
Abstract
Mobile health (mHealth) interventions are increasingly used to support community health workers (CHWs) in low-and middle-income countries. As near-peers within their communities, the credibility of CHWs is sometimes questioned—a recognized barrier to their efficacy. Nested within a large, randomized-controlled trial, this qualitative study captured the experiences of South African CHWs, called “Mentor-Mothers,” using tablets and animated videos to promote exclusive breastfeeding. We conducted in-depth telephone interviews with 26 tablet-carrying Mentor-Mothers. We analyzed interview transcripts using a Grounded Theory approach, then developed a theoretical framework, based on an emerging theme, for understanding how tablet technology boosts the perceived credibility of CHWs. Tablet-carrying Mentor-Mothers described an increase in their perceived credibility, which they attributed to overt and signaling effects related to enhanced credibility of (1) their messages, (2) themselves as messengers, and (3) the program employing them. Mobile technology investments in CHWs could enhance their credibility, translating into meaningful investments in the health of under-served communities.
Keywords
Introduction
Health delivery systems increasingly integrate mobile health (mHealth) interventions to support the work of community health workers (CHWs) in low-and middle-income countries.(Braun et al., 2013; Early et al., 2019; Ward et al., 2020) Much of the existing research has examined maternal child health interventions delivered through short messaging services (i.e., text messages) on feature phones. Fewer studies have explored the experiences of CHWs implementing interventions delivered via smartphone or tablet technology—capable of showing video content—in under-resourced communities.(Early et al., 2019; Mogoba et al., 2019; Smit et al., 2021; Yepes et al., 2016)
In these settings, CHWs bridge a critical gap between health systems and hard-to-reach communities who have limited access to formal healthcare. By counseling mothers on key preventive health behaviors, the CHW mentoring model has demonstrated significant benefits for maternal and child health in high-adversity settings.(Early et al., 2019; Gilmore & McAuliffe, 2013; Ward et al., 2020) Near-peer mentoring between individuals who face similar challenges and speak the same language—both literally and figuratively—allows CHWs to support important health behaviors like exclusive breastfeeding and safe infant feeding practices.(Nieuwoudt et al., 2019; Nor et al., 2012; Victora et al., 2016)
Despite their documented potential, significant barriers also impede the work of CHWs in under-resourced settings. Among these is a lack of perceived credibility within their communities.(Early et al., 2019; Kane et al., 2010; Mhlongo & Lutge, 2019; Rachlis et al., 2016) While they are uniquely qualified to reach and counsel their clients, the near-peer status of CHWs sometimes draws skepticism from clients who question their skills, training and legitimacy as members of the healthcare workforce.(Austin-Evelyn et al., 2017; Early et al., 2019; Rachlis et al., 2016)
In the education literature, credibility results when an authority figure demonstrates the skills and knowledge needed to achieve specific educational goals.(Pace & Hemmings, 2007) Similarly, CHWs engaged in community health promotion have expressed a need for the necessary equipment (i.e., scales and blood-pressure cuffs) to both perform important health-related tasks, but also to demonstrate the skills and knowledge that signal their legitimate affiliation with the healthcare system. More formal signifiers of their status, such as uniforms and badges, are also valued and desired by CHWs.(Austin-Evelyn et al., 2017)
While the impact of mHealth interventions on CHW credibility has not been well documented, these interventions have proven to be both acceptable to CHWs and, to some extent, effective in supporting behavior change, especially when they are aimed at improving the CHW-beneficiary interaction by facilitating communication. These interventions have been delivered using a variety of approaches, including CHWs showing videos or playing audio segments to clients before discussing the health messages through face-to-face counseling. (Coetzee et al., 2018; Gopalakrishnan et al., 2020; Ward et al., 2020)
Similar to the intervention used in our study, a qualitative study conducted in two Indian states (Bihar and Madhya Pradesh) explored an mHealth intervention integrating data collection and video health messages. Findings from that study suggested that the intervention was acceptable to CHWs, who reported a perceived increase in status, which they attributed to the new technology.(Gopalakrishnan et al., 2020) While encouraging data emerges on the use of mHealth interventions delivered via smart phones, researchers emphasize the need for more robust evidence demonstrating their impact on health-related interactions between CHWs and their clients.(Gopalakrishnan et al., 2020) Research exploring the effect of such interventions on CHWs’ credibility and status within their communities is urgently needed to drive technology access and policy recommendations supporting this critical cadre of the healthcare workforce.
The Philani Maternal Child Health and Nutrition Trust (Philani), operating in and around Khayelitsha, South Africa, implements a longstanding, nationally recognized CHW program.(le Roux et al., 2013; le Roux et al., 2015; Tomlinson et al., 2016) Philani’s CHWs, called “Mentor-Mothers,” conduct home visits with mothers and pregnant women living in their neighborhoods. Prior research at Philani (Coetzee et al., 2018) and in other under-resourced settings supports the feasibility and acceptability of equipping CHWs with tablet-based interventions to augment their health promotion efforts.(Gurley et al. (n.d.); Kumar et al., 2015; Vashistha et al., 2016) While mHealth technologies have shown promise, researchers have heavily underscored the need for additional research exploring their implementation at the community level.(Aranda-Jan et al., 2014; Kallander et al., 2013; Lee et al., 2016; Sondaal et al., 2016)
This qualitative study was nested in a large, cluster randomized-controlled trial of a mobile breastfeeding intervention.(Adam et al., 2021) Using a grounded theory approach, and by triangulating qualitative data with quantitative data gathered through the parent trial, we explore how mobile tablets and an animated video breastfeeding intervention shaped the experiences of Mentor-Mothers working in a high-adversity setting in South Africa. The perspectives of CHWs adopting tablet technology, are a critical addition to a sparse but increasingly relevant body of research on the acceptability, accessibility, and usability of smartphone and tablet-based, mHealth interventions.
Materials and Methods
Study Setting and Parent Trial Description
We conducted the Philani MOVIE study (Adam et al., 2019) in the informal settlements of the Western Cape Province, South Africa, between November 2018 and March 2020. The parent trial involved 1504 pregnant mothers living in the region and enrolled in the Philani Mentor-Mother Outreach Program.(Adam et al., 2019) This region is characterized by high infant mortality and crime rates compared with national data, as well as a relatively low prevalence of exclusive breastfeeding and poor maternal and child health indicators. (Figure 1)
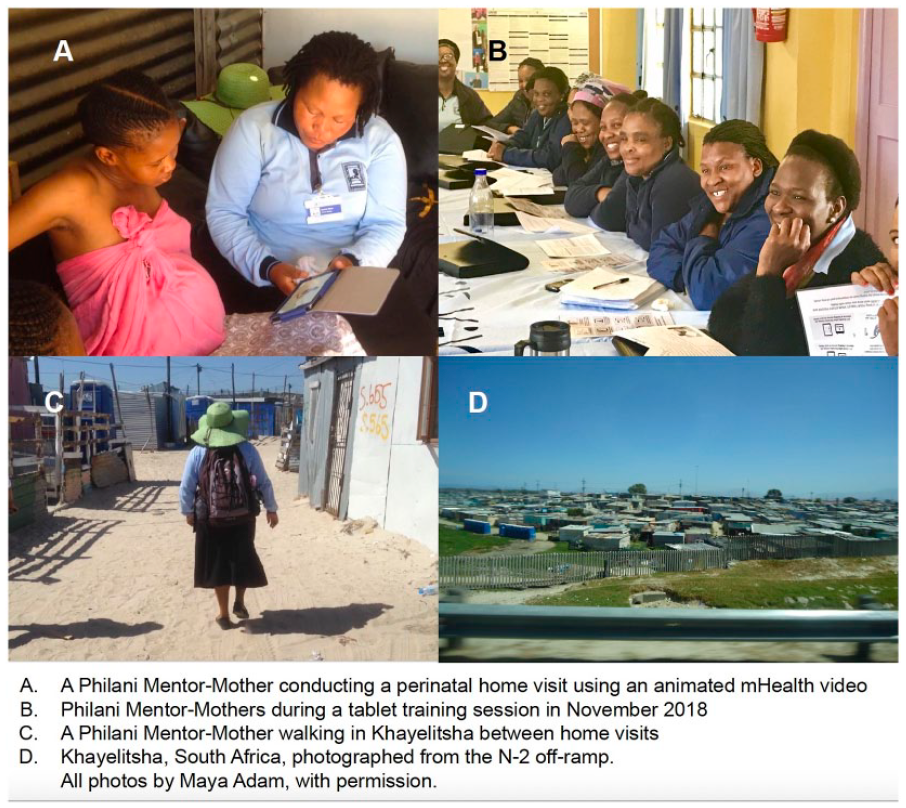
Philani Mentor-Mothers at work in Khayelitsha, South Africa.
Philani Mentor-Mothers are nominated by local community leaders because they have managed to raise thriving children in a high-adversity setting. Generally between the ages of 30 and 55, Philani Mentor-Mothers have typically completed grade 10 (where grade 12 completion is the end of high school) as their highest level of schooling. They receive 9 weeks of initial training, followed by ongoing supervision through Philani’s Mentor-Mother Supervisor program. After completing their training, they are assigned to a neighborhood based on residential proximity and paid a modest stipend for their work—typically 4 days per week. (le Roux et al., 2010)
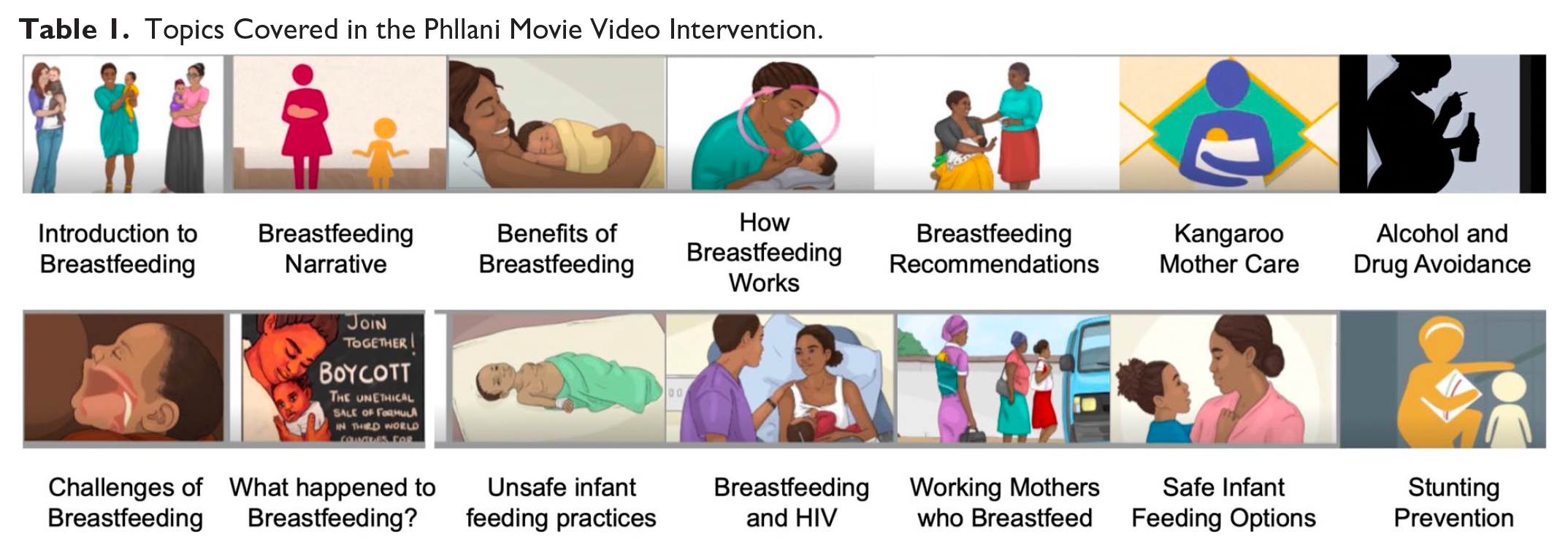
All Philani Mentor-Mothers participating in the Philani MOVIE study were given tablets to use in their home visits. Mentor-Mothers assigned to the intervention group (tablet + video), delivered animated health videos and collected infant feeding data on their tablets, while Mentor-Mothers in the control group (tablet only) used their tablets exclusively for collecting infant feeding data. Table 1 summarizes the topics presented in the Philani MOVIE Video Intervention.
Topics Covered in the Phllani Movie Video Intervention.

Main Findings of the Parent Trial
Quantitative outcomes of the parent trial (Adam et al., 2021) included: a small, but statistically significant improvement in maternal knowledge in the intervention arm at 1 month post-birth; no statistically significant differences with regard to breastfeeding rates or other infant feeding practices; similar time spent with clients across trial arms, but the intervention group substituted approximately 40% of their face-to-face counseling with video viewing and routinely used that time to perform other health-related tasks. Finally, overall video usage was high, with 84 Mentor-Mothers showing the videos 6435 times during the course of the study, according to tracking data from the tablets. The intervention group spent an estimated 20.72 minutes per visit while the control group spent an estimated 21.03 minutes with each client. These mean time estimates did not differ significantly between the two groups. Self-report data from both groups on video usage during home visits were integrated with tablet data to estimate the mean percentage of time spent watching videos. Intervention Mentor-Mothers reported spending an average of 39.7% of visit time showing videos while Mentor-Mothers in the control group spent an average of 1.9% of time showing videos due to a small amount of contamination of the control group. These data are shown in Figure 2.
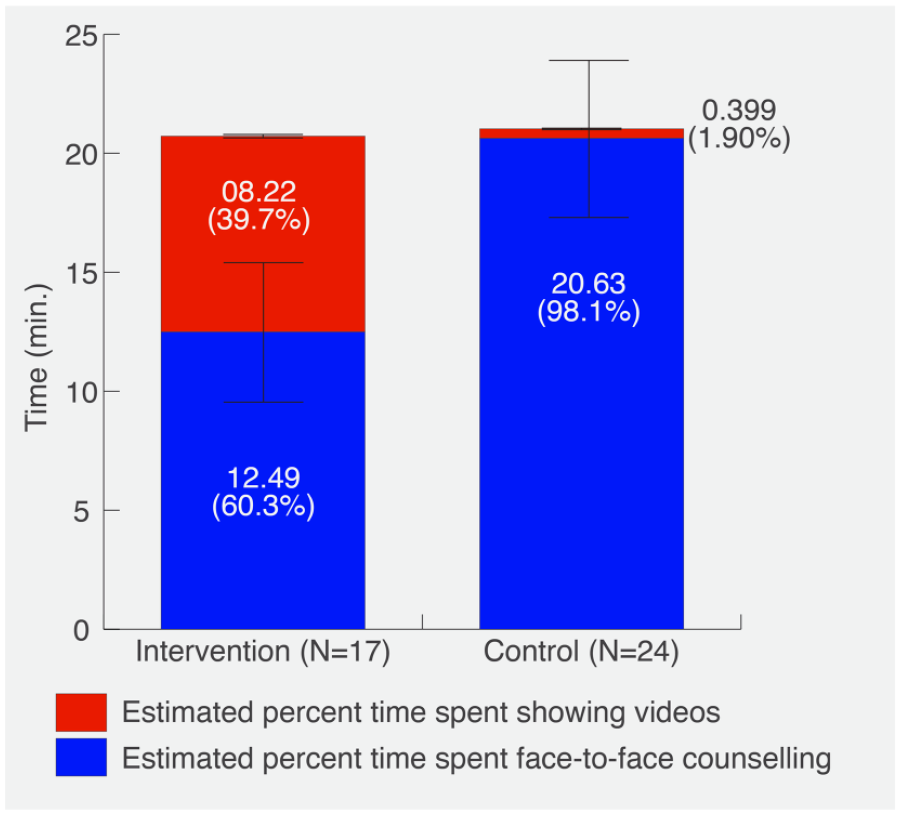
Estimated percent time spent showing intervention videos versus face-to-face counseling in the last home visit for intervention and control groups.
Qualitative Data collection
At the end of the study, we conducted qualitative, in-depth telephone interviews (IDIs) with 26 Mentor-Mothers who had used tablets during their home visits in the preceding year. We explored Mentor-Mothers’ typical daily work experiences, preconceptions about using the tablets prior to the start of the study and actual experiences integrating this new technology into their home visits.
While we had originally planned to conduct in-person, end-line focus group discussions, COVID-19-related restrictions on face-to-face data collection prohibited this. Out of necessity, we pivoted our approach, gathering data from June-August 2020 through telephone IDIs only. Participating Mentor-Mothers were selected using maximum variation purposive sampling, seeking to draw the broadest possible range of heterogeneous Mentor-Mother perspectives across age, experience and neighborhood types served.(Patton, 1990) IDIs were terminated when saturation and redundancy were reached.(Bowen, 2008; Patton, 1990; Tuckett, 2004)
Interviews were conducted in isiXhosa, after obtaining informed consent, by our co-investigator (NJ). All IDIs were then translated into English and transcribed by two co-investigators (NJ and BM) who checked each other’s translations to ensure that the core meanings of the interview texts were preserved. Weekly debriefings, involving the qualitative research team, served to support and enhance the performance of the interviewer as well as resulting in early identification of emerging themes.(McMahon & Winch, 2018) All co-investigators were trained in qualitative methods.
Data Analysis
After completing the IDIs, NJ, KK, and MA conducted a series of debriefings during which we developed and refined a template for thematic analysis.(McMahon & Winch, 2018) Aligned with a Grounded Theory approach, we began our analysis by reviewing the debriefing notes and interview transcripts.(Charmaz & Belgrave, 2012) We then selected a sample of diverse and representative transcripts for the initial phase of open, inductive coding using NVivo.(Bazeley & Jackson, 2013) We developed several categories and sub-categories, which we then modified based on themes that we observed to be emerging during the data analysis. In response to emerging themes, we began to develop a set of theoretical notions, which we tested in the context of additional debriefings as a research team, revisiting transcripts and earlier debriefing notes regularly. In this way, we developed a set of core themes, aligned with prior research on qualitative interviewing using a Grounded Theory framework.(Charmaz & Belgrave, 2012) These themes were used to construct a theory that provides insight into an unexpectedly prominent finding: the gains in perceived credibility reported by the Mentor-Mothers and attributed directly to the use of this tablet technology in their home visits.
Results
Implementation Experiences
Overall, Mentor-Mothers in the intervention group described a consistently positive experience integrating the Philani MOVIE videos into their work, with no major barriers. Philani’s policy was to replace tablets that were damaged or stolen as this was an area of initial concern raised frequently by the Mentor-Mothers during their training sessions. Post-implementation, Mentor-Mothers reported carrying their tablets to their home visits on most days, although they sometimes had to gauge whether it was safe enough to reveal the devices in certain settings: “I would first assess the household situation, for example if it was only women. If there is a person, I don’t trust I would not take out all my resources.” [Mentor-Mother #4] “It wasn’t safe sometimes, but I carried it every day and I’d make sure I don’t take it out until I’m indoors.” [Mentor-Mother #12] “No, I didn’t feel safe, but I was careful, I looked around. I know the area I worked in, so I knew in which places I could take out my tablet and places where I couldn’t.” [Mentor-Mother #5]
Generally, Mentor-Mothers found the intervention better suited for use in the pre-natal rather than the post-natal period. Pregnancy was reported as an opportune time to engage women in discussion and potentially influence their feeding decisions, mostly because they had more time to view the videos. New mothers had limited time for visits with Mentor-Mothers, often due to the additional chores associated with caring for a new child and returning to work.
Intervention Delivery Patterns
Some Mentor-Mothers watched the videos with their clients during home visits, while others preferred handing the device to the client while they completed paperwork: “I would tell them they are going to watch a video about the importance of breastfeeding, give them to watch and encourage them to ask questions, if she has questions while watching I’d pause the video and clarify for them. Once they are done watching I ask if there is something they need explanation of.” [Mentor-Mother #12] “So as they are listening you are able to use the time to write the things you have talked about, ‘. . . and by the time you finish writing . . . they are done watching . . . I then ask them what they have learnt and what they found beneficial . . .” [Mentor-Mother #4]
Clients were shown videos at each visit (bi-weekly until the 36th week of pregnancy, then weekly until 1 month post-partum). Mentor-Mothers made exceptions when they felt it was unsafe to use the device or the client was experiencing extenuating circumstances that did not allow for a normal visit (e.g., social issues or other constraints that precluded routine counseling).
While Mentor-Mothers were encouraged during tablet training sessions to show all intervention videos at least once to each client, they selected specific videos for each visit based on their clients’ needs and circumstances. This level of autonomy in tailoring health promotion messages to the needs of the client is part of the Philani care model: “You can tell what a household is like right? You notice that this woman is refusing to breastfeed, do you understand? Or you notice that the house has a lot of bottles, alcohol is loved, such things, do you understand? You then show them the video of people drinking, to let them see the dangers. So, you don’t just play any video, you first observe the situation in that household.” [Mentor-Mother #18]
Videos focusing on the benefits of breastfeeding, breastfeeding for HIV positive mothers, unsafe feeding practices and alcohol avoidance were among the most frequently used. Mentor-Mothers listed these topics as key areas of concern, but also expressed a desire for additional videos addressing other priority health topics, e.g. umbilical cord care and tuberculosis prevention, among others. Mentor-Mothers also suggested several topics relating to social and mental health issues, including child-centered parenting, preventing and addressing domestic violence in the home and the psychosocial impact of alcohol abuse.
Mentor-Mothers also described using the videos to support their own continuing education and ensuring consistency of the health messages delivered to their clients: “For me the video was really helpful because I realized my knowledge, when I educated using those videos . . . they opened up my mind. We learnt some new points.” [Mentor-Mother #21] “Even when I’m done, I might have left other things out which the mother would then learn from the videos . . . so, they have been very helpful, even to me as a mentor mother I have learned.” [Mentor-Mother #12]
Overt Versus Signaling Effects
The tablets and video intervention had both overt and signaling effects, some negative and some positive, on the Mentor-Mothers’ preconceptions and implementation experiences as they transitioned to using tablet technology.
Mentor-Mothers described, at length, their feelings of being overwhelmed, especially when unanticipated social issues would arise: “If there is any abuse or the client is stressed, and you want to find the root cause, that session can take up to an hour or 2 hours, until the mother stabilizes. You don’t leave the mother worried . . . It can also be difficult for us to help our clients cope with all these things that happen in our communities.” [Mentor-Mother #81]
While they appreciated the need for innovative educational materials, this was overshadowed by a general feeling of insecurity about learning and integrating new technology, despite the availability of remote technical support to help Mentor-Mothers troubleshoot problems they experienced in the field: “It seemed like it was going to be hard to use tablets, as if we were going to do something unfamiliar but when I got to the field I realized that what I thought was going to be hard, it’s something I am always doing only that there was an additional tool.” [Mentor-Mother #18]
Mentor-Mothers also described the longstanding challenge of securing and maintaining their clients’ attention for the duration of the visit: “When we first used tablets I got a bit worried because we already knew our clients so I thought it would be difficult because most of them get irritated during visits and having to now ask them to take time and sit down because you want to show them something, I was a bit worried about that.” [Mentor-Mother #4]
Personal safety was the final concern described by Mentor-Mothers as they described their early fears that the tablets would leave them vulnerable to theft.
“I was excited but also worried given that our communities are cruel . . . I might go to a household for a visit and find that one of the children is a thief and then they follow you after the visit or tell others that you have a tablet, but that never happened.” [Mentor-Mother #9]
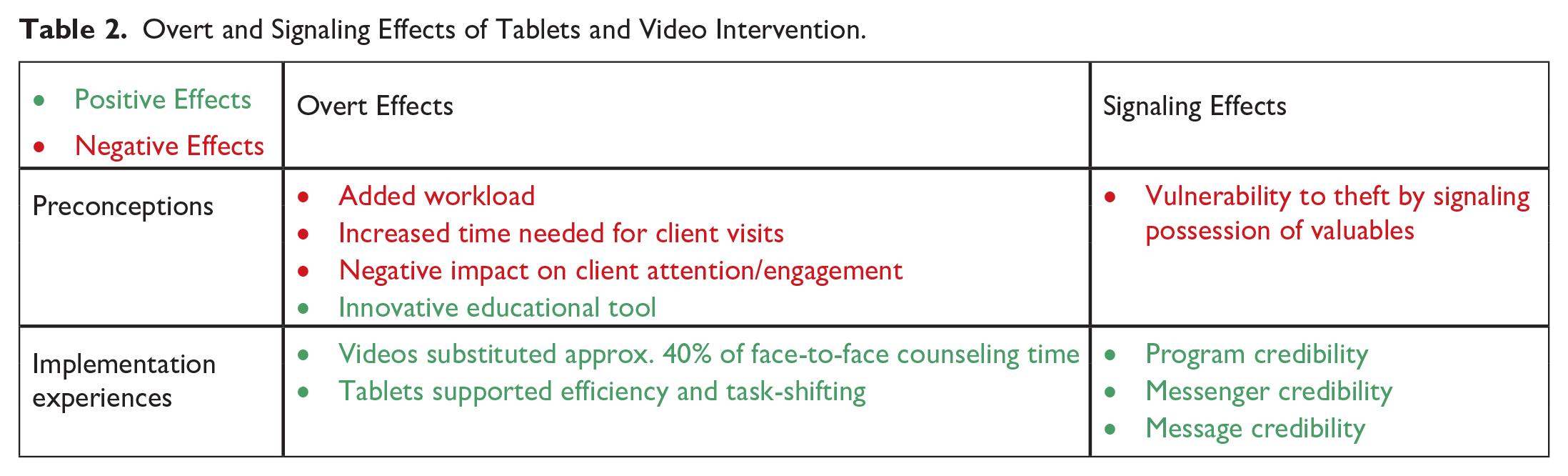
Early concerns about overt effects, like added workload, increased demands on their time and potential negative impacts on client engagement, were counterbalanced by early excitement about using an innovative educational tool. During implementation, Mentor-Mothers described a freeing up of their time and, as a result, a capacity-generating effect of the tablets, relative to their pre-implementation practices. Concerns about the tablets identifying them as targets for theft and violent crime did not materialize and Mentor-Mothers developed behavioral practices that they felt supported their personal safety. The signaling effects relating to perceived credibility resulted in Mentor-Mothers describing a generally very positive experience of implementing this innovation. Table 2 summarizes the overt and signaling effects described by Mentor-Mothers using tablets and the video intervention.
Overt and Signaling Effects of Tablets and Video Intervention.
Promoting Mentor-Mother Credibility
Mentor-Mothers described a perceived lack of credibility within their communities as a barrier to their work. As members of the communities they serve, Mentor-Mothers said their knowledge, skills and program credibility are frequently questioned by their clients. In this regard, Mentor-Mothers underscored the important role of videos and tablets in signaling their credibility: “There is stigma to be undermined in the township as if we don’t know what we are talking about. Amavidiyo . . . anike umsebenzi wethu isidima: The videos gave weight to our work.” [Mentor-Mother #12] “ikhulisa umsebenzi wethu - [The tablets] elevate our work. Because you’d find that we were undermined, like we are illiterate, so [with tablets] we looked like we had done computer studies.” [Mentor-Mother #3]
When outlining the manner in which credibility was bolstered, Mentor-Mothers consistently raised topics that centered around three key themes: (a) message credibility, (b) messenger credibility, and (c) program credibility. In terms of message credibility, Mentor-Mothers highlighted that because the videos echoed their health messages and promote client engagement, Mentor-Mothers felt that their words and education efforts were elevated: “Mothers believe what they see, they don’t believe what they hear . . . so knowing that I could show them videos I knew my work would be made easier because I’d be talking about something they can see as well.” [Mentor-Mother #5] “It had a beautiful effect on my job, like when you educate and see the content in the videos, you know you are talking about something they can see in the videos, which adds weight.” [Mentor-Mother #12]
Regarding messenger credibility, Mentor-Mothers described gains in their perceived status resulting from the technology savviness they were able to demonstrate by knowing how to use their tablets during home visits. They felt these gains were manifested in greater client engagement while they were operating the tablets.
“It’s like I have a laptop, meaning it upgraded my job, so much that my clients know that now with the laptop I am the same as those working in offices.” [Mentor-Mother #13] “When you switched on the videos you would notice that even the one washing the dishes would be interested, you know that the screen is big and bright and showed everything clearly . . . Before you know it they would have gotten a chair to join . . . They are surrounding you . . . they want to watch, very interested.” [Mentor-Mother #18]
Finally, in terms of program credibility, Mentor-Mothers described how having a technological tool—one that holds value within their communities—not only allowed them to demonstrate their own training and skills, but also gave community mothers the impression that Mentor-Mothers worked for a well-funded, “reputable” and credible program.
“[The tablet] means to the client that you’re educated and you have a reputable post at a reputable company.” [Mentor-Mother #3]
Figure 3 presents a framework for conceptualizing the synergistic signaling effects of tablet technology on perceived credibility in the context of CHW home visits. Tablet-carrying Mentor-Mothers described an increase in their perceived credibility within the community, via three main dimensions: (1) message (i.e., videos echoed the Mentor-Mother’s messages), (2) messenger (i.e., Mentor-Mothers felt that showcasing technology skills and being entrusted with a tablet bolstered their credibility); and (3) program credibility (i.e., tablets signaled a reputable program and a broader investment of resources into CHWs’ services).
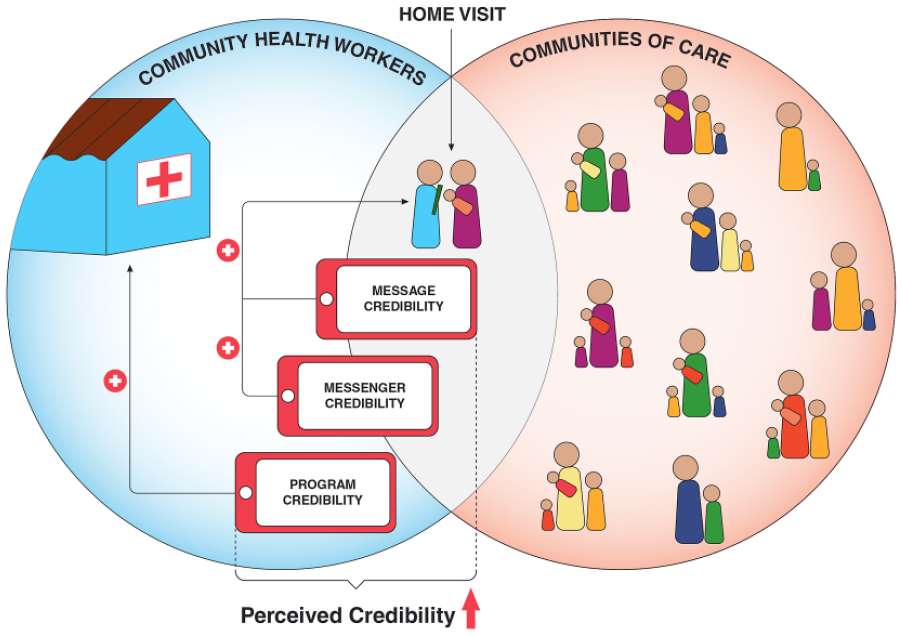
Dimensions of perceived credibility attributed to tablet technology use by CHWs in the context of home visits.
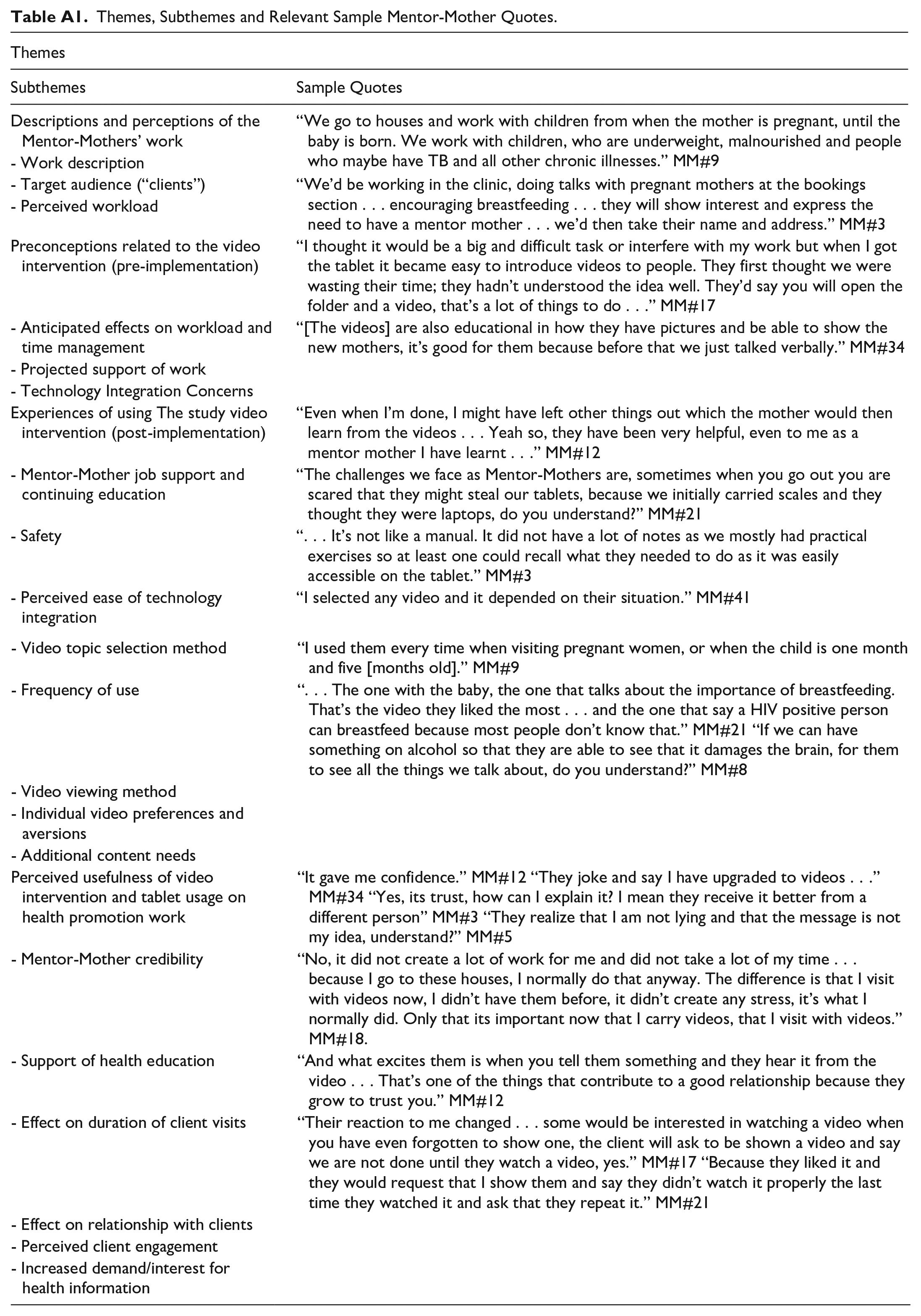
Table A1 presents additional themes, subthemes, and sample Mentor-Mother quotes.
Discussion
The near-peer status of CHWs has been a documented double-edged sword in the pursuit of effective community health promotion. Embedded and well-integrated in their communities, CHWs have easy physical access to their communities, language familiarity and first-hand experience with the challenges facing their clients. The benefits of the CHW model have led to their acceptance as a critical cadre at the frontline of health services delivery. However, the similarity of their profiles and the proximity of their experiences to those of their clients, often breed skepticism about their credibility. This mistrust can undermine engagement with their services as well as impacting their motivation to perform. (Thondoo et al., 2015)
Our study suggests that equipping CHWs with tablet technology, including animated mHealth videos, bolsters their perceived credibility through three key signaling effects, while augmenting their overall experience of delivering care through a combination of overt and signaling effects. These findings become particularly relevant when viewed in the context of prior research suggesting that CHW programs are more effective when the beneficiaries value the services being provided and when CHWs feel their perceived credibility is high within their communities.(Kane et al., 2010)
In our study, the Mentor-Mothers’ positive experiences using the video intervention to support their face-to-face counseling—and integrating tablets into their general workflow—align with the main drivers of information technology acceptance described in the Unified Theory of Acceptance and Use of Technology. These include enhancing job performance, reducing perceived effort and enhancing social influence, which is linked to perceived credibility.(Venkatesh et al., 2003) Our study suggests that early CHW concerns about the challenges of learning to use new technology can be overcome with appropriate early training sessions and access to remote technical support when technical issues arise in the field.
By reducing the burden of face-to-face counseling, (by approx. 40% in our study), accessible mHealth videos could potentially lighten the workload of CHWs while simultaneously supporting consistency of messaging across clients. This potential—for technology to partially replace face-to-face interactions with CHWs—is a point of controversy in the ongoing discussion around mHealth interventions. A significant body of research emphasizes the need for ongoing face-to-face counseling coupled with, rather than replaced by, mHealth interventions.(Chang et al., 2013; Jennings et al., 2013; Ward et al., 2020) This coupling of humans and technology is especially valuable in under-resourced communities where trust and empathy lie at the heart of effective healthcare delivery.(Agarwal et al., 2019; Fried et al., 2015; Sripad et al., 2018)
Other research suggests that thoughtfully designed and innovative mHealth interventions have the potential to be broadly disseminated and yield similar results to traditional health promotion approaches. Additionally, these interventions may help to overcome some of the challenges and expense of face-to-face counseling, by partially freeing up CHWs’ time. These findings become especially relevant in places where face-to-face counseling opportunities with CHWs are limited.(Chen et al., 2018; Santarossa et al., 2018) Furthermore, the need for accessible, science-driven mobile messaging to be spreadable without face-to-face interactions, is perhaps one of the most salient global takeaways of the COVID-19 pandemic. When face-to-face contact is limited by external forces, mobile video interventions can be powerful assets for community health promotion, although not as powerful as when they are delivered by trained CHWs.
Limitations
Mentor-Mothers in our study developed practical and effective strategies for ensuring their safety while using valuable technology equipment in high-crime communities. For security reasons, some Mentor-Mothers opted not to use their tablets in certain settings, (i.e., when these were felt to be unsafe). Since it was practiced consistently, this selectivity could have resulted in preferential delivery of the intervention, which may have skewed Mentor-Mothers’ experiences of using it. However, the high overall usage of the video intervention during the study suggests that the effects of such preferential delivery were likely to be relatively small.
Policy Implications
Our study suggests that equipping CHWs with tablet-based interventions, including engaging and accessible mHealth videos, training them to use these and providing them with ongoing tech support, could yield measurable gains in their perceived credibility and their experience of delivering care to their communities. By reallocating a portion of their funding to enable the successful adoption of tablet-based and smartphone interventions by CHWs, government health agencies and community-based organizations could be taking an important step towards improving community health outcomes.
In the context of ongoing task-shifting within the healthcare workforce (Fulton et al., 2011; Geldsetzer et al., 2019; Zachariah et al., 2009) or where the capacity of CHWs is limited, our study suggests a potential role for tablet-based video interventions to partially substitute face-to-face time spent delivering foundational health messages.
Finally, research exploring the reasons for fragmentation of CHW programs in Southern Africa have highlighted an urgent need for harmonization of CHW programs.(De Neve et al., 2017) The scalability of tablet-based video interventions across CHW programs could support such harmonization, thus reducing fragmentation and enhancing the integration of different CHW programs within a country or region.(De Neve et al., 2017)
Equipped with tablet technology, evidence-based, animated video interventions and the support needed to successfully deploy these, CHWs stand to gain much-needed credibility within their communities. Supporting this important cadre of the healthcare workforce with the tools they need to thrive could translate into a valuable investment in the health of the communities they serve.
Footnotes
Appendix A
Themes, Subthemes and Relevant Sample Mentor-Mother Quotes.
| Themes | |
|---|---|
| Subthemes | Sample Quotes |
| Descriptions and perceptions of the Mentor-Mothers’ work | “We go to houses and work with children from when the mother is pregnant, until the baby is born. We work with children, who are underweight, malnourished and people who maybe have TB and all other chronic illnesses.” MM#9 |
| - Work description | |
| - Target audience (“clients”) | “We’d be working in the clinic, doing talks with pregnant mothers at the bookings section . . . encouraging breastfeeding . . . they will show interest and express the need to have a mentor mother . . . we’d then take their name and address.” MM#3 |
| - Perceived workload | |
| Preconceptions related to the video intervention (pre-implementation) | “I thought it would be a big and difficult task or interfere with my work but when I got the tablet it became easy to introduce videos to people. They first thought we were wasting their time; they hadn’t understood the idea well. They’d say you will open the folder and a video, that’s a lot of things to do . . .” MM#17 |
| - Anticipated effects on workload and time management | “[The videos] are also educational in how they have pictures and be able to show the new mothers, it’s good for them because before that we just talked verbally.” MM#34 |
| - Projected support of work | |
| - Technology Integration Concerns | |
| Experiences of using The study video intervention (post-implementation) | “Even when I’m done, I might have left other things out which the mother would then learn from the videos . . . Yeah so, they have been very helpful, even to me as a mentor mother I have learnt . . .” MM#12 |
| - Mentor-Mother job support and continuing education | “The challenges we face as Mentor-Mothers are, sometimes when you go out you are scared that they might steal our tablets, because we initially carried scales and they thought they were laptops, do you understand?” MM#21 |
| - Safety | “. . . It’s not like a manual. It did not have a lot of notes as we mostly had practical exercises so at least one could recall what they needed to do as it was easily accessible on the tablet.” MM#3 |
| - Perceived ease of technology integration | “I selected any video and it depended on their situation.” MM#41 |
| - Video topic selection method | “I used them every time when visiting pregnant women, or when the child is one month and five [months old].” MM#9 |
| - Frequency of use | “. . . The one with the baby, the one that talks about the importance of breastfeeding. That’s the video they liked the most . . . and the one that say a HIV positive person can breastfeed because most people don’t know that.” MM#21 “If we can have something on alcohol so that they are able to see that it damages the brain, for them to see all the things we talk about, do you understand?” MM#8 |
| - Video viewing method | |
| - Individual video preferences and aversions | |
| - Additional content needs | |
| Perceived usefulness of video intervention and tablet usage on health promotion work | “It gave me confidence.” MM#12 “They joke and say I have upgraded to videos . . .” MM#34 “Yes, its trust, how can I explain it? I mean they receive it better from a different person” MM#3 “They realize that I am not lying and that the message is not my idea, understand?” MM#5 |
| - Mentor-Mother credibility | “No, it did not create a lot of work for me and did not take a lot of my time . . . because I go to these houses, I normally do that anyway. The difference is that I visit with videos now, I didn’t have them before, it didn’t create any stress, it’s what I normally did. Only that its important now that I carry videos, that I visit with videos.” MM#18. |
| - Support of health education | “And what excites them is when you tell them something and they hear it from the video . . . That’s one of the things that contribute to a good relationship because they grow to trust you.” MM#12 |
| - Effect on duration of client visits | “Their reaction to me changed . . . some would be interested in watching a video when you have even forgotten to show one, the client will ask to be shown a video and say we are not done until they watch a video, yes.” MM#17 “Because they liked it and they would request that I show them and say they didn’t watch it properly the last time they watched it and ask that they repeat it.” MM#21 |
| - Effect on relationship with clients | |
| - Perceived client engagement | |
| - Increased demand/interest for health information |
Acknowledgements
We wish to acknowledge the Philani Maternal Child Health and Nutrition Trust and the Digital Medic creative team who developed the videos, as well as the donors who supported this study: the Patrick J. McGovern Foundation and the ELMA Foundation.
Authors’ contributions
MA, CP, TB, SM, IL, JG, and JJ led the intervention development and study design. NJ, BM, NM, MA, NM, and IL led the data collection. MA, and SM, NJ, BM, JG, KS, and MG conducted and advised on data analysis. MA, SM, JG, AV, and TB drafted and revised the early versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Patrick J. McGovern Foundation and the ELMA Foundation.
Ethics approval
This study has been granted ethics approval by the Stanford University Internal Review Board, (protocol #46667).
Consent to Participate
Consent from each participant was obtained through written affirmation that the participant had read the information sheet and consented to take
part in the study. Neither patients nor members of the public were involved in the design, or conduct, or reporting, or dissemination of this research.