
Abstract
Low-income U.S. patients with co-occurring behavioral and physical health conditions often struggle to obtain high-quality health care. The health and sociocultural resources of such “complex” patients are misaligned with expectations in most medical settings, which ask patients to mobilize forms of these assets common among healthier and wealthier populations. Thus, complex patients encounter barriers to engagement with their health behaviors and health care providers, resulting in poor outcomes. But this outcome is not inevitable. This study uses in-depth interviews with two interprofessional primary care teams and surveys of all six teams in a complex patient program to examine strategies for improving patient engagement. Five primary care team strategies are identified. While team member burnout was a common byproduct, professional support offered by the team structure reduced this effect. Team perspectives offer insight into mechanisms of improvement and the professional burdens and benefits of efforts to counter health care marginalization among complex patients.
Keywords
Introduction
Health systems struggle to provide effective care for “complex” patients who have overlapping behavioral, physical, and socioeconomic problems. The global burden of disease attributable to behavioral issues, specifically mental and substance use disorders, accounts for 7.4% of disability-adjusted life years and are the leading cause of years lived with disabilities (Whiteford et al., 2013). Poverty is associated with higher prevalence of co-occurring physical and behavioral health conditions, and greater illness severity for both types of conditions in the United States (Cunningham et al., 2018). Such outcomes are at least in part due to complex patients struggling to receive adequate care in the complicated and expensive U.S. health sector that largely rewards patients with higher socioeconomic status and better health (Shim, 2010). Complex patients experience problems with affording care (Cunningham et al., 2018), maintaining consistent relationships with primary care, and navigating the intersection of multiple forms of marginalization that affect health behaviors and health care access (Fleming et al., 2017; Komaromy et al., 2018). New efforts have emerged, however, that seek to encourage complex patients (who are often pejoratively labeled “super-utilizers” due to above-average use of expensive emergency department services) to engage with primary care to improve quality and decrease costs. Extensive research shows how health care teams function in contexts including palliative care and general internal medicine wards (e.g., Conn et al., 2009; Goldsmith et al., 2010; Martin et al., 2008; Propp et al., 2010), but little is known about the experiences of primary care teams working exclusively in complex patient programs. Team perspectives can offer insight into mechanisms of improvement and the professional burdens and benefits of efforts to counter health care marginalization among complex patients.
Primary care interventions for complex patients frequently utilize interprofessional teams to address the costs and quality of ambulatory care (Bodenheimer & Berry-Millett, 2009; Grinberg et al., 2016). Teams can offer a holistic focus on patient care by drawing on the skills of multiple health professions including community health workers (CHWs), primary care providers, and nurses. Interprofessional teams demonstrate improved health service outcomes, such as reduced emergency room use and hospitalizations (Bodenheimer & Berry-Millett, 2009; Gaglioti et al., 2017; Yaggy et al., 2006), increased outpatient mental health and primary care use (Gaglioti et al., 2017), and reduced health care costs (Hardin et al., 2017). There is growing evidence that interprofessional teams also contribute to improvement in some health service elements of complex patient “engagement” in care. While patient engagement has multiple definitions, it generally entails three patient attributes: cultivating motivation and ability to address health issues (health literacy), working with health care providers (shared decision making), and participating in improving care and health outcomes (quality improvement) (Coulter, 2012). Research consistently links low-income patients to low engagement (Greene & Hibbard, 2012), which is worrisome, given evidence of significant relationships between measures of engagement (e.g., the Patient Activation Measure) and both health behaviors like tobacco use and health outcomes like depression severity (Greene et al., 2015; Greene & Hibbard, 2012).
Given the adverse health and social forces affecting complex patients, it is noteworthy that interprofessional teams are able to improve elements of patient engagement related to health services. But the professional behaviors and experiences underlying these improvements remain largely unexplored. The few reports examining perspectives of interprofessional team members on the care, engagement, and social needs of patients are confined to specific disease settings and are largely conducted outside of the United States. (e.g., Loeliger et al., 2016; Suri et al., 2007).
This research draws on triangulation between surveys and in-depth qualitative interviews with U.S. primary care teams working in a Project Extension for Community Healthcare Outcomes (ECHO) program called ECHO Care, which exclusively serves complex patients, to understand the team strategies underlying improved patient engagement. The professional insights from this research also offer opportunities for enhancing training and support of interprofessional teams by exploring the challenges and liabilities associated with engagement promotion that may be mitigated in future interventions.
Background: Intervention
This study takes place in the context of ECHO Care, which is a team-based approach to primary care delivery for patients with complex medical, behavioral, and social needs. The ECHO Care model builds on two key strategies: (a) interprofessional Outpatient Intensivist Teams (OITs) providing intensive ambulatory care and (b) teams participation in the “Complex Care ECHO Program” that provided weekly teaching and consultation for the OITs with a panel of disease specialists (including addiction, chronic pain, psychiatry, pharmacy, counseling, CHWs, and various subspecialties in internal medicine). The specialists and the OITs came together via simultaneous video-conferencing for 2 hours weekly and developed integrated care plans for the most complex and challenging patients cared for by the OITs (for more on the ECHO Care intervention and ECHO Model see Komaromy et al., 2016, 2018).
Six OITs were established in primary care clinics across New Mexico. OITs included a nurse practitioner (NP) or physician assistant (PA), a nurse, two CHWs, and administrative support. Two of the teams also included a counselor or social worker. The six OITs provided comprehensive primary care and support for a combined total of 770 patients between 2013 and 2016 and provided care exclusively for ECHO Care patients. Patient eligibility criteria include Medicaid enrollment, having at least two chronic health conditions, and either two or more hospitalizations in the previous year, with one in the past 6 months, or three or more Emergency Department visits in the previous 6 months. Patients had an average of six chronic health conditions. Chronic mental illness and/or substance use disorders were diagnosed in 96% of ECHO Care patients. Upon enrolling in the program, 43% of patients reported needing housing assistance, 90% were unemployed, and 78% reported fair or poor health.
To address the complex social and medical needs of the patient population and facilitate functional team dynamics, OIT members received initial training in team-based care and patient engagement prior to beginning patient care. Ongoing training addressed additional topics in these two areas, as well as training on avoiding burnout (Table 1).
Outpatient Intensivist Team (OIT) training modules.
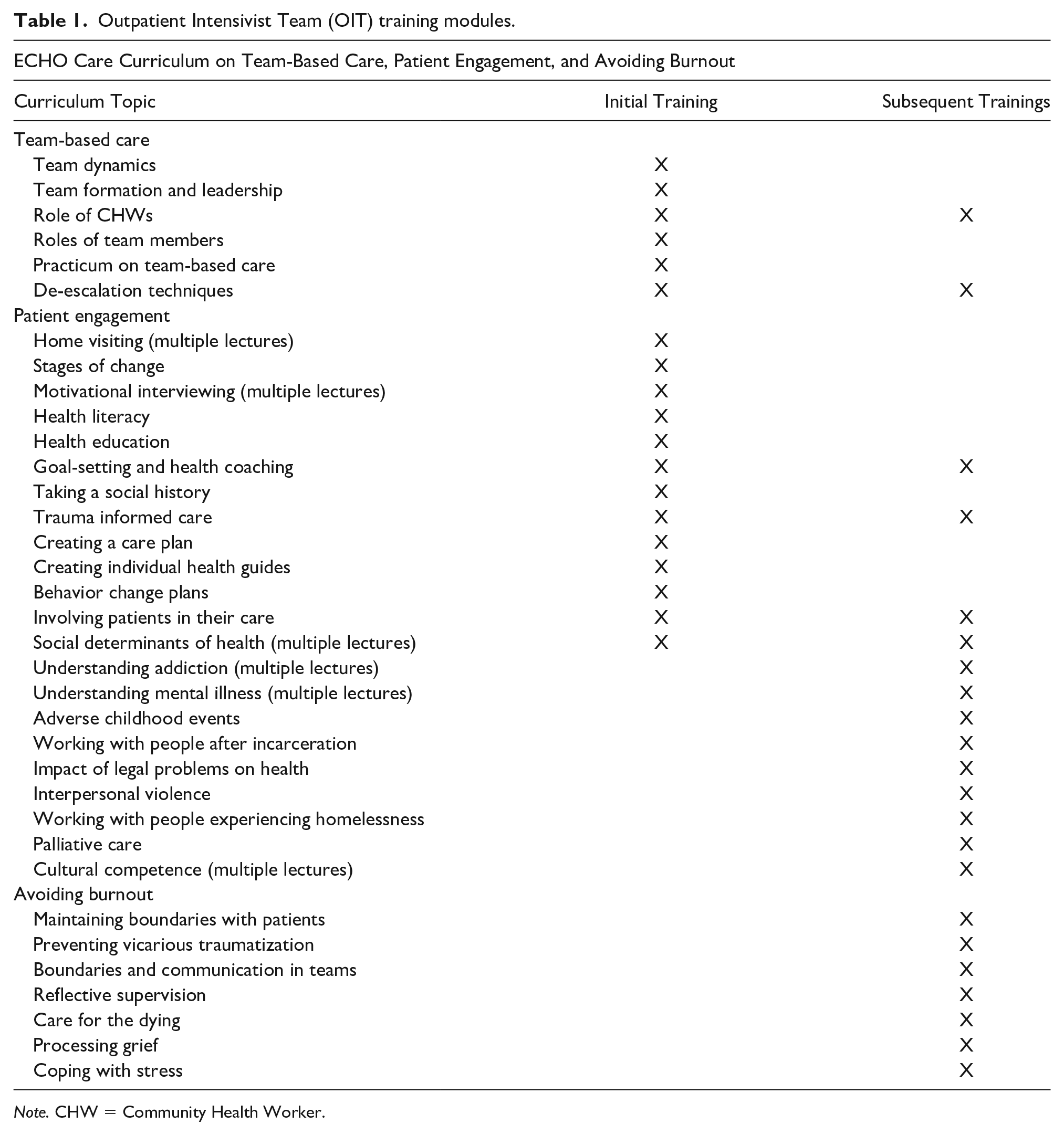
Note. CHW = Community Health Worker.
In ECHO Care, OITs worked closely with each other and with their patients to provide medical and behavioral care as well as address social needs, such as housing and food access. Patients received services both in the clinic and in their homes. Patients had direct phone access to OITs and received intensive services depending on individual needs, including home visits to fill medication boxes, drop-in, and extended time clinic visits, and team member accompaniment to appointments with medical specialists or social services.
Methods
Methodology
Constructivist grounded theory (Charmaz, 2006), a systematic approach to collecting and analyzing qualitative data, guided the research. We chose this methodology to allow an inductive understanding of survey and interview data. We began our research with the broad research question of how patients and primary care teams experienced ECHO Care. The responses of primary care teams, which are the focus of this article, are part of a larger study on how complex patients, patients’ friends and family, and primary care teams negotiated health behaviors and health care within the ECHO Care program (for analysis of patient and contact experiences, see Komaromy et al., 2018).
Data Collection and Analysis
We conducted a survey of all six OIT members and qualitative interviews with members of two OITs over 2015–2016 to understand the perceptions of OITs about providing care for complex patients. Surveys solicited input from all OIT members as a part of ECHO Care program evaluation. OIT staff at all six ECHO Care sites received the survey in January 2015, and new OIT members received the survey in December 2015. Twenty-seven (27/30 = 90%) OIT members responded. Individuals who did not return the survey included two administrative assistants and one CHW. OIT surveys used closed- and open-ended questions to explore team member roles, professional development, and solicited evaluations of the ECHO Care model but did not explicitly focus on patient engagement. Only the open-ended qualitative responses are included in the analysis presented below.
Theoretical sampling was used to select OIT interview participants who could best speak to the functioning and dynamics of the ECHO Care program. Specifically, of the six teams, two teams that were fully staffed to satisfy the program model were selected to participate. The remaining four teams had vacancies at the time of data collection, and thus were not fully implementing the ECHO Care program and were not selected. All team members participated at both sites included in the sample, except for one part-time administrative assistant (n = 9). Participants included four CHWs, one PA, one NP, two registered nurses (RNs), and one administrative assistant. Five participants were from one clinic site, and four were from the second.
Collection and analysis of OIT interview and survey data followed the analysis of in-depth patient interviews, and thus was influenced by the themes identified in patient narratives. The analysis of 20 patient interviews began by the authors and an additional study team member “open coding” several interviews, which entails generating a list of phrases that summarize the meaning and importance of data (Charmaz, 2006). Open codes were then used to examine all potential themes in the patient data. The authors drew upon the diverse multidisciplinary nature of the research team (both medical and social science expertise) to consider a range of interpretations of the patient data, including examining how ECHO Care patients struggle against structural forces of marginalization and considering how the severity of patient conditions also affects health service use and health behaviors. The authors discussed the open codes and “memoed,” or wrote brief analyses of significant and/or frequent codes from the patient data, to sort codes into a “focused code” list that organizes codes into thematic categories. The simultaneous processes of coding, memoing, and collecting data from patients and contacts centered on how ECHO Care affects patient engagement, and this became the focus of the later OIT interviews as well.
In-depth, semistructured interviews with OIT members focused on the theme of patient engagement identified through the analysis of patient interview data. Interviews were used to answer the question, “What primary care team strategies improve patient engagement and how do team members experience this work?” The OIT interview guide was drafted by one team member with a social science background (Erin Madden) and refined by all authors to capture themes salient to both social science and applied health science. Interview guides included questions about professional experiences addressing patient social marginalization, how OIT members define and promote patient engagement, and questions about burnout and fidelity to the ECHO Care model. Erin Madden and an additional study team member conducted interviews, which were held one-on-one with OIT members in their offices and audio recorded. Each interview lasted between 1 and 2 hours and were collected between November 2015 and March 2016. OIT data collection occurred simultaneously with analysis. OIT data collection ceased when the authors agreed theoretical saturation of the major analysis themes was achieved. This entailed interview participants repeating specific strategies for promoting engagement and repetition of the professional burdens and benefits of undertaking such strategies by multiple participants without the addition of new perspectives.
Analysis of transcribed interviews began after the completion of the third OIT interview. Five of the authors participated in this second round of open coding, which produced additions to the existing focused code list generated from patient data. Additional codes expanded upon existing engagement themes by providing conceptual elaboration on what engagement means to primary care professionals, outlining the ways primary care teams solicited and encouraged engagement improvements, and exploring costs and consequences of these team efforts. Focused codes were applied to all OIT interviews as well as OIT open-ended survey responses using NVivo 10 software (2014) by Erin Madden and one study team member, along with concurrent additional memoing. Memos were discussed in coding team meetings and compared with coded excerpts from interviews and with survey responses. Differing interpretations of data that arose during the creation of the focused code list or the review of memos were discussed in coding meetings and decided upon by consensus. This analysis process explored the nature of complex patient engagement from the perspective of primary care teams, as well as team experiences facilitating this engagement process. We compared the in-depth interview findings with OIT survey data to assess the generalizability of these findings to additional primary care teams within the ECHO Care model. The open-ended comments on survey questions included OIT member perceptions of professional challenges and how their work affects patient health behaviors, and thus allow us to reflect on our in-depth interview findings to assess how pervasive the engagement themes are across OITs.
Ethical Considerations
All research was approved by the University of New Mexico Human Research Review Committee, HRRC #12-617. Informed consent was obtained for both surveys and interviews. The surveys and interviews were conducted by individuals not directly involved with ECHO Care’s implementation. These included graduate and undergraduate students, a PhD-level researcher employed outside of ECHO, and a research employee working in a different ECHO program. Participant interview data were re-read for accuracy and de-identified after transcription to maintain confidentiality. Surveys did not collect participant names. All data, including surveys, audio files, and interview transcripts were stored in encrypted password protected servers only accessible to study team members.
Findings
This section explores how OIT members perceive “pre-engagement” characteristics among patients, key features of OIT efforts to address health and social forces marginalizing patients and to improve patient engagement, and insight into liabilities of OIT efforts to promote engagement. The processes explained in this section are also illustrated in Figure 1.

Primary care team strategies for improving engagement among complex patients. Positive relationships between factors indicated by plus signs, and negative relationships indicated by minus signs. Direction of factor relationships indicated by arrows.
Pre-Engagement Traits and Engagement Goals Among Complex Patients
Pre-engagement behaviors are activities patients reported to OITs that are detrimental to health and health care outcomes. OIT members describe these behaviors as common prior to enrollment in ECHO Care. In an interview, a CHW describes patient pre-engagement health care utilization, “they don’t keep their appointments, there’s a lot of no-shows . . . that’s them not being engaged.” Most OITs agree with this in their survey responses, such as an NP saying, “The problem is many have transportation [and] disease-oriented reasons they do not go to clinics, so if you ask them to come to clinic, they no-show.” Another CHW explains pre-engagement patient relationships with health care, “starting off, they’re pretty hesitant, very distrustful of any entity that works with them.”
In addition to health service issues, interviews revealed pre-engagement health behaviors and social conditions, such as OITs describing high frequency of substance use among many patients, “a lot of our guys have substance abuse problems; prior addictions, current addictions.” OITs explain that substance use also combines with other forces of marginalization like poverty to reinforce other pre-engagement traits such as medication nonadherence. One PA explains, “given the choice between medicine and food, they’re going to choose food every time; and usually medicine or heroin? They’re going to choose heroin every time.”
OITs note in both interviews and surveys that once patients are enrolled in ECHO Care, the teams seek to promote “engagement” with care, which is a term explicitly used in several OIT interviews referring to improved patient health care behaviors. This outcome, illustrated on the right side of Figure 1, represents several changes from pre-engagement traits. A CHW explains in an interview, “being engaged means they’re keeping their appointments, or if they can’t make it, they call in and reschedule.” The CHW adds, To go to the emergency room, that’s part of their life for the last—however many years, and that’s where they got whatever they needed. And we think it’s a success when we see just one ER visit over the last six months instead of every week.
Similar comments about improved health service behaviors are noted frequently in surveys. Another CHW lists “intercept[ing] an unnecessary emergency department visit” as a patient engagement goal. Reducing substance use and improving nutrition and diet are also components of engagement noted by OITs. In an interview, a PA describes one patient’s improvements, “We started her on Suboxone to keep her off the opioids. . . . [she’s] five months sober . . . this is probably the longest period of time she’s ever been off of both drugs and alcohol for the past 18 years.” An NP describes another patient during an interview, she’s working out daily on an exercise bike . . . She’s disabled and I don’t think she’s going to get a part-time job anytime soon. But maybe in another 12 months down the road, if she reaches a point where she feels stable enough, she could start thinking about volunteering.
OITs note the intersection of health problems, health behaviors, and other social challenges like unemployment when they describe the difficulties facing their patient population. The next section outlines how health care professionals seek to address these overlapping sources of disadvantage in their efforts to improve patient engagement.
Mechanisms Promoting Engagement Among Complex Patients
OITs discuss several strategies for promoting patient engagement, such as addressing life challenges that hinder patient ability to both improve health behaviors and their use of health services. These strategies are illustrated in Figure 1 as links between patient pre-engagement and improved patient engagement. Each OIT strategy also contributes to engagement by fostering strong emotional connection between the OIT and patients, as described in the following paragraphs.
Interaction availability and social support
OITs explain how allowing patients to call and text with team members, allowing drop-in clinic visits, and long (~1 hour) appointments help to maintain communication with patients. These forms of OIT availability also provide social support to patients. An administrative assistant says in an interview how her job often entails phone conversations with patients who may have medical concerns, or simply want to interact. She says, There’s one patient who I speak with weekly . . . a lot of it is just that she’s so lonely she’ll call and chat and tell me about her neighbor or how she feels or what she watched on TV . . . a lot of these folks are extremely lonely and just need an ear.
Phone calls and in-person extended clinical interactions frequently facilitate improvements in patient quality of life. A CHW explains in an interview, The relationship-building is the biggest part. That’s what’s been able to improve the quality of life for patients with multiple medical issues on top of mental health issues, having that time to spend with them. Not only the time you’re spending with them [in the clinic], but on the phone . . . Sometimes they call every hour, and we’ll talk to them. You’re getting on my nerves, but I’ll still talk to you! . . . They need someone to pay attention to them . . . in a regular medical setting you don’t get to do that.
This CHW also describes how the availability of the team for medical and nonmedical matters helps to improve engagement with an elderly patient with high anxiety and posttraumatic stress disorder (PTSD) and who was initially distrustful of health care, “We just go and hang out with her, we let her show us her apartment. Just spending time with her has been what changed her feeling of need to go to the emergency room.”
An RN explains the importance of allowing OITs and patients flexibility in scheduling, the reason [complex patients] fall through the cracks is because they don’t follow the norms. [Other patients] have an appointment at 10 o’clock and will show up at 9:45. Our guys come in on Friday for their Thursday appointment . . . we work on rolling with it and accepting it and also teaching [patients about maintaining appointments].
Surveys overwhelmingly reflect similar comments, such as a PA commenting, I found most patients really like having [phone and in-person] access to our team, whether it is for illness, urgent situations, or just reassurance. There are some patients that will go to the emergency room because of what they can get there, but most are willing to come to us. Or at least call us first.
OIT interviews and surveys make a direct connection between engagement improvements and their team availability, flexibility, and social support. These patient–team interactions are fostered by both OIT member efforts and the professional latitude allowed to providers in the ECHO Care program.
Addressing material needs
Because complex patients have limited financial and social resources, OITs note significant efforts in applying for and securing material assistance for patients. One PA says in an interview, “Housing is instrumental, and a big part of what OITs do is that extra-medical stuff, outside of the medical realm. That’s because people don’t really participate in their own health if they’re not housed.” A CHW describes assisting a homeless patient, We worked with [that patient’s] case manager to get her set up in a place to live. And to be honest . . . as far as resources and getting stuff done, some things might never happen for these people. So, we helped her by going to a warehouse, and maybe I shouldn’t say this, but we personally moved her furniture so she wouldn’t have to sleep on the floor.
OIT members not only try to foster complex patient engagement with health service efforts, they also seek to address other forms of social marginalization like housing insecurity that make engagement in health care and health-promoting behaviors difficult. Survey comments almost universally noted the importance of tackling social and financial barriers for improving engagement, such as a PA who writes, “I have two individuals [in the OIT] helping patients solve social issues such as housing, food, etc. And this improves the patients’ quality of life, and therefore their health and many times control of their diabetes, etc.”
Nonjudgmental approach
OITs note the importance of maintaining what they call a “nonjudgmental” disposition when working with complex patients. This approach is not simply the absence of judgment, but an actively positive and accepting approach toward patient lives. A CHW explains during an interview, I don’t judge them. I don’t really care what they’ve been convicted of or whether they’re on drugs . . . I just try to talk to them like people and being really open. If I walk in your house, and I’m like, “oh, there’s your cat. Can I pet your cat?” That’s huge. Or finding out their kids’ names, taking a genuine interest in them as a person rather than this thing we need to accomplish, like, “stop drinking, that’s your goal . . .”. Everybody sees them [as] an alcoholic, they have diabetes, they do heroin. But that’s not all of them.
Being nonjudgmental is tied to some of the approaches described above in the interaction availability and social support section. But it is not only that OITs offer interaction opportunities, it is also the disposition of OITs as accepting of what patients share about themselves. Surveys reflect such attitudes across the six OITs. For example, an RN explicitly connects being nonjudgmental to engagement and writes, Most of our patients have burnt a lot of bridges. They learn after time with us that we do not judge, and that we are here for them through the good and bad times. They test us and we show them time and time again that we are on their side. Simply gaining trust in the team allows them to engage more effectively in other aspects of their health care and life.
OIT members acknowledge complex patients have often experienced judgment and exclusion in their previous health care interactions and broader social worlds. OIT members manage their professional dispositions such that patients receive messages of acceptance to build health care relationships that can foster better health outcomes.
Adjusting engagement approaches to patient health literacy and cognitive ability
OITs describe assessing patient capacities and adjusting engagement efforts accordingly. A CHW describes her adjustment process with a patient who entered into the program with cirrhosis from alcohol use, and who was unsure of how to manage the large number of medications he was prescribed by other doctors. She says, [the patient] was really, really sick when we first met him. And helping him [consisted of] figuring out his medications because he had stockpiles. . . . assisting him with filling his pill boxes . . . [he has] really low health literacy. . . . you have to step back and change your diction and your vocabulary a little.
A CHW speaks more generally about this approach, The challenge is when they’re stuck [in their engagement improvement process], whether that’s because of substance abuse, or whether that’s a mental health disorder, that limits their understanding of the situation. That’s where you have to be a lot more patient and really simplify what your expectations are, and slowly build up to a grander goal.
This theme also emerges several times in survey data, such as a CHW explaining that working in an OIT helped him develop a flexible approach to engagement, “[I am now] more empathetic and [have a] better understanding [of] some of our patients.” He adds that he pays more attention to “their life situations, health illiteracy, lack of resources, and [the presence of] a lot of judgments on their lives.” Adjusting vocabulary, providing hands-on assistance with medication management, and calibrating expectations to patient abilities are ways OITs create health care spaces that are tailored to complex patient resources. This provides an environment in which health care expectations are not held to the standards of middle-class healthy patients, and instead new modes of interaction are stablished by OITs that better support complex patients.
Goal-setting
Finally, the process of including patients in defining care goals is a component of engagement improvement identified by OITs. OITs explain that goals are not just an endpoint; goals are also an opportunity to work collaboratively with patients on imagining future health and health care changes.
An RN explains in an interview how organizational contexts can either limit or facilitate collaborative goal-setting, In the ER [where I was previously employed,] the goal is movement, and here our goal is embracing [patients] into becoming partners with us. In the ER, we’re diagnosing and stabilizing and getting them to wherever it is they need to go. And here, we work with them to figure out what they need to improve.
The RN credits the structure of ECHO Care with allowing OITs to spend more time with patients, and thus fostering patient-provider collaboration in setting goals. One CHW explains in a survey response that working in ECHO Care facilitates, “learn[ing] to be more patient with others, meet[ing] patients where they are at, and guid[ing] others at their pace,” which demonstrates an inclusive patient-centered approach to setting health goals according to patient ability and priorities.
Yet, some providers in addition to soliciting patients’ goals, do note their own goals for patients. For the most part, these goals reflect aiming for a “care, not cure” approach to engagement trajectories and endpoints. In an interview, an NP explains, If the goal is always going to be people getting better, this isn’t the population you want to work with, because you’re going to lose at least as many of those fights as [you] win . . . and if that’s your goal, you’re not going to last very long because you’re going to get burnt out by the fact that your people aren’t “getting better.” So, I have other goals . . . to focus on people and work hard on making them understand you care. Build those bonds. And hopefully over time that will translate into better care for themselves and be open to you helping them.
The NP explains that the complex patient population often is characterized by physical and behavioral issues that may never be eliminated. A “care, not cure” approach to engagement goals is often reflected in survey answers, such as an NP who quotes Mother Teresa when describing his personal approach: “Do small things with great love.” And an RN explains she focuses on improving patient health, but does not expect levels of patient recovery that result in self-sufficiency, “Unfortunately, many of our patients will not re-enter the workforce but do live with a better quality of life [due to ECHO Care].” Some providers could find these chronic issues discouraging. OITs mitigate pessimism by adjusting health and health care goals to focus on building longitudinal relationships with patients and aiming for patient-defined incremental improvements in health behaviors and well-being.
Engagement Promotion Burnout: Causes and Buffers
Due to the challenges experienced by complex patients, and the limited resources of primary care clinics, OITs still struggle with engagement promotion. OITs explain two sources of burnout, as well as how their team structure can reduce burnout.
Burnout due to patient complexity
The nature of the patient population, in terms of their levels of illness and resources, contribute to professional burnout. A CHW explains her high burnout in an interview, The level of illness [among patients], and it’s not just medical illness. It’s mental illness. It’s substance abuse. It’s homelessness. It’s lack of resources. It’s time . . . we never have enough time . . . we get them too late. They die too soon. We don’t have enough time with them in the clinic. Even though ECHO is structured differently, it never works out that way . . . we’re supposed to be allotted as much time as we want [with patients] . . . but it’s not really fair to people that are having issues to be like, “well, I’m only going to see this person for four hours today.” There’s too many people and there’s too many issues.
Even the flexible schedule and high ratio of OIT members to patients may feel inadequate to address the significant needs of complex patients. Similar comments are made in many surveys, such as a CHW explaining struggles due to patient behavioral health problems, Sometimes it is hard to educate and agree with some patients due to behavioral situations such as withdrawing from drugs or [alcohol]. Their personality changes constantly and they don’t like to follow advice on specific situations (Medications, keep going to ER instead calling the OIT first).
OIT strategies for providing inclusive high-quality care cannot always produce engagement improvements among complex patients due to their severe health problems, nor can strategies always counter the social forces of marginalization that result in resource scarcity among the complex patient population. When OIT members experience the limits of their substantial efforts to remedy these issues, this can result in frustration with their work.
Burnout due to limited capacity
Several providers also attribute some of their burnout to the finite resources of teams working in primary care clinics. An RN says during an interview that while teams help, the team alone is not always enough support. She explains when providers are attending to other patients and an additional patient arrives needing care, teams feel stretched too thin. She muses about how to solve this issue, What if . . . there was back-up for teams if the provider is out [caring for a different patient]? Then everyone isn’t scrambling around trying to figure out what to do with the patients when they show up, and there’s a little more support for teams. [The current ECHO Care model] is small and intimate, which is nice in many ways, but also does leave us on an island.
This RN suggests teams may need additional personnel support to meet patient needs and avoid burnout. Survey comments similarly reflect limited resources for meeting complex patient needs. For example, a PA writes about burnout due to difficulties recruiting and retaining staff, “[The] drawback to teams is that it has been impossible to fully staff and therefore the full model has not been able to be implemented.” While only fully staffed teams that demonstrated the functioning ECHO Care model were interviewed, surveys included teams with both short-term and long-term position vacancies, such the team of the quoted PA. Teams that lacked enough CHWs or nursing support for extended periods may experience even greater burnout than fully staffed teams. Complex patients require large amounts of support. At times, patient needs may remain unmet given the real resource limits of even intensive team-based models like ECHO Care.
Teams as burnout buffers
OIT members explain that working within a team defends against burnout when the input of all team members is valued, when each team member has a clearly defined primary role and when there is good communication within the team about the patients. An NP explains how his team functions, We’re fairly autonomous, and the community health workers, probably 90% of what they do is totally on their own, they really focus on the social [issues]. I have them help with certain medical things, [like] I have them bring me back my [pill] boxes [from patients]. If [the CHW] notices something during [a visit with] the patient, a specific clinical problem . . . they’re my eyes and ears . . . I have a lot of trust in them.
He elaborates on how information is shared during the times when the team meets together, [at] our weekly meetings, I appreciate all of us being in the same room so I can hear everything going on . . . Different members will jump in. We have a lot of that back-and-forth. . . . I like the level playing field with everybody.
While there is sharing of information and some tasks, most tasks for addressing patient marginalization and promoting engagement are clearly divided between OIT members, as the NP describes taking on clinical efforts and CHWs take on social support work. Three quarters of the surveys reflected similar feedback on these features of successful teams, such as a CHW who explains how the team structure facilitates “Identifying and solving problems. . . . [and] help[s] me learn from others’ experiences and vice versa.” And an RN explains the value of the team division of labor in a survey response, “It’s nice to know that one individual is not responsible for every facet of the patient’s care.” Within this division of labor reflected in interviews and supported by survey data, each member is able to provide feedback about patients and information has bidirectional movement between OIT positions.
The team support helps maintain high OIT functionality when multiple team members work with a patient so that no one person gets severely burnt out dealing with patients who are particularly challenging. A CHW describes the team coming together after one of their patients died, We just got word another one of our patients died, seems like they’re dying every week . . . having an open dialogue to support each other, whether we sit in silence or we talk about it. . . . I know that some of the thoughts I am having and some of the things we saw [with the patient] are shared by various members because he was our [collective] patient.
An administrative assistant notes in their survey response, “I do think [a team model] is a much better way to provide patient care to mostly difficult patients. Taking care of such complicated patients without a team would be very difficult.” OIT members support each other emotionally through the emotional toll their work may take, which reduces professional exhaustion.
Discussion
Complex patients face overlapping challenges related to physical and behavioral health problems, as well as social disadvantages including low income, low social support, and poor access to housing. Members of ECHO Care’s OITs explain their professional strategies for addressing the material, health, and interpersonal challenges that contribute to low patient engagement with health-promoting behaviors and produce sub-optimal health and health care outcomes.
Interprofessional teams offer insights into engagement that are not easily recognized by patients. Three engagement strategies identified by OITs also align with patient perceptions of mechanisms promoting engagement, which we described in a previous publication (see Komaromy et al., 2018, for analysis of complex patient interviews). Complex patients describe their own engagement improvements as stemming from health care teams that are available outside of appointments and provide social support, that address patient resource problems, and that maintain a nonjudgmental approach toward patients. This patient and primary care team agreement highlights several ways professionals adjust the tone and content of clinical interactions with patients. However, OIT members also identify two additional subtle strategies used to promote patient engagement: adjusting to patient literacy/ability and collaborative goal-setting. OIT experiences provide guidance for how primary care teams can address issues of health literacy and patient disempowerment when working with complex patient populations.
While OITs explain how they adjust to patient health literacy and cognitive abilities, not surprisingly, patients did not comment on their health care team members making this type of modification (Komaromy et al., 2018). OIT members, on the contrary, were acutely aware of their approach and often describe “meeting patients where they are at,” which means OIT members changing their language, patient expectations, and level of intervention to assist each patient in a meaningful way. In general, U.S. health care institutions demand and reward high patient health literacy (Shim, 2010), which entails patients operating as independent, informed, and motivated individuals with access to health-promoting resources (Sørensen et al., 2012). Health literacy is thus usually tied to engagement; health literacy describes the tools patients are expected to use to achieve engagement in health-promoting behaviors and engagement with health services. Those with low health literacy (due to limited cognitive ability, low education, or other factors (Clouston et al., 2017)) often face barriers to engagement and experience worse health outcomes. For example, those with low health literacy demonstrate less medication adherence (Miller, 2016), impaired development of chronic disease self-management skills (Mackey et al., 2016), more hospitalizations and unnecessary visits to emergency departments (Berkman et al., 2011), and among elderly patients, higher mortality (Berkman et al., 2011). These poor outcomes show low health literacy is often (intentionally or unintentionally) punished in health care.
OITs in ECHO Care demonstrate how professionals can work to counteract punishment of low health literacy. OITs do not expect high levels of health literacy from complex patients. OITs instead adjust their care to complex patient health literacy levels, and, over time, the tailored care they provide improves patient engagement. OITs do this by using simple vocabulary, helping patients organize medications, and maintaining patience in their interactions, among other strategies. These adjustments demonstrate how providers may change their practices in ways that align with growing calls for health care organizations—and not individual patients—to take actions that minimize the contribution of low health literacy to health and health service inequities (Institute of Medicine, 2003; Koh et al., 2013). The Institute of Medicine outlines several ways in which the demands of health systems and organizations can be adjusted to promote “health literate health care organizations” that better support patients with varied skills and resources. These include meeting the needs of patients with low health literacy without stigmatization and addressing low health literacy during all care planning stage, especially critical care points like prescribing new medications (Koh et al., 2013). OITs in this research demonstrate how primary care teams can translate these organizational recommendations into professional practices.
OIT members also identified collaborative goal-setting with patients as a strategy for improving complex patient engagement. OITs contrast goal-setting in ECHO Care with other fast-paced health care environments like emergency departments that rarely solicit patient goals, let alone undertake an intensive patient-led process of identifying and working toward incremental health and health care improvements. Goal-setting in many health care contexts is a recognized component of promoting chronic illness “self-management,” which entails patients becoming active participants in addressing and supporting their own health and well-being (Lorig & Holman, 2003). Interventions promoting self-management advocate for collaborative goal-setting with patients but often emphasize patients becoming increasingly “empowered” to meet their goals, which means becoming responsible for managing their own conditions, solving their own problems, and synthesizing health information largely on their own (Funnell & Anderson, 2004; Lorig & Holman, 2003). For patients like those in ECHO Care who face overwhelming socioeconomic problems and physical, mental, and substance use conditions, this concept of goal-setting is a poor fit. Instead, OITs emphasized better engagement outcomes stem from working with complex patients over long periods to define modest care goals that still include significant primary care team involvement, rather than expecting cures and independence as care outcomes.
OITs explain that patients experience better health care engagement with this goal-setting approach, and OIT members also describe finding professional satisfaction in focusing on care goals, and not only health outcomes. This “care not cure” approach may also be a key to avoiding burnout. By setting attainable goals, such as gaining patient trust and improving patient health behaviors by small degrees, team members can provide compassionate care without becoming overly attached to the (often unlikely) possibility of achieving cures for complex chronic physical and behavioral conditions among patients with limited resources.
OITs also buffered burnout by drawing on team emotional and professional support. Teams regularly spread responsibilities across positions, offer consolation during patient deaths, and help each other with patients needing high levels of care. OIT members describe drawing on several collective traits and resources that comprise adaptive reserve, a term coined by Miller et al. (2010) to characterize resilience in the face of professional challenges, especially those accompanying organizational change. Specifically, OITs demonstrate nurturing team communication and relationships during weekly face-to-face meetings, facilitating teamwork through dividing tasks and reinforcing each other’s efforts as needed, as well as allowing time for team reflection, such as coming together to process feelings when a patient dies. Survey research assessing burnout mitigation among nurses and physicians finds these traits are significantly associated with lower levels of burnout during change implementation (Huynh et al., 2018). OITs illustrate that elements of adaptive reserve also may function to protect against burnout in other health care contexts, namely, among interprofessional teams working with marginalized patient populations in need of diverse forms of health and social care.
Despite these buffers reducing burnout severity, professional frustration and exhaustion were still side effects of team engagement efforts. While research on professional burnout shows organizational factors contribute more strongly to provider burnout compared to patient factors (Huynh et al., 2018), burnout in this research stems from both patient complexity and organizational resource limits. OITs describe burnout due to the prevalence of high illness severity and multiple diagnoses in the patient population, as well as the prevalence of poverty and social isolation among their patients. Organizational contributors to burnout include lack of adequate staff, especially during times when multiple patients experience crises simultaneously. An RN’s call for “back up” for her team speaks to how even a five-person interprofessional primary care team may not be enough to promote engagement and counteract the health and social forces fueling marginalization among their complex patients. OITs provide insight into why and how physicians on the “front lines of care,” such as family medicine and emergency medicine, are at highest risk for professional burnout (Blackwelder et al., 2016; Shanafelt et al., 2012). However, OITs do not demonstrate experiences associated with all types of burnout, which may entail emotional exhaustion, depersonalization (i.e., uncaring disposition toward patients and work), and/or low feelings of personal accomplishment (Blackwelder et al., 2016; Cain et al., 2017). In describing frustrations with addressing patient complexity and finite organizational resources, OITs identify causes of emotional exhaustion. They do not mention in either interviews or surveys that such frustrations result in low feelings of empathy, reduce their motivation to do their work, or undermine their sense of accomplishment. These forms of burnout may be less common in the OITs because team members were recruited explicitly to work solely with complex patients. Health professionals who may struggle to empathize with this patient population, or who do not feel motivated to work with such a marginalized patient group may have self-selected not to pursue a position with ECHO Care or may have shown such dispositions during recruitment and were not selected for hiring.
Limitations
While this research combines interview data with a larger survey, both samples are small and were not randomly selected. Thus, we cannot speak to how common our findings are across interprofessional primary care teams more generally. The sociocultural setting of the clinics employing the OITs included in this research also should be considered as a factor affecting the extension of these findings to other contexts. Both clinics are located in New Mexico, one in an urban county and another in a rural county. The urban clinic is part of the primary care network of a large safety net hospital, and is located in a racially and ethnically diverse and low-income neighborhood. The rural clinic is part of a large rural network of federally qualified health centers in New Mexico and is located in a majority Hispanic county with poverty rates above the state average. The rural clinic and the urban clinic are both located in designated medically underserved areas. Future research may seek to include a larger number of interprofessional teams in a variety of health care organizations and geographic regions to understand how the strategies we outline may vary in their feasibility and effectiveness.
Conclusion
This research illustrates the professional processes that facilitate health care engagement among patients who are marginalized in the health care sector due to illness complexity and socioeconomic status. The experiences of health care professionals working with such complex patients have implications for the hiring, training, and support of individuals and teams in complex care. Professional recruitment for primary care teams working with complex patients should highlight willingness to undertake the effective engagement promotion practices illustrated by ECHO Care’s OITs. In addition, OITs received multiple trainings both immediately after hiring and during their tenure in ECHO Care, which may explain some of their engagement strategies. Other interprofessional teams working with complex patients may similarly benefit from initial and ongoing training support. Future research may determine additional forms of organizational support for primary care teams, especially those addressing emotional exhaustion. While OITs illustrate effective engagement efforts, these should not come at the cost of burnout among team members. Health services research may begin exploring interventions to avoid burnout by listening to OITs, who point to internal team support as useful for buffering professional frustrations. OITs suggest operating multiple interprofessional teams at the same clinic (as opposed to only one, as was the case with ECHO Care), thus signaling organizational efforts to promote interprofessional primary care teams must consider institutionalizing team “back up” by offering additional personnel support during periods of intense patient need. With this adjustment and support for executing the five interprofessional team strategies outlined by OITs, sustained engagement among complex patients is possible. The U.S. health sector remains unequal, expensive, and complicated, but this research demonstrates that health professionals and programs can support patients at the margins of the health sector through targeted efforts by interprofessional primary care teams.
Footnotes
Authors’ Note
Andrea Zurawski is now affiliated with Cecilia Health, New York, New York, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Grant Number 1C1CMS330973-01-00 from the U.S. Department of Health and Human Services, Centers for Medicare & Medicaid Services. The content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the U.S. Department of Health and Human Services or any of its agencies.