
Abstract
A gender dysphoria diagnosis is currently required in the UK to access NHS transition-related treatment. However, this approach has been criticised by academics and activists as pathologising, ‘gatekeeping’ transgender identities, and can be viewed by the transgender community as a barrier to necessary medical care. The present research examines transmasculine experiences of gender transition in the UK, focusing on exploring the barriers encountered during identity development and medical transition. Semi-structured interviews were conducted with three individuals, and nine individuals took part in a single focus group. The data were analysed using Interpretative Phenomenological Analysis producing three main themes: ‘Conceptualising Stages of Transition’; ‘NHS Communication and Support’; and ‘Medicalisation, Power and Non-disclosure’. Participants conceptualised access to transition-related treatment as an intrusive and complicated process that negatively impacts identity development. They spoke of barriers such as lack of trans-specific healthcare knowledge, insufficient communication and support from healthcare professionals, and restricted autonomy arising from the pathologisation of trans identities. Results suggest transmasculine individuals may face numerous barriers when trying to access healthcare, and therefore, a move towards the Informed Consent Model could ameliorate many of these barriers and would empower service-users to make informed choices.
Keywords
Introduction
In the UK, the word transgender is an umbrella term to encompass all individuals whose gender differs from the sex they were assigned at birth (Ellis et al., 2015). Here, we use the term transmasculine to refer to individuals who are transgender, were assigned female at birth, and align with a masculine gender role; such as male, masculine, or non-binary. Some transmasculine people may seek to transition socially by changing their name, pronouns, and appearance, whereas others will also decide to engage with gender identity services (GIS) to access medical interventions, such as hormones and surgery.
Current NHS guidelines state that the maximum wait between GP referral and first appointment should be 18 weeks (NHS, 2019); however, the reality is that some people face waits of up to 5 years (Baska, 2022). Though the World Professional Association for Transgender Health (WPATH) Standards of Care (SOC-8) state that ‘an individualised approach to clinical care is considered both ethical and necessary’ (Coleman et al., p. 545), the NHS service specifications for transition-related treatment pathways describe a linear model in the order of social transition, hormonal interventions, and then surgical interventions (NHS England, 2019). Transgender service-users show dissatisfaction with the rigidity of this approach and demonstrate how it is often perceived as a barrier to autonomy and individualised care (Harrison et al., 2020; Willis et al., 2020).
To access NHS GIS, individuals must first be diagnosed with gender dysphoria (GD), as outlined in the DSM-5 (American Psychiatric Association; APA, 2013). However, the necessity of a GD diagnosis pathologises trans identities by focusing only on emotional distress arising from bodily dysphoria (Ashley, 2019). Service-users can therefore feel forced into adopting a ‘distress narrative’ to access medical services (Waszkiewicz, 2006). A recent meta-analysis of qualitative research into GD highlighted that social environment frequently played a role in gender distress, and the authors state that many of these experiences are not accurately captured by DSM-5 criteria (Cooper et al., 2020). The NHS medical model places additional barriers for those who do not fit into the discrete categories of ‘male’ or ‘female’, which can lead to non-binary people feeling forced to hide their identity in order to access necessary medical services (Harrison et al., 2020). This is despite NHS publications which emphasise a commitment to meeting the healthcare needs of non-binary service-users (NHS England, 2019).
Trans-led research suggests abandoning the medical model in favour of the ‘Informed Consent Model’ (ICM) (Cavanaugh et al., 2016; Ashley et al., 2021). This model attempts to ameliorate the ‘gatekeeping’ aspect of accessing transition-related healthcare by removing the necessity of a GD diagnosis. This can empower transgender people to decide if they are ready to medically transition through the routes and methods they would prefer (Schulz, 2018). Here, the role of the clinician is to collaborate with the service-user to come to an informed decision by providing comprehensive information about transition-related healthcare. In this way, the ICM works to de-pathologise and destigmatise transgender experiences. The ICM has been increasingly practiced worldwide but has not yet been used within NHS services; an oft-cited argument being that ICM will increase transition-related ‘regret’ (de Vries et al., 2021). However, a review of USA clinics which adopted the ICM demonstrated that within twelve clinics, representing a total of 1,944 patients, there were only three cases of ‘regret’ (0.1%) resulting in reversal of transition-related treatment (Deutsch, 2012). In comparison to this, research into WPATH surgeons’ experiences of patient regret of transition-related treatment (Narayan et al., 2021) found that within 18,125 to 27,325 patients, 36 ‘reversal procedures’ were performed (0.2%–0.3%). Therefore, the ICM is unlikely to increase cases of transition-related ‘regret’.
At the same time as navigating healthcare services, a transgender individual will also be undergoing a process of identity development. Many theories regarding transgender identity development are ‘stage’ models, which typically emphasise the role of emotional distress and medical interventions (Kuper et al., 2018). These stage models (Devor, 2004; Hiestand & Levitt, 2005) follow similar themes. Early stages are characterised by confusion, gathering information, and seeking community. Identity acceptance, in these models, often leads to social, then medical, transition. Despite the popularity of stage models, there are concerns that they overlook generational, cultural, and geographical differences (Bilodeau & Renn, 2005). Furthermore, they typically indicate that identity develops along a linear trajectory, which does not align with the lived experiences of many trans people (Kuper et al., 2018).
Transmasculine individuals can face unique challenges in identity development and access to healthcare. Vegter (2013) describes how trans men may enact ‘compensatory masculinity’, whereby they intentionally emphasise stereotypic masculine behaviours to achieve social validation of their male identity. Additionally, Reisner et al. (2015a) demonstrated that both enacted and anticipated discrimination within healthcare was significantly associated with substance use in a sample of 2,578 transmasculine adults in the US. Despite these distinct difficulties that affect transmasculine people, they are underrepresented in discussions of access to healthcare; one qualitative meta-synthesis of stigma in trans healthcare reported that only four of the twelve studies included transmasculine participants (Velasco et al., 2022).
There is a paucity of qualitative healthcare literature about the experiences of trans people in the UK; one exception is Harrison et al.’s (2020) Interpretative Phenomenological Analysis of eight trans people seeking medical transition. The authors describe the importance of social acceptance and illustrate the dissatisfaction expressed by participants regarding long waiting times and lack of support. However, ethical research with trans communities should avoid pathologising lived experiences (Henrickson et al., 2020); therefore, the centralisation of GD throughout Harrison et al.’s (2020) article is a significant limitation. Meyer et al. (2020) discuss similar difficulties experienced by trans adults in the US, highlighting the gatekeeping and often stigmatising stance of clinicians, and position these struggles as a matter of unmet expectations. While the work of Harrison et al. (2020) and Meyer et al. (2020) provides valuable insights into some difficulties faced by trans people, the continued underrepresentation of transmasculine perspectives (25% and 37%, respectively) confers a significant gap in our understanding of transmasculine experiences of healthcare, which we seek to address in this article.
To fully support transmasculine individuals at all points in their transition, we must understand the ways in which they conceptualise routes, methods, and ‘stages’ of transition. We use a social-constructionist framework which endorses the notion that meaning-making occurs in a sociocultural context; therefore, to understand the meaning-making activities of individuals, we must first understand their lived experiences and the narratives they use to interpret these experiences (Smith et al., 2021). This article seeks to distinguish how transmasculine adults in the UK understand identity development in the context of seeking transition-related healthcare. When our participants were given a space to speak openly about their experiences, they took this opportunity to detail their struggles of accommodating their needs with the reality of what is available to them through the NHS. Therefore, this article also incorporates discussions of barriers to healthcare that some trans people face in the UK.
Method
Study Design
A qualitative study was conducted with transmasculine adults in the UK, using semi-structured individual interviews, followed by a single focus group. Semi-structured interviews were chosen as they allowed for individual participants to raise their own concerns, while keeping consistency in the overall topics discussed. Ethical approval was granted by the University of Hull Psychology Research Ethics Committee (REF: FHS128). Data were collected in 2019, prior to the COVID-19 pandemic. This research was trans-led, the lead interviewer (TJM) is a trans man, and other members of the research team, including the co-interviewer (KR), identify as LGBTQ.
Recruitment
Participants for individual interviews were recruited via posting on a private Facebook peer support group for transgender people in the UK. To ensure informed consent, individuals were provided with a Participant Information Sheet, outlining the purpose of the study, ethical considerations, and confidentiality.
Recruitment for the focus group took place after the individual interviews had been conducted, transcribed, and analysed. Focus group participants were recruited from a private retreat for transmasculine adults. All attendees were invited to take part in the focus group via a general announcement at the beginning of the retreat and were provided with a Participant Information Sheet to help them make an informed decision.
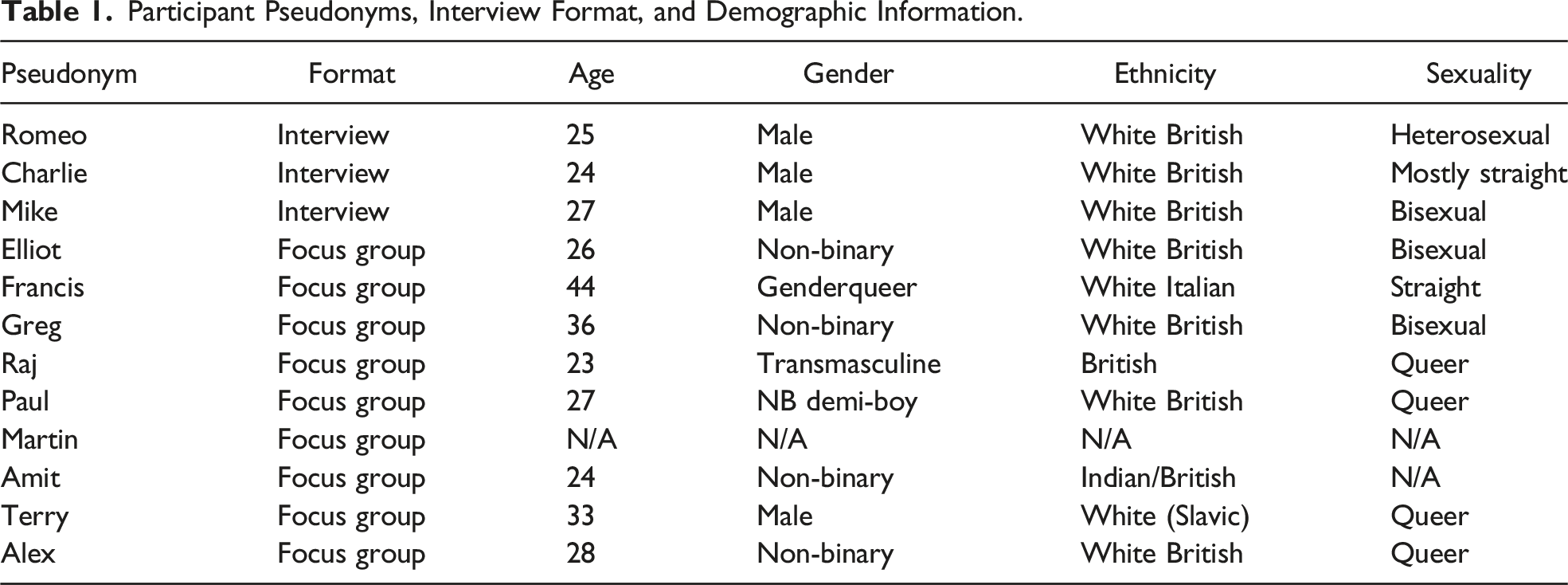
Participants
Participant Pseudonyms, Interview Format, and Demographic Information.
Data Collection
Two separate semi-structured interview schedules (SSISs) were designed and used for the interviews and the focus group. The interview SSIS consisted of ten open-ended questions, with multiple prompts. Questions included ‘What were/are the aims and goals of your transition?’. The focus group SSIS was developed after analysis of the interviews. This SSIS also consisted of ten open-ended questions and multiple prompts, such as ‘Can you describe what role GIS has played in your transition?’.
Each individual interview was conducted by the lead author, in person and in a private setting. Participants were given an information sheet and then provided written informed consent. The individual interviews were audio-recorded and lasted up to 69 minutes. The audio was transcribed verbatim, anonymised, and analysed before developing the SSIS for the focus group.
The focus group took place in a private setting and two researchers attended. One conducted the focus group (TJM), while the other researcher (KR) took notes regarding aspects that may be missed on the recording, such as layout of the room and non-verbal interactions. All participants provided written informed consent. The focus group was audio-recorded and lasted 97 minutes. The audio was transcribed verbatim and anonymised.
Following the interviews and the focus group, all participants were provided with further information about the study, sources of support, and contact information for the researchers.
Data Analysis
Interpretative Phenomenological Analysis (IPA) was used to analyse the data (Smith & Osborn, 2003). IPA is an approach which emphasises in-depth explorations; thus, a small sample size aligns with the idiographic nature of this methodology and guidance provided by Smith et al., (2009). IPA is particularly suitable for this research due to its focus on understanding personal meaning-making during key life transitions and the use of a social-constructionist framework to explore lived experiences.
Due to the idiographic commitments of IPA, individual interviews are typically preferred, allowing for the experiential claims and concerns of the participant to be centralised (Smith, 2004). However, studies have reported benefits from utilising focus groups. One such benefit is allowing for an analysis of real-time, interactive sense-making which Tomkins and Eatough (2010) call a ‘multiple hermeneutic’ whereby the researcher attempts to make sense of the attempts made by the participants to make sense of their own and others’ experiences. Although the use of a focus group could be seen as neglecting the individual in favour of the group, we have paid particular attention to individual narratives, and, following Tomkins and Eatough’s guidance, added an additional iterative loop to the analysis of the focus group in order to better situate individual narratives within the group context.
The interview analysis was informed by standard IPA practice (Smith et al., 2009), whereas the focus group analysis was informed by the work of Palmer et al. (2010). This article uses the terminology specified in Smith et al. (2009). The data collection and analysis occurred prior to changes in terminology outlined in Smith et al. (2021). Two authors (TJM and KR) conducted each step of data analysis. Each transcript was read numerous times before annotating the descriptive, linguistic, and conceptual aspects of the data. Reflecting both the transcript and the initial annotations, a list of emergent themes was established for each interview in the order they appeared in the transcript. These emergent themes, and corresponding locations of significant extracts, were then printed on individual labels; we then searched for commonalties and divergences across all data, and manually arranged the themes to create superordinate themes. As part of the interpretive process, we kept reflexive journals to remain accountable to any potential areas of bias.
The focus group data followed these same steps of analysis, with an additional examination of roles and relationships, and organisations and systems. Particular attention was given to sense-making interactions between participants. These steps reflect the social and interactional context in which the data emerged. To preserve individual contributions to the focus group, we created a table which mapped each participant’s responses to the questions posed and to each other.
The interviews and focus group were analysed separately before a final stage of bringing together the two analyses. The structure of the final superordinate themes for both interviews and the focus group was discussed between all authors to develop and confirm interpretations. Verbatim extracts which best illustrate the themes were chosen to centralise the voices of the participants.
Results
Superordinate Themes and Related Sub-Themes.
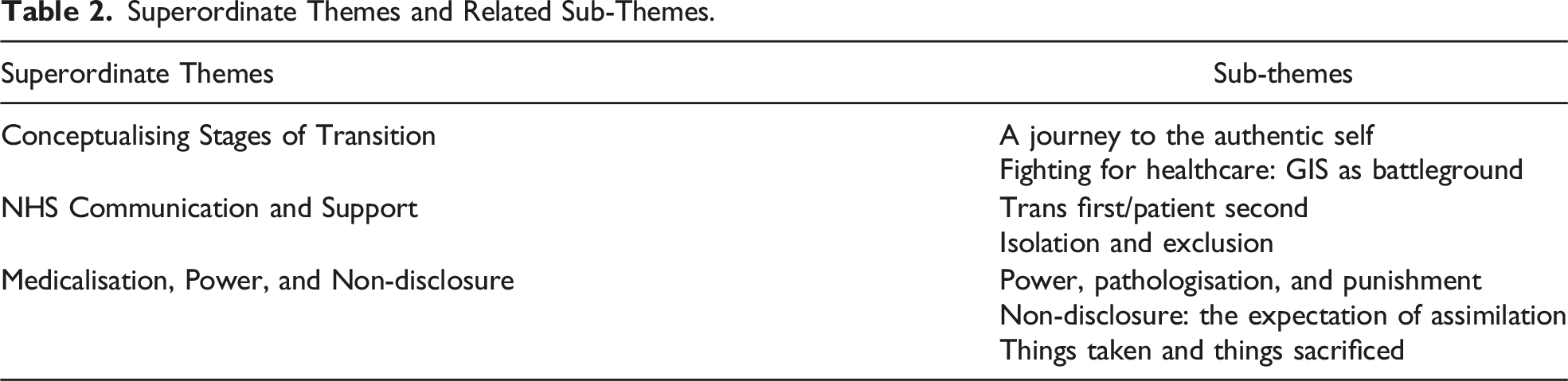
Conceptualising Stages of Transition
Participants described certain necessary revelations in their transition, such as seeking information and experiences of self-discovery. For many, this was followed by coming out to family and friends. Importantly, although these were described as the first ‘stages’ of trans identity development, multiple participants stated that these are also ‘ongoing’ and ‘a life-long process’. Participants also illustrated a parallel process taking place, navigating the health services capable of facilitating their medical transition. This, too, was conceptualised by participants as ‘stages’:
Note the real-time sense-making of the group; the theme of searching (for one’s true self) is introduced by Greg and then elaborated and refined by others (searching for acceptance and for answers). Here, the solitary nature of self-discovery is expanded to incorporate a relational component; Paul’s fear of sharing their trans identity with others is contrasted by Amit’s desire to connect with other trans people.
This interaction brought consensus within the focus group regarding the earliest ‘stages’ of transition. All held that this is a truly personal odyssey, acknowledging that a person’s transition goals, and the resources available to them, will create vastly different experiences. This was mirrored in the interviews; Mike [II] described how he ‘knew [he] would never have the money to go private, so [he] took the standard route of GP and [GIS] and jumping through hoops’. Romeo [II] also acknowledged that personal transition goals are variable, yet are restricted by narrow GIS pathways: I know that for some people, this route just isn’t for them, because maybe they want chest surgery first or whatever, and the gender clinic don’t always let you. But I know the gender clinic told me that this is the best route.
Regardless of their personal choices or desires, every participant contributed to an emerging experiential theme; that they are tasked with convincing GIS of their authenticity: ‘I’d say the first stage is the convincing stage, then admin, then testosterone, then more admin and waiting, and then top surgery’ (Charlie, II). Here, GIS ‘stages’ were not described as helpful, but as arbitrary and intrusive challenges. This theme is further demonstrated by Greg [FG], who evoked striking imagery of fighting one’s way through a videogame: Once you’ve made it past the waiting list then you’re ready to face the first boss: the gender clinic. They’re gonna make you jump through hoops and will ask a million intrusive questions (…) and if you’re lucky then they’re gonna prescribe you hormones. Then maybe two years after that you level up and
Greg’s description of GIS clinicians as a ‘boss’ not only portrays clinicians as a series of challenging enemies to be defeated within a videogame but also characterises them as gatekeepers with the power to obstruct their efforts to reach personal transition goals. The metaphor of GIS access as a battleground was evoked by multiple participants who spoke of sacrifice and defeat. At times, the concept of transition was objectified, described as ‘not theirs to take’ (Romeo, II), or ‘stolen’ from them (Paul, FG). This calls to mind the image of one physically wrestling with the object of transition, with service-users on one side and GIS on the other. Perhaps the tension in this relationship is worsened by the utterly personal nature of transition, juxtaposed with the knowledge that an outsider must become involved and that they have authority to permit or deny you in your journey.
NHS Communication and Support
While wrestling with the proverbial ‘object of transition’, the group reflected on how the roles of clinician and patient were skewed by their status as trans. Amit (FG), Elliot (FG), and Charlie (II) described feeling ‘terrified’ that their GP would refuse to help. These fears, in many cases, were realised; It’s so important when you’re beginning to transition that your GP is on your side, if they’re not then you’re gonna have a hard time.
Mike’s use of the phrase ‘on your side’ again depicts service-user and clinician in opposition to one another and illustrates the importance of having a GP as an ally in their battle for healthcare. This fight would also take the form of educating their GP and advocating for themselves. For some, the fight did not solely concern access to transition-related healthcare but all NHS healthcare. Raj (FG) expanded on how their fear of being denied a referral to GIS led to sacrificing their mental healthcare in order to ensure access to medical transition: I’d just been referred [to GIS] … my mental health wasn’t great, but I didn’t wanna go to the GP for medication for mental health, because then I risk the referral [not] being put through. And so, I thought okay I’ll deal with my mental health problems, but first this referral needs to go through, and that was the priority.
Participants who had accessed NHS mental health services expressed the belief that their transgender identity negatively impacted the care they received. The mood of the focus group became melancholy as they shared their losses. For example, Alex (FG), who was experiencing depression, reported a change in their treatment after notifying their Community Mental Health Team (CMHT) of their trans status, because their case was now seen as more complex. Alex’s experience was reflected in that of other focus group participants:
Repeated failures of this kind undermined the confidence in their care providers, and for many, it became clear that they must ‘fight for every step’ (Amit, FG). Paul’s reference to their past suicide attempt was absorbed into the group’s conversation as easily as any other statement, and there existed an unspoken acceptance of serious trauma as a feature of accessing NHS services as a trans individual.
For the ten participants who sought treatment through the NHS, all reported complaints with the GIS referral and diagnostic process, but specific attention was given to a lack of communication and long waiting times. Waiting times held a unique experiential significance to all ten NHS service-users; Mike (II) and Romeo (II) provided particularly emotionally evocative descriptions: Being on the waiting list takes forever, and [GIS] don’t seem to understand what a big deal it is, how horrific it is. You wait alone for your appointment, there’s no support or information … you’re just left in the dark with no idea.
Like others, Mike and Romeo described feeling isolated and ignored during significant waiting times, with little acknowledgement from services over the seriousness of delay. The darkness and horror of the waiting times is made all the more understandable by the mutual mistrust and apparent resistance they had faced.
In contrast to these narratives of struggle, two participants reflected positively on their referral process to GIS. One participant, Alex (FG), reported that their NHS experience was ‘actually okay’, whereas Charlie (II) sought private medical care when he discovered that waiting times far exceeded NHS guidelines. Although Alex and Charlie did not perceive their experience as negative, neither did they perceive it as wholly positive.
Medicalisation, Power, and Non-disclosure
Participants perceived GIS as adversaries and feared the unilateral power held by their clinician to halt or delay a vitally important process. Referring to their initial experiences with GIS as the ‘convincing’ stages, participants described a reluctance to be authentic due to the perceived risk. In reference to their decision to prioritise their medical transition over their mental health, Raj (FG) reiterated the potential danger of disclosing mental health struggles: ‘[GIS] put you in the position where I’m gonna hide that stuff, because of the risk’. Thus, participants felt obligated to hide their struggles and were left no recourse of seeking help.
Participants described their belief that GIS respond to perceived doubt or uncertainty by delaying or refusing transition-related interventions. Romeo (II), who had been waiting (at the time of interview) for seven years to begin HRT, said: Even if I say the slightest thing, like if I feel a little bit depressed, then they jump on it and they stop the whole process. It’s as if they’re looking for a reason to stop you, or a reason to say you’re doubting yourself, or that they doubt you.
Like Romeo, many participants conceptualised the delaying or halting of transition-related care as a punitive measure. Further, it is clear that they felt as if it was punishment for a personal failure, internalised the blame, and learned to only say what they thought GIS wanted to hear.
This extract illustrates how GIS may play a negative role in identity formation, by introducing doubt where there previously was none or by implying there is a ‘best’ (and thus, a worst) way to transition. Despite Romeo seeing himself as ‘socially’ the same prior to attending GIS as he did after being denied treatment, his experience of being ‘rejected’ by GIS sowed self-doubt, because he implicitly trusted their expertise (‘well, they’re doctors’).
In narratives that mirror Romeo’s, others described feeling discouraged as their lived experiences were ignored and they felt pressured by GIS to ‘perform’ (Amit, Francis, and Elliot; FG; Mike; II) and ‘jump through hoops’ (Terry, Paul, and Greg; FG; Charlie and Mike; II). Non-binary individuals, such as Elliot (FG) and Amit (FG), deliberated over whether to disclose their non-binary identity: “They might withhold treatment, it’s a very real fear … and so when I went to my assessment I was like, do I disclose that I’m non-binary?” (Amit), whilst binary and non-binary individuals alike, such as Mike (II) and Raj (FG), discussed feeling forced to “assimilate” into a cis-normative society. These experiences of invalidation, in addition to pressure to conform to clinical expectations, intensified their existing distress.
Participants frequently discussed the power exerted over them by GIS; Amit (FG) attributed this power imbalance as the reason they could not be truly authentic: ‘[GIS are] considered experts, so they do hold the power, and so it means you can’t tell them certain things’. Furthermore, some participants voiced the opinion that they felt powerless in their own transition and were ‘stuck in the system’ (Francis, FG). This lack of control over their own situation was felt so profoundly within the focus group that it provoked a passionate discussion of the necessity for, and the costs of, fighting for your rights.
The group context seemed to expand the participants’ sense of struggle beyond themselves, and it was transformed into a burden shared by those in the room, and the transgender community at large, who are allied in the same fight. There was a sense that an element of sacrifice was inherent when seeking transition-related healthcare, and it is notable that the necessity of sacrifice was never questioned. Most poignantly, the feeling of determination and hope in the room was palpable, and this is in contrast to Romeo’s (II) account in which he evoked a feeling of despair and isolation. This contrast is exemplified by the narrative of things ‘sacrificed’ among the focus group versus Romeo’s narrative of things ‘taken’; the first implying an element of choice or agency, which is not apparent in Romeo’s descriptions.
Discussion
This article contributes to the growing field of transgender health by using IPA methodology (Smith et al., 2009). The use of IPA enabled us to gain a unique insight into the role healthcare services play in the identity development and meaning-making activities of transmasculine individuals in the UK. IPA methodology allowed us to engage with multiple levels of analysis, such as linguistic choices, emotions, and beliefs underlying the statements of participants, whilst maintaining an idiographic focus, which provided an advantage over alternative qualitative methods such as thematic analysis, which would not have enabled the full interpretative account that is provided. The use of a focus group appeared to generate a sense of camaraderie between participants, and whilst this may have affected the tone and content of accounts provided, it also encouraged those present to challenge the views of themselves and others in a supportive environment, resulting in rich and novel data of benefit to this study.
The stages of transition outlined by GIS as an appropriate guide to a successful transition were rejected by our participants, and instead were viewed as a method of gatekeeping access to medical treatment. It emerged that one’s process of transition should be guided by introspection, information-seeking, and flexibility; this supports the arguments made by Kuper et al. (2018), that current models do not accurately account for the fluidity and complexity of lived experiences.
Our findings demonstrate how identity formation can be influenced by medical services. The NHS pathway was criticised for its one-size-fits-all approach; rather than being supported through their transition, participants described being ‘stuck in the system’. Participants emphasised the importance of information-seeking; however, the same participants also believed that GIS discourage and punish this crucial activity. This can result in service-users receiving incorrect information from unverified sources or hiding questions and doubts that could be resolved through discussions with clinicians. This is reflected in previous IPA research; Harrison et al. (2020) reported similar findings whereby participants felt pressured to ‘prove’ their identity to GIS. Our results expand on this by demonstrating the ‘sacrifice’ and ‘loss’ transmasculine people endure throughout this process. The negative impacts on service-users have been explored by Lehmann et al. (2021), specifically in relation to ‘impression management’ (i.e. presenting oneself as the most compliant and expected version of a trans patient). Lehmann and colleagues argue that continuous impression management can lead to exhaustion and burnout, and causes service-users to feel they cannot disclose concerns about their mental wellbeing. Often, GIS appointments take place after years of waiting following the initial referral, which itself may follow fractious interactions with GPs. The intense pressure to ‘prove’ their identity is therefore understandable.
Our analysis revealed that none of the participants believed that there was any superior manner of transition, nor one singular goal shared by transmasculine people who are seeking medical transition. However, the medical model that is utilised by the NHS is underpinned by the problematic ontological assumption that the goal of transitioning for all trans people is to become cisgender (McKinney, 2021). Often, this leads to unmet expectations on behalf of both service-users and healthcare providers (Meyer et al., 2020), and may contribute to the severe lack of trust in GIS evidenced in our findings. These unmet expectations led some to question the assumption that GIS would act in their best interests, and transformed institutional failures to personal invalidation and neglect.
Being transgender negatively impacted participants’ access to all NHS services. It was a major source of anxiety that their GP would be unsupportive or ill-informed. This finding supports Heng et al.’s (2018) systematic review, which found that a lack of healthcare provider knowledge was a frequent experience for transgender people. Furthermore, Taylor’s (2013) reflections on the necessity of self-advocacy and health literacy were a common theme in our findings. A recent study (Willis et al., 2020) explored this further and found that trans adults seeking medical interventions are positioned as reluctant educators for their GP and reiterates that self-advocacy is a necessary and stressful aspect of seeking transition-related healthcare.
Power inequalities inherent in the rigid GIS diagnostic framework were apparent in our analysis; feeling powerless and lacking in autonomy was a common experience. Those who did not fit the expected male/female binary felt it necessary to adopt a binary identity to access medical transition; these findings lend support to Lykens et al. (2018) who found that non-binary individuals sometimes ‘borrow’ a binary identity to receive healthcare. Our participants expressed frustration with the gatekeeping role of healthcare providers – such gatekeeping has been described as ‘unethical’ and ‘dehumanising’ in literature (Ashley, 2019). A striking finding was the shared experience of ‘sacrifice’ when interacting with GIS. To adhere to stereotypes and experience fewer barriers was to sacrifice authenticity, but to present authentically, thereby forcing GIS to acknowledge the diversity of trans experiences, was to sacrifice timely access to necessary interventions. In response to these findings, and in line with extant literature which communicates mass dissatisfaction with the current diagnostic model (Harrison et al., 2020; Willis et al., 2020), we strongly advocate for a transition to the Informed Consent Model (Schulz, 2018).
Such a change in protocol would mitigate many barriers to transition-related healthcare. It would empower service-users to make informed choices in collaboration with clinicians and would place the UK at the forefront of ethical transgender healthcare. Studies indicate that ICM services are currently growing in popularity (Ashley et al., 2021; Reisner et al., 2015b) and demonstrate that ICM is associated with high patient satisfaction (Spanos et al., 2021). Furthermore, service-user involvement, particularly for minority groups, is fundamental to providing patient-centred healthcare (Eyssel et al., 2017).
We propose the following immediate practical improvements. Increased support for service-users during waiting periods is necessary. This support may include transgender-specific counselling or psychotherapy as was recommended by Harrison et al. (2020) or might consist of more frequent contact, in which transparency about the waiting times is appropriately communicated to service-users, so they don’t feel ‘left in the dark’. Furthermore, an NHS-wide commitment to LGBTQ-specific training is recommended to improve access to all services for transgender people. Additionally, measures to facilitate multi-disciplinary working are recommended; participants frequently discussed the difficulty of accessing mental health services and GIS simultaneously. Dhejne et al. (2016) state that those who attend GIS have higher psychopathological symptoms; therefore, streamlining multi-disciplinary working in this context is a pressing issue.
It is our hope that by understanding how trans individuals conceptualise ‘stages of transition’, future research will be better situated to examine experiences that take place within them and may enable the provision of tailored support. IPA focuses not on the objective circumstances of a person, but their experiences and views. As such, criticisms of the inner workings of the NHS are here described through the lens of the patient, and accounts of these processes may, of course, differ from that of care providers. As such, further research could examine the subjective experiences of GIS clinicians to advance our understanding of how unmet expectations arise, and researchers may also wish to convene international consensus development conferences, to learn from clinics that provide the ICM and examine experiences of trans healthcare providers globally. Furthermore, through participatory methods, researchers could explore opportunities to foster therapeutic relationships between service-users and clinicians. The findings of this research are limited in that all participants were seeking medical interventions, and it would therefore be useful to conduct an idiographic inquiry of trans identity development from the perspective of individuals who do not wish to medically transition. We also recognise that the theoretical generalisability of this research is limited by the homogenous nature of the sample, and their views and experiences may not apply to other trans populations.
In conclusion, in light of the myriad barriers that emerged from our analysis, adoption of the ICM would, we suggest, be evidence of a renewed commitment to engage more equitably and effectively with a patient population which has, our participants’ experiences suggest, been poorly served.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was granted by the University Psychology Research Ethics Committee (REF: FHS128).
Data Availability
Two authors (TJM and KR) conducted each step of data analysis.