
Abstract
Oral cancer is a considerable public health problem, and a low level of awareness and knowledge about this tumor and its risk factors is prevalent. To gain a profound understanding of risks groups and to identify suitable communication strategies for a prevention campaign in Northern Germany, an exploratory research was realized. In semistructured face-to-face interviews, the participants of the study (n = 28) described their individual oral cancer-related perceptions and information-seeking behaviors. A computer-assisted qualitative data analysis showed a vague but also deterring picture of cancer combined with restricted attitudes toward the topic and an inactive or even avoiding information behavior. Four underlying cognitive patterns of self-distancing were identified: (a) optimistic bias, (b) fatalism, (c) hedonism, and (d) pragmatism. The main challenge of oral cancer prevention is to deal with the target groups’ informational and cognitive barriers.
Keywords
Oral cancer is a considerable public health problem, and a low level of awareness and knowledge about this tumor and its risk factors is prevalent which goes along with perceived low self-efficacy and high levels of uncertainty regarding opportunities of prevention and early detection (Hertrampf, Wenz, Koller, & Wiltfang, 2012; Horowitz, Canto, & Child, 2002; Patton et al., 2004). This is particularly crucial because the survival rates could be increased, and the severe side and long-term effects (e.g., Röing, Hirsch, Holmström, & Schuster, 2009) could be mitigated if early detection was improved. Early detection requires that people at risk are informed about the existence of oral cancer, its signs, symptoms, risk factors, and preventive measures (Scott, Weinman, & Grunfeld, 2011). Consequently, preventive health communication should particularly aim at raising awareness and knowledge and reducing uncertainties and barriers of dealing with the issue (Scott, Grunfeld, Auyeung, & McGurk, 2009; Scott et al., 2011).
Thus, health promotion related to oral cancer requires that the target groups are both willing and able to deal with the health-related messages that aim at motivating them to engage in health behaviors. That also means that messages need to be designed adequately in many respects (e.g., Witte, Meyer, & Martell, 2001). One main effort is that the information given is adjusted to the target groups’ cognitive dispositions toward the topic, their informational needs and behaviors. The article focuses on health-related information-seeking behaviors and on informational barriers that need to be hurdled when we aim to reach target groups with health communication efforts. Two main questions are resolved: (a) Which factors drive active health information-seeking behaviors about oral cancer and how do people search for this information? (b) What are the main barriers of seeking information on oral cancer and how can information avoidance be understood?
Therefore, our study aims to describe the target groups’ knowledge and information behavior regarding oral cancer and tries to identify and understand the individuals’ beliefs, motivations, and needs on which their information behaviors, especially their defensive and aversive dispositions toward information, are based.
Background
In Europe, an estimated 67,000 new cases were diagnosed with oral cancer in 2008 (International Agency for Research on Cancer & World Health Organization, 2010). Since the year 2000, an increasing trend has been observed in Germany, with now more than 13,000 newly diagnosed cases annually; the relative 5-year survival rate is low (48% for men and 61% for women), and more than 4,000 patients die of this disease per year (Robert Koch Institut & Gesellschaft der epidemiologischen Krebsregister in Deutschland, 2013). The survival rates could be remarkably higher if the tumor was detected earlier (Sankaranarayanan et al., 2005). But, most of oral cancer patients are still diagnosed at advanced stages (Scott, McGurk, & Grunfeld, 2008).
This problem is multifaceted and complex (Papas, Logan, & Tomar, 2004), and health communication efforts require addressing sociodemographic and socioeconomic factors as well as the individuals’ informational needs and behaviors. There is profound empirical evidence that inequalities in education, income, and occupation—that is, a low socioeconomic status—are closely linked to health and risk-related psychosocial and behavioral factors, to disparities in health status and health care (Adler & Newman, 2002; Goldman, Diaz, & Kim, 2009; Mackenbach et al., 2008; Oduro, Connor, Litwin, & Maliski, 2012; van Lenthe et al., 2004). This can also be observed for oral cancer which is particularly prevalent among elderly people and among men (Andersen, Lassen, & Clemmensen, 2008; Conway et al., 2008): A low socioeconomic status, regular smoking, and alcohol consumption are described as main risk factors of developing oral cancer. Analogous to other types of cancer, these factors interacted with a lower level of knowledge and awareness (Hertrampf et al., 2012; Scott et al., 2011).
Moreover, lack of information and knowledge is revealed to be the key problem. Studies show the patients’ difficulties to interpret initial symptoms and a low level of perceived ability to get help for oral symptoms, leading to a delay in seeking help (Austoker et al., 2009; Scott et al., 2008; van der Waal, de Bree, Brakenhoff, & Coebergh, 2011), and the level of knowledge and awareness in the public has been described as insufficient (Hertrampf et al., 2012; Horowitz et al., 2002; Patton et al., 2004). Even if people had already heard of oral cancer, they often did not believe that their symptoms were an indication (Grant, Silver, Bauld, Day, & Warnakulasuriya, 2010).
Thus, one of the main challenges in oral cancer communication is to close the existing knowledge gaps that are connected to different socioeconomic levels (Niederdeppe, 2008). Against this background, preventive efforts have to face the crucial interconnections between (a) risk factors of oral cancer, (b) awareness and knowledge about this tumor, and (c) the socioeconomic status (Scott et al., 2011).
Information Seeking and Avoiding as Key Factors for Effective Health Promotion
Active health information seeking is known to have a strong influence on health-related behavioral intentions and decisions and is determined by psychosocial, sociodemographic, socioeconomic, and environmental factors (Johnson & Case, 2013; Lambert & Loiselle, 2007). Cancer-related issues cause psychological distress and uncertainty which is particularly relevant in the view of the fact that most people do not possess comprehensive knowledge on this topic (Hesse, 2009). Information acquisition can help to reduce uncertainties, remove ambiguities, improve preventive behaviors, and support decision making on early detection and treatment options (uncertainty management; see Brashers, 2001). For these purposes, individuals can choose from many different sources such as mass media, websites, family members, and friends as well as health professionals (Kelly et al., 2010).
Research shows that people are more susceptible to information if they feel involved in the issue, if they are able to understand the information given, if they perceive it relevant, and if they expect to derive benefits from it (e.g., Rimal & Juon, 2010; Rimal & Real, 2003; Turner, Rimal, Morrison, & Kim, 2006). These studies also provide evidence that people have a higher motivation to deal with health information if they perceive risks for themselves and if they experience self-efficacy for themselves.
However, people do not always welcome health information and also engage in information avoidance, which is a common behavior in everyday life (Narayan, Case, & Edwards, 2011). For example, Emanuel et al. (2015) showed for a representative U.S.-American sample that 39% of the population preferred to avoid information about personal cancer risks.
The uncertainty management theory (UMT; Brashers, Goldsmith, & Hsieh, 2002) suggests that the type of health-related information behavior (seeking or avoiding) is closely linked to the individual’s perception of uncertainty which is defined by the perceived discrepancy between one’s current level and the desired level of uncertainty. In a state of uncertainty, information seeking can reduce uncertainty that is distressing, whereas information avoidance can maintain perceived uncertainty that allows for hope and optimism (Barbour, Rintamaki, Ramsey, & Brashers, 2012; Brashers et al., 2002; Brashers et al., 2000). Thus, information behavior can both be used to reduce, to maintain, and to raise uncertainty (Barbour et al., 2012). Uncertainty is not necessarily a negative and uncomfortable emotional state but can even be desirable in certain situations (Barbour et al., 2012; Brashers, 2001; Brashers et al., 2002). Distancing oneself from potentially existing worries and perceptions of uncertainty can help to reduce cognitive dissonance in everyday life (Festinger, 1957). When the individuals’ uncertainty appraisal suggests that more information about the topic or risk might cause discomfort and raise cognitive discrepancies they might not be able to cope with, they tend to decide to maintain a certain degree of information insufficiency and thus avoid further information on the risk. Thus, it might also be useful to distance oneself from undesired messages and to purposely avoid information (van’t Riet & Ruiter, 2013).
Furthermore, the strategy of uncertainty management depends on the individual’s skills to gather information. To successfully find information can be complicated by the nature of information or the complexity of information-seeking behaviors (Brashers, 2001). Accordingly, self-efficacy assessments influence health-related information behaviors. Especially, under the condition of low self-efficacy, the disposition toward information avoidance becomes more likely (Barbour et al., 2012; see also Goodall & Reed, 2013). Taken together, cancer information is multifaceted, complex, emotionally distressing, and often very disturbing. This can increase the tendency to not actively seek or even avoid information to reduce complexity and to cope with these uncertainties.
According to UMT (Brashers, 2001), our study assumes that both information seeking and avoiding are a rational strategy for coping with health-related issues. Against this background, we aimed to explore the underlying cognitive patterns of people’s information seeking or avoiding behaviors, taking into consideration the issue-specific problem awareness, people’s beliefs, and their openness toward information and preventive advice regarding oral cancer.
Method
The data presented here were part of a formative evaluation study (see Atkin & Freimuth, 2001) that aimed to identify and describe the main target groups of prevention and early detection prior to an oral cancer awareness campaign in Northern Germany (Baumann et al., 2016). We intended to uncover and explore the target group members’ relevant cognitive and behavioral patterns associated to the people’s information seeking or avoiding behaviors regarding oral cancer as a specific health issue. Particularly, aversive beliefs, defensive mechanisms, and cognitive barriers of dealing with the issue which all cause reactance and inhibit successful processing of persuasive health communication were taken into consideration (Case, Andrews, Johnson, & Allard, 2005; Dillard & Shen, 2005).
Thus, our study aimed to explore the individuals’ perspectives on oral cancer. The goal was to provide a profound analysis of the risk group’s beliefs, motivations, and needs on which the individuals’ oral cancer-related information behaviors are based (Atkin & Freimuth, 2001). Particularly, the people’s complex patterns of personal, situational, and contextual factors of dealing with the topic—also referring to their defensive motivation and barriers of dealing with the issue—were intended to be understood. Our results should also guide further quantitative evaluation and finally give information for campaign development. For these purposes of gaining insight into the empirical problem, particularly, qualitative research methods are supposed to be helpful.
Participants and Procedure
To comprehensively deal with the purpose of the study, we decided to follow a triangulation approach. We involved three different subgroups in our sample that provided different perspectives on the object of research. The first group consisted of people at risk who are predominantly male, aged 60 years and above, with low socioeconomic status (SES), living in urban areas with an excessive alcohol and/or tobacco consumption. This is the main risk group for oral cancer (Hertrampf et al., 2012).
To comprehend problem awareness and risk perception, informational needs and communication behaviors with special regard to symptom detection, we included persons with diagnosed oral cancer and skin cancer in the face being in aftercare treatment as a second group of participants. The majority of patients are men at the age of 60 years and above (Andersen et al., 2008; Conway et al., 2008). Their retrospective assessments were supposed to help adjust the campaign strategy to the effect that people at high risk who might have already experienced some symptoms that should be clarified might become susceptible to the campaign. For this subsample, it has to be considered that they are probably not suitable to uncover the typical patterns of information behaviors as their self-perceptions and experiences as patients will have overlaid their memories.
As a third subgroup of our sampling strategy, we additionally recruited relatives of oral cancer patients because the individuals’ health behaviors and health-related decisions are also significantly influenced by the social environment (Sallis, Owen, & Fisher, 2008). This is particularly important in the context of oral cancer as the people at risk are predominantly males at an older age who are known to be supported by their wives and family members in regard to health-related information and medical decision making.
In October and November 2011, 28 persons were recruited to take part in the study: 18 subjects at risk (SR); 7 subjects affected from oral cancer or with skin cancer in the face (SA); 3 relatives of subjects affected (RSA). A description of the sample is given in Table 1. People diagnosed with oral cancer and skin cancer in the face and their relatives were recruited in a German Clinic of Oral and Maxillofacial Surgery in the setting of their regular aftercare by the medical staff. People at risk were recruited via different local social service providers, an alcoholics support group, and by additional snowball sampling. Before any appointments for interviews were made, every participant received written information on the project and expressed his or her written consent. The data were strictly handled in an anonymous form only. The project was approved by the Ethical Committee of the University Hospital of Kiel, Germany (AZ: D 462/11).
Sample Description.
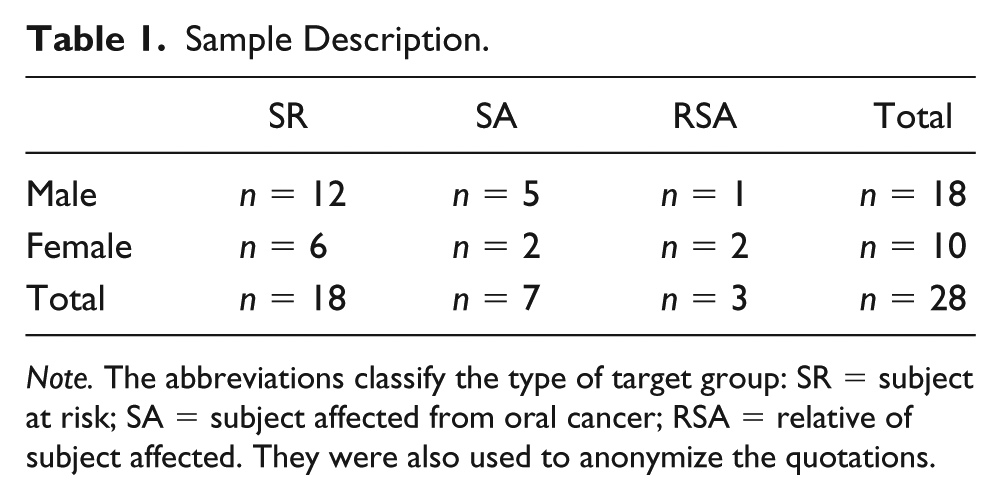
Note. The abbreviations classify the type of target group: SR = subject at risk; SA = subject affected from oral cancer; RSA = relative of subject affected. They were also used to anonymize the quotations.
Overall, 19 interviews (14 single interviews, four interviews in pairs, and one interview in a group setting) were conducted. This mixture of different interview settings resulted from the different situational parameters of access to the field and the participants’ preferences. Our primary objective was to offer rather natural and comfortable interview settings and to lower the barriers of participating as far as possible. Originally, only individual interviews were planned as method of data collection. In four cases, patients recruited in the clinic were accompanied by their spouses and preferred to be interviewed in pairs. Recruitment of participants with very low SES and excessive alcohol and tobacco consumption who fit our sampling criteria turned out to be particularly challenging. We only had the opportunity to talk to six members from a support group for former alcoholics. They requested to realize the interview setting as a group session. We are aware of the fact that these different types of interviews have different methodological implications. For example, participants in the group setting may have been influenced by group dynamics, and the group characteristics may have affected the results. But our research objective was only to explore the different patterns of information seeking and dealing with information related to oral cancer by single persons. Analogous to the single interviews, the interviews in pairs and in the group setting focused on the collection of information from individuals and not on interpersonal group dynamics and interactions between participants, not on uncovering the role of relationships or situational mechanisms of social interactions. So, we did not motivate participants in the pair or group setting to interact with each other, and we addressed each respondent with our questions separately. This means, we approved this methodological lack of conclusiveness caused by different interview settings in favor of field work pragmatics, the participants’ preferences, and comfort.
In the first step of computer-assisted qualitative content analysis, every interview was analyzed separately and the results were considered regarding differences which may stem from the different interview techniques. As data analysis did not indicate interpretable differences between the participants’ statements in different interview settings, we did not split the results according to the interview technique. To provide transparency, references to the participants’ statements are marked with the type of interview (“I” = individual interview; “P” = interview in pairs; “G” = group setting).
Persons with diagnosed oral cancer were interviewed after their regular aftercare in the Clinic of Oral and Maxillofacial Surgery in a conference room of the clinic. The other interviews were conducted on the participants’ request in their homes or in the rooms of the local social service providers. The interviews took between 35 and 90 min. At the beginning of each interview, the participants were informed about the study, and they agreed to give written consent for their participation.
Interview Guide
A flexible research approach was required to determine the individuals’ barriers and triggers to dealing with oral cancer and to identify motivational and emotional patterns, underlying feelings of uncertainty, and the openness toward information about the topic. All interviews were conducted face-to-face and tape-recorded. The same semistructured interview guide was used in all interviews. The questions comprised the participants’ level of knowledge and their cancer-related decisional strategies, information and communication needs, patterns, and barriers. The participants were asked to describe their perceptions and experiences regarding cancer in general as well as oral cancer in particular and to make recommendations for suitable ways of information and message strategies in oral cancer prevention. The key topics were addressed as open questions by the interviewer. Supplementary questions were used to deepen an issue and to maintain a natural flow of conversation. The facilitator was a female communication researcher and member of the project team, being experienced in qualitative interview techniques.
Analysis
The goal of qualitative analysis is the enhancement and widening of our perspectives on social phenomena. Thus, it is important to identify the different attitudes, opinions, and behaviors regardless of how many people expressed them. The focus is on the individual, and we aim at identification and understanding—not at quantification—of individual patterns of mind-sets. Thus, instead of frequencies, we concentrate on the identification of different phenomena.
Each of the interviews was transcribed verbatim. Numbers were used as pseudonyms for the individual participants. A qualitative content analysis based on the principles of coding step by step according to Mayring (2000) was conducted for the whole text material by one empirical researcher who also realized the interviews, experienced in computer-assisted qualitative data analysis. First, the material is divided into content analytical units that are subsequently coded with categories being in the center of the whole analytic process. The coding scheme was developed by combining inductive and deductive strategies of developing and applying categories by means of coding (Mayring, 2000): The major topics and dimensions of analysis (e.g., the individuals’ health and risk status, health consciousness, health, risk, and prevention behavior; informational needs, health information–seeking behavior, evaluation of information obtained; cancer-related experiences, cognitions, and emotions) were derived from the interview guide and served as main categories of the first draft of the coding scheme (deductive category application). This basic structure was differentiated and modified during the course of qualitative data analysis and helped to identify and to organize more specific codes developed from the participants’ single statements (inductive category development). In this process, the large amount of material was reduced to those units of meaning being particularly relevant for the scope of research. Going through several stages of iterative category development and assessment, modifications and revisions of codes (feedback loops) allowed discovering reasonable structures in the data and theoretical saturation. The coding was carried out by Atlas.ti (version 6.2; Friese, 2012). The data set contains every interview-transcript (primary documents), the units of analysis (quotations), and every category (codes) that was used and links these codes to the original quotations of the study participants in the transcripts. This allows others to comprehend and re-enact the whole process of qualitative data analysis. A second researcher of the team comprehensively reconstructed the analysis of coding, identification, and interpretation of patterns described in the next section.
One problem we want to mention is that the quotations used to prove and to illustrate our findings and interpretations were in German and had to be translated for this article. Of course, every translation is always also an interpretation of text, and our post hoc translations carry the risk of being also shaped by our theoretical consideration and interpretations. Therefore, one person with and two people without any relatedness to the study and to communication science translated the quotations for us, and we compared the translations.
Findings
Our participants knew about different types of cancer, but actually they were not aware of oral cancer in particular. They associated behavioral cancer risks such as alcohol or tobacco consumption mostly with cancer types such as lung or colon cancer which already gained public awareness. Thus, participants did not consider oral cancer as a possible consequence of these risk factors. The participants described their level of knowledge and awareness of oral cancer as being rather low. They reported to have a vague but, at the same time, threatening and deterring picture of this disease. Some participants assumed that their perceptions were influenced by sad stories or traumatic experiences with cancer in their families (e.g., SA, female, 60–70 years old, I; SR, female, more than 80 years old, high prevalence of cancer in family, I).
The following description of findings is divided into two categories. First, the question of how participants sought for information about oral cancer is addressed. Second, we will focus on the barriers leading to inactive information and communication behaviors and identify patterns of self-distancing.
Seeking Information About Oral Cancer
Overall, the participants of our study appeared to be rather restrained and of low proactivity regarding information and communication seeking. They predominantly described themselves as taking a passive role in communication matters. Even if they were affected from oral cancer or were aware of their risk status, they did not consequently want to deal with the topic in more detail to avoid raising fears and uncertainty. For example, a patient’s husband stated that he was not interested in gathering more information because this would have only stirred him up: “And you’ve got the feeling that you’re in good hands so that I don’t have to inform myself through all kinds of media. Because that’s just upsetting and makes me feel unsure” (RSA, male, 70–80 years old, P).
Active health information–seeking behavior
Most participants of our study rather let themselves be informed by others instead of actively seeking health information. Even if they were interested in health topics in general or were aware of their own risk status, dealing with cancer-related information was usually not considered before they felt the threat coming closer to their own life and social environment. A female person at risk explained that she would not read something about oral cancer without any specific reason: I only seek information if one of my friends or acquaintances is affected. I’m sure as hell I wouldn’t read about it without any reason. I don’t read things like that just for fun. Maybe someday I’ll need to, maybe someday I will. (SR, female, 60–70 years old, I)
Media sources
Participants showed interest in media information about oral cancer only as long as messages corresponded to their informational needs and capacities. Several participants claimed the media to cover the topic in a compact and factual manner (e.g., SA, male, 60–70 years old, I; SR, male, 60–70 years old, smoker, I; SR, members of an alcoholic support group, men and women, aged 50+, G). They appreciated reports about people affected, but these stories should focus on the matters of fact and avoid a sensationalistic, dramatizing style charged with too much emotion. Moreover, the participants preferred authentic stories about ordinary people instead of exaggerating stories on celebrities.
Information on this topic was preferably selected if people could link the issue directly to their own person, to their family members, and to their individual contexts of life. A male oral cancer patient pointed out that awareness for the topic in the media required messages capable to create a feeling of proximity and similarity between the media content and the user: “I read the newspaper or watch eagerly TV when they suffer from the same illness, maybe I also look for other media. Now I’m much more interested in it than before. That’s true, actually” (SA, male, 70–80 years old, smoker, P). Overall, compared with interpersonal sources, information both from traditional mass media and from the Internet were perceived as less important and primarily served complementary informational needs.
Health professionals
The participants of the study described health professionals to be their major reference persons and the most important source when health-related problems and feelings of uncertainty occurred. The intensity of communication and information behavior appeared to be influenced by the people’s experienced quality of health care and support from health care professionals. One husband of an oral cancer patient (70–80 years old, P) reported that as long as he felt to be in good hands, he did not feel the need for additional information and advice. The participants of the alcoholics support group (SR, men and women, aged 50+, G) emphasized that the feeling of being accompanied by medical experts lowers their barriers of seeking medical treatment. Face-to-face interaction with the doctor provides the opportunity to get answers and to assure oneself by asking questions immediately. Thus, medical experts might particularly help to bridge the gap to individual members of the oral cancer high-risk group.
Social context
Furthermore, the social surroundings appeared to play a major role for people with high perceptions of risk and concerns, particularly, in case of cancer suspicion or detection. Particularly, spouses provided emotional support when cancer was suspected or diagnosed. They supplied social proximity and support for those who needed someone to listen to or someone who was just there. One participant at risk summarized that he received medical advice from his doctor and mental support from his wife: “Expert support: I’d get from the physician. Emotional support from my wife” (SR, male, 60–70 years old, smoker, former alcoholic, I).
In our sample of people at risk, people affected from oral cancer and their relatives, low levels of proactivity in information seeking, the need for informational and social support in health provision, and barriers of dealing with the topic were dominant. These results guided our next step of qualitative data analysis, that is, identifying patterns of self-distancing which might help to understand these dispositions better.
Patterns of Self-Distancing
The next step of the qualitative analysis was to identify the main dimensions characterizing the different determinants of interest and openness toward oral cancer–related information and communication which provide the main explanations and dimensions of self-distancing. These were the components of patterns of self-distancing which were identified in the subsequent step of analysis. The following categories indicating personal, situational, and contextual factors were extracted from the interviews as main reasons for the rather passive self-conceptions accompanied by inactive information and communication behaviors:
stressful events and contexts of life, for example, problems at work or being pressed for time, financial problems, crisis in personal relationships
lack of social support by family members and friends
general skepticism against cancer prevention measures
loss of confidence in health care and health professionals
lack of knowledge and risk perception about cancer
low level of health-related self-awareness and self-efficacy
habitual risk behaviors, especially, high alcohol and tobacco consumption that may evoke cognitive dissonances
These factors have a close match to the determinants of health-related information seeking and avoiding behaviors outlined in the literature (Johnson & Case, 2013; Lambert & Loiselle, 2007). The character of our data allowed us to gain deeper insight into the underlying cognitive mechanisms. Based on our interview data, we reinterpreted these determinants and their interrelations against the individual backgrounds of our participants’ complex and dynamic situation-dependent contexts of life. Four multidimensional patterns of self-distancing from the problem of oral cancer and of managing uncertainties and fears associated to this topic were identified.
Optimistic bias
Generally, estimating the own person as less vulnerable than others—that is, perceiving comparably lower levels of risk—makes the individual feel less threatened. Consequently, feelings of uncertainty and awareness for opportunities or the need to take preventive efforts does not arise, and information about the issue that might address risk perceptions and issue involvement is ignored. The optimistic bias acts like a protective cognitive barrier that allows a person to avoid deeper concerns. For example, one male participant at risk (60–70 years old, I, see below) argued that he was physically fit, that he had lived healthy and was not genetically predisposed and thus did not expect to be very much at risk. He even used these arguments as a legitimation for his general skepticism and his decision not to take part in any cancer early detection examination at all. Another participant (SA, male, I, see below) admitted that—until he was affected from oral cancer—he had thought that something like this could not affect him at all and therefore he did not care about prevention or early detection at all: Basically, I reject (offers for cancer check-ups) . . . . Simply because there is no case of cancer at all in my own family. Therefore, I assume that I won’t be hit by it quite as fast. I don’t know if that’s true. (SR, male, 60–70 years old, I) Of course, I know that life is unlasting . . . I always thought: “I was a sportsman once, so something like this cannot affect me.” (SA, male, 70–80 years old, smoker, affected from oral cancer, P) In fact, I am a very difficult case. I think by myself, I’m not involved in it anyway. And second, maybe, yes, I will be hit anyhow. But then, well, one could actually fight it, do something against it by healthy behavior. (SA, male, affected by skin cancer, I)
Fatalism
A fatalistic view results from the internalization of the idea that being affected from oral cancer is a question of destiny. One participant at risk (male, 60–70 years old, I) stated that if somebody is predestined to be affected, he or she will be affected but nobody knows who will be affected at what time. Not believing in the opportunity to protect oneself from being affected at all is directly linked to the denial of believing in self-efficacy and to distrust effective health prevention and early detection, even if the perception of being at risk might be salient. Thus, feelings of fear and uncertainty are stifled, and individuals will try to preserve themselves from factual information on prevention and early detection as both would rather be confusing than supportive. A male patient (SA, 70–80 years old, smoker, P, see below) summed up that he would not have wanted to know before that he was once to be diagnosed. Another participant, whose mother died from cancer although she never drank or smoke, felt vindicated that he would not be able to prevent cancer at all (male member of an alcoholics support group, P16/G, see below). So, he drew the conclusion that it did not matter whether he went on smoking or quit: I keep smoking nevertheless. It’s my attitude that I cannot be overcautious. If I’m destined to get it, I’ll get it. That’s what I say. In fact, I will not be able to prevent cancer at all. My mother, for example, did neither smoke nor drink. (SR, male, 60–70 years old, smoker, high prevalence of cancer in family, I) Everybody can be affected, that’s for sure. You don’t know exactly who will or who won’t be. I at least don’t know. I’m optimistic and don’t bother. (SR, male, 60–70 years old, I)
From this perspective, staying healthy is a question of fortune and efforts to improve health by preventive behaviors and dealing with cancer risks in more detail are regarded as useless. Thus, the problematic nature of one’s own cancer-related risk behavior is trivialized and used as an argument to neglect self-efficacy and to qualify the responsibility for one’s own health.
Hedonism
From a hedonistic perspective, risks that may emerge from unhealthy lifestyles are accepted, and the consequences are hazarded. Threatening information about negative consequences of health risk behaviors emphasizing the individual’s responsibility for health counteracting the own dispositions would be bothering or provoking, and therefore, they are likely to be rejected to avoid cognitive dissonances. This facilitates enjoying an opulent lifestyle as long as possible and frees oneself from endeavors of staying physically fit. A male patient (SA, 70–80 years old, smoker, P, see below) who had been a heavy smoker admitted that it was his own fault that he was affected from oral cancer; he would not have changed his behavior not even if he had known that he would be affected one day. Overall, this prioritization of enjoyment of life and satisfaction of needs leads to ignorance of warnings about health threats and to not caring about opportunities of cancer prevention and early detection: I don’t want to know in advance about the big check-up or something regular. I was hit like one can be hit by a cold, and that’s it. It’s my fault, I was a heavy smoker. That’s my attitude, isn’t it. I was just lucky until now. (SA, male, 70–80 years old, smoker, affected from oral cancer, P)
Pragmatism
Considering their advanced age, particularly, older people at risk tended to deem healthy behavior and cancer prevention not to be necessary anymore. This perspective is characterized by the acceptance of the finite nature of life or even by an indifferent attitude toward it. This attitude can particularly develop if people do not have strong social networks (anymore). Consequently, there is no motivation of dealing with health-enhancing efforts which is accompanied by indifferent attitudes toward health and risk information. Information is not actively rejected; it is probably tolerated but not used interestedly. One woman aged more than 80 years (SR, high prevalence of cancer in family, I) concluded that she had lived a good and happy life, and now, she would not try to avert the risk of dying from cancer anymore: “When I imagine something happening to me, I also would say: ‘I lived a fine life, and now it’s alright.’” A man affected from oral cancer (SA, 70–80 years old, smoker, P) expected not to live for many more years anyway and thus admitted not to go to the follow-up examinations as long as he felt fine.
I’m feeling quite fine. And so I don’t go to the check-up. I’m 72, young lady. I’m going to have to die someday. (SA, male, 70–80 years old, smoker, affected from oral cancer, I) You know, I’m 63 now, and when in two years, they’d diagnose cancer and tell me I’d only have another 3 years to live, I would make the best of it. Would live with cancer until the end of my life. (SR, male, 60–70 years old, physical and mental impairments, I)
Discussion
The qualitative analysis demonstrated the complexity of the motivational determinants of information and communication behaviors about oral cancer. It gave insights into the cognitive barriers of dealing with oral cancer–related topics and prevention efforts in (high) risk groups in Germany. With regard to the issue of cancer in general and oral cancer in particular, the data particularly revealed difficulties and challenges of dealing with this frightening topic that makes people prefer not to seek or even to avoid information. This can be interpreted as a consequence of high levels of uncertainty perceived negatively, accompanied by deficits in knowledge and a lack of strong self-efficacy beliefs (Brashers, 2001).
Nevertheless, the participants were rather passive in health and cancer communication matters. This is concurrent with studies emphasizing the important role of social context factors on outcomes like risk knowledge and information seeking about cancer (Hovick, Liang, & Kahlor, 2014). The low level of knowledge about oral cancer and problem awareness reported by our participants is in line with findings from previous studies on oral cancer awareness (Hertrampf et al., 2012; Horowitz et al., 2002; Patton et al., 2004; Scott et al., 2008; Scott et al., 2011). However, they did not react on these challenges by acquisition of information that may help to gain a better understanding of the problem and coping-oriented behaviors. These results correspond to research on cancer-related information seeking, particularly, among people from high-risk groups with low educational levels (e.g., Goldman et al., 2009; Lee, Ramírez, Lewis, Gray, & Hornik, 2012; Oduro et al., 2012). It can be assumed that people rather feel at risk of even increasing their perceptions of uncertainty, fear, and helplessness by additional information instead of deriving benefits from them.
Our participants preferred to let themselves be informed by others instead of actively seeking health information from media sources. Obviously, they do not rely on these sources to be supportive in coping with uncertainties and fears and instead rely on their social surrounding and health professionals. Information from these “relevant others” are tailored to the individuals’ dispositions and needs, provide the opportunity to interact and ask again whether something remains unclear. These results point to the importance of self-efficacy beliefs (Barbour et al., 2012; Brashers, 2001): Although information from the media can be overwhelming, interpersonal channels provide information preselection, offer the opportunity of addressing this mental overload, and also provide emotional and functional support. This reduces the risk of increasing uncertainty that evokes negative feelings (Brashers, 2001; Brashers et al., 2002).
The described stepwise process of coding and interpreting the participants’ statements in qualitative analysis (Mayring, 2000) revealed different barriers of dealing with oral cancer and four underlying cognitive and behavioral patterns among typical members of (high) risk groups. They were interpreted as strategies of distancing oneself from potentially existing worries and perceptions of uncertainty, and they help us understand why people avoid information (Brashers et al., 2002). The phenomenon of optimistic bias is well known in other health contexts (Helweg-Larsen & Shepperd, 2001) and has also been discussed for oral cancer (Humphris & Field, 2004). Optimistic bias appears as a strategy of post hoc rationalization that legitimates informational ignorance; the optimistic bias represents a positively evaluated type of uncertainty that is supposed not to be “irritated” by additional information.
The fatalistic view on cancer, particularly, among risk groups with low SES, has been tackled by Niederdeppe and Levy (2007) and has also been described with regard to oral cancer by Lowry and Craven (1999). Fatalism is characterized by a low level of self-efficacy perceptions. In this vein, information is perceived as useless as it may not provide a positive impact for the individual. Rather, information is evaluated in an economic way: It is supposed not to provide any benefit, and thus, it is needless to engage in information seeking.
The pragmatic and the hedonistic perspectives we found refer to strategies of dealing with cancer risks which—to our knowledge—have not yet been focused in cancer communication. They may complement the range of cognitive barriers that prevention efforts have to face in addressing risk groups. The pragmatic perspective clearly focuses on a cost–benefit ratio and evaluates the potential benefits of information in relation to the emotional and further costs that may occur negatively. Some participants take into account their remaining lifetime and decide that it is not worth engaging in information anymore.
From a hedonistic point of view, such a cost–benefit ratio is undertaken as well. The core question is: What are the emotional and functional costs for health-conscious and preventive behaviors? What would I have to dismiss? In this context, additional information might evoke additional stress and cognitive dissonance people generally try to avoid.
The barrier patterns are partly related to motivational key factors of uncertainty management, particularly, to uncertainty perceptions, self-efficacy, or the desire for cognitive consonance as influencing factors of different strategies for uncertainty reduction (Barbour et al., 2012; Brashers, 2001). These four patterns of self-distancing—optimistic bias, fatalism, hedonism, and pragmatism—help to understand why people try to protect themselves from threats by virtual barriers which—from a health expert’s view—would help to improve prevention and early detection but actually can make members of the risk groups particularly difficult to reach by preventive communication efforts (Hartwig & Waller, 2006). We identified different underlying mechanisms which could to be linked to different strategies of dealing with health and cancer-related information, or, more precisely, information avoidance.
Our analysis emphasizes the importance of dealing with strategies of self-distancing and cancer-related information avoidance. Based on our results, we developed the following tentative assumptions on the interrelation between cancer-related cognitive mechanisms and different strategies of health information avoidance: Although (a) optimistic bias seems to be associated to information ignorance, (b) fatalistic beliefs might rather lead to the self-protective denial of information, (c) hedonism seems to evoke active information rejection, and (d) pragmatic beliefs might rather be accompanied by indifference toward information. To understand these strategies of self-distancing better in the future, we would recommend taking an information economic perspective into consideration as well.
Limitations and Future Research
This qualitative research approach aimed at looking beyond the surface and existing scientific knowledge about risk awareness and knowledge about oral cancer and information seeking and avoiding behaviors among people at risk (Hertrampf et al., 2012; Horowitz et al., 2002; Patton et al., 2004; Scott et al., 2008; Scott et al., 2011). This methodological approach is in line with studies focusing on early detection and oral cancer patients’ attitudes and behaviors (Scott et al., 2009; Scott, Grunfeld, Main, & McGurk, 2006; Scott et al., 2011) and underlines that qualitative methods of data collection and analysis are indispensable for exploring in depth the personal and cultural constructions of cancer and risk perceptions, informational needs, and decision-making processes dealing with life-threatening and emotionally charged health issues such as cancer (Hay & Craddock Lee, 2009; Sandelowski, 2004). Of course, using an interview guide restricts openness of the interview in favor of comparability of answers, which is always a decision based on weighting pros and cons of semistructured interview techniques.
The strategies of self-distancing were derived as distinctive motivational patterns, but individuals are not necessarily limited to one of these perspectives. Our results rely on participants who were able and willing to articulate their feelings and thoughts and who retrospectively reported their experiences and behaviors. Some of our interview partners came from educationally disadvantaged backgrounds, were physically and mentally impaired and socially disadvantaged (e.g., homeless, disorientated). This had an effect on their ability of verbalization, on their capacities to articulate their feelings and thoughts and to describe their experiences and behaviors. Here, our situational and problem-oriented way of data collection reaches its limits. Instead, an ethnographic approach would have provided deeper insights.
Moreover, there might be a methodological bias due to the fact that different interview techniques—single interviews, interviews in pairs, one interview in a group setting—were combined which might have affected the findings. Possible effects of the group setting were not taken into account or could be controlled during data collection and analysis. We used the same interview guide, treated the group members during the interviews as individual interview partners, and analyzed each participant’s data as individuals. The decision for this methodological approach was based on the aim of comparability. This is accompanied by the fact that the potential of the group situation has not been exhausted. In general, the aim of comparability and the use of an interview guide can be critically evaluated because it decreased openness and subject-centeredness.
Based on the identification of the target group for oral cancer prevention, this study was conducted as the second step to guide the development and implementation of an oral cancer prevention campaign strategy, particularly, addressing people at risk in Northern Germany. We identified four distinctive patterns of information (non)motivation which should be regarded in the progress of the formative analysis and later on in the campaign planning process. Based on our qualitative data and explorative analysis, we can develop hypotheses on the interrelations between cognitive mechanisms and different strategies of health information avoidance. A focus on the avoidance of information still seems to contrast with most information-campaign research (Case et al., 2005). Further steps of formative evaluation providing evidence on the prevalence and empirical relevance of these cognitive patterns and their interrelations to different types of information avoidance by quantitative research might help to guide oral cancer campaign development. Against the background of the theoretical considerations outlined in this article and our exploration of different self-protective behaviors and uncertainty management strategies by self-distancing from the topic and by avoiding information, we can first conclude that information avoidance cannot be treated as the opposite pole to information seeking, that is, avoiding is not equivalent to not seeking. This requires to develop theoretical models which specify information seeking and avoiding behaviors separately and not only by using one outcome variable covering information seeking as a continuum with extensive seeking and avoiding as two conditions of the same phenomenon. Second, our data indicate that information avoiding is not a unidimensional construct which is only rarely mentioned in the literature to date (e.g., Case et al., 2005). Instead, there are different types of avoiding which need to be differentiated and explained differently.
Footnotes
Acknowledgements
We thank our participants and all the contact persons who facilitated the interviews for their cooperation and for the informative interviews.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by the Friede-Springer Foundation, the Schleswig-Holstein Cancer Association, the German Society for Dentistry and Oral Medicine, the Cancer Research Foundation Head and Neck, the Ministry of Labour, Social Affairs and Health of Schleswig-Holstein, the Schleswig-Holstein Society for Dentistry and Oral Medicine, the Medical, Dental and Pharmaceutical Associations of Schleswig-Holstein, the Association of the Statutory Health Insurance Dentists of Schleswig-Holstein, and donators for supporting the project “Improvement of early detection of oral cancer in the population of Schleswig-Holstein.”