
Abstract
Through this constructivist grounded theory study, it was our purpose to create a substantive theory to explain how rural-dwelling, working-age adults with disabilities define and pursue well-being. Twelve rural-dwelling participants were interviewed up to 3 times to understand the processes involved in defining and pursuing well-being. From this exploration, we suggest that well-being is not a set state to be achieved and then enjoyed, rather well-being results from establishing and maintaining membership in the rural community. Membership facilitated access to the array of material and psychological supports needed for a sense of well-being. Findings support the assumption that urban models of care are insufficient for rural areas. This study also provides an understanding of how individuals in this population mobilize resources to overcome functional limitations and environmental barriers to establish group membership and create a sense of well-being. Implications for health care practice and policy are discussed.
Keywords
Disability among working-age adults is a significant issue in rural America, and evidence suggests a systematic relationship between impairment rates and geography (von Reichert, Greiman, & Myers, 2014). While rural Americans account for a small percentage of the total U.S. population, rural dwellers have higher rates of disability: 17.1% of rural Americans report some type of disabling condition compared with 11.7% of urban adults (Research and Training Center on Disability in Rural Communities, 2017). Similar statistics are found worldwide with a higher prevalence of disability in rural communities than in urban areas (World Health Organization, 2011). The higher rates of disability in rural areas persist across gender, race, and type of impairment. Data also indicate that the disparities in disability exist across all age groups, and the highest differences occur in working-age adults (Myers, Greiman, von Reichert, & Seekins, 2016).
Despite the disparities in disability between urban and rural areas, we know very little about the experience of living with a disability in rural America. This is problematic given the influence that sociocultural and environmental factors have on well-being for people with disabilities (Drum, 2014; Harrison, Umberson, Lin, & Cheng, 2010). Cultural expectations regarding social role performance or social activities may impact rural dwellers’ well-being because of the importance placed on shared cultural experiences. Harrison (2009) stated that age-based cultural norms have a direct bearing on the process of disablement as social role success is dependent upon individual ability within cultural expectations of roles and behaviors. Eng, Salmon, and Mullan (1992) argued that determinants of health-related behavior are rooted in the intricate relations between individuals, organizations, neighborhoods, families, and friends. Thus, it is important to understand how disability affects rural-dwelling individuals’ fulfillment of normative, albeit culturally derived, social roles and how rural dwellers adapt to impairments and mobilize resources to pursue well-being. The research question driving this study is as follows:
Next, we present the study and findings. Last, implications of the findings for rural health care service delivery, research, policy, and program development are discussed.
Method
After approval from the university institutional review board, we conducted a constructivist grounded theory study (Charmaz, 2006) using the constant comparative method of data analysis (Strauss & Corbin, 1998). Constructivist grounded theory is a methodology in which the constructionist point of view is developed through interpretive understandings of individuals’ experiences and aims for “abstract understandings that theorize relationships between concepts” (Charmaz, 2014, p. 228) and attempts to make sense of the studied phenomenon by conceptualizing it in abstract terms without explicit causality (Rieger, 2018). Specifically, it was chosen to study well-being in rural-dwelling, working-age adults because working-age adults are assumed to choose the location of their homes, to voice their rationales for their choices, and to explain how their choices impact their pursuit of well-being.
Sensitizing Framework
We used a sensitizing framework that incorporated symbolic interactionism (SI; Blumer, 1969) with tenets from Amartya Sen’s (1992) capabilities approach to structure the data collection and analysis. Sensitizing concepts refer to background ideas that inform the overall research problem by drawing attention to important features of social interaction (Charmaz, 2003). In inductive research such as grounded theory, a sensitizing framework can provide points of departure in data collection and can serve as a foundation for the interpretation and analysis of data (Bowen, 2006).
The foundation of SI is comprised of three assumptions: (a) people strive and act toward what represents meaning for them, (b) meaning arises out of social interaction, and (c) meaning is dealt with and modified through interpretive processes (Blumer, 1969). Thus, a core principle of SI is the inseparability of the individual and the context within which that person exists. Using SI as a sensitizing framework facilitated examination of the preconditions necessary for human agency and the meanings associated with various actions. The capabilities approach (Sen, 1992) holds that when evaluating well-being, the person’s ability and capacity to function—what a person can do or be—should be captured and studied, rather than common variables such as income, wealth, or happiness. The capabilities approach explicitly acknowledges that depending upon a person’s circumstances, he or she may require different kinds or different amounts of goods or services to be able to transform those resources into valued outcomes.
Recruitment
Participants were recruited through community gatekeepers such as church staff and Veterans’ Services Officers, newspaper classified advertisements, word-of-mouth, and professional networks. Sampling and recruitment methods are detailed elsewhere (Thurman & Harrison, Manuscript under review). Participants were offered US$25 for participating in each interview. We recruited participants purposively based on the inclusion criteria of age, rural residence, English language, and self-report of physical or sensory impairment. Participants had to be between the ages of 35 and 70 years of age. This age group was targeted because the urban–rural disparity in disability is highest in this age group (Myers et al., 2016) and because the adult years are considered a period of time when health, function, work, and independence are of paramount importance (Priestley, 2003).
Participants were required to reside in a county in Texas classified as noncore (typically defined as <10,000 residents) according to the Office of Management and Budget (OMB) rural classification codes (U.S. Department of Agriculture, Economic Research Service, 2017), be community-dwelling, understand spoken or written English, and be able to communicate verbally in English or through an interpreter. Participants also had to respond “yes” to one of the subset of questions from the American Community Survey (U.S. Census Bureau, 2014) designed to identify people who may experience mobility, hearing, and/or vision impairments. Between June 2017 and January 2018, 22 people contacted the first author and/or gave a gatekeeper a message consenting for contact. Each was called by the first author, screened for inclusion, and told the study details. Ten were ultimately ineligible to participate because they did not meet inclusion criteria. No one who was eligible for the study declined to participate after being informed of the study details.
Sampling Methods
Consistent with constructivist grounded theory, purposive sampling was initially used to identify participants for the study. Thus, we targeted those who met the criteria of age, rural residence, and disability. As the study analysis matured, theoretical sampling became necessary. For example, faith was identified as an important concept early on during data collection. Therefore, we enrolled a participant who met the inclusion criteria and had been a pastor in several rural communities across the state. This enabled us to gain the perspective of someone who could share personal and professional experiences regarding the role of faith in pursuing well-being while living with a disability in the rural context. After the core category was identified and during the selective coding stage of data analysis, we recruited one urban-dwelling participant with a physical disability. This informed conceptual boundaries and discouraged stereotypes from emerging within the theory.
Ethical Considerations
At the beginning of each interview, the researcher reviewed the comprehensive information sheet regarding the possible risks and benefits of the study as well as expectations of participants. After any questions were answered, informed consent was obtained. As part of the informed consent process, participants were told that if they shared with the researcher that they were being abused or neglected, they would be referred for assistance. In addition, participants were told that if they scored above 13 on the Kessler-6 Psychological Distress Scale (K6; Kessler et al., 2003), they would be assessed for suicidal ideation and referred to a mental health provider.
All efforts have been made to keep the identities of the research participants anonymous. Therefore, because of the small communities from which these participants were recruited, some identifying diagnoses were changed to ensure that any readers would not be able to identify a participant based upon a distinct diagnosis or condition.
Data Collection
Data collection and analysis took place between June 2017 and February 2018. Data were collected from 12 rural-dwelling and one urban-dwelling, community-residing individuals with various disabilities. Data included 20 interviews (participants were interviewed 1 to 3 times), each lasting 1.5 to 3 hours, field notes, survey data, and memos of theoretical reflections and insights. Second and third interviews were scheduled with participants on an ongoing basis throughout data collection as needed for theoretical development. Interviews were audio recorded and professionally transcribed.
The interviewer asked open-ended questions relating to perceptions of how the person’s impairment affected his or her life over time, activities that he or she enjoys doing, qualities of their rural communities, and people with whom they interact on a regular basis. Participants were also asked to explain daily routines as well as if and how their disability affected relationships and routines. As data analysis began to suggest categories, interview questions were refined based on the identified categories in the evolving theory. Thus, later interviews were theoretical with a focused approach to elicit dimensionality and nuance of the theoretical concepts. For example, early interviews identified the importance of social networks; theoretical interviews probed participants’ experiences of friends, family, and colleagues within the context of living in a rural environment with a disability.
Field notes were written after each participant interview and during visits to rural counties to document the activities in which participants engaged and the contexts in which those activities took place. Field notes included observations about the community and helped to identify, explore, and explain the social structures and contexts of participants. Demographic data collected included age, race/ethnicity, length of residence in county, educational level, income level, housing type, family structure, employment status, occupation, and age at onset of impairment.
Information on well-being was collected via two standardized well-being instruments. The K6 (Kessler et al., 2003) is a six-item screening scale to identify nonspecific psychological distress in the general population (Kessler et al., 2002). The questions ask respondents how frequently they experienced symptoms of psychological distress during the past 30 days. Responses range from “none of the time” coded 0 to “all of the time” coded 4. The six items on the scale are then summed to yield a number 0 to 24 with a score ≥ 13 indicating nonspecific psychological distress and possible serious mental illness (Kessler et al., 2003). The scale has demonstrated internal consistency and reliability (Cronbach’s α = .89, Kessler et al., 2002). The ICEpop CAPability measure for Adults (ICECAP-A) is a measure of capability well-being and focuses on five attributes: attachment, stability, achievement, enjoyment, and autonomy (Al-Janabi, Flynn, & Coast, 2012). Each attribute can take one of four levels ranging from full capability to no capability (Flynn et al., 2015). Initial investigations of this scale support construct validity (Al-Janabi et al., 2013), discriminant validity (Mitchell et al., 2017), and convergent validity (Goranitis et al., 2016).
Data Analysis
Analysis of interview transcripts and field notes focused on the meanings, intentions, and actions of study participants. Each interview transcript was read multiple times to gain a sense of the whole before initiating coding. During this process, our analytic team came together on six occasions to examine the emerging theory about well-being in rural-dwelling adults with disabilities for logic, conceptual clarity, defining borders, and explicating relationships between concepts. Case-based dialogues were used among the group to convey the process of pursuing well-being as a rural community member with a disability. Specifically, the first author (who collected the research data) presented cases to the team that she believed represented emerging categories. Through dialogue, the team refined and combined categories.
Data collected in the field notes were incorporated into the final analysis of the theory. This was done by engaging in theoretical memoing throughout data collection and analysis. The theoretical memos enabled the transformation of the descriptions of social context found in the field notes into theoretical accounts explaining the conditions and preconditions that predicted behaviors. As an example, the field notes of one interview contained data about the participant’s perceptions of the lack of formal services for people in his age group living with a disability in rural Texas. These data were extracted into a theoretical memo regarding the importance of informal networks and how, in lieu of formal services, these informal networks were leveraged to have needs met.
Qualitative Rigor
The quantitative data collected via demographic surveys and standardized well-being instruments were qualitized to extract additional information and to confirm interpretations (Sandelowski, 2000). This helped to compare interview data and researcher observations recorded against objective standards for measuring well-being. For example, one participant in particular struggled with her declining physical and social capacity; this was evident in her interview as she was unable to effectively participate in the social processes needed to pursue well-being. Comparing her interview data and field notes with the well-being instruments indicated that her inability to engage in the social processes identified in this study influenced her well-being; she indicated moderate psychological distress and ranked herself fairly low on the well-being attributes included on the ICECAP-A. Thus, this comparison enabled the research team to further check the boundaries of the emerging theory by analyzing participant stories against their well-being scores. This process also served as a method of triangulation thereby enhancing the transferability of the study.
Transferability was also addressed by providing detailed descriptions of the participants, data, and context and by reporting of data using participants’ direct quotes. To enhance credibility of the data analysis and interpretations, the first author reviewed emergent interpretations with the second author of this article who is an expert in qualitative methodologies and disability. Reflexivity was maintained through on-going documentation in a research log, juxtaposing these reflections against the data, and discussing the reflections with an expert advisor. As an example, we studied interview transcripts to interrogate implicit assumptions made by the wording of questions or probing for context. Insights gained from these types of exercises were recorded in the research log and studied as a way of staying true to the intent of the research.
Sample
Twelve rural-dwelling adults between 35 and 70 years participated in this study. The mean age of the rural participants was 60.5 years (SD = 8.16). In general, the study participants were predominantly married, older, White women who used accommodations for mobility or hearing. Of the rural participants, eight (67%) were women; 10 (83%) identified as non-Hispanic White, one (7%) identified as African American, and one (7%) identified as 25% Native American and 75% non-Hispanic White. The age at which participants acquired their impairment(s) ranged from 4 to 59 years of age. All participants reported a functional limitation because of mobility or sensory impairments, or both; three also reported a mental health diagnosis. Mobility and sensory impairments were due to osteoarthritis, paraplegia, multiple sclerosis, neurodegenerative illness, acute hearing loss, genetic hearing loss, diabetes, and heart disease. Ten of the 12 rural participants (83%) used some type of assistive device or accommodation. Two (15%) used wheelchairs, and one of these also had a service dog; three (23%) used walkers or canes depending upon where they were; two (15%) had personal attendants; two (15%) used hearing aids; and one (7%) used a power lift chair at home and occasionally used an electric scooter when running errands.
Eight (67%) of the rural participants were currently married, one (8%) had never been married, one (8%) was divorced, and two (15%) were widowed. Nine (69%) had children, and four (30%) had grandchildren. All of the participants had graduated from high school, eight (61%) had earned either an Associate’s Degree or a Bachelor’s Degree, and three (25%) of the rural participants had completed a graduate degree. Despite the high level of education of this sample, only one (8%) of the rural-dwelling participants worked full-time. Three of the participants worked only part-time because of their disability, and two were self-employed and worked to the extent that opportunities were available and their individual capacity allowed. Two of the participants had taken early retirement. Three (23%) were unemployed, but only one of those participants was actively seeking employment. At the time of the study, four (30%) rural participants reported having financial difficulty and relied upon public assistance such as supplemental nutrition assistance program benefits or a community food pantry; two others reported having used public assistance in the past.
Two participants scored over the cutpoint of 13 on the K6 scale indicating psychological distress. Both were asked if they were contemplating suicide or were having suicidal thoughts, and both denied any current suicidal ideation, but one did report having had suicidal thoughts in the past. Because serious psychological distress includes mental health problems severe enough to cause serious impairment and to require treatment, both participants were referred to local mental health providers. One of these participants reported a diagnosis of bipolar disorder and was under the care of a psychiatrist; she was provided with additional information on local social service agencies for income and job assistance.
Setting
Participants lived in six different counties in Texas. The mean population of the rural counties was 6,828 (see Table 1). None of the participants had spent their entire lives in their current community, but 10 (76%) participants had lived in their current locations for more than 15 years. Four (30%) of the participants had been born and raised in urban areas. Interviews took place in participants’ homes or offices, local cafés, and public libraries within the respective rural communities. To observe participants in community places and in private spaces, participants were asked for follow-up interviews in their homes if the first interview was held in a public space.
Rural County Data.
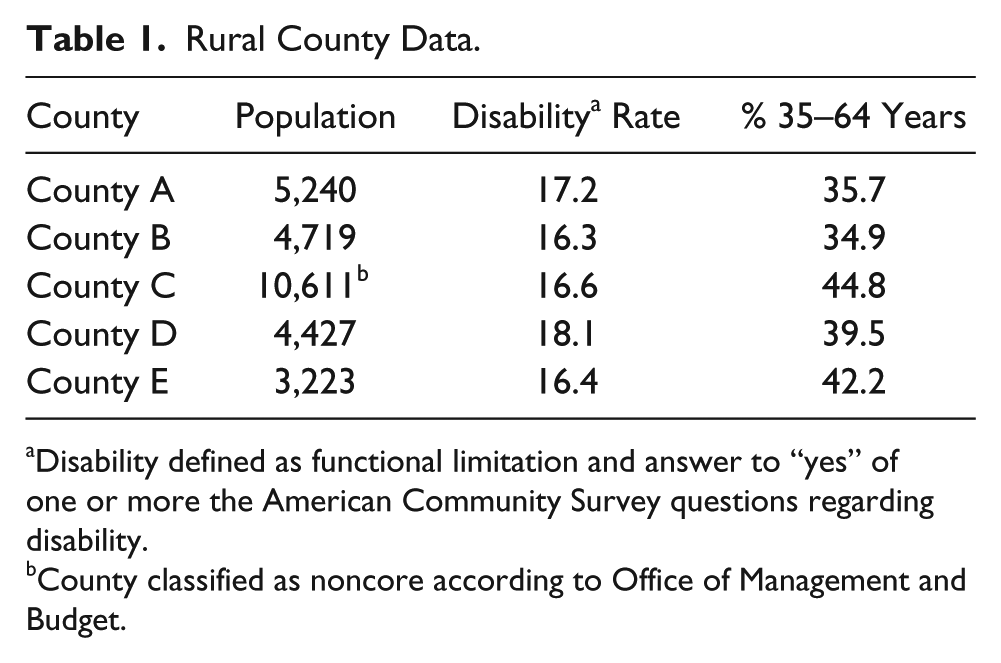
Disability defined as functional limitation and answer to “yes” of one or more the American Community Survey questions regarding disability.
County classified as noncore according to Office of Management and Budget.
Findings
Well-being is facilitated by living in a community with others in accordance with shared history and personal values and to the fullest extent of one’s abilities. This process is depicted in Figure 1. The six conceptual categories that drive the definition and pursuit of well-being include values, rural attitude, demands, set expectations, strategic participation, and membership.

Model of well-being.
Values
Congruence between participants’ individual values and the cultural values of the rural environment contributed to the development and maintenance of a rural attitude, which is discussed in the following section. Participants described rural communities as places where people hold one another accountable and lift one another up and where one can still get things done with a “handshake agreement.” That is, mutual trust between community members allowed opportunities for resolving difficulties without the need for outside intervention. In turn, this facilitated a sense of freedom to collaborate on creative solutions to overcome some of the difficulties associated with living in a rural area. For example, one participant described working with a nearby jurisdiction to secure transportation for disabled veterans from his rural county to the nearest Veterans’ Affairs health care facility. He said, . . .see, this is how easy these problems are to fix if you—I mean, we just got on the phone. It took about two months because it involved federal money, and there had to be a little paperwork, now . . . but in the end, it was a handshake agreement, and it works great.
Another shared value was strong Christian faith. Faith played two key roles in participants’ lives: a source of comfort and guidance and a source of community and belonging. Many described turning to God for solace and believing that strength to overcome adversity came from God. This is not to say that participants had a fatalistic perspective on life but rather recognized a personal responsibility for cultivating well-being. One participant described this perspective when he declared that refusal to seek help, engage in therapy, or take prescribed medications is “denying God the ability to help work through this.” The church was also valued for its role as a cultural institution that provided resources, services, and support for community members. One participant who did not identify as religious nevertheless valued the church and recognized its importance, saying, if you are an active member in church, and we have 20 here I believe, you have a church family that will come check on you and keep track of you, but if you’re not, then you need to have good neighbors or some kinfolk somewhere because there’s nobody to go around and see these folks.
A Rural Attitude
For this study, rural was operationalized using a geographic definition—counties in Texas categorized as noncore (typically less than 10,000 residents)—but for these participants, having a rural attitude encompassed a relational understanding of rural whereby rural was constituted of experiences and interpretations. A relational approach to rurality has been described as an emphasis on the significance of networks and connections and holds that all entities are “equal components within a network, each with a capacity to change outcomes through their participation or non-participation” (Woods, 2011, p. 41). Similarly, in this study, a rural attitude was characterized as participating in shared practices, supporting one another, possessing a deep knowledge of and appreciation for the materiality of the place and was developed in contrast with and relative to urban space and society.
That participants interpreted their rural lives in contrast to time spent in urban environments is not surprising as rural has always been defined and imagined as relative to urban space and society (Woods, 2011). In contrast to the familiarity of the rural area, participants perceived that in a city, people are invisible and nobody sincerely cares. Participants appreciated being known to others, and this was facilitated in their small communities via everyday exchanges (e.g., being greeted by name at the doctor’s office), organized events (e.g., community festivals), or employment activities (e.g., interviewing community members). In addition, the rural participants described a sense of unease when reflecting on the urban area and uniformly regarded urban environments as loud, stressful, and expensive and valued the calm, quiet surroundings of the rural areas. One participant described living in the country saying, the land comes to own you, you don’t own the land, you know. This is—it’s the wealth that is indescribable. Uh, you go to the city and it’s cacophony, it’s—it’s people everywhere, it makes me nervous. I can’t stand it.
Participants reconciled with the difficulties associated with living in a rural area by focusing on the positive aspects of their communities. For example, participants valued the accessible and familiar health care services available to them in the rural area. Specifically, informal social relationships between participants and their health care providers were important. One participant, who traveled an hour and a half for specialty visits, described the convenience of attending the same church as her primary care physician: My doctor was there. I could stop, and it’s like, “excuse me, I’ve got this cat bite,” and he wrote out a script, called it in to the thing. I mean, listen, that doesn’t happen in a big town.
Demands
Demands represent the product of participants’ ongoing judgments about the influence of disability on their ability to participate in their communities. This definition is in keeping with the “demands of illness” construct in which demands of illness are illness-related events experienced by individuals or families in response to health problems; they are different from illness stressors, hardships, or problems (Woods, Haberman, Packard, Jensen, & Strickland, 1993). Examples of demands shared by these participants include educating others about their impairments, strategizing to normalize life, and managing expectations.
Most participants perceived there was a social demand to educate others about their impairments. Often, this took the form of proactively warning others of what they saw as personal shortcomings to manage others’ expectations of their abilities. One participant told a prospective employer “I’m unreliable” to prepare the employer for a potentially unpredictable work schedule. Participants also asserted their abilities to others to continuously challenge social perceptions of people with disabilities. A different participant told family and friends, “I’m not dead yet.”
Participants strategized to normalize life as a way to facilitate social participation in the community. For example, in his community where many men work in the oilfields, one of the participants re-organized his day to begin at the local coffee shop at 4:30 a.m. so that he could engage with the oilfield workers. Over time, he expected to meet certain people, and he became a familiar face to the other men in his community. This expectation of encountering and interacting with others reinforced the importance of participation and served to establish membership in his community.
For those who experienced greater severity impairment, managing demands was more difficult. One participant experienced demands that ultimately resulted in a reappraisal of self. She regretted the tears she shed as she discussed the difficulties involved with her day-to-day life saying, “I don’t want to be so emotional. I’m a tough cookie.” For her, living in a rural area created additional demands. No one else with her diagnosis lived in her community, so she perceived a demand to educate others about her diagnosis. However, the uncertainty of her everyday life, the progression of her illness, and her shrinking social network had prevented this education from taking place. Furthermore, there were no opportunities to engage with others who had experienced or were currently experiencing similar degenerative conditions. This limited her ability to anticipate her future in the long term and to make plans on a daily basis. She said, “this disease has taken me away from my city, my business—It hasn’t taken me away from my family yet, but it’s trying.”
Set Expectations
Participants in this study set expectations regarding their everyday lives in their communities, and these expectations contributed to a rural attitude and to strategic participation. The rural community allowed participants to master daily routines that facilitated participation. For most participants, however, routines fluctuated due to the unpredictable nature of their impairments. Thus, routines were dependent on whether the day was a “good” day or a “bad” day. On good days, participants were able to engage in everyday activities such as getting dressed, going to work, feeding the livestock, or going to church without much trouble. On bad days, however, routines were greatly altered. For example, instead of going to his part-time job or tending to his donkeys and goats, one participant described the experience of a bad day saying, Um, on bad days, you know, when you can’t do what you need to do, it makes one feel useless or inadequate, but I’m not a depressing kind of person, so I don’t—I just wait until the next day, hoping that it will be better.
As they adapted to changes in physical capacity, participants altered routines to accommodate declining abilities. However, the rural environment served as a buffer against potential negative psychological effects of declining physical or social capacities. That is, there was not as much coming and going of outsiders, and people were familiar to one another. As they engaged in daily routines over time, participants expected to interact with certain known others, and mutual trust and respect had developed. Therefore, as participants were less able to do the things they did before, mundane encounters were meaningful. Being greeted by name when walking down the street or entering the bank provided a sense that participants were recognized as trustworthy community members. This sense of being known to others provided incentive for participants to continue to engage in their routines to maintain membership in the community even when it was difficult to do so.
Strategic Participation
Strategic participation is the participants’ selective and planned involvement with and within the context of their rural communities. Participants emphasized their ability to freely choose whether to participate or not. However, they did not impulsively decide to participate; they strategically chose what courses of action to pursue and then developed detailed plans for successful participation. For example, one participant valued her membership in a local social group and served in several leadership roles. However, the clubhouse where the group met did not, until a recent renovation, have an accessible restroom for her. To participate in the group, this participant ensured that she had a female urinal in her van to use if needed.
Participants also carefully appraised available opportunities. Frequently, participants had to balance activities that honored family and community with opportunities for career advancement or more income. When discussing his current job, one participant said, “this was a step down, career wise.” But, he prioritized his health and the needs of his family over his personal desire for career advancement. A common refrain was “I’m not doing this for the money” when asked about current employment, and three participants refused the US$25.00 participant incentive for this study. Instead, participants wanted opportunities to be useful, to contribute to their communities, and to choose how and when to act.
Membership—The Core Category
The main concern for this sample of working-age adults with disabilities was membership in their rural community. Membership is defined as a feeling of belonging and being part of something greater than one’s self and is sustained by ongoing contributions to the collective. This sense of establishing and maintaining membership and subsequently belonging to a group dominated how participants described their personal histories and lived experiences and accounted for the majority of the variation in the data.
Membership conveyed that participants belonged and were regarded as contributing participants in their communities. Membership also provided access to support from other community members when needed. When one participant was asked to describe what it was like to live in her community of about 350 people, she said, you know everybody . . . here you break down on the side of the road probably five people will stop before you figure out what’s wrong.
She went on to say, some days when you hurt so much you can’t move, you can’t sit, you can’t lay down, you know, and ah but you know, like I had problems I could call one of my cousins or [a friend] or nearly anybody else in the community and they would get somebody out. So, there’s—there’s ah even if you aren’t actually related everybody in the area tries to help.
Membership provided a sense that social and instrumental support was not charity or a handout but rather was an opportunity to share with others and to build a stronger community. Group membership also allowed for reciprocation of the goodwill offered by others. Reciprocation was integral both to the maintenance of membership and for providing a sense of competence and purpose. One participant described this process of reciprocation succinctly. When asked why he spent so much time and effort engaged in work and volunteer activities when there were days that he could not walk due to his pain and mobility limitations, he said, To give me the opportunity to give back. To help—because if you—the best way not to feel sorry for yourself is to help somebody else. That’s the best cure. And it gives me that opportunity, um, it makes me feel necessary, fulfilled, uh, and there’s some perks that come along with it. People appreciate what I do, and when they see me on the street, they tell me, and that makes me feel good.
In contrast, a different participant had been unable to maintain her previous role as a contributing member to her rural community. She was 50 years old at the time of our interview and had been living with a progressive neurodegenerative disease for 7 years. She struggled with the unpredictable nature of her illness, the limitations her illness has imposed, and her perceptions that others view her as a sad and tragic story without much to contribute to the community. She tearfully recounted how she “came home to do nothing” after her diagnosis. Thus, despite the fact that she had been a well-known business owner and community volunteer for many years, as her physical and social capacity declined, her social status changed thereby making membership more tenuous.
Discussion
Findings of this study support a long-held assumption that relying upon models developed in urban or suburban areas is insufficient for adequately addressing the health care needs of rural dwellers (Gangeness, 2010; Long & Weinert, 1989). Findings also support previous rural-focused research indicating that a sense of belonging can facilitate well-being (Caxaj & Gill, 2017) and are unique because they detail the social processes by which rural-dwelling adults with disabilities mobilize resources to overcome functional limitations to establish group membership and create a sense of well-being.
At a time in our country when we are struggling to discover efficient and cost-effective approaches for providing long-term services and supports (LTSS) that maximize health and maintain respect for human dignity, this study provides a framework for the provision of services in rural areas. LTSS represent a substantial component of national health care spending: US$219.9 billion in 2012 (O’Shaughnessy, 2014). Forty-three percent of people receiving LTSS are between the ages of 18 and 64 (O’Shaughnessy, 2014) and the population of adults in need of LTSS is proportionately larger in rural versus urban areas (Rural Policy Research Institute, 2017). Thus, ensuring culturally appropriate and person-centered interventions and policy solutions for adults living with disabilities in rural areas should be a priority.
Using a capabilities perspective (Sen, 1992) facilitated an understanding of the processes by which individuals in this population are empowered to make decisions about important aspects of their life, how they convert their resources into activities and outcomes they consider important, and how they assign meaning to and place value on particular outcomes. In this study, participants indicated that they have an established social process that facilitates well-being; this process includes the reciprocal exchange of services in the context of living in a rural environment with a disability. It is suggested, therefore, that health care and LTSS providers should seek to capitalize on the established social ecosystems within the rural community. For example, an important early step for service providers and policy makers working in rural areas would be to engage people with disabilities in community assessments, program development, and policy evaluation. Stakeholders could seek to establish relationships with rural community members living with a disability as well as traditional community gatekeepers such as church pastors. Prior evidence supports the importance of rural churches in facilitating social connectedness and providing healthful opportunities for community engagement (Plunkett, Leipert, Olson, & Ray, 2014). Tapping into these informal networks would yield insight as to how people with disabilities engage in the reciprocal exchange of services. Subsequently, formal community-based organizations could seek to reinforce and augment these established processes.
This research also supports the utility of a social constructionist perspective to policy development (Harrison et al., 2013). The extensive evidence regarding shortcomings of rural areas and the associated negative health implications (e.g., Davidsson & Södergård, 2016; Meit et al., 2014) underscores the urgency to attend to rural well-being. The knowledge constructed between the researcher and the participants in this study painted a nuanced picture of the history, culture, and social relations that were identified as significant influences on well-being. Capitalizing on the assets of rural areas could, therefore, yield interventions and policies that are more culturally appropriate. For example, convening regular walking groups at a local park or town square inclusive of people with disabilities—even those who may use a wheelchair or electric scooter for mobility—could serve as a source of social interaction, exercise, and connection with the outdoors. Previous research has demonstrated the utility of regular walking groups in the rural context. Grant, Pollard, Allmark, Machaczek, and Ramcharan (2017) explored social relations in the context of a walking program in a rural community in the United Kingdom and found that community walks offered personal and social opportunities. Strengthened friendships and support, mutual monitoring of health and well-being, and practical support all emerged from the communal walking group (Grant et al., 2017).
Previous literature regarding social support among adults with disabilities in the rural context is mixed. Social support refers both to the emotionally sustaining and instrumentally beneficial qualities of social relationships (Umberson & Montez, 2010) and is consistently identified as a critical factor for maintaining health and quality of life for people with disabilities. Some evidence indicates that satisfaction with support is greater in rural adults with disabilities (McPhedran, 2011) while other research supports the notion that social support is more limited among rural dwellers with disabilities (Danzl et al., 2013; Goodridge et al., 2015). Findings from the current study indicate that social support is a component and an outcome of membership, and it is the acquisition and maintenance of membership status within the specific rural community that is important for well-being. Membership, however, extends beyond the receipt of social support. This is consistent with work that holds that meaningful connection to others forms a central focus through which psychological, symbolic, social, and material goods are distributed and needs are met (White, 2017). Thus, findings from this study indicate that it may not be the quantity of social support that is important, but rather the interpretation of being a member of a group and belonging to a network of reciprocity that is fundamental. The rural participants understood that they required support and assistance from others to overcome barriers and engage in meaningful activities; well-being emerged from confidence in knowing that there would be someone or some cause to which they could lend support in the future.
In this study, participants valued the ability to choose from among an array of options and to feel empowered to choose to not participate in particular activities. While health benefits may be associated with a particular course of action, the ability and act of choosing to participate (or not) is itself important for well-being. This finding is consistent with prior research that found that decisional autonomy and self-determination is frequently more important than the ability to independently perform activities by oneself (Harrison et al., 2010). It is also in keeping with the capabilities approach as formulated by Sen (1992) who contended that the ability to choose between meaningful options is itself a valuable part of living, and a life with meaningful choice can be considered to be of higher quality.
Limitations
This study was limited because of the small sample size and the lack of diversity within the sample. While there was one African American participant and one participant who identified as part Native American, the sample was primarily White. Experiences for people with disabilities in rural areas where residents are predominantly African American or Latino may be very different. In addition, people with disabilities who are marginalized (such as lesbian, gay, bisexual, transgender, and queer [LGBTQ], members of non-Christian religions, and foreign-born or non-English speakers) may have significantly different experiences of well-being. This study did not include participants who were living in institutional settings, but their experiences would also yield important insights as to the distinctive influences that the rural context may have on well-being. We suggest that further research is needed with individuals from various living contexts, class backgrounds, and racial, ethnic, and sexual identity groups to fully reflect the diversity of experience of disability in rural America. Another limitation is the inclusion of only one negative case. While exploring well-being in rural environments among people with disabilities, we had to make decisions based upon the resources available to us. The concepts were conceptually abstract, so we focused on theoretical sampling and repeat interviews to gain nuance without making the data unwieldy. A larger pool of negative cases in future studies could provide more complexity and explanation to the theoretical concepts presented here. Data were collected over a short period of time (7 months) and therefore do not represent well-being across the disablement trajectory of these participants. However, participants were diverse in terms of functional abilities and life histories which provided nuance and dimensionality to the theoretical concepts. Future studies could incorporate a life course approach to provide a framework for examining how the rural environment interacts with earlier life experiences to shape well-being.
Conclusion
This study builds on the previous literature and extends this knowledge into theoretical advances in two distinct areas: rurality and disability. As suggested by Morse (2018), qualitative research cannot be done out of context of the research that preceded if advances to practice are to occur. The uniqueness of this work is that it advances our understanding of well-being in the lives, context, and space of rural adults with disabilities. Well-being can be thought of as a collective experience; through ongoing membership, emotional and material needs are satisfied, meaningful social relationships develop, and self-confidence and self-valuing occur. Ultimately, a nuanced understanding of well-being such as identified in this study can facilitate thinking among practitioners and policy makers about how life can be made better for individuals in the communities in which they live.
Footnotes
Acknowledgements
We are grateful to Alexa Stuifbergen, Dean, University of Texas at Austin School of Nursing; Debra Umberson, Professor of Sociology and Director of the Population Research Center at the University of Texas at Austin; and William Sage, Professor of Law and Medicine at the University of Texas at Austin for their comments on an earlier version of this manuscript. We also thank five anonymous reviewers for their helpful insights. Finally, we say thank you to each of the individuals who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided in part by the Robert Wood Johnson Foundation. The views expressed here do not necessarily reflect the views of the Foundation. Support for this work was also provided by the Southern Nursing Research Society, the Center for Excellence in Aging Services and Long-Term Care, and the Cain Center for Nursing Research at the University of Texas at Austin School of Nursing.