
Abstract
The end-of-life trajectory of cancer patients in palliative care (PC) elicits an anticipatory grief (AG) process in family caregivers (FCs). Although widely recognized, AG lacks conceptual clarification. This study aims to qualitatively explore the experience of FCs of patients with terminal cancer to identify the core characteristics and the specific adaptive challenges related to AG in the context of end-of-life caregiving. Data were collected through in-depth semi-structured interviews conducted in a clinical sample of 26 FCs of cancer patients in PC. Findings from thematic analysis suggest that the AG experience is characterized by traumatic distress from being exposed to life-threatening conditions and the separation distress induced by loss anticipation and current relational losses, challenging the FCs to long-term emotional regulation effort demands. These results contribute to the conceptualization of AG and may inform intervention programs for the main challenges the FCs face when adjusting to loss during end-of-life caregiving.
Introduction
With the aging of the population, chronic disease care has been transferred to outpatient treatment, involving the family in caregiving tasks that become more complex and demanding as the illness progresses (Aoun, Kristjanson, Currow, & Hudson, 2005; Weitzner, Haley, & Chen, 2000). The family caregiver (FC) definition includes any family member, friend, or partner who maintains a significant relationship with the patient and provides some kind of care (Hudson & Payne, 2009). Given their high level of involvement in caring tasks and their affective proximity to the patient, this population is vulnerable to high levels of distress during caregiving and bereavement (Raschick & Ingersoll-Dayton, 2004; Waldrop, 2007). Distress is commonly defined as prolonged internal suffering that can range from self-focused processing of negative emotions and stressors to an intensely aversive and prolonged processing of emotional states (Brosschot, Verkuil, & Thayer, 2018). In addition to stressors directly related to caregiving and their impact on their personal life (e.g., sleep deprivation), FCs must manage expectations and emotions associated with the fear of losing their significant other, a phenomenon designated as anticipatory grief (AG) (Wittenberg-Lyles et al., 2012).
Caregiver AG stems from the expectations surrounding the relative’s death, giving rise to a wide range of manifestations that are socially and culturally associated with grief in response to the loss of a significant other (National Cancer Institute, 2011). Although widely used in research and clinical practice, this concept has been very controversial due to contradictory results concerning its adaptive role in bereavement outcomes. Inconsistencies are attributed mainly to its conceptual uncertainty and to methodological errors in the evaluation of the construct (G. Fulton, Madden, & Minichiello, 1996; R. Fulton, 2003; Reynolds & Botha, 2006). Based on a review of empirical studies, Nielsen, Neergaard, Jensen, Bro, and Guldin (2016) stated that AG is a complex risk factor for prolonged grief disorders, in combination with the caregiver’s perceived losses during caregiving, their relation to the patient, and the caregiver’s attachment style, coping mechanisms, and emotion regulation. This definition recognizes the multidimensionality of the phenomenon, but further research is needed regarding its underlying mechanisms.
In a previous scoping review (Coelho, de Brito, & Barbosa, 2018), we concluded that the anticipation of death at the terminal phase of illness may be the distinctive aspect of AG that encompasses several progressive functional and relational losses in the pre-death grief manifestation continuum. Other aspects, such as separation anxiety and avoidance, were also highlighted as nuclear characteristics of AG. However, most literature is focused on the FCs of patients with dementia (e.g., Blandin & Pepin, 2017; Liew, 2016; Shuter, Beattie, & Edwards, 2014; Sikes & Hall, 2017). Compared with dementia patients, the death trajectory of cancer patients is characterized by a more abrupt functional decline (Teno, Witzen, Fennel & Mor, 2001), which may influence the FC experience. For example, Sanderson et al. (2013) stated that dealing with terminal cancer exposes the caregiver to very shocking images, which can be registered as traumatic memories, resulting in feelings of powerlessness. Therefore, we intend to qualitatively explore the experience of the FCs of patients with terminal cancer to identify the core characteristics and specific adaptive challenges posed by AG in the context of end-of-life caregiving.
Methods
Participant Selection and Study Procedures
Relatives of adult cancer patients accompanied by an outpatient palliative care service were approached by the resident psychologist (the first author) at the first consultation (from October 2015 to October 2016) and were invited to participate in a larger study, involving quantitative and qualitative data. Inclusion criteria were (a) being an adult caregiver (over 18 years old) and (b) being directly involved in the patient care. Those who agreed to participate in an interview gave their informed consent and were recruited to this study. Participants were mostly people with high levels of psychological distress related to the advanced illness, who simultaneously accepted a psychology consultation, so we consider that this is a clinical sample.
The interviews took place in the palliative care unit and were scheduled according to the availability of the participants; they were conducted by a trained psychologist with experience interviewing the bereaved population in clinical practice and for research purposes. For ethical reasons, taking into account the sensitive nature of the theme, the interviews were conducted individually, with full respect to the subjects’ emotional state, specific concerns, and personal rhythm. The interviews were transcribed verbatim in Portuguese. This research was approved by the Ethical Committee of the Hospital.
Data Collection
Data were collected through in-depth semi-structured interviews over a period of 12 months. The average duration of interviews was 60 min (range: 35–120 min). The interview script included the following main topics: (a) perceived experience and circumstances of caregiving (e.g., “How has your experience been as a caregiver for your relative?,” “What, in your opinion, has been the most difficult aspect?,” and “How do you handle it?”); (b) perceived evolution of the disease (e.g., “How do you see the current state of your family member’s illness?” and “What do you think might happen next?”); (c) perceived changes in the caregiver’s personal life and in the relationship with the patient (e.g., “How has this illness changed your life?” and “What changes do you notice in your relationship with your relative?”). Initial answers were probed for more details (e.g., “Can you tell me more about this?” and “Could you give me an example?”). Particularly difficult issues, such as the proximity of death, were not directly questioned unless they were introduced by the participant. In these cases, the interviewer asked about the emotional impact of this experience (e.g., “How do you feel about the death of your relative?”).
Data Analysis
Analysis of the interviews was conducted by one coder and two consultants. 1 According to suggestions from Levitt (2015), the interviewer is the researcher, who has a closer connection to the data and is able to recognize other meanings that may be hidden when only transcripts are used, thus allowing an analysis that is highly consistent with the participants’ experiences. A qualitative thematic analysis was conducted to capture recurrent patterns (themes) and implicit meanings using mixed inductive (i.e., derived from the data) and deductive generated coding (i.e., theoretical-based constructs). The process was guided by guidelines from Braun and Clarke (2006) that include the following six steps: (a) familiarization with the data: repeated readings of the interviews, searching for meanings, and noting initial ideas; (b) generation of initial coding: systematically coding interesting features of the data (semantic or latent content); (c) searching for themes: gathering codes into a hierarchical category system and then looking for potential themes, a higher level concept; (d) reviewing themes: checking the coherence of the pattern at the level of the coded data extracts and, then, in the entire data set; (e) defining and naming the themes: identifying the specificity of each theme; and (f) producing the report: beyond description, this implies interpreting the data and making an argument in relation to the research question. Data saturation was achieved when new data were no longer attained. To establish validity, the coder and the two consultants analyzed the data openly and discussed and resolved inconsistencies. Qualitative data analysis was assisted by the computer software NVivo 12.
Results
Participant Characterization
The sample was composed of 26 participants, mostly female (n = 23), aged 27 to 78 (median: 55.5), and the majority were adult children (n = 14) or spouses (n = 10); the remaining participants were a parent and an aunt. The levels of education among the participants were 4 years (n = 1), 6 years (n = 4), 9 years (n = 5), secondary (9), and graduate (6). Over half of the participants (n = 14) cohabited with the patient at the time of the interview.
Findings
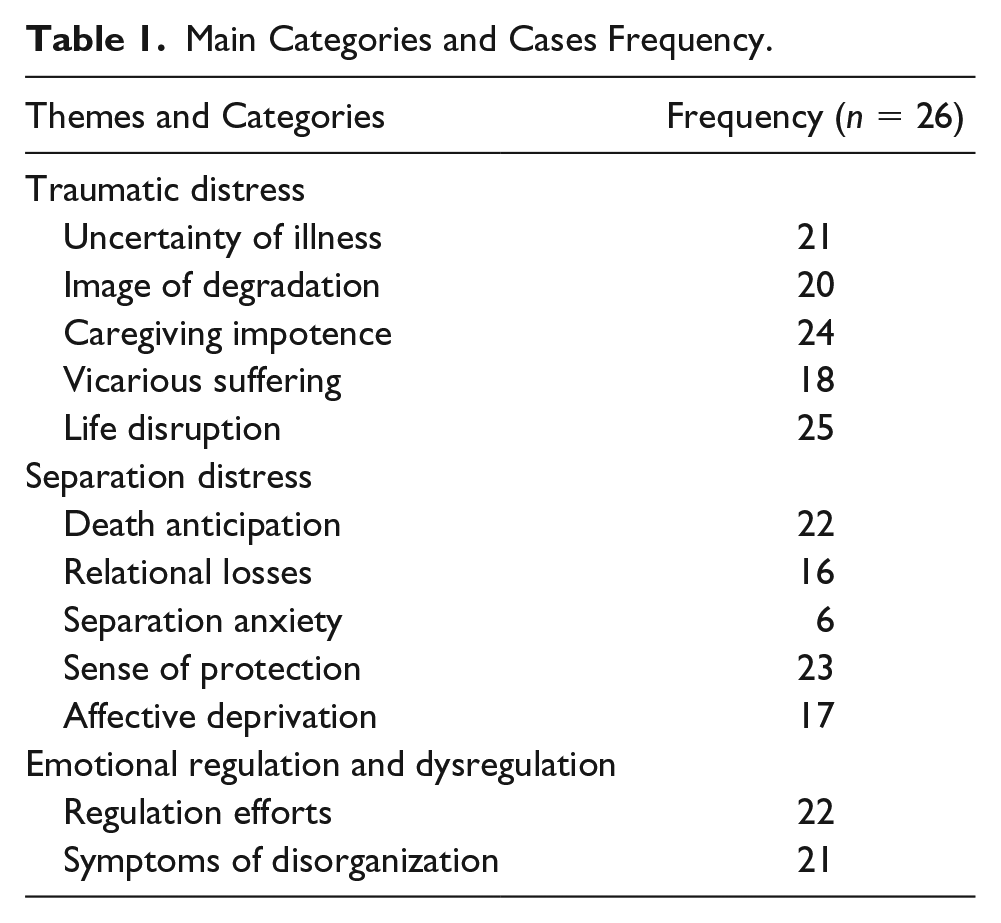
During thematic analysis, references were coded and organized into three main themes: (a) Traumatic distress, (b) Separation distress, and (c) Emotional regulation and dysregulation. A summary of the main themes and categories, along with the frequency of cases, is displayed in Table 1. Subcategory frequency is presented in brackets throughout the findings section. Next, themes are described in terms of commonalities and variances. Commonalities include the circumstances and/or manifestations described by most participants. Variances represent the range of individual responses to stress. Participant quotes are used to illustrate the meaning attributed by the FC. However, some results emerged through implicit meanings and, thus, are difficult to capture by a single reference.
Main Categories and Cases Frequency.
Traumatic Distress
Uncertainty of illness
Most FCs (21/26) emphasized difficulty in dealing with the uncertainty of the illness, related to the unpredictability and ambiguity of events, in terms of the onset of illness, the course of symptoms, and their cause: “It is a pain that suddenly appears, coming from nothing . . .” FCs were frequently plagued by doubts and a generalized preoccupation with the uncertainty of the future: “The future, which is uncertain. The unknown.” In response to uncertainty, several participants (11) showed an attitude of hypervigilance toward the illness signs, mainly after crisis episodes: “Every day, in the morning, I looked at his eyes to see if they were yellow again.” When the cancer diagnosis was particularly sudden and unexpected (2), this especially caused a general sense of insecurity and hopelessness. In contrast, for others (10), uncertainty allowed them to postpone the threat and keep hoping for a small recovery or the prolongation of life: “We do not know what will happen next. He has always recovered after coming to the hospital. I’m always holding on to this hope.”
Image of degradation
The majority of FCs (20) mentioned the patient’s progressive decline, referring to their extreme thinness and frailty, loss of autonomy, and cognitive impairments: “I feel like my husband is disappearing.”; “Things are not well . . . she is losing her abilities and becoming a child.” All these losses contribute to the creation of an image of degradation that contrasts with the previous representation of the now ill person. Despite being informed about the illness progression, this confrontation with extreme fragility causes strangeness and insecurity: “. . . because everything is happening . . . strange things . . . no matter how much we read and know . . . I do not feel prepared for these situations . . .” Indeed, in some cases (6), it provoked a shock reaction, described as traumatic: “So fragile, a person who was so strong (cries)! So strong! . . . It’s very traumatic!.” This reaction was generally triggered by the fact that the decline is very pronounced and sudden: “What strikes me the most is the degradation of the person, so fast, from one day to the next.”
Vicarious suffering
Most FCs (18) identified manifestations of patient suffering and were able to empathize with the other’s emotional state. However, the continuous exposure to the other’s suffering also caused the FCs psychological distress, which sometimes (6) became overwhelming, particularly in cases of identification and emotional contagion: “The worst thing is . . . my great terror is to see the state of my father, the suffering of my father, to imagine what my father thinks . . .” However, there were also participants (3) for whom continuous exposure to the other’s suffering gave rise to a state of habituation and desensitization: My neighbour said that she could not see it; she was really upset. My sister-in-law was also crying a lot . . . but not me . . . I know it was painful for me, but I’ve seen it so many times . . .
Caregiver impotence
As the disease progressed, the patient’s suffering became more difficult to manage, leading most FCs (24) to experience feelings of impotence, either in preventing the other’s suffering or in keeping the disease from progressing. Some (12) focused on external causes, such as professional faults or a lack of social support. Other participants (4) complained about the patient’s refusal behavior in cooperating with caregiving. However, limitations were also perceived as failure in helping the patient (16): “I feel incapable. I cannot get him to react.” In an attempt to compensate for these limitations, some participants invested obstinately in caregiving. They avoided asking for help and tried to always be present and available for the patient, thus becoming more vulnerable to exhaustion. In contrast, for another group of FCs (7), feelings of impotence facilitated the awareness of caregiving difficulties and their need for help. In addition, by recognizing their inability to control the course of the disease, they tended to focus on providing comfort to the patient not to feel so helpless before the inexorable advance of the disease.
Life disruption
Many FCs felt that their own life had been invaded and indefinitely interrupted by the illness. For example, most participants gave up work, leisure time, and other pleasurable activities: “Now it’s just my mother, home, and job. This is my life. Because I do not have time.” They claimed that providing care was a grueling schedule, depriving them of all strength and vitality: “Having to give this energy, we run out of strength . . .” Pressure to provide care and excessive demands are associated with a generalized sense of physical and/or emotional exhaustion (18): “It’s all happening at the same time. I’m getting tired, very tired.” In particular, sleep deprivation substantially contributes to this sense of resource depletion, converting emotional exhaustion into physical fatigue. FCs reported that they feel invaded and that their life is suspended. In addition, caregiving also affects family and social relations, contributing to the isolation of the caregiver. For example, one participant stated that because she provides care, she has neglected her marital relationship. However, these personal restrictions also led FCs to recognize the need to request and accept support (8): “I had to ask them for help, otherwise I would not be able to bear all this.”
Separation Distress
Anticipation of death
The possibility of death was mostly (22) addressed in an implicit way by recognizing the irreversibility of the disease. However, FCs (6) described situations of imminent death and the constant threat of losing their relative: “I was really disoriented! I thought: ‘and if he dies here, what do I do?’” and “It’s a fear . . . I’m afraid he’ll die, I’m always seeing if he’s still breathing . . .” Of those who spoke about the proximity of death (11), almost half (5) stated they were not prepared for it. However, FCs (5) also expressed a desire to hasten death: “I swear, I’ll never have the courage to say this to anyone else, but I just wanted my dad to die fast, not realizing what was happening.” Consequently, the possibility of death was felt with much ambivalence: Although it represented definitive separation from the loved one, it is the only way to terminate the other’s suffering, as well as their own distress: “Sometimes I think: this is not forever. In addition, then I think: but I’m talking about the life of a person I love. If this is not forever, it’s because I’m going to lose that person.”
Relational losses
Several FCs perceived changes in the relationship that affected their sense of attachment to the ill relative, eliciting feelings of grief and longing. The majority (8) referred to the loss of dialogue and presence: “I feel alone, now that I do not have anyone to talk to . . . to [patient’s name], I cannot tell anything . . .” and “I miss his company.” Others mentioned they were losing protection (3), especially when there is a reversal of roles, as in the case of the father–daughter relationship: “Now, I have to be the one to help him. The strong man, to whom I have so often asked for help: ‘Daddy, help me, something happened in my life’. Now I cannot do it anymore . . .” They also expressed sorrow for past life (4) and for the future that they will not share with the patient (3).
Separation anxiety
A few FCs (6) openly showed signs of distress related to anticipated separation. However, most participants were preoccupied by the idea that something bad would happen to the patient when they are not present. This feeling contributed to maintaining the relationship, despite the changes it had undergone. However, this feeling can also be an impediment to the subject’s sense of security and autonomy, which was reflected in a fear of being alone (3): “It scares me because I do not like being alone. I never liked it . . . just thinking that one day I’ll be alone, and I do not have anyone to take care of me . . . it scares me.” Others (2) could not even think of their family member’s future absence and immediately deviated from the subject.
Sense of protection
Most FCs (22) expressed a desire to help by meeting the other’s needs. The responsibility that comes with caregiving involves making decisions for the well-being of the patient, which can give rise to moral dilemmas (15). For example, FCs must decide whether to ask for another medical opinion, whether to invest in more treatments, and which is the best place for care. Retrospectively, these doubts are subject to rumination: “At the time, it seemed that this was the solution . . . But now, I do not know . . . as things are getting worse, it comes back to my memory to wonder if it was the best decision.” The excessive responsibility for the other gives rise to overprotective attitudes. In some cases (3), participants impose their decision in an authoritarian way, sometimes infantilizing the patient. Overprotection may also be the source of closed communication (16). FCs inhibited their expression of emotions and avoided talking about illness and death to prevent the significant other from suffering (3): “I am always afraid that they will give her the news as they gave me. In the appointments, I always say: ‘Oh, beware, she does not know anything . . .’.”
Affective deprivation
Many FCs (17) did not feel appreciated for their efforts, so they felt a great sense of affective deprivation due to the disparity between what they were giving and what they received. This uncovers the FC’s relational needs, leading them to review previous failures in the relationship (14): “My husband was a very selfish person. He only thought about himself and did not give me the affection I needed.” FCs also expected that, at this stage, there would be more contact and affection, and when it did not occur, they felt frustrated (2): “I would like that, at the end of life, she would think: ‘I’m here for a short time, I’m going to dedicate myself to others.’ But this is not happening. She is still angry and complaining with me.” Others (3) continued longing for an idealized relationship: “I wish she would look at me, and we could both create that bond, only for a moment. I just wanted to feel it (cries).” In contrast, some participants (4) reported that now the patient showed more caring and concern than ever before.
Emotional Regulation and Dysregulation
Self-regulation efforts
Several caregivers (14) shared the belief that by inhibiting their feelings, they were protecting each other from emotional distress. Hence, they tended to cover up the painful aspects of their experience: “I’d rather shut up, so I would not hurt anyone.” However, many of them (10) were aware of the need to set boundaries and find some way to compensate for the emotional and physical burnout of caring for their relative. In an effort to self-regulate, some participants (5) tried to distract themselves with work. Others (2) sought relief by walking in nature, by practising meditation, or by connecting with God. There were also those who used cognitive strategies of self-reassurance (4): “I’m going to get hurt, with scars, but life goes on . . . I am strong, I will survive.” Finally, some sought help from family and friends for distraction and instrumental aid (3), but rarely for emotional support, because they were convinced that the others were not available for sharing painful feelings.
Symptoms of disorganization
The AG experience elicits some degree of emotional dysregulation (21). Manifestations include mood instability, impatience and irritability, anxiety, anguish and panic, as well as other signs of acute stress. Physical signs (8) included appetite and digestive changes, tachycardia, and muscle tension. Cognitive manifestations (12) comprise intrusive and ruminative thoughts, recurrent dreams, dissociative experiences, and disorganization of speech. The devastating impact of the other’s illness was also reflected in feelings of abandonment, helplessness, and loss of faith and purpose in life (3), leading one participant to suicidal ideations. Some of these individuals felt unable to manage their emotional state and had a fear of losing control: “I am afraid, I don’t want to fall . . .” Social and occupational difficulties manifested in a disorganization of habits, generalized distrust of others, and isolation for self-protection.
The main themes and categories were organized in a conceptual map that shows the dynamic relationship between the concepts (Figure 1).
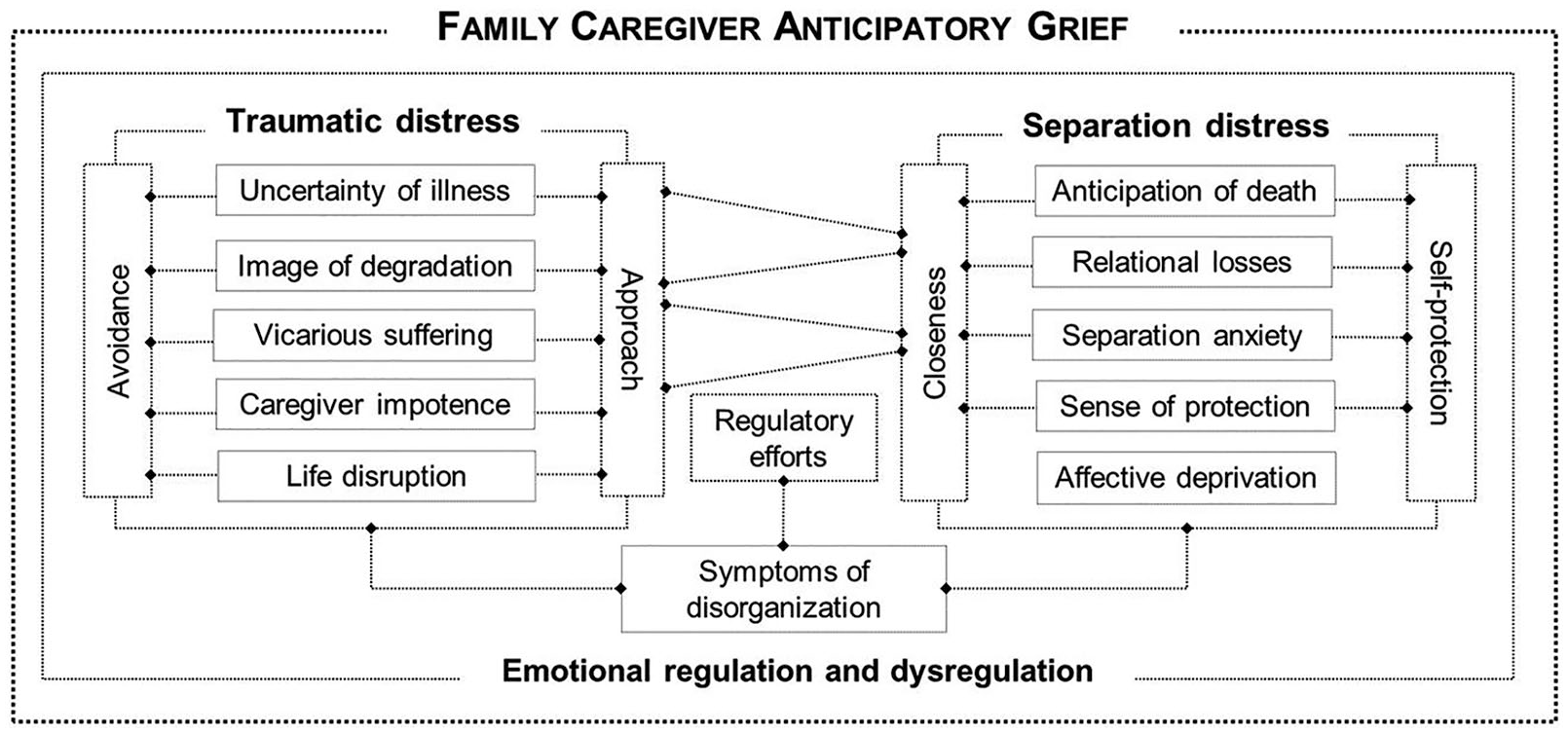
Conceptual map configuring the FC AG core characteristics and their relationships.
Discussion
This exploratory descriptive study aimed to contribute to the conceptualization of AG by qualitatively analyzing the testimony of a clinical sample of cancer FCs of patients in PC. The findings suggest that this phenomenon involves several core characteristics that were grouped into two main dimensions. First, traumatic distress is related to continuous exposure to life-threatening conditions, resulting in a generalized sense of having a lack of control over illness circumstances and one’s own life. Second, separation distress, elicited by the perceived threat to the relationship, stems from the current relational losses and unavoidable future separation. A third dimension, emotional regulation and dysregulation, is not a specific attribute of the AG process, but as evidenced in other studies (Camacho, Pérez-Nieto, & Gordillo, 2018; Fernández-Alcántara et al., 2016), it has a central role as a moderator of grief.
Emotional regulation refers to an individual’s efforts to manage the experience and one’s expression of emotions to achieve one’s personal goals (Gross & Thompson, 2007). In contrast, emotional dysregulation reflects difficulties in modulating emotions, either by underregulation (insufficient control) or misregulation (ineffective control) (Tice & Bratslavsky, 2000). Emotional dysregulation is reflected, for example, in emotional ambivalence, that is, conflict about whether to express feelings that may also lead to ambivalent feelings (Gohm & Clore, 2000). As suggested by the data, FCs’ tendency to inhibit their feelings contributes to emotional ambivalence and disorganization symptoms. However, we argue that this conflict arises from the very circumstances of end-of-life caregiving. In other words, the FC is required to address the threat of death and separation while protecting the patient’s life and welfare. Balancing these apparently competing positions constitutes, in our view, the major dilemma the FC has to deal with, from which many other adaptive challenges derive.
The perspective of grief as an oscillatory process is well documented in the literature. This idea has hallmarks of the dual process model of coping with bereavement (Schut, 1999), which establishes a regulatory coping process of oscillating between approach and restoration positions. Specifically, in AG phenomena, Rando (1986) described a delicate balance between mutually conflicting demands of simultaneously holding onto and letting go of the patient. Recently, Breen, Aoun, O’Connor, Howting, and Halkett (2018) also drew attention to this vacillation process, emphasizing that FCs either focus on circumstances of illness and caregiving (here) or preparation for the future (after). In line with these perspectives, we articulated the circumstances and relational aspects, stating that the AG oscillation process occurs both between and within two different levels: managing the perceived threat to the other’s life and that to the relationship. As a result, we propose a conceptual model that identifies the AG core characteristics and configures them as adaptive challenges that require constant balance between two competing positions.
Traumatic Distress: Managing the Threat to the Other’s Life
Caregiving in life-threatening conditions exposes FCs to several unexpected and threatening events, causing traumatic distress. In accordance with Roth and Cohen (1986), we understand that FC responses to perceived threats to the other’s life correspond to the dynamic organization of defensive behaviors when facing an inevitable threat, involving an approach and avoidance pattern. An avoidance orientation protects the individual from anxiety-arousing stimuli and their consequences. An approach orientation, in contrast, allows for appropriate action by noticing the threat stimuli and making it more controllable.
One of the aspects that threatens the individual’s sense of security is the uncertainty of illness, which is caused by the unpredictability of events and the consequent lack of control over illness circumstances (Shilling, Starkings, Jenkins, & Fallowfield, 2017; Strauss, Kitt-Lewis, & Amory, 2019). This generalized sense of insecurity may develop into a permanent state of hypervigilance and may lead to a heightened startle reaction (Brosschot et al., 2018). However, similar to other studies (Janze & Henriksson, 2014; Wong, Liamputtong, Koch, & Rawson, 2017), we found that uncertainty is also related to hope in that it allows the threat to be postponed. Hence, in the face of uncertainty, the FC is challenged with balancing vigilance regarding the illness signs, while still holding on to hope.
As the illness progresses, major changes in behavior and extensive body deterioration may lead the FC to feel that they no longer recognize the terminally ill relative (Dumont, Dumont, & Mongeau, 2008). This experience, evoked by the patient’s functional decline, was designated as the image of degradation. The sharp contrast with the previous representation of the relative provokes reactions of shock and strangeness and is, thus, a main factor that impacts the psychological well-being of the caregiver (Schumacher, Dodd, & Paul, 1993). In addition, many of these functional losses are ambiguous, because the changes fluctuate and are unclear (van Wijngaarden, van der Wedden, Henning, Komen, & The, 2018). Consequently, the FC is challenged to review the previous image of the patient, integrating fragility, while trying to preserve the inner representation.
Witnessing the other’s degradation and inherent suffering evokes in the FC an experience of vicarious suffering; this feeling corresponds to affective empathy, defined as sharing or feeling another person’s emotional state (i.e., “feeling what another person feels”), which is associated, by excess or by fault, to increased emotional distress (Jutten, Mark & Sitskoorn, 2019). The state of compassion fatigue is characterized by physical, psychological, and social exhaustion that reduces one’s ability to and interest in enduring suffering and caring for the other (Lynch & Lobo, 2012). To balance the emotional costs of empathy, the FC is challenged to dissociate from the patient’s emotional and physical state, while remaining sensitive to the other’s suffering.
Being exposed to the other’s suffering without being able to prevent it gives rise to caregiver impotence, which reflects a feeling of intense powerlessness and frustration (Sanderson et al., 2013). Difficulties may be attributed to external factors (i.e., lack of support) or internal factors (i.e., personal faults). The latter seems to have a more devastating effect on the caregiver’s sense of self-efficacy. Notably, caregiver impotence also led FCs to reformulate expectations and recognize their inability to reverse the situation and stop death from happening. Thus, the challenge consists of balancing the acknowledgment of the limits of caregiving, while maintaining some sense of control.
As a result of their exclusive dedication to the terminally ill patient, FCs experimented with personal constraints, creating a sense of life disruption. When the demands become excessive and the resources become depleted (e.g., deprivation of pleasurable moments), this situation gives rise to a state of emotional and physical exhaustion, with several implications in the FC’s physical and mental health (Schubart, Kinzie, & Farace, 2008; Sharpe, Butow, Smith, McConnell, & Clarke, 2005). Although some FCs avoid recognizing the devastating impact of caregiving to prevent the patient from feeling a burden, this mind-set also challenges the FC to recognize their limits and to mobilize resources.
Separation Distress: Managing the Threat to the Relationship
As a consequence of the functional decline of the patient and the disruption of life, the FC experiences changes in their sense of connectedness with to patient, which threatens the security of the attachment and/or reactivated thoughts of previous relational failures. In addition, the proximity of death represents the last and most important threat, leading the FC to anticipate the inevitable loss. As a way of regulating the risk to the relationship, FCs are prone to seek proximity or to withdraw from the other for self-protection against feelings of rejection and loss (Murray, Holmes, & Collins, 2006). Shifts in motivation for seeking or avoiding contact seem to be related to ambivalent feelings, which are prevalent in close relationships at the end-of-life caregiving (Reblin et al., 2016). In fact, several aspects are likely to generate ambivalence in this relational context.
First, the anticipation of death, defined as an awareness of the proximity of the other’s death. In addition to being an ancestral fear that is biologically sustained and responsible for the survival response, individuals are imbued with implicit and explicit emotional representations that are influenced by sociocultural attitudes and beliefs, which contribute to death anxiety (Panksepp, 1998). Thus, despite recognizing the irreversibility of the illness, many participants could not mention the proximity of death. However, death was also anticipated as a way of escaping from suffering and the burden of caregiving. Hence, the FC is challenged to assume the inevitability of death, despite not wanting the separation.
Another aspect that creates ambivalence is grieving the loss of the relationship while the significant other is still physically present. According to other studies (Beng et al., 2013; Pusa, Persson, & Sundin, 2012), we found that the feeling of loss exists even before the patient’s death. Relational losses include, for example, missing the patient’s company and protection, their previous life together, and their unlived future. This contributes to a sense of being disconnected from the patient, which is perceived as a sign of distance and as a rupture in the relationship. Therefore, to keep affectively investing in the significant other, the FC is challenged to relinquish some aspects of the relationship, despite their wishes to preserve or even strengthen the connection with the patient.
As a consequence of this disruption in contact, both the patient and FC experience intense solitude. Loneliness was found to be correlated with anxiety in caregivers of patients in the terminal stage of cancer (Soylu, Ozaslan, Karaca, & Ozkan, 2016). Separation anxiety is manifested mainly in the FC’s reluctance to move away from the patient. There are two main reasons for that: First, because the FC is afraid that something bad will happen to the patient in their absence, they have to be present to ensure the patient’s safety; and second, because they are aware that they do not have much more time to be near the ill relative, they want to enjoy all the time they have together. Thus, the challenge consists of valuing the other’s presence, while maintaining one’s autonomy.
The need to ensure the patient’s safety corresponds to the sense of protection. As noted by Martz and Morse (2017), FCs are prone to feel guilty in the transition to end-of-life care, so they mitigate this feeling by being present and ensuring that the patient is peaceful. This feeling translates into an attitude of “protective buffering” (Langer, Rudd, & Syrjala, 2007) from all the sources of distress and internally from their own feelings, leading to chronic emotional inhibition and the avoidance of painful subjects related to illness and death. The challenge lies in balancing protecting the other and attending to one’s own needs.
Due to a lack of reciprocity in the caregiver relationship, the FC is prone to experience affective deprivation. In addition, this feeling can uncover previous relational failures and the loss of expectations of affection, thus contributing to a generalized sense of dissatisfaction that adds ambivalence to the relationship. As noted by Harding and Higginson (2001), caregiver ambivalence reflects difficulties in making decisions toward their unmet needs. Thus, to preserve the relationship, FCs are reluctant to address pending issues, so they tend to suppress relational needs that should be expressed.
Conceptualization of AG in the FC
A clear and comprehensive definition of AG is difficult to achieve, mainly due to the multidimensionality and complexity of this experience. However, based on these results, we propose that FC AG is defined as the family response to the perceived threat to the other’s life and the subsequent anticipation of loss in the context of the end-of-life caregiving relationship.
Clinical Implications
For most FCs, despite being emotionally intense, this feeling is part of the adjustment process of advanced illness. It is important to keep in mind that under conditions of an ongoing, real threat, emergency reactions, including avoidance and hyperarousal, can be understood as natural, protective, and adaptive responses (Diamond, Lipsitz, & Hoffman, 2013). However, due to the accumulative effect of incidents, some people may feel that the circumstances are unbearable, resulting in a sense of overwhelming distress and symptoms of emotional disorganization. These feelings correspond to a failure in enduring, that is, the innate capacity of getting through a life crisis (Morse & Penrod, 1999). Psychological intervention programs directed at this population should identify the main challenges the FC is struggling with to promote the clarification of dilemmas and to develop specific strategies for supporting emotional regulation and preventing symptoms of emotional disorganization.
Limitations and Future Research
There are some limitations to this study. First, recruitment was conducted by the resident psychologist of the palliative care team, which means that the people who agreed to participate in the study were those who were open to psychological consultation, which is mainly a clinical population. Therefore, we probably did not capture the experiences of those who consider themselves to be more adjusted to such situations. Second, the characteristics of the sample, especially the high academic level, are not representative of the general population of caregivers. Future research is needed to investigate the role of emotional regulation in explaining individual differences in dealing with AG challenges and their impact on subsequent bereavement. Likewise, it is important to verify the relationship between each of AG dimensions in preparedness for death and the subsequent adjustment to the loss. This analysis should be extended to the nonclinical population to identify patterns of adjustment and their deviations. Finally, we suggest that mixed-method research be used to verify and develop the results obtained in this study.
Conclusion
Taken together, findings from this exploratory study provide an in-depth description of FC AG core characteristics that go beyond the mere identification of grief symptoms, contributing to the expanded comprehension of grief’s multidimensional and dynamic nature. For most participants, caring for a terminally ill relative is considered a very disturbing experience, requiring much emotional regulation effort to manage both the threatening circumstances of end-of-life caregiving and the anticipated loss. By inhibiting their own feelings of distress to protect the significant other, FCs are generating ambivalent feelings that hinder the readjustment of the relationship. However, the balance between these two positions (i.e., anticipating loss, while protecting the other) also challenges the FC to adjust to the reality of imminent loss. The results may inform clinicians in creating intervention programs focused on the identification and management of these specific challenges posed by AG in the context of end-of-life caregiving.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.