
Abstract
Systematic approaches are essential when adapting interventions, so the adapted intervention is feasible, acceptable, and holds promise for positive outcomes in the new target population and/or setting. Qualitative research is critical to this process. The purpose of this article is to provide an example of how qualitative research was used to guide the adaptation a web-based intervention for family carers of persons with dementia residing in long-term care (LTC) and to discuss challenges associated with using qualitative methodologies in this regard. Four steps are outlined: (a) choosing an intervention to adapt, (b) validating the conceptual framework of the intervention, (c) revising the intervention, and (d) conducting a feasibility study. Challenges with respect to decontextualization and subjective reality are discussed, with suggestions provided on how to overcome them. The result of this process was a feasible and acceptable web-based intervention to support family carers of persons with dementia residing in LTC.
Introduction
Qualitative methodologies are enormously valuable and essential in developing (Duggleby & Williams, 2016; Wigginton et al., 2019) and evaluating (Johnson & Schoonenboom, 2016; Mannell & Davis, 2019) new complex health interventions as they offer insights to the conceptual understanding of frameworks and/or theories guiding the interventions. They also provide insights from the experiences of people who will benefit from the intervention or for whom the intervention is intended. As such, they also have a critical role to play in adapting interventions to new target populations and/or settings. Adapting interventions changes the content to reflect the characteristics and core values of a group while preserving the central tenets of the intervention itself (Collado et al., 2013); this refers to adapting an intervention before it is implemented with a new population and or setting.
Interventions are often adapted for different populations and/or settings to save time and money while increasing the likelihood of achieving successful outcomes (Card et al., 2011). Unfortunately, the majority of interventions are adapted during implementation, which threatens intervention fidelity and decreases the likelihood of successful outcomes (Escoffery et al., 2019). Careful planning is needed (Card et al., 2011) to adapt an intervention before implementation so that it is feasible and acceptable to a new target population and has positive outcomes.
The importance of adapting interventions has become more critical with the pressure to scale up interventions for use in diverse settings (Power et al., 2019). A recent scoping review of methods of adapting public health interventions identified 13 adaptation frameworks which had not yet been evaluated (Escoffery et al., 2019). Within these frameworks, there are common steps in which qualitative research methodologies would inform the process of adaptation: (a) assessing the community or population of interest, (b) understanding the intervention to be adapted, and (c) evaluating the adapted intervention. Methods such as community consultation and the utilization of the literature were suggested by the author. However, these methods do not necessarily provide the rich conceptual understandings that qualitative research designs provide in a systematic and rigorous way. None of these frameworks addressed the use nor emphasized the importance of using qualitative research in the adaptation process (Escoffery et al., 2019). This is a critical gap in the literature, as qualitative research can help establish if the central tenets of an intervention are applicable to different populations and settings and also assist in identifying the core values of a group to guide the adaptation of an intervention. As well, qualitative methodologies are well suited to uncover and reveal the contextual aspects of different settings and the perspectives of diverse populations to avoid a mismatch of an intervention or program with a setting and population.
Several articles have described how to utilize qualitative research to develop interventions (Duggleby & Williams, 2016; Gamel et al., 2001; van Meijel et al., 2004). As well, the Medical Research Council (2019) in the United Kingdom has specific guidelines to help with intervention development. Using key components of the Medical Research Council guidelines, previous articles describing how to utilize qualitative research to develop interventions, and the literature outlining steps to adapt interventions, we developed guidelines for adaptation of interventions utilizing qualitative research designs. The purpose of this article was to provide an example of how qualitative research was used to adapt a web-based intervention for family carers of persons with dementia residing in long-term care (LTC) and to discuss challenges associated with using qualitative methodologies in this regard.
Case Example
The urgent need to support family carers of persons living with dementia is well documented (Prince et al., 2015). Web-based interventions show promise for increasing the mental health of family carers caring for a persons living with dementia in the community (Boots et al., 2014; Hopwood et al., 2018; Zhao et al., 2019). Three systematic reviews focusing on web-based interventions for family carers of persons with dementia reported the potential benefit of web-based interventions for improving the mental health of family carers (Boots et al., 2014; Hopwood et al., 2018; Zhao et al., 2019). They also suggested the delivery of interventions in a web-based format has benefits such as flexibility and convenience, as carers can access them when they wish. However, it was not clear if any of the studies reviewed included family carers of persons with dementia residing in LTC.
Family carers provide significant care to their families/friends residing in LTC (Duggleby et al., 2013; Mullin et al., 2013) and, at the same time, can experience significant changes in their roles/relationships, physical and mental health, and hope. Indeed, the mental health of family carers might actually worsen after the institutionalization of their family member as carers experience feelings of blame, self-doubt, isolation, and powerlessness (Gaugler et al., 2012). Carers of persons living with dementia residing in LTC are an at-risk group (Ducharme et al., 2005) and as such, interventions that support family carers of persons with dementia residing in LTC are essential for their quality of life. Adapting an existing, efficacious, web-based intervention would be important to support this population.
My Tools 4 Care (MT4C) is a flexible self-administered web-based intervention for family carers of persons living with dementia in the community (Duggleby, Ploeg, et al., 2018). It includes interactive activities, as well as resources to support carers. MT4C was evaluated and found to be feasible, acceptable, easy to use and showed promise in increasing hope in this population (Duggleby, Ploeg, et al., 2018). MT4C was then adapted for family carers of persons living with dementia residing in LTC using a variety of qualitative methodologies at different stages of adaptation. The adapted intervention (known as MT4C-In Care) was evaluated and found to be feasible, acceptable, and easy to use and increased carers hope, self-efficacy, and decreased feelings of guilt and grief (Duggleby, Jovel Ruiz, et al., 2018).
Adapting a Web-Based Intervention
The following processes were utilized to adapt a web-based intervention (MT4C) for family carers of persons living with dementia residing in LTC using qualitative research: (a) choosing an intervention to adapt, (b) validating the conceptual framework and the essential components of the intervention, (c) deciding on the needed revisions and revising the intervention, and (d) completing a feasibility study of the adapted intervention. These four steps are outlined in Table 1, along with questions utilized to guide the adaptation and the contribution of qualitative research in the process.
Steps in Adapting an Intervention and the Contribution of Qualitative Research.
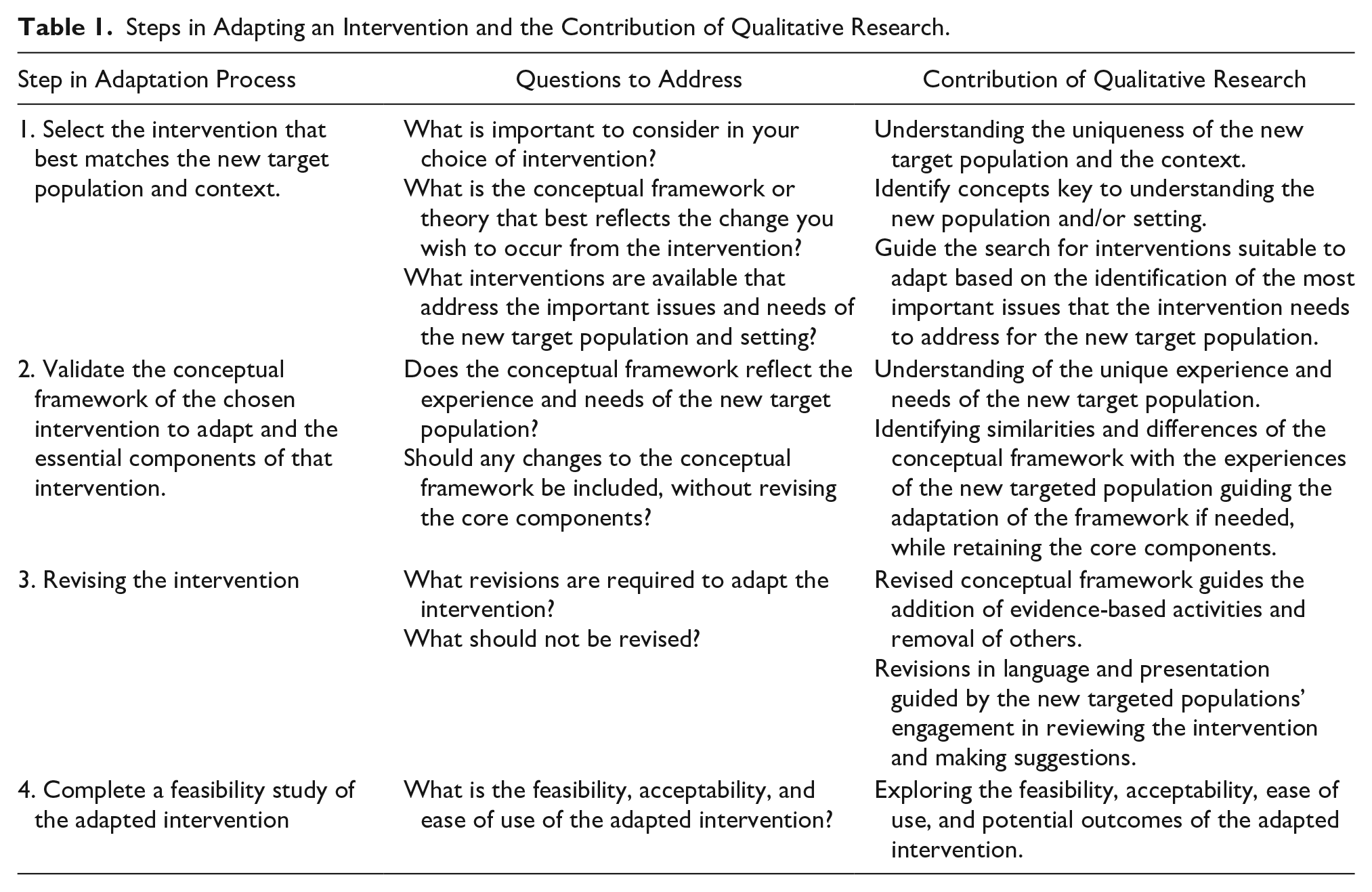
These four steps in adapting an intervention outlined in Table 1 are also discussed in more detail below demonstrating how the four steps were used in adapting MT4C for the new target population and setting.
Choosing the Intervention to Adapt
As presented in Table 1, there are three ways that qualitative research may contribute to choosing of the interventions by (a) understanding the uniqueness of the new target population and context, (b) identifying important concepts key to conceptual understanding of the new population and/or setting, and (c) guiding the search for interventions suitable to adapt based on the identification of the most important issues that the intervention needs to address.
Uniqueness of the new target population and context
Family carers of persons living with dementia are challenged to cope with many transitions that occur across all stages of dementia. For carers these transitions involve learning new tasks, making significant adaptations to the physical and/or social environment, and changing their roles and relationships (Duggleby et al., 2011). As a result, many carers experience significant physical and mental health challenges, including caregiver distress and burnout (Donelan et al., 2011). Little is known about the transition experience and effective interventions to support carers when their family member living with dementia resides in LTC (Afram et al., 2015; Garity, 2006).
Our research team had previously conducted two qualitative studies on the experiences of family carers of persons living with dementia which helped us to delineate similarities and differences in the experiences of family carers of persons with dementia residing in the community versus those of persons residing in LTC (Duggleby et al., 2013; Peacock et al., 2014). Both studies used interpretive qualitative designs (interpretive description and phenomenology) which resulted in a rich understanding of the carer’s experience. The findings of these studies suggested that family carers of persons living with dementia in the community and those residing in long-term care are very much involved in the care of the person living with dementia (Duggleby et al., 2013; Peacock et al., 2014). Similarities in their experiences included feelings of loss and hope and experiencing significant transitions involving learning new tasks, making significant adaptations to the physical and/or social environment and changes in their roles and relationships (Duggleby et al., 2013; Peacock et al., 2014). However, carers of persons living in LTC needed to advocate for their family member and build relationships with LTC staff (Peacock et al., 2014). Negative interactions between family carers and LTC staff and perceptions of poor care had a negative impact on family carers (Peacock et al., 2014). These differences suggested that the setting in which their family member was living significantly changed their caregiving experiences. The two qualitative research studies helped to identify differences in experiences when a family member is living in the community with their carer as opposed to residing in LTC. Without these two studies, we may have not been able to identify the differences in this population and the need to adapt an intervention to reflect these differences.
Concepts key to understanding of the new population and context
Our qualitative work suggested that family carers of persons living with dementia experienced life-changing transitions (Duggleby et al., 2013). Transitions are processes triggered by change during which a new situation is incorporated into a persons’ life (Meleis, 2010; Olsson & Ek, 2002). The disruptive nature of transitions results in uncertainty, distress, and loss of hope putting carers at risk for changes in their health (Ducharme et al., 2011). As our goal was to support carers and improve their quality of life, transitions as a concept and as such transition theory were an important concept to understanding the new population and setting.
Guide the search for available interventions
Not all of the web-based interventions identified in three systematic reviews (Boots et al., 2014; Hopwood et al., 2018; Zhao et al., 2019) reported the conceptual framework that guided their development, but the majority were based on stress and coping theories with a focus on burden (Duggleby, Ploeg, et al., 2018) and, as such, may not address the transitions experienced by this population. Based on our understanding of the experience of family carers of persons with dementia residing in LTC, we determined the intervention chosen to be adapted should be one developed based on transition theory. It was important that the chosen conceptual framework of the intervention was transition theory, as the conceptual framework guiding an intervention delineates how changes occur as well as the central components needed for an intervention to be effective (Duggleby & Williams, 2016).
We found two interventions based on transition theory to support family carers of persons with dementia (Ducharme et al., 2011; Duggleby, Ploeg, et al., 2018). Both were developed for family carers of persons with dementia living in the community and were evaluated positively. Although one showed promise in supporting family carers, it was time intensive, as it consisted of seven in-person 90-min psychoeducational individual sessions (Ducharme et al., 2011). The other, titled My Tools 4 Care (MT4C), was a web-based intervention that was evaluated and found to increase hope in family carers of persons with dementia living in the community (Duggleby, Ploeg, et al., 2018). MT4C is a multicomponent flexible intervention tailored to the individual as a family carer could choose the interactive activities in which they wished to engage in when they wanted. Using qualitative research as a guide, MT4C appeared to be the most appropriate for the new target population and setting as it was based on transition theory, and resulted in positive outcomes for carers.
Validate the Conceptual Framework of the Intervention
To validate the conceptual framework of the intervention, we again turned to our understanding of the unique experience and needs of the new target population and examining similarities and differences of the conceptual framework with the experiences of the new targeted population. Although we identified transition theory (Meleis, 2010) as a potential conceptual framework that would be congruent with our understanding of the changes experienced by family carers of persons with dementia residing in LTC, it was important first to validate the adapted transition conceptual framework that guided the development of MT4C. The conceptual framework for MT4C was developed through a series of research studies on transitions experienced by family carers (Duggleby et al., 2011, 2014). This work delineated the process of transitions that family carers experienced when caring for a person with dementia living in the community. The core components of the process of transitions were (a) coming to terms, (b) connecting, and (c) redefining normal (Duggleby et al., 2011). Validating the conceptual framework was a very important step in the adaptation process, as it delineated what should be preserved that was core to the effectiveness of the intervention and what should be adapted in the intervention for the new target population and setting.
There is an ongoing debate in the literature regarding concerns about adaptation of interventions and fidelity (Escoffery et al., 2019). Intervention fidelity refers to the extent to which the adapted intervention adheres to the intervention that was originally developed. Validating the conceptual framework and core components of an intervention ensures the internal logic of the intervention and critical steps contributing to the intervention effectiveness are maintained. However, the previous qualitative research that guided our understanding of the unique experiences of carers of persons living with dementia residing in LTC were studies of the overall caregiving experience (Duggleby et al., 2013; Peacock et al., 2014) and not focused on the transition experience. To address this issue, we utilized qualitative methods (thematic and conversation analysis) to study transitions experienced by family carers of persons with dementia residing in LTC (Cottrell et al., 2020). The findings of this study were then compared with the MT4C conceptual framework and were found to validate the framework and the essential components. Figure 1 represents the validated MT4C conceptual framework with the addition of the conceptual understanding of transitions that was gained through the qualitative research. These additions are noted in bold in Figure 1.
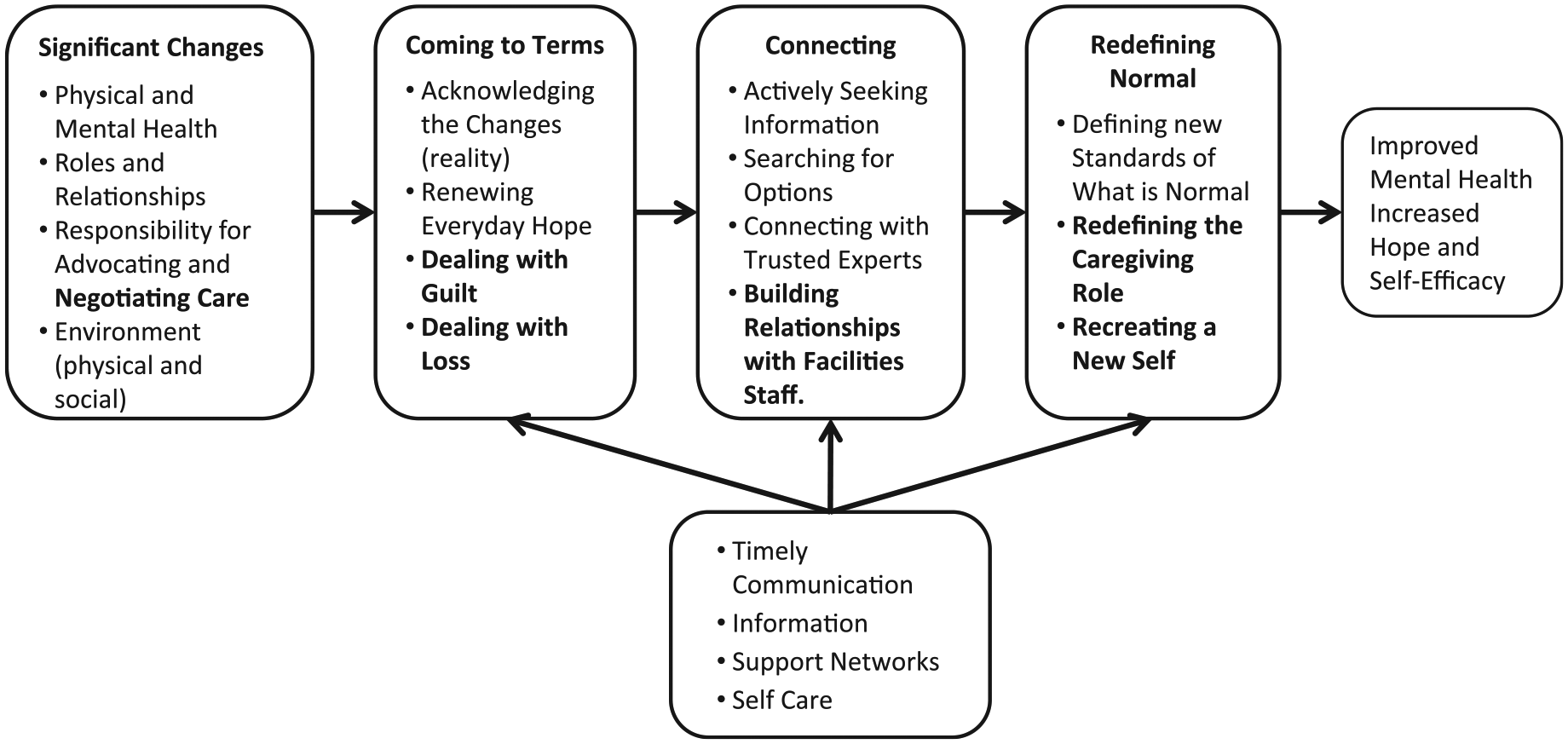
MT4C-In Care Transition Framework adapted from Duggleby, W. Swindle, J. and Peacock, S. (2014, p. 24).
Under the concept of “Coming to Terms”, “dealing with guilt” and “dealing with loss” were added, as carers described their feelings of loss related to (a) self, (b) control of their family members’ care, (c) support networks, and (d) progression of their family member’s dementia. They were continually dealing with guilt as they felt they were relinquishing the care of the family member to the facility. Adding to the concept of “Connecting” was the importance of connecting and “building relationships with LTC staff” as a way to deal with their transitions. “Redefining the caregiving role” and “recreating a new self” were added to the concept of “Redefining Normal.” The outcomes of “Redefining Normal” were improved mental health and increased hope and self-efficacy. As such, we were able to keep the critical components of MT4C’s conceptual framework at the same time revise it to reflect the new population.
Revision of the Intervention
Revision of the conceptual framework, while keeping the core concepts, helped to guide the adaptation of the intervention in terms of content without threatening the fidelity of the original intervention. Adaptations need to be carefully chosen so as to not alter the internal logic of an intervention and ensure the critical steps contributing to the intervention effectiveness are maintained (Reinschmidt et al., 2010). Reinschmidt et al. (2010) suggest acceptable changes to adapt an intervention, which include (a) translating language or modifying vocabulary, (b) replacing cultural references, (c) modifying some aspects of activities, and (d) adding relevant evidence-based content to make the program more affective.
Carers of persons living with dementia residing in LTC were engaged through a descriptive qualitative study utilizing focus groups to review MT4C to determine what needed to be adapted while keeping the essential components (Duggleby, Jovel Ruiz, et al., 2018b). The original intervention (MT4C) designed for family carers caring for persons with dementia residing in the community had an interactive section titled “About Me.” This section contained guided evidence-based activities to help carers think about and cope with the transitions they experience. For example, activities in this section included “understanding your inner strength” and “what gives you hope.” Users could also add formatted text, photos, and attachments in this section. Based on the adapted conceptual framework, additional interactive activities were added to MT4C to develop the adapted intervention, titled “My Tools 4 Care-In Care” (www.mytools4careincare.ca). These additional interactive activities relevant to the context of LTC included (a) dealing with guilt, (b) communicating and advocating for their family member with staff, (c) how to deal with loss and grief, and (d) activities to assist with end of life decision-making.
Other adaptations important to consider are that language and presentation are acceptable to the new target population (Escoffery et al., 2019). Qualitative focus groups of carers of persons living with dementia residing in LTC were engaged in reviewing MT4C and were asked about language and presentation (Duggleby, Jovel Ruiz, et al., 2018). Wording was revised and additional pictures were added. Because most of the family carers were over the age of 65 years, the format of the web-based intervention was based on best practices for use of websites by older adults (Kuerbis et al., 2017). For example, larger displays and fonts were utilized on a plain and uncluttered page with contrasting colors. Navigation/menu items were placed on the upper left-hand side, and extraneous information/animation that may easily overload working memory was eliminated.
Complete a Feasibility Study of the Adapted Intervention
The United Kingdom Medical Research Council Guidelines (Skivington et al., 2018) for the development of complex interventions and their evaluation recommend that a feasibility study be completed to determine whether the intervention is feasible and acceptable to the target population. Feasibility (or pilot) studies are used to try out the intervention on a small scale before a larger more comprehensive investigation (Thabane et al., 2010). Feasibility study assessments of intervention acceptability and the degree of adaptation required will also be key considerations for future scale-up and sustainability of such interventions (Milat et al., 2012). Qualitative research should also be important at this stage in adapting interventions, as it will confirm the intervention has been successfully adapted to the new target population, setting, and context (O’Cathain et al., 2015).
We used a mixed methods design for the feasibility study of MT4C-In Care (Duggleby, Jovel Ruiz, et al., 2018). This design included a descriptive quantitative design which included quantitative process and outcomes measures and Sandelowski’s (2010) descriptive qualitative design with semi-structured qualitative audio-taped interviews. Participants reported in their qualitative interviews that MT4C-In Care helped them deal with the significant changes they experienced by (a) encouraging them to reflect on their experience, (b) reinforcing their goals as carers, and (c) communicating better with staff (Duggleby, Jovel Ruiz, et al., 2018). These outcomes were identified in the rich interviews that were key to the adaptation of the intervention and would not have been identified in the quantitative surveys we used to measure feasibility, acceptability, and ease of use.
Challenges
Several challenges are related to utilization of qualitative research to guide the adaptation of interventions, such as decontextualization and subjective reality, which are discussed in more depth below.
Decontextualization
Utilizing qualitative research to guide the adaptation an intervention decontextualizes the participant experience from its context, similar to developing a new intervention. Duggleby and Williams (2016) suggested decontextualization occurs when the findings of a qualitative study are distanced from its context and applied to a broader context. This is similar to using qualitative methodologies to develop measurement instruments (Coyle & Williams, 2000). Coyle and Williams (2000) suggested the use of a cyclical approach of ongoing utilization of qualitative methodologies when evaluating the intervention to deal with this challenge. For example, mixed methods approaches should be utilized in feasibility studies and pragmatic randomized controlled trials to determine whether the context is similar to the qualitative studies utilized to adapt the interventions. Mixed methods designs have also been found to be useful particularly in the integration of cultural specificity into the development of an intervention (Nastasi et al., 2007) and in understanding how the intervention works (Holter et al., 2020). As well the qualitative data may provide additional understanding of the issues that are most important to the targeted population to further revise the adapted intervention (Strolla et al., 2006).
Qualitative methodologies are important to use throughout the process of adapting and evaluating interventions.
Subjective Reality
Another challenge is reflected in the subjective epistemological position of qualitative research (subjective reality) in which knowledge is a reflection of different viewpoints and explanations (Dahnke & Dreher, 2011). Subjective reality is a strength of qualitative methodologies but is an issue when qualitative research is used to develop interventions that are meant to predict and control changes in a persons’ behavior (Duggleby & Williams, 2016). Qualitative research expects and embraces diversity, contradiction, and fluctuations (Duggleby & Williams, 2016) and, as such, is an important issue in transitions as processes of change. As suggested by Duggleby and Williams (2016), one strategy for dealing with this challenge is to develop complex interventions that are flexible and allow for variations and fluctuations. When adapting interventions, it is important to select an appropriate intervention to adapt that could be tailored to the individual. Tailoring involves the flexible use of an intervention to accommodate personal values and choice on a case-by-case basis (Collado et al., 2013). An important characteristic of complex interventions is their flexibility to be tailored to the individual (Craig et al., 2008). MT4C is a flexible self-administered web-based intervention in which family carers of persons with dementia living in the community can choose the activity they wish to engage with, when they want, and for as long as they want. This aspect of MT4C was important to maintain in the adapted intervention MT4C-In Care so that it can be utilized by diverse populations and increase its potential effectiveness.
Consideration of these challenges is important as they provide additional information to guide the adaptation of interventions. These considerations underscore the importance of using qualitative methodologies to inform which intervention to adapt and how it should be adapted, as well as guide ongoing evaluation.
Conclusion
Researchers may utilize qualitative research in a carefully planned way as outlined in this article to adapt interventions so that they are feasible, acceptable, and result in positive outcomes in a new target population. As such, it addresses a knowledge gap by adding to our understanding of the possible contributions that qualitative research makes to the adaptation of interventions. The challenges of using qualitative methods were discussed to provide further insight into important considerations in adapting interventions. The four steps utilized in adapting MT4C were successful, as the new intervention (MT4C-In Care) was found to be feasible, acceptable, and easy to use by family carers of persons with dementia residing in LTC (Duggleby, Jovel Ruiz, et al., 2018). Future research could include using these steps to adapt interventions to support carers of persons with other conditions such as cancer, or congestive heart failure. As well the process outlined in this article provides a framework for adapting programs for different settings. As such, it is a promising direction for qualitative research to guide the adaptation of health-based interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding from the Canadian Fraillity Network Catalysis Grant for the research. No funding was received for authorship, and/or publication of this article.