
Abstract
Lesbian, gay, bisexual, transgender, and queer (LGBTQ) communities of color experience intersecting systems of oppression that limit access to health care, safety, and other basic resources. Important research has documented these disparities, their antecedents, and consequences. However, little research has examined the strengths of multiply marginalized LGBTQ communities. Drawing from a health equity framework, this study is based on interviews with 38 LGBTQ-identified people of color in New York City. We used framework analysis to examine participants’ perspectives on the role of community in enhancing health and well-being. Community strengths identified by participants included (a) safety, acceptance, and support; (b) interconnectedness and resource sharing; and (c) advocacy, collective action, and community potential. Recommendations for policy, practice, and future research are suggested, including efforts toward community power building.
Keywords
There is a dearth of research focused on the strengths of lesbian, gay, bisexual, transgender, and queer (LGBTQ) communities of color. In States of Injury: Power and Freedom in Late Modernity, feminist theorist Wendy Brown (1995) posited that by focusing solely on the pain and trauma of oppression—what she termed the “wounded” subject position—marginalized people’s ground for gaining power becomes directly tied to overcoming the injuries of oppression. Undoubtedly, research on LGBTQ populations has brought attention to poor outcomes related to marginalized social statuses. In contemporary social science research particularly, we see artifacts of this hyperfocus on the wounds of LGBTQ oppression, including the historical pathologization of homosexuality and gender nonconformity, which has long dominated scholarly discourse on gender and sexual minorities, often casting LGBTQ people as deviant, sinful, and sick. As developmental psychologist Savin-Williams (2008) noted, there is an [. . .] irresistible and overpowering attention to the problematic nature of same-sex oriented populations rather than a focus on their capacities to adjust, thrive, and lead exceptionally ordinary lives. It is as if same-sex oriented populations are only interesting to the extent that they differ in the negative. (p. 137)
In recent LGBTQ health and mental health literature specifically, much attention has been given to documenting disparate rates of health care access, utilization, health and mental health outcomes, and disease burden. Indeed, research on health disparities and how they interconnect with social determinants, such as access to economic resources, health care, exposure to violence and discrimination, is critical. Rigorously collected and examined data on the sociostructural systems of disadvantage and marginalization that limit the capabilities and opportunities within these communities is essential for advocating for awareness, resources, practices, and policy regarding these disparities. Simultaneously, much is lost when the mechanisms of mutual care and survival forged by community members in light of systems of oppression are not examined. And so, there remains an open call to “understand what constitutes a ‘health-enabling community context’” and to engage in inquiry that highlights the strengths nurtured by communities situated within “very real power imbalances that generate health inequalities.” (Campbell & Murray, 2004, pp. 189, 191). This article responds to this call by employing a health equity approach to understanding health-enabling qualities of marginalized communities, particularly LGBTQ communities of color. Exploring how individuals perceive the role of community in enhancing health is critical toward reaching a more nuanced, grassroots understanding of the formal and informal mechanisms through which communities become and stay well.
Literature Review
Health Equity Promotion Model
The current study was guided by the health equity promotion model, a multidimensional, context-sensitive approach to examining factors that facilitate and inhibit equity in health for LGBTQ people (Fredriksen-Goldsen et al., 2014). This health equity perspective recognizes minority stress theory and psychological mediation theory as leading explanations of LGBTQ health disparities. Fredriksen-Goldsen and colleagues (2014) argued, however, that these theories largely fail to explain why some LGBTQ people remain healthy in the face of adversity. Despite documented health disparities, research shows that many LGBTQ people are connected to communities, engage in health-promoting behaviors, and enjoy good health (Fredriksen-Goldsen, Kim, Shiu, Goldsen, & Emlet, 2015) Examining LGBTQ health from a health equity perspective allows researchers to attend to well established health-adverse pathways (e.g., smoking; forgone care; sexual risk behaviors), while exploring behaviors (e.g., engaging in physical or leisure activities), psychological resources (e.g., positive identity appraisal/identity affirmation), and social resources (e.g., social connectedness, participation in social activities) that lead to positive health outcomes among community members. Because we know little about these health-promoting mechanisms, it is essential that research continues to identify the individual- and community-level strengths that might allow LGBTQ people to maintain or attain wellness as they face adversity and marginalization (Fredriksen-Goldsen, Kim, Bryan, Shiu, & Emlet, 2017).
In addition to the integration of processes that help explain positive health outcomes, the health equity promotion model posits that the availability of health-promoting opportunities depends on an individual’s intersecting social identities and positionality, his or her structural and environmental contexts, and changes in these experiences across the life course (Fredriksen-Goldsen et al., 2017; Fredriksen-Goldsen et al., 2014). For example, a recent study of lesbian, gay, bisexual, and transgender (LGBT) older adults found that African American and Hispanic participants had lower levels of identity affirmation (e.g., feeling proud of their LGBT identity) and social support (i.e., perceived instrumental, informational, affectionate, and social interaction support), yet higher levels of spirituality (i.e., spiritual beliefs, meaning, and support) compared with the non-Hispanic White participants (Kim, Jen, & Fredriksen-Goldsen, 2017). Lower levels of health-enabling factors were associated with worse physical and psychological health, whereas increased access to spiritual resources was correlated with improved psychological health outcomes. The finding that LGBTQ people of color may have less access to social support as a mechanism to wellness, aligns with additional research that indicated that African American/Black men who have sex with men (MSM) had fewer people to rely on for social support and were less likely to report coping through the receipt of help or emotional support from others than White MSM (Buttram & Kurtz, 2015; Buttram, Kurtz, & Surratt, 2013). As social support remains a primary correlate of wellness, however, it is important to continue to explore how LGBTQ people of color describe their primary sources of support and the ways in which they harness the supports that are available to them to achieve optimal health. For example, it may be meaningful to focus specifically on support from others within the LGBTQ community.
Health-adverse factors that inhibit health equity for LGBTQ people
Barriers to health equity for LGBTQ people exist at both the social-structural and individual levels. Social-structural-level health-adverse factors include stigma, oppression, and social exclusion (Fredriksen-Goldsen et al., 2014). These social determinants expose LGBTQ people to stressors that heighten the risk for experiencing mental and physical health issues, such as depression, anxiety, substance use, cancer, and HIV, relative to their heterosexual and cisgender (i.e., nontransgender) counterparts (Krehely, 2009; Romanelli & Hudson, 2017). LGBTQ people of color in the United States experience exponential effects of belonging to multiple stigmatized groups, for example, being a sexual/gender minority and a racial/ethnic minority (Wilson & Yoshikawa, 2007), as well as elevated likelihoods of identifying with other stigmatized experiences like homelessness, mental health issues, and poverty (D. Meyer, 2015; U.S. Department of Health and Human Services, 2015). LGBTQ people of color, and particularly low-income sexual minority women and transgender women of color, experience elevated likelihoods of experiencing hate violence, including assault and homicide, and are more vulnerable to involvement with law enforcement (Mountz, 2011; National Coalition of Anti-Violence Programs, 2016). In fact, in one study, 47% percent of transgender people of color reported having been incarcerated at some point in their lives, many of whom were denied health care and subjected to sexualized violence, abuse, and other discriminatory treatment while incarcerated (Lydon, Carrington, Low, Miller, & Yazdy, 2015). LGBTQ people of color also experience higher levels of unemployment and underemployment, hiring and workplace discrimination, lower levels of educational attainment, and significant risk of poverty (Badgett, Lau, Sears, & Ho, 2007; Buttram & Kurtz, 2015).
These intersecting experiences may suggest elevated care needs given the social-structural stressors endured by LGBTQ people of color. However, disparities in health care access for LGBTQ people of color are profound. LGBTQ people of color experience higher rates of being uninsured, delaying or avoiding health care, and delaying or not getting needed prescription medication compared with White and heterosexual counterparts (Krehely, 2009). Social-structural factors, including intersectional stigma and poverty, as well as individual influences, such as depression, are likely prominent barriers to engaging in health care among LGBTQ communities of color (Quinn, Reed, Dickson-Gomez, & Kelly, 2018; Romanelli & Hudson, 2017). Other individual-level health-adverse factors include behaviors (e.g., drug use), psychocognitive processes (e.g., stress), and biological factors (e.g., allostatic loads), as well as likelihoods of victimization, abuse, and discrimination based on intersecting social identities (e.g., gender identity/expression, sexual orientation, race/ethnicity, and socioeconomic status).
Health-promoting factors that foster health equity for LGBTQ people
Assets and strengths that facilitate health equity for LGBTQ people also exist at the social-structural and individual levels. At the individual level, health-promoting strengths include behaviors, psychological and psycho-cognitive processes, character strengths, and navigational capital. Health-promoting behaviors may include diet, exercise, and engaging in preventive care (Fredriksen-Goldsen et al., 2014). Positive psychological and psycho-cognitive processes, such as problem solving and active coping, may mediate the effects of stressors, both general and minority specific, on health (Hatzenbuehler, 2009). Ngamake, Walch, and Raveepatarakul (2016) tested various coping strategies among sexual minority participants as the main mechanism of the relationship between perceived discrimination and psychological distress. Although results only indicated that participants who employed disengagement coping strategies (i.e., substance use) to deal with discriminatory experiences were more likely to report depression, anxiety, and stress symptoms, adaptive coping strategies were also examined, including education, advocacy, and resistance. In light of these findings, the authors suggested that it seems we know more about the coping strategies to discourage, rather than encourage among sexual minorities and more research is needed to understand the resilience and coping resources of LGBTQ people. Integration and disclosure of one’s stigmatized identity/identities may also, in some cases, be a health-promoting factor, as it may increase opportunities to interact with other LGBTQ people and increase positive social identity and sense of community (Fredriksen-Goldsen et al., 2014; I. H. Meyer, 2003). While disclosure may also elevate a person’s vulnerability and risk of hostility from others, disclosure has also been associated with health-promoting factors such as acceptance, the rejection of stereotypes, and the resistance of discrimination (Harper, Brodsky, & Bruce, 2012; Scourfield, Roen, & McDermott, 2008).
Health-promoting character strengths include altruism, generosity, empathy, hope, optimism, courage, bravery, and creativity (Buttram, 2015; Kwon, 2013). For transgender people specifically, pride in identities, spirituality, and hope for the future have been identified as character strengths and expressions of resilience (Singh, Hays, & Watson, 2011; Singh & McKleroy, 2011). Furthermore, navigational capital (Yosso, 2005) among LGBTQ people serves as a health-promoting resource. Navigational capital includes the ability to find safe and supportive LGBTQ spaces and people (Harper et al., 2012) and the ability to access health care and financial resources (Singh & McKleroy, 2011).
Although these individual health-promoting factors remain important to consider, a hyperfocus on the individual level minimizes the importance of social context (e.g., by obscuring the impact of poverty or race) and ignores the interconnectedness and interdependence of communities (Adams, McCreanor, & Braun, 2013). Furthermore, the emphasis on individualized characteristics and behaviors-related health has neither adequately accounted for the health of marginalized groups such as the LGBTQ community, nor had an enduring effect on reducing health disparities (Adams et al., 2013; Scott-Samuel, Stanistreet, & Crawshaw, 2009). As such, more research is needed to identify social-structural-level health-promoting influences on health, a primary aim of the current study.
At the social-structural level, this includes increased social capital, quality of community connectedness, and integration into communities (Fredriksen-Goldsen et al., 2014; Kertzner, Meyer, Frost, & Stirratt, 2009). Other social-level health-promoting factors include living places where there are relatively large numbers of other LGBTQ people (Hatzenbuehler, Keyes, & McLaughlin, 2011). For transgender people, connection to a supportive community and serving as a role model have been identified as health-promoting characteristics (Singh et al., 2011; Singh & McKleroy, 2011). Engaging in social action, advocacy, and activism have also been posited as health-promoting factors as these activities demonstrate resilience in the face of oppression and may increase hope and optimism for the future (Kwon, 2013; Singh et al., 2011; Singh & McKleroy, 2011). Alternatively, research completed among transgender individuals specifically has suggested that involvement activities intended to enhance the status of transgender people in society (i.e., collective action) may expose trans-advocates to more discrimination, which in turn can result in heightened psychological distress (Breslow et al., 2015). More research is needed to detail how it might be possible for LGBTQ individuals to stay involved in collective action to promote the well-being of the community and, at the same time, stay healthy themselves.
Current Study
In this exploratory study, we employed a health equity perspective by examining key health-promoting community strengths as identified by LGBTQ-identified adults of color. By situating participants as experts on their own community perceptions, we took an exploratory approach to understanding how individuals understand the role of community in enhancing health and well-being. We asked the questions, (a) What are the strengths of your community? and (b) What about your community keeps you healthy? Identifying key health-related protective factors from the perspective of community members gives insight into community strengths and what is working well in communities. This information is useful for informing future practice, policy, and research in attending to, bolstering, and staying close to the communities that they intend to impact, serve, and empower.
Method
Grounded in a social constructionist perspective, this study took a phenomenological approach to exploring perceptions of health and community. In-depth interviews were the primary method for data collection in this study, which centered on participants’ expert knowledge and authority regarding their lived experiences, and allowed for the exploration of participants’ perceptions of health concerns and health-promoting strengths in their communities.
Recruitment and Sample Description
Purposive and snowball sampling techniques were used to identify participants (Patton, 2002). Flyers with information about the study were posted at 12 LGBTQ-specific health and social service providers around New York City (NYC). Special effort was paid to identifying local agencies that served particular groups within the LGBTQ community, including elders, young adults, and people experiencing homelessness. These flyers included a brief description of the study, inclusion and exclusion criteria, details about compensation, and researcher contact information (name, email address, phone, and address). When a potential participant contacted the research team, a screening interview was conducted over the phone to determine eligibility. Inclusion criteria were (a) self-identification as LGBTQ (including respondents with sexual and gender identities other than lesbian, gay, bisexual, or transgender, such as “pansexual” or “questioning,” and who generally identified with the LGBTQ community) and (b) older than 18 years of age. Upon establishing that the potential participant qualified for the study, the interview was scheduled. At the completion of the interviews, participants were also provided with business cards and study information and were asked to share the cards with other potential participants. The final sample consisted of 40 LGBTQ-identified adults; however, as the current analysis is focused on the perceptions of LGBTQ people of color, two White-identified participants were excluded from the current analysis. Table 1 displays key characteristics of the sample (N = 38) grouped into broad demographic categories, including sexual identity, gender, race, age, self-reported socioeconomic status, and disability status. Participants provided this information during the interview process through open-ended questions on a written questionnaire. Some participants indicated membership in more than one group. For this reason, and due to rounding error, totals in some areas equal more than 100%. Members of the subsample were between 21 and 68 years of age (M = 46). A majority identified as African American or Black (66%), cisgender women (29%), and bisexual (47%). Over half of participants self-identified as poor (55%), and close to half (47%) of participants within the subsample identified as living with a disability.
Sample Description.
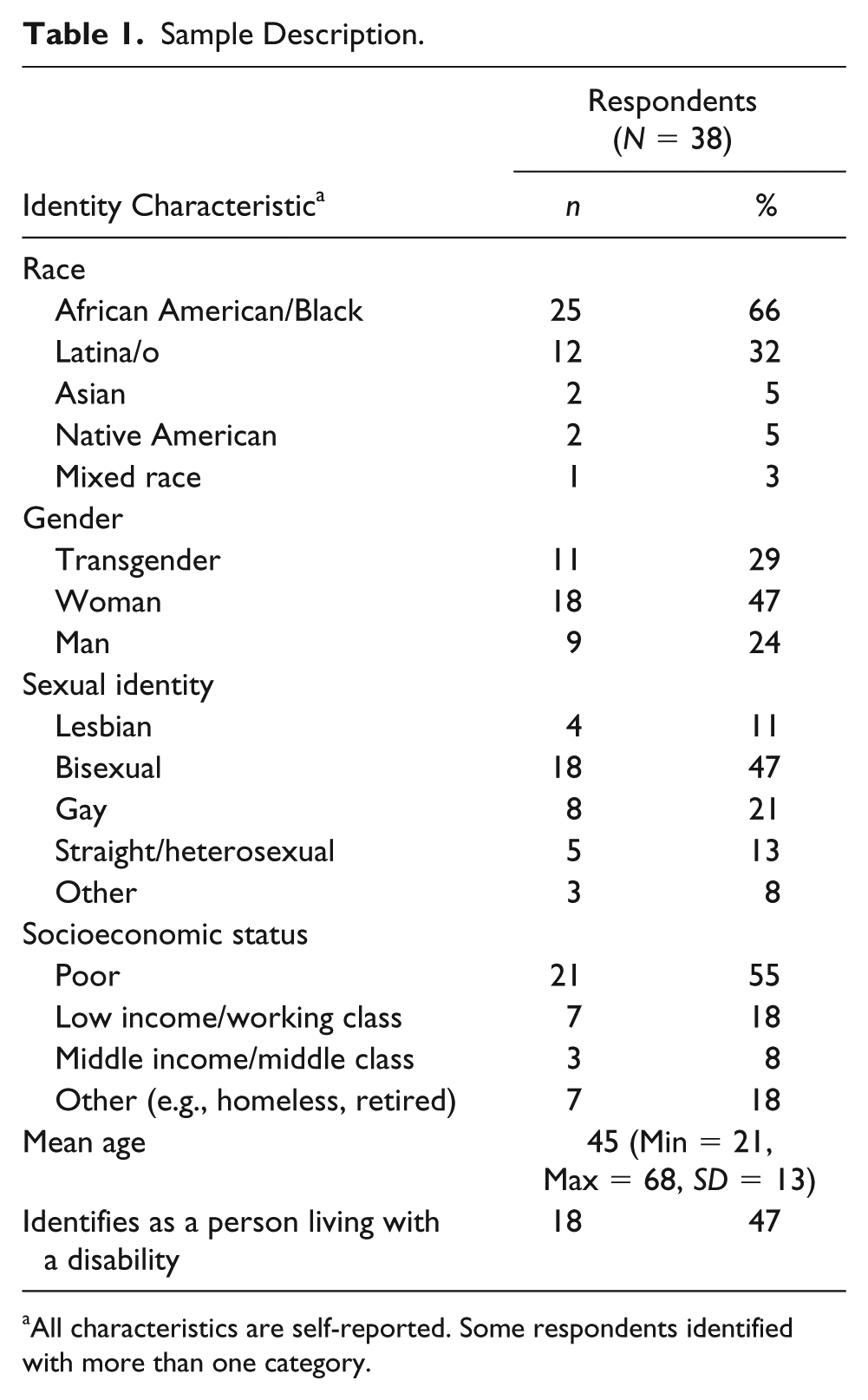
All characteristics are self-reported. Some respondents identified with more than one category.
Procedure
Two earlier studies informed the development of the interview guide: the Honor Project, conducted by the Indigenous Wellness Research Institute at the University of Washington (see Evans-Campbell, Walters, Pearson, & Campbell, 2012), and the Community Borderlands study, the dissertation work of Hudson (see Hudson, 2015). The interview guide was piloted with an LGBTQ-identified adult of color, who gave feedback on the framing and sequencing of questions. Interview domains of the final protocol included perceptions of health, structural barriers, ties to community and community health, and the role of community health centers. Romanelli, who has a background in clinical social work and who received interview training by Hudson, conducted the interviews. Data for the study were collected using semistructured, one-on-one in-depth interviews and a questionnaire on self-reported demographic information between August 2016 and October 2016. Before starting the interview, the participants gave their consent to participate in the study. The interviews lasted around 90 minutes and took place in a private office in the University. The interviewer used techniques such as episodic interviewing, which included focusing on a specific time and place (e.g., “Can you tell me about a time when your perceptions of health changed?”), and subjective, everyday knowledge (e.g., “What does health mean to you?”; Flick, 2000). This study was approved by the human subjects division at New York University. Because of the length of the interview, travel time, and high cost of living in NYC, participants received US$40 cash as compensation. Immediately following each interview, the interviewer completed a written debrief document that included information about participants’ nonverbal cues, standout moments, and emergent themes (Padgett, 2016).
Analysis
Data were examined using framework analysis techniques (Ritchie & Spencer, 1994; Ritchie, Spencer, & O’Connor, 2003), an approach increasingly used in health research. The steps included in this analytic method were (a) familiarization with the data, (b) identifying a thematic framework, (c) indexing and pilot charting, (d) charting/summarizing data in the framework, and (e) mapping and interpretation (Ritchie & Spencer, 1994; Ward, Furber, Tierney, & Swallow, 2013). Accordingly, Hudson became acquainted with the data by reading transcripts multiple times, reviewing postinterview memos, and extracting the interview sections specifically related to the research question. Romanelli, having collected the data, reviewed sections extracted by Hudson and checked for the completeness of the subset of data. Data were analyzed using open coding with the assistance of Atlas.ti (v7.5.15). This study’s research was driven by general patterns of responses in the interview that emphasized community strengths. Development of codes and themes was data driven, which ensured that the data were not forced to fit into a priori codes (Srivastava & Thomson, 2009). Codes were organized into categories, and relationships among categories were mapped. The patterns across data and the related key issues facilitated the identification of our initial framework. When engaging in framework analysis, initial frameworks are tentative and can be refined (Ritchie & Spencer, 1994) and should be informed by existing ideas. In general, framework analysis does not focus on generating entirely new theory (Ward et al., 2013). Thus, we reexamined the literature after constructing our initial framework to understand the emergent framework relative to Fredriksen-Goldsen et al.’s (2014) health equity promotion model. Finally, guided by both theory and the data, we engaged in charting data in the framework, mapping relationships, and interpreting results.
Quality and Credibility
Numerous strategies were employed to enhance the quality and credibility of this study. Particular diligence was paid to criteria identified by Patton (2002) for conducting rigorous qualitative research from a social constructionism perspective, including approaches to data collection, analysis, and interpretation. The authors engaged in researcher reflexivity with attention to ethical considerations during data collection. Specifically, the authors’ social locations and positionalities as LGBTQ researchers with identities offering varying levels of privilege and disadvantage were deliberated. The authors’ subjectivities related to the topic of study, study participants, and the interview process were discussed and documented during this reflexive process. Biases or potential biases held by the authors, such as those related to the importance of health care engagement, were identified while engaging in this process, which ultimately permitted a consistent interrogation and evaluation of data collection techniques. The repeated and systematic evaluations of the study’s data collection processes guided minimal, but necessary, revisions to the interview guide (Patton, 2002). In addition, to increase the sampling pool, participant recruitment and outreach to local LGBTQ organizations continued throughout the data collection period. Throughout the study, participants and the data collection processes were approached with earnestness in ethics, including openness, honesty, transparency, and respect (Davies & Dodd, 2002). Approaches including theory triangulation, a systematic search for alternative explanations, and analyst triangulation (Patton, 2002) were used to enhance the quality of the analysis and interpretation of findings. To achieve theory triangulation, the authors inductively reanalyzed data, looking for possible divergent themes, and deductively applied various theoretical perspectives. This approach ultimately confirmed that the health equity promotion model was well-fit for the study and also led to the exploration of alternative community experiences. As required for analyst triangulation, both authors analyzed the data and documented this process using an audit trail, memos tracking insights, and identifying questions and challenges throughout the analysis. The analytic process was completed by the authors both independently and collaboratively over a period of approximately 9 months, which allowed for peer checking and reflection throughout the analysis.
Results
Health-promoting community strengths identified by participants were organized around three themes: (a) safety, acceptance, and support; (b) interconnectedness and resource sharing; and (c) advocacy, collective action, and community potential. These three themes reflected the key strengths of LGBTQ communities that enhance health and create the possibility for wellness.
Safety, Acceptance, and Support: “I Can Go as Me and Not Be Judged” (N = 14)
Participants reflected on community acceptance and support as salient contributors to the overall wellness of LGBTQ community members at an individual level. Community acceptance and support not only promoted a sense of safety in physical spaces, but permitted community members to feel emotionally safe as well. When among other community members and in spaces intended specifically for LGBTQ people (e.g., LGBTQ community/health centers), participants described feeling strong, connected, understood, supported, loved, and “a part of something.” One participant suggested that community members “keep each other strong. Keep each other above water . . . if one is hurting, somebody come over and talk to you, give you a little, ‘You need a hug.’ Ask if you’re all right.” Another participant emphasized the importance of fostering these feelings among community members: Love is very powerful. Kindness is very powerful. I don’t know. Just by me loving you that day and put my arms around you, “Hey girl, you look down. If you need me, I’m here for you.” I could have saved your life and not even know it.
Participants also described that the community encourages authenticity in both physical and emotional expression. For example, one participant, who identified as transgender, cited feeling more comfortable and affirmed in LGBTQ community spaces: When I go to the LGBTQ centers, I feel more comfortable. [. . .] they are more diverse. They are more real. And they understand you most of the time. [. . .] I feel like I can go as me and not be judged. People will treat me as me.
This idea of being “more real” was consistently expressed by participants. This came through in not only what was communicated, but also how the message was communicated. For example, another participant stated, I think that also the LGBTQ community is more open and willing to talk about things that matter, and we’re willing to just be open and not try to gloss over certain issues that need discussing. I think the open line of communication from the LGBTQ community is amazing.
Communication in this open and straightforward manner was suggested to improve the connection of community members. Because of this deep connection with each other, community members provide steadfast support to each other when in need.
I like real people. I’m connected to real people. And you’re real to me, because I love how you just say what’s on your mind and you don’t sugarcoat [. . .] We clash ’cause you say something I didn’t like. I say something you didn’t like. But I like real people. I like authentic people. It doesn’t get any better than that. But I know at the end of the day, “Come here girl, let me put my arms around you. I’m sorry for what I said. I was really mad and stuff like that.” So if you’re real, I’m connecting to you. [. . .] They come to your aid with fierceness, and it’s real. I don’t have to second guess, I know you got my back. And that makes me feel good.
Along with deepening community connection, some participants linked direct communication styles to improved health. One participant described that she and her friends are very “blunt” to avoid any misinterpretation of their messages because “there’s certain things you just can’t sugarcoat.” When asked how this might relate to health, the participant responded that straightforward messages may more likely influence health decisions. For example, if a friend is weighing options surrounding condom use while engaging in sex work, she would “make sure” the friend was using condoms by directly communicating: Screw if the man wants to pay you more not to use a condom. You’re being stupid just for a couple of extra dollars not to use a condom. You’re willing to cut down days of your life for a couple of dollars? What’s more important, a couple of dollars or your life? So, being blunt with things like that really do help your health.
Overall, the sense of safety and acceptance, cultivated through open, honest, and often brave communication across potential conflict and difference, was seen as a community strength among participants. Participants expressed that their well-being was inextricably tied to being able to be themselves not only without fear of rejection, but also with the expectation of being embraced and accepted.
Interconnectedness and Resource Sharing: “We Are Each Other’s Backbone” (N = 18)
Distinct from providing emotional support (e.g., acceptance), participants also highlighted a sense of interconnectedness between LGBTQ community members that focused on the exchange of resources and material support. This interconnectedness, for many, resulted in the creation of a network that community members have come to rely on to maintain and improve their health, as well as support the health of others. Participants articulated that community members were often bonded by similar experiences and, because of these similar backgrounds, they were able to exchange relevant and beneficial health information and resources with each other. Participants described being given information about or referred to doctors, health clinics, legal services, and housing resources by other LGBTQ community members and community agencies. One participant explained, I stay healthy because the community always giving information. It’s a lot of support groups, a lot if agencies, a lot of pamphlets, a lot of . . . They always giving condoms, stuff like that. It’s so many places that you can go and get information.
In addition to describing what types of information and resources are shared among community members, participants also described the ways in which the information and resources are exchanged. Participants consistently referred to a network of community members and community agencies on which they relied. For example, one participant stated, “Each one teach one. If you find out about something, we tell each other. Like, I say through word of mouth, networking.” Participant 34 confirmed networking as one of the ways the LGBTQ community becomes and remains healthy, “I went here; they were very nice; they took good care of me . . . and then of course then you know about it, you go and tell another friend, and another friend.” Another participant expanded, If their friend don’t know what to do, I’m pretty sure their friend can point you in the right direction for somebody who do go . . . Somebody who does know what’s going on. Or that person know what’s going on but can’t help you, somebody can point you in the right direction to get the help that you need. So, the community itself, it’s a really strong community.
The sense of interconnectedness and mutuality expressed by participants indicated healthy community relationships. The health-promoting community characteristics of interconnectedness seemed to build from a sense of acceptance and support, and also allowed communities to engage in the third theme: advocacy and collective action.
Advocacy, Collective Action, and Community Potential: “We All Stand Up” (N = 15)
Participants expanded upon and extended their perception of how interconnection supports the wellness of the LGBTQ community by describing the community’s immersion in social justice advocacy efforts. The community is described as “Always trying to empower themselves. Always speaking out about injustices” and, in these efforts, participants feel the community is “strong” and “powerful.” By engaging in advocacy, LGBTQ community members are moving beyond the provision of internal support—such as giving socioemotional or material support to each other—and working toward community equity and advancement through systemic change. For example, as advocates, LGBTQ community members are attempting to affect external structures and environments by interfacing with elected officials who are likely to respond to their constituents: This community, we don’t sit in the silence. [. . .] If anything we are beating those doors down. We are saying, “We are here. We exist.” [. . .] We hold the elected officials accountable. We hold City Council, Town Hall, all kind of things. You need to know who the elected officials are in each borough, because this is how you move some shit [. . .] And this community, we have resources. We have vast resources, and look at people like Menchaca and Mendoza. And Assemblyman Keith Wright, and Senator Perkins. [. . .] They listen to us. A Black trans woman going into the State Office to have a meeting with the Senator. That’s big, that’s big. And we all can do that, because we all will not settle [. . .] We don’t settle. So, we light some fire under people’s asses. [. . .] We could move some things.
Community members are also working for change through grassroots level. For example, some participants described their involvement in protests and rallies. These protests and rallies were described to occur in response to oppressive legislation or violence and are the community’s way to communicate their collective demand for change.
When there is an attack against us we all get together. If we had to protest you’d see something definitely . . . we all feel like we’re family and we all come out and help each other. Probably when everything is quiet you don’t feel that, but when something big happen you feel like a big movement.
Another participant confirmed, We organize like no one else. This community organizes, and we mobilize, and we show up in drones. When one of the sisters got hit, beat with a hammer over in Woodhaven, we got that rally together. It was the lesbians, the gays, the bi, we were all there. So our community comes together. We may not speak to each other every day. You may not like me, I may not like you. I don’t give a damn, but can we please come and make sure that the community is better for all of us? ’Cause you and I are just small pieces to a bigger puzzle.
Both of these examples acknowledge and reflect that, at times, the community may appear fragmented or less interactive, but community members are able to overcome these differences in times of need and respond as a unified front with the common goal for justice.
Community-level organizations are also at the forefront of grassroots advocacy promoting equity within the LGBTQ community. By addressing the multiple, intersecting oppressions that many LGBTQ community members face, these organizations work to advance the health and well-being of the community.
The Center, Queers for Economic Justice, these are organizations that I have volunteered my time to [. . .] Welfare Warriors, you have women that are on welfare and just fight that stigma with welfare [. . .] There’s a lot of going on in a lot of organizations [. . .] I think as much as we can, we’re doing the best we can with as much as people are willing to help change the stigma. I was with Queers for Economic Justice before they even had an office. That was some grassroots. And I can only speak on low-income areas, because that’s my community. I’m a low-income gay woman and that’s all I know [. . .] Audre Lorde, Ira’s House. There’s a few places that really do try to support good health, not only physically but mentally.
While advocacy efforts made by both organizations and community members have improved the lives of LGBTQ people, participants also acknowledged that there is much more work to complete: And we are breaking so many barriers and stigmas and stuff like that. Because look, it took a long time for the whole damn government to be like, “Marriage equality.” But then you got me over here saying, “Fuck marriage equality. We need more than marriage equality. We need housing, education and jobs.”
In sum, participants pointed to efforts of community power building, leadership, sociopolitical engagement, and critical consciousness raising as key community strengths.
Some participants cited that the community stays healthy by focusing on the belief that the best is yet to come for the community. Emphasizing this belief as an asset of the community, one participant stated, “We are better than ever before. We are rising.” Overall, the theme of community potential reflected a sense of growth and possibility. The LGBTQ community was described as forward thinking in more than one sense. To be sure, for many participants, the sense of potential was grounded in the community’s creativity, artistry, innovation, and resourcefulness. One participant stated, “There’s amazing cool, quirky, unique things coming out of the LGBTQ community, creative projects, ideas, innovation, a new perspective that’s really needed.” Several participants, however, described non-LGBTQ people’s problematic relationships with the community’s ingenuity and potential. While one participant initially stated, I believe that my community is really, really strong. Coming from where we come from to where we are now, we have made changes for decades, constantly growing [. . .]
They went on to say, So many of us are the silent stars of this world [. . .] So the strength that we have is, I think it’ll still be untold.
This participant expressed that despite consistent changes and evolution over time, the potential of community members might not be broadly acknowledged by society, with those individuals remaining as “silent stars.” For this participant, believing in the LGBTQ community’s “untold” story and future was a primary source of health in the community.
Alternative Community Experiences
While the majority of participants could identify strengths and strategies that contributed to the overall health and well-being of the LGBTQ community, five participants provided alternative perspectives. Of these five participants, two stated that they were not connected to the larger LGBTQ community, or not connected in a way where community members affected their health. When asked to describe some of the ways that the LGBTQ community stays healthy and also the ways the community helps them stay healthy, one of these participants initially stated, “I don’t try to get into that . . . I don’t let everybody into my business.” The interviewer followed up asking the participant if she felt connected to the LGBTQ community, to which the participant responded, I get connected, but there’s a part when it goes too deep into my business. I stay away from that. That’s not for me. I go to campaigns, I go to dinner, they have functions, I can do that.
In this response, the participant expressed her reticence around going “too deep,” likely viewing health as a personal and individualized issue, not one related to or influenced by community. The second participant initially began to describe her own strengths and when redirected to reflecting on the community replied, “Well I don’t really go to too many gay communities and stuff like that. I used to go to clubs and stuff like that, but I stopped.” When asked about her shift away from the LGBTQ community, the participant answered, “I became a parent.”
Two other participants described how they stayed healthy and provided advice for how other people could follow suit. When redirected to the community, the individualized perspective of health persisted in participant responses. Although this may be due to miscommunication between interviewer and participant, or misinterpretation of the question, a study on gay men’s definitions of health and ways to improve health showed that the majority of participants viewed health and health promotion from an individual or personal responsibility position (Adams et al., 2013). This individualized, rational choice perspective also remains a dominant view of health. As our study was primarily interested in community wellness, it may have been difficult for these participants to break from the dominant discourse that health is an individual responsibility. It is also possible that feeling like an outsider to the community also contributed to these two participants’ responses. Indeed, one participant consistently used “they” language when referring to health-promoting behaviors of LGBTQ communities, for example, “They just need to get annual checkups” and “They should be more for each other, watch out for each other, have each other’s back.” The second participant explained that a lot of her LGBTQ friends “have passed away already,” perhaps in part explaining the distance between this participant and the community.
Finally, the last participant with an alternative perspective initially answered the question with an individual health behavior (i.e., “we eat salads”) and when redirected to the community, this participant asserted that the LGBTQ community is divided and members are not willing to come to the aid of anyone outside their direct social network. Specifically, this participant stated, I feel like the LGBT community is so divided within themselves that—we’re unified, but we’re unified in our own cliques [. . .] I just hang out with who I hang out with. And I don’t talk to no one outside of my circle. And you know, I empathize with what you’re going through, but I’m sorry, I can’t help you.
The participant went on to describe being a “loner” who doesn’t “have a clique” within the LGBTQ community to rely on. Each of the participants with an alternative perspective on community health may have been isolated from the larger LGBTQ community. Potential connections between this finding and participants’ identities are explored in greater detail in the following section.
Discussion
This study explored health-promoting community strengths as identified by LGBTQ adults of color in NYC. Using a person-centered approach, ways in which community promoted health and wellness from participants’ perspectives were explored. Three major themes were identified: (a) safety and acceptance, (b) interdependence and resource sharing, and (c) advocacy, collective action, and community potential. The former two themes are consistent with a larger body of literature that identifies four underlying and distinct dimensions of social support that function to enhance well-being via the provision of emotional, tangible, informational, and companionship support (Cohen & Wills, 1985; Wan, Jaccard, & Ramey, 1996). The first theme—the fostering of safety and acceptance by the LGBTQ community as a strength and health-promoting factor—aligns with the function of emotional support, that a person feels valued and accepted (Cohen & Wills, 1985; Wan et al., 1996). The ability of a community as a whole to relay value and acceptance to its members might lie within the sociopsychological characteristics of a sense of community, such as belongingness, emotional safety, emotional connection, personal investment, influence, and fulfillment of needs (McMillan & Chavis, 1986). Ultimately, receipt of emotional support generally results in improved esteem, affect, and trust (Gottlieb, 1988; House, 1981; Wan et al., 1996). One recent study (Lyons, 2016) completed with a sample of older gay men emphasized the importance of emotional support in promoting health. The study tested the relationship between varying social support typologies and psychological distress. While the receipt of emotional, belonging, and practical support were all associated with decreased psychological distress in univariate regressions, in the multivariate regression model only emotional support remained related to decreased psychological distress (Lyons, 2016). As others have found, among LGBTQ people, the receipt of emotional support might mitigate the negative effects of pervasive heterosexism/cissexism on health and well-being (Fredriksen-Goldsen et al., 2014). For example, community members with strong support systems can readily rely on their network for emotional support, including increased interactions and validation of their experiences, if they encounter discriminatory events (Szymanski, 2009).
In addition, within this first theme of safety and acceptance, another form of support, “belonging support” (Holt-Lunstad & Uchino, 2015), emerged from the participants’ descriptions of how LGBTQ community members communicate with each other. Communication styles were described as “blunt,” as messages were not “sugarcoated” by LGBTQ peers, and linked to positive individual health behaviors, such as condom use. This finding parallels research completed with HIV-affected African American communities in which participants described the importance of relationships with other people living with HIV (Mosack, Stevens, Brouwer, & Wendorf, 2016). Specifically, participants indicated that they had a shared connection with other HIV-positive individuals and felt a level of trust that was not assumed with HIV negative people. In this trust, participants were able to have frank, unambiguous, and uncensored conversations about their problems including HIV-related health issues, drug use, and sexual risk behaviors. Our findings add to the idea that those with shared characteristics (e.g., shared identity, shared illness) may be uniquely equipped to provide support that enhances health and health behaviors of others within the group because the support provided is perceived as free of judgment. Because some LGBTQ people of color may experience nonacceptance, negative messages, and stigma from their family or racial/ethnic communities (Buttram & Kurtz, 2015; Kim et al., 2017), support from within the LGBTQ community, specifically, could be essential for wellness. This search for “belonging support” may also lead LGBTQ people of color to find their own niche communities or subcultures within the larger LGBTQ community; for example, they may join House and Ball communities to feel validated, accepted, and connected to the queer community (Kubicek, McNeeley, Holloway, Weiss, & Kipke, 2013).
The second theme—interconnectedness and exchange of material support/resources between community members to maintain or improve health—aligns with the functions of tangible and informational support, the provision of material resources and needed services, and the provision of advice, suggestions, and direction, respectively (Cohen & Wills, 1985; Wan et al., 1996). Many participants described receiving referrals and connection to affirmative providers and programs (as well as other resources such as legal services and housing) from other LGBTQ community members in their network. Along with the previous theme of acceptance, this idea of community reciprocity and interconnectedness may be seen as two core domains and functions of community, especially among LGBTQ communities. Related to the reciprocal exchange of material support/resources specifically, LGBTQ people may view this as a way to make a positive contribution to their community, especially if they had been helped similarly in the past (Wong, Sands, & Solomon, 2010). These findings also suggest that, for some, access to an informal care network can facilitate entry into formal support networks and systems (i.e., the health care system), when needed. This aligns with a study of transgender women of color who described that members of their social networks assisted with eased access to transition-related health care by offering recommendations for affirming providers and accompaniment to services (Pinto, Melendez, & Spector, 2008). Supportive network members might also encourage transgender individuals to continue to seek and receive health care if they have had prior discriminatory health care encounters, reducing the occurrence of forgone preventive and needed services (Hudson, 2019; Romanelli, Lu, & Lindsey, 2018).
Alternatively, some participants described a reliance on each other for health resources and information (e.g., condoms), rather than a formal care system. Past research indicates that people of color may rely more readily on their informal network (e.g., family, friends) when they have a health need (Lindsey, Joe, & Nebbitt, 2010). Given LGBTQ people and people of color’s historical exclusion and experiences of discrimination from formal care systems (Wilson & Yoshikawa, 2007), the insular reliance on an informal care system might be an adaptive strategy to attain and maintain wellness. The first two themes also support the suggestion that disclosure and acceptance of stigmatized identity may be a health-protective factor. Disclosure will permit access to not only tailored health services (Romanelli & Hudson, 2017), but also to previously described social supports. For example, prior research indicates that LGBT youth not out to their parents perceive their family as offering limited emotional, appraisal, and informational support (Muñoz-Plaza, Quinn, & Rounds, 2002) and those with greater internalized homophobia perceive the receipt of less emotional support (Kapadia, Halkitis, Barton, Siconolfi, & Perez Figueroa, 2014). Overwhelmingly, participants identified safe and accepting spaces as strengths of their communities, but also acknowledged the lack of welcoming, nonclinical settings for building community. For example, an absence of leisure activities and leisure spaces for the community, especially those that do not focus on alcohol (i.e., bars, clubs), was cited by participants. This might limit the opportunities for the community to provide and benefit from companionship support (i.e., participating in leisure and recreational activities with others to distract from problems and improve mood; Cohen & Wills, 1985; Wan et al., 1996). Recent research among LGBTQ older adults has shown that being able to participate in leisure activities is associated with good mental health (Fredriksen-Goldsen et al., 2017). As the role of leisure and companion support in wellness has been established (Lloyd & Auld, 2002), future research might consider how to enhance this dimension of support for LGBTQ communities of color, specifically.
The final theme—advocacy, collective action, and community potential—represented an investment in improving the opportunities for health and well-being for community members, as well as future community members. The forward thinking and sense of growth and possibility described by community members also reflected a strong sense of future orientation, a concept consistently associated with wellness (Lindstrom Johnson, Blum, & Cheng, 2014). This theme clearly reflected the strengths and resilience of LGBTQ people of color in the face of adversity. Participants who spoke of activism and advocacy in their communities as facilitating health may understand that some of the biggest health risks LGBTQ people of color face are due to the structural and social issues that have been, and will continue to be, addressed in part by grassroots community organizing and other forms of advocacy and activism. As Singh (2013) suggested, involvement in and witnessing of advocacy may be associated with enhanced orientation toward the future. However, the concept of potential, from participants’ perspective, did not seem to only revolve around hope and optimism. Rather, participants identified their individuality, creativity, and resourcefulness as sources of possibility for the future. This finding echoes the research of Buttram (2015) whose results indicated that African Americans/Black MSMs identify participation in creative outlets such as poetry, fashion, design, and dance as a source of resilience and a means to achieve wellness. These qualities are tools of survival in marginalized communities.
Alternative Perspectives
Five participants communicated alternative perspectives on community strengths and health-promoting factors. These participants who described not being connected to the community, responded with individual-centered, rather than community-centered, strengths, and described division within the community. Interestingly, four of these five participants identified as bisexual, a subgroup who may be more isolated within the larger LGBTQ community. Not only are bisexual people the target of negative attitudes, minority stressors, and microaggressions from heterosexual people, but from lesbians and gay men as well (Bostwick & Hequembourg, 2014; Roberts, Horne, & Hoyt, 2015). Prior research has generally linked these stressors to social isolation, loneliness, and poor relationships with the LGBTQ community (Mereish & Poteat, 2015). Among bisexual people specifically, feelings of invisibility, isolation, and loneliness have been identified (Bostwick & Hequembourg, 2014; Mereish, Katz-Wise, & Woulfe, 2017). Furthermore, three of the less connected participants were above the mean age of the sample, with ages in the 50s. It is possible that some disconnection is connected to generational differences and/or aging (Masini & Barrett, 2008). Indeed, a recent study found that some older generations of sexual minority communities feel left behind and erased by young queer people in a “postgay identity movement.” This may lead to feelings of social isolation, rejection, and subsequently poor mental health outcomes among aging populations (Salway & Gesink, 2018). The respondents in the current study seemed to be isolated and disconnected from the larger LGBTQ community and thus unable to identify community strengths related to health.
Limitations
Despite the important contributions of this study’s findings, limitations must be considered. First, all interviewees were at least somewhat connected to the larger LGBTQ community or other LGBTQ community members; interviewees self-selected to participate after viewing study information at LGBTQ specific organizations or were referred by other LGBTQ study participants. Thus, the experiences of more isolated LGBTQ community members may not be represented in study findings. As the study was completed in an urban setting, it must be noted that there is a thriving and visible LGBTQ community in NYC. LGBTQ people outside of metropolitan centers might have less access to the supportive networks described by the current study’s participants. Past research completed in rural and nonmetropolitan settings suggests that LGBTQ people in these environments might not have easy access to a community and also describes a dearth of resources and support available (Paceley, 2016). Therefore, these populations may have unique strengths, resiliencies, and strategies for staying healthy. Findings from this study should not be considered representative or generalizable to all LGBTQ communities.
Second, there was little time to build trust and rapport with participants as only a single face-to-face interview was conducted. Because the interview questions broached sensitive topics, the limited time may have inhibited participants’ responses. Any discrepancies between the interviewer and participants’ social identities may have also affected the content of both the questions asked by the interviewer and responses given by participants. For example, based on social location, positionality, or lack of knowledge about some aspects of the community, the researchers might have consciously or unconsciously avoided certain topics or failed to ask certain questions. Third, this study did not ask participants to disclose personal health information (e.g., specific diagnoses, treatment histories) or complete any diagnostic measures. Because of this, the analysis could not account for the relationship between the cited strengths and health-promoting factors cited by participants and their actual health status. Finally, the authors did not employ any mechanisms to detect relationships among participants or the extent to which participants’ communities of reference were overlapping. Future research should pay attention to the social networks among participants, especially as a method to delineate any specific community strengths and health-promoting factors employed among unique LGBTQ communities.
Implications
Implications of this study revolve around the central assumption that in order for community strengths to be truly centered in research, policy, and practice, existing power relations need to shift in favor of communities, and new relations need to be forged across these power configurations. In concrete terms, this would require from health care organizations and institutions a commitment to community self-determination and listening to and centering the needs, concerns, and accomplishments of communities. This type of shift would also include uncovering potential opportunities to connect emerging community power with the existing, but amenable, sources of relative power, for example, community organizations, local policy makers, philanthropists, and researchers.
Research
Consistent with recommendations made by leading expert research and advocacy organizations (Ard & Makadon, 2012; Graham et al., 2011), we suggest that more data be collected regarding LGBTQ-identified populations and communities. Information that ought to be collected includes, as one might expect, identity characteristics and histories related to gender identity, gender expression, and sexual orientation. Furthermore, research should continue to pay attention to diversity within communities and be sure to include LGBTQ people from different social positions and backgrounds, including nonbinary people, people living with disabilities, low income, immigrant, best served in other languages, and so forth. To extend finding from this study, future research should examine more closely formal (e.g., agencies, community centers) and informal (e.g., social network) communities, to understand how information is shared and collective action is organized within and across these configurations. Future studies should continue to explore the connections between community belongingness, advocacy/collective action, and health. For example, what are the specific mediating/moderating factors that drive relationships among these constructs? What specific role do intersecting social identities such as age, race, socioeconomic status, and ability, as well as past trauma and geography, have in shaping experiences of health and community? Furthermore, research should continue to explore LGBTQ communities of color as the “healthy” subject, as opposed to the “wounded” subject, detailing additional aspects of community strengths and assets.
Policy and Practice
Community workers—psychologists, social workers, advocates, and agencies—play a critical role in shaping avenues for collective community strengths to make tangible impacts in communities. Critical community psychology is one potential disciplinary foothold from which to work with, for, and alongside members of marginalized communities to identify and build upon grassroots strengths, to enhance their/our ability to mobilize, to build power in their/our communities, and to enact that power over policy and economic resources. Specifically, insights from this study demonstrate the imperative of acknowledging and raising up LGBTQ people of color’s voices in activist networks and community organizing.
Participants in this study pointed to the need for more nonclinical, intergenerational spaces for LGBTQ people of color to gather and build community safely, which is a clear, specific, and (likely) achievable goal for those who work in community organizing and organizations. Such low-risk contexts would serve to build trust and information-sharing channels that might improve the health and health seeking of marginalized communities through raising awareness and reducing stigma. Addressing such barriers and enhancing health access through community power building requires collective action, channeling of resources into communities, leveraging resources already existing in communities, mutual support and care, and the sense of possibility.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the McSilver Institute for Poverty Policy and Research, New York University.