
Abstract
A multidisciplinary literature theorizes the nurse–patient relationship. Nurses’ experiences with and within people’s social worlds are comparatively underexamined. The purpose of this dimensional analysis inquiry was to uncover dimensions of social relationships in nurses’ caring for adolescents and emerging adults with life-limiting illnesses and injuries. Semi-structured interviews with 21 nurses across roles and care settings in the United States occurred concurrently with theoretical sampling and inductive analysis. From the perspective of Caring for You Around You and within a context, Assessing Right for You, Diagnosing the Circle, and Planning Right for Me establish the conditions under which nurses shift between witnessing and participating in social relationships as they engage in the process I Draw and Redraw the Circle. The findings contribute a theoretical explanation of why and how nurses engage in relational care. Contextualizing the findings in nursing theory, family-centered care, and professional ethics elucidates directions for inquiry and practice.
Keywords
Adolescents’ and emerging adults’ relationships with their families, friends, peers, teachers, and other adults are developmentally and socially complex. Social relationships are widely acknowledged to be a critical context of youth development (Crosnoe & Johnson, 2011). During adolescence, people explore their senses of self and worldviews through their relationships (Hartup, 1993; Moore & Boldero, 1991). In emerging adulthood, a life stage of in-betweenness and transition, individuals continue to develop their identities within social communities (Arnett, 2000, 2014). A young person’s experience of a life-limiting illness or injury steeps these relational developmental processes in additional complexity. They may experience new relationships with health care providers and fellow patients (Ramini et al., 2008; Spratling, 2012; Tippl, 1995; Ward-Smith et al., 2007), as well as shifts in their relationships with friends and family (Hedström et al., 2004; Williamson et al., 2010; Zebrack, 2011). Nurses caring for developing adolescents and emerging adults must consider many relationships.
Attention to relationships features prominently in theoretical conceptions of nurses’ caring. As Allen (2014) commented in an exposition of the nature of nurses’ work, “the profession’s self-understanding is so tightly bound up with patient relationships” that social aspects dominate articulations of what nurses do (p. 136). A meta-synthesis of the concept of nurses’ caring unsurprisingly foregrounded the social, advancing the following definition of caring: “a context-specific interpersonal process that is characterized by expert nursing practice, interpersonal sensitivity, and intimate relationships” (Finfgeld-Connett, 2007, p. 202). Specifically, nurses’ performance of psychosocial care centers on and emerges from the relationships they have with the people for whom they care (Halldorsdottir, 2008; Li, 2004; Shimoinaba et al., 2013). Within a family-centered care model, nurses additionally care for a person’s “family,” broadly defined as supporters with biological, social, spiritual, or psychological ties (Benoot et al., 2020; McAndrew et al., 2020). Taken together, previous theoretical treatment of relationships in nurses’ caring suggests nurses enact the nurse–patient relationship and fulfill their caring obligations within a person’s larger relational community.
Although extant theoretical work holds value in elevating the relational components of nursing care, conceptual understanding of the day-to-day intricacies of social relationships in nurses’ caring is underdeveloped. Previous empirical inquiry provides a glimpse into some of the specific ways nurses care for people by attending to their relationships. Across the life span, caring for people with life-limiting conditions may involve nurses’ incorporation of the meaning of close relationships, contextualization of end-of-life care preferences in social communities, and formation of connections with the people for whom they care (Clark & Fasciano, 2015; Granero-Molina et al., 2014; Kane et al., 2004; Mast & Gillum, 2018; Prince-Paul, 2008; Weaver et al., 2016). These empirical studies offer insight into some of the dimensions of nurses’ involvement in relationships in the context of life-limiting illness or injury. Theoretical explanation of how nurses operationalize attention to and participation in all dimensions of relationships is an emerging area for further development.
Theoretical development of the nature of relationships in nurses’ caring holds especially critical implications for improving the care of adolescents and emerging adults with life-limiting illnesses and injuries. Significant knowledge gaps exist in understanding how to best care for young people and their families, as the end-of-life stage of adolescents’ and emerging adults’ lives remains largely understudied (Beerbower et al., 2018). The integration of relationships into end-of-life care as a means of honoring and validating identity merits particular focus given the well-established salience of relational identity development during adolescence and emerging adulthood (Leonard et al., 2017). From a clinician’s perspective, health care providers’ relational knowledge also can deepen awareness of a young person’s nearing death and inform how to support decision-making about transitions (Kobler et al., 2020). Among health care providers, nurses often occupy an especially privileged position, caring intimately for young people and families navigating day-to-day life with a life-limiting illness or injury. Nurses’ perspectives are critical in conceptualizing and executing high-quality end-of-life care sensitive to the emotional and relational needs of adolescents and emerging adults.
Purpose
Philosophically grounded in Symbolic Interactionism, this inquiry aimed to inductively explore how the meaning of social relationships derived through social interactions drives human action and behavior in the social world. Symbolic Interactionism is a grand social theory considering how social interactions guide the ways people assign meaning and act toward social objects (Blumer, 1986; Mead, 1934). The three premises of Symbolic Interactionism have direct application to the purpose of this inquiry. In alignment with Herbert Blumer’s first premise (1986), “human beings act toward things on the basis of the meanings that the things have for them,” and this inquiry was open to the ways a nurse may act differently toward a young person based on whether they conceptualize the meaning of that individual as “patient,” “person,” or even “friend” (p. 2). The second premise, which states that the meaning of objects derives from social interaction with the self and others, underscores how the ways nurses, families, friends, and young people act toward each other and themselves create the meaning of social relationships in care (Blumer, 1986). Third, Blumer postulated that action based on the meaning of objects is not an application of preexisting meaning, but rather the result of a person’s “interpretive process” (Blumer, 1986, p. 5). A friend, family member, or nurse is a social object that may carry a different meaning for different people and in different contexts.
This interactionist inquiry posed the question “what is the nature of social relationships in nurses’ caring for adolescents and emerging adults with life-limiting illnesses and injuries?” to examine all the conceptual possibilities and interpretive differences in the meaning of social relationships in nurses’ caring. Engaging nurses’ stories of day-to-day care work offered an opportunity to uncover how social relationships operate in nurses’ care of young people experiencing life-limiting illnesses or injuries.
Method
The poorly understood and subjective nature of social relationships impelled a qualitative mode of inquiry. As an interactionist method, dimensional analysis held particular utility in interpreting the socially constructed nature of this complex phenomenon (Kools et al., 1996). Investigators using dimensional analysis method ask and answer the question “what ‘all’ is involved here?” by identifying implicit and explicit dimensions of a phenomenon and designating their relationships in an explanatory matrix (Schatzman, 1991, p. 310). Consistent with the dimensional analysis method, data collection and analysis proceeded concurrently and iteratively (Schatzman, 1991).
Ethics Approval
The Institutional Review Board (IRB) at University of Pennsylvania approved the study. The study was determined to be exempt from Category 2 under the 2018 Common Rule. The IRB approved the study protocol and all study documents, which included the recruitment flyer, informed consent form, interview guide, and a distress protocol. The distress protocol detailed a plan to pause or stop the interview if a participant expressed or appeared to be in distress and included available counseling resources for follow-up.
Participant Selection and Sampling
This inquiry aimed to inductively uncover how nurses conceptualize “end-of-life” within their nursing practice and care setting rather than rely on existing biomedical prognostic models. Life-limiting illness or injury operationally included any physical or mental health condition or state that might result in death, such as intentional and unintentional injuries, acquired conditions, congenital conditions, acute conditions, and progressive conditions. Nurses’ care settings could be hospitals, ambulatory clinics, emergency departments, hospice centers, psychiatric facilities, or home care in both pediatric and adult institutions in three neighboring states in the Mid-Atlantic region of the United States. Experience caring for adolescents and emerging adults included care for people between the ages of 12 and 24 years (Arnett, 2000).
Recruitment began through networking with nursing faculty, nurse managers, nurse practitioners, and registered nurses via email and LinkedIn. Initial purposive sampling enabled the deliberate selection of a heterogeneous group of nurses with direct experience caring for young people with life-limiting illnesses or injuries. After a few interviews with nurses in the purposive sample, theoretical sampling with snowball technique proceeded concurrently with data collection and analysis until theoretical saturation. Concepts from the emergent data analysis drove theoretical sampling to build on and from preliminary theoretical understanding (Conlon et al., 2020). Theoretical saturation occurred when additional interviews confirmed the dimensions, offering no additional insights or theoretical clarification (Hennink et al., 2017; Morse, 2015). No participants dropped out of the study.
Data Generation
One-time interviews with nurses took place from July 2019 to January 2020. Participants chose a location that was comfortable and convenient for them for a one-on-one audio-recorded interview. Locations included coffee shops, reserved breakout rooms, conference rooms at nurses’ places of work, and nurses’ homes. Interested participants received a copy of the informed consent form via email before the interview. Interviews began with an informed consent process that included verbally walking through the consent form together and obtaining written consent. The semi-structured interview guide included open-ended questions and probes related to nurses’ approaches to care, conceptions of the meaning of end-of-life, and experiences witnessing and participating in young people’s social relationships. Two pilot interviews with a convenience sample of nurses who have experience caring for people at end-of-life in pediatric oncology and critical care helped to develop the initial interview guide. Continual adaptation and purposeful refinement of the guide occurred throughout data collection to saturate the dimensions and test theoretical relationships (Conlon et al., 2020). Taking field notes before and following each interview enabled description of the setting and context, as well as the continual reflection on researcher positionality. Audio-recorded interviews lasted from 25 to 65 minutes, averaging 47 minutes. Transcripts were carefully reviewed to assure verbatim transcription accuracy after transcription through Rev, an encrypted automated transcription service.
Data Analysis
Proceeding simultaneously with data collection, data analysis was an inductive and iterative process of moving between reading transcripts for gestalt, selecting vignettes, dimensionalizing, and coding. Ranging in length from a few lines to a few pages, sections of the transcript that were particularly dense, confusing, contradictory, or otherwise rich sources of information became vignettes. Dimensionalizing, inductive coding, analytic memoing, and dialogic engagement helped to fully unpack selected vignettes. Dimensionalizing expands data bits and codes into their dimensions and properties in ways that help uncover implicit dimensions and make analytic decisions (Kools et al., 1996) (Figure 1).

Excerpts from dimensionalization sessions.
Open, axial, and theoretical coding with constant comparative technique proceeded concurrently with the processes of reading transcripts for gestalt and selecting vignettes (Glaser, 1965). Four undergraduate research assistants and student nurses participated in coding subsets of transcripts. Line-by-line open coding helped to break codes free from speakers’ intended contexts, fracturing the data into small meaning units (Graneheim & Lundman, 2004). With three interview transcripts densely open coded, patterns became evident and organizing in vivo codes into conceptual groupings began. Axial codes labeled these groupings. After open coding and axializing the first six interviews in their entirety, the focus shifted to fracturing and dimensionalizing vignettes from the remaining interviews. Coding vignettes became a way of theoretically sampling from the data to test and refine theoretical relationships (Hennink et al., 2017). Theoretical codes took shape from patterns in axial codes, providing opportunities for additional abstraction and interpretation. Reflection on the nature and dimensions of theoretical codes determined their placement in the explanatory matrix which visually represents the dimensions of a phenomenon through perspective, context, conditions, processes, and consequences (Figure 2). The theoretical codes that became components of the matrix compose the findings of this analysis, illustrated through quotes from nurses’ interviews.
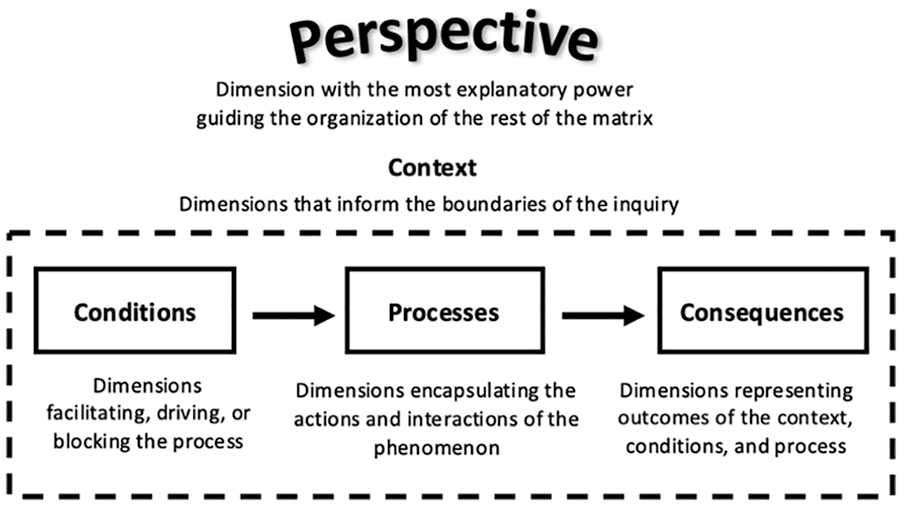
Explanatory matrix of dimensional analysis.
Maintenance of Rigor
Continual critical reflection on positionality and social location enhanced rigor in this post-positivist inquiry. Interview participants co-constructing data with a fellow nurse often used detailed medical terminology and expressions of “you know how it is” that implied common socialization in nursing. At other times, positioning as an academic created distance from nurse participants working in the clinical setting. During the recruitment phase, several consulted clinicians suggested that nurses in certain settings might be unable to speak to the phenomenon of social relationships because the people they care for are in very poor health or deeply sedated. Reflection on deontological orientation helped examine the ways the belief that all people are infinitely worthy of social connection drove design decisions to include all care settings.
This inquiry also attends to Graneheim and Lundman’s criteria for trustworthiness in naturalistic inquiry (Graneheim & Lundman, 2004). A thorough description of the participants in this study increases readers’ ability to assess the transferability of the findings to another group. Detailed procedural, sampling, and analytic memos comprised an audit trail that enhances dependability (Guba, 1981; Thomas & Magilvy, 2011). Frequent reviews of this audit trail occurred with colleagues in a qualitative dialogic engagement collective and team meetings with research assistants. Collaboration with professionals who have clinical expertise in pediatric and adult nursing care enabled ongoing assessment of emerging findings’ confirmability.
Findings
The findings of this dimensional analysis constitute a theoretical explanation of the nature of social relationships in nurses’ caring. In approaching the social relationships of adolescents and emerging adults at end-of-life, nurses assess, plan, diagnose, intervene, and evaluate. The explanatory matrix emerges from the vantage point of the nurse (Me) caring for the adolescent or emerging adult at end-of-life (You). The perspective, Caring for You Around You, guided the organization of other dimensions into context, conditions, processes, and consequences (Figure 3). The contextual dimensions Accept and Except, Handling Time, and Where I Care form the conceptual boundaries of this inquiry. The conditions of Assessing Right for You, Diagnosing the Circle, and Planning Right for Me drive the process of I Draw and Redraw the Circle. The process ultimately creates the consequence of Evaluating the Connection.

Social relationships in nurses’ end-of-life care.
Participants
Twenty-one nurses participated in this study (Table 1). Nurses’ current functional roles included registered nurse (n = 10), nurse practitioner (n = 9), and clinical nurse specialist (n = 2). Most settings where nurses practiced were institutions focused on the care of pediatric patients (n = 13). Eight nurses practiced in institutions that care for adults. Most nurses worked in inpatient settings including inpatient units (n = 10), intensive care (n = 5), and the emergency department (n = 1). Four nurses worked in outpatient clinics and one in home care. Most participants practiced in urban academic medical centers (n = 18). Others practiced in rural settings.
Self-Reported Demographics.
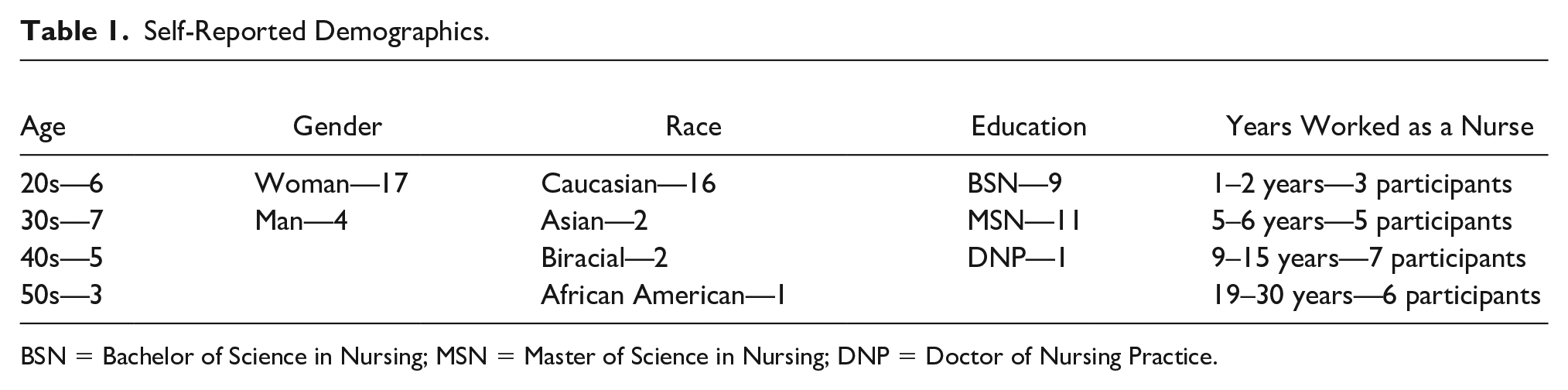
BSN = Bachelor of Science in Nursing; MSN = Master of Science in Nursing; DNP = Doctor of Nursing Practice.
Perspective
The theoretical code Caring for You Around You held the most “explanatory power” and thus became the perspective of the explanatory matrix that determined the relative salience and relationships between other dimensions (Kools et al., 1996; Schatzman, 1991, p. 318). Adolescents and emerging adults with life-limiting illnesses or injuries exist at the centers of circles of social actors. Regardless of the size or composition of the circle, the perspective of Caring for You Around You substantiates the unidirectionality of caring for and about, rather than with, a person with a life-limiting illness or injury. The circle emerges from and explains the relationships between context, conditions, processes, and consequences.
Nurses are initially outside the circle. Sometimes nurses traverse the circle to care for an adolescent or emerging adult directly. One participant described how as a nurse she is often a “third person,” breaking through people’s desires to protect their parents and determining how young people are really feeling. In other cases, nurses care for young people indirectly, through relationships and interaction with the social actors of the circle. For example, one nurse cared by way of the circle to address a young person’s concern that his lack of appetite upset his mom. By supporting his mom in understanding that her son was getting all the nutrition he needed, this nurse cared for the person at end-of-life. Nurses explain performing caring by way of the circle in terms of their obligation to and responsibility for the person at the center. The reasoning “I was truly gonna care for him, in some ways I felt like I was caring for his girlfriend as well because if I kept her comfortable and content, um, then she was able to provide that care to him . . . I was providing nursing care almost like through her” exemplifies caring by way of the circle. Nurses care by way of the circle to achieve care for the adolescent or emerging adult at the center.
After a person dies, the circle becomes decentered. Nurses temporarily lose the focal point of their care before shifting to caring for the circle. Accustomed to concentrating on the person at the center, some nurses described feeling uncertain about how to quickly recenter focus to the family after a young adult dies. For other nurses, a sense of closeness that emerged in caring for the person by way of the circle resolved uncertainty about continuing those relationships after the circle loses its center. Commenting on his decision to attend a person’s funeral, one nurse drew on the nature of his connection with the family, explaining, “I did go because I had that connection with both the patient and the family.” Caring for You Around You represents nurses’ resolute focus on the person at the center during a young person’s life and the shift to caring for the circle after a young person’s death.
Context
The context of the explanatory matrix circumscribes the conceptual boundaries of the inquiry. Creating the environment in which social relationships exist, the contextual dimensions of this analysis included three elements: Where I Care, Accept and Except, and Handling Time.
Where I Care determines the boundaries of social relationships that result from the distinction nurses make between “inside” and “outside.” Inside and outside refer not to physical localities but rather to the qualities of a setting that make relationships appropriate or off-limits. For example, one participant considered visiting the hospital room of a young person she was not assigned to take care of that day to be “outside” her care setting and thus inappropriate. Nurses often expressed, “it’s frowned upon in the hospital to be friends with them outside of the hospital setting.” However, one nurse emphasized how he uses his fundraising organization as a way of responding to young people’s questions about meeting up outside the hospital: “I can kind of fall on (my fundraising team) and just kind of be like, ‘well, look, um, you know, I have this event coming up, maybe, you’re welcome to come’.” The health condition–focused fundraising event retains the qualities of “inside” Where I Care and thus the appropriateness of social connection in that setting. Similarly, from the perspective of Caring for You Around You, a funeral is “inside” the care setting if a nurse conceptualizes their attendance to be care for the circle. The sharp distinction between inside and outside Where I Care forms critical boundaries for social relationships as assessments of the safety and comfort of the person and nurse depend on the relative location to the setting of care.
Accept and Except establishes norms and exceptions for who and what is acceptable in the circle. Nurses’ associations with certain cultures, relational labels, and developmental stages determine acceptance and exceptions. For example, one participant’s acceptance of a large number of visitors in a young person’s hospital room derived from her assumption, “it’s just like that’s Hispanic.” Legal considerations of who is next of kin also drive acceptance, evident in a participant’s declaration that “obviously parents can stay overnight (in the hospital).” At the same time, the complexity of the end-of-life phase sometimes creates exceptions to what is typically accepted. One nurse reflected on shifts in her application of certain relational labels: Parents shouldn’t be child’s friends . . . but at the same time like they’re spending so much time with this parent that their parent becomes their friend . . . it’s a different dynamic of a relationship I feel like when it becomes like end-of-life.
Nurses made exceptions so that they could align their expectations with the observed realities of young people’s social worlds at end-of-life. How a nurse reconciles typical adolescent development with the context of life-limiting illness or injury similarly drives what they Accept and Except. One participant’s identification that a person’s friends are at “an age where people are doing their own thing” helped her rationalize why friends were not visiting the young person she was caring for. Accept and Except specifies and explains how a nurse determines who is acceptable in the circle.
Handling Time encapsulates the notion of time being a fragile object that nurses, the circle, and young people hold gingerly. Time is needed to build and maintain the relationships that create the circle. In the expectant period of uncertainly moving toward life’s end, spending remaining time can be a zero-sum game. One participant observed the social dynamic between a person’s parents and girlfriend and questioned, “are the parents willing to share like their last like couple days with you? . . . do you give the girlfriend her own time? But then like you’re losing your time.” Time at end-of-life is a commodity taken and given, but also marked and created. Several nurses described how they and the circle supported and became part of a young person’s marking of time whether centered on prom, a 21st birthday, or a last Valentine’s Day with a fiancé. Handling Time also includes attempts to create time through legacy work and extensions of the social world. One nurse shared a conversation she had with an adolescent who was speaking about knowing where she will go after she dies. Connecting her current caring to her caring for other young people who have died, she told the adolescent, “[there are] three kids (in heaven), they are all nice kids, you know so you can join.” This nurse cares by offering the person a notion of future time, beyond the present world. Analogously, time is not limited in an absolute sense and will continue for the nurse and circle after the person dies. One participant recalled a young person’s mom explaining the absence of the person’s sister: “We don’t want her to come (to the hospital) because like she needs friends like those are the people that are going to support her when her sister dies.” In this case, the continuing nature of time explains and contextualizes social relationships in the present. Spent and created, limited and continued, marked and lost, time at end-of-life represents a series of contradictions. Time and the strategies nurses, the circle, and young people at end-of-life use to handle it provide context for understanding the nature of social relationships in nurses’ caring.
Conditions
In the dimensional analysis method, conditions shape the processes, driving the actions and interactions of a phenomenon (Kools et al., 1996). This dimensional analysis revealed three conditions: Assessing Right for You, Diagnosing the Circle, and Planning Right for Me.
Assessing Right for You is a nurse’s assessment of the capacity, safety, comfort, and situational needs of the young person at the center. Sometimes assessment of capacity leads nurses to determine that the person is unable to interact as a social being because of cognitive impairment, sedation, or death. One participant commented on the changes nurses sense in young people nearing end-of-life: “we always make the practice as a nurse of like, us like neuron nurses, that like you watched them, their personalities die before they do.” Another nurse’s statement, “they’re usually neurologically devastated, so we don’t get to actually work with them, just their families,” reflects how the assessment of capacity guides the focus of nurses’ caring. From the perspective of Caring For You Around You, a nurse shifts to caring for the circle when the young person no longer can interact as a social being. In addition to capacity, Assessing Right for You necessarily includes an appraisal of safety. Sometimes nurses are trying to keep people protected from the threats of the circle as a whole; a person with low white blood cell counts “can’t be around people” or a person who is sedated must be “kept calm” with limited visitors. Other times, nurses are looking to keep people safe from specific social actors in the circle, such as fellow patients. One nurse, for example, expressed her wariness of connections between people with eating disorders that might reinforce life-threatening disordered eating behaviors. Having considered capacity and safety, nurses Assessing Right for You explore a young person’s comfort. Determinations about the size and composition of the circle are often based on comfort, whether a nurse is allowing a person’s dog onto the hospital unit or creating visitor restrictions to exclude social actors who are not comforting. When assessing comfort, nurses continually notice a young person’s situational needs as evident in the distinction one nurse makes between a “rough day” and a “good day”: “[T]he patient had a rough day . . . Everyone can stay tonight . . . if he had a good day and things that stabilized, then we needed to get some people out of that room.” Nurses’ considerations of capacity, safety, comfort, and situation direct how the condition of Assessing Right for You drives the process of social relationships in nurses’ caring.
In Diagnosing the Circle, nurses witness and evaluate the composition and dynamics of the circle. As one nurse relayed, “my role as a nurse is to know you as a person and so I want to, I need to know what’s important to you. So if that’s people than I want to know about that.” Nurses take stock of “who’s in your circle” in the context of Where I Care, Accept and Except, and Handling Time. Nurses gather evidence about outside Where I Care from visual cues such as photographs in a person’s inpatient room or discussions about a person’s family structure with a social work colleague. Within the context of Accept and Except, nurses note the absence of expected members of the circle or the presence of unexpected ones. One participant, for example, reflected that an adolescent “has so much more relationships than like the immediate circle” even if only parents are present at the bedside. Nurses noted that in the context of life-limiting illness or injury, front desk, environmental services, or dietary staff are often underconsidered members of the circle. Nurses also examine fluctuations in the circle’s composition that exist in the context of Handling Time. One participant described how in the middle of an illness the support system weakens, but at end-of-life social actors become more visibly present again, with everyone coming “out of the woodwork” as death nears. After identifying the circle’s social actors within the context, nurses consider the actors’ relational roles. In many cases, the contextual dimension Accept and Except dictates relational roles. One nurse’s justification “because she was the sister, not the parent” or another nurse’s conclusion that maintaining normalcy is the “role that friends play” denotes what is acceptable for whom. When assessing relational roles, a nurse often identifies “the gatekeeper.” The gatekeeper, usually a mother but sometimes a significant other, filters who is part of the circle to shield the person at the center. One participant’s description of a gatekeeper illustrates some of the dimensions of this role: “anybody who wanted to visit in hospital, it had to be cleared with mom . . . And mom was very much like not everybody gets to be part of this.” After determining who is in the circle and their relational roles, nurses characterize the strength and health of relationships the circle has with the person at the center. Labeling social actors based on the condition of Assessing Right for You is part of diagnosing. Some social actors are “incredible” and “helpful,” whereas others are the “wrong crowd” or not a “model figure.” A nurse additionally characterizes the gestalt health of the connection by labeling relationships as “commendable” or “poor.” A nurse’s diagnosis drives the process of I Draw and Redraw the Circle.
Planning Right for Me involves an assessment of clinical utility, safety, and comfort similar to Assessing Right for You. However, Planning Right for Me is decidedly centered on the nurse rather than the young person. Nurses considered clinical utility as they reflected on the therapeutic value of cultivating and maintaining social relationships in the fulfillment of their professional role. Connecting with a person at end-of-life, as one nurse summarized, “maintain[ing] a relationship when you need it,” can be a clinical tool for assessing congruence with goals of care or inspiring legacy work. In addition to clinical utility, Planning Right for Me involves a nurse’s assessment of physical, psychological, and professional safety. A hospital room packed with visitors creates physical hazards for a nurse trying to care for a person at end-of-life. A visitor’s comments threaten nurses’ psychological safety in ways that require implementing restrictions. As one participant summarized, “we’re trying to be compassionate, but yet strict and about our safety.” In Planning Right for Me, nurses also consider professional security, both in their relationships with and responsibilities for the person at the center. Overall, nurses experienced tension when the boundaries between nurse and friend blur. They acknowledged potential professional liabilities involved in having deep relationships with the people for whom nurses care. One participant elaborated on how social actions can become risks to professional security when he stated, “they’ve always warned us, look, be careful because if you say or do the wrong thing, you might, you might lose your job.” Another nurse relayed, “I want to be their friends and I, I try to be their friend. Um, however, I do get nervous too because I know that I have to maintain like, uh, uh, professionalism to it.” A nurse’s sense of professional safety might modify their response to a young person’s social relationships. For instance, one nurse’s worry about “get(ting) in trouble” with the charge nurse if a person and their significant other were sharing a hospital bed informed her approach to the process of social relationships. Planning Right for Me finally involves a nurse’s personal comfort based on their sense of closeness to the situation. Some nurses expressed the rapport-building benefit of being close in age to a person they are caring for, whereas others reflected on the challenge: They could be like my friend or peer outside of the hospital . . . especially in those cases, I feel like I put up more of a like I’m your nurse this is like the expectation . . . I’ll talk with you about like small things, but like I don’t really want to get into big conversations with you or like I don’t want you to feel like I’m your friend . . . I’ve definitely like lied to patients that I’m older than I am.
In a nurse’s attempts at Caring for You Around You, closeness in age can be a liability requiring distancing. A nurse might similarly plan to maintain distance when a young person they are caring for reminds them of their relational identity as a parent. Taken together, nurses’ assessments of clinical utility, safety, and comfort compose a plan for the process.
In the situation-specific theory of social relationships in nurses’ caring of adolescents and emerging adults, the conditions Assessing Right for You, Diagnosing the Circle, and Planning Right for Me interact to drive the process. In Planning Right for Me, a nurse sometimes determines that based on clinical utility, safety, or comfort they, or they alone, are not “right.” In these cases, nurses return to conclusions drawn in Diagnosing the Circle to team up with or substitute themselves with other health care team members. Assessing Right for You and Planning Right for Me continue to drive the process even when a social worker or child life specialist carries out that process. One participant’s statement, “we want [security guards] to be the bad guys” who restrict visitors, underscores the continuing emphasis on people’s and nurses’ safety. Notably, the relative salience of the conditions can differ between nurses. For example, one nurse’s assertion, “it’s about what’s good for the patient not what’s good for me,” reflects his differential weighting of the conditions Assessing Right for You and Planning Right for Me. Acting in emergent combination, the conditions facilitate or block the process.
Process
I Draw and Redraw the Circle changes the size and composition of the circle. From the perspective Caring for You Around You, a nurse sometimes cares for a person directly, drawing the circle smaller by setting limits on who is in the circle. Based on Assessing Right for You and Planning Right for Me, one nurse reasoned, “I’m going to protect my patient and so I’m going to keep everybody and everything away from it so nobody can hurt my patient.” Critically, this nurse frames her redrawing of the circle in terms of caring, noting “sometimes you really need to set those limits because that’s how you care for someone.” Nurses care by altering the size and composition of the circle based on their assessments, diagnoses, and plans.
The contextual and conditional dimensions feature prominently in whether a nurse remains outside the circle or draws themselves into the circle. Within the context of Handling Time, nurses acknowledge that time is limited and sometimes draw the circle to deliberately keep themselves outside. One nurse, for example, diagnosed the circle, assessed right for you, and emphasized the importance of “being aware that they’re having these social interactions. So you should not put yourself in, in their interactions and you should give them time.” Driven by the condition Planning Right for Me, nurses may keep themselves outside of the circle by encouraging a young person’s engagement in peer friendships: you know with school that’s what they teach you like you really need to like set boundaries and the families like they go through such a hard time of their lives that like we become their support system. But I feel like you really need to change your mindset as like a provider and as a nurse. And kind of how I feel like it’s most important is to encourage like, you know, your relationships, and like friendship bonds, like from high school or from your neighborhood.
Importantly, even in cases where nurses remain outside the circle, nurses are constantly Assessing Right for You, Diagnosing the Circle, and Planning Right for Me. One participant explained, “because I think that mom was open about what was happening with her child, I was always very comfortable giving them space.” Even when she was outside of the circle, this participant was sure to maintain her comfort and the person’s comfort.
Based on the conditions of assessing, diagnosing, and planning, nurses sometimes redraw the circle to include themselves. One nurse recalled staying in a person’s intensive care unit (ICU) room all night because this was “helpful to the patient,” especially when his diagnosis of the circle suggested others were not often physically present. Similarly, when the family is not with a young person in the outpatient infusion setting, a nurse may step in to socially engage with the young person. Whether the circle is large or small and the nurse inside or outside, I Draw and Redraw the Circle is how nurses care.
Consequences
The consequence of the conditions of assessing, diagnosing, and planning and the process of I Draw and Redraw the Circle is Evaluating the Connection. Evaluation is how a nurse reacts and responds to the processes in ways that cyclically reinforce or alter the conditions. Professional safety features prominently in this evaluation. Nurses rely on their assessments, diagnoses, and plans to justify the appropriateness of relationships they form through I Draw and Redraw the Circle. Describing being part of a person’s circle, one nurse underscored that his concern about the person’s social health led to the close relationship he had with the person: “I mean, nothing ever was inappropriately asked about social events or not, but we talked about other happenings on the unit, upcoming events at, at, in his life.” Nurses are quick to emphasize that because the conditions drive the social connections formed through I Draw and Redraw the Circle, these connections are right for the person and the nurse.
Drawing the circle in a way that includes themselves may lead nurses to develop a level of closeness that transcends the boundaries of Where I Care and Accept and Except. One nurse commented that the closeness some of her colleagues have with young people exists “outside” of Where I Care and beyond the typically accepted labels for the nurse–patient relationship: a level of closeness that is like past [young people] wanting to have you as a nurse. That’s a level of closeness where it’s like, like people came in from home to see the family after he had died . . . I haven’t achieved that level in my nursing career yet. That’s a level of closeness that is almost like friendship.
In close relationships, the boundary between the symbolic objects “nurse” and “friend” blurs and nurses may experience social connection outside of Where I Care.
Nurses additionally evaluate themselves as assessors, diagnosticians, planners, and drawers by considering how connection with the person and the circle affected their well-being. The contextual variable Handling Time again holds particular significance, as nurses’ deep attachments with a person nearing end-of-life can be emotionally challenging when a person dies. At the same time, the continuing nature of time creates the possibility a nurse might have a lasting relational connection with other social actors in the circle. One participant shared that a person’s mom calls her each year on the anniversary of the person’s death. These calls both mark time and affirm this nurse’s continued presence in the circle, “you’re a part of our family,” even after the circle has lost its center. Before, during, and after a young person’s death, nurses experience consequences of being inside and outside the circle.
Discussion
From the perspective of Caring for You Around You, the explanatory matrix offers a theoretical foundation for understanding the nature of social relationships in nurses’ caring for adolescents and emerging adults with life-limiting illnesses or injuries. Where I Care, Accept and Except, and Handling Time together form the context in which the conditions Assessing Right for You, Diagnosing the Circle, and Planning Right for Me drive the process of I Draw and Redraw the Circle and ultimately the consequence of Evaluating the Connection. Overall, the nature of social relationships in nurses’ caring unfolds in alignment with the five stages of Ida Jean Orlando’s Deliberative Nursing Process Theory: assess, diagnose, plan, intervene, and evaluate (Orlando, 1961). This inquiry’s findings suggest nurses use the same steps in managing the complexities of social relationships to provide relational care.
The situation-specific theory of social relationships in nurses’ end-of-life caring for adolescents and emerging adults both corroborates and diverges from extant theory. The perspective Caring for You Around You aligns with a biopsychosocial model (Engel, 1977) and supports dominant social constructions of family-centered clinical care as evolving from an absolute focus on the person at the center (Jones et al., 2014; Noome et al., 2016). The findings of this dimensional analysis importantly expand on previous conceptions of family-centered care by specifically explaining how and why nurses interact with or become part of the circle. Some previous empirical investigations similarly describe the ways nurses invite the family in, give the person’s loved ones time alone with the person, or become part of the circle if there is no family present (Broom et al., 2014; Noome et al., 2016; Zomorodi & Lynn, 2010). However previous inquiry also reveals cases where the circle “reject(s) the nurse,” suggesting that sometimes gatekeepers retain control over the circle’s composition (Ramvi & Ueland, 2019, p. 207). The positioning of the nurse as the drawer also diverges from Krishna and Kwek’s Ring Theory of Personhood (Krishna & Kwek, 2015). In the Ring Theory of Personhood, the person at end-of-life determines which relationships are in the relational ring and which are in the societal ring (Krishna & Kwek, 2015). Although the transitory nature of who is in the circle mirrors the findings of this inquiry, adolescents and emerging adults do not choose who is part of the circle. Rather, from the perspective of Caring for You Around You, the composition of the circle is decided for them and around them based on the conditions and within the context. Future investigation inclusive of the circle’s and the young person’s perspectives will deepen and refine understanding of who is the drawer under what circumstances.
The limitations forming the boundaries of this preliminary situation-specific theory incite additional directions for future inquiry. This study takes a notable step toward heterogeneous sampling across care settings, nurses’ functional roles, and illness or injury foci. However, additional heterogeneity is imperative especially in terms of outpatient and home care settings, psychiatric illnesses, and participant demographic diversity. The socially constructed association of end-of-life with physical illness and increased acute care utilization demands deliberate consideration of life-limiting psychiatric illnesses and non–acute care settings. Second, this inquiry intended to broadly uncover all conceptual dimensions of social relationships in nurses’ caring. The findings do not comment on potential differences by type of illness or injury, care setting, geographic area, or characteristics of the nurses such as developmental stage or years of nursing experience. Methodologically, an a priori decision that these differentiating factors were salient to the phenomenon would have been conceptually limiting and incongruent with dimensional analysis method. Future inquiry can explore care setting and nurse differences to additionally elucidate the dimensions of social relationships in nurses’ caring.
Implications for relational care in practice and policy rely on developing understanding of all the dimensions of social relationships in nurses’ caring for people with life-limiting illnesses and injuries. In the performance of person and family-centered care, the conception of the nurse–person and nurse–circle relationships as therapeutic tools is coupled with a pervasive insistence on maintaining professional boundaries and emotional composure. The intentional distance nurses maintain from the person for whom they care marks the nurse–patient relationship as limited in time, place, and purpose, distinguishing this relationship from other relationships (Halldorsdottir, 2008). The context and conditions of this situation-specific theory mirror the boundaries of time, place, and therapeutic intent. However, this inquiry also revealed that nurses sometimes care by becoming part of the circle before, during, and after a young person’s death. In this way, nurses might enter dual relationships, assuming a second relational role in addition to their professional role (Kagle & Giebelhausen, 1994; Reamer, 2003). The existence and implications of friendship in nurses’ caring is an open question for future inquiry.
Maintaining professionalism and deep social connection takes an emotional toll on nurses, especially those caring for persons and families transitioning from curative to palliative or end-of-life care (Broom et al., 2014). How nurses participating in relational care navigate the dual nature of relationships in nursing care remains largely absent from practice recommendations and professional codes of ethics. In their piece on professional boundaries in end-of-life home care, Abrams and colleagues (2019) argue for “a positive, relationship-based and inclusive attitude to professional boundaries which reconsiders them as including relational care.” Answering this call will require grounding practice and policy changes in theoretical understanding of the complex nature of social relationships in nurses’ caring. This situation-specific theory of social relationships in nurses’ caring lays foundation for future research and relational practice efforts to support all who are involved in young people’s experiences of life-limiting illness or injury.
Footnotes
Acknowledgements
The author wishes to express deep gratitude to the nurses who shared their stories and much appreciation for the contributions of Sarah H. Kagan, PhD, RN, FAAN, Christine K. Bradway, PhD, RN, CRNP, FAAN, Cynthia A. Connolly, PhD, RN, FAAN, Barbara Medoff-Cooper, PhD, RN, FAAN, Clare Whitney, Ph.D., MBE, RN, and research assistants Anna Bennett, Atalya Barosy, Ariel Tan, and Alana Windmueller. The author acknowledges the Rita and Alex Hillman Foundation for doctoral funding support through the Hillman Scholars Program in Nursing Innovation.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author was supported by the University of Wisconsin Department of Family Medicine and Community Health Primary Care Research Fellowship, funded by grant T32HP10010 from the Health Resources and Services Administration.