
Abstract
Many studies have reported on issues of accessibility and quality of health care among the different vulnerable subgroups in urban locations. To date, no study has been done on the challenges faced by health care–seeking migrants (those traveling to cities for health reasons). This qualitative study used in-depth interviews and nonparticipant observation to examine the health problems, health care–seeking trajectories, and challenges faced by health care–seeking migrants in Delhi, India. Participants described long courses of health care seeking, typically from the district to the state capital to the national capital. There were variegated paths to health care seeking characterized by delays in service utilization, progression of disease, and cost escalation. The challenge relating to the delay in receiving health care was exacerbated by the residency status of health care–seeking migrants. In conclusion, health-related migration is associated with shared but also unique barriers to health care seeking. India’s urban health care reform agenda needs to cater to the needs of this population.
Keywords
Introduction
Access to health care has been a recalcitrant challenge in the global transition from the Millennium Development Goals to the Sustainable Development Goals era (Hatefi et al., 2016). The lack of access to health care is a pressing problem faced by poor populations in particular (Das & Hammer, 2007; Ensign & Bell, 2004; Moore-Nadler et al., 2019; Nicholas et al., 2016). Where access barriers have been confronted globally, quality is the remaining challenge keeping health systems from reaching all those in need (Margaret et al., 2018).
In India, the intertwined issues of access and quality have been a protracted challenge in the context of health care seeking. In 2016, India ranked 145 among 195 countries in the Global Burden of Disease Study Healthcare Access and Quality (HAQ) Index (Fullman et al., 2018). The “poor functioning” of facilities often forces people from the rural hinterlands to seek care in “overstretched” urban hospitals (Bajpai, 2014, p. 8). This is in part due to the design of the Indian health system.
The public health system in rural India is based on population-based norms following a tiered system that offers basic care at the community level through Sub Health Centers (SC), the first point of contact between the community and primary health care system. Above this level are Primary Health Centers (PHC), where medical officers are stationed, catering to a population of 20,000 to 30,000, followed by Community Health Centers (CHC), the first referral unit intended to provide 24 × 7 and specialist services wherever possible (Chokshi et al., 2016). Further up the referral chain are district hospitals, which are largely focused on secondary care with some tertiary facilities, followed by medical college hospitals mostly located in urban centers, where most tertiary services are available. There is also a pattern of the most advanced tertiary care being offered in a small subset of medical college hospitals, both public and private (Public Health Foundation of India, 2011), which are almost always located in state capitals or the national capital.
Urban health service delivery in practice does not follow such norms because of population density and other factors, including governance. A report of the National Urban Health Mission’s Technical Resource Group (NUHM TRG) found that in urban India, three types of patterns of health care provisions/delivery exist. In the first pattern, typically that of smaller cities, the state department of health has the entire onus of providing health care, although in some cases, nonmedical services relating to public health are managed by the municipal officer (Ministry of Health and Family Welfare, Government of India, 2014). In the second pattern, health care is provided by facilities under the urban local body (ULB). Because the ULB generally has a maternity hospital, a few urban health dispensaries, and a unit of volunteers under it, many health care services end up being provided by the district hospital or medical college hospital, under the state’s jurisdiction. In the third pattern, medical and nonmedical public health functions are managed by the ULB, whereas medical college hospitals are managed by the state government. This is the case in Delhi, where our study was located (Ministry of Health and Family Welfare, Government of India, 2014). This categorization, notwithstanding, urban service delivery is characterized by great diversity and influenced by a broader range of stakeholders and legacies, including colonial infrastructure and norms, various urban development projects introduced by municipal, state, and national entities (Ganesan et al., 2017).
Perhaps the most salient feature of urban health service delivery is the massive predominance of and reliance upon the private sector for care, diagnostics, and medicines (Sengupta & Nundy, 2005). This is part of a well-known phenomenon called the “mixed health systems syndrome” common in low- and middle-income countries (Nishtar, 2010, p. 74).
These patterns have critical implications for health care seeking both for rural populations requiring specialist care and urban dwellers who may require care but face challenges in accessing it. As must be evident, it also implies traveling—physically—across the aforementioned referral chain to seek care for more advanced health conditions.
India’s NUHM took into account the peculiarity of urban health service delivery as well as the uniquely vulnerable populations that would require care. The NUHM Framework document states that it would have high focus on: 1:10:1-Urban Poor Population living in listed and unlisted slums; 1:10:2-All other vulnerable population [sic.] such as homeless, rag-pickers, street children, rickshaw pullers, construction and brick and lime kiln workers, sex workers, and other temporary migrants (Ministry of Health and Family Welfare, Government of India, 2013, p. 3).
As seen here, the situation of migrants is underscored.
In India’s National Sample Survey (NSS) Migration rounds, health care is one of the reasons reported for migration. Migration for this purpose has been defined as follows: “Healthcare: Persons sometimes moved from one place to another due to the availability of better medical facilities for treatment or conditions, unsuitable weather in the last UPR 1 (Usual Place of Residence)” (Ministry of Statistics and Programme Implementation, Government of India, 2010, p. 13). According to the 2010 NSS (which is based on data gathered in 2007–2008), 3,76,400 male migrants (0.7% of total male migrants) and 2,64,700 female migrants (0.1% of total female migrants) reported health as a reason for migration (Ministry of Statistics and Programme Implementation, Government of India, 2010).
Studies have been done on the health-related concerns of people migrating for work within India. This includes the health problems of migrant construction workers (Adsul et al., 2011) and morbidity of migrants engaged as laborer and in other informal work (Karn et al., 2003), as well as on the symptoms and care-seeking behavior of migrant brick kiln workers (Thomas et al., 2014). Another study examined the impact of out-of-pocket expenditure on illness, in addition to the socioeconomic status and Below Poverty Line (BPL) status of patients seeking care at a public facility in Delhi to understand inclusion and exclusion of patients from the social safety net (Bajpai et al., 2017), but it did not necessarily distinguish between Delhi-based patients and health care–seeking migrants. Some concern over the financial challenges faced by specific groups of health care–seeking migrants has been raised by health providers, calling them “cancer refugees” (Khan, 2018).
To our knowledge, there have been no studies looking specifically at the challenges of health care–seeking migrants. Filling this gap, the aim of our study was to trace the trajectories of seeking health care of health care–seeking migrants and examine the challenges faced by them while accessing health care at a large tertiary public facility in Delhi.
Method
Qualitative field research methods including in-depth interview and nonparticipant observation were employed between 2016 and 2018. This analysis is part of a larger qualitative study whose goal was to understand from the perspective of urban vulnerable groups (homeless, health care–seeking migrants, migrant workers, fisherfolk)—the health burdens, trajectories of health care seeking, and challenges faced while seeking health care, as well as architectures of service delivery and experiences of providing health and related services to marginalized urban dwellers from the perspective of health system actors charged with serving their needs (Mathew et al., 2018). Fieldwork on health care–seeking migrants was carried out between June and October 2018.
Health care–seeking migrants were recruited based on the aforementioned NSS definition (Ministry of Statistics and Programme Implementation, Government of India, 2010). We also ensured that the recruited participants belonged to low-income backgrounds. If we found during the course of interview, they belonged to middle class or higher levels of affluence, the interview was discontinued. Based on this criterion, two interviews were terminated. This was done based on the premise that higher income health care–seeking migrants would, by dint of their economic status, have recourse to better or other health care–seeking options in the city, whereas relatively poorer health care–seeking migrants would need to rely on the public sector health apparatus more substantially.
The study comprised multiple phases: First, a nongovernmental organization (NGO) supporting treatment seeking of poor patients was identified. These patients sought treatment at a large government tertiary-level facility, where migration for health reasons is an established and publicly known phenomenon. A social worker with the NGO was invited to participate in the study.
Following this, participants were recruited for in-depth interviews through convenience sampling, with the input of social workers who work closely with these populations. These participants were mainly staying in dharamsalas (rest houses) managed by the facility administration. Subsequently, on the suggestion of social workers, we were able to recruit participants staying in a shelter maintained by another NGO. At this shelter, we asked the participants from which pharmacy they purchased medicines, after which we interviewed a pharmacist at the store. In addition, patients were approached to participate in the study while they were waiting outside the hospital. The sample of health care–seeking migrants was partly respondent driven, that is, nominated by members of vulnerable groups or by providers. As part of nonparticipant observation, field notes were also jotted down during each visit to the field.
Written informed consent was taken prior to each interview. All participants were provided participant information sheets and explained the purpose of the study. They were requested to sign on the consent sheet or have the interviewer sign on their behalf in case participants gave verbal consent. The study used and adapted interview guides piloted and used in an extensive field-based policy recommendation process undertaken by researchers, health officials, and activists affiliated with the NUHM-TRG in 2013 (Ministry of Health and Family Welfare, Government of India, 2014). Interviews were recorded and stored on password-protected laptops that belonged to team members. All interviews were transcribed verbatim by the team members and other consultants. Transcriptions were done into phonetic English.
Member checking was done with three providers (Mays & Pope, 2000). Due to the unfixed duration of stay and place of residence of the health care–seeking migrants, it was not possible to do member checking with them. Data (in-depth interviews and field notes) were analyzed by three team members, using a grounded theory approach of inductive generation of themes (Glaser & Strauss, 1967) and ATLAS.ti 8.4 software (ATLAS.ti, n.d.).
In the first perusal of data, open coding was used to generate a free list of emerging themes, with corresponding sample text falling under key categories of the research tool. Based on this initial free list, further coding of interview summaries was carried out by members of the research team reconciling and merging codes as necessary, through periodic discussion. For instance, upon discussion, we merged the code: healthseeking_nodonorsupport (defined as—When a patient is unable to get financial support from NGOs for treatment) with another code: challenge_financial (defined as—Patients face difficulty affording services or getting financial support to pay for health. This includes people feeling cheated for money).
Following this, a series of discussions were undertaken, and additional themes added to the codebook. Themes were then collated and grouped, and then perused again to develop codephrases for each theme. The study received ethical clearance from the Institutional Ethics Committee of Public Health Foundation of India.
Results
This section details demographic information, health problems, health care–seeking trajectories, and the challenges faced at a tertiary-level public hospital in Delhi.
Participant Characteristics
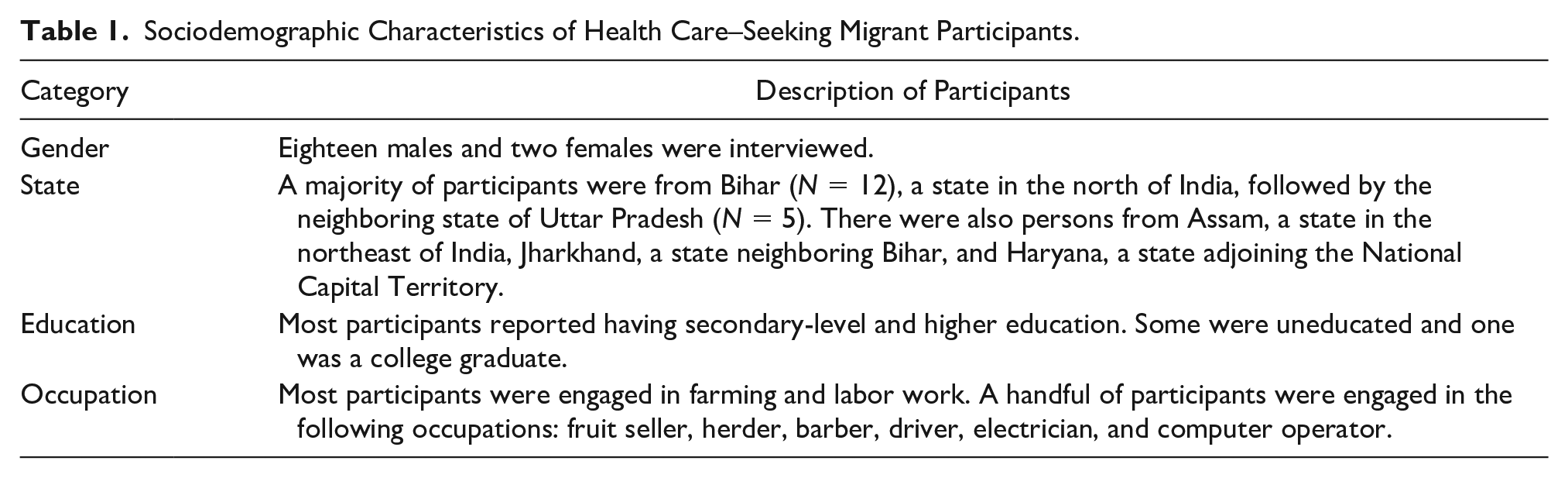
Twenty health care–seeking migrants (see demographic information in Table 1) and five providers (comprising two doctors, two social workers, and one pharmacist) rendering services to the subgroup were interviewed. Four providers were male, one was female.
Sociodemographic Characteristics of Health Care–Seeking Migrant Participants.
Health Problems
The illnesses that participants reported ranged from cancer to liver problems, tumors (of the bone and the brain), sickle cell anemia, and orthopedic injuries including accidents, electric shocks, and gunshot wounds. Some participants exhibited patterns of multimorbidity.
For instance, one participant had hepatitis B, kidney failure, blood pressure, and disability caused by injury, while others reported dental, neurological, and orthopedic problems, alongside a diabetes diagnosis, as well as concurrent palpitation, breathlessness, insomnia, weakness, and headache. Illness causation as understood by participants was in some cases linked to delayed health care access, described as follows: When treatment is delayed, the disease intensifies . . . The level of pollution here is such that when I drink water, it leads to a problem, it aggravates the cough. When cough worsens for a cancer patient, it affects the lungs quickly. So, these are the issues faced by cancer patients—Health care–seeking migrant, Male
Health Care–Seeking Trajectories
Although the course of health care seeking varied for each of the participants, several commonalities were observed. In some cases, health care–seeking migrants were referred from a hospital in the hometown to the public hospital in Delhi. In other cases, participants chose to seek care at the facility in Delhi because of the prohibitive cost of treatment in the hometown or experiences of inadequate care.
While we probed as much as possible, in some cases, the trajectories were not clear and precise, and in the remaining cases, there was no definite way of knowing if participants had provided a comprehensive picture of the course they had undertaken. It was also not clear in all the cases whether a formal referral was made from a hospital or if it was a mere recommendation by a doctor, or whether the acquaintance (who typically had been a patient and in some cases staff at a government facility) of the patient had suggested that she or he visit the particular government facility in Delhi. However, some patterns did emerge (see Table 2).
Illustrative. Some of the Patterns of Health Care Seeking Among Participants (Health Care–Seeking Migrants) From Different States in India.
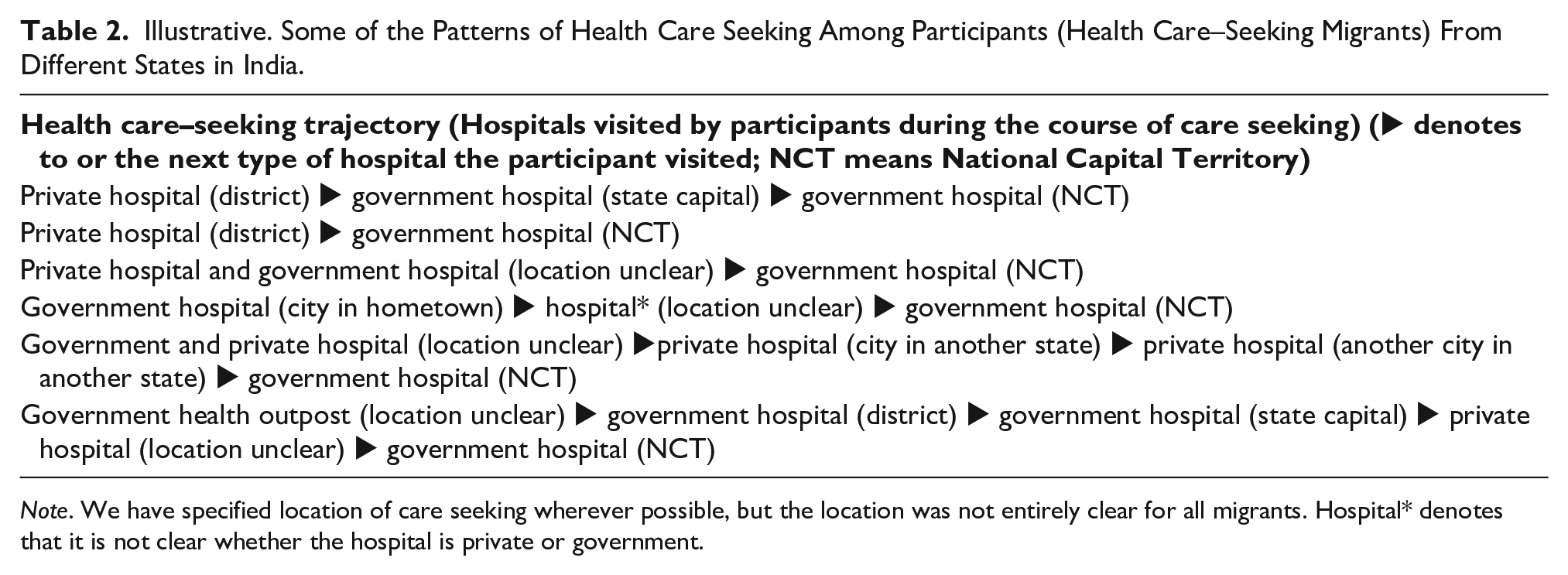
Note. We have specified location of care seeking wherever possible, but the location was not entirely clear for all migrants. Hospital* denotes that it is not clear whether the hospital is private or government.
Table 2 shows that each of the participants visited at least one or more hospitals (either private and/or government) before coming to the tertiary-level public hospital in Delhi for health care. While most participants followed a different course of care seeking prior to their arrival in Delhi, both in terms of the type of hospital (government/private) visited as well as the level of care (hospital in district or state capital or other cities), on their arrival in Delhi, they came directly to the specific government hospital. One participant from Bihar said he was referred from a hospital in his hometown to a facility in Delhi: I went to a government hospital as well as a private hospital . . . I sought treatment in the city close to the village . . . I could not get the treatment there. I was referred from there to [name of hospital]—Health care–seeking migrant, Male
Overall, participants gave mixed responses for the type of facility preferred. Some of the participants preferred government over private, whereas others preferred private, and a few others disliked both private and government facilities. Private hospitals appeared to be the first point of contact among many participants. For a few others, a government facility was the first point of contact. In a few cases, participants went only to private hospitals or only to government hospitals before coming to Delhi for seeking care. We did not observe a clear pattern of public versus private health care seeking by disease type: Trajectories were highly variable.
Participants reported escalating levels of care from the local level upward—in effect, going up the referral chain. For instance, one health care–seeking migrant was referred from a private hospital in the district to a government hospital in the state capital, and thereafter, he was referred to Delhi, the national capital. In another case, the patient was referred from a district government hospital to a government hospital in the state capital, and then to a national government facility in Delhi. Even when the course of health care seeking appeared to be similar in terms of the type of facility visited, the level of care was not clear in all cases, making it difficult to generalize the course of care seeking.
Patients of private hospitals undertook varied courses of health care seeking, in some cases visiting government facilities. A participant from Haryana was referred from a private hospital in a city to a private hospital in another city of his domiciliary state, after which he came to Delhi. A participant from Bihar went from a lower level government hospital to the district government hospital, after which he went to a government hospital in the state capital. Thereafter, at a private hospital, he was advised to visit a government facility in Delhi: At the district level, there is a government hospital, I was sent there . . . Then I went to Patna, Bihar’s capital, Patna. There I went to a government (hospital) . . . Patients were lying like they were dead . . . There was no one to take care of them . . . Then I rushed to a private hospital . . . I was asked by the doctor to go to Delhi, to [name of hospital]—Health care–seeking migrant, Male
Another variant of private care seeking was seen in the instances of health care–seeking migrants from Bihar being referred from a private hospital in their hometown to a tertiary facility in Delhi: I went to a doctor in [name of place] . . . That was a private (doctor) . . . They did a CT (scan) and said that I have brain tumor. So, they referred me to [name of hospital]—Health care–seeking migrant, Male I went to a private hospital so that I would get cured early . . . I was kept there for two days . . . I was referred . . . I was asked to go to [name of hospital], so I came to [name of hospital]—Health care–seeking migrant, Male
The foremost reason for coming to Delhi to seek treatment was the lack or poor quality of health facilities in the hometown: A provider indicated that as many as 40% of patients visiting this facility were from one state, Bihar, who faced these challenges. In public health facilities in their hometowns, participants said that the quality of health services was poor because of inadequate infrastructure, lack of amenities, poor sanitation in health facilities, long drawn out bureaucratic procedures, inadequate attention given by the doctor, unavailability of medicines, and ineffective treatment. The unavailability of specific specialty services such as stem cell treatment in recently established branches of tertiary care facilities forced people to seek health care in the national capital, where service provision for such treatments was more established. Private facilities were criticized for continuing treatment, despite being unable to diagnose the disease. Participants typically identified these facilities with extracting large sums of money or “loot,” and being exploitative.
In Bihar’s capital Patna, there is “loot.” Doctors are not concerned about the disease, they are interested in extracting the maximum possible amount of money. Big buildings have been constructed by “loot”—Health care–seeking migrant, Male
In some cases, recommendations made in the participant’s village or by the family led people to seek care in Delhi: I have a younger brother, he also has a problem. He has cancer. He is undergoing treatment here. So, he brought me here. He said come with me [name of hospital]. I will have you seen there—Health care–seeking migrant, Male
It bears mentioning that most participants referred to their trajectories with a sense of frustration and sometimes, exasperation. In some cases, requests were made to the research assistant about financial support for treatment seeking, help finding jobs, and so on. Trajectories were felt to be long, tiring, and sometimes isolating (involving being away from family and or their regular lives for extended periods of time). Moreover, in the case of all participants, care seeking was still ongoing, bringing a range of challenges to their lives, as we explain in the next section.
Health Care–Seeking Challenges
Long wait times and the role of contacts
Complicated administrative procedures
Delays in getting care, lack of diagnosis
Recurrent medical costs and malpractice
Chronic nonmedical expenses
Long Wait Times and the Role of Contacts
Participants typically came early in the morning and waited several hours at the outpatient department (OPD). They reported large patient loads, and that this resulted in not being given quality time by the doctor and proper investigation of the issue. In some cases, intrafacility networks and political connections made it easier to access care by enabling patients to meet the doctor out of turn; however, this was problematic for other patients as they had to wait longer. Patients were even assisted with bureaucratic procedures in the facility by social/political networks. A participant spoke about the assistance he received: It was the MP [Minister of Parliament] who helped me: he got me a number in the queue, got the card made . . . You need contact with politicians, otherwise it is not possible to get work done at [name of hospital]—Health care–seeking migrant, Male
Complicated Administrative Procedures
Participants found it tough to get through bureaucratic procedures in the facility. The obligation of filling up forms was problematic for illiterate patients. They were often not aware of the location of specific departments and sources of support available to facilitate care seeking. Even the providers found it difficult to connect people to services: Lack of education plays a huge role, I think. Because sometimes we also face the problem, we are not able to make the person understand. That’s because they are so uneducated, they are not able to understand basic things—Health provider, Female
Difficulties relating to bureaucratic norms extended to the lack of possession of necessary documentation such as the unique identity, or Aadhaar card. 2 Lack of an ID proof was a hurdle for doing laboratory tests in Mohalla (neighborhood) clinics. Some of the participants did not have BPL card which entitles them to subsidized care at government facilities. The procedure of getting a BPL card was fraught with problems because not everyone was entitled to it. With government funds being one-time grants, financing revision surgeries became a challenge even for patients having BPL cards. The procedure of getting these identity cards made was fraught with problems as patients had to go back to their hometown to get required paperwork issued by local administrators for this purpose. There were other challenges, too: One patient for instance was not able to get an Aadhaar card made because her fingerprints were not consistent, making it impossible to receive funding for her treatment. Even the possession of an identity proof did not guarantee immediate care as patients had to follow lengthy bureaucratic procedures, such as getting the required signatures from government departments in Delhi to activate their entitlements. Another bureaucratic challenge related to the time taken to procure out-of-stock medicines, forcing people to purchase it elsewhere. These factors delayed or stalled the treatment process.
Delays in Getting Care, Lack of Diagnosis
In some cases, delays were associated with the failure to diagnose the illness, and a few patients found the treatment to be ineffective. Participants typically faced delays in getting treatment in time: Waiting lists extended up to a year or more for diagnostics and operations.
I am being treated here at [name of hospital]. Understood? I have been referred to this facility from Patna. From [name of hospital] Patna. (It has been) five months. I was supposed to get operated. But the operation has not been conducted yet—Health care–seeking migrant, Male
Delay in treatment sometimes increased the chance of disease progression and, in some cases, even death. The time lag for the sanction of money was often huge, increasing the chance of disease recurrence, especially in cases where the patient had cancer: Someone who has finished his chemotherapy, will have one-month time, in which the surgery should be done. But we delay that, because the money isn’t coming through. And every delay of two weeks, increases the chance of the recurrence of the tumor by about I think 10 per cent—Health provider, Male
Some participants reported having to often wait long durations or keep returning to the city for diagnostic tests or to refill prescriptions. The delays additionally added to the burden of expenditure for patients for costs related to staying in the city. Delays also led to exasperation and burnout on the part of participants and their family members.
Recurrent Medical Costs and Malpractice
Most participants noted that they lacked the wherewithal to afford treatment and, in most cases, were dependent on external sources of funding. Participants spent vast sums of money on medicines and diagnostics. For one participant the cost of medicines ranged from Rs 7,000 (US$99.25) to Rs 18,000 (US$255.21) at each prescription renewal. For another participant, the cost of medicines was Rs 18,000 (US$255.21) to 20,000 (US$283.57) per month. Another participant spent Rs 400 (US$5.67) to 500 (US$7.09) per round of medicines. The cost of a single diagnostic test ranged from Rs 300 (US$4.25) to Rs 1,000 (US$14.18) to Rs 10,000 (US$141.78) each. A chemotherapy patient noted that the cost of each injection was Rs 47,000 (US$666.39). Costs were not just high in Delhi: One participant noted that he had already spent nearly Rs 60,000 (US$850.71) on treatment in Bihar state of India. To meet these costs (relating to diagnostic tests, operation, medicines, injections, equipment, and procedures such as dialysis), some participants had mortgaged or sold off their land.
Owing to the long waitlists in the public facility, many participants were asked to get tests done in private diagnostic facilities. In some cases, there were informal tie-ups between the facility and private MRI centers (making corruption inevitable) for diagnostics. In these cases, touts (individuals “for hire” who are paid to facilitate receipt of services) typically persuaded patients to undergo tests in private diagnostic centers. Conversely, tests conducted outside were not accepted by physicians because the required guidelines were unmet. This resulted in tests having to be retaken (at greater and in any case repeated expense) leading to additional costs and waiting time. Because participants had ceased to be employed due to illness, they gradually exhausted the major sources of support (borrowing from relatives and funding from the NGO/government), leading to impoverishment. A provider described this process: A poor man arrives at a facility and stays there till the evening, waiting. But the doctor is not there. Where does he get health services? Challenges! It would be sufficient even if he is able to enter the health system. He wants health services, which is why he mortgages. He mortgages his land. This is an instrument of pauperization. It makes a poor person poorer. The health system is an instrument for pauperization. A person who can barely manage to get his meals, is being asked for Rs10-20,000 (139.94 USD to 279.88 USD). He has fractured his bone, so he is asked to pay Rs 10–20,000. He will sell some part of his land and get poorer—Health provider, Male
Chronic Nonmedical Expenses
Because health care–seeking migrants were on long-term treatment, they had to visit the facility a few times during the year, which meant additional expenditure of travel (both intrastate
3
and interstate travel)
4
from the hometown to the city, as well as supplementary expenses on food
5
and accommodation. Delay in treatment was another factor that prolonged the duration of stay in the city, increasing nonmedical expenses as well and contributing to impoverishment. Inability to afford accommodation rendered health care–seeking migrants homeless and exposed them to vagaries of the environmental and living conditions on the streets. One health care–seeking migrant said that he got malaria while sleeping on the footpath in Delhi: I used to sleep on the footpath here. So, I got it (malaria) from the mosquito or some such thing. So, when I came here, I did not know of this place of stay (shelter). At that time, my treatment was going on at [name of hospital], so I was there (on the footpath)—Health care–seeking migrant, Male
Discussion
This study examined the health burdens, health care–seeking trajectories of health care–seeking migrants, and challenges faced seeking health care in the city. The findings listed a range of diseases, including those that affected more than one participant such as orthopedic injuries, kidney problems, tumor, and cancer, in addition to comorbidities that affected a few participants. Comorbidities have also been seen in urban poor populations in other studies (Alford et al., 2007; Sanjay et al., 2014). We conclude then that health care–seeking migrants are not necessarily facing health concerns that are drastically different from other urban dwellers, with some noteworthy exceptions, like sickle cell anemia.
This study sought to trace health care–seeking trajectories of participants in the lead up to their visit at the health facility in Delhi. The findings highlighted that recommendations given in networks as well as formal referrals shaped health care seeking. A study done in India showed that just about one tenth of people at secondary and tertiary health facilities had come through a proper referral channel (Nath et al., 2008). It was out of our scope to examine what proportion of patients followed formal referral channels; however, this is a critical area of further study.
During the analysis, while some patterns of health care seeking were identified, participants largely had distinct courses of health care seeking. A unique finding of this study was that participants followed long and complex courses of health care seeking, often seeking care at both public and private health facilities, and typically moving across levels of care, for instance from the district level to the state to the national capital—bringing to the fore the multiple facets of health care seeking. The layered pattern of health care seeking also pointed to the challenges faced in locating an appropriate health care provider on a regional level.
The findings also showed that the majority of participants relied on private facilities at some point during the course of care seeking. According to the 2014 NSS, 79% spells of ailment 6 in urban areas were treated in private facilities in India (Ministry of Statistics and Programme Implementation, Government of India, 2016). A leading reason for seeking health care in Delhi from states like Bihar and Uttar Pradesh was the paucity of quality public health care services regionally. This is consistent with findings of another study where these states reportedly have poor quality health services and inadequate specialty services (Bajpai, 2014). A study done in Rio de Janeiro showed that participants sought health care in the private sector because they perceived it as an assurance of receiving the required treatment and because of the feeling of disempowerment they felt in their interactions with doctors in the public health system (Castiglione et al., 2018). Tertiary health facilities were set up in the last decade to meet the shortfall of quality health services (“Bill on AIIMS-Like Institutes Introduced in Lok Sabha,” 2012) but have not bridged service gaps, as seen in our analysis. This concurs with another study which has noted that an expansion of services and setting up of facilities do not a priori translate into improved utilization of services (Thaddeus & Maine, 1994).
A significant reason for seeking care at a public facility in Delhi (where services are free) was health care expenditure incurred in the hometown. Numerous studies have similarly cited financial constraints as barriers to seeking health care (Angus et al., 2012; Christiani et al., 2008; Lin et al., 2015). The participants had low levels of education and were engaged in low-income occupations, which made it difficult for them to arrange for medical expenses. Thaddeus and Maine in their work on maternity care in 1994 noted that other than the quality of care, socioeconomic characteristics also shaped care seeking (Thaddeus & Maine, 1994).
Besides the economic background of the participants, expenses incurred to access private health care services aggravated their financial insecurity. This was the case with participants from Bihar who associated private health facilities with the term “loot.” This is consistent with findings of another study done on African migrants in China that showed that doctors were motivated by profit generating to the exclusion of care giving (Lin et al., 2015).
The challenges faced by participants in the health system did not stop in the hometown but extended to their experience at the public facility in Delhi. This study highlighted issues of access such as the routine problem of long queues, also seen in another study in a slum settlement in Delhi (Barua & Pandav, 2011). Another study done in Rio de Janeiro showed that the even while appointments were scheduled weeks in advance, the doctor was absent on the day of the appointment (Castiglione et al., 2018).
An interesting finding of the study was the role played by politicians in enabling easier and faster access at the facility. This squares largely with the findings of another study that found that individual political activism in Lebanon played a role in enabling better health care access, especially for low-income individuals (Chen & Cammett, 2012). Another study in the rural Ashanti region of Ghana noted the role of local political leaders in arranging for the transport of sick people to hospitals (Amoah et al., 2018). We found in our study that political connections matter in urban areas as well.
Our findings additionally highlighted the bureaucratic problems of paperwork. A study conducted on homeless and drug-using youth in Los Angeles, California, found that bureaucratic procedures required the participants to go back and forth between multiple health care providers to receive care (Christiani et al., 2008). Another highlight was the impact that the lack of possession of documentation such as BPL card and Aadhaar had on the treatment process. Other studies have also shown that some people unjustifiably get excluded from getting the BPL card, thus depriving them of access to subsidized health services (Ahankari et al., 2017; Bajpai et al., 2017). This study additionally showed that even people possessing a BPL card found it tough to finance revision surgeries because of the criterion of one-time grants, leading to delays in treatment.
The findings of this study described the various contours of delayed health care access. Delayed treatment had a critical bearing on the life of patients, a significant finding of this study. Thaddeus and Maine put forward a model of three delays in health care that typify public health systems in developing countries. The delays are in (a) deciding to seek care, (b) arriving at facilities, and (c) the provision of appropriate care (Thaddeus & Maine, 1994). The decision to seek care for the participants we interviewed arose at fairly advanced stages of disease (sometimes due to late diagnosis). For these and additional reasons (see Figure 1), we found a feedback loop between the third and second delays that were affected by aspects of facility access and quality of care. Aspects like wait times, complicated administrative procedures, and recurrent costs/malpractice meant that treatment was often delayed. Many of our participants suffered from chronic or debilitative diseases that worsened due to misdiagnosis and more so due to long waiting list for diagnostics and operations magnifying the problem of delays. Patients had no option but to get tests done at private centers, but they often lacked the money for this. And so, health would worsen as would economic status.
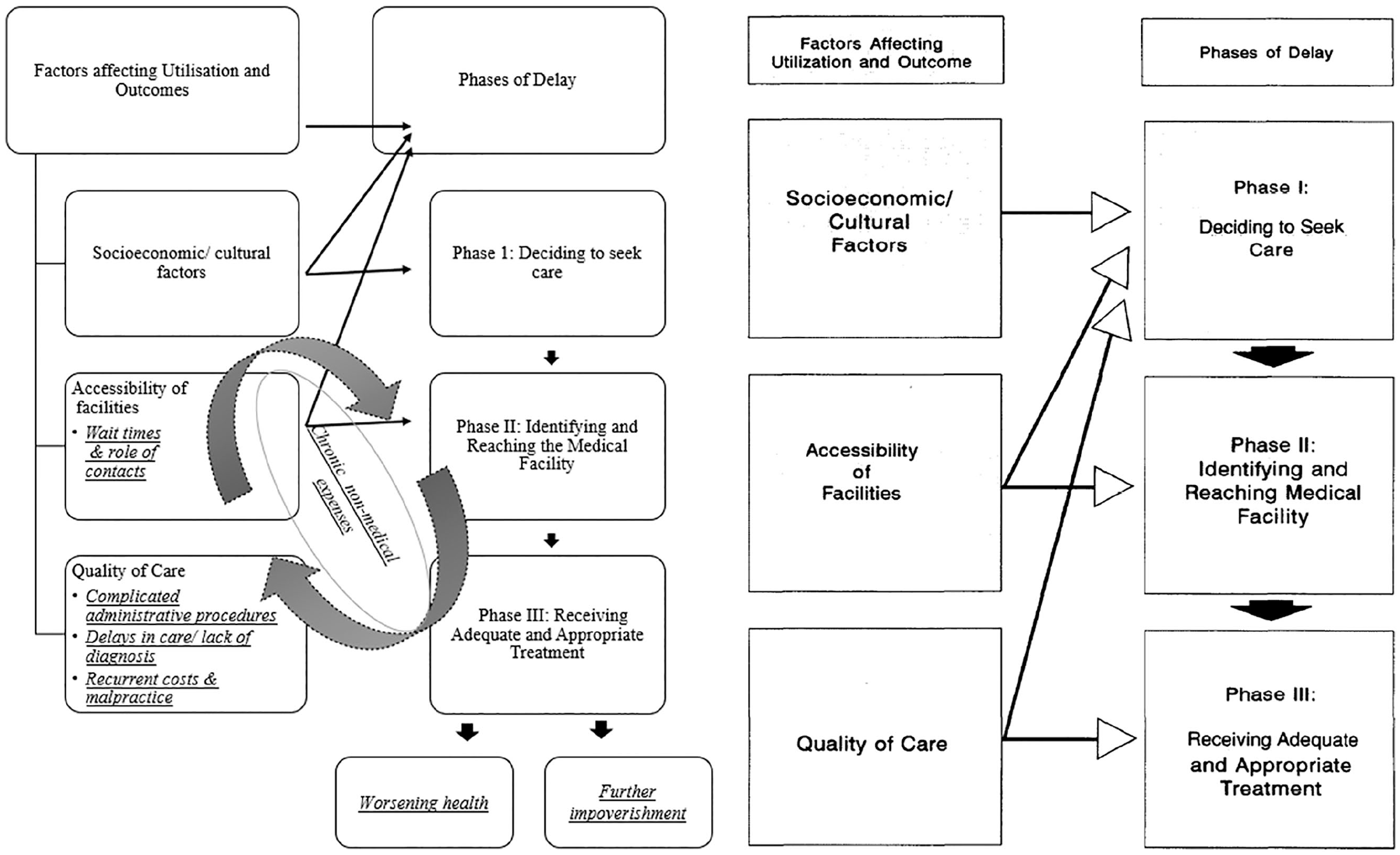
Iterative delays in health care seeking among health care–seeking migrants, as shown in Part A.
While health care–seeking migrants came to a government facility in Delhi with the hope of getting free treatment, they often ended up paying for treatment procedures. Furthermore, the financial condition of some participants was exacerbated by nonhealth-related expenses, to the point they ended up on the footpath unable to afford rent payment. This has also been commented upon by those in the profession (Khan, 2018).
Other studies have highlighted the high out-of-pocket expenditure on health care and the resultant impoverishment (Berman et al., 2010; Bhojani et al., 2012). The incidence of impoverishment resulting from out-of-pocket health expenditure is more than 4% in India (Wagstaff et al., 2018). While most studies look at impoverishment and out-of-pocket expenditure using quantitative measures, this initial qualitative exploration of the nature of catastrophic expenditure can help to identify how this phenomenon progresses and what entry points there may be to redress it. This is a major area of further research.
The findings of this study showed that while access to and quality of health care in the hometown forced people to seek health care in Delhi, the issues of access ranging from long queues to the lack of identification continued to be hindrances in getting care at the public facility in Delhi. This study also delved into the specifics such as the role of political connections and the relation between social determinants of health and delayed treatment.
This study may be important both from the point of view of migration studies (see, for example, Bhattacharya, 1998; de Haan, 1997), especially considering the fact that they come to the city for an unfixed duration, and studies on urban, underserved populations (Bam et al., 2014; Daiski, 2007; Kim et al., 2013).
To our knowledge, this is the first study conducted on health care–seeking migrants, a subgroup that needs to be included in urban health policymaking. This population is among those at risk of poor health and impoverishment from health care seeking, a major barrier to the attainment of universal health coverage identified in literature (Adams et al., 2018). There is more toward ensuring universal access to health care to include health care–seeking migrants, but research with them is an important first step. For instance, our study sheds light on a particular group of “temporary migrants” identified in the NUHM, for whom health is a central concern. This group should be identified in future policy work on urban health. Health care–seeking migrants in fact share many challenges with other urban groups—including waiting times problems with medical and nonmedical costs and so on (Ministry of Health and Family Welfare, Government of India, 2014; Nambiar et al., 2016), but also face unique challenges specifically related to delayed care seeking at the tertiary level. Procedures and care seeking is expensive in these cases, and the reliance on the private sector drives health care–seeking migrants ever closer to impoverishment. Quite often, moreover, their health status is debilitating to begin with, exacerbated by treatment delays, and worsens in the course of health care–seeking migration. Policy measures to remedy this may include ready or subsidized access to diagnostics as has been made available at the primary care level, and the possibility of support for nonmedical expenses (like sanitation, shelter, and food) for migrant patients at subsidized costs or gratis through the support of charitable institutions. Further review of effective policy measures, perhaps drawing from the situation of other countries, may prove useful in developing this.
Limitations
The study had several limitations. First, this study focused on health care–seeking migrants seeking care at a single, tertiary-level public sector hospital in Delhi. It is, therefore, not generalizable to other contexts, for primary health care seeking, or even to cities in India where health migration may be occurring. Our submission is that the uniqueness of this facility is an important factor in understanding the nature of health migration—for which this particular facility was a big draw. Second, we did not get a systematic breakdown of out-of-pocket expenditure, as participants were unable to remember the precise estimate. Third, we did not enquire about the possession of insurance cards or Rashtriya Swasthya Bima Yojana (RSBY) to participants, although this also did not come up spontaneously in any of our interviews even as RSBY has been in existence for many years and ought to have been availed for many conditions discussed. Fourth, we were unable to speak to an equal number of men and women because of the high refusal rate of the latter. This suggests there may be a gender dimension to care seeking in the population that we need to be mindful of from a research ethics standpoint but also in relation to the topic of health migration. Another limitation of this study is that we were not always able to connect individuals to support which is both ethically problematic and points to the need for further inquiry on the ethics of research with highly vulnerable urban populations. Finally, we had also wanted to speak to the health care–seeking migrants multiple times, but their duration of stay was not fixed. They had to go back and forth between their hometown and Delhi for treatment. In the future, more nimble research study designs—perhaps drawing from the discipline of migration studies—may allow for such an analysis.
Conclusion
This study is among the first to qualitatively examine the characteristics, health care–seeking trajectories, and challenges of health care–seeking migrants in India. Many of the challenges faced by health care–seeking migrants are ones that are shared with other groups in the country; however, we found that there are variegated paths to health care seeking which are characterized by delays in service utilization, progression of disease, and cost escalation.
The challenges associated with health care seeking had become an inextricable part of the lives of health care–seeking migrants, while they sought to work a way around it. Social determinants of health such as costs of food, housing, and travel added an additional layer of problems, showing the varied set of challenges affecting the health care–seeking migrants. Thirteen years since the launch of the National Rural Health Mission (NRHM) and 5 years since the launch of the NUHM, there is clearly a need for the urban health care reform agenda to acknowledge and cater to those migrating for health.
Footnotes
Acknowledgements
The authors thank Jyotsna Negi, Madhuri Dutta, Hari Sankar, and Kamalini Mukhopadhyay for their insightful comments and feedback. The authors acknowledge the Public Health Foundation of India for administrative support and their nongovernmental organization partner Centre for Equity Studies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Indian Council of Social Science Research (grant number G-38/2015-16/ICSSR/RPS).
1.
“Usual place of residence (UPR) of a person was defined as a place (village/town) where the person had stayed continuously for a period of six months or more” (Ministry of Statistics and Programme Implementation, Government of India, 2010, p. 22).
2.
“Aadhaar number is a 12-digit random number issued by the [Unique Identification Authority of India] UIDAI (‘Authority’) to the residents of India after satisfying the verification process laid down by the Authority. Any individual, irrespective of age and gender, who is a resident of India, may voluntarily enrol to obtain Aadhaar number . . . Aadhaar is a strategic policy tool for social and financial inclusion, public sector delivery reforms, managing fiscal budgets, increase convenience and promote hassle-free people-centric governance” (Unique Identification Authority of India, Government of India, n.d.).
3.
Travel from the railway station in Delhi to the facility was also cited as a notable expense.
4.
Subsidized train fare was available for limited ailments like cancer, thalassemia, and dialysis (Ministry of Railways, Government of India, n.d.). Yet some health care–seeking migrants had ineligible conditions, while others did not know about the subsidies; this added to the nonhealth-related expenses.
5.
Participants were reliant on food that was distributed by nongovernmental organizations as well as religious and nonreligious charitable trusts. However, participants reported that there were occasions when they were not able to get food from these sources.
6.
A spell of ailment is defined as “a continuous period of sickness due to a specific ailment” (Ministry of Statistics and Programme Implementation, Government of India, 2016).