
Abstract
The Max Bramer keynote address at the annual Special Care Dentistry Association (SCDA) conference provided an opportunity for reflection on our journey as health care professionals to humanize care for all people, and particularly those who are disabled. It is important to review the history of disability and discrimination to understand the progress made to date, and then consider the array of steps possible in further refining the humanistic dimensions of dental care. The typologies of tourist, traveler, adventurer, and scout were formulated to consider varieties of humanized care found within articles published in Special Care in Dentistry. Considering exemplars for each of these four typologies leads to reflections about how dentistry can embrace understanding, improve training of new dental professionals, tailor care for people with disabilities, and advocate for equity.
Keywords
Max Leo Bramer was a pioneer in what was called for many years “dental care for handicapped individuals.” (“Reports from Academy of Dentistry for the Handicapped,” 1983). He devoted 55 years of his career to the treatment of some of the most challenging patients: frail older adults, hospitalized and critically ill people, children with multiple chronic conditions, and people with intellectual and developmental disabilities. On the occasion of the 32nd annual meeting of the Special Care Dentistry Association (SCDA), I offer remarks in the same vein that Dr. Bramer might if he were here: to celebrate the work that has been done in special care dentistry and to point out work yet to be done to humanize the care of special needs patients. The goal is to explore paths to humanizing care by attending to the art and craft of dentistry and the health professions more generally. Today, we will consider ourselves as travelers in the world of human ability and disability, reflect on our journey through disability history, and seek ways to improve the quality of care provided to those with special health care needs.
The imagery of a traveler is appealing to me, and filled with metaphorical possibility. Since I just returned from a month in the wilds of Montana and Idaho, I can speak about the roads that took me there. The utilitarian freeways are marked with bold, four-lane efficiency. Those freeways typically connect major metropolitan hubs in a direct route. Freeways are designed for speed and note that travelers should proceed with haste. If you are in a hurry, that maximum speed limit is seen by many travelers as a mere suggestion. Because of the pace and volume of freeways, people on bikes are redirected from the freeway. It is just not safe for bikers. Similarly, strollers, tricycles, and wheelchairs are not welcome on the freeway. It is designed for the most-fit kinds of vehicles adapted to that particular mode of transportation. The backroads are more suited to vehicular diversity. The lower speeds and more circuitous meanders accomplish a different purpose. Travelers on the by-ways may be looking for changing leaves in autumn. They may be looking for little gems, like the Hells Backbone café in Boulder, UT, or the Slice of Pie shop in Rolla, MO. Sometimes, people drive backroads just for the pleasure of an explore. “Let’s go on a Sunday drive,” as my father used to say, just for the sheer joy of it. With that spirit of adventure, we can consider journeying into the world of humanistic care for people who live with disability. We may—or we may not—share the experience of disability, but we can learn.
Considering the Language of Disability in Special Care Dentistry
The first stop on our journey is a semantic one. What is the meaning of special care dentistry, and what is the relationship of special care dentistry to disability? At the broadest level, “special health care needs” encompasses people who have chronic disabling conditions, age-related special care needs, and the 60 million Americans, roughly 19% of the population, who self-report as having a disability. Within the subset of people with a disability are those who have developmental disabilities arising before age 22. Among those with developmental disabilities are people with intellectual disability, a combination of cognitive and adaptive function challenges (Schalock & Verdugo, 2019).
In critical disability studies, there is a different conversation taking place. With more attention to emancipatory and critical approaches, such as crip and queer studies, we have an opportunity to re-think the medical paradigm of naming and labeling. Cover terms like “special needs” and “children with special health care needs” are being challenged by the disability community (Cokley, 2020; Gernsbacher et al., 2016). One concern is that by shying away from the word disability, we mis-represent people with disabilities using a dysphemism (rather than a euphemism) that does more harm than good. How will people with disabilities identify with a community and culture of disability if health care professionals divert disability social identity using substitute wording? Owning the disability label recognizes the political power of people with disabilities that wrought the Americans with Disabilities Act in 1990 and the Amendment to that act in 2008. Those acts were made possible through the work of people who self-defined as disability rights advocates working on behalf of a disability community. They did not identify as “people with special health care needs,” (with all the vague and multiple meanings implied). Let us, as travelers, consider carefully the language we bring with us, and the language of the people who live where we are visiting, in a time, place, and space of disability.
Situating Special Care Dentistry in a Historical Disability Context
In celebration of the 30-year anniversary of ADA legislation, The New York Times published a special issue in February of 2020, part of which reviewed the history of the Willowbrook State School in New York. Beginning in 1947, children with developmental disabilities were treated inhumanely, often for the entirety of their lives. By 1963, the facility housed over 6,000 intellectually disabled people in a building designed for a maximum capacity of 4,000. The overcrowding and neglect that resulted is legendary. Willowbrook closed for good in 1987. What happened over those years offers us a cautionary tale of abuse directed at people with intellectual and developmental disabilities. From eugenics to asylums, people with disabilities have been maltreated, sometimes with the participation of physicians and nurses who contributed to their marginalization and misery (Weiser, 2020).
To understand the legacy of disability and discrimination that preceded a call to humanize care for people with disabilities, we can start with Charles Darwin’s 1859 publication of The Origin of the Species by Means of Natural Selection. Darwin’s half-cousin, Francis Galton, applied some of those ideas to the social realm by exploring the inheritability of ability and the cultivation of “improvements” in the human race. The intention of eugenics, a term Galton coined, was ridding society of misfits and breeding a pure, advantaged race. The eugenics enterprise influenced Oliver Wendell Homes, a U.S. Supreme Court Justice to write in 1927: It is better for all the world, if instead of waiting to execute degenerate offspring for crime, or to let them starve for their imbecility, society can prevent those who are manifestly unfit from continuing their kind. Three generations of imbeciles are enough. (Solomon, 2019b, p. ix)
We may also recall that shortly thereafter Hitler’s campaigns of genocide began with gassing the disabled. And the sentiment to eliminate difference and disability continued. In 1968, ethicist Joseph Fletcher wrote in The Atlantic Monthly that there was no reason to feel guilty about putting a Down syndrome baby away, whether it’s “put away” in the sense of hidden in a sanatorium or in a more responsible lethal sense. It is sad, yes. Dreadful. But it carries no guilt. True guilt arises only from an offense against a person, and a Down’s is not a person. (Solomon, 2019b, p. x)
We have since seen a shift in public sentiment, such that it is no longer acceptable to call people with Down syndrome “Mongoloid idiots” (Catapano & Garland-Thomson, 2019) or “retarded.” More to the point, it is no longer acceptable to endorse the eradication of disabled people, with the exception of ongoing debates about prenatal testing for genetic difference as a form of population eugenics.
These changes over time in disability language and thought bring to mind the historical map leading from eugenics to pride across eras of understanding. Places such as Willowbrook represent a period of Institutionalization (approximately 1600–1900) (Jenks, 2019). Warehousing people with disabilities gave way to the Professional Movement (approximately 1850–1950) that introduced surgical and other interventions for people with intellectual and developmental disabilities reliant on medical classification and experimentation. The Parent Movement (approximately 1950–1980) addressed educational improvements through parent advocacy. The current era may be considered part of the Self-Determination Movement (1980-present) that coalesced in the passage of the historic Americans with Disability Act (ADA) (Wehmeyer, 2013). The addition of disability studies and crip theory in the modern era enriches our understanding of how impairment and barriers to self-determination limit the participation of people with disabilities in daily life.
Personhood in Practice Settings
One window into ongoing social change is the way we use referential language. People-first language is one way of recognizing that a human is first and foremost a person, and whatever impairment they may have does not diminish that personhood. Identity-first language, in contrast, offers a different perspective, one that acknowledges the manifold and edifying ways disability identity coheres. One is autistic rather than a person with autism, deaf rather than a person with deafness. Departing from an individual-centered viewpoint, identity-first language challenges the idea that we can remake discrimination by changing language to people first. Disability is part of identity and not separated from personhood.
Even as political action and disability pride has advanced social discourse, the practice settings of dentistry, medicine, and nursing have yet to catch up. For example, an internist in western Massachusetts was frustrated by the inaccessibility of specialist care for her patients. She would refer patients who used wheelchairs for specialty care, only to discover they had been turned away. To get to the bottom of the issue, she devised a “secret shopper” study to find out why (Iezzoni, 2016). She telephoned 256 medical specialty practices across 4 US cities. The fictional person needing the appointment was portrayed as a woman who used a wheelchair, was obese, with hemiparesis, and unable to transfer independently to an exam table or chair. Among the 256 practices queried, 22% said that they could not accommodate the patient, 4% said their building was inaccessible, and 18% reported they could not transfer the patient to a chair or exam table. Gynecology was the worst of the eight specialties, with an inaccessibility rate of 44% (Iezzoni, 2016). The refusal of 22% of practices to schedule the fictional patient violated the ADA. Most shocking was the blithe, matter-of-fact way office staff refused an appointment for a person with a disability. Dentistry may face similar challenges. The SCDA organization may want to devise a plan to establish a baseline accessibility measure for people with disability who are accessing basic and specialty dental care, and advocate for measurable progress.
Another example of dehumanization in health care played out this year with the coronavirus pandemic. Disability advocates and organizations raised concerns about triage and rationing of life-saving hospital beds and ventilators on the basis of disability (Disability Rights Education & Defense Fund, 2020). Lawsuits based on the ADA as well as the Affordable Care Act specified problematic responses to COVID-19 to include categorically excluding people with disability from access to scarce ICU beds or ventilators, implicitly considering people with disability to have lower quality of life in resource allocation assessments, or failing to reasonably accommodate people with disability in hospital settings. Just as a coalition of states was preparing a suit to end discrimination in health care allocation of COVID-19 resources, Twitter updated its hateful conduct policy. The policy was expanded on March 5 2020 to include a ban on language that dehumanizes people on the basis of their age, disability, or disease. Given the spread of the novel coronavirus SARS-CoV-2, hateful and sometimes racist tweets surfaced that devalued disabled lives. This ban applies to epithets and nonhuman comparisons. Examples of banned speech may include this Tweet: “People with a disability are subhuman and shouldn’t be seen in public,” or “COVID is culling weaklings from the herd, and that includes people with disabilities.” (Heasley, 2020).
The Why and How of Dehumanization
With these examples in mind, we may ask ourselves, why do people dehumanize others? According to Haslam and Stratemeyer (2016), there are likely four reasons. First is reciprocal dehumanization. When one group experiences their own dehumanization, a reciprocal response can be paraphrased as, “they dehumanize us, so they are not human.” A second reason is instrumental: People are a means to an end. Viewing people in this transactional way reduces concern or empathy for them, and dims our awareness of their capacity for experience and emotion. Third, stereotypes and epithets flatten representations. In this case, language shapes our figures of speech, and offers a shorthand communication that says “that’s how disgusting they are” by associating people with animals, machines, or referring to people as “subhuman” or undeserving of care and compassion. The final reason is burdensomeness. This is the reason most associated with the clinician/patient relationship. In this instance, people who dehumanize others in a helping relationship come to view interactions as emotionally exhausting. Clinicians resist feeling emotionally drained by people they consider burdensome and may resort to viewing those patients in dehumanizing ways to blunt their emotional exhaustion (Haslam & Stratemeyer, 2016). People then become things: “billables” or “visits” or “widgets.” To address this, we may be able to work with clinicians, and provide better institutional recognition, reimbursement, and resilience training and support. When clinicians feel more cared-for and supported, particularly when caring for challenging patients, they are less apt to dehumanize their patients (Zhang et al., 2015).
Even more to the point, why is clinician dehumanization of disabled patients an important issue? Part of the answer is that thinking of people as objects or lesser-beings has implications for the caring professions. First of all, dehumanization has been associated with increased social distance between providers and patients, more stigma, and objectification of people’s minds, bodies, and experience. According to a study by Sanson et al. (2020), patients who are made to feel like they are incapable of being understood and go unheard can feel reduced solely to a “body to be violated” (p. 7) resulting in a loss of dignity (Sanson et al., 2020). Dehumanization results in less empathy toward the patient experience, less willingness to help, and less compassion. From this equation, we can see that ascribing humanity to patients results in our more compassionate treatment toward them, our recognition of their dignity as human beings, and respect for their inherent worth. Solidarity and compassion may heal the healer, as well. In a study of mental health professionals, researchers found that ascribing humanity to mentally ill patients had an effect on the providers, too. The most humanistic providers felt a desire to address their own mental health issues, seeing something of their patients in themselves. In this case, “they” became “I” and both patient and provider were part of the circle of humanity (Martinez, 2014).
To sum up, we can agree with Joseph Conrad, who said: The history of intellectual and developmental disabilities (IDD) in the United States is, in many ways, a triumphant story reflecting an increasingly progressive attitude acknowledging the equality of all persons. The law now recognizes people with IDD as citizens, possessing an equal right to education, health care, and employment—each of which represent milestone victories. (Conrad, 2018)
Humanizing Dentistry
In reviewing our journey through disability history, we are now set to consider the third part of our purpose today. Together, we will explore paths to humanizing dental care by attending to the art and craft of dentistry. To do so we must consider the concept of humanizing care. Humanizing care is entering the lifeworld of the person before us, and listening with humility to their story. It is recognizing a patient’s unique experience of life and health, and supporting their personal sense-making journey toward an embodied, whole life. Forms of dehumanization were graphically clear from our review of the history of disability, with words and phrases like “objectification, passivity, homogenization, isolation, loss of meaning, loss of personal journey, dislocation, and reductionist body” (Todres et al., 2009, p.70). The forms of humanization are just the opposite: “insiderness, agency, uniqueness, togetherness, sense-making, personal journey, sense of place, and embodiment” (p. 70). These dualisms arise from the phenomenological tradition, primarily from Husserl’s notion of the lifeword and embodiment. Heidegger’s philosophical emphasis on human freedom and connection added social connection to humanizing the individual. Merleau Ponty’s ideas about the body subject and body object are also reflected in the humanzing care tradition (Todres et al., 2009).
Humanizing Through Listening and Learning
Humanizing care is the holistic view of human variation and ability and a response to the “vexing failures of medicine—with its relentless positivism, its damaging reductionism, its appeal to the sciences and not to the humanities in the academy, and its wholesale refusal to take into account the human dimensions of illness and healing” (Charon, 2006, p. 193). Skepticism about a reductionist model of disability permits reimagining “normal.” This pivots us toward a second consideration, that the awareness of social and structural environments link impairment with disablement. Third, we gain appreciation for the wellness continuum, regardless of disability, and the potential for people of all abilities to achieve high-level wellness. Fourth, providers assume a stance as empathetic and compassionate professionals available to patients and their families. Emotional competence is achieved by the recognition and comprehension that we all are human, which is at the core of compassion (Farr & Barker, 2017). There is real suffering in the world, and our patients with and without disabilities suffer and endure. Arthur Kleinman (2014) urged us as professional caregivers to step outside ourselves and look in as if an observer on our endeavors and our relationships—personal and professional—to acknowledge the strength, compassion, courage, and humanity with which we ourselves endure or help to make bearable the hard journeys of others. These are the qualities that make acceptance and striving, if not noble, then certainly deeply human—worthy of respect of ourselves and those whose journeys we share. (p. 120)
Fifth, cultural competence matters, given the intersectionality of disability with race, class, and culture. Last, we consider self-awareness about one’s own biases, with a liberal dose of humility as we come to learn how to better humanize care. Taken together, these aspects of humanizing bring together the medical and dental sciences with the humanities, and we are enriched because of that connection. Humanizing technical skills, or merging the art with the craft, connects us as healers to those who suffer and seek care. In its general outlines, our journey to humanize dental care for people with disabilities is the journey we make with every patient, to embrace their humanity and further their goals for oral health.
This idea of listening and learning as we travel toward a humanistic model of care is highlighted by the saying “Nothing About Us without Us.” That motto epitomizes the work of disability advocacy. It prevents the objectification of disability experience. Daniel Simpson wrote an essay about his life as a blind man (Simpson, 2019, p. 257) that was published in the book, About us: Essays from the disability series of the New York Times (Catapano & Garland-Thomson, 2019). One day, he was approached at a New York City intersection by a mother and her teenaged son. Surely, his white cane drew their attention. “My son is losing his sight,” the mother said. Then her son spoke with Daniel, asking questions and trying to learn more about what to expect as his sight faded away. Like most of us, Daniel was probably in a hurry and disinclined to engage in this conversation on the street as he was headed home. Even so, he patiently responded to the young man’s questions as graciously as he could. During their exchange, the young man’s mother started crying. By way of explanation, she offered, “When you have to go to a place, it’s nice to know someone who’s already been there.” (Simpson, 2019, p. 257). It felt a little melodramatic to Daniel Simpson at the time, but I find it profound. There are ambassadors with disabilities in dental practices who will tell us about their experiences, and help us as professionals begin to understand. That is the first part of the journey we take to humanize dental care: listening to people with disability about their experience, the places they have been, and the joys and challenges they have encountered. There is a level of trust afforded us by those with disabilities who share their unique stories, and we must be responsible in how we interpret and incorporate them into best practices in humanizing care (Rance et al., 2017).
Cultural humility is closely related, and extends from listening. One of the lessons we can learn from the disability history we just reviewed, and from American history and human history for that matter, is that people are seeking new lands, better opportunities, and fresh starts. In the lyrical words of scripture recorded in Hebrews 11, we “see the promises” of “a better country,” “afar off,” and in seeking that “heavenly country” we can acknowledge that we are “strangers and pilgrims on the earth” who are visiting, with humility, a new place. This can be seen with disability and humanizing care. We are strangers and pilgrims, and we approach new lands and new experiences with humility on the journey to humanize care. Our best cultural informants are the people who have been there before us, and live there.
My Experience With Humanizing Approaches
Let me offer a couple of examples of humanizing in dental care that come from my own experience. My son is a young man with an intellectual disability. Some years ago when he was a high school student, we scheduled removal of his wisdom teeth. Our family dentist sent us to a new dentist, who told us he could handle the procedure in his office. As the procedure began, I could hear screaming in the operatory from my uneasy perch in the waiting room. I surmised that the extraction was not going well. After one wisdom tooth was removed, the dentist returned my groggy, angry, and combative son to me in the waiting room. We had a conversation about what the next step would be. Throughout the next few weeks we worked on a new plan. I was in touch with this dentist and his staff, and appreciated the way he recognized my son’s uniqueness. “Don’t worry,” he said.
We know how to work with your son. We will take our cues from him as to what he needs. We’ll arrange the setting and the surgery so that he is as comfortable as possible. This doesn’t need to be traumatic,
he told us. I appreciated that, and now recall the dental care he received as a positive example of technically expert and humanized care.
The second example of humanized care features two UCLA dental students, Jonina Capino and Alyssa Rifalato. They are creating a web-based oral health education module using universal design principles. The website will promote oral health practices for people with intellectual and developmental disability. By casting actors with discernable intellectual disability as role models, the final product will offer resources by and for people with disabilities. From the Peanut Butter Falcon (Nilson & Schwartz, 2019) movie, to videos and apps like this, we are seeing—literally seeing—disability on center stage as part of the human experience. I am proud, as you are, of our students who are doing this work.
Now, with a firm understanding of the definition of humanizing care and the associated conceptual underpinnings and tenets, we can imagine the art and craft of humanizing dental care as fellow travelers. To do that, I worked with Cherisse Watts, a PhD student in nursing. Cherisse is exploring Black and Latinx families’ experiences with early childhood developmental screening and intervention. We sampled the last 10 years of publications in the SCDA professional journal, Special Care in Dentistry (SCD).
Method
From volume 30 (2010) to volume 39 (2019), we surveyed each of the six issues per year of Special Care in Dentistry, inclusive of editorials, case reports, reviews, and research articles. Articles were retained if they addressed children, youth, or adults with special health care needs, developmental disability, autism, intellectual disability and (optionally) their families, caregivers, and dentists. We noted dental issues or concerns associated with patients with special health care needs such as edentulation and caries, as well as cross-cutting issues such as cost, barriers to care, and accommodations in treatment. Articles were excluded if they addressed patients who were exclusively medically complex, at the end of life, undergoing cancer treatment, or receiving inpatient medical care. A total of 52 articles were identified for review. As a synthesis of published literature, this project was outside the scope of Institutional Review Board review for human subjects’ research protection.
Organizing Scholarship Into Typologies of Humanizing Dental Care
Following a holistic reading of each article, we identified aspects of dental care that elaborated on the conceptual dimensions of humanizing care. Our purpose was to explore the ways humanized dental care is practiced. We asked of each article, “In the process of providing dental care, how does the profession humanize care for people with developmental disabilities?” Each article was then coded holistically with the relevant aspects of humanizing care in a descriptive content analysis method (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005), connecting our purpose to the dimensions of humanizing care (Todres et al., 2009). Next, articles with similar content codes were clustered together into categories of humanizing with similar dimensions. We formulated typologies of humanized dental care, organizing the typologies from the most basic type of journey to the most advanced, and labeled the typologies Tourist, Traveler, Adventurer, and Scout (Table 1) to indicate differentiated and dynamic approaches to humanizing dental care.
Journey Typologies for Humanization of Care.
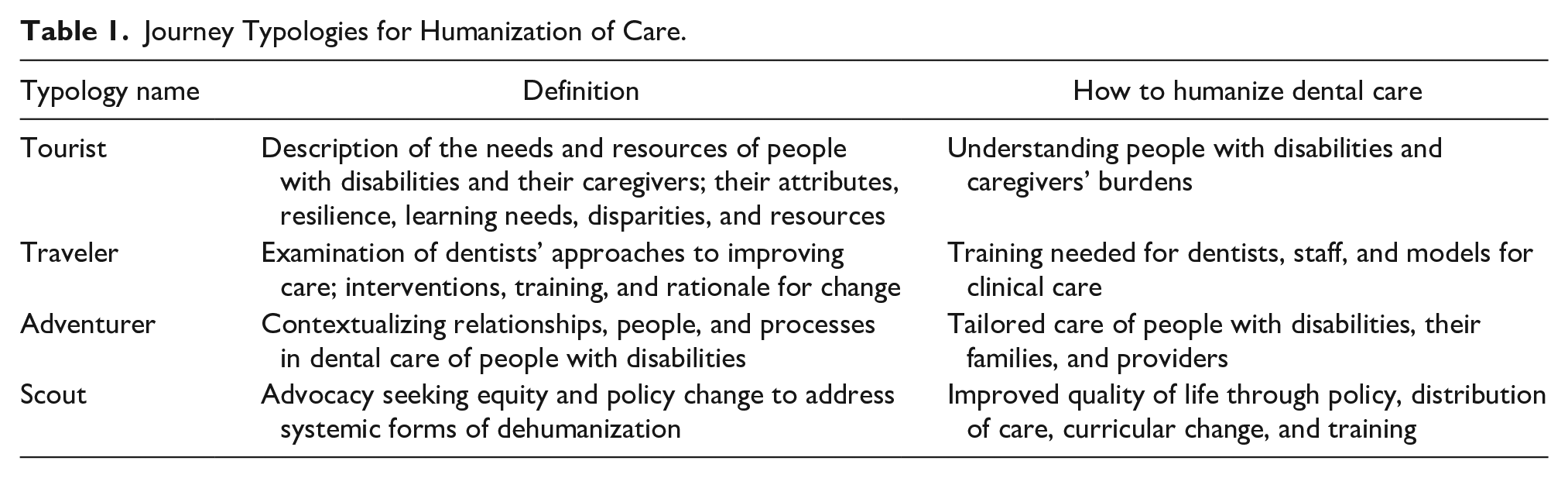
Tourist articles described the needs and resources of people with disabilities and their caregivers, including their attributes, resilience, and disparities. This humanized health care by increasing understanding of disabilities and caregivers’ burdens. Next, the typology of traveler included articles that examined dentists’ approaches to improving care, including interventions, training, and rationale for change. This humanized care by improving clinical care models. Adventurer articles contextualized the relationships, people, and processes of dental care of people with disabilities, and moved toward tailoring care. Finally, articles in the scout typology sought equity through advocacy and policy change to address systematic forms of dehumanization and improve quality of life through policy changes at the level of the health system or educational system.
Findings
Of the 52 articles we reviewed, most were tourist types, followed by adventurer, traveler, and scout (Figure 1).

SCD journal article typologies.
The content analysis process was set up to categorize articles by similarity in humanizing values and approaches, and consider the diversity among articles as we refined the definitional descriptors of each typology. After the initial categorization, we rechecked the classification based on the final and elaborated descriptors for each typology.
Tourist
The tourist is a curious traveler. Tourists spend time getting acquainted with new territory, learning the language, and looking at the new place. The results of studies in this typology offer a description of the needs and resources of people with disabilities and their caregivers. For example, Barros et al. (2019) described the quality of life and caregiver burden of parents of children and adolescents with disabilities in Brazil by studying 336 parents of children/youth with cerebral palsy, Down Syndrome, and autism spectrum disorder. Caregivers were most often mothers (90%) who lived in poverty, were religious, and were married. An assumption in some quality of life and disability research is that parenting a child with a disability is “caregiving,” and is different from mothering (Barros et al., 2019). Another assumption is that parenting a child with a disability affects quality of life and is a “burden” (Fine & Glendinning, 2005). One of the points the authors raised in the discussion was that caregivers of people with disabilities had worse quality of life (QoL) with increased caregiving burden. They proposed better education for mothers of children with disabilities and support for mothers’ oral health practices (Barros et al., 2019). A second exemplar of the tourist typology explored dental care experiences of adults with developmental disability using a focus group design. Provocatively entitled, “They stole her teeth” (Salmasi et al., 2015), the idea of tooth extraction (experienced as a theft) referred to a thematic finding of broken trust, inadequate informed consent, and poor communication between dentists and people with intellectual disability. The authors concluded that “One way for dental professionals to build skills in developing trust and enhancing communication would be to have more time devoted in dental school to treating individuals with special needs.” (Salmasi et al., 2015, p. 226). Descriptive studies in the tourist typology offered detailed facts about people with disability and their caregivers by closely examining their abilities, interests, burdens, and quality of life.
Traveler
The traveler typology focused on empathy, understanding stigma, and dental interventions to improve the quality of the patient care experience. Findings were about the dentist or dental practice. The following are two exemplar studies. The first is by Meurs et al. (2010) of the Netherlands. They explored whether more information about patients with intellectual disability translates into better cooperation during dental visits. Their team hypothesized that providing dentists with patient-specific disability information would improve patient cooperation during the dental exam. The patients were 57 people with intellectual disability, randomly assigned to a control condition (of limited information given to the dentist) and others to an experimental condition (more extensive information) prior to the oral exam. The hypothesis was not supported. Cooperation was not predicted by more preparation on the part of dentists. How interesting! How do we humanize care if learning about the human being before us does not improve their cooperation with the oral exam? The authors concluded that assuring that practicing dentists achieve a firm base of cumulative experience with patients with intellectual disability may be more important than preparing for each individual patient. Dentists with extensive experience and expertise were capable of picking up relevant nonverbal information early in the visit, and they modified their care on-the-spot to achieve a cooperative and mutually beneficial encounter (Meurs et al., 2010).
In another study, SCDA members’ attitudes and behavior toward patients with Autism Spectrum Disorder (ASD) were analyzed (Weil et al., 2011). The majority of dentists believed their dental team was knowledgeable and comfortable treating patients with ASD. The pattern of results showed that the more dentists liked to treat children with ASD, the more patients with ASD they treated (r = .313; p = .018). The more ASD patients they treated, the more accommodations they made to overcome problems with communication, social interactions, and aversion to change. The vast majority of dentists offered environmental and personal modifications for patients with ASD, including familiarization visits, special scheduling, special previsit instructions, and the option to have a parent in the operatory. They concluded that preparing dentists to care for patients with ASD may improve everyone’s experience: patients and dentists. They also noted that more effort is needed to build willingness to care for these underserved patients (Weil et al., 2011). Articles in this typology reinforced depth of experience as a precursor to humanized and mutually satisfying care for patients with disabilities and their dentists.
Adventurer
The adventurer seeks to understand the complexity of the individual experience, often through qualitative inquiry that evocatively renders embodied experience. Articles in this typology offered contextualized descriptions of tailored dental care. One group reviewed the literature about educational and therapeutic behavioral approaches to dental care for patients with ASD (Nelson et al., 2015). They considered how to improve quality of care by implementing specific practices suited to the needs of patients and caregivers. After reviewing a number of promising best practices, they emphasized several: preparation for the first office visit, strategies to increase success during the visit, and creative environmental changes that can increase comfort in the office environment. Taking time to understand children with ASD as individuals may prove most helpful, a recommendation aligned with humanizing care (Nelson et al., 2015). Assistive technology to aid in communication with patients and caregivers was suggested by the other exemplar article in this typology (Grewal et al., 2015).
Straying from the SCD articles for a moment, a compelling example of the adventurer typology produced by the New York University Dental School can be found in video format. The YouTube video highlights how to provide humanized care for patients with special care needs. Violette Kline, a young self-advocate, was hesitant, anxious, and fearful about receiving dental care. Yet “here [at this practice] I don’t feel as much anxiety,” she reported. “The people here are trained to figure out how to deal with kids with different needs and stuff” (NYUDentistry, 2019). From the moment she arrived in the waiting room, patients like Violette have multisensory experiences to help relieve their anxiety. Dental students learn how to talk with patients and personalize their care during their special care clinic rotation, setting a foundation of experience for a productive career in humanizing care for people with disabilities and other care needs.
Scout
The final typology scout, emphasizes advocacy, equity, and policy change to address systemic forms of dehumanization. To improve quality of life, exemplar articles fitting this typology address policy, distribution of care, curricular change, and training. An obvious barrier to oral health care, according to Williams et al. (2015), is finding a dentist willing to treat a complex patient with special care needs. Strikingly, 20% of the population of adults with special care needs do not have a dentist. This raises the policy-level problem of constrained access (Williams et al., 2015). The “insider” perspective of the patient came through in this article, as we realized how difficult it is for someone with a cognitive disability to locate a dentist. Another exemplar of this typology was a policy vignette posted by Jeffery Hicks in 2015 that called for designating patients with intellectual disability as a medically underserved population by the U.S. government (Hicks, 2015).
Discussion
Overall, what have we learned from reviewing a decade of articles in Special Care in Dentistry about humanizing dental care for people with disabilities? By organizing the scholarship produced by dentists into typologies of tourist, traveler, adventurer, and scout, we can more clearly appreciate the possibilities for humanized dental care. Across the typologies, dentists offer increasingly contextualized, individualized, storied, and embodied experiences with their patients. Dentists have creatively changed the physical environment of care to minimize aversive sensory experiences and considered ways to enrich their skills in providing humanized care for patients with disabilities. At the policy level, we see advocacy for better access to care, more educational pathways for dentists in the special care area, and more tailored resources for this patient population.
We also learned “how to” lessons from this body of scholarship. How to observe, listen, involve, practice, feel, persist, and trust. Merging the humanities and disability studies with dentistry, we see movement from the medical model that looks at disability as the problem. When disability diagnoses drive care, we foreground impairment. This is most evident in the tourist typology. The aim of dental care is to alleviate or mitigate the effects of the impairment on oral health and improve quality of life. Another group of publications could be aligned with a social model of disability. Problems faced by patients with disabilities stem from prejudice, stereotypes, and environments that are ill-fitted with a disabled person’s needs. Progress can be made in dental education, office layout, and reimbursement models.
A final group of articles could be considered more aligned with a humanized model of disability, where we redefine what is “normal” to include variation and different abilities. In this humanized model, dentists published about the spiritual dimension of dental care, cultural competence and empathetic, compassionate approaches at the intersection of the person and environment. There was also an awareness of biases held by dentists and in the health care structure that constrained humanistic practice. This is the kind of research and policy work we foresee as offering the most interesting journey. As we draw from the medical model along with the social model and reflect with humility on our practice, we can learn more from our patients and reshape our craft to better meet their needs. As Rosemarie Garland-Thomson (2011) reinterprets disability, a focus on the particularity of people and the relationships between people is needed. In dynamic encounters “between flesh and the world,” some bodies and minds do not fit with the ways social life is constructed and enacted in practice (p. 592). From mis-fitting to fitting, we give up explaining patients’ distinctiveness and attend to how we can best fit our care and our clinical spaces to the particularities of patients with disabilities. We are past the point of simply studying the outcomes of care, the dollars saved, or the esthetic improvements that result. It is time for us to turn our attention to humanizing the processes of care to provide goodness-of-fit for patients with disabilities.
How might we focus both on the technical challenge while still recognizing human dignity? We must protect against indignity by remembering patients’ humanness, that there is indeed a person living within the body (Hawley & Jensen, 2007). Humanizing care is a holistic, all-encompassing approach that takes all of this into consideration. First and foremost, the individual needs of the patient in front of us must be recognized and incorporated into their plan of care. Caregivers and family members often play a major role in decision-making about the plan of care. Continuing to build on relationships with caregivers and family members is crucial, especially when it comes to oral care at home and what it should entail. It is important to remember that they are truly care partners in a collaborative effort.
In the words of Andrew Solomon: Disabled lives are lives, and are charged with inherent dignity . . . Most people with disabilities contribute to the world they inhabit. Some have rich lives despite their disability, but others would say they have rich lives at least in part because of their disability. (Solomon, 2019a)
It is an honor to celebrate with you the progress being made to recognize human dignity in dentistry.
Footnotes
Acknowledgements
We thank Dr. Eric Sung, UCLA School of Dentistry, for sharing his experiences as a dentist for children and adults with intellectual and developmental disabilities.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The keynote address was sponsored by the Special Care Dentistry Association.