
Abstract
Vaccines are some of the most cost-effective public health interventions for reducing disease burden and mortality. However, in recent years, health systems have faced a growing challenge with increasing number of parents who choose not to vaccinate their children. This decision has important implications for the health of communities worldwide, and despite a considerable amount of research that reinforces vaccine effectiveness and safety, there is uncertainty surrounding the factors that may encourage vaccine hesitancy in parents. In this interpretive review of 34 qualitative studies, we examine the factors that bolster vaccine hesitancy, rejection, and delay, and identify the overlaps and relationships between these factors. We depict our findings using the metaphor of a gear train where each gear represents one of seven factors: previous experiences; “natural” and “organic” living; perceptions of other parents; experiences interacting with health care providers; information sources, challenges, and preferences; distrust in health system players; and mandatory vaccine policies.
Keywords
Introduction
Vaccines are a key part of health care systems worldwide. Their successful administration aids in containing the spread of disease which may otherwise be harmful or even deadly to citizens, especially those with compromised immune systems (Andre et al., 2008). Vaccination has proven to be extremely effective in preventing infectious diseases. For example, the World Health Organization (WHO, 2017) estimated that vaccines prevented 10 million deaths between 2010 and 2015 worldwide.
Vaccination is one of the most cost-effective public health interventions for reducing disease burden and mortality. Ortega-Sanchez et al. (2008), for example, estimated that the meningococcal vaccine saved the United States government US$551 million in direct costs and US$920 million in indirect costs from 1993 to 2002. Similarly, Ray et al. (2006) reported that the pneumococcal vaccine prevented 38,000 cases of disease within its first 5 years of use with an estimated US$112,000 cost per life saved in the United States. When considering the effects of herd immunity, an additional 109,000 cases were prevented (Ray et al., 2006).
Although vaccines have been key drivers of disease prevention and cost containment, there is an increasing number of citizens, including parents of young children who are foregoing vaccination. For example, a 2017 National Immunization Survey by the United States Centers for Disease Control and Prevention (CDC) found that the number of fully unvaccinated children increased from 0.3% to 1.3% in one year (Jenco, 2018). These parents commonly report hesitancy and reluctance toward vaccines. The SAGE working group on vaccine hesitancy defined it as the “delay in acceptance or refusal of vaccination despite [the] availability of vaccine services” (MacDonald, 2015, p. 4161). However, other scholars have recognized that even parents who accept vaccines may also express some hesitancy (P. McDonald et al., 2019).
Vaccine hesitancy has existed since the introduction of vaccines for disease prevention. While it has evolved over time, the foundational arguments—questioning the safety and efficacy of vaccines—persist today. Schwartz (2012) explains how vaccine hesitancy is a natural outcome of vaccine introduction because as vaccines reduce the prevalence and incidence of disease, patients, parents, and even many health care professionals have little firsthand familiarity with the diseases that vaccines prevent . . . the benefits of vaccines are then difficult to discern, while the risks . . . become comparatively more visible. (p. 51)
As a result of increasing cases of parents who reject or delay vaccines, children have become more susceptible to acquiring vaccine-preventable disease. Recently, the WHO reported a 30% increase in the number of measles cases between 2016 and 2017 globally that could be attributed to vaccine hesitancy (The Lancet Child & Adolescent Health, 2019). Media reports of measles outbreaks in large metropolitan cities have increased; these reports also associate outbreaks of vaccine-preventable disease with the rising prevalence of vaccine hesitancy (Canadian Broadcasting Corporation, 2019). On September 5, 2019, the CDC reported 1,241 cases of measles, the largest number of cases in the United States since 1992 and more than a 300% increase in the number of cases from 2018 (CDC, 2019).
Previous research has identified various reasons that may explain the rise of vaccine hesitancy. Smith (2017) reported common misconceptions in vaccine-hesitant parents such as a belief that vaccines are toxic, natural immunity is better for young children, and that there is collusion between health care providers and pharmaceutical companies. Dubé et al. (2018) reviewed 22 qualitative studies using the socioecological framework to depict the multiple factors that may contribute to vaccine hesitancy: experiences, emotions, ways of thinking, information sources, family and friends, perceptions of disease risk, and trust in health care systems. At the same time, other research reinforces the idea that vaccine decision-making is complex and multifaceted (Dubé et al., 2016). Each parent rationalizes vaccine hesitancy uniquely, and different interventions may be effective for addressing diverse values and beliefs underlying vaccine rejection, delay, or hesitancy.
Multiple primary studies have been published that identify the rationales parents may use to make decisions about vaccines for their children. The study published by Dubé et al. (2018) is a useful resource for policy and practice because it comprehensively lists the factors that may encourage vaccine hesitancy. However, to our knowledge, no review has provided a theoretical interpretation of vaccine-hesitant parents’ decision-making. The objective of this study is to examine the factors that bolster vaccine hesitancy and identify some overlaps and relationships between these factors. We do this by examining how parents navigate the vaccination decision-making process for their children and infants.
Method
Searching, Screening, and Extracting Data
In this review, we adopted a systematic search that adapted the strategy documented in a previously published review on the decision-making process of vaccine-hesitant parents (Dubé et al., 2018). In addition to the articles included in that previous review, we conducted an updated search on June 23, 2019 in the same databases. Our search strategy for MEDLINE is available as a supplementary file (Supplementary File 1).
We conducted initial screening to obtain potential articles eligible for inclusion. After reviewing titles and abstracts, we reviewed the full text of potentially eligible articles to further assess their eligibility. We aimed to find articles that examined how parents (mothers and fathers) navigated the vaccination decision-making process for their children or infants on common childhood vaccines. We retrieved descriptive characteristics from included studies. The eligibility criteria, descriptive characteristics and analysis, and our approach to quality appraisal can be found in Supplementary File 1.
Data Analysis
We employed the qualitative research integration methodology to analyze included studies (Sandelowski & Barroso, 2003). This methodological framework integrates findings from multiple, qualitative studies to produce a new interpretation of the phenomenon while also retaining important elements of original study findings. Building a conceptual model from multiple articles renders findings with a greater number of participants and wider range of dimensions than any one article alone (Harden et al., 2004; Mays et al., 2005). Primary data for this review were authors’ conclusions and assertions. However, the original excerpts were also extracted to support primary data where possible.
We performed multiple iterative cycles of coding by hand informed by constructivist grounded theory and the constant comparative method (Charmaz, 2014). In the first cycle, we conducted open coding of five articles to understand the types of themes, categories, and concepts represented in the included literature. Both authors coded the same five papers independently, outlined their preliminary thoughts in an analytic memo, and then discussed their coding. At this point, we formulated a preliminary coding schema consisting of themes from the initial five articles. We then applied the preliminary coding schema to the remaining articles. After reviewing all articles, we conducted focused coding. We used line-by-line, concept-by-concept, and section-by-section analyses to identify the dimensions of themes and categories represented in the coding schema as well as the underlying meaning and context of findings (Charmaz, 2014; Saldaña, 2015). Then, we produced narrative summaries for each theme that UM synthesized to form an integrative summary of the topic.
Results
Through database searching and reviewing the articles from Dubé et al. (2018), we identified 619 relevant hits, of which 120 were duplicates. We screened 499 articles for relevance and eligibility and excluded 429. We then reviewed the full text of 80 articles and excluded 46 for various reasons associated with methodology and relevance. In total, 34 articles were included in this analysis representing 32 distinct studies. Supplementary File 1 contains a PRISMA diagram showing the article screening process.
Interpretive Findings
Parents in included studies described a myriad of reasons that encouraged them to forego vaccinating their young children. However, the reasons for vaccine hesitancy or refusal were unique for each parent. On one hand, parents delayed some vaccines because they were incompatible with their organic, natural way of living. On the other hand, parents chose to delay other vaccines because of their previous experiences with vaccine side effects. Parents also wanted to better understand vaccine schedules and administration by searching for information about vaccine safety and efficacy from a variety of sources. However, some parents refused vaccines altogether if they encountered contradictory information that raised the ambiguity in making a vaccination decision. These examples show how parents might prioritize distinct reasons to not vaccinate their children. These examples also show a need to better conceptualize the various reasons for rejecting or delaying vaccines.
In the following sections, we discuss how different factors encourage vaccine hesitancy. We have visually depicted the interrelations between these factors using the metaphor of a gear train comprising seven gears (Figure 1). Each gear represents one of the following factors: previous experiences; “natural” and “organic” living; perceptions of other parents; experiences interacting with health care providers; information sources, challenges, and preferences; distrust in health system players; and mandatory vaccine policies. Although some reasons may be prioritized over others, we believe that parents continue to reflect on the reasons most relevant to their decision-making context. We use reasons as the predominant term to refer to the different factors that promote vaccine hesitancy, and we use rationales to indicate the combination of reasons that encourage each parents’ vaccine decision. While we believe that there are a limited number of reasons that parents may use, the rationales for each parent is unique.
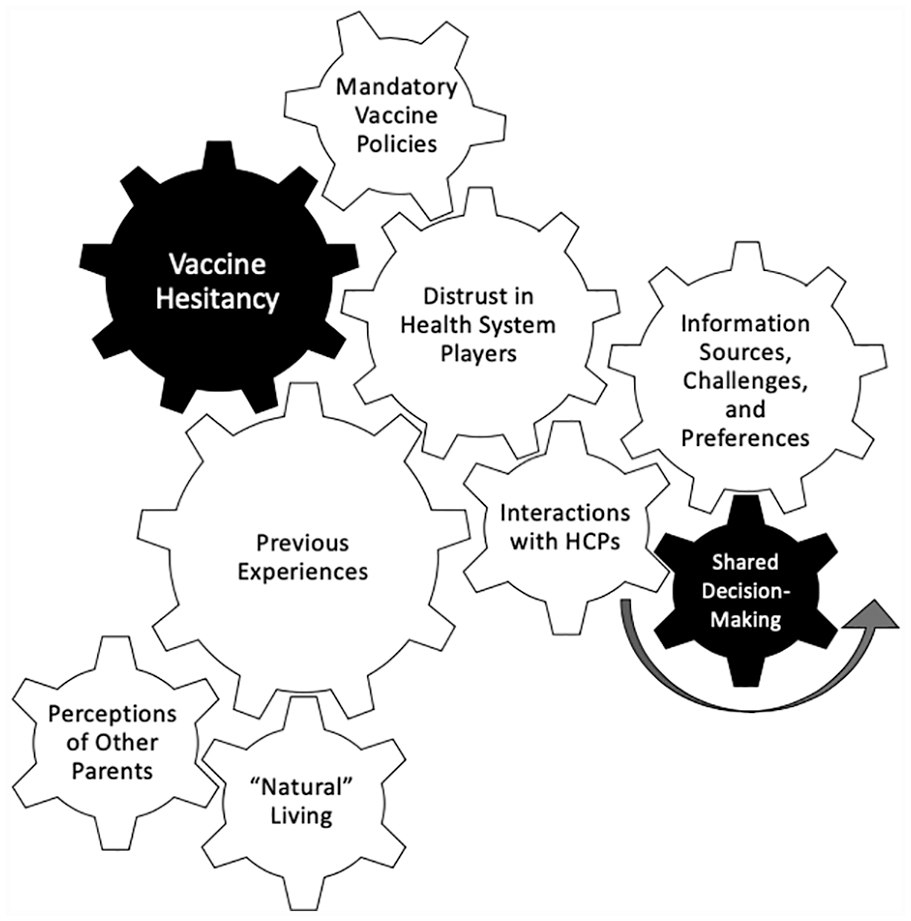
A gear train depicting the overlap between factors that promote vaccine hesitancy.
We use a gear train as a metaphor to enhance our understanding of vaccine hesitancy. Metaphors may be used in qualitative research to illuminate the experiences and perspectives of individuals or to provide a new perspective to view the phenomenon of interest (Carpenter, 2008). Metaphors can also be transferred within or between disciplines (Walker & Avant, 2005). However, our use of the gear train is not meant to derive exact conclusions regarding whether or not each parent would reject or delay a vaccine depending on their reasons or rationales. We believe that such conclusions are challenging to make because rationales are unique to each parent’s philosophy and experiences vis-à-vis vaccines. Instead, our metaphor intends to improve our understanding and display of parents’ perspectives and experiences.
According to the physical sciences discipline, the gear train moves as a system. Although there may be multiple gears in the gear train, when a force is applied to one gear, all other gears will rotate but at different rates. In our figure, there are two types of gears: input gears (i.e., gears where an initial force is applied to cause rotation) and output gears (i.e., the final gear that receives the force applied by input gears). Input gears comprise the seven factors that promote vaccine hesitancy and the shared decision-making (SDM) gear. Larger gears with more “teeth” will exert more force on the entire system; similarly, certain factors that promote vaccine hesitancy may have greater significance for some parents. The size and number of teeth of each factor was determined by the extent to which they were discussed in the included literature.
The gear train metaphor shows that when one factor is prioritized, other factors also serve important roles in encouraging parents to delay or reject vaccines. All factors are somehow connected to each other through the gear train, even if they are not linked directly. Similarly, there are numerous connections and combinations between gears referring the compendium of ways parents can rationalize their decision to forego vaccinations.
Previous Experiences
Fear of vaccine side effects
Parents in multiple studies expressed a belief that vaccines are unsafe and dangerous (Alstyne et al., 2018; Austvoll-Dahlgren & Helseth, 2010; Blaisdell et al., 2016; Dubé et al., 2016; Enkel et al., 2018; Helps et al., 2019; Meleo-Erwin et al., 2017; Senier, 2008), and that they can have permanent, long-lasting adverse effects on their children’s adult life (Blaisdell et al., 2016; Enkel et al., 2018; Senier, 2008; Swaney & Burns, 2019). Parents were particularly concerned about the unintended long-term side effects of vaccines that they believed were unknown to health care providers (Alstyne et al., 2018; Carrion, 2018; Harmsen et al., 2013; McCoy et al., 2019; Meleo-Erwin et al., 2017; Senier, 2008; Wilson et al., 2008). In a number of studies, parents reported a fear of the following side effects that they believed to be associated with vaccines: asthma, allergies, fever, fuzziness, febrile seizure, multiple sclerosis, articular rheumatism, and neurodevelopmental disorders (Alstyne et al., 2018; Carrion, 2018; Peretti-Watel et al., 2019; E. Wang et al., 2015; Wilson et al., 2008). The most feared side effect was autism, mentioned in 10 studies (Alstyne et al., 2018; Hatoková et al., 2018; Helps et al., 2019; McCoy et al., 2019; P. McDonald et al., 2019; Peretti-Watel et al., 2019; Senier, 2008; Swaney & Burns, 2019; E. Wang et al., 2015; Wilson et al., 2008). Parents in one study feared autism because of the drastic personality change that it may cause in their children: . . . He’s just so charming, and he’s so full of love, and he really makes people happy, even strangers . . . And the thought that, you know, that personality could get turned off [from vaccines] is horrible. (Senier, 2008, p. 220)
Fear of long-term side effects was often associated with the belief that vaccines will overwhelm their child’s underdeveloped immune systems (Alstyne et al., 2018; Hatoková et al., 2018; P. McDonald et al., 2019; Reich, 2014; Vandenberg & Kulig, 2015; Wilson et al., 2008). This belief was often accompanied with the idea that children already receive too many vaccines (Harmsen et al., 2013; McCoy et al., 2019; Meleo-Erwin et al., 2017; Swaney & Burns, 2019).
Parents also believed that children are extremely sensitive to the properties and chemicals in vaccines (Blaisdell et al., 2016; Enkel et al., 2018; Harmsen et al., 2013; P. McDonald et al., 2019; Reich, 2014; Senier, 2008; Vandenberg & Kulig, 2015; E. Wang et al., 2015). In four studies, parents mentioned that they feared adverse reactions from the mercury content of vaccines (Alstyne et al., 2018; P. McDonald et al., 2019; Vandenberg & Kulig, 2015; Wilson et al., 2008). Other chemicals that were particularly problematic for parents included formaldehyde, aluminum, animal DNA, thimerosal, and human tissue (Alstyne et al., 2018; Vandenberg & Kulig, 2015; E. Wang et al., 2015). Parents who mentioned that children were sensitive to vaccine properties also suggested that a one-size-fits-all approach does not work for every child (P. McDonald et al., 2019; Reich, 2014; Senier, 2008; Sobo et al., 2016). These parents believed that vaccination schedules are rigid and unresponsive to the unique needs of each child (Reich, 2014; Senier, 2008). In six studies, parents expressed that flexibility in vaccination schedules may encourage vaccination by spacing out vaccines and avoid overwhelming their child’s underdeveloped immune system (Alstyne et al., 2018; Enkel et al., 2018; Hatoková et al., 2018; Helps et al., 2018; Reich, 2014; E. Wang et al., 2015): I probably would have followed an alternate schedule if it had been an option just cause I think spacing them out I think, and this is a crazy decision I guess, there isn’t really evidence suggesting it is more healthy or less healthy but probably, I don’t know, in my mind it seems like a better idea to space them out. (E. Wang et al., 2015, p. 6706)
In 23 studies, parents described how they perceived that the risk of adverse side effects from vaccines to be higher than the risk of acquiring vaccine-preventable disease (Attwell, Meyer, & Ward, 2018; Attwell, Ward, et al., 2018; Blaisdell et al., 2016; Dubé et al., 2016; Enkel et al., 2018; Gullion et al., 2008; Harmsen et al., 2013; Hatoková et al., 2018; Koski & Holst, 2017; McCoy et al., 2019; P. McDonald et al., 2019; Meleo-Erwin et al., 2017; Painter et al., 2019; Peretti-Watel et al., 2019; Reich, 2014, 2018; Senier, 2008; Sobo et al., 2016; Swaney & Burns, 2019; Vandenberg & Kulig, 2015; E. Wang et al., 2015; Ward et al., 2017, 2018). This belief was conflated with three ideas. First, parents claimed that vaccine-preventable diseases were easily treatable (Attwell, Ward, et al., 2018; Blaisdell et al., 2016; Painter et al., 2019; Sobo et al., 2016; Vandenberg & Kulig, 2015). Under this idea, parents believed that they were capable of identifying the symptoms of vaccine-preventable disease and administering treatment themselves (Attwell, Ward, et al., 2018; Blaisdell et al., 2016; Harmsen et al., 2013; Reich, 2014; Ward et al., 2017). This idea was often bolstered by parents’ self-confidence in knowing their child’s unique health care needs better than anyone else: [I’m] a parent who is very in tune with their child, you know, I’m gonna know that something is wrong. I feel like if they’re coming down with an illness, I have that mother’s instinct. I’m so in tune with my kids I can tell they’re sick, before they show any symptoms. (Blaisdell et al., 2016, p. 484)
Second, parents also insisted that vaccine-preventable diseases have less severe side effects than vaccines (Enkel et al., 2018; Gullion et al., 2008; Hatoková et al., 2018; P. McDonald et al., 2019; Reich, 2014; Swaney & Burns, 2019; Vandenberg & Kulig, 2015). This idea caused parents to reduce their perceived severity of vaccine-preventable conditions: . . . every single person had chicken pox and never once was anybody hospitalized. We all had it; I just can’t take seriously the idea that this is that dangerous a disease that we need to mess with it. (Senier, 2008, p. 216)
In general, vaccine-hesitant parents overemphasized their subjective risk judgments to maximize the risk of vaccinations while at the same time minimize the risk of vaccine-preventable diseases to support their decision to not vaccinate (Blaisdell et al., 2016; Dubé et al., 2016; Helps et al., 2018, 2019; Miller et al., 2008). Supporting their decision to forego vaccines, parents often exaggerated risks of vaccine side effects to be 100%, fixated on the rarer side effects of vaccines, or advanced their belief that vaccine-preventable diseases no longer existed in their communities precluding the need to vaccinate in the first place (Hatoková et al., 2018; Peretti-Watel et al., 2019; Swaney & Burns, 2019).
Finally, parents also advanced the idea that acquiring vaccine-preventable disease was an important part of their children’s natural growth (Attwell, Meyer, & Ward, 2018; Attwell, Ward, et al., 2018; Harmsen et al., 2013; Koski & Holst, 2017; P. McDonald et al., 2019; Miller et al., 2008; Reich, 2018; Vandenberg & Kulig, 2015; Wilson et al., 2008). The “body as a temple” metaphor was evident in multiple studies, emphasizing that natural immunity was the strongest protection against all infections and that vaccine-preventable diseases were essential for children to develop lifelong immunity to these infections. As one parent responded to another’s comment on an online discussion forum about chicken pox: I wish we lived closer and I could come over for a chicken pox party! I hope you can see that this is a good thing to have and that it will give your daughter lifelong immunity and strengthen her immune system. (Reich, 2018, p. 5)
Although there are thousands of viruses and bacteria that contribute to children’s immune system, parents fixated on the idea that vaccines fully prevent their children from strengthening their immune system (Koski & Holst, 2017).
Skepticism of vaccine effectiveness
In seven studies, parents were adamant in their belief that vaccines were ineffective in reducing the incidence of vaccine-preventable diseases (Alstyne et al., 2018; Dubé et al., 2016; McCoy et al., 2019). This belief was reinforced by the perceptions that vaccines do not cover all viruses and bacteria (Dubé et al., 2016), do not provide lifelong protection because they require continuous booster shots, viruses mutate quickly, and there are still outbreaks of vaccine-preventable diseases despite the high uptake of vaccines (Harmsen et al., 2013; P. McDonald et al., 2019; Ward et al., 2017; Wilson et al., 2008).
Parents in four studies were skeptical of the effectiveness of herd immunity (Helps et al., 2018; P. McDonald et al., 2019). In some cases, parents did not fully understand herd immunity or did not completely appreciate that vaccines are meant to primarily prevent disease at the community level for children who are at a higher risk of acquiring vaccine-preventable disease (Swaney & Burns, 2019). On the contrary, parents in one study believed in the validity of herd immunity but regretted its existence because it would prevent their children from “naturally” strengthening their immune system by getting vaccine-preventable diseases (Harmsen et al., 2013).
“Natural” and “Organic” Living
Multiple vaccine-hesitant parents lived in environments that reflected an “off the grid” philosophy that was also labeled as a “constant vigilance” toward lifestyle choices (Alstyne et al., 2018; Attwell et al., 2017; Attwell, Meyer, & Ward, 2018; Attwell, Smith, & Ward, 2018; Blaisdell et al., 2016; Carrion, 2018; Dubé et al., 2016; Gullion et al., 2008; Harmsen et al., 2013; Hatoková et al., 2018; Helps et al., 2018; McCoy et al., 2019; Peretti-Watel et al., 2019; Reich, 2014, 2018; Senier, 2008; Sobo et al., 2016; Swaney & Burns, 2019; Vandenberg & Kulig, 2015; Ward et al., 2017, 2018). This philosophy included eating organic foods, cooking homemade meals, avoiding frozen foods, avoiding food preservatives, growing vegetables at home, and using filtered rain water (Attwell, Smith, & Ward, 2018; Carrion, 2018; Helps et al., 2019; Peretti-Watel et al., 2019; Reich, 2018; Sobo et al., 2016; Ward et al., 2018). In addition, this organic lifestyle also influenced routine behaviors and daily life activities, for example, having healthy sleep cycles, using glass instead of plastic to drink water, using wooden instead of plastic toys, minimizing screen time, having regular exercise, avoiding cleaning products, getting adequate sunshine, and using natural sunscreen (Helps et al., 2018, 2019; Peretti-Watel et al., 2019; Ward et al., 2017, 2018).
Parents used their natural and organic way of living to guide their health care preferences. Generally, parents rejected biomedicine and avoided taking medications (Attwell, Meyer, & Ward, 2018; Carrion, 2018; Hatoková et al., 2018; Reich, 2018; Vandenberg & Kulig, 2015). This way of living was often accompanied by a belief that Western medicine produces nonnatural medications that compromise children’s bodies (Attwell, Ward, et al., 2018; Helps et al., 2018; Koski & Holst, 2017; P. McDonald et al., 2019; Meleo-Erwin et al., 2017; Vandenberg & Kulig, 2015; Ward et al., 2018). This way of living also promoted a belief that taking pills creates a “perpetual cycle of sickness” (Attwell, Ward, et al., 2018; Helps et al., 2019; Ward et al., 2017): “it’s just been perpetual, like going to the doctor, going to the hospital, having surgeries trying . . . to fix things” (Attwell, Meyer, & Ward, 2018, p. 1623).
Parents preferred treatments that used natural products such as herbal teas and essential oils (Hatoková et al., 2018; Helps et al., 2019; McCoy et al., 2019; Peretti-Watel et al., 2019; Reich, 2018; Swaney & Burns, 2019; Ward et al., 2017). For parents who used both allopathic and complementary/alternative medicine, they reported having higher confidence in natural products, home remedies, vitamins, probiotics, and food choices in treating disease (Attwell, Meyer, & Ward, 2018; Attwell, Ward, et al., 2018; Attwell, Smith, & Ward, 2018; Koski & Holst, 2017; P. McDonald et al., 2019; Alstyne et al., 2018). Due to a preference for natural treatments, parents viewed vaccines as incompatible with their natural lifestyle because they were composed of artificial ingredients (Carrion, 2018; Helps et al., 2018; Ward et al., 2017). In one study, parents described how information from allopathic medicine on “natural health” contradicted vaccination: I’m going “I don’t know,” cause all the doctors are telling me that I’m only supposed to give my baby breast milk—like “breast milk is the be all end all, don’t give formula to your baby, don’t do this, don’t do that.” And then I’m gonna inject all these things into my baby? And it was just kind of this—I don’t understand how these two things go together. (Carrion, 2018, p. 2190)
Another component of the natural lifestyle was the approach to parenting that included natural births, long-term breastfeeding, and avoiding baby formula (Attwell, Ward, et al., 2018; Carrion, 2018; Helps et al., 2018, 2019; Reich, 2014, 2018; Sobo et al., 2016; Swaney & Burns, 2019; Ward et al., 2017, 2018). In general, this approach was prompted by the perception that disease strengthens immune systems at a young age (Attwell, Ward, et al., 2018; Blaisdell et al., 2016; Dubé et al., 2016; Harmsen et al., 2013; Koski & Holst, 2017; McCoy et al., 2019; P. McDonald et al., 2019; Miller et al., 2008; Senier, 2008; Vandenberg & Kulig, 2015; Wilson et al., 2008). Parents in seven studies expressed a high confidence in the power of breastfeeding to enhance their child’s natural immunity, thereby foregoing the need to vaccinate (Attwell, Meyer, & Ward, 2018; Attwell, Ward, et al., 2018; Helps et al., 2018; Reich, 2014; Sobo et al., 2016; Swaney & Burns, 2019; Ward et al., 2017). These behaviors prompted parents to believe that having healthy kids who are not consistently sick and also adopted healthy, organic lifestyles reduced the risk of infections and also the need for vaccination (Alstyne et al., 2018; Attwell, Meyer, & Ward, 2018; Attwell, Ward, et al., 2018; Attwell, Smith, & Ward, 2018; Carrion, 2018; Harmsen et al., 2013; Helps et al., 2019; Koski & Holst, 2017; Senier, 2008; Vandenberg & Kulig, 2015; Ward et al., 2018). However, it is important to note that parents’ preconceptions of a healthy environment also included limiting exposure to “external threats” (Attwell, Smith, & Ward, 2018; McCoy et al., 2019; Swaney & Burns, 2019; Ward et al., 2017), which involved isolating children from geographic areas where diseases were perceived to spread, for example, child care centres and public schools (Blaisdell et al., 2016; Harmsen et al., 2013; McCoy et al., 2019; Reich, 2014; Sobo et al., 2016). Reducing “external threats” also included avoiding long-distance traveling (McCoy et al., 2019; Ward et al., 2017, 2018). This finding is particularly interesting because it contradicts some parents’ desire to expose their children to sources of vaccine-preventable disease to strengthen their immune systems. It is important to note that not all parents who adopted an organic way of living rejected vaccines. Vaccine rejection and organic way of living were complementary in some cases because parents were able to negotiate their preconceptions of organic living to include the “artificial” nature of vaccines (Attwell, Meyer, & Ward, 2018). In other cases, parents asserted the need to introduce vaccines in a more natural way to make them more amenable to the organic way of living (P. McDonald et al., 2019; Wilson et al., 2008).
Perceptions of Other Parents
Parents who vaccinated their children expressed mixed feelings toward those who chose to forego vaccines. On one hand, these parents perceived vaccine-rejecting parents as irresponsible, “completely uninformed, uneducated, imbecilic, [and] risk takers” (Carrion, 2018; Helps et al., 2019; Reich, 2018; Swaney & Burns, 2019; Ward et al., 2017, 2018; Wilson et al., 2008). The parents who made these judgments avoided vaccine-rejecting parents to keep their children safe from exposure to vaccine-preventable disease (Enkel et al., 2018; Reich, 2014). On the flip side, vaccinating parents described how they lost close friends when they shared their views on vaccines: I brought up the moral issue of vaccinating and protecting the vulnerable members of the community, and people really didn’t like that. And that seemed to be a flashpoint for them, a cognitive dissonance . . . I was [troubled by it] at the time. (Attwell, Meyer, & Ward, 2018, p. 11)
Overall, both vaccinating and vaccine-hesitant parents preferred to interact with parents who shared their values, beliefs, and attitudes toward vaccines (Attwell, Meyer, & Ward, 2018; Reich, 2014, 2018; Ward et al., 2018). Despite this polarization of attitudes, some parents expressed the need to not exclude vaccine-hesitant parents from conversations surrounding the potential adverse outcomes of vaccine rejection and delay (Enkel et al., 2018; Helps et al., 2018). These parents often empathized with how difficult it was for parents to make a decision that would affect the health of their children and advised that health care providers should make an active effort to understand the various factors that lead to vaccine hesitancy (Helps et al., 2019; Sobo et al., 2016; E. Wang et al., 2015).
Some vaccine-hesitant parents resented being labeled irresponsible for not vaccinating their children, a decision that these parents viewed as exercising their freedom of choice (Reich, 2018; Ward et al., 2017). Other parents felt disheartened at the criticism that they were “free riders” of herd immunity that the broader community established through vaccination (Reich, 2014; Senier, 2008; Ward et al., 2018). Vaccine-hesitant parents noted that they did not want to be labeled as an “anti-vaxxer” because they perceived the label to hold an extreme negative connotation and that did not represent their values and beliefs accurately (Helps et al., 2019).
Some vaccine-hesitant parents described how they regularly interacted with parents who held strong views about vaccines. In these situations, vaccine-hesitant parents in two studies adopted a nonconfrontational strategy that focused on ignoring criticism: I think it’s to the point where we need to keep quiet about our health choices if we are not within a like-minded community. I used to feel like I was a rebel and was educating people when the subject came up . . . but now I just nod and smile if I am with a group that might not accept my views. (Reich, 2018, p. 6)
This strategy was often used to maintain existing networks. The same parents also explained how they used social media as a distant platform for engaging in conversations about vaccines to avoid stigma from their social circle (Reich, 2018). Some vaccine-hesitant parents regretted choosing to vaccinate their children previously and as a result felt that it was their duty to educate other parents to prevent them from making the mistakes they made (Reich, 2018).
Vaccine-hesitant parents also questioned the lack of questioning in vaccine-accepting parents on the pros and cons of vaccines (Reich, 2014; Wilson et al., 2008). At the same time, these parents expected respect from others for their decision to not vaccinate (Meleo-Erwin et al., 2017; Ward et al., 2018). This finding emphasizes how vaccine-hesitant parents view the vaccination decision as a personal decision: It doesn’t really matter, does it, what they think, because they’re not their children . . . They’re our children. (Ward et al., 2018, p. 1125)
This quote shows how vaccine-hesitant parents prioritize their foremost responsibility to ensure their children’s safety and health. The health of communities is not the primary reason for vaccinating in these parents, although they might acknowledge it as another parents’ reason to vaccinate.
Experiences Interacting With Health Care Providers
Parents in six studies identified how an informed discussion about both the benefits and risks of vaccines was rarely initiated by their health care provider (Miller et al., 2008; Wilson et al., 2008; Zamir & Israeli, 2017). Vaccine-hesitant parents who expressed concerns about the potential vaccine side effects felt that their health care provider did not provide the opportunity to share these concerns (Austvoll-Dahlgren & Helseth, 2010; Carrion, 2018; Sobo et al., 2016; Ward et al., 2018). Parents also described how there was a general lack of discussion about the risks of vaccines and alternative methods and schedules for administering vaccines (Helps et al., 2019).
Parents in nine studies found that health care providers who discussed the potential side effects of vaccines adopted a dismissive demeanor to parents’ concerns: I just got hit with sometimes just absolutely ridiculous statements. My GP, for example, she just told me something that if she had any scientific knowledge she never would have made the statement she made . . . and she was so rude and dismissive . . . So I was just, like—each interaction like that erodes my trust further. (Ward et al., 2018, p. 1126)
Interacting with a health care provider who exhibited a dismissive attitude prompted parents to look for health care providers who were more respectful and open to having a balanced discussion about vaccines (Peretti-Watel et al., 2019). This desire was especially apparent for parents who expressed a strong fear of judgment from their health care providers (Dubé et al., 2016; Helps et al., 2019; Sobo et al., 2016; Ward et al., 2018; Zamir & Israeli, 2017).
Parents in 14 studies felt an intense pressure from physicians and nurses to vaccinate their children (Alstyne et al., 2018; Carrion, 2018; Gullion et al., 2008; Hatoková et al., 2018; Helps et al., 2018, 2019; McCoy et al., 2019; Peretti-Watel et al., 2019; Senier, 2008; Vandenberg & Kulig, 2015; Ward et al., 2017; Wilson et al., 2008): “my experience is that they give you the [information] papers when they want you to get the shot. So, here’s a stack of ten papers, but here’s the nurse standing there with the needle” (Gullion et al., 2008, p. 406). As demonstrated by this quote, a dismissive tone was combined with an implicit pressure to vaccinate that may have reinforced their decision to not vaccinate (Dubé et al., 2016). For the majority of parents, however, this experience eroded their trust in health care providers, especially when physicians declared that they would not treat the parent and their children if they chose not to vaccinate (Dubé et al., 2016). Interestingly, parents in eight studies explained how vaccine hesitancy in their health care providers encouraged their own decision to refuse vaccines despite showing openness to full acceptance (Carrion, 2018; McCoy et al., 2019; P. McDonald et al., 2019; Meleo-Erwin et al., 2017; Painter et al., 2019; Peretti-Watel et al., 2019; Swaney & Burns, 2019; E. Wang et al., 2015): They wanted to give me a booster, and I kind of hesitated because I kind of had to think about it. I didn’t know they were going to ask me that and she was just like, “Well, I wouldn’t, we are so over vaccinated nowadays.” So anyway, I was like, “That’s interesting.” She probably could have convinced me the exact opposite way, too, at that point. (Carrion, 2018, p. 2188)
Parents desired respect from health care providers when deciding whether or not to vaccinate their children (Alstyne et al., 2018; Koski & Holst, 2017; Miller et al., 2008; E. Wang et al., 2015; Ward et al., 2017, 2018; Wilson et al., 2008). Closely linked to the desire for respect was a need for an environment that allowed for questions to be asked about the potential risks and side effects of vaccines: It’d be really nice if, like, when doctors have patients that are questioning vaccines, a lot of them are just like, “If you don’t follow the schedule then you’re stupid.” And some of them won’t even see patients that don’t follow the schedule . . . They’re not really listening to people’s concerns. (Sobo et al., 2016, p. 540)
As demonstrated by this quote, some parents preferred to interact with health care providers who listened to their concerns about vaccines. Overall, providers who exhibited a respectful demeanor during health care encounters motivated a number of parents to vaccinate their children (Carrion, 2018; Helps et al., 2019; McCoy et al., 2019; Peretti-Watel et al., 2019; Reich, 2018; Senier, 2008; Sobo et al., 2016; E. Wang et al., 2015). Suggestions for improving interactions with health care providers included locating resources for parents, speaking in an accessible language, providing an overview of how disease and vaccines work, and working with alternative medicine communities (Alstyne et al., 2018; Hatoková et al., 2018; Helps et al., 2019; Koski & Holst, 2017; Miller et al., 2008). With health care providers that created trustful, respectful, and communicative relationships, parents in 11 studies found that they were more likely to accept vaccines, or at least agreed to delayed schedules over full rejection (Carrion, 2018; Helps et al., 2019; Senier, 2008; Sobo et al., 2016; Wilson et al., 2008). For parents who delayed vaccines, a positive experience also sustained communication and engagement with health care providers that ultimately led to vaccine acceptance in the future (Helps et al., 2019).
Information Sources and Challenges
Information sources
Parents in included studies used three avenues for acquiring information about vaccines: allopathic medicine providers, complementary and alternative medicine (CAM) providers, and the media and internet.
First, information from allopathic medicine providers was viewed differently between parents who accepted all vaccines and those who delayed some. Fully accepting parents were generally more open to information provided by physicians and nurses, but at the same time less likely to discuss or question this information compared with parents who expressed some hesitancy (Dubé et al., 2016; Helps et al., 2019; Miller et al., 2008; Wilson et al., 2008; Zamir & Israeli, 2017). Conversely, vaccine-hesitant parents believed that information from physicians was one-sided, unbalanced, and biased toward the positive benefits of vaccines (Alstyne et al., 2018; Attwell et al., 2017; Austvoll-Dahlgren & Helseth, 2010; Gullion et al., 2008; Reich, 2018; Senier, 2008; Sobo et al., 2016; Vandenberg & Kulig, 2015; E. Wang et al., 2015; Ward et al., 2017).
Vaccine-hesitant parents were also concerned that information regarding vaccines was not tailored to the unique characteristics, pros, and cons of each recommended vaccine (Enkel et al., 2018). Providing information tailored to each vaccine may increase parents’ confidence in information from physicians by providing parents with details about the characteristics, rationales, and ingredients of each vaccine separately (Austvoll-Dahlgren & Helseth, 2010).
Second, vaccine-hesitant parents often relied on information from CAM providers, especially when information from allopathic medicine providers did not satisfy their information needs (Dubé et al., 2016; Sobo et al., 2016). Parents felt that it was easier to have an open and honest discussion about vaccines with CAM providers compared with physicians (Dubé et al., 2016; Sobo et al., 2016). One study found that although CAM providers promoted different views of vaccines compared with allopathic medicine providers, some discouraged vaccination by overemphasizing the potential side effects while simultaneously downplaying the potential consequences of not vaccinating (Attwell, Ward, et al., 2018).
Third, albeit parents viewed media campaigns and articles published on the internet that supported vaccines, they remained skeptical of these information sources (Attwell, Meyer, & Ward, 2018; Austvoll-Dahlgren & Helseth, 2010; Carrion, 2018; Dubé et al., 2016; Enkel et al., 2018; Gullion et al., 2008; Harmsen et al., 2013; Hatoková et al., 2018; Helps et al., 2019; Miller et al., 2008; Painter et al., 2019; Senier, 2008; Vandenberg & Kulig, 2015; Ward et al., 2017). For example, parents’ interpretation of anecdotes from parenting blogs that opposed vaccines varied from skepticism to being swayed to not vaccinate (Helps et al., 2019; P. McDonald et al., 2019). These diverse reactions show how each parent values information sources differently according to their personal conceptualizations of information reliability. By valuing some information as more meaningful than others, parents prioritize information that is aligned with their personal belief systems (Alstyne et al., 2018; Helps et al., 2019; McCoy et al., 2019; Peretti-Watel et al., 2019; Reich, 2014, 2018; Sobo et al., 2016; Swaney & Burns, 2019; Wilson et al., 2008).
Challenges in finding information
Although parents felt that they were generally informed about vaccines, they expressed confusion and cognitive overload by the quantity of information available to them (Blaisdell et al., 2016; Harmsen et al., 2013; Hatoková et al., 2018; Helps et al., 2019; Miller et al., 2008; E. Wang et al., 2015). What was particularly challenging for parents was when they had to decide on which sources of information to trust: “we searched for all kinds of information, and the problem is: there is too much and you do not know how to filter. What is an opinion, what is a fact? Who is trustworthy, who is not?” (Harmsen et al., 2013, p. 5).
Parents’ trust decreased when sources that were considered credible by the public contradicted each other. Parents felt that because information was easily accessible, information could be personally curated to create a narrative that supported any belief—positive or negative—regarding vaccines (Koski & Holst, 2017; McCoy et al., 2019; Reich, 2018; Sobo et al., 2016). This realization reinforced parents’ concerns with fully trusting any one source of information; instead, they surveyed several sources that increased quantity of information they had to manage and caused confusion.
Distrust in Health System Players
Vaccine-hesitant parents expressed a strong distrust in health care workers who heavily promoted childhood vaccines. These concerns were linked to four major “players” in the health care system: pharmaceutical companies, physicians, the government, and academic research.
There were four primary ways in which pharmaceutical companies modulated their influence on different components of the health care system. First, parents in four studies asserted that pharmaceutical companies motivated specific types of research and research questions that supported a provaccination agenda (Dubé et al., 2016; Senier, 2008; Sobo et al., 2016). Second, parents described how their physicians may have been “paid off” by pharmaceutical companies to pressure them to vaccinate their children (Attwell et al., 2017; Blaisdell et al., 2016; Vandenberg & Kulig, 2015; Wilson et al., 2008). Third, multiple examples of drug and vaccine recalls strengthened mistrust in pharmaceutical companies (Alstyne et al., 2018). In the event of a recall, parents questioned the safety of vaccines and whether comprehensive testing was being conducted before introducing them to the public (Sobo et al., 2016). Fourth, the perception that pharmaceutical companies place greater importance on maximizing profits decreased trust in pharmaceutical companies: [T]he whole pharmaceutical thing, to me it’s just a big money making scheme . . . They’re a business. They make money from people being sick, so they don’t want to find a cure for this or that, because that means people won’t rely on their drugs to help them get through their disease, or whatever it is that’s making them sick. (Attwell et al., 2017, p. 70)
Vaccine-hesitant parents in five studies strongly distrusted the government and health care providers and perceived them to have strong ties with pharmaceutical companies (Blaisdell et al., 2016; Helps et al., 2018; McCoy et al., 2019; Vandenberg & Kulig, 2015). Parents reported that the relationship between government officials and pharmaceutical companies created policy changes that aimed to optimize vaccination rates (Attwell et al., 2017). Another reason for distrust in parents was their inability to communicate and express concerns to physicians regarding the possible adverse effects their children may experience after being vaccinated (Austvoll-Dahlgren & Helseth, 2010; Carrion, 2018; Helps et al., 2019; Miller et al., 2008; Sobo et al., 2016; Ward et al., 2018).
Parents believed that research that increased pharmaceutical company profits was promoted and published over studies that focused on the potential side effects of vaccines (Alstyne et al., 2018; Attwell et al., 2017; Senier, 2008; Sobo et al., 2016). Parents in two studies went as far as to say that research on the shortcomings of vaccines was being actively withheld from public knowledge (Attwell et al., 2017; Sobo et al., 2016).
Mandatory Vaccine Policies
Parents in nine studies reported anger and frustration when fear was used as the predominant strategy to pressure people to vaccinate their children (Alstyne et al., 2018; Attwell, Smith, & Ward, 2018; Helps et al., 2018, 2019; P. McDonald et al., 2019; Reich, 2018; Swaney & Burns, 2019; E. Wang et al., 2015; Wilson et al., 2008): . . . if you apply pressure to people that have already chosen to be outside, it pushes subcultures and underground movements and already there is a wellspring of people . . . It’s like catching a fish, the harder you squeeze the more it slips away. (Helps et al., 2018, p. 163)
Parents also described how there were extreme pressures to vaccinate in the form of financial penalties (i.e., not receiving stipends by the government for child care) and social consequences (i.e., not being accepted by the public schooling systems; Hatoková et al., 2018; Helps et al., 2019; McCoy et al., 2019; Meleo-Erwin et al., 2017; Swaney & Burns, 2019; Wilson et al., 2008). Although some parents described how mandatory vaccine laws did not affect their decision to reject vaccines (P. McDonald et al., 2019), others considered moving to countries where mandatory vaccine policies did not exist (Helps et al., 2018). In other cases, mandatory vaccine policies may also limit early learning opportunities for some children if their parents chose to remove them from child care and preschooling (Helps et al., 2018). Parents struggled with limiting learning opportunities for children because of vaccines: They are making it very clear that unless your child is vaccinated they should not be allowed to attend child care or schools . . . and that’s where they are heading which is mind blowing, because as a teacher . . . how can vaccination be more important that the social and learning benefits of education? (Helps et al., 2018, p. 163)
Parents who generally supported vaccines expressed the desire to avoid mandatory vaccine policies (Alstyne et al., 2018; Hatoková et al., 2018). Instead, parents explained how vaccination policies should promote shared decision-making and choice among parents to be inclusive of a wide variety of beliefs: I think we’re a choice society, where people want to make choices. And that would be another way of advertising: you have two choices to vaccinate your kids. You can vaccinate them all at once or you can vaccinate them a bit at a time. And that gives some people, oh, I have a say in this, I have a choice, I’ve got some control in this. (Enkel et al., 2018, p. 6462)
Discussion
In this review, we examined how parents navigated the vaccination decision-making context for their children and infants in 34 qualitative studies. We depicted our interpretations of factors that promote vaccine hesitancy using the metaphor of a gear train, where each factor corresponds to one of seven gears: previous experiences; “natural” and “organic” living; perceptions of other parents; experiences interacting with health care providers; information sources, challenges, and preferences; distrust in health system players; and mandatory vaccine policies. Each of these factors or gears represents a reason that parents use to forego vaccinating their children. The gear train rotates as a system; when a force is applied to a gear, then all gears will rotate but at different rates. Similarly, although one factor may be the primary reason for parents to reject or delay vaccines, parents may consider other factors, and each factor may play a unique role in the vaccine decision.
Implicit throughout our findings has been parents’ preferences to apply the rules of SDM to vaccine discussions. For example, in parents’ experiences interacting with health care providers, we found parents’ general orientation toward providers who were more open to a wide range of beliefs about vaccines. We want to note that although the SDM literature is geared toward patient–provider relationships, we use this concept in this section to discuss factors outside patients and providers as well. For instance, we found how some parents explicitly expressed a preference for policies that allowed greater freedom over mandatory policies and financial penalties. SDM is a particularly useful concept because it anchors our discussion on the interrelations between the various factors that promote vaccine hesitancy. In Figure 1, we conceptualize SDM as another input gear that can shift the rotation of the gear train to oppose vaccine hesitancy. In the next section, we discuss how SDM has been conceptualized in the literature and examine how it can promote vaccine acceptance.
SDM
Creating an environment that is conducive for obtaining informed consent from patients is vital for medical practice. An essential component of informed consent is SDM whereby patients and health care professionals make collaborative health care decisions (Weston, 2001). SDM is particularly useful in situations where there is more than one medically acceptable option (i.e., preference-sensitive decisions). SDM focuses on supporting patients to navigate through conflicting values in the context of risks and benefits of a particular decision (Witteman, 2015).
SDM is important in today’s context where a growing number of patients express a preference for making shared decisions with their health care provider (Chewning et al., 2012). Moreover, some research has found that patients who are more involved in health care decision-making report a greater number of clinical benefits (Hack et al., 2006; Hibbard & Greene, 2013). At the same time, a considerable amount of research has created uncertainty surrounding the most effective treatment option for certain medical conditions. However, the same level of empirical uncertainty does not exist for vaccine safety and efficacy. In this lies a tension between parents’ expectation for SDM for all interventions (including vaccination) and health care providers’ inability or unwillingness to use SDM for vaccine-related conversations. While SDM is not applicable to vaccine conversations based on how it has been conceptualized academically, we believe that some elements—particularly information and open dialogue—can enhance the interactions between parents and providers.
The Role of SDM in Vaccine Discussions
Health care providers have certain paradigms and epistemologies that guide their medical practice. Vaccines are essential elements of improving the health of communities within the allopathic medicine paradigm. Therefore, discussions about vaccine side effects challenge long-held assumptions about public health. The lack of such discussions is bolstered by the limited availability of high-quality performance indicators of adverse vaccine outcomes, although this is changing (S. A. McDonald et al., 2018; J. Wang et al., 2018). The lack of data on long-term negative outcomes of vaccines circumscribes the extent to which we can conduct rigorous research to inform medical practice. There is also an overwhelming focus by researchers on certain possible side effects—for example, autism (Hviid et al., 2019)—that restricts opportunities to investigate the prevalence of other side effects that parents in this review expressed concerns about. Without the necessary information that health care providers need to have discussions on vaccine side effects, there is a gap in their decision-making paradigm.
An increasing number of health care professionals express challenges remaining up-to-date with advances in the field, and rationales for introducing new vaccines (Brownlie & Howson, 2006; Petousis-Harris et al., 2004). Kumar et al. (2016) asserted that because of the low incidence of vaccine-preventable disease today, a considerable number of health care providers have limited firsthand knowledge of disease risks. Because of the lack of data, information, experience, and space for this sort of dialogue, health care providers find themselves in a difficult position when challenged by vaccine-hesitant parents on some of the most foundational assumptions of public health: the safety and efficacy of vaccines. Health care professionals experience discomfort when facilitating discussions with parents on vaccine schedules and new advances in vaccines (Leib et al., 2011).
Having examined the studies included in this review, we have to acknowledge the partial accuracy of some beliefs of some vaccine-hesitant parents, while at the same time empathize with the struggles of health care providers interacting with this population. For example, we understand some parents’ position when they assert that there is insufficient long-term evidence on vaccine side effects to preclude their existence, as some health care providers may proclaim (e.g., Wilson et al., 2008). We also recognize the difficulty in trusting information when there is a considerable amount of polarized misinformation (e.g., Ward et al., 2017).
A key component of SDM that is especially apparent in this review is equipping health care providers with the necessary information to interact with vaccine-hesitant parents in a productive manner (Légaré & Witteman, 2013). A recent Cochrane review found that parents expressed a desire for balanced information on vaccines than what they had been receiving (Ames et al., 2017). For SDM, information needs to be balanced on both the risks and benefits of vaccines, which we suspect that health care providers are unaware of or uncomfortable in sharing.
But what happens when providers’ implementation of SDM is met with a lack of an evidence base that allows for a wholesome discussion of benefits and risks of vaccines? When patients request for more information on vaccine side effects, health care providers may experience dissonance that may cause some to retract in their willingness to implement SDM. Health care providers may emphasize the benefits of vaccines, which in turn parents may perceive as another “biased” perspective in the milieu of vaccination conversations. For some parents, “biased” information from their primary care provider may cause them to distrust all allopathic providers, as well as government officials, pharmaceutical companies, and academic research. A “biased” response may also be perceived by parents as paternalistic if allopathic providers are reluctant to engage in a conversation about the pros and cons of vaccines, despite parents holding the expectation of SDM, which they derive from health care providers in the first place.
We found multiple instances where parents reacted to providers’ unwillingness to dialogue about potential vaccine side effects by becoming further entrenched in their vaccine hesitancy beliefs (e.g., Carrion, 2018). On the flip side, having an open dialogue with physicians about potential risks caused some parents to accept vaccines eventually (e.g., Peretti-Watel et al., 2019). Gust et al. (2008) reported that a large proportion of parents accepted vaccines due to comprehensive information and assurances from their health care provider. These findings are particularly interesting in comparison with previous research that suggests that a “presumptive approach” is associated with higher vaccine uptake in parents (McClure et al., 2017; Opel et al., 2013). Although we acknowledge that the studies included in our review mentioned that some vaccine-hesitant parents accepted vaccines through provider persistence, we found that the more common reaction was to reinforce vaccine-hesitant attitudes, seeking out other health care providers—sometimes complementary and alternative providers who emphasized the side effects of vaccines—and resorting to information sources managed by anti-vaccine groups. Besides, the presumptive approach leads to lower satisfaction (Benin et al., 2006; Opel et al., 2015), which is linked to lower acceptance of interventions and provider recommendations (Barbosa et al., 2012; Dang et al., 2013).
Using SDM to Develop Vaccine Policies
SDM can also inform how to develop vaccine policies that meet parents’ expectation of SDM in vaccine conversations. In the United States, approximately 10% of parents expressed opposition to mandatory government policies (Kennedy et al., 2005). In this review, we found that vaccine-hesitant parents resented vaccine policies that predicated child care or access to public schools to vaccination (e.g., Helps et al., 2018). Parents viewed mandatory vaccine policies to limit their ability to make an informed decision.
Developing vaccine-related policies that incorporate certain elements of SDM may be effective in promoting vaccine acceptance in parents. First, decision-makers need to consider whether financial penalties are having their intended effect, or if they are unfairly targeting low-income and marginalized groups. Second, rather than using mandatory vaccines policies as the primary or only strategy, decision-makers might consider mandating interactions between parents and allopathic health care providers when parents express hesitancy. Mandating interactions will require extensive training on how to apply SDM in vaccine conversations. Third, although we strongly oppose any government’s decision to explicitly support vaccine rejection or delay, we recognize that to include a wider range of perspectives, governments should not exert coercive policies as the primary or only strategy. Governments might also consider allowing greater flexibility in the vaccine schedule.
Conclusion
This review examined 34 qualitative studies to clarify parents’ reasons and rationales for rejecting or delaying vaccines. We used the metaphor of a gear train to conceptualize the interrelations between the various reasons that promote vaccine hesitancy. We also examined how SDM can be used as a broad principle to promote vaccine acceptance, not just in vaccine conversations between parents and providers but also when developing vaccine policies. The findings of this review offer a starting point for increasing awareness of the real-life experiences, rationales, and challenges that encourage vaccine hesitancy.
Supplemental Material
Supplementary_File_1_Compiled – Supplemental material for The Factors That Promote Vaccine Hesitancy, Rejection, or Delay in Parents
Supplemental material, Supplementary_File_1_Compiled for The Factors That Promote Vaccine Hesitancy, Rejection, or Delay in Parents by Umair Majid and Mobeen Ahmad in Qualitative Health Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.