
Abstract
This qualitative study is conducted via focus groups with 47 Australian public service interpreters to investigate their responses to vicarious trauma (VT) in their practice, the influence of culture, and their views on how to maintain mental well-being. While participant interpreters employ various strategies to deal with traumatic client content and other work stressors, cultural inhibitors are found to prevent some from sharing their emotional vulnerability or seeking professional help. They indicated that they want to be treated with respect and as part of the professional team, rather than a machine or a shadow. Professional development is needed to clarify the limits of confidentiality, explain trauma and its vicarious possibilities, and to establish interpreters’ professional entitlement to briefing and debriefing. Stakeholders including educators, professional associations, interpreting agencies, and other professions and institutional users of interpreting services should work respectfully and collaboratively to prevent and help interpreters recover from VT.
Keywords
Introduction
Professional interpreters in Australia work in highly varied settings, where they often bear the brunt of having to relay difficult, emotional, or confronting messages to fulfill their role in the communicative event. Unlike other professions such as social workers, psychologists, doctors, and nurses, interpreters do not have institutionally facilitated avenues for professional supervision or debriefing to prevent the adverse psychological impact of traumatic material and to promote healing. In Lai et al.’s (2015) study of 271 Australian interpreters and translators covering 54 languages, 78% said they were affected by trauma-inducing content encountered at work. Interpreters in that study confirmed their exposure to all the variables probed, including clients expressing sadness, helplessness and isolation, or narratives about family violence, sexual assault, physical assault, traumatic events in their lives, life-threatening illnesses, loss of loved ones, child abuse, torture, murder, and criminal trials. Despite the distressing impacts of clients’ experiences on them, 70% of interpreters surveyed said they did not seek psychological assistance and 40% said they would avoid working in trauma-inducing contexts in the future (Lai et al., 2015) as a means of self-protection. There is a pressing need to further understand Australian interpreters’ responses to vicarious trauma (VT), the influence of culture on their help-seeking behavior, and what their views are on how to prevent and recover from VT. The current study serves to make contribution to formulating occupational health and safety (OH&S) best practice for vulnerable interpreters, with a view to promote their emotional health to sustain their career.
Context of Interpreters in Australia
Australia is highly multicultural and multilingual, with almost 30% (29.4%) of its population born overseas (Australian Bureau of Statistics [ABS], 2019), more than one in five (21%) who speak a language other than English at home (ABS, 2017), and one in 10 (10%) Aboriginal and Torres Strait Islander people who speak an Australian Indigenous language at home (ABS, 2017). The 2016 census reported more than 300 languages, including 150 Australian Indigenous languages, that were spoken in home, reflecting the linguistic diversity of Australia’s population (ABS, 2017).
The Australian government funds interpreting services to enable community members who do not speak English or are not proficient in English to access government and other services. Professional interpreters in Australia work mainly in community settings “provided for the public by central or local government . . . [including] legal, health and a range of social services such as housing, education, welfare and environmental health” (Corsellis, 2008, pp. 4–5). These interpreters are referred to as community interpreters (Chesher, 1997) or public service interpreters (Corsellis, 2008).
Professional interpreters in Australia tend to be freelancers, except for a small proportion who work as staff interpreters primarily in hospitals (FECCA [Federation of Ethnic Communities Councils of Australia], 2016). Most practitioners are registered with multiple interpreting agencies, from which they accept interpreting assignments. Prior to rapid adaptations of video remote interpreting by interpreters and professional colleagues under the COVID-19 crisis in 2020, it was the norm for interpreters to attend in person multiple interpreting assignments within a day, traveling from one assignment to the next at different geographic locations and for different job contexts (e.g., from a maternal and child health appointment for a new mother to a family conference in a palliative care unit). Most interpreters do not develop familiarity or deep social connections with their clients due to the transient nature of their work, and they do not have immediate access to debriefing or supervision with their professional colleagues, as they are not a direct employee of these organizations.
The National Accreditation Authority for Translators and Interpreters (NAATI) acts as a gatekeeper for awarding interpreter credentials and maintaining minimum standards for public service interpreting in Australia. From 2018, those who want to attempt a NAATI credential test must fulfill minimum training requirements stipulated by NAATI (further see https://www.naati.com.au/become-certified/) and pass a certification test demonstrating required skills and knowledge. Training was not mandatory pre-2018, as long as one passed a one-off performance-based test and an ethics test administered by NAATI. In principle, public services must use NAATI certified interpreters (Department of Social Service, n.d.). However, uncertified interpreters are still seen working due to either shortages of credentialed interpreters in certain languages or as a shortcut in “low-risk situations” (FECCA, 2016, p. 14) by some interpreting agencies or by certain institutions. As at December 31, 2019, there are 7,939 NAATI-credentialled interpreters in Australia holding various levels of NAATI credentials (M. Painting, personal communication, 2020, January 8).
Literature Review
VT is defined as “the transformation that occurs within the therapist (or other trauma workers) as a result of empathic engagement with clients’ trauma experiences and their sequelae” (Pearlman & Mac Ian, 1995, p. 558). Research into VT in interpreters is relatively recent and emerging, compared with the more abundant literature for emergency and rescue workers such as firefighters (e.g., Brown et al., 2002) and ambulance workers (e.g., Clohessy & Ehlers, 1999) and other helping professionals such as nurses (e.g., Beck, 2011; Raunick et al., 2015), psychotherapists (e.g., Arnold et al., 2005; Neumann & Gamble, 1995), and social workers (e.g., Cox & Steiner, 2013; Diaconescu, 2015; Michalopoulos & Aparicio, 2012). If professionals can be traumatized vicariously, “there is no reason to assume an interpreter would be immune to the same experience if working in the same setting” (Bontempo & Malcolm, 2012, p. 106). Literature has started to emerge for performing arts (Cristiano, 1998; Robb et al., 2018; Szlawieniec-Haw, 2018) on the susceptibility to VT of actors playing roles representing human suffering, distress, or violence, and the consequent importance of de-roling techniques. Interpreting can be seen as analogous to performing—with voice and to some extent with body language, where interpreters immerse themselves in their client’s emotional world to convey what is meant by the client. In the same sense as actors, such en-rolement may subsequently leave the interpreter with an “emotional hangover” (Lassken, 2016, p. 27) where they find themselves still connected to character traits and moods. Conveying “affect congruent with the content they translate” (Berthold & Fischman, 2014, p. 108) often requires interpreters’ empathy, and when they are emotionally invested in the content, it “may contribute even further to their identification with the client and increase the opportunities for associated distress” (Berthold & Fischman, 2014, p. 108).
Darroch and Dempsey (2016) conducted a systematic review of empirical research on interpreters and VT and located 11 studies. Key themes Darroch and Dempsey identified from the papers are as follows:
Emotional impact of interpreting: Exposure to distressing material and empathic engagement with clients can lead to interpreters’ negative emotions and distress, and symptoms associated with VT. Having to use the first person, that is, “I,” while interpreting creates emotional impact on interpreters. Most report experiences of “transference, projective identification, countertransference and over-identification reactions” (Darroch & Dempsey, 2016, p. 174), while some make reference to defense mechanisms such as numbing, denial, detachment, and disengagement to block their experiences and distract themselves. Positive experiences and growth are felt by some interpreters as the result of their empathic engagement with their clients.
Working with service providers: Some interpreters experience lack of respect and understanding of their work by service providers, and the strain their work causes them. The lack of protocol, information, and service providers’ understanding is regarded by many interpreters as source of work strain and negative emotional reactions.
The professional self versus the personal self: Conflict between professionalism and experiencing emotional difficulties are felt by most interpreters. Interpreters emphasize the importance of maintaining professional boundaries to do their jobs well and to protect themselves.
Coping strategies: Being familiar with the occupational environment and the processes of services helped interpreters to handle emotions better. Men are found in two studies to be less enmeshed with their clients and experiencing fewer emotional impacts, and that personality may be a mitigating factor in terms of whether one is able to cope with working in stressful settings such as mental health. Most interpreters use social supports to cope with the emotional impact from work, with talking to family friends and colleagues the most commonly seen. Findings are inconsistent in relation to interpreters receiving support and/or supervision. What is consistent is the fact that interpreters are “exposed to, and experience, emotional and vocational difficulties, which they need support in processing in order to cope with their experiences” (Darroch & Dempsey, 2016, p. 181).
Darroch and Dampsey’s (2016) meta-analysis provides a comprehensive overview of the prominent issues relating to interpreters and VT. The gaps of knowledge identified by the current authors are as follows:
Limited range of settings: Most of the studies in Darroch and Dampsey’s (2016) review as well as other available research (e.g., Green et al., 2012; Holmgren et al., 2003; Miller et al., 2005; Roberts, 2015) are focused on interpreters working with refugees and asylum seekers in mental health settings, rather than a broader range of public service contexts in which community interpreters work.
Interpreters’ perspectives: As a result of the above, most of the existing studies were conducted from the perspective of professionals such as mental health clinicians and social workers, rather than interpreters themselves.
Australian perspective: Most studies were conducted in the United Kingdom, with small numbers from other countries such as Denmark (Holmgren et al., 2003), Ireland (Gomez, 2012), New Zealand (Crezee et al., 2013), Switzerland (Loutan et al., 1999), and the United States (Engstrom et al., 2010; Mehus & Becher, 2016; Miller et al., 2005; Shlesinger, 2007). Only five Australian studies were located: two targeted at sign language interpreting (Bontempo & Malcolm, 2012; Clare, 2000), with the remaining three about spoken languages. Lai et al.’s (2015) is a quantitative study on public service interpreters, whereas the other two (Becker & Bowles, 2001; Lipton et al., 2002) are qualitative on seven and 15 interpreters, respectively, both in psychotherapy contexts and written from the therapist’s perspective.
Interpreters’ qualifications: Apart from the Australian studies referred to above, and Roberts’s (2015) U.K. study, other studies did not specify the qualification or certification status of the interpreters. It is likely that some interpreters in some studies are not qualified interpreters but simply bilinguals without interpreting credentials or training. The current study targets credentialed professional interpreters who are subject to minimum entry screening by a national authority, for example, NAATI in the case of Australia, thereby approaching the issue from an OH&S perspective, in the same sense as has been addressed in their professional colleagues such as social workers and psychotherapists. This research angle has rarely been explored but is critically needed by Australian interpreters.
Method
The current study is guided by the principles of action research, where practitioner-researchers look at their practice to check whether it is as they feel it should be (i.e., professional interpreters working with public service contexts in Australia), and when they feel the practice needs attention in some way, they identify an aspect to investigate (i.e., professional interpreters affected by VT) to take action to improve it (McNiff, 2013). The design of the study is informed by phenomenology, which aims at eliciting a description of the commonality of a lived experience (i.e., about VT) within a particular group (i.e., Australian community interpreters) by way of asking two broad questions: (a) What have you experienced in terms of the phenomenon? (b) What contexts or situation have typically influenced your experiences of the phenomenon? (Creswell, 2013).
Considering the potentially large sample size, the researchers decided to use focus groups for data collection, as opposed to individual interviews conventionally used for phenomenological studies. The decision was based on the suitability of focus groups for a homogeneous group, for example, people from the same profession (Liamputtong, 2011), particularly when they are from underrepresented populations who hold different cultural perspectives and diverse views (Liamputtong, 2010). The questions put to participants of the focus groups to capture their lived experience were as follows:
How have you handled VT to date—what strategies have you used?
How does your culture or religion view trauma and how do those views encourage or prevent you from seeking assistance if you feel VT?
What would be helpful in dealing with VT? What would you like to know?
As opposed to other forms of social research, where researchers tend to do research on other people, the current researchers “prefer to do research on themselves, in company with other people who are doing the same . . . No distinction is made between researchers and practitioners” (McNiff, 2013, p. 23). As action researchers, they demonstrate certain sets of beliefs, commitments, and hopes they share in their practice (McNiff, 2013). The chief investigator is an interpreting practitioner, educator, and researcher. She has a special interest in interpreters’ mental well-being and believes in advancing interpreter education with evidence-based research. Although the chief investigator belongs to the interpreter population being researched, she is aware of the importance of “suspending (bracketing) as much as possible the researcher’s meanings and interpretations and entering into the world of the unique individual” (Hycner, 1985, p. 281) in the process of data collection. The co-investigator is a social work practitioner, educator, and researcher, who has worked with interpreters in her practice domestically and internationally. In their university roles, the researchers collaborate in facilitating joint practice-based education for social work and interpreting students on how to work together. Learning about each other’s profession is a way to “exercise their individual and collective educational agency” (McNiff, 2013, p. 25), which revealed the inequity of interpreters’ lack of support in supervision and debriefing. This motivated and lent credibility and authority to the current study (Carpenter, 2017).
Participants
An electronic flyer was distributed through four nationally based interpreting agencies to recruit professional interpreters who met the inclusion criteria, being those who had had at least 3 years’ experience interpreting in trauma contexts and at least a weekly average of at least 3.5 hours exposure to trauma content—a level of exposure regarded by Australian interpreters as medium (Lai et al., 2015). As per Kruger (1988), we looked for those who “had experiences relating to the phenomenon to be researched” (p. 150). Purposive sampling (Patton, 2002), following the flowchart in Figure 1, yielded a total of 47 participants. Three meetings were scheduled on three different days at the university where the researchers are based. The participants chose a day which was convenient for them to attend.
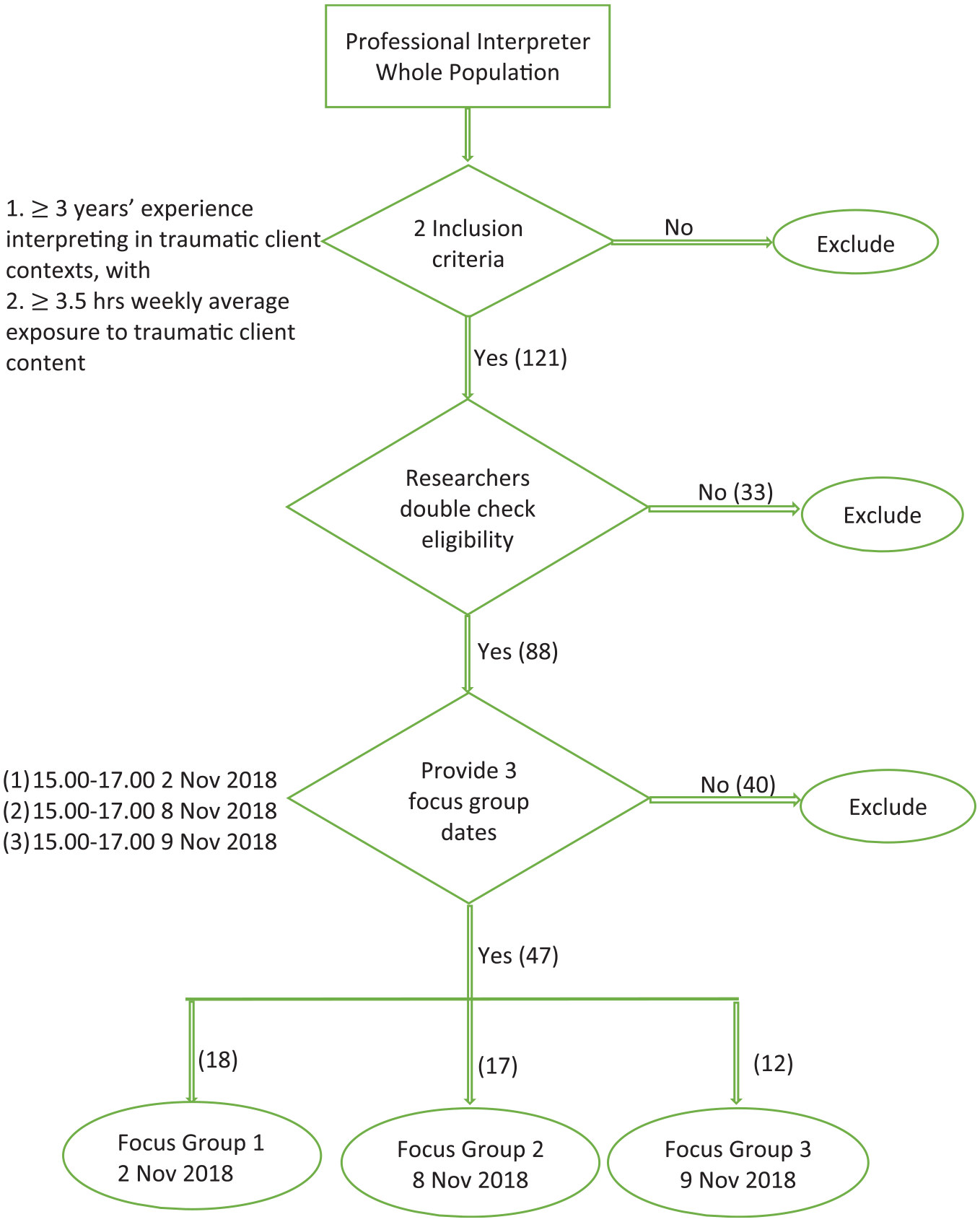
Sampling process.
Participants of the focus groups were emailed the information sheet about the study and focus groups. Written consent was received from the participants before commencement of the sessions. Participants were provided with contact details of a counseling social work psychologist who was on standby in case anyone became distressed during or after the meeting. Each participant was offered a gift voucher worth of AUD70 to compensate for their time during business hours. The researchers used their own research funds for this project and declare no conflict of interest.
The demographic information about the participant interpreters is summarized in Table 1. In line with our purposive sampling, 82% of the participants are credentialed by NAATI and all of them had prior interpreting training or education, as required by current standards in Australia (Supplemental File 1: Participants’ Language Other Than English).
Participants’ Demographic Data.
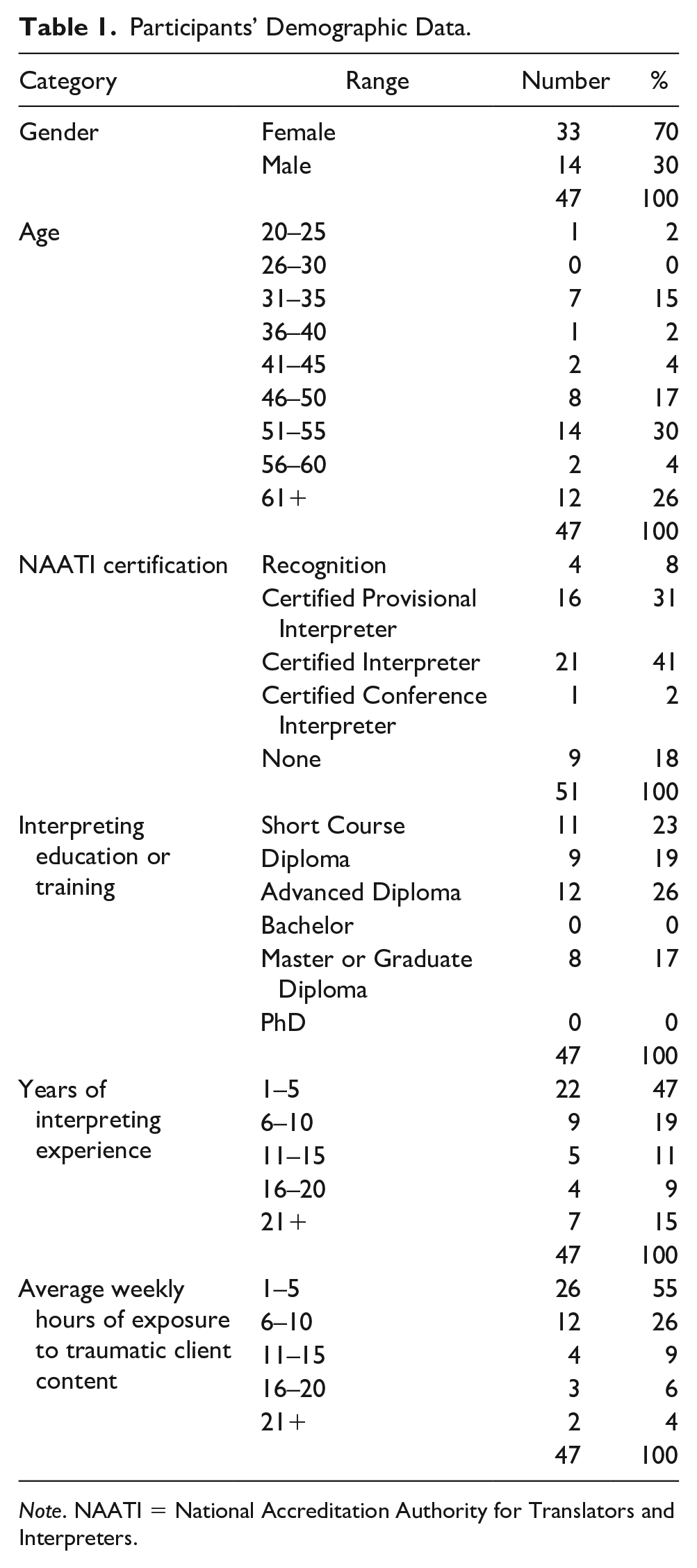
Note. NAATI = National Accreditation Authority for Translators and Interpreters.
Process
The project received ethics approval (# 21475) from the Human Research Ethics Committee of the university where the researchers are based. Approval was granted after the researchers were asked to amend the application to ensure no cultural identities could be attributed to individual interpreters in the research reporting to protect the participants’ privacy, particularly those from smaller LOTE (Languages Other Than English) communities. This was implemented in the way the findings and discussions are written in this article. A focus group guide was developed and followed across the three meetings (Supplemental File 2: Focus group guide).
Action research aims at “changing or improving a social situation, and involving those most affected” (Alston & Bowles, 1998, p. 164) to develop skills and knowledge to bring about change in their own environment. With this in mind, the researchers began the focus groups with some basic information about trauma and its vicarious impacts (by the co-investigator) and referring to the findings of Lai et al.’s (2015) previous study (by the chief investigator). This allowed the participants to also use the focus group activity to claim professional development points for their recertification. In each meeting, the researchers divided participants into groups of five or six people of random language combinations. Digital voice recorders at each table were switched on when participants began their discussions. The researchers floated around the tables to clarify points during the discussions, ensuring that the discussions were not “dominated by a vocal minority” (Davidson et al., 2017, p. 88). In addition to audio recording, each group was asked to note down summaries of their discussions on butcher’s paper. The researchers kept personal notes for their reflections of each meeting.
A research assistant transcribed orthographically the recordings with the assistance of the summaries captured on butcher’s paper. Member checking was conducted by emailing the participants the transcripts of the session they took part in, and they were invited to read only the sections they identify as related to the discussions at their table to lessen their burden. Only one participant came back asking to correct a misheard word. An inductive approach (Willig, 2013) under the qualitative paradigm was used to analyze the data, where the researcher “approaches the data without a theoretically informed coding frame. The themes that emerge from such an analysis are firmly grounded in the data and do not reflect the researcher’s theoretical commitments” (Willig, 2013, p. 60). The researchers conducted the data analysis in two phases. In the first phase, they started by reading the transcripts independently a number of times for familiarization. This enabled them to identify what they regarded as central issues in each focus group meeting (Patton, 2002), and then they documented their own initial thoughts and impressions. This phase is in keeping with the first three steps recommended by Braun and Clarke (2006) for thematic analysis, that is, familiarization with data, generate initial codes, and search for themes. In the second phase, the researchers examined the initial themes emerged from the first phase, establishing their connections, similarities, and differences across all focus group meetings (Avraham et al., 2014). They then arrived at their own list of themes emerged from all data. This phase reflects Braun and Clarke’s (2006) Steps 4 and 5, being reviewing themes, and defining and naming themes. The researchers then conferred to compare their individual analyses to identify differences between them and arrive at final agreement after discussion. This process revealed the researchers identified similar meanings from the data. Where they diverged was clustering of meanings, for example, “lack of appreciation by professionals” and “lack of appreciation by interpreting agencies” delineated by the chief investigator were labeled more broadly as “feeling under-appreciated” by the co-investigator. The researchers also agreed on combining three themes relating to three different stakeholders to form a super-theme “interpreters want professional support.” Through the process of validating and modifying the themes and data coded under each theme, the researchers were able to construct a holistic context of the phenomenon under study with enhanced trustworthiness (Davidson et al., 2017).
Findings
Six themes are identified and presented in this section. Quotes from participants are provided, where appropriate, to ensure credibility. During data analysis process, codes were attached to quotes, for example, F1-T1-W, to denote focus group number, table number, and gender of the speaker (refer Table 2). However, for simplicity of presenting findings in this section, only gender will be indicated, that is, W (for female) and M (for male), for quotes used.
Participant Coding.

Theme 1: Cultural Views Inhibit Sharing Vulnerability
Many participants reported that when they feel emotionally distressed as a result of their work, they do not discuss it with anyone because of embarrassment or fear of being ridiculed as being weak. Taboos on expressing vulnerabilities, negative feelings, or sadness were linked to culture by some. For example, the following statement reveals a cultural interpretation of trauma.
In my culture, [trauma is] something to do with violence, death, or serious sickness nearly causing death—diseases many people would consider quite taboo to even talk about, because they lead to death. (M)
One participant said, “My culture says, Keep all your problems in your home; don’t talk about it with others” (W), which was concurred by another participant at the same table: “Many issues are considered taboo, we cannot discuss them” (W). Emotional vulnerability is regarded by some cultures as “bad luck, a message from God and fate, [a] punishment” (M). They should instead “Get over it! Be a man!” (M). Participants find it hard to justify taking action for their vulnerable feelings, as those feelings are not considered serious enough to warrant professional intervention or attention from others. Some regard that revealing vulnerabilities may invite questioning of their competence by their community members: Our community, they don’t know about vicarious trauma. They are not familiar with all these terms and about the situation. They are seeing us that, ok, you are weak and . . . probably we can’t work with you next time. Or maybe they will say that interpreter was not good . . . The good interpreter is the one that shows that they like a superwoman or superman, you know, but the weak one, is the emotional one. (W)
Apathy about the use of debriefing or counseling was expressed by participants who were not accustomed to the idea, as one participant put it: If I’ve lived something traumatic, me myself, or heard something traumatic, if I repeat it, I feel like I’m doing it again . . . I don’t feel I can talk about it. It doesn’t make me feel better. (W)
Theme 2: Impact of Empathy with Trauma Clients
Participants in the focus groups concurred that having to relay clients’ difficult stories in the first person, that is, using “I,” exacerbates the internalization of the traumatic material. Where the interpreter has had similar experiences, it can affect them significantly because they feel “torn apart in the heart” (W). Others find it hard to contain their empathic reactions, wishing they could have assisted the client. One interpreter recounted her experience in a medical appointment, where she interpreted for the doctor but received no responses from the male patient. She asked the doctor if she spoke the right language for the patient. It was not until this point the doctor, in addition to assuring her that the language was the correct one, told her that the patient had been tortured by ISIS for 2 years and had since stopped communicating. The interpreter became angry and tearful sharing the experience: . . . like, excuse me! Tell me before we start so I know who I’m dealing with. I’m a human being and he’s my father’s age. At that very moment my father came into my mind. What if it was my father in that situation? . . . In our culture men are very proud. They control this and that, that’s the way. They are the leaders, they control, they are like the masters. And being in that weak situation . . . it’s really painful [to bear witness to it].” (W)
Another interpreter recounted an experience when she completed a 3-hour-long interpreting assignment at a hospital for a family with three children. The youngest had to go to Pathology for a blood test. The interpreter thought she would help by taking the child and letting Pathology know to look after the child, since the family was still needed by the hospital staff and could not go away at that point. She was later severely reprimanded by the hospital staff for overstepping her role as an interpreter. She stated, . . . I said, she’s seven years old. I didn’t think, honestly. But they look at us like this is not a professional attitude. We go back to the professionalism. So I felt, really I felt offended. You’re a mother. I’m a mother. What’s wrong with me? What does that mean if I show some support? I wasn’t advocating. I wasn’t talking. I showed support in such a small way. Does that mean that I’m not a professional? (W)
The example illustrates the fuzziness of demarcating where interpreting ends and ones’ humanistic propensity kicks in, when the interpreter may have overidentified with the client or is drawn to offer extra assistance beyond her role. Although the actual interpreting in this case may not have been traumatic, the consequences of the empathic action were regarded as unprofessional by the institution and the way it was conveyed to the interpreter created hurt and humiliation. Situations like this become stressors to interpreters.
Theme 3: Rejection of Utilitarian View of Interpreter
A theme emerged from participants’ experiences is related to their treatment by professionals as merely a “mouthpiece” as if they have no feelings. This contributes to work stress: Many professionals we deal with look at us as being machines; we are not humans . . . regardless of whether it’s medical, psychological, mental, even legal, sometimes even at the police stations, we have no idea what to expect. We go there for a job, even if it was at the middle of the night or early morning. We know nothing. All of a sudden, we are faced with all types of emotional information, that sometimes we are prohibited to react or to show any kind of reaction. And this comes all the time, building inside ourselves. We have no place to go or seek help. (W)
Others related to experiences of being treated like a “shadow—that we don’t even exist” (W), where sometimes the most basic pleasantry is lacking at the start of an interpreting assignment: . . . they don’t greet us in an appropriate manner, sometimes they don’t even tell us about the topic that they’re going to speak about . . . we go into the room and then they start speaking to the client directly without even mentioning our name or introducing us, which is rude. And you feel like you’re lost and you just want to speak, because you don’t know what’s happening. (W)
Interactions with other professionals sometimes leave interpreters hurt and scarred because of “the way the staff treat interpreters” (W) to the extent that they decide they will not accept jobs to interpret at the institution again. A strong consensus emerged from the participants that they want to be treated as fellow “human beings” (M), “equal professionals” (W), rather than the “other,” because “each time it seems like interpreter does not count as part of the team. Team is partnership with the professionals” (M).
Related to this theme is a general view that interpreters’ mental well-being is not adequately looked after by the institutions which use their service. Participants also “do not feel interpreting agencies care much about interpreters’ wellbeing” (W) in that there are few channels available for interpreters unless they seek them out themselves. One interpreter in this study said that the focus group was the first time in 35 years as an interpreter that anyone had asked her about the impact of the work on her emotional well-being.
Theme 4: Misunderstanding the Limits of Confidentiality
Some participants seemed to misunderstand confidentiality under the Code of Ethics (AUSIT, 2012), thinking it means they cannot talk with anyone, including seeking counseling or guidance, as this quote suggests: That’s the ethics of interpreting. You are not to divulge what you have heard in there. That means any information, . . . it’s just the guidelines that we are to abide by. (W)
For some interpreters, especially those whose culture does not subscribe to showing or sharing vulnerable feelings, the misapprehension extends to not speaking to a qualified counselor or supervisor, which does not help their sense of isolation and emotional distress.
Some participants pointed out that some professionals seem unaware that professional interpreters have a code of ethics and are committed to confidentiality and impartiality, resulting in the undermining of clients’ trust in the interpreter: I have been actually asked to leave the room two times because the client was from my country and when they realized from my accent I’m from their country, they were not happy to continue. There was no relationship at all. Not relatives. Not from my community. Just we happen to be from the same country . . . The professional could have explained that this session is confidential, and it’s a professional interpreter; that whatever is said here stays here, that’s it, so they could trust the interpreter. It’s not giving us a good image either, being asked to leave the room because the client is not feeling safe to share their information in the session. (W)
Theme 5: Coping Strategies
Participants reported multiple strategies for coping with the emotional toll of hearing others’ traumatic stories. Inspired by Avraham et al.’s (2014), the researchers separated the data collected into two major categories for ease of presentation: those seeking connections (i.e., engagement) with either their inner self or others, and those aiming for detachment (i.e., disengagement). The engagement strategies mentioned by participants can be further sorted into the following five categories:
Personal—including spiritual care, healthy lifestyle, self-care, hobbies;
Cognitive—including positive thinking, reframing, problem-solving, distraction;
Emotional—including meditation, relaxation techniques;
Physical—yoga, exercise, muscle relaxation;
Interpersonal—informal debriefing, peer support.
Among these strategies engaging in distraction were mentioned by most participants, as well as cognitive reframing and positive thinking, exemplified by statements such as “I take it as an educational opportunity for me to learn and upskill” (M); “The only way I deal with it is how I deal with everything. I look at it and ask myself how I can do better? Look for the positive, even when it is in the most traumatic you see, because I always look at the half-full cup” (M); “I kind of ponder over it and think to myself is there a better way to deal with this, or is there a solution for this; is there, you know, something we can do” (W). No mention was made in the data about organizational or professional engagement strategies such as debriefing, mentoring, supervision, or therapy. Statements relating to confiding in or seeking emotional support from peers, family, friends, and religion are more prominent.
In relation to disengagement strategies, participants mentioned the use of alcohol, negative emotional focus, avoidance, denial, disordered or over sleeping, disengaging socially, wishful thinking, and disengaging socially via television or gambling. It may be posited that discussing coping strategies in a focus group may have influenced participants’ decision on how much they reveal. The following statements indicate the coexistence of engagement and disengagement strategies of individual participants: Be “professional”—remain detached and cope. Learn to block. Do my job in a way that I remain objective and impartial. (M) Talk to myself and reason, and say: “different system, different culture.” It’s not mine [trauma] . . . Appreciate that it’s not your situation. Don’t talk about and it will go away. (M) If I just sit and think about it, I’ll be analyzing: maybe I should’ve [done] this, maybe this would’ve worked better, or you know, how else could I have done better. Most importantly, maybe I hope they know I’ve done the best I can. (W)
Theme 6: Interpreters want professional support
Although participants described various actions at a personal level to address their emotional disturbances from work, there was a strong message that they would like professional support. Their requests can be divided into three subthemes: be treated as a part of the team, access to employee assistance, and access to targeted professional development. These three subthemes correspond to three groups of stakeholders: institutional users of interpreting services, interpreting agencies, and professional organizations and interpreting educators.
Subtheme 6-1: Be Treated as a Part of the Team
A strong message was articulated by the participants that they want to be treated respectfully and as members of the professional team, and that professionals should have more training on how interpreting works and how to “work with” interpreters, rather than “use” interpreters. “Partnership” is a term used by several participants to express their preferred dynamics. All participants unequivocally asked that they be offered a briefing by the professional before an interpreting session to prepare them for ensuing emotional complexities, as exemplified by this statement: “It’s very important that the doctors or whoever is the profession, to give us a brief about the situation because we are not machines, honestly” (W). Participants want to be introduced to the client with explicit assurance that interpreters, too, respect confidentiality: At least the professional [could] give a brief definition that this session is confidential; it’s a professional interpreter; whatever is [said] here stays here . . . so they [i.e. the client] trust interpreters as well. (W)
Suggestions were made that professionals should develop their cultural sensitivities, including the appreciation of different cultural values, religions, and dialectal variance. Participants said they would appreciate more interaction with other professions, both individually and collectively, to promote ongoing interdisciplinary understanding.
Subtheme 6-2: Access to Employee Assistance
Despite expressing embarrassment, fear of criticism, and loss of work through expressing vulnerability, many participants said they would like the opportunity to debrief and make sense of the emotions they were left feeling after some sessions. “We do not feel interpreting agencies care much about interpreters” (W) was an alarmingly shared view, particularly in relation to the caring of the interpreter’s mental well-being. Participants requested “somewhere an interpreter can ring up and say, look, this is what happened today. I just need to talk about it” (W). Some interpreters suggested that interpreting agencies should facilitate free counseling services and employ a liaison officer or set up a mechanism to check on the well-being of their interpreters: We need to have free access to EAP [i.e. Employee Assessment Program], professional counselling, without being judged, without being tagged or labelled that you are unprofessional, you are unfit, you are not suitable for the job. (W)
Participants requested an easy way to provide feedback about their negative experiences of professionals or the organization they interpret for so that the same does not happen to the next interpreter. This would facilitate mutual understanding and respect, since they feel the current feedback mechanism is one-way, where interpreting agencies are predominantly interested in whether the interpreters have done anything inappropriate in the eyes of the institutional clients.
Subtheme 6-3: Need for Targeted Professional Development
A common view emerged that more professional development courses are needed for interpreters to raise awareness of the possible impacts of traumatic client content, the concept of VT, and the importance of self-care: . . . we do all sorts of professional development. We have about how to translate, how to interpret, but we don’t have anything about trauma . . . For instance, myself, for the first two years, I was exposed to trauma and I was traumatized. But I didn’t know that I was traumatized . . . I was sick, I was unwell for about two years. At the end I just went and asked the psychologist what’s wrong with me. She said that this is happening because of this [VT]. (W)
Participants were keen to see more research on the occupational impact on interpreters and managing VT. A suggestion was made that “emotional well-being” and self-care be added as a mandatory category under NAATI’s recertification requirements, as it is for social workers and psychologists. Currently, NAATI-certified interpreters have a 3-year recertification cycle, within which time a practitioner must fulfill the stipulated minimum practice hours and undertake professional development in three areas: (a) skills development and knowledge, (b) industry engagement with compulsory subcategory on ethics, and (c) maintenance of language (NAATI, n.d.-c).
Discussion
The findings affirm previous studies demonstrating that interpreters experience VT but have limited avenues for debriefing and recovery. The literature indicates that most helping professions, with whom community interpreters work, have processes in place for seeking supervision, debriefing, or counseling about the psychological impact of their work. Lai et al.’s (2015) study found that only 20% of the 271 Australian interpreters and translators surveyed would see a counselor about their VT, whereas 14% said they would see a therapist. Informal channels were used more by the respondents in that study, with 55% choosing to speak to their colleagues, followed 46% who spoke to their family members, and 38% to friends. By way of comparison, the only other known quantitative study of interpreters and VT is by Baistow (1999), where 295 interpreters from France, the Netherlands, Germany, Italy, Spain, and the United Kingdom were surveyed. Thirty-four percent of the respondents said their employer provided some kind of support service, and 20% had used the support service on some occasion, whereas 22% did not know if any service even existed.
Although the ethics approval of the current study prevents the identification of ethnic backgrounds of the persons espousing their views, it is still helpful to understand whether cultural factors play a role in some interpreters’ help-seeking behavior, the answer to which is affirmative as is revealed by the data under Theme 1: Cultural Views Inhibit Sharing Vulnerability. Counseling as a form of talking therapy is not necessarily a familiar concept to some participant interpreters. Many cultures do not have a word for counseling, and going to a counselor may not be a course of action people from such background normally take. Some scholars have criticized the narrow focus of counseling theories on feelings, thoughts, behaviors, or social systems, while ignoring spirituality, social class, and other biological, political, and cultural influences (Orozco et al., 2014). For example, Rassool (2016) asserts that counseling is taboo for some Muslims, who are reluctant to seek professional counseling because they consider it degrading or inappropriate to speak of one’s troubles to strangers. They prefer their concerns be addressed from a religious viewpoint and they may distrust mental health professionals, worrying that their Islamic values may not be respected. Lee et al. (2009) investigated Asian American young adults from Indian, Cambodian, Chinese, Indonesian, Korean, Taiwanese, Thai, and Vietnamese backgrounds and identified culture as a main factor inhibiting their help-seeking behavior. Mental illness tends to be highly stigmatized in these communities (Lee et al., 2009), and some cultures regard individuals with mental illness as being possessed by supernatural entities such as demons or spirits (Nguyen & Anderson, 2005).
Although all participants identified with their LOTE cultural background, some of them may have lived in Australia for a long time or are second-generation migrants, and therefore are more open-minded about help-seeking initiatives. Those who still find it prohibitive need encouragement to step away from their stereotypical cultural practice and acknowledge their need for psychological support. It is important that interpreters feel empowered to assert their rights for briefing and debriefing and understand what professional assistance entails so they access it when needed.
Theme 2: Impact of Empathy with Trauma Clients relates significantly to interpreters’ individual upbringing, socialization, and training. Effective empathic responses enable professionals to see the client’s world as they do while making professional judgment and helping clients make sense of their world. While this benefits clients, helpers must be made aware that the emotional hangover of empathy can develop into burnout and VT (Wilson, 2016). Empathy can arise in the course of, or around, one’s interpreting practice, which “brings up our own issues, our own life experiences, our own thoughts and feelings” (Harvey, 2003, p. 211). The example of the interpreter taking the child to Pathology highlights the challenge in real life in balancing empathy and their role boundaries, and the fact that stress and negative feelings may result from not interpreting but contextual situations surrounding it. Hsieh (2008) reports that interpreters sometimes offer empathy to provide a better service to their patients because “the social worker really didn’t do much at a cultural level” (p. 1377). The fact that interpreters are not in control and not invited to offer their insights or to provide help exacerbates interpreters’ sense of powerlessness. Clare (2000) pointed out feelings of survivor guilt by Australian Sign Language (Auslan) interpreters and posited a higher likelihood of VT due to lack of closure in many assignments.
The impact of using the first-person perspective to render trauma client’s utterances is reported as emotionally straining by many researchers (Bontempo & Malcolm, 2012; Gomez, 2012; Shakespeare, 2012; Splevins et al., 2010). Data in Theme 2 corroborate Darroch and Dempsey’s (2016) assertion that interpreters must cognitively “process by imagining the client’s perspective, so interpreting becomes far more intense than just hearing the words” (p. 175).
The way community interpreters are deployed in Australia means that it is unusual to have the same interpreter in subsequent client sessions. Only when the professional or the non-English-speaking client makes an explicit request would the interpreting agency endeavor to secure the same interpreter. Not knowing what happens to the trauma client with whom the interpreter has vested empathic engagement has the potential to prolong their emotional hangover, create anxiety, and intensify the sense of powerlessness.
As reported in Theme 3: Rejection of Utilitarian View of Interpreter, the “machine” analogy perceived by some professionals dehumanizes interpreters as a utility or an “accessary . . . [the professional] can pick up and drop at any point” (Hetherington, 2012, p. 49), neglecting the fact that the interpreter is a human being and a member of the service delivery team. Interpreting is an inherently stressful occupation (Kurz, 2003). The fact that interpreters are usually not given contextual information to make sense of an interaction (Bontempo & Malcolm, 2012) adds difficulty to their linguistic task to faithfully render utterances in the target language, adding to their job stress. Interpreters must manage other environmental (e.g., asking the professional to ensure noise outside the room is contained so the interpreter can hear everyone properly) and interpersonal (e.g., appropriately intervene when the client keeps talking without allowing interpreting) factors and their own intrapersonal demands (e.g., emotional distress felt inside the interpreter) (Dean & Pollard, 2001). Professionals’ lack of understanding of how interpreting works neglects the mental and psychological stakes invested by the interpreter to facilitate effective communication. Impartiality mandated by the interpreter’s code of ethics may “lead interpreters to believe that there is an expectation that they feel impartial as well as behave impartially” (Hetherington, 2012, p. 49, italics in the original). As Pearlman and Saakvitne (1995) observed, it is possible to act neutral in high-stress situations, but one cannot feel neutral. A misconstrued understanding of impartiality by some interpreters exacerbates their distress when confronted with their own empathic feelings. Bontempo and Malcolm (2012) similarly reject the myth of neutrality and assert “it is never possible to temporarily block oneself” (p. 110) for interpreters. Participants related their experiences of being scarred by insensitive treatment from professionals, and the feelings that they were not valued by the interpreting agencies which deploy them. Although these are not factors likely to precipitate VT, they become stressors for interpreters, which may potentially affect their mental well-being. Theme 3 corroborates Darroch and Dempsey’s (2016) meta-analysis of studies on interpreters and VT, where they identified “service providers’ conduct towards interpreters” (p. 177) as a common theme, and institutional users of interpreting services “lack respect and value for, and understanding of, interpreters, and the strain their work imposes on them” (p. 177). Valero-Garcés’s (2005) study, one of the 11 reviewed by Darroch and Dempsey (2016), revealed that 30% of interpreters’ emotional difficulties were linked to dealing with service providers.
Themes 5 Coping Strategies teased out what participants do to deal with VT, and the data seem consistent with common strategies reported in four other VT studies on interpreters (Doherty et al., 2010; Holmgren et al., 2003; Roberts, 2015; Splevins et al., 2010). The “engagement” and “disengagement” coping strategies reported under this theme bear resemblance to Auslan researchers Bontempo and Malcolm’s (2012) categorization, who refer to them as a positive versus negative (or active vs. avoidant) dyad. The complexities of interpreters’ responses as exemplified by the three statements at the end of Theme 5 warrant caution for a simple dichotomy. So-called negative coping strategies may in fact function as “essential defenses to protect against something much more painful” (Kagan & Schlosberg, 1989, p. 53) such as a re-experience of previous traumas, for example, as a refugee, displacement and loss, sexual or physical abuse, rejection, or abandonment.
It is acknowledged in the trauma literature that individuals may experience positive changes as a result of directly experiencing trauma, leading to enhanced psychological functioning compared with pretrauma levels (Linley & Joseph, 2005; Tedeschi & Calhoun, 1995). Just as helping professionals may acquire trauma vicariously from their client, they may also vicariously experience the growth similar to those described by direct trauma survivors (Tedeschi & Calhoun, 1995). These positive changes, however, occurred through processes of self-disclosure, emotional expressiveness and psychotherapy (Tedeschi & Calhoun, 1995), or supervision where counselors reported an optimistic perspective toward life when they discussed the effects of bearing witness to their clients’ resilience (Silveira & Boyer, 2015). This is not an option for most of the interpreters in this study and illustrates their need for debriefing and supervision.
Apart from what the participants do at the personal level to address psychological impact from work, Theme 6: Interpreters Want Professional Support emerged as an emphatic call for support from three groups of stakeholders: institutional users of interpreters, interpreting agencies, and professional organizations and interpreting educators. Subtheme 6-1: Be Treated as a Part of the Team closely relates to Theme 3: Rejection of Utilitarian View of Interpreters, in that this highlights the participants’ feeling of being overlooked as people and professionals’ treatment of them as “machines.” Hsieh (2008) observed the default conduit role deeply entrenched in the expectation of a nonthinking and robotic way of interpreting, exacerbated by the misconception that interpreters should not espouse personal opinions or feel emotional, despite working in contexts involving life and death issues. This conduit role can result in interpreters experiencing conflict and distress in their role performance and others’ role expectations (Hsieh, 2008). Subtheme 6-1 also reveals participants’ strong desire to be included in the service delivery team, and to be provided with briefing and debriefing, which, in their view, will provide the best possible mental preparation before and after the interpreting assignment.
Brämberg and Dahlberg’s (2013) model of collaboration between researchers and interpreters approximates what participants in this study would ideally like in terms of being part of the team, in that the interpreters were well briefed before they started, consulted about language and culture, and trusted to interpret meaning in the interview. Participants’ feedback about the lack of understanding by professionals of their role identified under Subtheme 6-1 is echoed in several other studies (Butow et al., 2012; Doherty et al., 2010; Roberts, 2015), all of which recommend training public service staff about the role of interpreters, in that it would enhance the interpreted experience and reduce the stressors felt by many interpreters.
Subtheme 6-2: Access to Employee Assistance is related to the second group of stakeholders, that is, interpreting agencies, being the interpreter’s usual employer. Most participants work with four main agencies in Melbourne. All offer EAP (Employee Assessment Program), but none actively promote it, resulting in many interpreters being unaware of its availability. Most alarmingly, almost all participants concurred with the precariousness of their freelance work and the apprehension about poorer job prospect if they admit that they are affected by trauma: Oh, so you have been affected? So it’s better you stay at home for a while. We can’t offer you any more jobs because, as you know, it’s full of trauma; it’s full of threat and you are not ready in a way we want . . . This is the way that usually they tell us. So it’s better to stay at home for a while, maybe one month or two months, and then, no income. (W)
Looking after interpreters’ psychological well-being is part of interpreting agencies’ duty of care as employers. Therefore, interpreting agencies should foster a sense of trust in their most important asset, ensuring interpreters will be supported, rather than fearing for their future work due to disclosure of distress from work.
Subtheme 6-3: Need for Targeted Professional Development relates to the third group of stakeholders: professional organizations and interpreting educators. Currently 12 universities and three public vocational colleges (or Technical and Further Education, TAFE) in Australia offer language-specific interpreting courses endorsed by NAATI (n.d.-a). Normally a language would only be offered when there is a viable student cohort and suitable teaching staff available, a situation resulting in a limited range of languages available to train at these institutions out of the 300 strong languages spoken in Australia. This results in a small range of well-catered-for languages where training is available at most institutions; these tend to be languages which attract international students as well as those better endowed from the more established ethnic communities. The status quo points to barriers to training for a large number of languages, causing critical shortages of trained interpreters in many new and emerging languages. This is because those languages are less likely to meet the number threshold required by institutions and less able to afford tertiary education. Since NAATI introduced mandatory minimum training in 2018, there is a stronger impetus for educational and training providers to include VT in their curricula or training course—a positive step forward. For those already working in the industry who were credentialed by NAATI pre-2018 and therefore may not have training, continuous professional development (CPD) courses on the topic become critical.
In the United Kingdom, there is little incentive for public service interpreters to join “a single national professional body . . . for peer networking, policies and CPD events . . . in the context of there being no statutory professional standards to which they are obliged to abide” (Roberts, 2015, p. 123). Australia is in a fortunate position to have strong professional organizations such as Australian Institute of Interpreters and Translators (AUSIT) and Translators and Interpreters Australia (TIA), which consistently offer CPD events and care much about their members’ mental wellbeing. Attending CPD ensures currency of the interpreter’s skills and knowledge and can be used to fulfill NAATI’s mandated recertification requirements. The suggestion by participants to introduce a specific category on mental well-being is worth canvassing with NAATI. In addition, what emerged under Theme 4: Misunderstanding the Limits of Confidentiality should also be addressed by formal courses and CPD by professional organizations. The understanding of confidentiality and how to navigate it while seeking support is imbedded in professional education such as for social workers; it should be the same for interpreters.
Limitations and Future Research Directions
Although the sample size of the current study is relatively large, this study did not quantitatively measure whether practitioners’ gender, years of practice, level of trauma content exposure, level of interpreting training, or level of NAATI certification correlate with their experiences of VT and their choice of coping strategies. This is due to limitations of the ethics approval where the study cannot reveal individual participants’ culture or linking personal views to their ethnic background. As a result, data collected in the focus groups were anonymous and collective in groups of five or six participant interpreters. It was, therefore, not possible to discern which interpreter said what nor link their comments to their personal profile. It also restricted the researchers to probe deeper into the relationship between participants’ help-seeking inclinations and their ethnicities, although cultural views of trauma were canvassed and emerged as relevant. This could be the basis for future research. Models of debriefing and professional supervision for interpreters should be pursued in the future as a matter of priority based on the data. Finally, interpreters’ vicarious posttrauma growth has not been explored in the Australian context with this population and should be considered for further studies.
Conclusion
Awareness of VT in interpreters in Australia is slowly growing, evidenced by an allocation of research funds for “best practice management of vicarious trauma for T&I [translating and Interpreting] practitioners” by NAATI (NAATI, n.d.-b), and by the inclusion of debriefing interpreters to avoid possible VT under Standard 9.6 of the Recommended National Standards for Working with Interpreters in Courts and Tribunals (Judicial Council on Cultural Diversity [JCCD], 2017). Given the important role interpreters play in delivering government services to community members who need language assistance, reducing the psychological occupational hazard to interpreters and maintaining their mental well-being is in the best interest of everyone involved.
In the spirit of the action research principles, this study provided debriefing opportunities for interpreters to articulate and share their experiences of VT and their thoughts for recovery and healing. Data analysis points to participant interpreters’ different understandings and processing of work-related VT. For some participants, cultural inhibitors prevent them from sharing their emotional vulnerability or seeking professional help. Key cultural inhibitors identified by the study are the stigmatization of mental health issues, the tendency to make light psychological distress versus physical illnesses, and the risks of losing community trust if seen as unable to cope because of work-related VT. The study shows that interpreters try in their own ways to deal with the emotional stress they feel from work, including various coping strategies, which may or may not help. Participant interpreters were clear in their requests to be treated with respect, as part of the professional team, rather than a “machine” or a “shadow,” be briefed about the context beforehand and offered debriefing and counseling after interpreted sessions. Data analysis points to the need for professional development to clarify the limits of confidentiality and to explain trauma and its vicarious possibilities. In asserting interpreters’ professional entitlement to briefing and debriefing, participants suggested training for professionals to learn how to work with interpreters professionally to achieve the best outcomes for their service users. The implications of this study are for interpreting educators, professional interpreter associations, interpreting agencies and other professions, and institutional users of interpreting services to be aware of the risk of interpreters’ VT and work respectfully and collaboratively to prevent and help interpreters recover from VT.
Supplemental Material
Supplemental_File_1_-_Participants_Language_Other_Than_English – Supplemental material for Professional Interpreters and Vicarious Trauma: An Australian Perspective
Supplemental material, Supplemental_File_1_-_Participants_Language_Other_Than_English for Professional Interpreters and Vicarious Trauma: An Australian Perspective by Miranda Lai and Susie Costello in Qualitative Health Research
Supplemental Material
Supplemental_File_2_-_Focus_group_guide – Supplemental material for Professional Interpreters and Vicarious Trauma: An Australian Perspective
Supplemental material, Supplemental_File_2_-_Focus_group_guide for Professional Interpreters and Vicarious Trauma: An Australian Perspective by Miranda Lai and Susie Costello in Qualitative Health Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.