
Abstract
Despite the potential for HIV treatments to transform the health needs of people living with HIV, receiving a positive HIV diagnosis can be a difficult experience and feelings of shock, distress and concerns for the future are commonly reported. Drawing on Michael Bury’s conceptualisation of ‘biographical disruption’, we utilised semi-structured interviews to explore experiences of HIV diagnoses among 34 people diagnosed with HIV between 2016 and 2020 and living in Australia. Interviews were conducted between January 2018 and August 2021. Despite significant advances in biomedical HIV treatments and prevention, participants commonly experienced HIV diagnosis as emotionally challenging. For those with limited HIV awareness, HIV was commonly understood as a likely fatal condition. For some participants, receiving a positive diagnosis also engendered a degree of uncertainty as to their anticipated life trajectory, particularly its impact on future sexual and romantic relationships, options for starting a family and migration opportunities. For some gay and bisexual male participants, receiving a positive diagnosis almost confirmed a life trajectory that they had worked to avoid and their own sometimes-negative attitudes toward people living with HIV were internalised, making adjusting to diagnosis more complex. While all participants reported challenges in adjusting to an HIV diagnosis, some ultimately came to experience living with HIV as bringing about unexpected and welcome changes to their lives. Our findings highlight the complex and intersecting medical, social and emotional needs of people living with HIV when receiving and adjusting to a positive HIV diagnosis.
Introduction
In recent years, there has been an increasing focus on the biomedical management of HIV and so-called ‘HIV normalisation’ (Philpot et al., 2020; Squire, 2013). Discourses of HIV normalisation emerge from a range of sources, including healthcare professionals and HIV advocates, and are often deployed to minimise the impact of HIV diagnoses on those recently diagnosed and to challenge HIV-related stigma (Moyer & Hardon, 2014). HIV treatments can reduce HIV viral load to undetectable levels, thereby eliminating the possibility of onward transmission and reposition HIV as a chronic, manageable condition (Bavinton et al., 2018; McDonald et al., 2016; Rodger et al., 2016). Despite these advances in the management and prevention of HIV, receiving a positive HIV diagnosis remains a challenging and difficult experience for many, and newly diagnosed people living with HIV commonly report feelings of shock, distress and concerns for their future (Bilardi et al., 2019; Rohleder et al., 2017; van Bilsen et al., 2020; Walker, 2019). In this article, we explore the experiences of HIV diagnoses among people recently diagnosed with HIV (between 2016 and 2020) in Australia. In particular, we highlight the potential for HIV diagnoses to provoke a sense of uncertainty for the future while also sparking a shift in how individuals perceive themselves.
The concept of HIV normalisation has received some criticism for too narrowly focussing on the clinical aspects of HIV care and overlooking the day-to-day social realities many people living with HIV experience (Rhodes et al., 2019). Moyer and Hardon (2014) draw attention to HIV as both medical and social, characterising HIV as an ‘exceptional’ condition owing to persistent and ongoing stigma. HIV stigma, they argue, continues even as treatments can transform HIV into a condition that is both chronic and non-communicable. In addition to reporting concerns about HIV-related stigma (Parker & Aggleton, 2003), including self-stigma (Pantelic et al., 2019), people living with HIV often report concerns about the impact of HIV on employment (Munson et al., 2021), sexual and romantic relationships (Flowers et al., 2011), and migration and travel opportunities (Körner, 2007).
Drawing on Michael Bury’s (1982) conceptualisation of ‘biographical disruption’, previous research has characterised HIV diagnosis as a moment in which one’s anticipated or imagined life trajectory is disrupted (Alexias et al., 2016; Campbell, 2021; Orsini & Kilty, 2021). For Bury (1982), the diagnosis of a chronic illness is an experience in which individuals not only confront a new medical and health reality, but also undergo a shift in perceptions of self and identity. For those who receive an HIV diagnosis, this might mean adjusting to a daily treatment regimen, increased engagement with healthcare systems and engaging in new forms of physical and emotional self-care. Chronic illnesses (including HIV) can also elicit new uncertainties around ongoing and future health complications, even when such conditions are managed medically.
Diagnoses are also social processes that have the capacity to construct and shape how individual identities are understood by others (Blaxter, 1978; Fox, 2011; Jutel, 2009, 2011). Perceptions of HIV and those living with the virus are commonly influenced by overarching social and cultural scripts (Carricaburu & Pierret, 1995; Flowers et al., 2011). Despite the advances made in biomedical HIV treatment and prevention, discourses about HIV draw on notions of social transgression, deviancy and engagement in immoral and unhealthy acts (Moyer, 2015; Pantelic et al., 2019; Treichler, 1987). Discourses of deviance and transgression may then be projected onto people living with HIV who become characterised as posing a threat to both the physical and moral health of the broader community (Baumgartner, 2007; Flowers et al., 2011). HIV diagnoses, then, can also work to (re-)define and shape individual identities as particular ‘types’ of (ir)responsible citizen.
Following Bury (1982), in this article, we conceptualise HIV diagnosis as a moment of ‘biographical disruption’ and argue receiving an HIV diagnosis can engender a degree of uncertainty over life trajectories and shift how individuals perceive themselves. In this article, we explore how HIV diagnoses were experienced, and highlight four overarching themes: (1) the potential for HIV to impact future work and migration opportunities; (2) uncertainties around opportunities for future sexual and/or romantic relationships; (3) HIV-related self-stigma and changing perceptions of the self; and (4) reclaiming a ‘spoiled’ identity.
Methods
Study Setting
The analysis in this paper is based on data from an ongoing, qualitative cohort study of people recently diagnosed with HIV in Australia. Ethics was approved by the UNSW Human Research Ethics Committee.
Eligibility and Recruitment
Eligible participants were 16 years or older, living in Australia, and had received an HIV diagnosis in 2016 or later. Recruitment occurred through self-referral or through referrals from sexual health centres, high caseload HIV clinics, and community-based HIV organisations. After enrolment, participants were contacted by email or telephone by a member of the study team and invited to be interviewed.
Data Collection
Semi-structured interviews were conducted face-to-face, via telephone, or through video conferencing software by authors one, two, and three. An interview schedule was developed based on prior learnings (Gianacas et al. 2015) and in consultation with key stakeholder organisations. Interviews were conducted between January 2019 and August 2021, were audio recorded, transcribed verbatim by a professional transcription service, and de-identified. Participants were assigned pseudonyms, and these are used throughout this article. Interviews explored the experience of HIV diagnosis, access to treatment and clinical care, HIV disclosure, sex and relationships, and engagement with psychosocial support services including community-based HIV peer support services. Broader questions were also asked about participants’ involvement with HIV community organisations and other people living with HIV, and gay and bisexual communities where relevant. HIV diagnoses were a pre-determined area of interest and questions pertaining to participants’ experiences of diagnosis included the delivery from healthcare workers, what prompted participants to undergo an HIV test, participants’ reactions to receiving an HIV diagnosis, and the kinds of support (clinical, psychosocial and/or community) services they engaged after diagnosis. Participants were invited to participate in follow-up interviews approximately 12 months later. These explored any changes to participants’ experiences of living with HIV, changes to treatment, and the impact of COVID-19 on participants’ access to HIV treatment and care.
Analysis
Interviews were entered into NVivo software version 12 and thematically analysed (Braun et al., 2019; Braun & Clarke, 2019). Upon interviewing 35 participants, it became evident that no further thematic areas were being identified and that effective data saturation had been reached (Saunders et al., 2018). In line with Braun and Clarke’s (Braun et al., 2019; Braun and Clarke, 2019, 2021) approach to thematic analysis, interview transcripts were read by members of the research team to ensure familiarity with the data. Conceptual and descriptive codes were then developed by authors 2 and 3 based on a close reading of a small number of interviews, and discussions with the larger research team. Using an inductive approach (Boyatzis, 1998) and drawing on existing empirical literature, the codebook was revised as remaining transcripts were analysed and new themes were identified in the data. To ensure reliability, regular meetings were held within the research team to discuss findings as they arose. Analysis for this article was conducted by author 1 and focuses primarily of participants’ accounts of receiving, and adjusting to, a positive HIV diagnosis.
Findings
Participant characteristics.
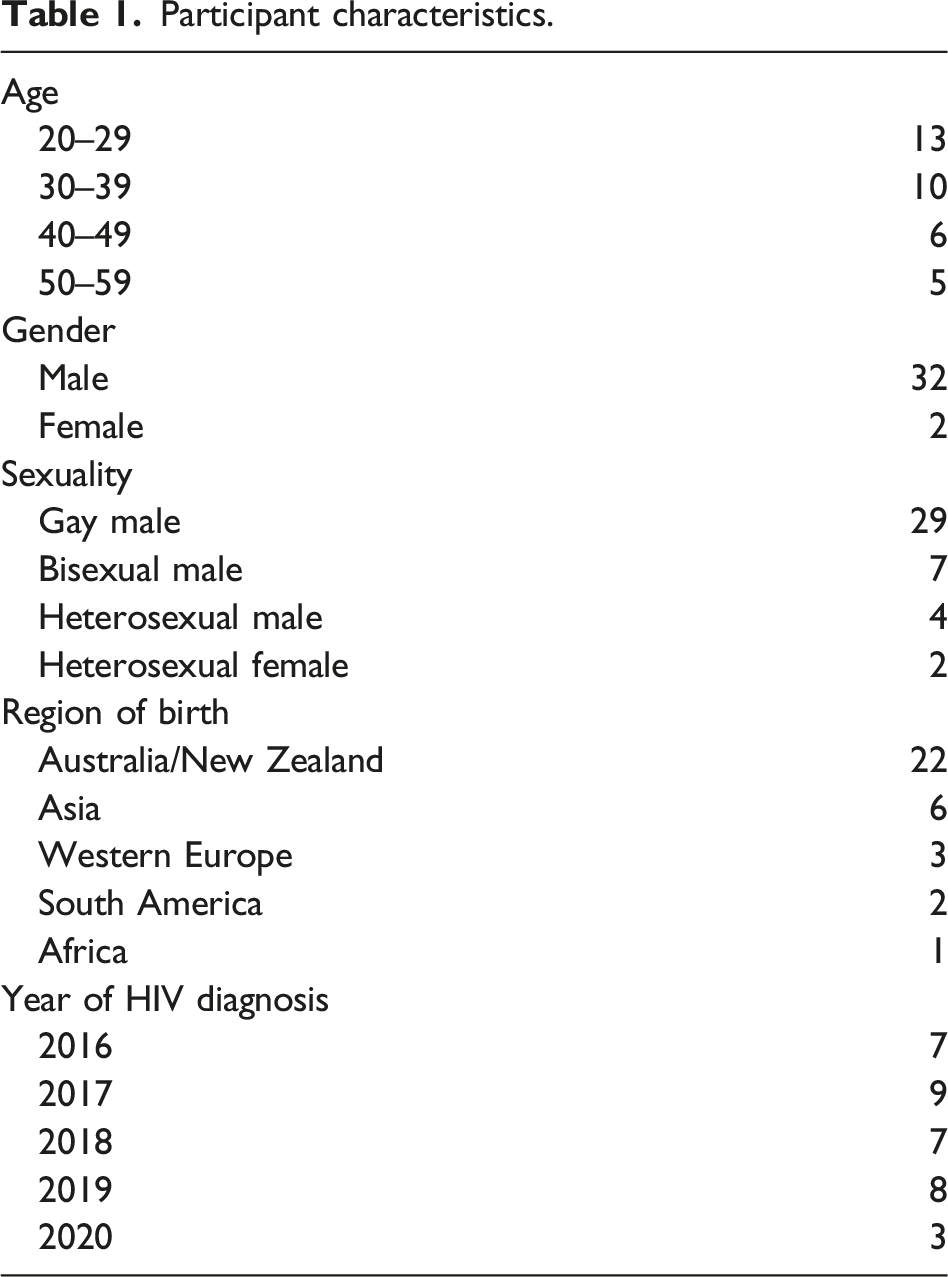
Participants recalled a broad range of reactions to being told they were HIV-positive and commonly described being shocked, overwhelmed, and having difficulty comprehending all the information being conveyed at the time of diagnosis. Some participants, particularly those with lower levels of HIV awareness, also recalled an initial belief that HIV would significantly reduce their life expectancy. At diagnosis, many participants also recalled a concern over the potential for HIV to limit their plans for future relationships, employment and migration opportunities. Among some participants, receiving an HIV diagnosis forced them to confront their own underlying, negative attitudes toward people living with HIV, attitudes which were then internalised at or shortly after diagnosis. All participants experienced challenges in coming to terms with their diagnosis. After a period of time, however, some participants came to experience HIV as bringing beneficial changes to their lives, including feelings of improved health and of HIV as an opportunity for personal and emotional growth. In the following sections, we describe four overarching themes: diagnosis and disrupted life trajectory; disruption of sexual, romantic and social relationships; diagnosis and contending with HIV (self-) stigma and; reclaiming a ‘spoiled’ identity.
Theme One: Diagnosis and Disrupted Life Trajectories
When reflecting on the period immediately following their diagnosis, participants commonly described a sense of HIV as making their plans for the future less certain. Pai had migrated to Australia from Southeast Asia in 2016 and was diagnosed with HIV shortly after his arrival. In his home country, Pai described sexual health facilities as ‘not easily available’ and a ‘lack of [HIV] information’ such that he had ‘never noticed that there’s treatment [for HIV]’. At the time of his diagnosis, Pai (gay male, 28) was unaware of HIV treatments and their role in transforming HIV from a likely fatal illness to a chronic, manageable condition. Given his limited HIV awareness, Pai recalled being ‘totally freaked out’ and having a ‘total meltdown’ when he received his HIV diagnosis. Pai went on to state: I have lots of plans in my mind. I want to get someone in my life, and I want to get a kid, maybe surrogates … All these things completely faded away … Without all the information [about treatment], I thought that this is the end. Sooner or later, I’m going to die.
Pai initially believed his diagnosis meant his life expectancy would be significantly shortened. Given this, Pai felt his hopes for the future, particularly in finding a partner and starting a family, had been foreclosed. Pai went on to describe ‘crying’ and being ‘completely blocked in my mind’ such that, despite the clinic closing at 5p.m., the diagnosing clinician and in-house counsellor stayed with him until 7p.m. to ensure he had all the support and information about HIV he needed. For Pai, it was his understanding of HIV as a terminal illness and his limited awareness of HIV that underpinned his distress and fear about disrupted future plans.
For many participants, receiving a positive HIV diagnosis was a moment in which their plans for the future were called into question. For some, limitations on work and migration opportunities were viewed as making their future less certain. As with Pai, Marlon (gay male, 37) was living in Australia on a temporary visa at the time of his diagnosis in 2017. Marlon received a reactive result to a rapid HIV test at which time the nurse stressed the role of treatments in minimising the medical impact of HIV. Despite having had only limited awareness of HIV treatments prior to his diagnosis, Marlon readily accepted that with treatment, HIV need not be ‘a death sentence’. However, Marlon’s diagnosis raised concerns for his future that extended beyond simply the medical aspects of living with HIV: I felt [I] lost my future. I felt [I] lost my family, lost my job. Lost everything … I didn’t think I was going to die at all. I didn’t think about the sickness, the treatment. I just thought [about] my future.
Marlon’s more immediate concern was how HIV would affect his relationships and employment opportunities, with his diagnosis instilling a sense of loss and uncertainty as to his future. Living in Australia on a temporary visa, Marlon’s diagnosis also made his plans to remain in Australia less certain. Australian immigration rules include a provision that considers a person’s likely healthcare and community service needs in Australia over a lifetime. As the lifetime cost of HIV treatment and care are considered to be too expensive by policymakers, non-residents living with HIV automatically fail this provision, even when HIV infection occurred in Australia. Marlon described feeling: numb in my body, and I just feel all of my dreams, all of my effort, I have no more future in Australia … I tried to do something proper to reach my goal to have [a] good future, better life … but when I got diagnosed with HIV, I just feel it stopped my dream. So [I] just feel [there is] nothing left for me.
Marlon arrived in Australia from Southeast Asia in 2012 and saw it as an opportunity for greater freedom, earning capacity and a chance to explore his sexuality in a way he felt unable to in his home country. After being diagnosed in 2017, Marlon felt his opportunity to remain in Australia and subsequent chance for a better future had been foreclosed. At the time of his interview Marlon had had his application for permanent residency denied by Australia’s Department of Immigration. While Marlon had appealed the decision, applied for a ‘health waiver’ and remained in Australia on a ‘bridging visa’, his diagnosis had made his imagined future in Australia and his perceived opportunities for a better life less certain.
Theme Two: Disruption of Sexual, Romantic and Social Relationships
Participants were cognisant of the social stigma of HIV among the broader community and the potential for rejection from sexual and romantic partners. Given this, receiving a diagnosis was accompanied by concerns and uncertainties about navigating sexual and romantic relationships. Imagining his future as someone living with HIV, Ronny (gay male, 42) recalled, ‘I was thinking … this is the beginning of my single life forever’. Despite being single at the time of his diagnosis, Ronny characterised HIV as the ‘beginning’ of a new chapter in his life in which he felt there was no possibility of entering into a relationship. Bunji (gay male, 41) similarly stated, ‘My biggest concern at the time was: who was going to love me now that I’ve got this virus’. For both Ronny and Bunji, HIV was seen as a barrier to any possibility of finding a partner.
Receiving an HIV diagnosis introduced the possibility of a shift in familial relationships for some participants, particularly as it raised concerns of the potential for rejection. Owing to her anticipation of HIV-related stigma, Amber (heterosexual female, 29) recalled a concern following her diagnosis that she might ‘lose a lot of friends and family’ Similarly, just as Bunji felt that HIV might limit the possibility of future romantic relationships, so too was he concerned over the impact his diagnosis might have on his broader social networks: That was what was going through my head [when I was diagnosed]: “I’ve let down my family. Oh fuck, I have to tell them this now. And I’m going to die on them, and they’re going to have to care for me, or [they’ll] abandon me.” All that stuff going through my head.
Just as Bunji was concerned for himself, his account also evokes a sense of responsibility he felt toward his family to remain HIV-negative, and the associated shame of having not done so. Bunji’s anxiety at receiving an HIV diagnosis was underpinned by a concern about how HIV might impact his familial relationships and that by telling his family he was HIV-positive, he might also experience rejection and abandonment.
Theme Three: Diagnosis and Contending With HIV (Self-)Stigma
While participants were generally aware of the potential for HIV-related stigma, except for sexual rejection, few reported having directly experienced stigma enacted by others. For some participants, however, their own perceptions of, and attitudes toward, people living with HIV had also been shaped by HIV-related stigma, a stigma that became internalised at diagnosis. Rhys (gay male, 35) stated: My biggest concerns were emotional and my own neurosis about not feeling adequate. And now, being in a new country, not knowing anyone, and now I have this disgusting disease. A lot of it was the self-loathing.
For Rhys, receiving a positive diagnosis elicited feelings of inadequacy that were exacerbated by having only recently arrived in Australia and therefore having limited social networks. Having migrated from southern Africa, Rhys’ perceptions of HIV were intimately bound with notions of class, race and socio-economic status: [HIV] is a class thing, very much. [Contracting HIV] is just something that would happen to the uneducated, the stupid. It’s so ignorant it’s ridiculous. It’s staggering, looking back on it … there’s definitely a cultural and a class connotation to HIV. There’s a stigma there, massively. Either you’re a massive drug user or you are low born, to say it like that. It’s just not something that would happen to someone from a good family.
Rhys’ experience of diagnosis was shaped by understandings of HIV that were inseparable from notions of (ir)responsible sexual citizenship (Weeks, 1998). Having grown up in a country in which HIV was highly stigmatised, Rhys associated HIV with particular types of person, with HIV considered a marker of social transgression and deviance. Although gay himself and therefore at heightened risk of contracting HIV, Rhys had considered HIV as peripheral to his life precisely because he saw himself as a ‘responsible’ citizen: ‘I grew up on a farm. I was in a stable, committed relationship. There was no way I could get it [HIV], in my head, even as a gay man’ Rhys’ perceptions of HIV became internalised and, in turn, his experience of diagnosis was underpinned by feelings of shame, inadequacy and of feeling deviant.
Echoing the experiences of Rhys, Percy’s experience of diagnosis was underpinned by negative perceptions of people living with HIV. Unlike Rhys who perceived HIV as far removed from his own experiences, however, Percy was in a romantic relationship with an HIV-positive partner, a partner to whom he attributed his seroconversion. Recounting his experience of being told he was HIV-positive, Percy recalled ‘wondering … how people would perceive me’ When asked how he thought others might perceive him, Percy responded: A whore, very promiscuous, IV drug user, dirty. Just a step below being gay, I guess. It’s almost like another sub-group of being in the LGBT community that’s ever further a minority. That was my perception.
Percy’s anticipation of these perceptions was underpinned by intersecting stigmas about same-sex male attraction, injecting drug use, and those who engage in so-called ‘transgressive’ social and sexual behaviours. Indeed, Percy described a hesitancy prior to his own diagnosis at entering into sexual and/or romantic relationships with people living with HIV: ‘I’m not going to lie, I still did kind of have a bit of a “mm” [uncertainty] when someone told me they were [HIV] positive’. For both Percy and Rhys, HIV diagnosis marked a shift in identity, a shift whereby they not only had to adjust to their diagnosis itself, but also come to terms with an internalisation of the intersecting stigmas of HIV identities they had previously held.
For some gay and bisexual participants, receiving an HIV diagnosis elicited memories of their coming out and a fear among family members that, because of their same sex attraction, contracting HIV was almost inevitable. Bunji (gay male, 41) came out as gay in the early 2000s, shortly after the development of highly effective HIV treatments. When describing his reaction to receiving his diagnosis, Bunji recalled thinking: “Wow! What does this mean for me?” Because I thought, “I’m going to die.” When I came out to my little sister about being gay and I was 19, she started crying. And I’m like: “Why are you crying?” She said, “Because I don’t want you to get sick like that man on TV and die.” She was talking about Tom Hanks from Philadelphia.
1
In the previous section, we described the way in which HIV disrupted participants’ imagined life trajectory and, in some instances, brought a degree of uncertainty to their lives. In Bunji’s account here, however, receiving an HIV diagnosis almost confirmed a trajectory that he had worked to avoid, a trajectory also seen by others as inevitable. The sense of HIV diagnosis as confirming a biography that had up until then been avoided manifested as a sense of failure for Zaid (gay male, 40). Zaid stated: There was a lot more going on than just the simple result. It was the fact that I felt like I had failed completely myself, as a person who has self-responsibility for sexual health [and] being on the forefront of trying to stop this illness.
Prior to his diagnosis, Zaid had done some work in sexual health promotion and raising awareness around HIV prevention and testing. As such, Zaid felt an additional layer of responsibility in ensuring he remained HIV-negative. By receiving an HIV diagnosis, Zaid no longer felt able to lay claims to responsible sexual citizenship, instead expressing a sense of having not only failed himself, but also the broader community.
Theme Four: Reclaiming a ‘spoiled’ Identity
To varying degrees, all participants experienced challenges in adjusting to their HIV diagnosis. After an initial crisis period associated with diagnosis (Flowers et al., 2001), however, some participants felt the experience of living with HIV had brought about positive changes to their lives. Ton (gay male, 34) explained: I feel like I’m just being more conscious with my health from that diagnosis. I’ve been more conscious with the things that I eat, been more engaged with regular exercise now.
Similarly, Angus (gay male, 28) described being ‘more informed of other parts of my health that I may have, not been ignoring, but just wasn’t thinking about’. Both Ton and Angus had initially experienced challenges in adjusting to their diagnosis. However, living with HIV had also motivated them to be more ‘conscious’ and ‘informed’ as to other aspects of their health, aspects they had not previously given too much attention to. Sherwood (gay male, 47) also perceived himself to be in better health since his diagnosis and commented: ‘I’m healthier, even though I’ve got a virus. I’m healthier and my health is monitored’’. Reflecting on the period immediately following his diagnosis, Sherwood recalled: I remember saying to myself: “okay, so as hard as it is to say, I’m middle-aged and my health is now going to be monitored for the rest of my life. Whereas if I was someone that [sic] was negative, I wouldn’t be monitored. My health wouldn’t be monitored the way it is being [HIV] positive.
For Sherwood, it was through his increased engagement with healthcare services that he came to experience himself as being in better health post-diagnosis. These narratives of being more engaged with healthcare professionals enabled some participants to challenge perceptions (including self-perceptions) of a ‘spoiled identity’ (Goffman, 1963) and make new claims to responsible and moral citizenship.
Through their engagement with HIV peer support services, some participants were motivated to become involved in HIV advocacy and support so that they too might help other newly diagnosed people living with HIV. For Bunji, it was a perceived lack of services for Indigenous Australian’s that moved him to advocate for this population: ‘[HIV] has given me purpose because there is no support for Indigenous people. It’s made me angry because I see people doing a mediocre job’. Although Bunji’s motivation was driven by a sense of frustration and anger, he nonetheless described HIV as bringing a sense of ‘purpose’ to his life. Similarly, Amber reflected on the impact of HIV on her own life, stating: I don’t think [HIV] has changed my life in a bad way. I actually think it’s changed my life in a good way. … I can become a facilitator or become a peer support [worker] for other people who are newly diagnosed. It’s given me something else good in my life to do.
Almost immediately after her diagnosis in 2017, Amber joined several HIV peer support and social groups and these played an important role in supporting her as she adjusted to her diagnosis. Over time, Amber became more involved with HIV peer organisations and took a more active role in helping others who had recently been diagnosed adjust to living with HIV. Amber was not motivated by the same sense of frustration described by Bunji. However, she too described a sense of purpose and of having ‘something else good’ to focus on. While not discounting the challenges experienced in adjusting to her diagnosis, Amber was ultimately able to experience HIV as bringing positive aspects to her life.
For some participants, it was precisely the social, psychological and emotional challenges of living with HIV that functioned as a moment for personal growth, particularly in terms of their own emotions and compassion for others. Oskar (bisexual male, 23), for example, commented ‘I think [HIV] has made me more empathetic’. In the previous section, we described how Rhys’ (gay male, 35) reaction to his diagnosis was underpinned by his associations of HIV with drug use, lower class and lack of education. At the same time, however, Rhys experienced his diagnosis as a moment of emotional growth: I also felt sick to my stomach. I felt disgusted that I had thought those things about people before without even thinking about it. I’d probably thought those things out of ignorance … It was a very humbling experience and probably not a bad thing all over.
Through his own experience, Rhys’ diagnosis illuminated his preconceptions as to the ‘type’ of person who might contract HIV. In having to confront his own prejudices, prejudices which became internalised, Rhys experienced this self-reflection as ‘humbling’ and ultimately a constructive aspect of his diagnosis.
Discussion
Participants described a broad range of reactions to receiving an HIV diagnosis. Reactions to diagnosis were often shaped by participants’ pre-existing awareness and experiences of HIV, interactions with clinicians in the diagnosis encounter, and participants’ social, sexual and romantic relationships at the time of diagnosis. For those with limited HIV awareness, HIV was often understood as a terminal illness and led to an initial belief their life expectancy would be significantly shortened. Participants commonly reported that in the initial diagnosis encounter, clinicians would emphasise the role of treatment in transforming HIV from a likely fatal illness to a chronic, medical condition. For some participants, this was readily and almost immediately accepted. For others, however, reconceptualising HIV as a manageable condition took a longer period of adjustment. Aligning with previous research, participants commonly stressed a concern about the social aspects of living with HIV over the medical (Flowers et al., 2011; Rhodes et al., 2019). In particular, participants highlighted anxieties over the potential impact of HIV on work and migration opportunities, as well as heightened complexities around navigating sexual, social and familial relationships.
In participants’ accounts, receiving an HIV diagnosis was commonly characterised as a moment of biographical disruption (Bury, 1982) that marked a shift in participants’ self-conceptualisation and anticipated life trajectory (Grace et al., 2015; Leyva-Moral et al., 2015; Locock et al., 2016; Mackworth-Young et al., 2020; Tan et al., 2020). The period immediately following diagnosis was commonly characterised as a period of uncertainty over how HIV would impact participants’ relationships with others, employment opportunities and immigration status (see Crossley, 1998). When diagnosed, people living with HIV are often confronted with a new reality in which they contend with new forms of engagement with, and reliance on, healthcare systems and pharmaceutical interventions. While this new reality perhaps most commonly appears in the diagnostic encounter, it is important to note that reactions to diagnosis are also influenced by existing social and cultural scripts (Flowers & Davis, 2013), scripts often also held by those who receive a diagnosis. Reflecting previous literature on HIV-related stigma, participants commonly noted an association between HIV and deviance, as well as an association between HIV and transgressing social and moral norms (Moyer & Hardon, 2014). These scripts map onto the bodies of people living with HIV, marking them as a threat to both the physical and moral health of the broader community (Ávila, 2015; Flowers, 2001). As both a physical and social condition (Flowers & Davis, 2013), newly diagnosed people living with HIV contend with adjusting to the medical and social aspects of living with HIV (Herek et al., 2013). This can be particularly challenging for those who hold pre-existing negative attitudes toward HIV and people living with HIV, as they not only confront the possibility of experiencing HIV-related stigma from others, but also contend with their own sense of self-stigmatisation. Our findings highlight the imperative of reducing HIV-related stigma: interventions to reduce HIV-related stigma not only have the potential to improve quality of life among people living with HIV, but also may reduce and disrupt the formation of self-stigma among those who are receive an HIV diagnosis.
The focus of our study was specifically on the experience of receiving an HIV diagnosis and so perhaps unsurprisingly, was emphasised in participants’ accounts as a particularly disruptive and significant event. Wouters and De Wet (2016) argue, however, that receiving an HIV diagnosis is not always necessarily the singular most disruptive event in the lives of people living with HIV. Similarly, Thompson and Abel (2016) caution against readings of chronic illness as biographical disruption that overstate diagnoses as occurring against stable, pre-existing life trajectories. For participants who were residing in Australia on a temporary visa, for example, their potential to remain in Australia was not guaranteed and instead relied to some extent on bureaucratic policies outside of their control. While receiving an HIV diagnosis certainly amplified some participants’ sense of uncertainty, their potential to remain in Australia was nonetheless an uncertainty that existed prior to the diagnosis itself.
In the current era of biomedical HIV treatment and prevention, there has been an increasing focus on so-called HIV normalisation, whereby HIV is framed as a chronic, but manageable, medical condition (Mazanderani & Paparini, 2015; Moyer, 2015; Philpot et al., 2020). As our data demonstrate, however, receiving an HIV-positive diagnosis remains a challenging experience despite medical advances, an experience that can disrupt one’s imagined life trajectory. Despite these challenges, a small number of participants ultimately came to experience living with HIV as bringing about positive changes to their lives in terms of both their physical and emotional wellbeing. Echoing the findings of Tsarenko and Polonsky (2011) and those of van Bilsen et al. (2020), the experience of living with HIV had also afforded these participants an opportunity for personal and emotional growth. Importantly, however, this reframing was not a linear process (Hollingdrake et al., 2022) and often took place only after a period in which they were supported to adjust to living with HIV.
Limitations
Except one participant who had refused treatment, all participants in our sample had access to ongoing HIV treatment, had sustained undetectable viral load, and were supported either by Australia’s universal healthcare system or had access to treatment and care through compassionate grounds. Similarly, all participants on treatment had been engaged in regular and ongoing care since receiving an HIV diagnosis. Globally, not all people living with HIV are afforded such access to care which would likely affect how HIV diagnoses are experienced. A large proportion of participants were recruited through community-based HIV peer organisations and their experiences are likely not representative of people living with HIV who are not engaged with these services. Also, our study did not specifically interrogate participants’ experiences of beginning and adjusting to treatment. Further investigations into the experience of HIV treatment itself, particularly around the point of diagnosis, are warranted.
Conclusion
Despite the potential for treatments to reduce the health implications of HIV and eliminate the risk of onward transmission, receiving an HIV diagnosis remains a challenging experience for some, even in the biomedical HIV treatment and prevention era. Reactions to HIV diagnoses vary considerably and are shaped by the intersecting medical, social and emotional needs of individuals. Despite the challenges of receiving and adjusting to a positive HIV diagnosis, living with HIV can also be experienced by some as an opportunity for personal growth. However, HIV-related stigma remains pernicious and also has the potential to shape the formation of self-stigma among individuals who have recently received a positive diagnosis. Indeed, some four decades into the known HIV epidemic, experiences of HIV-related stigma (including self-stigma) continue to negatively affect how individuals adjust to an HIV diagnosis. To properly support people living with HIV at diagnosis and beyond, it is important to consider the individual contexts in which diagnoses occur, while also working toward reducing social and structural inequalities and stigmas that can adversely affect individuals living with HIV.
Footnotes
Authors’ Note
Acknowledgments
We thank all participants in this study for their generosity in sharing their time and experiences for this project. We would also like to thank our partner organisations for their support of this study, particularly those who assisted with recruitment and referral of participants to this project. Thanks also to the reviewers for their constructive, and also to Chris Howard for his generous support, encouragement, and intellect.
Author Contributions
Conceptualization: Garrett Prestage, Steven Philpot, Dean Murphy; Methodology: Garrett Prestage, Steven Philpot, Dean Murphy; Formal analysis and investigation: Nathanael Wells, Steven Philpot, Garrett Prestage; Writing – original draft preparation: Nathanael Wells; Writing – review and editing: Nathanael Wells, Dean Murphy, Jeanne Ellard, Steven Philpot, Garrett Prestage.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The RISE Study receives funding from the National Health and Medical Research Council (NHMRC) Australia, and the health departments of the Australian Capital Territory, New South Wales, North Territory, Queensland, South Australia, Tasmania, Western Australia and Victoria.
Ethical Approval
All authors approved the article for submission. All procedures involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethics approval was provided by the UNSW Human Research Ethics Committee (HR180459). All participants provided written informed consent prior to their enrollment in this study.