
Abstract
Previous research suggests that a range of factors influence an individual’s physical activity (PA) participation, but studies among Nepalese adults are limited. In this qualitative study, we aimed to explore the multilevel influences upon PA participation among community-dwelling adults aged 40 years and above living in an urban setting in Kathmandu, Nepal. Men (n = 21) and women (n = 30) were purposively sampled to participate in one of nine focus group discussions. Types of PA undertaken constituted activities related to housework, farm work, and active travel. Individual-level barriers included lack of knowledge, lack of motivation, perceptions of already being active, personal limitations, and lack of time. Interpersonal barriers included household responsibilities and lack of support. Broader environmental barriers included lack of infrastructure for active commuting, poor safety, rising use of motorized transport, lack of resting areas, weak social norms about PA, declining agricultural engagement, mechanization, and improved access to technology and facilities. Some differences were observed between the gender and disease groups. Health benefits, integration into domestic work, opportunities for social interaction, and social support were the facilitators. Interventions focusing on families, highlighting the short- and long-term benefits of PA, addressing gender roles, and ensuring women are better supported represent opportunities to promote PA. Community-based interventions will be essential to establish social norms around PA and improve social support.
Introduction
Physical activity (PA) refers to the bodily movement for occupational, household, transport, and leisure activities that results in energy expenditure and produces health benefits (World Health Organization [WHO], 2019). Physical inactivity is a significant public health concern causing a substantial health and economic burden worldwide (Pratt et al., 2020). Around one in four adults worldwide do not meet the WHO recommendation of at least 150 minutes of moderate PA or equivalent per week (WHO, 2019). The rising inactivity level will have implications for the future burden of chronic diseases, including type 2 diabetes, cardiovascular diseases, hypertension, obesity, and breast and colon cancers (Warburton & Bredin, 2016). Evidence also shows that inactive individuals have a higher risk of premature all-cause mortality compared with those who are active (Warburton & Bredin, 2016). Strong links between PA and positive mental health, functional independence, healthy aging, and quality of life have been well documented, providing further impetus to address inactivity (Guthold et al., 2018; Paterson & Warburton, 2010).
In Nepal, the prevalence of low PA (those not meeting the recommended 150 minutes per week of moderate PA or equivalent) among adults aged 15 to 69 years has more than doubled between 2013 and 2019, with an increase from 3.5% to 7.4% and a further sharper rise among women (Aryal et al., 2014; Dhimal et al., 2019; Nepal Health Research Council, 2019). In 2019, 6.6% of men and 8.2% of women had insufficient levels of PA (Dhimal et al., 2019). Furthermore, middle-aged adults (40–69 years) and those residing in urban municipalities were more likely to have low PA (Dhimal et al., 2019). Occupational and transport-related activities are the dominant PA forms among Nepalese adults, with minimal engagement in leisure-time PA (Aryal et al., 2014; Nepal Health Research Council, 2019).
A range of individual, interpersonal, and environmental factors interact to influence an individual’s engagement in PA (Bauman et al., 2012). Studies in diverse social and geographical contexts have reported factors such as cultural expectations, social responsibilities, awareness of the links between PA and health, neighborhood safety and aesthetics, built environment, and weather affect PA participation (Al-Hazzaa, 2018; Barnett et al., 2017; Medagama & Galgomuwa, 2018; Uddin et al., 2018). The extent of the impact of these factors might be different for males and females as some of the barriers, such as household responsibilities, disproportionately affect females (Koyanagi et al., 2018; Uddin et al., 2018). However, there has been little research to date concerning the major influences upon PA in Nepal. One quantitative study among people with type 2 diabetes found that factors such as family responsibilities, a busy schedule, and family discouragement act as deterrents to engagement in PA. In contrast, factors such as physical fitness, strength and flexibility, better sleep at night, social interaction, and longevity were identified as facilitators (Kadariya & Aro, 2018). Another study among mothers of young children in Nepal suggested lack of leisure time, family responsibilities, feeling lazy, absence of parks and playgrounds, and feeling embarrassed to be physically active in front of others were major barriers (Oli et al., 2018).
Multitiered interventions addressing age- and gender-related determinants of PA are recommended in low- and middle-income countries (LMICs; Koyanagi et al., 2018). Understanding the barriers and facilitators among different population segments is crucial for the effective design and implementation of strategies to promote the adoption and maintenance of PA. Furthermore, exploration of the influences upon PA for men and women provides an opportunity to understand the role of gender, and explore whether simultaneous interventions or gender-specific tailored interventions are required. However, studies providing this information among Nepalese adults are almost nonexistent. Given the increasing life expectancy in Nepal leading to the rise in the proportion of middle- and older aged adults in the population (Chalise, 2018), and the trend toward increasing physical inactivity among this age group (Aryal et al., 2014; Nepal Health Research Council, 2019), a focus on PA research and interventions among adults is critical. Hence, the objective of this study was to explore the perceived barriers and facilitators of PA participation, particularly occupational and transport-related PA, among Nepalese adults aged 40 years and above to inform PA policies and programs in this context.
Method
Study Design
This is a qualitative study conducted in three wards of Budhanilkantha Municipality, Kathmandu, Nepal. The use of qualitative methods was intended to provide an in-depth understanding of PA and its complex components, not always covered by quantitative methods (Pearce, 2009). Focus group discussions were used as the data collection method to obtain diverse participants’ perspectives and generate explanatory insights through group interactions (Kitzinger, 2005). The study site was purposively selected to understand the reasons for growing physical inactivity levels in urban Nepal. The municipality consists of 13 wards and is inhabited by approximately 153,000 individuals (Budhanilkantha Municipality, 2019). It is approximately 30-minute drive from the center of Kathmandu and approximately 15-minute drive from the Ring Road that encircles the core Kathmandu city. This municipality is rapidly urbanizing and has witnessed a decline in farming, as residential buildings are rapidly replacing the agricultural land. Hence, the location was considered appropriate to understand the PA patterns of urban residents, as well as to explore PA trends in an area transitioning from a rural to an urban environment.
The ethical review board of two institutions, Monash University Human Research Ethics Committee (Number 18575) and Nepal Health Research Council (Number 2803), approved the study.
Participants
Participants were adults aged 40 years or above and included those with or without cardiometabolic conditions (e.g., high cholesterol, diabetes, or hypertension). The age inclusion criterion (age ≥ 40 years) was selected due to the higher risk of chronic diseases and the declining levels of PA in this population. A purposive sample was recruited with the help of Mothers’ group, female community health volunteers, and local leaders (mostly men). The research team first explained the study purpose, methodology, and eligibility criteria for participant selection to these groups, and potential participants were individually contacted to gauge their interest in taking part. The research team then spoke with potential participants to explain the study purpose, assess their eligibility, and discuss the data collection process, time, and venue. Those currently living in institutions such as hospitals or aged care homes, unable to engage in PA on a routine basis, or unable to consent were excluded.
Data Collection
Nine focus group discussions were conducted between September and December 2019. Men (n = 21) and women (n = 30) participated in separate focus groups (four male groups and five female groups) and were from different families. The groups were also homogeneous in terms of their disease status. Of the nine groups, four groups comprised participants with chronic diseases. Each focus group consisted of five to six participants, lasted on average for 75 minutes, and were conducted in the Nepali language. A Nepali researcher (Susan Paudel) trained in qualitative health research methods moderated the focus groups. Because she was not currently living in Nepal, we assume limited inherent bias that might have affected data collection, analysis, and interpretation. A research assistant, who was a member of one of the included communities and had a tertiary-level qualification in health science, assisted with obtaining consent, recording, and taking notes. The location for these focus groups was decided based on convenience to the participants. Five of the nine focus groups were conducted in a home setting, whereas the remaining four were held in a Mothers’ group hall.
The focus groups were moderated using a semistructured discussion guide (see Supplemental File 1), which was developed based on a review of relevant literature and finalized through review by the research team. A member of the research team (Susan Paudel) then translated the guide to the Nepali language and other Nepali researchers (not related to this study) cross-checked the translated version. The ecological model of the determinants of PA (Bauman et al., 2012; Sallis et al., 2015), which recognizes a range of individual-, interpersonal-, environmental-, social-, and policy-level factors that may affect an individual’s PA participation, guided the discussion questions. The model highlights that factors operating at multiple levels interact to shape human behavior and multilevel interventions will be most useful to bring sustained behavior change (Sallis et al., 2015).
A pilot focus group was undertaken with a similar population group to ensure that the focus group discussion (FGD) guideline captured the required information and the participants were comfortable with the flow, questions, and language. The guideline was slightly modified (order of the items) based on the participants’ recommendations and the researcher’s experience. The main topics explored were PA practices, perceived benefits, and barriers and facilitators, as these relate to general, occupational, and transport-related PA. The participants with chronic disease were also asked to discuss changes in their PA behavior and perceptions after diagnosis. Probing questions were asked for clarification and to elicit further details until all conversation subsided.
Each focus group started with a brief description of the project purpose, study methodology, and risks and benefits of participation. Participants were provided with the opportunity to ask questions before the consent process. Written informed consent was obtained from all the participants, and the focus groups were audio-recorded with permission. After the consent process and before entering into the core FGD questions, participants were asked to provide their brief introduction including their full name, age, education, marital status, and main occupation. The participants were provided with a lunch pack at the end of each session.
When no new information emerged (data saturation), as determined by preliminary data analysis carried out concurrently with data collection, participant recruitment and data collection were stopped (Saunders et al., 2018).
Data Analysis
The focus group recordings were translated in their entirety (verbatim) into English and transcribed, and then analyzed using a reflexive thematic analysis approach (Braun & Clarke, 2019). The transcripts were uploaded into NVivo 12 plus (QSR International, Melbourne, Australia) for initial coding and code refinement. Using a deductive process (Braun & Clarke), one researcher did the initial coding after reading and rereading the transcripts to identify codes corresponding to the individual, interpersonal, and environmental influences upon PA (Bauman et al., 2012). In addition, an inductive process (Braun & Clarke, 2019) was used to scrutinize the transcripts for explanatory barriers and facilitators. Initial codes were then discussed within the research team to generate secondary codes and hence themes in line with the ecological model. The initial coder then recoded the manuscript, and the other two researchers cross-checked this final coding. Finally, the transcripts and the audio-recordings were revisited to ensure the themes reflected all the topics and explanatory comments reported by the participants.
Results
Participant Characteristics
There were 51 people (30 women and 21 men) who participated in the nine focus groups. The age of the participants ranged from 40 to 69 years, with a mean age of 52 ± 7.7 years. Most of the male participants were aged 40 to 49 years, with lower secondary or secondary-level education and were retired or unemployed. Among the female participants, most were aged 50 to 59 years, had attained no more than primary-level education, and were in unpaid employment (homemakers). Almost half of the participants (n = 24) were living with chronic diseases (diabetes, hypertension, or raised cholesterol). The demographic characteristics of the study participants are presented in Table S1 (Supplemental File 2).
Engagement in PA
Almost all the focus group participants appeared to be meeting the WHO recommendation of 150 minutes of moderate or more intense PA each week. Most of their current PAs were undertaken as part of essential activities of daily living, rather than PAs carried out explicitly for health benefits, for example, engagement in transport-related PA because of the lack of access to public or private vehicles. Household activities were the dominant form of PA for women. A female participant stated, “Most of us have similar routine . . . our activities revolve around the house and kitchen garden.” Men were relatively less involved in household activities, whereas they appeared to be more active outdoors. A male participant added, “Also, because since women are mostly at the house, their burden of household works is higher than us. We are usually mobile. If there is no work at home, we will be roaming around.” Mornings were most busy in terms of workload, followed by evenings. For stay-at-home participants, afternoons (postlunch) seemed to be slightly relaxed and offered some leisure-time opportunities.
Differences were apparent in PA participation between people living with chronic diseases and those who were relatively healthy. The participants with chronic disease were more aware of the health benefits of PA and tried to meet the recommended exercise prescriptions included in their disease management plan. A male participant suffering from hypertension stated, “When I went to the hospital for a check-up, the doctor suggested me to do some exercise. After diagnosis, I am rather compelled to exercise or go for walks. To keep my body healthy, I must walk now.” Most of those with chronic diseases reported being more active and having a more regular pattern of activity as a result of their diagnosis, mainly through morning walks and exercising at home in the mornings. A female participant with chronic disease commented, “Now since I have got the disease, I think household activities are not enough, and we need to engage in more. I was not as active before I was diagnosed with these chronic conditions.”
Barriers to PA Participation
Participants discussed barriers to participation in total, occupational, and transport-related PA at the individual, interpersonal, and environmental levels. Individual-level barriers included lack of knowledge, lack of motivation, perceptions of already being active, personal limitations, and lack of time. Interpersonal barriers included household responsibilities and lack of support. In contrast, environmental barriers included lack of infrastructure for active commuting, lack of safety, increased availability of motorized transport, lack of resting areas, absence of supportive social norms for PA, decreasing agricultural engagement, mechanization, and improved access to technology and facilities. However, some differences were observed between the gender and disease groups and are explained under each theme below. Table S2 summarizes the themes, subthemes, and relevant quotes related to the barriers of PA participation (see Supplemental File 3).
Individual-Level Barriers
Lack of knowledge
Although the majority of the study participants were aware of the importance of PA and its benefits, they reported that a lack of knowledge among the public could be one of the barriers. Some of the participants seemed to be skeptical about the role of PA in disease prevention as there were people in their community who were highly active but were later diagnosed with chronic diseases. A male participant shared, Walking has benefits, but we should not walk a lot as well. There was someone who used to walk everywhere but now has been diagnosed with chronic disease. This has made me think that excessive walking is also not good.
Lack of motivation
Lack of motivation, referred to by some as “laziness,” was another barrier to PA that participants reported. In some cases, lack of knowledge was linked to a lack of motivation, although some other participants reported they were not motivated even though they had been diagnosed with one or more chronic conditions and PA was a part of their disease management plan. The level of urgency to complete household chores was identified as a factor affecting motivation. A female participant shared, “If there is something that has to be done urgently, we do not feel lazy. We will finish it irrespective of the volume of work. Otherwise, we feel lazy and do not feel like working.”
Perceptions of already being active
It was apparent that considering oneself as already sufficiently active further affected PA participation in non-domestic forms of PA. Females more commonly reported this than males. Female participants stated that they engaged in multiple activities, mostly related to household chores or kitchen garden maintenance throughout the day, and were often exhausted. Although agricultural work was seasonal, those who had cattle at home reported that they hardly got any rest.
Lack of time
Both men and women reported a lack of time to engage in PA, particularly for active commuting. Men involved in formal employment often reported lack of time during the weekdays because of their fixed office hours and lengthy travel times. In contrast, women stated that their hectic household routine left them with little time to engage in PAs or walk to their destination.
Personal limitations
Limitations because of increasing age and lack of confidence were less commonly reported individual-level barriers. Some participants also indicated increasing age was also affecting their engagement in farm-based activities: “In the past, I could plough the field continuously for 3 hours and still not get tired. These days, I have to take 5 minutes break every 30 minutes.”
Interpersonal Barriers
Household responsibilities
Although the burden of household and farming-based activities was reported to have significantly reduced compared with the past, it still presented a significant workload for women and was perceived as a barrier to engage in non-domestic forms of PA. Women were mostly occupied with household chores such as cooking, cleaning, doing the laundry, kitchen gardening, and looking after the family. Even men agreed that household responsibilities presented a significant workload for women. Highlighting the traditional gender roles that assigned household responsibilities to women, one female participant shared, “Even though we believe men and women are equal and the household works should be equally distributed, we cannot ask the male members to clean the dishes when we are sitting idle.”
Conversely, men were relatively more engaged in farm-based activities. Usually, the labor-intensive activities were assigned to them: “Women’s works in the field are relatively less labour intensive than what men do such as men plough the field while women carry the load, sow the plants or do the harvesting.” However, the discrepancies in work distribution were reported to be slowly decreasing, particularly in the younger generations: “Relatively younger men help their mothers/wives in household works.”
Lack of social support
Both men and women reported a lack of support as a critical barrier. Men more often reported lacking peer support, whereas women reported a lack of support from both family and friends. Females further mentioned that the lack of support from family members in sharing their burden of household work hindered their engagement in other forms of PA.
Environmental Barriers
Lack of infrastructure for active commuting
Participants shared that unsealed roads that do not have a hard, smooth surface of tarmac or concrete were too dusty during dry weather, and muddy during the rainy season, although even sealed roads had many potholes. In Nepal, the fiscal year ends around monsoon, and during this time, many maintenance activities are initiated to ensure that the allocated budget is spent. These unfinished works lead to poor road conditions during the rainy season: “Road and drain works are often started in the rainy season further worsening the road conditions. It was so difficult in the last few days even to reach the nearest bus stop.” Some indicated that in the absence of dedicated walking trails and footpaths, they had to share the roads with vehicles, which raised safety concerns. Fear of theft and risk of vehicles in shared roads was reported to make it challenging to participate in transport-related PA. Furthermore, incidents of theft and other criminal activities deterred walking alone, particularly for females.
Increased access to motorized transport
Extension of road networks, increased access to public transport, and ownership of private vehicles (cars and motorcycles) were reported as barriers for engaging in transport-related PA. Participants shared that they walked if there was no vehicle route or till the nearest bus stop. A female participant questioned, “Who walks if we have a choice of catching public vehicle close to home? Using vehicle will save time; we will reach to the destination earlier.” The effect of increased ownership of private vehicles was more applicable to men. None of the female participants owned a car or motorbike. One participant indicated that easy financing options to purchase vehicles was leading to increased ownership: “. . . If we had to pay all the money upfront, not everyone could afford.”
Lack of resting areas and basic amenities
Lack of resting areas such as parks or seating arrangements at regular intervals made it challenging to walk a longer distance, particularly for the elderly and those with a chronic condition. Other participants indicated that the lack of necessary facilities such as drinking water and public toilets also hindered PA participation. Participants also reported that increased density of buildings, which has led to decreased open spaces, was hindering their PA participation.
Absence of a social norm
The absence of a supportive social norm regarding PA was commented upon, with cycling given as an example because it was rare among the target group. Some participants also indicated that the fear of being judged by community members influenced their participation in PA: If we are walking when there is an option to take a vehicle, then people will think we are trying to save the bus fare and will start gossiping. To prevent this, we are forced to take the vehicle even if we do not want to.
Participants also indicated that transport-related walking has decreased compared with the past and will further decrease in the future. A participant said, In the future, if vehicle ownership [private or public] further increases, there will be very few people walking, and then, it will not be as normal and as accepted as it is currently. Those who walk will be the odd one.
A few also mentioned that there is a lack of role models: “We rarely see people of our age cycling around here . . . People have diverted to motorcycles, cars and buses.”
Decreasing agricultural engagement
Almost all participants reported that agrarian land was declining and was being replaced by buildings, particularly in urban areas. They perceived it to be the most significant contributor to decreasing occupational and domestic PA. High investments to purchase plowing and harvesting machinery, but low financial return along with lack of laborers, had forced many to lease their land to others. Highlighting the lack of labor help, another participant added, “Those who previously used to work as field labourers are either on foreign employment or are engaged in other employments.” Some participants also reported that with increasing education, engagement in agriculture would further decline, as people will be employed in sedentary occupations.
Mechanization
Both men and women reported that mechanization of household and farm activities had significantly reduced their household and occupational PA, particularly in urban areas. Besides, mechanization of household activities such as the use of washing machines or vacuum cleaners reduced women’s PA. However, this was most relevant to families who were economically better off: “Those who can afford, hire a house help or buy a washing machine to wash clothes. Particularly, in families who are economically better off, they do not have to do any of these activities at all.”
Improved access to technology and facilities
Some participants commented that increased access to modern technologies such as mobile phones, the internet, and television were hindering their participation in PA and increasing sedentariness. Two female participants also shared that closer access to shops limited their transport-related walking: “I also think that having shops all around, like there is a shop in every next house, has also decreased our walking.”
Facilitators of PA Participation
During the focus groups, participants were asked to share the facilitating factors that boosted their PA participation. Most of the factors that participants referred to as “facilitators” related to the removal of barriers mentioned above. Besides these, a few factors were identified that enhanced participants’ engagement in PA such as health benefits, integration into domestic work, opportunities for social interaction, and social support, which are explained below. Table S3 summarizes the themes, subthemes, and relevant quotes related to the facilitators of PA participation (see Supplemental File 4).
Health benefits
Participants mentioned that the health benefits of being physically active motivated them. Those without a chronic condition seemed to be more attracted toward the immediate benefits of PA such as positive thinking, weight loss, and improved sleep and appetite rather than the long-term disease-prevention benefits.: “. . . if we are busy, we get tired, can sleep well and our appetite improves. We feel hungry, and even simple food tastes delicious.” For some of the female participants, PA was also essential to maintain their weight and prevent unhealthy snacking. A female participant stated, I am not sure whether we will be protected from disease, but it helps in lowering our body weight and decrease our shortness of breath . . . Now, since I have started walking regularly, I have lost some weight and can walk a longer distance.
Another female added, “On days, when I take a nap in the afternoons, I tend to eat a lot, sometimes even junk foods, after waking up.” However, those who had already been diagnosed with chronic diseases and were prescribed exercise as part of their disease management plan were more conscious about being active regularly to prevent their health from further deterioration.
Integration into domestic work
Some of the participants indicated that they wanted to do the household and fieldwork manually to be physically active. A female participant questioned, “If we stop doing the household chores as well, what else will be doing”? However, some other female participants were not happy with the quality of output from home appliances, especially from washing machines: “They [washing machines] do not wash clothes properly; clothes will still have stains and also are quite harsh on the clothes.”
Opportunities for social interaction
Several participants indicated that they were motivated to be physically active because it provided opportunities to meet friends and helped to stay updated about social issues. A male participant said, “Compared to staying at home, if we walk around we get updated about social issues and sometimes could get some business as well [such as selling/buying land].” Another female participant added that walking up to the nearby park provided PA opportunities for elderly who otherwise are isolated at home and could not engage in other PA forms because of their physical limitations.
Social support
Some females indicated that encouragement and moral support from family members motivated them to undertake PA. One participant shared, “My family members will be happy if I am going for a walk. Sometimes when I complain about a headache, they relate this to the lack of exercise.” Peer support was important for both males and females. Participants shared that if they were with some friends, they were more likely to walk to the destination and even prolong their walk. Some participants also indicated that walking in groups or with friends also minimized the risks while walking in poorly lit and quiet neighborhoods.
The study results are conceptualized in line with the ecological model and depicted in Figure 1.
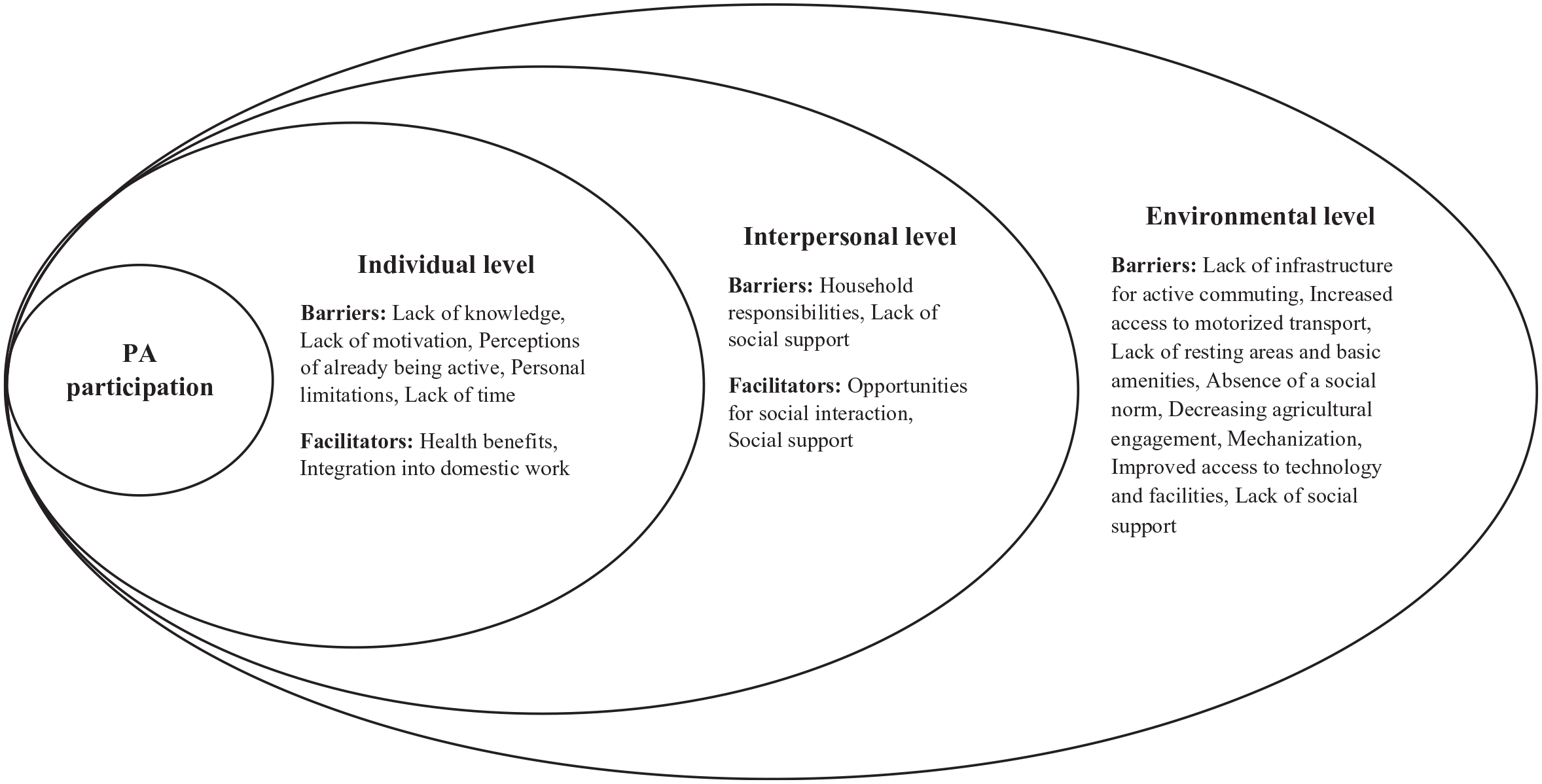
Conceptualization of barriers and facilitators of PA in Nepal “grounded” in the ecological model.
Discussion
In this study, we explored the multilevel influences on PA participation, including occupational and transport-related domains, among Nepalese adults. It adds to our understanding of the multiple individual, interpersonal, and broader environmental factors that interact to shape the PA behavior of adults in a low-income country undergoing demographic, socioeconomic, and epidemiological transitions. Furthermore, this study contributes to the scarce qualitative literature on barriers and facilitators of different domains of PA among nonimmigrant South Asians.
Most study participants reported being adequately active, although those with chronic diseases were more conscious about staying active. A Nepalese study has shown that almost half of the people with type 2 diabetes had only started PA after recommendation from their doctor upon diagnosis (Kadariya & Aro, 2018). A study from India has also found that those suffering from chronic diseases were more likely to be physically active than those who are not (Chandra & Nongkynrih, 2019). This appeared to be because PA was a part of their treatment and rehabilitation, and they were worried about an adverse prognosis caused by sedentariness. A previous systematic review of qualitative studies among migrant South Asians has indicated that primary prevention was often compromised as participants were less likely to visit a clinician unless they were sick (Horne & Tierney, 2012) and not everyone diagnosed with a chronic disease followed the doctor’s advice on PA (Little et al., 2017). Considering that lack of knowledge often limited PA participation, awareness raising using different mass media platforms will be vital; however, further research will be required to identify the most effective communication method.
Among participants, PA was mostly the result of routine activities or because there was no other alternative. Consistent with a previous Nepalese study (Kadariya & Aro, 2018; Paudel et al., 2020), women were primarily involved in household activities, whereas active commuting was the dominant form of PA for men. However, women with chronic diseases participated more frequently in other nondomestic forms of PA compared with those without these diseases.
Traditionally defined gender roles played a crucial part in shaping participants’ engagement in PA, particularly occupational PA. The burden of household and family responsibilities was a key barrier for women. They reported being exhausted with household chores, and either considered that they did not need to engage in other PA forms or were too short of time to undertake other PAs outside the home. Although younger men seemed to support female household members, older men were reluctant. This finding is consistent with previous studies from Nepal (Kadariya & Aro, 2018; Oli et al., 2018), South Asia (Medagama & Galgomuwa, 2018; Morrison et al., 2019), Saudi Arabia (Al-Hazzaa, 2018), and migrant Indians (Ramanathan & Crocker, 2009), which have reported gender norms, cultural expectations, and family responsibilities limited women’s PA participation. The patriarchal setting in many South Asian communities seldom allocates decision-making power to women (Herath, 2015). According to the 2016 Nepal Demographic and Health Survey (NDHS), around 42% of women do not participate in making decisions regarding their health care (Ministry of Health Nepal et al., 2017). This lack of decision-making power often leads to the distribution of non–income-generating activities such as household work to women, which reduces time to attend to their own well-being (Herath, 2015; Medagama & Galgomuwa, 2018; Patel et al., 2012). Furthermore, because South Asian women do not usually socialize outdoors during their youth, they find it harder to undertake outdoor PA during adulthood (Horne & Tierney, 2012). Nevertheless, women living with chronic conditions reported the need to engage in other forms of PA to get adequate health benefits.
Support from family members in sharing the household workload along with encouragement and moral support were instrumental in ensuring women initiate and sustain PA. Family support has been consistently reported as a facilitator for PA participation in multiple contexts (Mailey et al., 2014; Smith et al., 2017). A study by Ghimire (2017) has highlighted the crucial role of children and spouses in ensuring compliance to exercise among people with type 2 diabetes in Nepal. Another study among South Asian immigrants has emphasized the importance of sharing household responsibilities so that females get time for themselves (Rathanaswami et al., 2016), and our study supports this. Future interventions might consider involving family members and providing opportunities for being physically active with the family. A previous qualitative study has also shown that South Asians prefer family-based PA, and having a partner interested and participating in PA can act as a motivator (Gupta et al., 2017). This not only would enhance awareness about the importance of PA in the family but also could be valuable in addressing the traditional gender roles and ensuring women are well supported and feel safe.
The findings also suggest that participants were concerned about the decreasing trend of active commuting, and the probability of a further decline. They attributed this mainly to increased ownership of private vehicles such as cars and motorcycles, which mostly was independent of their economic status because of the availability of financing options. Motorcycles constitute 78.6% of total registered vehicles in Nepal, and the rate of motorcycle ownership has almost doubled between 2014 and 2018 (Ministry of Finance, 2019). It was primarily male participants in the study who owned these vehicles, and this finding is reflective of this age group across the country based on our observation. Men who were engaged in formal employment also reported that strict working hours and lengthy travel times made them exhausted, and there was no time for engaging in PA, in line with a previous study from Bangladesh (Mailey et al., 2014). Workplace PA interventions might be valuable to address decreasing PA and increasing sedentariness among those employed in desk-based roles.
Consistent with other LMICs (Nantulya & Reich, 2002), higher traffic congestion and poor road conditions increased road traffic accidents, making pedestrians more vulnerable. Lack of dedicated cycling or walking routes and inadequate streetlights further increased perceived risk and discouraged PA participation. Safety is a crucial factor that positively influences adults’ PA participation (Barnett et al., 2017). Our study findings are congruent with a previous review (Salvo et al., 2018) and a U.K.-based study among low-income families in an urban, deprived, multicultural community (Cronin-de-Chavez et al., 2019) that found that participants appreciated basic amenities such as resting areas, public restrooms, and drinking water facilities, and that these factors enabled PA. Older people and those with chronic diseases more frequently reported these barriers. In line with these studies (Cronin-de-Chavez et al., 2019; Salvo et al., 2018), our study also highlights the need for collaboration between health and other sectors such as planning, urban design, and transport to create built environments that support sustained PA.
Another barrier that was identified was the lack of support for PA at the community level, which was reflected in a social norm that PA outside of routine activities was uncommon and of low acceptability. Participants expressed concerns that they were likely to be the topic of gossip if they walked when there is the option of taking public or private vehicles. Consistent with our study, lack of social support has been reported as a barrier in studies from Saudi Arabia (Al-Hazzaa, 2018), Sri Lanka (Medagama & Galgomuwa, 2018), and Nepal (Ghimire, 2017; Kadariya & Aro, 2018). A qualitative study among people with diabetes in India has also found that participants were worried about being labeled “abnormal” when engaging in PA (Little et al., 2017). However, peer support was instrumental in promoting PA for both males and females, consistent with the studies among the Afro Caribbean populations (Alvarado et al., 2015) and South Asians (Horne & Tierney, 2012). Participants were more likely to commute actively and walk a longer distance if they were walking with friends. Another Nepalese study has shown that participants felt motivated and preferred going for a walk or engaging in other forms of PA with their peers (Kadariya & Aro, 2018). This highlights the importance of family, peer, and social support for promoting PA. Behavioral and social interventions such as buddy systems and walking groups may offer promise for social support (Heath et al., 2012). However, further research is needed to identify effective ways of generating these types of support among Nepalese adults. It should be noted that the telecommunication environment of Nepal has experienced rapid change in recent years. The COVID-19 pandemic may have also substantially changed how Nepali users of social media and internet-enabled devices access public health information, and the opportunities to obtain informational and other forms of support through these channels.
Almost all the participants mentioned that buildings had replaced agricultural land and open spaces, and national data show a decline in those involved in agriculture from 55% in 2011 to 51.5% in 2016. In the same period, engagement in professional/technical/managerial work has increased by 2% (Ministry of Health Nepal et al., 2017). Those who owned small pieces of land had either leased these to others or were adopting motorized agricultural equipment such as tractors. Not only farm work, but also household activities such as cleaning and washing clothes were becoming mechanized. Some of the women in this study considered that this eased their workload. In contrast, others preferred to do this work manually, either because they wanted to be physically active or were not happy with the quality of mechanized household work. This opportunity to integrate PA with domestic work provided a strong motive for participants, especially women, which has also been suggested in previous studies (Boutevillain et al., 2017).
PA participation differed across the seasons. Although females and those with cattle reported their workload remained constant throughout the year, farm work was seasonal. The study highlighted that walking was severely affected during the rainy season because of muddy conditions and potholes on the road. This was particularly relevant in the regions with unsealed roads. A Sri Lankan study (Medagama & Galgomuwa, 2018) has also reported that puddles, uneven roads and pavements, and being chased by unrestrained animals (e.g., stray dogs) limited PA participation. Another study from Bangladesh has reported that women feared falling over on muddy roads and uneven paths and the resultant embarrassment, which in turn discouraged PA participation (Morrison et al., 2019). This further reinforces the need for multisectoral collaboration in ensuring PA-friendly built environment.
Awareness and experience of the physical and mental health benefits of PA, as well as opportunities for social interaction, were given as motives for prioritizing PA, in line with previous studies from Nepal (Kadariya & Aro, 2018) and elsewhere (Cronin-de-Chavez et al., 2019; Horne & Tierney, 2012; Rathanaswami et al., 2016; Salvo et al., 2018; Wallace et al., 2016). Our study also highlighted that participants were more attracted to the shorter-term health impacts of PA, such as improved appetite and sleep and weight loss, rather than the longer-term gains, such as disease prevention. Getting better sleep at night, decreased fatigue, and increase mental alertness were found to be key motivators for being physically active in a previous study among people with type 2 diabetes from Nepal (Kadariya & Aro, 2018). Likewise, a qualitative study among Afro Caribbean women has also reported that the PA benefit of weight loss was more attractive than long-term health effects (Alvarado et al., 2015). This suggests that it might be necessary for future interventions to highlight both the short- and long-term benefits of PA participation.
Consistent with the ecological model (Bauman et al., 2012; Sallis et al., 2015), our study results indicated that PA behavior was shaped by the interaction within and between the determinants identified at the individual, interpersonal, and environmental levels. Among women, an example is an interaction between perceptions of already being active (individual level), household responsibilities (interpersonal level), and mechanization of household activities (environmental level). Interaction between these factors then hindered participation in PA. Furthermore, the elderly and those with chronic disease (personal limitations at individual level) were more likely to report lack of resting areas (environmental level) as a barrier. This reinforces that multisectoral and multitiered strategies are core to effective PA promotion.
Strengths and Limitations
The use of qualitative methods for data collection enabled exploration of the barriers and facilitators along with the local context of PA participation among Nepalese adults, not previously elicited by quantitative studies. Separate focus groups among male and female participants, further segregated by their disease status, provided an opportunity to understand the gender-specific factors and to explore changes in lifestyle following a disease diagnosis.
Notwithstanding these benefits, it should be recognized that participants were mostly from advantaged ethnic groups. Furthermore, we did not collect any information about the economic status of study participants, and PA perceptions relevant across different socioeconomic class might not have been captured. This study was carried out in a rapidly urbanizing area, and the findings must be interpreted considering that context. Because the participants were middle-aged adults living in urban areas, the study findings are not generalizable to other age groups and contexts. Further research is recommended to understand the PA patterns of younger age groups. The lack of interest, a schedule clash, or lack of time resulted in fewer male participants in the study. Participants did not have the opportunity to validate the themes as the focus groups were translated and analyzed in English. However, to confirm the common understanding of what was captured and understood, the researcher verbally summarized the key ideas to the participants after each focus group.
Conclusion
Applying an ecological framework, this study revealed how individual, interpersonal, and environmental factors are influencing PA participation among middle-aged adults in Nepal, who represent a high-risk group for chronic diseases. PA was found to primarily constitute routine household and transport-related activities, which were determined by the circumstances and the environment participants lived in. The study suggested the critical impacts that gender relations, economic development, technological change, the quality of the built environment, and community norms have upon PA in this context. PA promotion interventions focusing upon families and highlighting both the short- and long-term benefits represent an opportunity to facilitate the adoption and maintenance of behavior change and to ensure women are better supported. Community-based interventions will be essential to establish PA as a normative behavior. Beyond the level of the individual, engagement of policy makers responsible for infrastructure such as roads, urban design, and transport in design and implementation of structural interventions is vital.
Supplemental Material
sj-pdf-1-qhr-10.1177_1049732321993096 – Supplemental material for Exploration of Physical Activity Barriers and Facilitators Among Adults in Kathmandu, Nepal
Supplemental material, sj-pdf-1-qhr-10.1177_1049732321993096 for Exploration of Physical Activity Barriers and Facilitators Among Adults in Kathmandu, Nepal by Susan Paudel, Alice J. Owen and Ben J. Smith in Qualitative Health Research
Footnotes
Author Contributions
S.P. contributed to conceptualization, methodology, formal analysis, and writing original draft; A.J.O. contributed to validation, supervision, and writing—review and editing; and B.J.S. contributed to methodology, validation, supervision, and writing—review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.