
Abstract
Although medical interpreters are guided by a clear set of medical interpreting standards that are designed to ensure an accurate, clear line of communication between patient and provider, limited research has focused on interpreters’ actual experiences: how they integrate the medical interpreting standards into practice, challenges they might face, how they address those challenges, and with what consequences. To address these gaps, we explored experiences of 15 interpreters working in health care settings. As this is a relatively unexplored area and we are exploring social processes, we used grounded theory. Data were analyzed through open, axial, and selective coding. We found all interpreters intended to practice “within” the encounter and valued the medical interpreting standards. However, patient and provider expectations, requests, and a desire to protect patient–provider relationships led to significant deviations from specific elements of the medical interpreting standards. Findings highlight the need to revise medical interpreting standards.
Keywords
Introduction
More than 350 non-English languages are spoken in the United States, representing 62.1 million people, 19% of whom have limited English proficiency (LEP; U.S. Census Bureau, 2015; Whatley & Batalova, 2013), defined as “speaking English less than well” (U.S. Census Bureau, 2015; Whatley & Batalova, 2013, p. 1). Medical interpreters play a critical role in helping LEP patients communicate with their health care providers.
Medical interpreting became a nationally certified profession in the United States in 2009 (The National Board of Certification for Medical Interpreters, n.d.). As part of the national certification, medical interpreters are expected to follow the national medical standards for interpreting in the health care setting. The purpose of these standards is to increase the quality of medical interpreting in health care, focusing on nine tenets: (a) accuracy, (b) confidentiality, (c) impartiality, (d) respect, (e) cultural awareness, (f) role boundaries, (g) professionalism, (h) professional development, and (i) advocacy (National Council on Interpreting in Health Care, 2005). As part of the certification, interpreters are required to learn the interpreting standards of practice, code of ethics, and national standards for culturally and linguistically appropriate services in health and health care (the National California Learning Assessment System [CLAS] Standards).
Although these standards serve as a guide for interpreting best practices (National Council on Interpreting in Health Care, 2005), meeting them can be challenging in real-life settings (Angelelli, 2004; Brisset, Leanza, & Laforest, 2013; Hsieh, 2006). In a study of interpreters’ reactions to and opinions about the standards, Angelelli (2004) found that interpreters had difficulty meeting them because they sometimes conflict with workplace expectations (e.g., interpreters are expected to be cultural experts, which some are not), creating dilemmas for interpreters in managing the standards within the current clinical encounter. However, little is known about how interpreters manage situations when the standards are difficult to follow. Without understanding the conditions that influence interpreting, interpreting for LEP patients could ultimately lead to errors and poor health outcomes.
Background
Past research has focused on the role of the medical interpreter (Avery, 2001; Dysart-Gale, 2007; Hsieh, 2006, 2008), which has been dichotomized into two approaches: (a) the neutral and (b) the active (Avery, 2001). Specifically, the neutral approach views the medical interpreter as an “instrument” (Avery, 2001, p. 4), who simply passes the message on by providing an accurate and complete transmission of messages conveyed in one language into another language. Such interpreters are not intrusive or relational: They do not establish relationships with the patients or initiate any interventions of their own accord, regardless of the presence of miscommunication (Avery, 2001).
In contrast, the active perspective acknowledges that medical interpreters fulfill roles beyond that of an “instrument” (Avery, 2001, p. 4) and may be part of or have knowledge about the patient’s cultural context. Hence, when a misunderstanding occurs due to cultural factors or assumptions that affect the encounter, the interpreter intervenes (Angelelli, 2004; Dysart-Gale, 2005; Valero-Garces & Martin, 2008). Consistent with the active interpreter perspective, some interpreters feel they play an important role as friends, counselors, and advocates (Angelelli, 2004; Valero-Garces & Martin, 2008) and perceive their role as cultural brokers/mediators or covert codiagnosticians, whereby they actively evaluate the value of information and interpret it accordingly, without others knowing about their screening process (Brisset et al., 2013; Davidson, 2000; Kaufert & Koolage, 1984; Rosenberg, Leanza, & Seller, 2007). Although the current medical interpreting standards acknowledge both the neutral and active perspectives, the role of the interpreter as defined in the standards is consistent with the neutral position (National Council on Interpreting in Health Care, 2005). More research is needed to understand how the current standards play out in clinical settings and how integrating the two perspectives affect medical interpreters’ approaches to interpreting.
Hsieh (2008) examines medical interpreters’ understanding of their roles and the strategies they employ to carry them out. The author found that, despite medical interpreters’ familiarity with these roles, their self-perceived roles did not always coincide with those proposed in the standards. Instead, medical interpreters were found to adopt communication strategies that went beyond the “nonthinking, robotic” (Hsieh, 2008, p. 1), even though they saw themselves as assuming the conduit role. They used verbal (e.g., manipulating linguistic features) and nonverbal strategies (e.g., being silent, avoiding eye contact, standing behind speakers) to reinforce the provider–patient relationship, creating “an illusion of a dyadic interaction” and encouraging the establishment of rapport and trust between patient and provider. In fact, a systematic review of 61 qualitative studies of interpreters in health care settings found that role differences lead to different types of interpreting challenges (Brisset et al., 2013). For instance, greater interpreter advocacy leads to clinicians losing a sense of control or power during clinic consultations (Brisset et al., 2013).
Despite the existing knowledge about medical interpreters, little is known about how interpreters manage the current medical standards and the challenges they thereby face, including how the roles set out in the standards influence their approach and how and when interpreters deviate from the role set out in the standards. Therefore, the purpose of this study is to explore interpreters’ roles in working with LEP patients in health care settings, the challenges they face, the strategies they use in response to those challenges, and how their roles change as a result.
Method
Grounded theory was used to develop a conceptual model of interpreters’ experience of working with LEP patients, including the challenges they face and the strategies they employ to respond to those challenges. This methodology was selected because it is particularly well suited for understanding social processes and explaining the relationship between understandings or perspectives and actions in social situations (Corbin & Strauss, 2008; Strauss, 1987). Sampling, data collection, and analysis occurred through an iterative process (Corbin & Strauss, 2008; Strauss, 1987). The ongoing analysis was guided and informed by theoretical sampling through the modification of interview questions and selection of participants (Corbin & Strauss, 2008; Strauss, 1987). Data were inductively and progressively abstracted into a conceptual model as the study progressed (Corbin & Strauss, 2008). In particular, a conceptual model or “integrative diagram” is useful in bringing together the core process (e.g., deviating from the standards) with the conditions influencing that process and the strategies employed to implement it (Strauss, 1987; Thornberg, Perhamus, & Charmaz, 2012). This study was approved by the University of Wisconsin–Madison Institutional Health Review board (institutional review board [IRB]). Consent was obtained from the medical interpreters prior to their participation in the interviews.
Sample and Setting
Medical interpreters, including hospital- and clinic-based interpreters, were recruited from one large health care system in the Midwest. Recruitment flyers were emailed using the health care system. Potential participants were directed to contact the researchers if interested. Interpreters were eligible for the study if they were aged 18 years or older, self-identified as a medical interpreter, and were willing to participate in a face-to-face interview. Participants were provided a US $50 honorarium.
Data Collection and Analysis
Convenience and theoretical sampling were used to obtain the final sample of 15 interpreters. Convenience sampling was used at the onset of the study. For example, researchers recruited interpreters who responded to the flyers and met the inclusion criteria. Theoretical sampling was used for follow-up and further probing in response to the ongoing data analysis (Corbin & Strauss, 2008). Researchers deliberately recruited interpreters and modified interview questions to facilitate a comparative analysis of community membership and relationships that might highlight significant conditions influencing the nature and response to interpreting challenges. For example, on discovering that forming part of the same community as the patients influenced interpreters’ strategies, the researchers added a question to subsequent interviews about whether or how “same community membership” influenced interpreting and also sought additional interpreters who could inform them about whether or how they responded to this condition. This questioning also led to a discovery about the significance of interpreting in participants’ native versus second language. Sampling and interview question evolution continued until saturation of primary categories was reached, and integration across influencing conditions and interpreting strategies was identified.
Table 1 illustrates the evolution of the interview questions. Initially, data collection began with open-ended, nondirective questions, becoming increasingly focused as the analysis progressed. For example, an initial interview question was “Tell me what it is like to be an interpreter.” This was followed by several additional broad questions to address issues grounded in previous participants’ experiences and coded during data analysis. Participants often initiated their responses by stating they followed the medical interpreting standards of practice but encountered challenges. We subsequently asked, “Tell me more about the medical interpreting standards of practice.” As most participants described often being unable to follow the standards, we focused on interpreters deviating from them. This led to questions and discussions related to when and how standards were or were not followed. Individual face-to-face interviews lasted between 40 and 120 minutes and took place at a convenient location of the interpreter’s choice (i.e., home, library, or clinical setting). Interviews were audio taped and transcribed. Each participant was interviewed once, with the exception of one interpreter who called the researcher and requested a second interview because he wanted to share more about his experiences.
Evolution of Interview Question Examples.
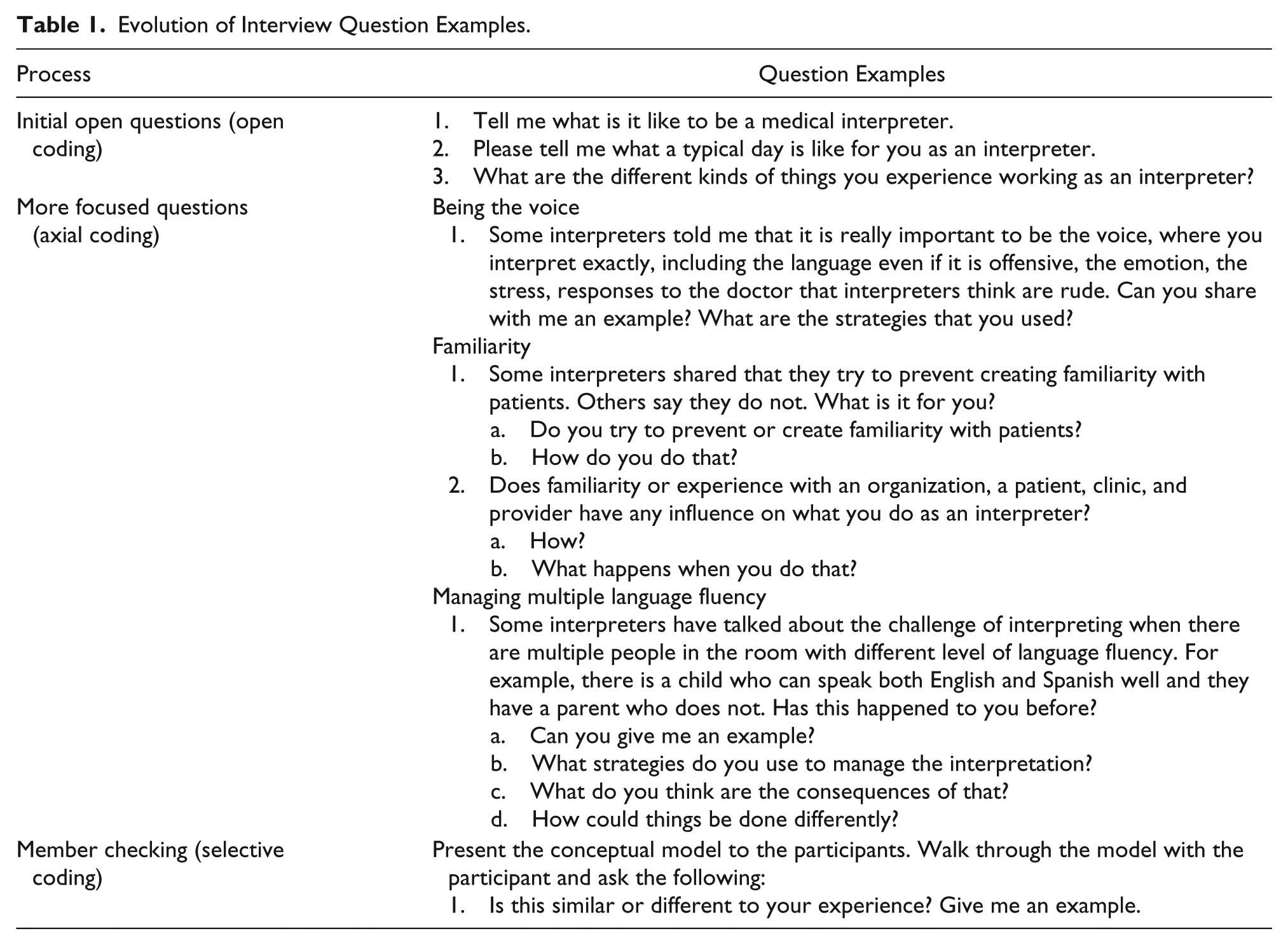
Data were analyzed using open, axial, and selective coding (Charmaz, 2014; Strauss, 1987). Open coding involved reading the data line by line and identifying and dimensionalizing categories (Bowers & Schatzman, 2009; Charmaz, 2014; Corbin & Strauss, 2008). Codes were assigned to categories, dimensions, and subdimensions, and organized into a matrix based on the categorical relationships identified during the analysis. For example, when participants talked about the implementation of the medical interpreting standards, for instance, in noting that it’s our goal to say what is said . . . and not to modify, add, or subtract from what’s being said because it takes away from the encounter, and it takes away from people’s ability to create a relationship or have the information they need [we coded these passages as implementing the standards].
The subdimensions of implementing the standards were “voluntary” (e.g., initiated by interpreters) and “involuntary” (e.g., forced by provider, clinic, or patient). For example, the major strategy was “being the voice,” within which we identified the subdimensions of “being the voice,” “being in the shadow,” and “behaving in the same way as the patient” as examples. We pursued interpreters’ strategies by exploring what it meant to be “in the shadow,” how they “stayed in the shadow,” and what “being the voice” involved. This included exploring how each of these subdimensions was altered by changing conditions and contexts. The modified interview questions reflected this.
The next phase, axial coding, involved breaking down and specifying the context associated with the categories (e.g., when, how, or under which conditions a phenomenon may occur, and which consequences, interactions, and strategies are connected to it). For example, interpreters deviated from the medical interpreting standard of accurately passing on what was said when they received requests from providers and staff. Hence, to identify the processes and core category, we asked participants in subsequent interviews about additional conditions that led them to deviate from the standards.
Finally, selective coding was used to articulate the core category and finalize the evolving conceptual model (Strauss, 2003). For example, one core category was balancing one’s interpreting role: being neutral and active while still meeting the medical interpreting standards. Saturation occurred when the team no longer identified or constructed new categories, subcategories, or links from the data. For this study, we reached saturation on the category deviating from the medical interpreting standards. Although identified as likely important for understanding medical interpreting work, we did not reach saturation on the following categories: (a) dealing with relationships outside of the health care encounter and (b) managing side conversations between providers and assistants.
Rigor
We employed multiple strategies to increase rigor (Charmaz, 2014). To ensure credibility, we described categories that covered a wide range of participants’ experiences and provided evidence for the findings using quotes from multiple participants (Charmaz, 2014). To achieve originality, we chose categories that provided new insights and built on existing literature (Charmaz, 2014). Memoing also took place after each data analysis session, so that conceptual decisions, analysis progression, and theoretical sampling decisions were clearly documented. For example, memos included details on researchers’ “hunches” (Strauss, 1987) about the data, emerging categories, newly discovered dimensions, relationships between categories, ideas for theoretical sampling, and changes to the conceptual model with a rationale for each change. Data analysis was conducted with a research team of three doctoral students and an experienced senior grounded theory methodologist. To generalize the results, we sampled for theoretically relevant diversity using theoretical sampling, which is particularly useful for analytic generalizability and allows for assessing the applicability of the study conclusions (Firestone, 1993).
Furthermore, for confirmability and transferability, and to determine whether the conceptual model was representative of participants’ experience, we presented the conceptual model to the interviewees as it evolved. In grounded theory, such member checking is used both to confirm what has already been documented and to expand the analysis by identifying additional dimensions or new conditions (Charmaz, 2014) and their associated strategies. We pursued this by asking participants to review and comment on the evolving conceptual model, its categories, and the relationships among the categories, as well as to identify whether or where they fit. This included commenting on how their own experience might vary from what was reflected in the conceptual model, as well as identifying gaps in the model. During member checking, all subsequent participants confirmed the conceptual model was consistent with their experience. In addition, participants also provided new examples of categories and their relationships. For example, several interpreters shared additional examples of strategies they used to preserve the relationship. By the eighth interviewee, we identified no additional categories or subcategories but continued to conduct member checking until we reached 15, at which point, the participants identified no new processes.
Results
Fifteen interpreters participated in the study. Their ages ranged from 26 to 62 years and the majority were female (n = 13, 87%) and Spanish language interpreters (n = 8, 53%; see Table 2 for details of the interpreters’ demographic characteristics).
Demographic Characteristics of Medical Interpreters.

All interpreters indicated following the medical interpreting standards, that is, accurately interpreting information. Interpreters consistently described their primary strategy for achieving this as “being the voice” of the patients and their providers, and “staying in the shadow,” consistent with their role as interpreters. Being the voice means interpreters “channel” word-for-word what is said by both patient and provider, interpreting as accurately as possible, which includes saying only what the patient and provider said. They described themselves as conduits between the patient and provider. One interpreter noted, “I train to be the voice of my patients. I train to be the voice of my providers.”
Staying in the shadow means the interpreters must refrain from interrupting or interjecting themselves into the conversation. They also agreed on the importance of interpreting precisely and completely, which included saying only what the patient and provider said, and not omitting, adding, or substituting anything, consistent with the medical standard of accuracy. In this way, they become the voice of the patient or provider, a conduit, while remaining outside of the interaction and, therefore, “in the shadow.” One participant noted, We say things as they are and never add or omit anything . . . So for us, it is really important that we follow the guides of interpretation and never use our own words or knowledge to add or to omit anything.
Being invisible also means encouraging patients and providers to avoid using third-person statements such as “Can you ask her where her pain is?” Such a statement acknowledges the presence of a third person, the interpreter. In addition, several interpreters also emphasized that to be in the shadow requires that they behave in the same way as the patient during the interpretation, which included maintaining the same tone of voice. One interpreter stated, “We can express in the same way. So like, if he, he did, ‘yes, I have a lot of pain’ [Participant mimics the behavior].”
Deviating From the Role in the Medical Interpreting Standards
Despite emphasizing the importance of following the medical interpreting standards, the participants’ descriptions of their work focused on when and how they deviated from the standards. Specifically, although the standards focus on the nine tenets of medical interpreting, interpreters mainly focused on deviating from the role of boundaries tenant. Interpreters described two general categories of deviating from their interpreting role: (a) deviations initiated by others involved in the interaction and (b) deviations initiated by interpreters (Figure 1). In addition, they discussed the strategies they employed to remain in their interpreting roles, the conditions that threatened accurate interpretation, and the consequences of following the standards (the conduit approach).

Conceptual model of deviating from medical interpreting standard: Role.
Deviations initiated by others involved in the interaction
“Other-initiated” deviations occurred when patients, providers, or staff made specific requests of the interpreters that, if honored, took them outside of their interpreter roles.
Requests from providers and staff
Requests from providers and clinic staff occur when (a) providers or staff recognize that patients cannot read or write, (b) patients appear not to understand the information they are given, (c) providers need a witness to verify medical procedures, and/or (d) the interpreter has a history with the provider or clinic. Consequently, interpreters are asked to perform a range of tasks that alter their role as interpreters. These tasks include helping the patient fill out surveys or other paperwork (e.g., reading and explaining consent forms for medical procedures), accompanying the patient to a procedure, and/or asking the interpreter to determine how to help the patient understand something. One interpreter shared an example of staff making a request: For example, yeah, we in the clinic, they were giving, ah, they were asking the patients to fill out a questionnaire about their childhood and they were asking very personal questions, and some, and when we were doing that, they asked the interpreters to be there and help the patients.
Regarding the instance of the provider needing a witness to verify medical procedures, one interpreter explained her experience with a doctor who asked her to be a chaperone for a medical procedure: Another one that’s awkward is when, this doesn’t happen often, but when the doctor, a male doctor usually has to have a female chaperone in the room if he’s going to do a pelvic exam, for example. And I had a male doctor who’s busy and be like “okay, well it’ll be okay cuz you’re in the room. So you can be the chaperon.” But I have no training to be a chaperone. That’s not part of my job and I don’t know what I’m chaperoning for any of this. So I’ll just “no, I’ll be behind the curtain.”
In relation to interpreter having a history with the provider or clinic, interpreters reported being asked to assist patients in the labs. One interpreter noted, “The provider will say, ‘you have been here so long, why don’t you take the patient to the lab?[sic]’” Consequently, interpreters indicated that such requests can lead to conversations with the patients, which can include questions related to their current health encounter, additional exposure of health information, or requests from the patients. Such requests bring the interpreters outside of their roles and out of the shadow, placing them in a difficult position during subsequent appointments with the provider (e.g., if patients share information relevant to their health and later decide not to share it with the physician but the interpreter believes the information to be important).
Requests from patients
Requests from patients occur when (a) the interpreter met with the patient prior to the clinic appointment to explain how interpreting works or obtain more details about the patient’s goals during the clinic visit, (b) the interpreter interpreted for the patient in the past and has previous personal health information about the patient, (c) the interpreter had an ongoing personal relationship with the patient, and/or (d) both were from the same community. In the first instance, whereby the interpreter meets with the patient prior to the clinic appointment, disclosure of the patient’s personal health information can occur outside of the encounter with the provider, either in the waiting area or in the clinic room, in the absence of the doctor. One interpreter recounted that when the mother of a teenager and provider left the clinic room, “The case for example the teenager ok, pregnant but don’t tell my mom or whatever. The patient tells you, ‘Ok, but don’t say this to my mom.’”
Having a prior or ongoing relationship or being from the same community also led to requests from patients, such as providing a ride to the clinic or attending community events outside of the health encounter. These requests were mainly from patients who were from the same community as the interpreter. One interpreter said she provided rides to patients when she first started working as an interpreter, bringing her out of her interpreting role: At first, I did things that were wrong. For example, I was picking up patients and give them rides because they asked me to do so, but I was too naïve. I didn’t know we weren’t supposed to do that . . . I felt terrible . . . what happens if you have an accident or whatever, imagine that? Terrible.
Many interpreters described having agreed to requests such as providing rides early in their careers but ending that practice over time because they realized the consequences of bringing personal relationships into their interpreting work. In addition, the interpreters recognized that such tasks take them too far out of their role and entail too great a deviation from the standards.
Familiarity
The interpreters reported a range of ways in which familiarity with providers, patients, health care systems, and language influenced their interpreting, thereby altering their ability to maintain the standards of role boundaries.
Familiarity with provider
Interpreters’ familiarity with providers, having worked with them previously or over time, often affected their ability to stay in the shadow. A greater familiarity between the interpreter and provider often led to providers asking interpreters to do things that fell outside of their roles, inconsistent with the medical interpreting standard of role boundaries. Examples include changing the provider’s statement to something the interpreter believes is more understandable or substituting statements for the provider to explain a procedure with which he or she knows the interpreter is familiar. One interpreter shared what a provider said to her: “You heard me explain this five million times, why don’t you just explain it to the patient what their follow up looks like.” Consequently, being familiar with the provider and health issue increases the likelihood of deviating from the medical interpreting standards of role boundaries, specifically by the provider’s explicit inclusion of the interpreter as an active participant in the interaction. This also increases the likelihood that the interpreter provides substantive health-related information without any oversight or review for accuracy.
Familiarity with patient
Several interpreters indicated that working with the same patient over time or being from the same community as the patient can bring them out of the shadow, causing them to deviate from the medical interpreting standards. An interpreter from “the same community” is one who speaks the interpreted language as his or her first language or identifies with the same ethnicity as the patient. For instance, several interpreters who were from the same community as their patients reported being cultural brokers between the patient and provider, causing them to come out of the shadow and use their own voice to facilitate patient comprehension or explain perspectives and cultural practices bidirectionally to providers and patients. For example, one interpreter shared his experience of directing comments to the providers in an attempt to bring cultural aspects into the interaction: So providers inquire about these things: “Did you use any medicine for this problem?” . . . they use some herbal things. They explained about the herbal things and the providers are not aware and they asked me, “What is this?” Then I tell them “yeah, this is our culture and traditional belief that these things work best in these situations curing for coughing or fever or some kind of pain.” . . . So [being from] the same community, I know what my people thinking or have belief of these things.
Also interpreters who are not from the same community but worked with a patient previously have clinical and biographical knowledge about the patient that is sometimes relevant. Interpreters describe coming out of the shadow to provide explanations when the provider lacks information or is unable to understand what the patient is saying. One interpreter said, This individual was senior citizen age, approximately, and they had someone else from their community with them, but I was getting those signs that I talked about like the responses were not what I was expecting. Ah, I had a hard time understanding what they were saying and so right within the first five minutes of the appointment, I basically said, “time out” to everyone in the room and said, “this interpreter, I am not confident that the interpretation is going well or going cleanly.”
Familiarity with the health care system
When patients are unfamiliar with the health care system, interpreters often find themselves having to provide them with explanations or information in addition to what providers say, bringing the interpreter out of the shadow. This was described by the participants as occurring when patients were inexperienced with Western health care systems or new to a specific health clinic or health condition. One interpreter shared an experience she had with a patient who was new to the United States: “The provider left and the patient was confused about whether the encounter was over. I had to tell her, ‘the appointment is done.’” Another interpreter recounted having to provide both patients and providers with explanations: I was interpreting for a pregnant woman now and one of them said something about, “I need to buy this baby stuff” and I did give her advice . . . Another person, who was pregnant said “I need to establish care with a gynecologist . . . The provider did not know that in Brazil, people establish care with a gynecologist instead of the primary care provider so I had to explain to the provider.”
Familiarity with the language
Interpreters’ familiarity with a patient’s language and relevant medical terminology in both languages played a critical role in determining whether the interpreter deviated from the medical interpreting standards. Many of the participants acknowledged the subtle differences between languages that could cause confusion and require them to “come out of shadow” to explain. For example, some patients have different dialects, accents, or are from geographical regions or generations with varying cultural norms and terminology. There are generational differences in language use, even within single communities. The participants described having to interpret for all these variations, making it difficult to interpret accurately, as a result of which patients often ask for explanations, forcing the interpreter to repeat, rephrase, or explain, and thereby bringing them out of the shadow. One interpreter described that Sometimes the providers . . . they assume that we are all the same, which is a big problem. And when you are talking about Mexicans, Puerto-Rican, Central Americans, South Americans, Cubans, Caribbean Islands, it’s different. Because they have somewhat different vocabulary . . . They think we’re all Mexicans.
Altering the conversation flow
The participants described a number of conditions that altered the conversation flow while interpreting, contributing to deviations from the medical interpreting standards. These included (a) keeping up with the conversation and/or (b) discordance between the patient’s language and that scheduled for interpretation, and (c) use of the third person.
Keeping up with the conversation
The participants indicated that when patients, family members, and/or providers talked “nonstop,” they had difficulty in accurately recalling what was said. Another condition that made it difficult to “keep up with the conversation flow” was when multiple people (often family) were in the room. One interpreter described what it was like when the provider talked continuously: “The provider said, ‘let me finish my statement’ but that was a long, long statement. I have a hard time remembering.” In these situations, the patients included the interpreter as a third person in the conversation, leading them to deviate from being the voice of both the patient and provider. Some interpreters said that some patients brought family members to the encounter, making it difficult to maintain or interpret the conversation flow due to multiple people talking at the same time. As an interpreter explained, It’s hard to interpret when the patient brings a lot of family members to the encounter, especially when there is more than one person speaking at the same time . . . The challenge is you have to figure out what both people are saying at the same time and how to interpret that to the provider.
Discordance in the language scheduled for interpretation
Several participants indicated that patient populations sometimes do not speak the language they were scheduled to interpret. Consequently, interpreters find it difficult to understand and accurately convey what is being said, that is, to be the patient’s voice. For example, some patients speak indigenous languages that are not documented in the medical record and for which there are no interpreters. When a patient speaks an indigenous language, she or he mostly brings an intermediary, typically a family member and often a child, to interpret for her or him. As a result, the interpreting situation flows from patient to child, from child to interpreter, and from interpreter to provider, leaving the interpreter unsure about the accuracy of the interpretation. One interpreter said, I was scheduled to interpret for a Spanish speaking patient but when I got to the encounter, I learned that the patient did not speak Spanish. He speaks an indigenous language and had his son present to translate from the indigenous language to Spanish. Then I interpreted the Spanish to English to the provider.
Patient or provider’s use of the third person
The participants indicated that the use of the third person also altered the conservation flow during medical interpreting. Both patients and providers use the third person in certain situations, for example, I started getting drawn into the situation because the patient switched from talking directly to the doctor in first person to talking to me as an interpreter referring to the doctor. The patient started saying “tell the doctor, tell him” when the patient started getting upset. He switched the way he was talking.
Deviations initiated by interpreters
Deviations are sometimes initiated by interpreters, depending on their personal goals. Interpreter-initiated deviation occurs, for instance, when interpreters try to (a) improve clarity, (b) advocate, (c) bring knowledge from another setting into a conversation, or (d) preserve relationships between patients and providers. In these instances, interpreters interject and deliberately alter the message from patient to provider or from provider to patient, deviating from the standards in terms of their roles.
Interjecting
The participants said they interject to improve clarity and accuracy, as well as to advocate and bring knowledge from other settings into the conversation with the provider. Interjecting is used when interpreters need clarification on an unfamiliar medical term used by the provider, to clarify what a patient wishes to convey to the provider, to clarify the interpreter’s role, and to slow down the conversation or stop the patient and provider from talking without a break for the interpreter to keep up. Interjecting is used when interpreters observe cues from the patient indicating she or he does not understand what is being said, at which point the interpreter must decide on whether to try to explain the content, do nothing, or tell the provider, the patient does not understand. One interpreter recounted asking for an explanation from the provider, saying “Doctor, would you mind giving some examples to make the interpretation more clear?”
In other cases, interpreters assisted the provider in clarifying the message without waiting for the patient to respond: like they say “describe the pain,” I might clarify with the provider “are you looking for duration, what aggravates it? Type of pain in the sense of throbbing, burning, stinging?” and let the provider provide that clarification of what you’re looking for.
In this case, the interpreter was familiar with the type of questions providers ask, and how patients generally understand such questions. Consequently, the interpreter did not wait for patient cues, indicating lack of comprehension.
Furthermore, a majority of the participants said they also interject when providers and patients use the third person. One interpreter shared, “I would say, ‘Just so you know, you can feel free to speak directly to the patient. You don’t have to say ‘ask her.’”
A few of the participants described sometimes interjecting when they knew something about the patient that was not offered during the conversation. In particular, they interjected to ask the patient whether she or he wants to share specific information with the provider, ultimately trying to improve accuracy. As one interpreter explained, They start, you know saying, “I’ve been taking my medications every week just like I’m supposed to.” When in the waiting room, they were like “No I don’t bother anymore. I don’t need it.” So I might check in like, “before you told me no” and I’m doing this as an aside [interpreter uses sign language]. So they know I’m not in the interpreting mode at the moment but I will just check in like “before you said, you’re not taking medications. You are? Ok?” and I would just make sure that, because I might like have little moments of self-doubt . . . Like “Did I misunderstand what you said before or said no?” So I’ll double check and go head. And so, if they want to lie then yeah.
In this example, the interpreter asked whether the patient wanted to offer the information he or she shared with her about the medications. As the patient said “no,” the interpreter did not interpret any information about not taking the medication.
Similarly, when providers have side conversations with a third party, often a medical resident or dental assistant, or when they perform dictation during the encounter, interpreters also interject to inquire whether the provider wishes the interpreter to interpret what is being said. One interpreter said, I was interpreting for a dental appointment and the dentist and dental assistant were having side conversations about their weekend and the patient is just sitting there. I interrupted and said, “Did you want me to interpret that? Just so that you know, anything you say, I will have to interpret for the patient.”
In this example, the provider said “no”; hence, the interpreter did not interpret the information to the patient. However, some participants indicated that in instances such as this, they would paraphrase or provide an interpretation of what was discussed instead, or interpreting directly.
Deliberately altering the message
The participants who described deliberately changing either the patient or provider’s statements by adding, omitting, or substituting information, consistently did so to preserve or protect the patient–provider relationship. This mostly occurred when the patient or provider used offensive language toward the other. As a result, interpreters described trying to soften the language or alter the emotional message. For example, when a patient uses profanity or makes offensive statements, interpreters may change the terminology or tone, or explain the patient’s response to the provider. As one interpreter described, I just sometimes, sometimes it’s just, I just have to add some explanations about the context of what the person’s saying a little bit. I had a patient who really awkwardly . . . it was in dental, she had a provider who was, seemed to be South Asian and speaks [sic] with an accent and the patient was like, “I love Hindu people! I always get along with Hindu people.” And I’m like this is ahmm a way of speaking in, I know this, I know Latin America, that people tend to say Hindu, it means it’s from India, Pakistan, or South Asia; it doesn’t necessary refer to their religion, but they are literally saying a religion from that region . . . So it’s really weird and uncomfortable.
Similarly, when the provider says something offensive to the patient or speaks in a way that suggests anger or disrespect toward the patient, interpreters often try to change the tone while maintaining the basic message. As one interpreter explained, “I say everything but I change the tone because if the patient is being yelled at by the provider, why does another person have to yell at him?”
Discussion
We found that interpreters work hard to meet the medical interpreting standards—being invisible, helping with communication between the patient and provider, and being the voice—but in certain circumstances deviate from those standards, specifically regarding their interpreting role. This is consistent with previous research (Angelelli, 2004; Hsieh, 2006). An interesting finding of our study is that the participants deviated from the medical interpreting standards because they wanted to enhance the relationship and/or communication between the patient and health care provider, or because the provider or patient pushed them in some way (e.g., through terminology use or requests) to deviate from the standards. This is consistent with previous studies asserting that interpreters encourage the establishment of rapport and trust between patient and provider (Hsieh, 2008).
We found that familiarity was a driving force behind interpreters’ deviations from the standards of practice; when patients, providers, and interpreters are familiar with each other, whether from having a relationship or working with each other over time, the interpreter is brought out of the shadow and unable to maintain the conduit role. However, it is not yet known whether familiarity between the interpreter and patient causes the patient to say more or less during a health care encounter, whether it invites interpreters to add their own ideas or opinions, and whether this has a positive or negative impact on the quality of patient care.
Consistent with other studies (Angelelli, 2004; Dysart-Gale, 2005), we found that the conduit model of interpreter communication (also known as being the voice) is incomplete; sometimes, the interpreters act almost entirely in accordance with this model and sometimes they deviate from it. Problematic integration (PI) theory might be a useful way to understand such deviations. According to PI theory, “people are constantly forming probabilistic and evaluative orientations to their own experience,” that is, seeking means by which to find answers to the issues or problems in their lives (probabilistic orientations) and determining whether their experience is positive or negative (evaluative orientations), which can result in problem identification (Babrow, 2015). Communication is critical in interpretation, as it is the major channel through which the PI experiences that are relevant to medical interpreters occur. Although we did not use PI theory (Babrow, 2015) in this study to explain the relationship between expectations and desires, future studies could use this model to explore cognitive and communicative responses to the challenges of following the medical interpreting standards, specifically regarding the tensions between interpreters’ perceived likelihood of deviating from the standards and their perceived value of the medical interpreting standards.
In addition, our findings illustrate the context-based nature of interpreting, that is, the quality of interpretation is dependency on whether one is familiar with the patient, provider, and organization, as well as on the languages one interprets. This finding also confirms LEP patients’ reports in previous studies about their observations of the challenges interpreters face during health care encounters (Lor, Xiong, Schwei, Bowers, & Jacobs, 2014; Squires & Jacobs, 2016).
Many participants discussed that variations in the patients’ linguistic abilities (e.g., not speaking Spanish but rather an indigenous language) affected their ability to interpret accurately. This finding is consistent with the work of Davidson (2000), who found that interpreters encountered the realities of different linguistic systems among patients who convey contextual information differently. This study found that particularly when the interpreted language is a second language for the interpreter, he or she may lack an understanding of linguistic nuances, which negatively affects the quality of the interpretation. Alternatively, interpreters may not be familiar with some of the medical terminology, requiring them to interject and ask for clarification. More research is needed to understand how interpretation quality differs depending on whether the interpreter is a native speaker of the language she or he interprets.
Clinical Implications
Our study findings have several clinical implications. Because the findings reveal that providers often make requests of interpreters that take them outside of their roles, leading them to deviate from the medical interpreting standards, training providers on how to work with medical interpreters and LEP populations could be a potential solution to address the challenges interpreters face. Second, judging from the deviations that occur when interpreters are obliged to interject due to comprehension issues and when multiple people are in the room, time is an important consideration. Reminders to patients and family members that only one person should talk at a time could also help to facilitate interpretation.
Furthermore, there should also be initiatives to help patients understand more about the interpreting process and interpreters’ roles to prevent patients from making requests outside of the encounter, as well as helping patients set realistic expectations of interpreters. In addition, there is a need for a platform on which interpreters can share patients’ requests with hospitals, clinics, and providers. Although most of the interpreters told us their role consists partly of informing patients about the interpretation process, they do not always feel it is necessary to repeat it or are not comfortable repeating it with patients they worked with previously. Hence, there needs to be a discussion on who should inform patients about how interpreting is done.
Policy Implications
This study’s findings have significant implications for policy. First, we learned that interpreters work hard to practice within their scope and recognize they are good for patients and providers. However, there are multiple conditions such as receiving requests from patients and health care providers that make it difficult for interpreters to meet the national standards. Thus, it is critical that hospitals, clinics, and providers recognize that the medical interpreting standards are important and try to prevent interpreters’ deviations from them. For example, providers can help by not asking interpreters to perform tasks for which they are not responsible, such as explaining something they have heard multiple times. There is an urgent need to revisit the medical interpreting standards. As this study’s findings show, even though the current medical interpreting standards are designed to acknowledge the dual perspective of being active and neutral, both are defined in a way that is more consistent with the neutral role. Policy makers should consider the standards’ feasibility in clinical practice to determine whether there is a need to modify them or increase the amount of training interpreters receive to equip them to navigate situations such as requests from patients and/or providers. Second, there is a need for integrating medical interpreters within the health care system to create a seamless process for medical interpretation. Third, it is critical that health care organizations take into consideration the language differences among LEP populations by providing medical interpreting services that are specific to patients’ languages.
Study Limitations
Our study is not without limitations. We only conducted interviews with interpreters. For this reason, we cannot comment on how deviations affect health care providers or patients. In addition, we only focused in depth on one interpreting phenomenon: deviating from the medical interpreting standards. Future research should focus on other areas such as how interpreting differs between interpreters who are versus those who are not from the same community as the patient.
Conclusion
This study provides insights into interpreters’ experiences in working with LEP patients in health care settings, the challenges they face, and the strategies they employ to respond to those challenges. We learned that medical interpreters typically follow the standards but, at times, deviate from them, mostly for good reasons, that is, to improve communication and/or build rapport between patients and providers. Future research is needed to examine how the medical interpreting standards can be adapted to the context in which interpreters work.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.