
Abstract
Individuals with Parkinson’s disease (PD) often experience poor mental and emotional well-being, which negatively affect their quality of life. Optimism is a protective factor which has been shown to promote resiliency, reduce distress in health crises, and protect against the effects of negative mental health outcomes. The current article utilized grounded theory methodology to examine personal accounts (N = 85) detailing how individuals were able to cultivate optimism despite challenges presented by PD. The grounded theory indicated that a process occurs in which individuals with PD move through the following five phases on their journey toward optimism: (a) diagnosis, (b) initial reactions, (c) adjustment, (d) acceptance, and (e) living with optimism. These findings indicate that individuals with PD often struggle to experience optimism. Nevertheless, by reframing optimism as a choice rather than a feeling, participants were able to make decisions that allowed them to progress on their journey toward optimism.
Keywords
Introduction
Parkinson’s disease (PD) is a motor system disorder that involves the loss of dopamine-producing brain cells. It is chronic, progressive, and degenerative and affects the central nervous system. Four primary PD symptoms include tremor or trembling, body stiffness, bradykinesia (slow movement), and impaired balance and coordination. Additional symptoms include poor mental and emotional well-being, urinary and colon problems, difficulty chewing, swallowing, speaking, and problems with sleep. PD often disrupts daily activities, especially as the disorder progresses (National Institute of Neurological Disorders and Stroke [NINDS], 2017).
PD is the second most common neurodegenerative disease in the United States with at least 50,000 Americans diagnosed annually (Hamza et al., 2011). Although most diagnoses occur among the elderly, 5% to 10% of PD patients are diagnosed under the age of 50 (NINDS, 2017). In addition, in a study completed by Mayo Clinic researchers, the prevalence of PD increased over a 30-year span between 1976 and 2005 (Savica, Grossardt, Bower, Ahlskog, & Rocca, 2017). PD is also chronic and costly. The average cost for an individual’s medication is US$2,500 a year. Additional surgeries can add up to US$100,000 per individual. The overall annual cost of PD in the United States is nearly US$25 billion (Parkinson’s Foundation, 2019).
In addition to the physical and financial impact of PD, emotional well-being may be affected as well. With the increasing prevalence of PD in the United States and the unique challenges accompanying it, understanding how this chronic illness impacts individuals may be of growing concern to mental health professionals. Previous research suggests that chronic conditions may influence emotional well-being. Research suggests that individuals with chronic back pain may oscillate between hope and despair (Corbett, Foster, & Ong, 2007), and, among clinicians, attention to patient fears may be beneficial (Sanders, Foster, Bishop, & Ong, 2013). Although emotional responses to chronic pain have been examined in previous literature, research examining emotional responses to PD is lacking. The purpose of this qualitative study is to examine patients’ emotional experiences following a PD diagnosis and to identify the process of finding optimism.
Background
Research suggests that poor mental and emotional well-being often accompany PD. Common symptoms include anxiety, depression, emotional changes, apathy, hallucinations, irritability, somatization, and obsessive-compulsive behaviors (Aarsland et al., 2007; Kulisevsky et al., 2008; Nègre-Pagès et al., 2010; NINDS, 2017; Siri et al., 2010). Depression-apathy and depression-anxiety are the most frequent comorbid diagnoses that accompany PD (Dissanayaka et al., 2010; Oguru, Tachibana, Toda, Okuda, & Oka, 2010). Mental and emotional experiences surrounding PD are important to consider because research suggests they may significantly affect patient well-being and quality of life (Gómez-Esteban et al., 2011; Schrag, Jahanshahi, & Quinn, 2000).
Poor mental and emotional well-being are difficult for PD patients to evade because they are closely linked with the symptomology, progression, and treatment of PD (Berney et al., 2002; Bronstein et al., 2011; Houeto et al., 2002; Kulisevsky et al., 2008; Perriol et al., 2006; Temel et al., 2006). For example, sleep is often affected by PD and can lead to experiences of depression, stress, and fatigue (Ylikoski, Martikainen, Sieminski, & Partinen, 2017). PD symptomology, medications, and complications can also lead to nutritional deficiency, which has been linked with negative emotional well-being (Fereshtehnejad et al., 2014). Furthermore, research suggests that certain medications used for the treatment of PD may cause depression (Kulisevsky et al., 2008). In addition, deep brain stimulation may cause or exacerbate preexisting mental health diagnoses (Berney et al., 2002; Bronstein et al., 2011; Houeto et al., 2002; Perriol et al., 2006; Temel et al., 2006). Greater understanding of the effects of PD symptomology on patient well-being may help clinicians improve patient quality of life.
As negative emotionality is frequently experienced by PD patients and can adversely affect patient well-being (Dissanayaka et al., 2010; Gómez-Esteban et al., 2011; Oguru et al., 2010), identifying ways to cultivate positive emotionality may help improve quality of life (Hurt et al., 2014). Previous research suggests that specific processes may indirectly buffer negative outcomes. For example, Pearlin, Menaghan, Lieberman, and Mullan (1981) suggest that coping interventions and social support may protect individuals from depression by minimizing processes leading to depression. In the same way, optimism may facilitate positive emotional experiences that buffer patients from negative emotionality linked with PD. According to Karademas, Kynigopoulou, Aghathangelou, and Anestis (2011), positive perceptions such as optimism may protect patients against the effects of negative mental health outcomes. Optimism has also been shown to promote resiliency and reduce distress in health crises (Allison, Guichard, & Gilain, 2000); buffer effects of stress and enhance well-being for individuals with chronic illness (Gustavsson-Lilius, Julkunen, Keskivaara, Lipsanen, & Hietanen, 2012); and fuel motivation to protect health (Carver, Scheier, & Segerstrom, 2010). Furthermore, positive perceptions of illness are linked with better patient outcomes (Evans & Norman, 2009; Hagger & Orbell, 2003). Optimism can also improve various facets of life for individuals diagnosed with PD, and the effects of optimism can be long-lasting. This benefit may be especially helpful for individuals diagnosed with PD. Research suggests optimism can be maintained throughout the duration of PD, despite PD’s progressive nature (Gison, Rizza, Bonassi, Donati, & Giquinto, 2015).
Although previous research has explored links between optimism and improved well-being and quality of life for individuals diagnosed with PD, very little research examines how individuals diagnosed with PD find optimism. This qualitative, grounded theory study sought to examine the underlying process that individuals diagnosed with PD experience on their journey toward optimism. The study was guided by the following research question: What is the process of finding optimism after receiving a PD diagnosis? We aimed to discover common experiences of PD patients as they progressed from receiving their PD diagnosis to finding a new optimistic perspective.
Method
Constructivist Grounded Theory
The goal of a grounded theory study is to develop an explanative theory which describes a basic social process (Starks & Brown Trinidad, 2007). Given our interest in understanding the process by which individuals with PD develop optimism, constructivist grounded theory methodology was utilized in this study (Charmaz, 2014). This methodology is especially appropriate when investigating a given phenomenon when no current theory exists (Charmaz, 2014; Corbin & Strauss, 2008; Echevarria-Doan & Tubbs, 2005). Grounded theory methods are used to construct theories inductively from the data through an iterative process in which researchers move back and forth between the data and the developing theory (Charmaz, 2014). This process allows researchers to develop a theory that is grounded in the data (i.e., research participants’ experiences), rather than from preexisting ideas.
Researcher Reflexivity
Constructivist grounded theory acknowledges the influence of the researcher on the research process (Charmaz, 2014; Daly, 2007). Researcher reflexivity requires that researchers acknowledge any biases or relationships to the topic being studied that may influence the research process (Charmaz, 2014; D’Aniello & Fife, 2017). All of the researchers have training as marriage and family therapists. Our training is rooted in systems theory, which leads us to consider the individual and their social context instead of simply focusing on internal processes. The first two authors also have specific interest in medical topics due to personal experiences with family illness, and the third author has previous research experience with the impact of illness on individual and family well-being, as well as extensive experience with grounded theory. Throughout the research, we remained aware of personal interests, conflicts, and professional training and remained committed to a rigorous process of analysis in which we strove to remain faithful to the accounts and experiences of the research participants. For example, we utilized memos during the analysis to record our thoughts and insights about the data, which included reflections on our own experiences and preconceptions about chronic illness and optimism. We discussed these reflections as a team to avoid premature foreclosure on the meaning of the categories or forcing the analysis to fit our preexisting ideas (Charmaz, 2014).
Sampling and Participants
Data were collected from the American Parkinson Disease Association (APDA) website, www.apdaparkinson.org/story/. The APDA works to assist those with PD in having a high quality of life. They fund educational programs, promote public awareness, and support research (APDA, 2017). As part of their services, APDA encourages individuals living with PD to post stories of optimism to help ignite and inspire a sense of optimism in others. The website invites individuals with PD to share what makes them optimistic to provide hope for others that dignity and optimism are possible when living with PD. Each post was copied from the website into an Excel spreadsheet and given an identification code for use in the analysis process.
The ability to obtain demographical information was limited by the passive analysis that was conducted with these data. Most of the participants chose to share only their first name and photograph with the public. Demographical information such as gender, age, relationship status, occupation, and socioeconomic status were not available for most participants and would have required assumptions to be made by the researchers. Therefore, similar to other studies utilizing online data (Cravens, Whiting, & Aamar, 2015), no conclusions can be drawn based on sample characteristics. A total of 85 first-person accounts from individuals with PD were used for the study.
Ethical Considerations
This study was approved by a university institutional review board. It was considered an exempt study as the data used were publicly available, and the researchers had no contact with participants. While no clear guidelines for Internet-based research currently exist, ethical considerations were addressed as recommended by Heilferty (2011) in an article discussing ethics when using online illness narratives. Decision-making in qualitative studies using data such as those used in the current study is typically grounded in the protection of participants, autonomy, confidentiality, and privacy (Heilferty, 2011). In addition, Eysenbach and Till (2001) provide questions for researchers to consider when utilizing online data: (a) are the posts public or private? (b) what is the size of the website? and (c) what is the level of perceived privacy of the membership community? In consideration of these potential ethical issues, this study used data from participants who voluntarily reported to a public access website for the purpose of sharing their story of optimism with others. Participants were not put at an increased risk because they chose to share their information publicly when they submitted their story. The APDA website also has a privacy tab which details the agreement each participant is entering when sharing their story. In addition, the data collection process did not require any interaction or contact by the researchers with the participants. All the posts used were free of identifying information. The posts are generally anonymous, even via a Google search. Similar studies using information from online data sources found this de-identification process to be acceptable to achieve general autonomy (Cravens, Leckie, & Whiting, 2013).
Analytic Process
For the current study, we utilized constructivist grounded theory as described by Charmaz (2014). The analysis was completed through several stages: initial coding, focused coding, axial coding, and theoretical coding. Although the stages are described sequentially, we utilized a recursive process of constant comparison throughout the analysis to develop a substantive grounded theory (Charmaz, 2014; Glaser & Strauss, 1967). Analysis began with initial coding in which we independently analyzed each participant’s account using word-by-word and line-by-line coding. Following our independent analysis of the participants’ accounts, we met to review our coding and discussed the similarities and differences in codes, which codes could be collapsed together, and which codes were central to the research question. When discrepancies arose in our analysis, we discussed the different meanings and deliberated until we reached a consensus.
Next, during focused coding, we compared our initial codes with our data, considered patterns in participants’ accounts, assessed which codes best accounted for the data, looked for gaps in our data, and identified prominent themes. We then utilized axial coding to understand the relationship between the data and the codes that were prominent in the analysis. Axial coding helps clarify and extend the analytic power of emerging ideas (Charmaz, 2014). We considered which codes could be grouped together, which could be categories and subcategories, and how the categories and subcategories were related. We worked together to distinguish the main categories and codes which could be grouped as subcategories under the newly identified main categories. Coding continued in a recursive process until saturation was reached.
Our next step was theoretical coding. This required us to carefully review the data and our analysis to solidify the relationships between the main categories and the order of events related to the process of developing optimism. An initial model was created to represent the different categories, subcategories, and their relationships. A fidelity check was conducted as part of theoretical coding. We presented our findings to several colleagues and invited questions and feedback for clarification of the developing grounded theory and to bring to light any codes or categories which may have formed from our own preconceptions of the data. With helpful input from our colleagues, we refined the grounded theory and the model of developing optimism, which we present below.
Results
Theoretical Model
Results revealed that individuals who found a new perspective after a PD diagnosis undergo a process of changing perspectives that begins with receiving their diagnosis and ends with behaviors and emotions exhibiting optimism. Through data analysis, the theoretical process model, shown in Figure 1, was created and includes five different phases. It is important to note that while this model presents a path toward optimism, challenges ebbed and flowed for participants throughout their journey. Phase 1 details the circular process of symptom recognition and physician interaction which occurred while the diagnosis was solidified. Some participants recognized their PD symptoms and others had family members who recognized their symptoms, which then prompted a visit to a physician. Others had an interaction with their physician and then began to recognize their symptoms. Participants’ initial reactions to their diagnosis are detailed in Phase 2. They discussed their own positive and negative reactions, and some discussed their family’s reactions as well. After the initial reaction, some participants experienced a period of adjustment while others moved straight into acceptance. Phase 3 describes the process of adjustment in which participants discussed struggling with physical changes, having to relocate, and changing careers. For participants who experienced a period of adjustment, finding support aided them in moving toward acceptance. In the fourth phase, acceptance, participants were ready to face the challenges of their diagnosis, created bucket lists, and made changes to their diet and hobbies. The most prominent and important aspects of Phase 4 were healthy lifestyle and hobbies. Experiences in Phase 4 prepared participants to move into Phase 5, living with optimism. This phase detailed behaviors and emotions experienced when participants found a new optimistic perspective. This process is described in further detail below.
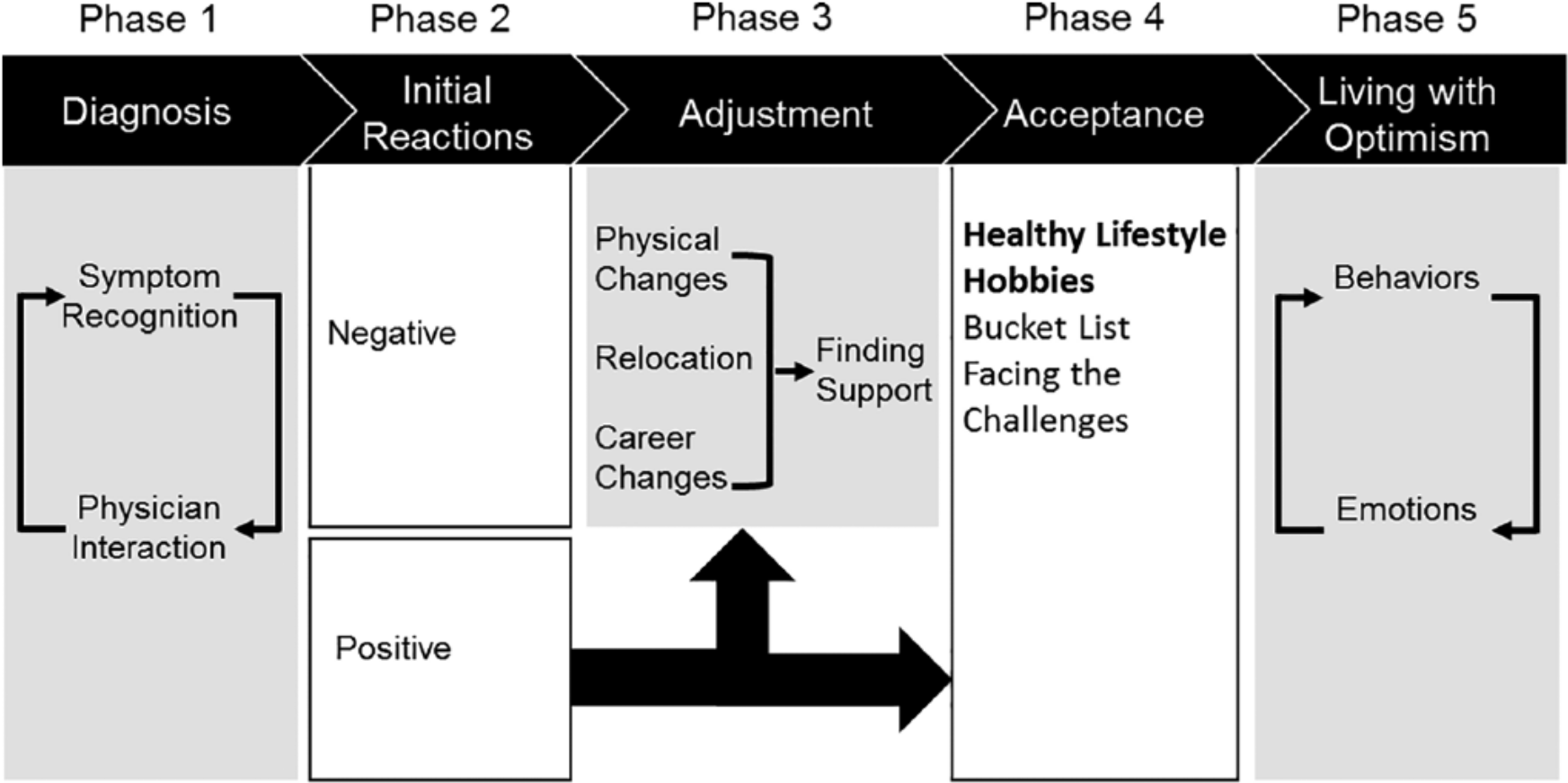
Stages of finding an optimistic perspective.
Phase 1
Diagnosis
The process of finding optimism began after participants received their diagnosis. This phase reflects the circular process between the two categories: symptom recognition and physician interaction. For some participants, they or someone else recognized their symptoms, and then they sought physician care. For others, their physician was the source of their symptom recognition. Whether the symptom recognition prompted their physician interaction, or their physician interaction prompted their symptom recognition, most participants described a process of diagnosis which cycled between the observation of symptoms and medical testing, which resulted in their PD diagnosis. There were some participants who went through many cycles of symptom recognition and physician interaction to be diagnosed: As a result of unexplained symptoms: hand tremors, change of gait and arm swing, I was prompted to seek medical evaluation . . . The neurologist was pleasant and affable. I was subjected to a series of clinical tests and evaluations . . . At the culmination of the series of physical tests . . . the pronouncement: Parkinson’s Disease . . . 100% surety . . .
Receiving their PD diagnosis always preceeded and provided a natural transition into Phase 2, initial reactions.
Phase 2
Initial reactions
During this phase, nearly half of the participants discussed the initial reactions to their PD diagnosis. This phase was made up of two categories: positive and negative reactions. Participants largely described their own personal reactions to receiving their PD diagnosis but several also described their family members’ reactions as well. A large majority of the initial reactions described by participants were negative. Participants generally experienced feelings of disbelief, anger, sadness, denial, and even depression. One participant shared, “My first reaction was to cry, and cry I did for several days. I was inconsolable.” Positive initial reactions were seen from participants who had spent significant amounts of time in Phase 1 waiting for their diagnosis and lived with uncertainty for extended periods. One participant explained, For whatever reason, I was terrified of the possibility of Parkinson’s, . . . As time went on and my walking deteriorated to the point where it was a major struggle to walk down the hall, . . . and I became more open to getting a firm diagnosis, no matter what it was . . . Eventually, I traveled to a clinic that specializes in a team-based approached to diagnosis, and within two days they had made a positive identification of Parkinson’s and prescribed medication. I cannot begin to describe the relief that I felt as the medication began to help.
While this was typically the stage that participants spent the least amount of time in, it was important because it determined their path of finding their new optimistic perspective. Participants who had a positive reaction often experienced a shorter adjustment period than those who expressed a more negative initial reaction or skipped the adjustment period altogether. Those who had a negative initial reaction, or whose families had a negative reaction, experienced a prolonged adjustment process.
Phase 3
Adjustment
The adjustment phase described the period in which a vast majority of participants were dealing with several changes brought on by their PD diagnosis. Our analysis of the participants’ accounts led us to identify four key factors of adjustment: physical changes, relocation, career changes, and finding support. Participants discussed the physical changes they saw in their bodies. Physical changes were seen in participants’ physical movements and shaking of limbs but were also reflected in other less thought about areas such as their handwriting: “I started writing with my left hand and compensated every symptom very easily. My walk started to bother me somewhat in my mid 20’s and I also started having symptoms in my left side.” Often, participants went through a series of adjustments with their medication due to their physical symptoms. Some of the participants even discussed relocation to be closer to treatment facilities.
It was also relatively common for participants to change career trajectories or quit working altogether. Some participants were able to find less demanding work while others were encouraged to quit working altogether due to the stress they were experiencing and its negative effects on their physical symptoms. Some of the participants were upset by no longer being able to do their job, such as one participant who shared, I did not choose this profession . . . I sacrificed a lot to graduate from law school and practiced for 22 wonderfully interesting years. I don’t know why my higher power made it not possible to practice law, something I loved to do (not many people can say that about their job).
Other participants discussed their career changes as a more positive change: I ended up losing my job and wasn’t sure what to do. Since I liked to write and I like humor, I began writing my memoir. I ended up with a file of humorous Parkinson’s Disease stories. I found that I enjoyed writing humor. Not only because it is fun, but it is play and helps me feel better physically.
Despite the physical, location, and career changes, finding support was the key factor in moving participants from the adjustment phase into the acceptance phase. Family, friends, faith, and support groups were frequently mentioned by participants when discussing where they found support. Family members and friends helped with physical and emotional support, but they also assisted participants with logistical tasks such as planning or cooking. It seems that the emotional support was the piece of finding support that was the most important in helping participants feel as though they were not alone. One participant shared, I also joined a PD support group and was able to learn so much! I also shared with the group by teaching 5 minutes of fitness each month. During these last 10 years of living with Parkinson’s, no day was like the last. I had to give up a lot of the physical activities my husband & I shared . . . but with the help of caring & supporting family members, a few special friends, doctors & my husband I have been back to moving & finding my groove while starting to improve!
Phase 4
Acceptance
The acceptance phase immediately followed the adjustment phase and described the period when nearly half of the participants began to embrace their new lifestyle. Acceptance was the first outcome observed in which participants’ perspectives on their PD diagnosis began to change. A shift was seen from having to adjust to living with a diagnosis they did not ask for, and often were devastated to have, to beginning to modify thoughts about their life and future. Acceptance encompassed participants leading a healthy lifestyle, finding new hobbies, creating a bucket list, and facing the challenge of their diagnosis. All these items were positively focused on the future and gave participants things they could be actively doing to improve the outcome of their diagnosis.
Healthy lifestyle
The transition into a healthy lifestyle was achieved by maintaining a healthy diet and creating an exercise routine. Participants shared that diet and exercise were important pieces of prolonging the onset of their symptoms. Some individuals shared that maintaining a healthy lifestyle created a sense of control and allowed them to feel optimistic about the future: “I finally got moving in the right direction with exercise and appropriate medications for my treatment with my movement disorders specialist. I liked the idea of increasing exercises & physical activity instead of increasing medications.” Participants discussed seeing improvements as a result of their exercise routine: As I continued to do fairly well, I kept increasing my weekly amount of exercise. I took up tai chi to help with balance. I added a yoga for Parkinson’s class. I walked as much as I could. I started working with a personal trainer. I exercised 5, then 7 hours a week. Now I have very little wearing off, very little dyskinesia, and I exercise roughly ten hours a week.
Hobbies
Participants used hobbies, including physical activity they incorporated into their new healthy lifestyle, as a form of therapy where they could set and accomplish goals for themselves: “They say exercise is the best therapy and I have chosen to pursue powerlifting and the beautiful sport of Olympic Weightlifting.” “I went to Hawaii and caught a marlin, did 2 triathlons (sprints), earned my Black Belt in Taekwondo, acted in several plays, and a variety of other activities.” Some viewed their hobbies as something they could do despite limitations they endure as a result of their diagnosis: “I have given up working and driving but am learning new songs and practicing old piano music.” Still, others described their new hobbies as a source of connection: “I’m blogging about my experiences and have developed a social media website with apps dedicated to light and feel lit within, no matter your storm in life.” Another commented, “I have kept busy spending time with grandchildren, quilting, gardening, doing volunteer work and advocating for Parkinson’s.”
Bucket list
Some participants made a list of things they wanted to do before their symptoms progressed and they were no longer physically able to do them. “I pulled money out of my retirement and took my children to England while my mobility was still high.” For several participants, this gave them something to look forward to and to be excited about in the future: “I immediately got out my bucket list and thanked God for the challenge and started knocking down my list.” Their bucket list was also a way in which they could keep up with their lifestyle changes. “I keep adding to my bucket list: zip lining with my 12-year old grandson as soon as he weighs 80 lbs., soaring, parasailing, and returning to quilting.”
Facing the challenge
This category was a little different for participants depending on whether they went through the adjustment period or skipped it. One participant who had a positive initial reaction and skipped the adjustment phase shared, “Rather than withdrawing and feeling depressed, I made it a goal to engage life more, living each day to the fullest, embracing and savoring every moment and surrounding myself with people who nourish me.” One participant who quickly went through the adjustment period said, “After some self-assessment & introspection, I elected to meet Parkinson’s head on as a life challenge.” A participant who was in the adjustment period for longer before moving to acceptance wrote, I didn’t understand the many facets of Parkinson’s Disease until I attended a support group meeting where I learned that Parkinson’s Disease does not discriminate between age and symptoms of the disease. It was then that I decided then to get educated and take a positive step forward.
In all four of the categories, it is evident that there was a similar shift in which participants were beginning to find a new optimistic perspective of their PD diagnosis. While many of the categories were somewhat intertwined, they were also distinct and individually important methods through which participants were able to begin moving toward living with optimism. These categories were the final step before participants were able to move into living with optimism as described below in Phase 5.
Phase 5
Living with optimism
This phase described all the participants’ experiences when they were able to embrace an optimistic perspective of their PD diagnosis. It consisted of two different categories which exhibited participants’ new perspective on their PD diagnosis: behaviors and emotions. These were circular, symbiotic categories in which participants did behaviors which led to feelings of optimism and had feelings of optimism which led them to exhibit more optimistic behaviors. These categories collectively constructed the participants’ new perspective on their diagnosis.
Behaviors
This category included participants doing things such as striving for achievement, advocating for PD, and giving back to others. These behaviors mainly included actions which led to feelings of optimism. Some of these behaviors were done to promote the individual’s own success, while other behaviors were aimed specifically at promoting the success of others. Striving for achievement, for example, was one way that participants were able to do things they did not do before their diagnosis or things they thought they would not be able to do after receiving their diagnosis. One participant’s comments are representative of this: I didn’t let Parkinson’s Disease stop me from making my dreams into a reality. I went to college, and I was one of the first of my class to get an Economist degree. I worked as an Economic Analyst for the Stock Exchange Magazine, and I was very proud of myself because I published more than 20 articles. I meet the love of my life.
Advocating for PD and giving back to others were somewhat connected. However, advocating for PD was defined as one of the behaviors which was used to promote or provide public support and awareness for the disease, research, or policy surrounding the disease. For example, I shared my story on a Facebook Status because I was tired of people saying “why are you shaking?” And I said you know what? The world needs to know that this condition doesn’t have any age. And that in fact we have to create awareness and get people involved in knowing and engaging themselves with it.
Another participant described advocating by becoming a participant in a research study: “Next month I will begin participating in a study . . . to help researchers study a young onset patient.” Other participants discussed advocating for PD by heading committees and raising money for research: As an advocate, I was the Chairperson for Coordinating Volunteers for the Passage of Proposition 71 (California Stem Cell Research Initiative) in San Diego County. I also spoke before the Senate Committee on Health and Human Services on behalf of Parkinson’s patients and the need for stem cell research funding. I have advocated for additional support for research by attending the California Life-Science Day, at the state capitol in Sacramento. I have also done interviews with local television and print media. Parkinson’s may have changed my life, but I won’t let it stop it.
Giving back was seen when participants decided to do things which would help motivate and encourage others with PD. Some participants led support groups, figured out where they struggled in their own journey, and used giving back as an attempt to make the lives of others living with PD better: “Parkinson Disease may change our bodies, but we still can give back to our communities and make a difference in other’s lives.” While giving back, participants found that they became more inspired in their own personal journey with PD: In helping others find theirs, I have created a purpose for myself and the amazing thing is I found that I began to enjoy life more! It was not just service to others; it became a pathway to regain my lost dignity and optimism, and sense of value as a person.
Whether giving back helped others or themselves, it was the act of doing services for someone else that seemed to allow participants to continue to feel optimistic and live with this new perspective and find meaning for life.
Emotions
This category encompassed feelings of hope, determination, and gratitude/having a positive attitude. This category also described times when participants had internal experiences of optimism, which often led to doing optimistic behaviors. Participants discussed feeling hopeful for the future due to medical and technological advances while others relied heavily on their faith for support. Some participants felt that it was important to maintain a balance between hope and realism about their diagnosis: “We live in reality, but we live with hope. There is still much I can do. I can dance with my heart . . . my body will follow.” Participants were also hopeful that there may someday be a cure, and optimism was the way to get there: I have chosen to be optimistic about my PD diagnosis and show that optimism by exploring an array of new medical technologies that are being advanced on a broad front of disciplines. I believe that an active research effort, combined with grass roots support and out-reach, position the realm of PD sufferers to be on the cutting edge of advancement and hope for the future.
For the participants overall, hope was the day-to-day feeling they called upon to move themselves toward determination.
Determination was an internal process that often stemmed from hope and was a state of mind in which participants, for a variety of reasons, decided that they would not let themselves be defined by their diagnosis. They exhibited determination a day at a time: “My motto is: Just because I am a statistic does not mean I have to, nor do I want to, be treated like one! I take things one day at a time.” Some displayed determination by reaching goals: “Today, 15 years into my PD, I am in the best shape of my life and determined to remain that way, if not get in better and better shape!” Other participants discussed being determined to live their lives as an example for others: “I wanted to show my 3 boys that with faith, perseverance, and hard work you could do just about anything you wanted.”
Showing gratitude/having a positive attitude was evidenced by participants’ desires not to be defined by their disease: What I want my story to convey is that there is life after diagnosis. My motto is “Live with Parkinson’s, don’t LIVE Parkinson’s.” I did not let this disease define me—I hear people call themselves “parkies.” This makes me cringe. I am not a disease. I live with Parkinson’s in the background, yes, it always there, but if you let come into the foreground, it will consume you.
Participants discussed having found a fighting attitude toward the disease: “I’ve decided that I’m not going to ‘live with’ PD but instead, I’m going to ‘fight’ it every step of the way through knowledge, diet, exercise, and most importantly, attitude.” He continued, “While PD may have taken away some parts of my life, it’s also given me a new purpose, focus, and direction, and that’s not a bad thing.” They also discussed how having a positive attitude is one of the most important things that someone living with PD can have: A positive attitude is the primary tool we have to personally combat this disease. This is the attitude that drives me to maintain a schedule of 30 meds every 24 hours, to exercise as much as possible, and to sing in public.
Overall, having gratitude/a positive attitude seemed to be what some participants viewed as the most important part of maintaining their new perspective of living with optimism. It is important to note that while finding a new perspective seemed to be somewhat of a linear progression, participants certainly experienced difficulties throughout this process. However, once participants found optimism, it seemed that they were able to carry that perspective throughout the remainder of the challenges they faced. This was obvious not only in the language used to describe challenges, but also in the underlying tone of their posts.
Discussion
This study examined how individuals with PD find optimism. For the participants in this study, finding optimism involved cycling through various phases, which is common for individuals following the diagnosis of a serious illness (Boer et al., 2014). Existing research suggests that learning to live with a chronic illness is a process, and patients often experience emotional ups and downs (Albaugh, 2003; Rapport, 2018; Robinson, 2017). However, the journey to finding optimism may vary according to the diagnosis, the nature of the illness, and prognosis (i.e., whether the illness is treatable, chronic, progressive, or terminal; see, for example, Rapport, 2018).
This study highlights the importance of processing positive and negative emotional responses following the diagnosis of PD. Most of the participants’ initial emotional responses were negative, which echoes findings in previous research on patients diagnosed with chronic illness (Boer et al., 2014; Due-Christensen, Zoffmann, Willaing, Hopkins, & Forbes, 2017; Robinson, 2017). In light of our findings, it is important to consider that symptoms of PD might heighten negative emotional responses. Because PD is a neurological disorder, both mood and cognitive abilities are often affected, leading to anxiety, depression, and cognitive impairment (NINDS, 2017; Parkinson’s Foundation, 2018). It is important to recognize that a PD diagnosis not only represents a devastating, life-changing event, but the physiological effect of PD on participants’ mental states may intensify their negative emotional responses. Although emotional expressivity, especially negative emotional responses, may seem counterproductive on a journey toward optimism, most of the participants that expressed their emotions also described their process of accepting the PD diagnosis. This finding is not surprising because previous research suggests that the processes of acknowledging and expressing emotions may be linked with better adjustment to challenges surrounding chronic illness (de Ridder, Geenen, Kuijer, & Middendorp, 2008). These findings are also similar to a grounded theory conducted by Vann-Ward, Morse, and Charmaz (2017), which illustrates the social and psychological processes individuals with PD face. Specifically, it was found that making sense of symptoms, defining turning points, experiencing identity dilemmas, reconnecting the self, and envisioning a future were important to preserving individuals’ sense of self (Vann-Ward et al., 2017). It is possible that acknowledging and processing emotions is a precursor to the acceptance of a PD diagnosis.
Similar to other research about living with chronic illness (Robinson, 2017), the grounded theory in this study highlights the important role of acceptance in helping PD patients achieve optimism. Many of the participants that moved into the acceptance phase responded with lifestyle changes and altered mindsets. These changes may have helped participants cultivate a sense of mastery or control as they learned to live with PD symptoms. Determination was exhibited by participants as they expressed a desire to “beat” PD through diet and exercise. Despite challenges associated with initiating and maintaining healthy behavioral changes (Newson et al., 2012), most of the participants partook in some form of exercise. This may be due to the physical and cognitive benefits exercise provides for individuals diagnosed with PD. According to one study, physical exercise promotes global cognitive function, processing speed, sustained attention, and mental flexibility in individuals diagnosed with PD (da Silva et al., 2018). Several participants described benefits of dietary changes as well, a finding that is consistent with research suggesting that a nutritional diet will improve quality of life and cognitive functioning for patients with PD (Yun, Lim, Woo, Ahn, & Choue, 2012). Many of the participants also developed new hobbies, which created positive experiences and may have promoted optimism. This finding supports previous research suggesting that creative activities may help patients learn to cope with chronic conditions (Reynolds, 1997). Lifestyle changes may have provided participants with a sense of control over their situation, which supports prior research suggesting that mastery is a common coping strategy for individuals experiencing illness (Stiegelis et al., 2003; Taylor, 1983). However, research participants’ determination and proactive behavior described in their blogs contradicts other research suggesting that apathy is a frequent symptom of PD, affecting up to 51% of PD patients (Kirsch-Darrow, Fernandez, Marsiske, Okun, & Bowers, 2006). It may be that the sampling of individuals who shared stories of optimism resulted in a group of participants that was uniquely proactive in its response to diagnosis. Although a lack of motivation, common to basal ganglia disorders (Shulman, 2000), may create obstacles for patients with PD, the participants in this study exhibited extraordinary determination as they accepted their diagnosis and responded with positive lifestyle changes. This approach could be helpful for patients who struggle emotionally with a PD diagnosis.
Optimism described by participants in this study includes two components, “emotions” and “behaviors.” Emotions, or “feeling” optimism, were expressed by participants in this study as they described happiness, gratitude, and hope; however, behaviors, or “doing” optimism, seemed to have a far greater impact on participants’ ability to achieve optimism. For example, optimistic “behaviors” were mostly comprised of advocacy for PD and giving to others, both of which seemed to help participants find meaning. This finding is important because previous research suggests that finding meaning may be a positive coping strategy for individuals with a chronic illness (Taylor, 1983). Although research on chronic illness linking finding meaning with advocacy and giving is lacking, previous research does link performing acts of kindness with an increased sense of well-being (Lyubomirsky, Tkach, & Sheldon, 2004), and finding meaning with better acceptance and adjustment (Yen et al., 2009). Furthermore, participating in an illness community can provide support for self and others (Berard & Smith, 2019). More research is needed to explore how individuals with chronic illness can find optimism through advocacy and giving to others.
Limitations
Some limitations were created by the nature of secondary data analysis. For example, we were unable to control the data collection process with the participants; therefore, we were unable to ascertain which questions were initially presented and unable to provide any follow-up questions. In addition, the participants who shared their story of optimism on the APDA website had access to other participants’ posts as well, which likely influenced the content they provided. Although it was difficult to determine the influence of the existing stories of optimism, differences in codes and emerging themes discovered in the analysis indicated that influence was likely not strong. In addition, previous studies using online data have suggested that the online format may allow for the avoidance of other biases and could balance out the drawbacks of not having contact with participants (Gavin, Rodham, & Poyer, 2008).
Furthermore, due to the passive nature of the analysis used in this study, no detailed information could be collected about participant demographics, the length of time the participants had lived with the disease, nor the severity of their symptoms. What is known about the participants is that they self-identified as living with optimism, which is likely not true of the entire population of people diagnosed with PD. Our participants were also interested in telling their story of optimism to inspire others. In addition, these individuals had access to a computer and Internet and were in some way connected with the APDA. It is important to acknowledge that while we cannot draw conclusions based on sample characteristics, this group may differ from the general population of individuals living with PD.
Another limitation was that the theoretical sampling could not be completed. This would have been beneficial in helping narrow the model and categories, and in allowing participants to have input during this process (Charmaz, 2014). We acknowledge that the current study, and all research, is partially motivated by values and biases of the researchers. While experiences of illness cannot always be summarized simply as “good” or “bad” (Corbin, 2003), our findings may not fully encompass the negative experiences surrounding PD in comparison with other qualitative studies examining chronic illness (e.g., Jessup & Parkinson, 2010). Therefore, these findings can be viewed as one representation of this phenomenon, but not necessarily the final word, as is consistent with the constructivist paradigm under which this study operated. To balance this, researchers used several steps, as discussed above, to ensure that the findings were supported by the data and allowed the participants to speak for themselves (Charmaz, 2014). It is our hope that these stories of optimism provide insight into the process related to finding optimism after receiving a PD diagnosis. Clinicians who better understand this process will be better prepared to assist individuals and families who are experiencing a PD diagnosis.
Clinical Implications
Optimism can be beneficial for individuals who are diagnosed with a serious illness, particularly in terms of mental and emotional well-being. For example, cancer patients with greater optimism are able to maintain a more positive mood, hold greater expectations they will achieve their life’s goals, and experience less stress from their illness (Sumpio, Jeon, Northouse, & Knobf, 2017). Results from our study suggest that finding optimism is a process for individuals diagnosed with PD. Clinicians working with this population can assess for themes associated with each of the five phases to identify clients’ progress toward optimism. Specifically, clinicians can create space for individuals with PD to process emotions following a diagnosis, which may allow them to better adjust to challenges (de Ridder et al., 2008). This step may be crucial in the process of accepting PD and moving toward optimism. In addition, clinicians can help patients with PD gain a sense of mastery in other areas of their life as they lose control to PD symptoms. Lifestyle changes may help PD patients cultivate mastery and experience physical and cognitive benefits (da Silva et al., 2018; Reynolds, 1997; Yun et al., 2012). Furthermore, clinicians can encourage clients with PD to advocate for PD and give to others. This may help clients find purpose and meaning, leading to optimism.
Research Implications
This research involved secondary data, so future research could gather more data to build on these findings. Interviews, focus groups, or surveys could explore our findings and be used to create specific interventions. Additional studies could assess for the effectiveness of implementing interventions based on these five phases. Future research could also further explore the effect of giving and advocacy on individuals diagnosed with PD.
Conclusion
The process of finding optimism was outlined in five phases identified by this grounded theory. Each of these five phases appears to be an important step in the theory of developing optimism following a PD diagnosis. Although the process of finding optimism varied among the participants, most of these phases were experienced at some point by many of the participants in our study. Our hope is that the information provided will be helpful in providing resources for individuals and clinicians for improving the quality of life and well-being for individuals diagnosed with PD.
Footnotes
Acknowledgements
The authors would like to thank Dr. Amber McCord for her assistance with the graphical design of Figure 1.
Authors’ Note
Julie Gardenhire and Natira Mullet are co-first authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.