuber, & Galea, 2007; Armstrong et al., 2006; Laveist, Isaac, & Williams, 2009).
Another important adoption barrier was a perception that the OOPP was not advantageous compared with preexistent techniques, which included the use of folk remedies, such as injecting the victim with salt or milk, slapping them, putting ice on their genitals, or smacking their feet. Lankenau, Wagner, et al. (2012) discussed how previous success using these remedies reduced the frequency of trained participants responding to an overdose using OOPP training techniques. The present study results corroborate that finding as study participants indicated that previous success using these remedies also reduced the prospect of adopting the OOPP. Moreover, many untrained participants reported an interest in OOPP training; however, they perceived that electing to be trained would take away time needed to procure funds for drugs, or would extend intervals between drug doses. Such competing priorities among PWIDs have been empirically documented (Best, Day, McCarthy, Darlington, & Pinchbeck, 2008; Swan et al., 2010). In particular, Swan et al. (2010) found that chronic drug use competes with adopting treatment for HCV as the “need for drugs crowds out other concerns” (p. 759), which echoes findings in the present study pertaining to OOPP adoption.
Naloxone, irrespective of its life-saving effects, causes opioid withdrawal. Several studies have reported withdrawal as an adverse reaction to naloxone administration by laypersons (Dettmer, Saunders, & Strang, 2001; Doe-Simkins, Walley, Epstein, & Moyer, 2009; Strang et al., 2008; Tzemis, Al-Qutub, Amlani, Kesselring, & Buxton, 2014). Prevailing literature highlights how members of drug-using networks assist one another in withdrawal avoidance by sharing drug doses to offset symptoms (Bourgois & Schonberg, 2009). In this study, while some participants were willing to administer naloxone irrespective of causing withdrawal, others stated it as a deterrent to program adoption or adherence. In particular, fears of physical or social consequences for administering naloxone underscored this apprehension.
While results demonstrate that the OOPP diffused to those who participate in larger drug-using networks, the diffusion process was halted among those who tended to interact less frequently with such networks. Unaware participants who were outside of drug-using social networks more often identified as Black and/or as women than those who do participate in these networks. Participants who did not depend on such networks for housing or drugs also tended to socialize with other PWIDs less and use drugs alone in the confines of their home. Fewer reports of HCV among the unaware group could indicate less injection equipment sharing by virtue of less participation in drug-using social networks, or less access to screening services. Ultimately, isolation resulted in being effectively hidden from various harm reduction services, messaging, and support.
Public Health Implications
Increasing adoption rates of the OOPP requires surmounting study-identified barriers. Barriers to adoption, including concerns regarding time or believing training was unnecessary, might be addressed by staff or champions. The diffusion of innovation suggests that this is accomplished by using “champions to promote preventive innovations” (Rogers, 2002, p. 992). Enhancing and encouraging champion efforts with immediate OOPP training to potential adopters could expand impact. Focusing on developing champions who are women of color, who have received trauma-informed training, and who are nonjudgmental toward sex work might enhance champion efforts for women who inject drugs (WWIDs) as their needs are complex and may differ from men’s (Azim, Bontell, & Strathdee, 2015; Blankenship, Reinhard, Sherman, & El-Bassel, 2015; Sheard & Tompkins, 2008). In addition, enhanced structural interventions tailored for women, such as childcare, housing, and employment programs, might increase the host organization participation by otherwise isolated WWIDs (Pinkham, Stoicescu, & Myers, 2012), which could in turn increase OOPP adoption.
Using a “train-the-trainer” model within an OOPP could resolve issues related to acquiring naloxone on the street by encouraging persons who distribute naloxone kits to others to provide a quick overview of how to appropriately use it, especially as some persons prefer informal diffusion from peers with personal experience, which can enhance trust (Meagher-Stewart et al., 2012). Analogously, secondary distribution of safer injection equipment and education is recommended due its effectiveness and reach (Benyo, Curry, & Raymond, 2006). Efforts to apply a secondary distribution model to OOPPs might be comparably impactful. Bennett, Bell, Tomedi, Hulsey, and Kral (2011) similarly recommend harnessing the power of overdose peer educators to reach those who do not use public health services. Likewise, Convey et al. (2010) found that altruistic peer educators were successful in maintaining a peer-led HIV-risk-reduction program among drug users, suggesting this may also be an appropriate approach to amplify and sustain an OOPP.
Efforts to conduct OOPP trainings within drug-treatment centers, opioid substitution therapy programs, and recovery houses could result in increased awareness of overdose prevention and increased participation. Treatment facilities should consider allowing training to occur onsite and distribute naloxone kits. While harm reduction programs, such as OOPPs, are often believed to be in conflict with treatment goals, the ongoing opioid crisis demands pragmatic response.
Limitations
The present study is susceptible to various limitations. First, data collection and analysis might be influenced by the interviewer’s history, vulnerabilities, and potential biases, and could limit study confirmability (Connelly, 2016; Harris, 2015). Second, interviews collected in semiprivate locations might not have provided the discretion necessary for fully forthright responses. Third, data collection using face-to-face interviews is susceptible to the social desirability bias, which could influence participant responses to some questions. The present study is also subject to recall bias as participants were asked to retrospectively describe witnessed overdoses within the past two years, which were numerous for some participants. Finally, the host organization moved locations during the time period of data collection, which might have dampened participation and OOPP adoption. However, this was not reported to be an issue by participants. Credibility efforts—including peer-debriefing, member-checking, keeping detailed field notes, and prolonged engagement with participants—were undertaken in an effort to mitigate the effects these limitations may have posed, and enhance data and analysis of trustworthiness (Connelly, 2016).
Conclusion
OOPPs are a promising intervention in reducing the opioid overdose death burden but must be diffused to the intended audience for adoption and subsequent impact. Participants who were offered OOPP training directly by harm reduction staff frequently adopted this program. Concerns regarding time, drug withdrawal, or irrelevance of training could be addressed by harm reduction staff during one-on-one interactions. Harm reduction staff were highly influential towards encouraging positive health behaviors among PWIDs in the study’s setting, highlighting their importance in efforts to reduce fatal opioid overdoses. Persons entirely unaware of the OOPP, and available harm reduction services, were essentially hidden from important harm reduction messaging. Efforts to reach this group are imperative and ought to include active dissemination by harm reduction staff and peers.
Footnotes
Acknowledgements
We would like to acknowledge the support of local harm reduction facilities, in addition to Drs. Amy Carroll-Scott, Mariana Chilton, and Randall Sell; Mr. Jose Benitez; and dear friend Steven R. Matt.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.