
Abstract
This study investigated factors influencing success of physician scientists in Academic Medical Centers. These organizations and individuals drive healthcare in the United States. Translation of scientific discovery to medical practice moves at an astoundingly slow and ineffective rate. We must understand what contributes to physician scientist success to speed up translation. Through a lens of dialectic process theory, a grounded theory approach identified emergent factors from lived experiences of 31 individuals, at various experience levels, with MD and PhD degrees. Role balance, autonomy, organizational support, teamwork, life-cycle mentorship, and relational capacity were relevant factors impacting success. Role balance was important for success. Teamwork, organizational support, and life-cycle mentorship helped individuals grow, achieve balance, and respect, but relational capacity emerged as a critical driver for realizing both individual and organizational success. One person cannot execute these complex roles on their own, but development of deep and meaningful relationships through teamwork, collaboration, and life-cycle mentorship are essential for life satisfaction and success.
Keywords
Introduction
Academic Medical Centers (AMCs) in the United States (US) have evolved over the last 125 years and are mission driven in healing, teaching, and research. In order to meet institutional goals, AMCs are managed similar to for profit corporations, but retain official nonprofit status with community missions. Physician scientists are individuals who invest significant time and effort in research while seeing patients in clinical practice. Although it is recognized that many physician scientists are MDs who do not hold a PhD, but those that hold both MD and PhD degrees were specifically chosen for this initial exploratory study because of the proliferation of MD-PhD training programs including Medical Scientist Training Programs (MSTPs) in the US (Harding, Akabas & Andersen, 2017). They are extensively trained to better carry out the institutional missions of discovery and treatment. Physician scientist success is intricately tied to AMC success; however, success is difficult to define for these individuals (Gotian & Andersen, 2020; Marsh & Todd, 2015). For our study population, physician scientist success is defined as those who can identify the right scientific and medical problems and subsequently find clinical solutions through research (i.e., they both problem posers and problem solvers) (Gotian & Andersen, 2020).
Schafer (2010) said physician scientists are indispensable to the medical research enterprise because they bring a unique perspective by asking scientific questions based on their direct experience with patients. Prior to 1965, in a different era of medicine, physician scientists simply assumed that scientific discovery for patient benefit would be translated widely into clinical practice (Pickering, 1964). However, today, factors influencing experiences of physician scientists in their environments must be examined to ensure advances in biomedical research will effectively translate into meaningful healthcare for society (Bloom, 2003).
Several decades ago, prominent physician scientists challenged physician scientist roles. In two seminal articles, physician scientists were portrayed as “an endangered species” (Wyngaarden, 1981) and warned that the time had come for “the end of the physician scientist” (Gill, 1984). The former stated that only 10% of all physicians in the country were part of academia and at any given time there were 1,000 open positions for physician scientists in AMCs. Subsequently, in an era of translational medicine (described by Zerhouni, 2007) it takes 17 years to translate 14% of research findings into clinical practice (Balas & Boren, 2000). This difficult and complex problem must be addressed to achieve increased success rates and shortened translational times. This is possible; for example, it took less than 10 years for the drug bortezomib to go from concept to successful treatment of multiple myeloma (Sánchez-Serrano, 2006). It is believed that better understanding the roles of physician scientists in AMCs is warranted. Although there is an abundance of literature regarding healthcare and academic medicine, there is a paucity of literature examining how physician scientists think, feel, and reason about the competing demands on their time and effort, which directly affects their success and organizational success (Rubio, Primack, Switzer, Bryce, Seltzer, & Kapoor, 2011). Billions of dollars are spent annually on medical research, healthcare, and physician scientist training. Thus, factors influencing physician scientist success have tremendous societal implications. Therefore, the research question is what factors most influence physician scientist experiences and contribute to their success?
Background and Theoretical Framework
Physician Scientist training programs such as the original MD-PhD programs and then subsequently MSTPs have origins in the Yellow Berets Program, a training program at NIH where medical doctors were trained under leading laboratory scientists. This emanated from the start of the Korean War in 1950 through the end of the Vietnam War in 1973 where many American physicians were inducted into military service through a “doctor draft”. They fulfilled obligations by conducting clinical research in the NIH associate training program and labeled themselves “yellow berets” (Khot, Park, & Longstreth, 2011), and ten of those Yellow Berets went on to win the Nobel Prize. The success of these trainees demonstrated the need for continued formalized training of physician scientists (Park, 2003). However, there was a shift in prevailing sentiment just decades later that MD-PhD programs were not sustainable going forward (see Wyngaarden, 1981, Gill, 1984, Askt, 2010, etc.).
Theoretical Framework
The slow transfer of research findings to clinical practice calls for research on processes governing the translational science. Physician scientists are key agents working in AMCs that have significant impact on these processes. Therefore, this study aimed to discover factors that influence physician scientist success to explain process change (speeding up translational science) in organizations (AMCs) (Van de Ven & Poole, 1995). To uncover novel factors, we decided to not limit our research by a predetermined conceptual framework; instead, under the framework of the dialectic process theory (Van de Ven & Poole, 1995), we took a grounded theory approach to generate theory based on the data we collect. Despite success with the “yellow berets” program that led to MD-PhD and MSTP training programs, leading scholars have been concerned that physician scientists will “vanish” or become “extinct” because they cannot effectively execute their primary roles simultaneously within AMCs that have conflicting goals and limited resources. Van de Ven and Poole (1995) referred to this as a dialectic process theory where there is a “thesis” and an “antithesis” in-play that result in conflicts, which organizational agents must continuously work to balance or create “synthesis”. Although the extant literature suggested work experience, motivation and skills, environment at work and institutional mission (described below) as factors influencing physician scientist success, we believe that there are additional important factors not detailed by this literature, which motivated this study.
Work Experience
The lived work experience of a MD/PhD is defined for purposes of this study as how they spend their time in an AMC and whether they are able to be both a physician and a scientist (Bloom, 2003; Gill, 1984; Huang, 1999; Jackson, Palepu, Szalacha, Caswell, Carr & Inui, 2003; Ley & Rosenberg, 2005; Rabatin, Lipkin, Rubin, Schachter, Nathan, & Kalet, 2004; Varki & Rosenberg, 2002; Wetherall, 1991). Individuals who are both MDs and PhDs are assumed to reside at the crossroads of academia and healthcare (Begley, 2004; Bloom, 2003; Drazen, 2002).
The work experiences of multiple competing roles are influenced by many factors that in turn impact role performance of physician scientists in AMCs. Further impact exists in translation of science from the laboratory to the clinic and from the AMC (Crowley et al., 2004; Pober, Neuhauser & Pober, 2001; Sung et al., 2003) to the practice of medicine (Westfall et al., 2007; Westfall et al., 2009; Zerhouni, 2007). It is important to understand work complexities of physician scientists, along with discovering emergent factors not yet studied, to better understand lived experiences in AMCs. Additionally, it would be important to examine the impact this has on scientific knowledge dissemination to benefit patients in the community. Physician scientists leverage their considerable skill sets and motivations to carry out their various roles.
Motivation and Skills
In academic medicine, motivation is defined as the reason why individuals set specific goals around research and teaching expectations and how to inspire the improvement of clinical skills (Rabatin et al., 2004; Wright & Beasley, 2004). Motivation for individual physician scientists likely depends on a number of different intrinsic and extrinsic factors as predicted by Self-Determination Theory (Ryan and Deci, 2000). Recent work from the same authors indicated that both intrinsic motivation and well-internalized forms of extrinsic motivation predict an array of positive outcomes across various educational backgrounds, and environmental contexts (Ryan & Deci, 2020). For the current study, physician scientists were asked about motivation for research, teaching, and clinical care activities they perform, by academic rank, balance between personal and professional life, and alignment with institutional mission for reaching mutual success or dealing with challenges (Andrews, 2002; Beasley & Wright, 2003; Ley & Rosenberg, 2005; Rabatin et al., 2004; Solomon, Tom, Pichert, Wasserman & Powers, 2003; Straus, Straus & Tzanetos, 2006). Thus, the goal here was not to disentangle intrinsic versus extrinsic motivation for these complex roles, but rather to investigate motivational role factors that impact long-term career paths of physician scientists (Ley & Rosenberg, 2005; Holcombe, 2005; Solomon et al., 2003; Straus et al, 2006. In AMCs, motivation is reduced regarding scientific and academic careers more than ever before because of increased clinical care pressures, which point toward the risk of physician scientists leaving AMCs (Lowenstein, Fernandez, & Crane, 2007).
Having both technical skills exhibited by utilization of cognitive competencies (IQ) and non-technical skills like emotional and social awareness, the ability to listen and communicate well with others, while managing relationships (EQ) are necessary to achieve success (Sarla, 2019). The combinations of these skills drive the level of physician scientist expertise at the interface between the art and science of medicine (Drazen, 2002). Skills (both IQ and EQ), as explained by Holcombe (2005), are divided and influenced by three categories: (1) Academic Clinician—patient care priority, but enrolls subjects into clinical research; (2) Clinical Academician—primary skill set is academia (teaching) and clinical care; and (3) Physician Scientist—basic laboratory research translated to clinical practice. Physician scientists are the most difficult to recruit, retain, promote, and support in an AMC because these are the individuals most responsible for the transfer of medical knowledge into the practice of clinical care (Holcombe, 2005). Others have broken down the combined skill sets of physician scientists (Goldstein & Brown, 1997; Schechter, 1998) as follows: (1) Basic Science Researchers (MDs and PhDs); (2) Disease-Oriented Research (MDs and PhDs); and (3) Patient-Oriented Research (MDs).
The skills required to perform these roles were discussed with physician scientists to understand their experiences and why certain skills prevail over others in AMCs. Opportunities for utilization of these skill sets are greater than ever and the physician scientist is positioned to rapidly make discoveries impacting clinical patient care; however, it is increasingly difficult for a single individual to simultaneously utilize all considerable skill sets (Goldstein & Brown, 1997). How physician scientists leverage their motivations and skills are key components to environmental cultures at work.
Environment at Work
Environment is defined as the traditional setting where the physician scientists most often perform their translational research work (i.e., the AMC). Nonprofit AMCs and physician scientists face growing fiscal pressure from enterprises within healthcare environments. These pressures include managed care and reduced reimbursements that threaten the existence of such individuals and their ability to translate science into healthcare (Bloom, 2003; Huang, 1999). The AMC environment is outdated and thus scholars have postulated for the creation of a revised national environment where the next generations of physician scientists can improve the lives of people worldwide (Rosenberg, 1999a, 1999b). This supportive environment has five components: (1) the ability to succeed in AMCs as the home for physician scientists (objective of this current research); (2) complete with more varied PhD opportunities; (3) the establishment of a national center for clinical research; (4) creation of a network among all NIH supported institutions conducting clinical research (i.e., the CTSAs; Zerhouni, 2007) and; (5) the creation of an environment where other research sponsors, including insurance companies or industry, partner with NIH and AMCs to drive the clinical research agenda. The climate in the AMC must be conducive to making the physician scientist feel essential to the progress of academic medicine (Rosenberg, 1999b). The engagements of community-based research practices are changing clinical research environments and expanding physician scientist reach to clinical settings where translational medicine can be more frequently realized (Westfall et al., 2009). However, we do not yet see sufficient evidence of more effective translation to the community practice of medicine and we need to understand why those barriers continue to exist. Perhaps misalignment with institutional missions is one of the major barriers.
Institutional Missions
The institutional mission of an AMC is defined as a focus toward translating basic research more efficiently into clinical research opportunities with the ability to impact the quality of global health care (Westfall et al., 2007). This fact has been critical over the past 2 years during a global pandemic. The NIH Roadmap further defines and outlines the role of AMCs and the NIH is setting the future organizational research standards (Zerhouni, 2005; Zerhouni, 2007). Institutional mission is critical because the majority of clinical research occurs in the AMC setting, but most patients receive care in outpatient primary care settings (Westfall et al., 2007). Many agree that the primary mission of AMCs is to move scientific discovery to meaningful clinical outcomes (Pober et al., 2001; Zerhouni, 2005; Zerhouni, 2007). Yet, these institutions continue to face serious obstacles around funding (Crowley et al., 2004), regulatory barriers (Kim, Ubel, & De Vries, 2009), internal undervaluation of AMC mission, and the professional satisfaction for physician scientists to pursue a career solely in clinical medicine (Dickler, Korn, & Gabbe, 2006). Physically, the academic and clinical environments often overlap; however, there is a divergence of philosophies that continue to separate the missions of academic and clinical medicine, which is challenging for physician scientists (Bromley, 1999). This is particularly true in translational research or where these worlds intersect because this research is hindered by high costs (Sung, et al., 2003), slow translation of results (Glasgow, Lichtenstein, & Marcus, 2003), lack of funding (Crowley et al., 2004), poor IT systems (Scott, 2007), regulatory burdens (Kim et al., 2009), and a shortage of investigators (Sung et al., 2003). These long-standing challenges interfere with clinical and translational research (Crowley et al., 2004; Kramer, Smith, & Califf, 2012). Physician scientist success is critical to overcoming these challenges in the complex environments of academia and medicine.
Method
We conducted an inductive qualitative study based on semi-structured interviews of physician-scientists (i.e., individuals that have earned Medical Doctor (MD) and Doctor of Philosophy (PhD) degrees) (Gotian & Andersen, 2020). The research employed grounded theory as outlined by Strauss and Corbin (1998), and subsequently extended as constructivist grounded theory per Charmaz (2006), as the primary means of data collection and analysis. This method was used to better understand the literature gap from physician scientists as “endangered species” to MD-PhD training programs that are more robust than ever before. The methodology also enables researchers to understand more precisely the meaning of events, situations, emotions, and participant lived experiences (Strauss & Corbin, 1998). Collections of narratives were thoroughly analyzed multiple times to derive themes about actual experiences in order to discover emergent factors that enable the researchers to generalize and disseminate this knowledge as related to the research question under investigation.
Participants
Summary of Interview Sample.
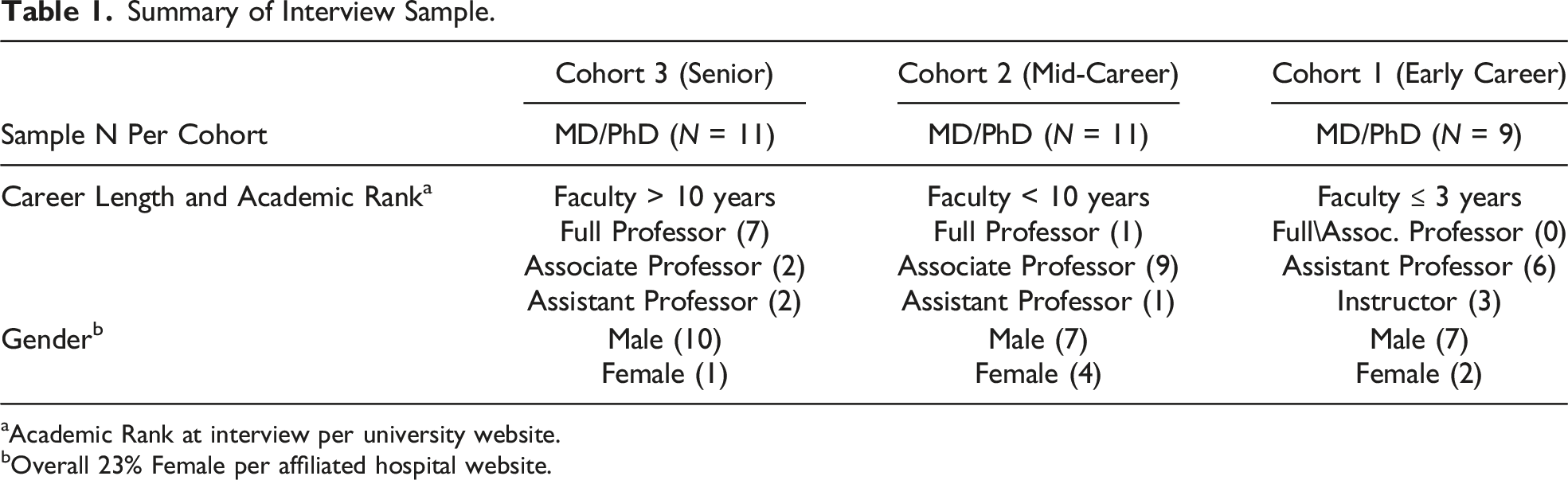
aAcademic Rank at interview per university website.
bOverall 23% Female per affiliated hospital website.
All participants had earned both a MD and a PhD degree either in a combined degree program (N = 22), earned the MD and subsequently a PhD (N = 6) (Varki & Rosenberg, 2002), or earned the PhD and subsequently a MD (N = 3). The participant’s areas of medicine specialty and primary scientific areas of their PhD were recorded. This sample did not differ by medical specialty area or PhD degree from extensive data collected on MSTP programs by Brass, Akabas, Burnley, Engman, Wiley, and Andersen (2010). See also Supplemental Table 1.
Two participants in Cohort 1 and one in Cohort 2 were not currently grant funded (all others had funding).
A total of 62 interview candidates were contacted by e-mail after being identified either through the investigator’s contacts with the SOM’s MSTP program or the investigator’s contacts in the credentialing offices of the AMCs. A 50% interview participation rate from those contacted was achieved at time of perceived theoretical saturation.
Data Collection
Institutional Review Board (IRB) approval was obtained from the university’s IRB in accordance with 45 CFR 46 (protection of human subjects in research). In depth, semi-structured interviews were conducted over 6 months. Physician scientists were invited to participate in 60-minute, face-to-face interview.
The interviews took place on the shared campus of the AMC. Each interview environment was private, which ensured confidentiality of participants and security of data collected. Interviews were audio recorded (Charmaz, 2006), with the permission of the participants during the IRB approved informed consent process and utilized a digital voice recorder to ensure comprehensive transcription. External experts provided transcription services and digital recording were then deleted from the voice recorder.
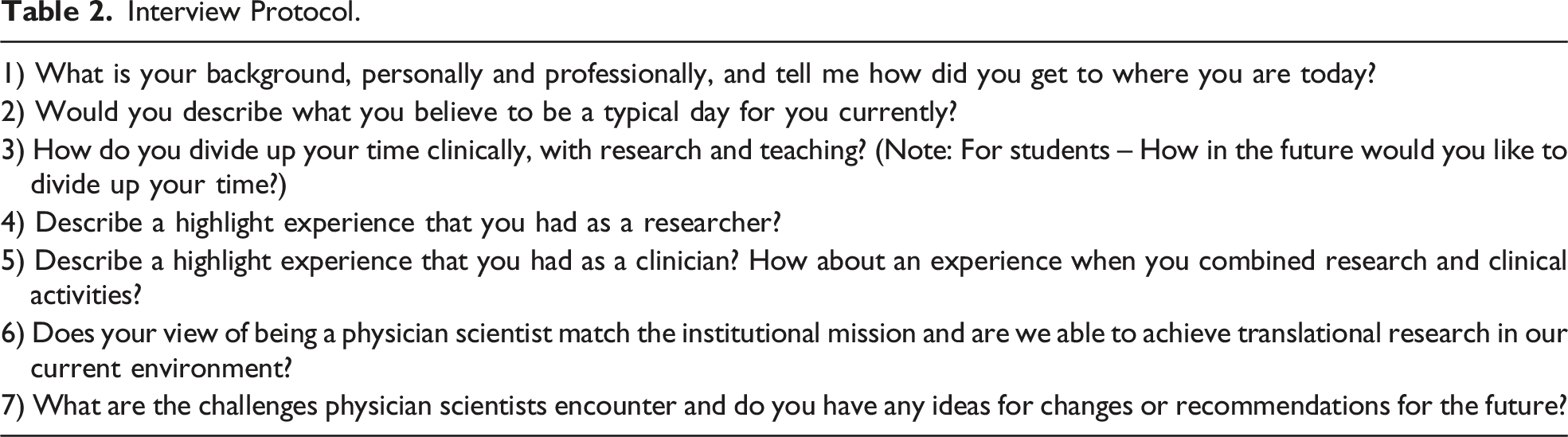
Interview Protocol.
Data Analysis
Analysis of the interview data began upon transcription of the first interview and continued beyond the completion of the last, utilizing a constant comparison approach (Charmaz, 2006). Words and phrases were parsed from the interview data using a three-stage procedure of open coding, axial coding (Strauss & Corbin, 1998), and selective coding (Glaser, 1998; Saldana, 2009). Open coding involved iterative line-by-line readings of each interview transcript to identify bits of text with study applicability. The primary researcher reviewed each transcript by listening to the audio recording to ensure transcription accuracy during open coding. Transcribed interviews were uploaded into a qualitative data analysis software package (MAXQDA 10). The primary researcher created and applied codes within the software package for the first three interviews before employing a constant comparison method against all other interviews throughout the coding process. During open coding, any and all statements were identified that appeared to be of interest and each was categorized in the software with bits of similar meanings captured from other interviews. These categories of data were defined, labeled, and refined throughout open coding. This phase yielded 5,146 coded moments, an average of 166 coded moments per transcript, and 257 unique codes.
In a second phase of interpretation, axial coding was used to discover emerging patterns, themes driven by basic-level concepts, and abstracted to higher-level categories (Charmaz, 2006; Saldana, 2009; Strauss & Corbin, 1998). The categories were continuously refined, relabeled, and sub-categorized to achieve finer and finer distinctions between categories until themes or factors emerged from the interview data (Charmaz, 2006). During axial coding, 69 higher-level categories emerged from interview concepts and were sorted around 25 factors along with the trimming down, refining, or re-categorization of information during continued searching for the most relevant themes in lives of physician scientists.
In the third stage, selective coding was used to prioritize key ideas. Selective coding is progressively refining themes or factors by going into the literature to yield additional insights (Glaser, 1998). This is an abstraction process to move from many factors to the key number of manageable factors. High-level concepts were created, serving as the key concepts that drive the findings of the research. Six final selective codes emerged as the relevant factors (themes), defined by 24 sub-categories from the data, and were compiled into a codebook.
Next, inter-rater reliability was established for the codebook as exported from MAXQDA software. A complete copy of the codebook was provided to two associates after 15 of the 31 transcripts were coded. Each associate coded five separate transcripts utilizing the codebook and these were subsequently compared against the transcripts coded independently by the primary researcher. Questions and discussion occurred after each transcript was coded to ensure clarity of the data. Inter-rater reliability of 83% and 87% was achieved, respectively. This exercise significantly improved the understanding and consistency of coded data while verifying the initial recognition of factors and sub-categories.
Finally, the primary researcher utilized the post inter-rater reliability codebook with a constant comparison approach to review the remaining transcripts and found no emergent codes indicating theoretical saturation. Terminologies of code labels were again refined and final definitions were created for each of the six factors and 24 defining sub-categories. The entire analytical process is summarized in Supplemental Figure 1 and is similar to components of the detailed qualitative research process articulated by Anfara Jr., Brown, & Mangione, 2002.
Findings
It was recognized early in the coding process that codes clustered in two principle domains of lived experiences that the researcher identified as “professional life” and “personal life”. Subsequently, it was clear that emerging factors often belonged in both personal and professional domains. Many participants (27 of 31, 87.1%) discussed these overlapping domains as a sense of “life satisfaction” that they expected when they felt accomplishment or success. It is from this idea of physician scientist life satisfaction as discussed by participants (e.g., “whenever you can definitively answer a question and help a patient, its profoundly satisfying. I love that. I love that part of the job” – Interview 2-019) that six factors emerged as necessary conditions for success in their roles at AMCs. These findings are depicted in Figure 1 and described in more detail below. Depiction of emergent findings.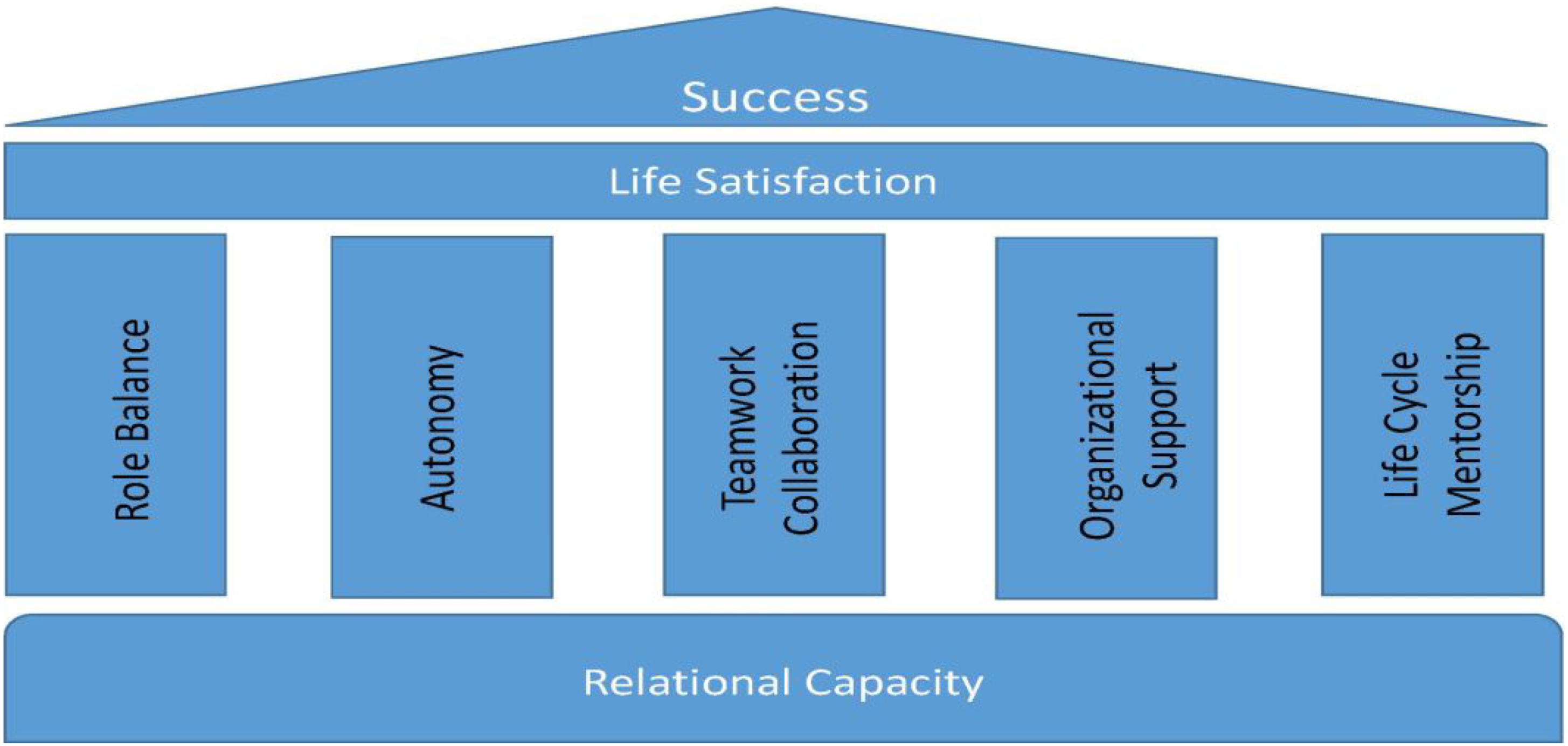
Finding 1: Role Balance
Once people were in balance at work (i.e., as a scientist, clinician, and teacher) and in life (i.e., personally and professionally), they felt in charge of their own destiny. Individuals achieving such control were able to not only balance competing roles, but also excel individually while contributing to organizational success. This balance was discussed as necessary to feel satisfied with life and career choices. “Yes, I am probably the easiest person to get to a yes on balance because I feel good about it and it’s all totally enmeshed” (Interview 2-004).
In experiences where balance was achieved, discussion of successes outnumbered discussions of challenges. The concept of balancing work roles was meaningful: “I realized that everything I did at work, no matter whether it was good or bad, was made better by having a balance in work life” (Interview 2-020). Many pressures existed organizationally to “see more patients” and spend less time teaching or conducting research. When organizational pressures became too intense to achieve role balance, three participants decided to choose one work role over others. In these three cases, two gave up research and teaching to concentrate on clinical care and one gave up clinical care to concentrate on laboratory research. All three felt that they were not utilizing their full repertoire of skills and training once that choice was made. Thus, life satisfaction did not seem complete and overall organizational mission was no longer an immediate primary concern.
Role balance was most relevant for senior and mid-career physician scientists. They had to experience significant competing time demands in uncontrolled work situations to understand the importance of striving for and achieving balance. Early career physician scientists felt more often that they could still “conquer all things equally.” The early career group was aware of “coming” role balance issues because senior colleagues warned them to stay within their limits and to learn to say “no” to challenges and tasks impacting too much on their roles.
Finding 2: Autonomy
The sense of autonomy or independence was often described as critical to success and as a measure of growth and respect for the physician scientist, such as, “I feel independent because I can do everything I need by myself. That is critical to success” (Interview 1-027), or “But, in reality, that was opportunity for me to do some independent work because he basically left me his grants, lab, personnel and put me on the road to success” (Interview 3-031).
This was interesting and complex because, on the surface, it appeared to conflict with teamwork and organizational support (see findings 3 and 4 below, respectively). However, while autonomy was important for individual success and growth, complete autonomy was not always good for organizational success that required teamwork or organizational support. This finding seemed dependent on the success level measures (e.g., individual vs. organizational). Therefore, autonomy was important for success, but complete autonomy did not necessarily ensure success.
Early stage physician scientists were more likely to discuss teamwork, and not autonomy, as important to them or influential to their experiences. However, mid-career physician scientists often singled out autonomy as a key variable to their success and sense of personal satisfaction. Autonomy or independence to this group meant, “peer respect” and frequently aligned with setting up his or her individual scientific laboratories. Autonomy was clearly important to the senior cohort, but they saw a more complete vision of both the individual and institutional needs where autonomy, mentorship, and teamwork all co-existed.
Finding 3: Teamwork
Teamwork emerged as a clear and strong finding. Clinically and scientifically, physician scientists in teams felt they could conquer all challenges: “So we team up with our colleagues at Hopkins and together we collaborate to take on the most deadly of cancers” (Interview 2-023). This epitomizes the strong sense of a movement toward team science and collaborative care experienced by all three cohorts. Collaboration is key to future survival by these individuals in volatile clinical and scientific funding environments. Scientists can no longer be experts at everything there is to know in their field and this is a good thing because it means that technology is advancing and others can help you diagnose your patient or design the next experiment in the lab (Interview memo 3-030).
We found strong similarities across the three cohort experience levels for teamwork. The senior cohort was preaching this sense of teamwork and collaboration to the mid-career and early career physician scientists. Therefore, all seemed to agree in general about the importance of teamwork for future success both scientifically and clinically. The results indicate that teamwork will help move findings from the laboratory to the patient more quickly as well as from the AMC to the community practice of medicine at a more effective rate.
Finding 4: Organizational Support
Organizational support was not just about dollars or resources being allocated, but also the ability to have time to learn and grow while establishing yourself as a contributor. Established contributors also needed time and autonomy to have a say in their schedules and how much effort they spend on teaching, research, and clinical care. This perception of support is as important as the actual physical resources allocated, though the latter is usually established first. This factor seemed to vary considerably depending on experience levels of physician scientists. More senior individuals wanted support to train future generations, which included the ability to mentor and coach more junior colleagues. The senior group generally felt they had achieved success and were somewhat less dependent on organizational support.
However, to the mid-career and early stage physician scientist organizational support was at the forefront of their minds. They wanted assurances that if there were gaps in funding that the organization would financially support them, that they would have protected time especially for research, and they did not want to hear about only seeing more and more patients: “So there’s no value to publishing a paper as intellectual drive is not valued. It’s patient care, patient care and Relative Value Units and no administrative support. There’s just no support at all” (Interview 2-016). There was also this sense of having to do more work if you did not receive the proper institutional support, which seemed to take away from opportunities to succeed individually and do more for the overall organizational mission as well. “The University or the Division should support 30% salary for MD/PhDs, but they only support 10% of salary so the other 20% you have to earn clinically and you have to do extra work to be a scientist” (Interview 2-013). Therefore, with organizational support success emerges through balance and creates opportunities where meaningful relationship building through teamwork is encouraged.
Finding 5: Life-Cycle Mentorship
Mentorship is not a novel factor for physician scientist success. However, during the interviews and data analyses it became clear that mentorship alone was not what participants were speaking about, but rather they were indicating that mentorship has no end point in the successful career of physician scientists. Even the most experienced individuals continue to learn and grow and be mentored throughout their careers, which we termed as a Life-Cycle Mentorship. For example, one participant said that “Your mentor lets you write grants with them, not all mentors are like that, mentorship is very, very key and critically important” (Interview 2-007). This type of discussion led to much insight into thinking about general mentoring (i.e., someone that guides you to benefit you and not them) and emerging into life-cycle mentorship (i.e., being the mentee, gaining respect from your peers, and emerging as a competent mentor for others; supporting others yet simultaneously being supported). Successful physician-scientists are always being mentored and eventually mentoring. There was devastation when mentorship was poor. For example, “He could have ruined my life, but I was stubborn, and did not let it happen” (Interview 1-011) and accolades when life-cycle mentorship was achieved: “She was famous, I mean she’s a true giant and yet claimed she was learning from me too” (Interview 3-006). This construct was strongly related to picking advisors who wanted to help people find their own careers medically and scientifically and not just extend their own career through the hard work of others. This also related to development of patient-physician relationships as mentorship taught lessons needed to respect and listen to patients.
Information gathered by experience levels and academic rank differed the most here. This highlights the idea of “life-cycle mentorship”. Early career physician scientists only discussed having good or bad mentors and the need for this support, mid-career individuals predominantly discussed the need to gain respect from their peers in order to become good mentors while hoping to give back to others (i.e., “when I was promoted, I still needed support, but now I was supporting others too” – Interview 2-019), and senior level participants realized that while they must teach the next generation they must also continue to learn from junior colleagues.
Finding 6: Relational Capacity
Finally, and perhaps most importantly, relational capacity emerged as a critical success factor. We did not immediately identify this terminology for this construct. Initially it was coded as “social relationships” which included friends and family support as evidenced by social identity formation: “My mother’s an MD; my father’s a PhD, so I became an MD/PhD and its how I related to both. All in the family history, I guess” (Interview 2-020). Eventually, the “social relationships” code evolved into “trusting and developmental relationships”, but that code also contained elements of collaboration, teamwork, and/or mentorship. However, something more compelling was emerging through the interviews so the naming of this finding evolved into “relational capacity” or the ability to develop deep and meaningful bi-directional relationships with others through interaction and influence. This need for deep and meaningful relationships in all aspects of life permeated throughout all interviews. “I enjoyed my second lab, it was rewarding, I had a good relationship with my mentor and the people in the lab, it went both ways, and we were getting published and presenting together” (Interview 1-002).
We did not find significant differences between experience and academic rank with regard to relational capacity. All three cohorts discussed the strong need to have good relationships both professionally and personally, to feel good about themselves, and the need for others to experience their journeys with them. This concept referenced life-cycle mentorship (described above), but it was decided to make that a separate finding and not a sub-category of relational capacity based on the emergent strength of each finding. Relational capacity was relevant to life and job satisfaction and even a sense of general happiness, so it was not merely discussed in the context of work, but also often outside of work. “I could not have done this without significant family support and having good partners and relationships is absolutely critical” (Interview 3-012). Also, “My husband is the modern man. Other than cooking, he pretty much runs the house and everything, so it’s great that I have him and that he is not in medicine” (Interview 1-011). This is clearly where the personal and professional needs of the physician scientists merged in a way that supported their entire being and experiences.
Discussion
Physician scientists in AMCs appear to feel less valued by management. This is not conducive to reaching either individual or institutional goals that may create success in this environment. However, our findings indicate that with proper role balance, autonomy, organizational support, and teamwork, physician scientists are not “endangered” (Rosenberg, 1999b; Weatherall, 1991; Wyngaarden, 1981) or “vanishing” (Akst, 2010), but rather there is growth in the physician scientist career pipeline (Ley & Rosenberg, 2005; Rubio et al., 2011) and our findings show increased need for life-cycle mentorship and relational capacity. These findings support the continued emergence of both technical and non-technical skills as described by Sarla, 2019. There is a surge of medical students and resources in dual-degree programs in the past decade (Jeffe et al., 2014). The vast majority of these individuals navigate role and organizational challenges to stringently balance their roles well. Brass, et. al. (2010) supports these findings by concluding that increasing dropout rates from MSTP programs and graduates who migrate to private practice are not justified by their extensive data collection. We believe that this provides opportunity for the findings from this study to be valuable in the following areas across AMCs.
Organizational Environment
AMCs are dynamic nonprofit organizations operating in uncertain environments with physician scientists struggling to balance multiple competing/dialectic roles while working very hard to achieve institutional success and develop their own identities (Rosenblum, Kluijtmans, & Ten Cate, 2016). Hirschtritt, Heaton, & Insel (2018) called this an evolving research ecosystem in which physician scientists must prepare for in order to understand human health and disease. Bloom (2003) and Rosenberg (1999b) agree that novel approaches to supporting physician scientists must include measures of productivity and role balance fostered through relationship building and teamwork.
The results show that physician scientists in AMCs are indeed a highly select group of individuals charged (sometimes overwhelmingly so) to simultaneously conduct research and to care for patients. The time is now to help physician scientists to flourish. Our data supports, in a contemporaneous manner, that physician scientists are “people too”. They need social and family support to achieve a sense of role balance. Additionally, they need help through organizational support (e.g., recognition) in volatile times for both physicians and scientists. These needs can be increasingly met through teamwork and collaboration; in particular, the development of trusting relationships (i.e., life-cycle mentorship and relational capacity) in order to increases life satisfaction.
Role Balance Leads to Life Satisfaction
It is critical to balance personal and professional domains (what we called a sense of life satisfaction). Morel and Ross (2014) reached similar conclusions. We believe that AMC management must monitor and support these individuals especially when this balance reaches critical tipping points (Boyatzis, 2006) such as the loss of grant funding, changes in the healthcare market place, or institutional re-organization. If management does not support them at these times there seems to be a loss of autonomy or independence, which appears to be a primary factor as to why physician scientists leave AMCs (Lowenstein et al., 2007). The fear of losing these individuals, or them not being able to use all the skills that they have, is what led to “the endangered species or dying breed” attitudes promulgated initially by Wyngaarden (1981) and Gill (1984). We saw only three of 31 (9.7%) individuals who choose one role or another from our sample (i.e., they felt they could not achieve balance or satisfaction as both a physician and a scientist). However, there were many more (26 of 31, 83.9%) that complained about their roles and a lack of understanding or insight about environmental AMC challenges. Management must pay attention to complaints and try to better understand what factors can alleviate issues. Data here provides additional insight to move AMCs closer toward physician scientist support.
Working in Collaboration
Management throughout AMCs must also encourage teamwork in both clinical practice as well as in team science. This is a non-financial form of organizational support (i.e., allowing time for teams to develop). When the physician scientist becomes overwhelmed or out of balance in trying to manage his or her role, it is a clear sign that they cannot solve the problem of inefficient translational science on their own (Faxon, 2002; Henke, 2003). They need teamwork and collaboration from other physician scientists to strategize about complex clinical cases that they face daily (Archer, 2007) and to design proper experiments and research studies to determine the underlying factors of disease. Collaboration and teamwork are not opposed to independence and autonomy. Autonomy is necessary for individual success of highly trained individuals such as physician scientists, but teamwork is necessary to coalesce these individuals together to achieve broader institutional or societal goals.
Collaboration and teamwork are based on an even simpler premise of building strong relationships with others. This first appears in our findings as mentorship then it evolves into life-cycle mentorship. It is important to understand that this finding is beyond basic mentorship that occurs every day in AMCs (Jackson et al., 2003; Rabatin et al., 2004) and in other organizations. This is the idea of being mentored early in one’s career, gaining acceptance through peer respect to become a mentor, and ultimately prioritizing giving back of knowledge to junior colleagues while continuing to gain additional insights through younger colleagues (Varki & Rosenberg, 2002). Every career needs mentorship, but a life-cycle mentorship for physician scientists’ illuminates the importance of proper mentorship at all career stages to help with efficiency and effectiveness in carrying out roles.
Building Meaningful Relationships
The idea of relational capacity (e.g., development of deep and meaningful relationships through bi-directional interaction and influence) appears foundational not only to teamwork and mentorship but also the other emergent findings of role balance, autonomy, and organizational support that together allow for satisfaction and success. Relational capacity has a more human characteristic that fits with our discussion earlier of physician scientists as being “people too”. They are not merely an asset to be allocated by management nor are they “all knowing” perfect individuals either. They are challenged and need others to help them succeed. Help or support comes from other physicians and scientists, administrators, allied health professionals, research assistants, extended family, friends, etc. Despite extensive training and education, no individual is going to speed up the translation of science to medical practice single-handedly; they are not going to solve healthcare’s economic crises by merely seeing more patients either. Therefore, building deep and meaningful relationships are a pre-requisite for success in this context. Based on lived experiences of the researchers, relationship building is not something explicitly or frequently discussed or encouraged in the manner described by study participants.
Group Differences by Experience Levels
Finally, we saw some distinct and important perspectives of emergent findings based on levels of experience across three cohort samples. This indicates that physician scientists have perspectives that evolve over time and AMC management cannot address all of them using a single approach. Early career physician scientists are still out to solve all problems in the medical sciences whereas the later career individuals are more open to the value of teamwork and building relationships to tackle complex problems. They have different perspectives on the role (but not the value) of mentorship depending on experience levels. These groups all saw the importance of organizational support, but it was clearly more strongly articulated (usually via negative experiences) by early and mid-career physician scientists. These findings show that differences among groups of physician scientists are important and in need of additional study.
Implications and Recommendations
One implication from this work is to continue to build the concept of relational capacity because there is no reason to believe that this is not a generalizable finding to other professions and organizations. Evidence of utilization of this term exists scarcely in the literature reviewed post study data collection. It was used in one nursing article to discuss relationships between patients and caregivers (Hartrick, 1997). We recommend that AMCs must promote and provide opportunity for employees (including physician scientists) to work on their relational capacity (non-technical) skills. They must understand how to interact and properly influence one another appropriately and with the institutional mission in mind. AMC management must work on navigating organizational complexities by reverting back to fundamental building blocks of organizational behavior (i.e., how all employees can support and respect one another to achieve mission goals). AMCs and physician scientists recognize the importance of teamwork and mentorships as relevant management principles necessary to achieve desired outcomes. However, individual success cannot be completely sacrificed for the betterment of the institution. The implication is that these principles need to be kept consistently in mind along with the other emergent findings so that physician scientists are treated as valued resources, with individual and collaborative experiences, that enhance institutional missions. It seems that this is a viable route to ensure that physician scientists and AMCs will positively impact society through more efficient and effective knowledge transfer in medical sciences. Collaborative efforts help drive advancement of translational medicine (Henke, 2003; Mintzberg, Jorgensen, Dougherty & Westley, 1996; Pisano & Verganti, 2008) and study data suggest that functioning toward collaboration through teamwork, relational capacity and mentorship helps balance competing priorities of clinical care, teaching and research for physician scientists.
AMCs do not always consider the whole person in providing support on the journey of the physician scientist because the institution wants to capitalize on the funding, markets, or the prestige that individuals bring to achieve their personal and professional passions (Carmichael, 2012). It is at this juncture that we find physician scientists today in AMCs. Management must care for physician scientists and physician scientists must care for the mission of the organization in a similar manner as they do for their patients to be successful. From this logic, we recommend career and leadership training curricula for physician scientists across all experience levels.
Conclusion
Dialectic process theory (Van de Ven & Poole, 1995) predicts a perceived imbalance between the roles of being a physician and a scientist. However, our study reveals that conflicts can be better managed through, autonomy, teamwork, organizational support, life-cycle mentorship, and relational capacity to a point of synthesis and improved balance between the significant roles that these individuals play. Relational capacity is a foundational finding as the non-technical skill that often gets lost in complex organizational settings, especially in the case of individuals with a high degree of technical training. AMC management must recognize these emergent factors and how they relate to physician scientist success and organizational success.
Limitations and Future Research
A limitation of this research lies in the sample. It did not include physician scientists who hold the MD degree without the PhD degree. In addition, the sample was collected only in one region of the country. The decision to examine only participants with both degrees was due to the proliferation of MD-PhD training programs and MSTPs, together with sample from the same CTSA site, limit the generalizability of these results to some extent. Future inquiries will include physician scientists that hold an MD without a PhD and a larger sample size across more AMCs. Future research will also explore group differences in ethnicity, type of degree (MD physician scientists versus MD/PhD), and gender. Even though we collected gender data of the participants in this study, the overall sample size of 31 participants (7 females) was not large enough to generalize any meaningful group differences based on gender. Therefore, this will be examined in more detail in future studies utilizing conceptual depth criteria to better understand theoretical saturation of the sample (Nelson, 2017).
The idea of relational capacity that we discovered in this study appears to be a critical factor that is not well-defined in the literature. We plan to further develop this emergent construct in quantitative studies in which heterogeneity of much larger samples (estimated at N = 500) will be possible. Efforts will be made to establish a nomological network for relational capacity and allow for continued study of physician scientists in AMCs to deductively test emerging constructs and causal relationships described herein.
Supplemental Material
Supplemental Material - Discovering Factors that Influence Physician Scientist Success in Academic Medical Centers
Supplemental Material for Discovering Factors that Influence Physician Scientist Success in Academic Medical Centers by Philip A. Cola, and Yunmei Wang in Qualitative Health Research
Footnotes
Acknowledgments
The authors would like to thank the phyician scientists who shared their time and lived experiences with us for this research. It is greatly appreciated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.