
Abstract
Cancer diagnosis and treatment can be physically arduous, disrupting patients’ social and work lives. Understanding the extent of these problems is key to addressing patients’ needs, but specific psychosocial challenges have not yet been well studied in resource-limited settings. A qualitative study was conducted in the capital and two regions of Ethiopia with the aim of exploring psychosocial challenges among cancer patients. A total of 14 in-depth interviews (IDIs) and 16 focus group discussions (FGDs) were done with cancer patients, health professionals, community representatives, and religious leaders. Four separate interview guides were used to facilitate the interviews and discussions. All transcribed documents, field notes, and reflexive memos were entered into NVivo 12 software, and deductive thematic analysis using the social-ecological model was applied to summarize the main findings. At an individual level, emotional distress, suicidal risk, denial, and refusal of treatment were identified immediately after diagnosis while hopelessness, feeling depressed, and fear of death were commonly reported psychosocial challenges during the course of treatment. Involvement of family members in major treatment decisions was recognized at an interpersonal level. Our result also revealed that cancer patients had strong social support from family members and close friends. In the community, traditional medicine and religious rituals were considered an alternative treatment for cancer. The findings indicate that counselling and psychoeducation are crucial for cancer patients, family members, and close friends. Awareness creation programmes should be delivered through collaboration with religious leaders and traditional healers.
Introduction
A cancer diagnosis may threaten one’s physical, emotional, and social existence (Emory Winship Cancer Institute, 2019; Gorman, 2003). Psychosocial challenges are the dynamic interactions among the physical, emotional, social, and cultural factors that come into play during the cancer trajectory (Merighi, 2016). The physical changes that arise from cancer or its treatment are the most common causes of psychological disorders among cancer patients. For instance, common chemotherapy side effects, such as hair loss, fatigue, and weight changes, have a huge psychological impact on cancer patients (Nikbakhsh et al., 2014; Rosa & Ferrell, 2023; Zainal et al., 2013). The need to adapt to hair loss, cognitive issues, and fluctuations in weight may have unexpected consequences on body image and self-perception (Emory Winship Cancer Institute, 2019; Fingeret et al., 2014). In particular, the type of cancers that require surgical removal of body parts may lead to disruptions in self-perception, appearance, physical ability, social relationships, and cognition (Brierley et al., 2019; Fingeret et al., 2014; Hubbeling et al., 2018).
In addition to its physical implications, some cancer treatments affect cognitive functioning: thinking, memory, word retrieval, problem-solving, executive function, and multitasking (Merighi, 2016). For this reason, many people living with cancer lose their independence and autonomy, as cognitive functioning may decrease over time and cancer affects every aspect of daily life. Therefore, they are forced to rely on family, friends, and health care professionals to perform everyday tasks (Head & Iannarino, 2019; Merighi, 2016; Wang et al., 2015).
Moreover, symptoms of depression, anxiety, and hopelessness are frequent among patients with cancer (Doherty et al., 2019). More than one-third of cancer patients are emotionally distressed and about one in five cancer patients express the need for psychosocial support (Bergerot et al., 2016). Anxiety is one of the leading psychological challenges associated with cancer, and all cancer patients undergo a level of anxiety at some point in their disease trajectory. This level of concern increases as patients identify how severe their condition is with the stage of presentation and how the treatment progresses (Saleh Baqutayan, 2012). Depression is another common disabling disorder that affects approximately 15%–25% of cancer patients (Nikbakhsh et al., 2014; Wondimagegnehu et al., 2019; Zainal et al., 2013).
The overall burden, severity, and type of psychological disorders vary hugely depending on the stage of cancer, type of treatment received, duration and cost of treatment, and availability of psychosocial support (Doherty et al., 2019; Emory Winship Cancer Institute, 2019; Merighi, 2016). The cancer site also plays a major role in the distinct challenges confronted by cancer patients, reflected by isolation, stigmatization, and loss of autonomy (Gorman, 2003; Merighi, 2016; Zebrack et al., 2007). Some studies identified that breast and cervical cancer patients have a higher prevalence and a severe form of these disorders. For instance, symptomatic anxiety and depression among breast cancer patients were reported as high as 32% and 28%, respectively, while among patients with other types of cancer (such as esophageal, colorectal, and thyroid), it was ranging between 3% and 15% for both disorders (Alemayehu et al., 2018; Nikbakhsh et al., 2014).
Not only clinical factors but also external environmental factors such as geographic setting, sociocultural context, and socio-economic status of the patients play a major role in the variation across the continents (Doherty et al., 2019; Grassi & Watson, 2012). Particularly in low- and middle-income countries (LMICs), the majority of cancer patients are diagnosed at an advanced stage of the disease, which contributes to the high mortality rate and poor prognosis of the disease (Martie et al., 2018; World Health Organization [WHO], 2018). According to a systematic review in sub-Saharan Africa, the percentage of patients diagnosed at Stage IV cancer ranges from 4% to 70% (Jedy-Agba et al., 2016). This may have direct implications for the type and severity of psychosocial challenges faced by cancer patients in those settings. However, the number of studies conducted in LMICs is very minimal, and the available evidence suggests that there is a difference in the psychosocial challenges and needs among cancer patients in Western countries and LMICs (Herce et al., 2014; Hubbeling et al., 2018; Travado et al., 2017). This variation might be due to differences in medical decision-making, pressure for collusion, extreme poverty, and cultural expectations about emotional and spiritual responses to severe illness (Ahmadi et al., 2019; Cain et al., 2018). In addition, differences in levels of education, occupation, values, and religious beliefs among low-income populations have been observed to influence patients’ greatest fears and concerns at the end of life (Elsner et al., 2012).
Understanding the cultural, social, and emotional experiences in LMICs is critical for improving the psychosocial and spiritual aspects of palliative care; however, specific psychosocial challenges have not been well studied in these settings, particularly in Ethiopia. Previous studies of cancer in Ethiopia were more quantitative, focusing on stage of diagnosis and survival (Abebe & Abebe, 2017; Eber-Schulz et al., 2018; Gizaw et al., 2017), awareness of cancer (Aweke et al., 2017; Chaka et al., 2018), health-seeking behaviour (Habtu et al., 2018), and screening service uptake (Geremew et al., 2018). However, the psychosocial challenges experienced by cancer patients were not well explored in a qualitative study looking at the social, cultural, and religious structure of the community. Therefore, the aim of this study is to explore the psychosocial challenges among cancer patients in Ethiopia, an LMIC with very limited structures and resources to support the identification of and clinical response to cancer patients’ psychosocial needs. The social-ecological model was used to explore the multiple levels of psychosocial challenges. This model is a theory-based framework emphasizing the interactive effects of personal and environmental factors at individual, interpersonal, organizational, community, and public policy level (Bronfenbrenner, 1977; Bronfenbrenner & Ceci, 1994). Hence, realizing the magnitude and depth of unique psychosocial challenges from different sociocultural perspectives may have paramount importance. We believe that the current study will generate evidence on how to address these specific needs of cancer patients and can be used as an input for designing context-based, effective, and applicable supportive care in resource-limited settings.
Methods
Study Design and Place
We conducted a qualitative study in four rural and two urban hospitals located in Addis Ababa, Oromia, and the Southern Nations, Nationalities, and Peoples’ Region (SNNPR) of Ethiopia. These four rural hospitals (St. Lukas Catholic Hospital, Negist Elleni Mohammed Referral Hospital, Butajira General Hospital, and Assela University Teaching and Referral Hospital) and two urban hospitals (Bete Zata Hospital and Tikur Anbessa Specialized Hospitals) were purposively selected.
Study Participants and Sample Size
Focus group discussions (FGDs) were conducted with cancer patients, health professionals, community representatives, and religious leaders in each study site, totalling 16 FGDs. On average, five to nine participants were included in each FGD, amounting to 121 participants: 31 from Butajira, 28 from Hossana, 27 from Weliso, 26 from Assela, and 9 from Addis Ababa city. Cancer patients above 18 years of age and on follow-up during the data collection period were included in the FGDs. In addition, 14 in-depth interviews (IDIs) were conducted with six cancer patients, five health professionals, and three patient relatives. Purposive sampling and theoretical saturation techniques were used and a maximum variation of participants was achieved by recruiting patients with different types of cancer and health professionals from various specialties. An attempt was also made to achieve diverse perspectives by recruiting participants from different religious denominations (Pariona, 2017) and by considering the community role, place of residence, age, and gender of the participants.
Data Collection and Tools
Four separate interview guides (for IDI/FGDs conducted with cancer patients, health professionals, community representatives, and religious leaders) were prepared based on the study objective. We purposively used both IDI and FGD data collection techniques in order to complement and triangulate our findings. The FGDs enabled us to explore the overall psychosocial challenges observed/recognized at community and organizational levels while the IDIs were very crucial to understand the situation from patients’ perspective through freely discussing any psychosocial challenges including sensitive issues.
Questions about any form of psychosocial challenge that cancer patients face throughout the disease trajectory were included. We asked whether the diagnosis or the medical treatment affected their social, financial, spiritual, and family life. Questions about personal feelings, challenges in relation to their interaction with community members, and the presence of stigma or discrimination were included in the interview guide. We also asked about the presence and utilization of alternative treatment options, such as traditional healers and religious places in their village. In addition, religious leaders were asked if cancer patients often visit their institution, how long they stay, what specific needs they have, and what kind of care or support do they offer to cancer patients. A principal investigator and research assistant conducted all the FGDs and IDIs. On average, IDIs were held for 21–47 min and FGDs took 65–102 min. The FGDs and IDIs with health professionals, cancer patients, and relatives were held in their respective hospitals while FGDs with community representatives and religious leaders were done in the compound of kebele offices (the smallest administrative unit in Ethiopia). After conducting the preliminary analysis and summarizing the main findings, the research team decided to use the social-ecological model (Bronfenbrenner, 1977; Bronfenbrenner & Ceci, 1994) to deductively explore the psychosocial challenges at individual, interpersonal, and community/organizational levels. This model is a theory-based framework for understanding the multifaceted and interactive effects of individual, interpersonal, and community/organizational factors that determine behaviours and for identifying behavioural and organizational leverage points and intermediaries for health promotion within organizations (Akinyemiju et al., 2022; Bronfenbrenner & Ceci, 1994). Daily debriefings were held on emerging thematic areas and the data collection continued until we reached the theoretical saturation level particularly through comparing and contrasting emerging ideas from each participant categories in the different study sites. All the interviews were audio-recorded, and notes were taken during the interviews and discussions. Subsequently, all recorded interviews were transcribed and translated verbatim after repeatedly listening to the recorded audios.
Data Analysis Procedures
Data analysis started in the field while conducting the first nine IDIs in Addis Ababa. Based on the daily debriefing held among the research team, it was possible to identify emerging thematic areas that require further exploration. All transcribed documents, field notes, and reflexive memos were entered into NVivo 12 software. A principal investigator and research assistant coded each document line by line, and deductive thematic analysis (Bingham & Witkowsky, 2022; Caulfield, 2019) was used to categorize and explain the emerging thematic areas under each level in the social-ecological framework. At the beginning, sentences of importance were highlighted and divided into meaning units. Then, the meaning units were condensed and labelled with short codes; all codes were compared to identify similarities and differences. Connections between codes were searched and categories were developed based on the codes’ manifest content. As we recruited participants from various categories, they may look at the situation from different perspectives, depending on their age, type of cancer, profession, role in the community, and so on; therefore, we attempted to check similarities and differences in the emerging categories across these subgroups. Finally, emerging categories and concepts identified at individual, interpersonal, organizational, and community levels in the social-ecological model were constantly compared, tested, and revised to be fitted in their respective themes and sub-themes. At the individual level, we identified various psychosocial challenges experienced by cancer patients and expressed at different phases of the disease trajectory. Therefore, we further subcategorized into two sub-themes, whereas we merged the identified sub-themes under organizational and community levels into one theme. The findings were discussed, re-categorized, and modified to ensure reliability and better explanation. Disagreements were discussed until consensus was reached.
Ethics
Ethical clearance of this study was obtained, and written informed consent was taken from all participants. Confidentiality of the data was maintained.
Results
Characteristics of Participants Involved in the IDIs and FGDs in Five Towns in Ethiopia, 2019.
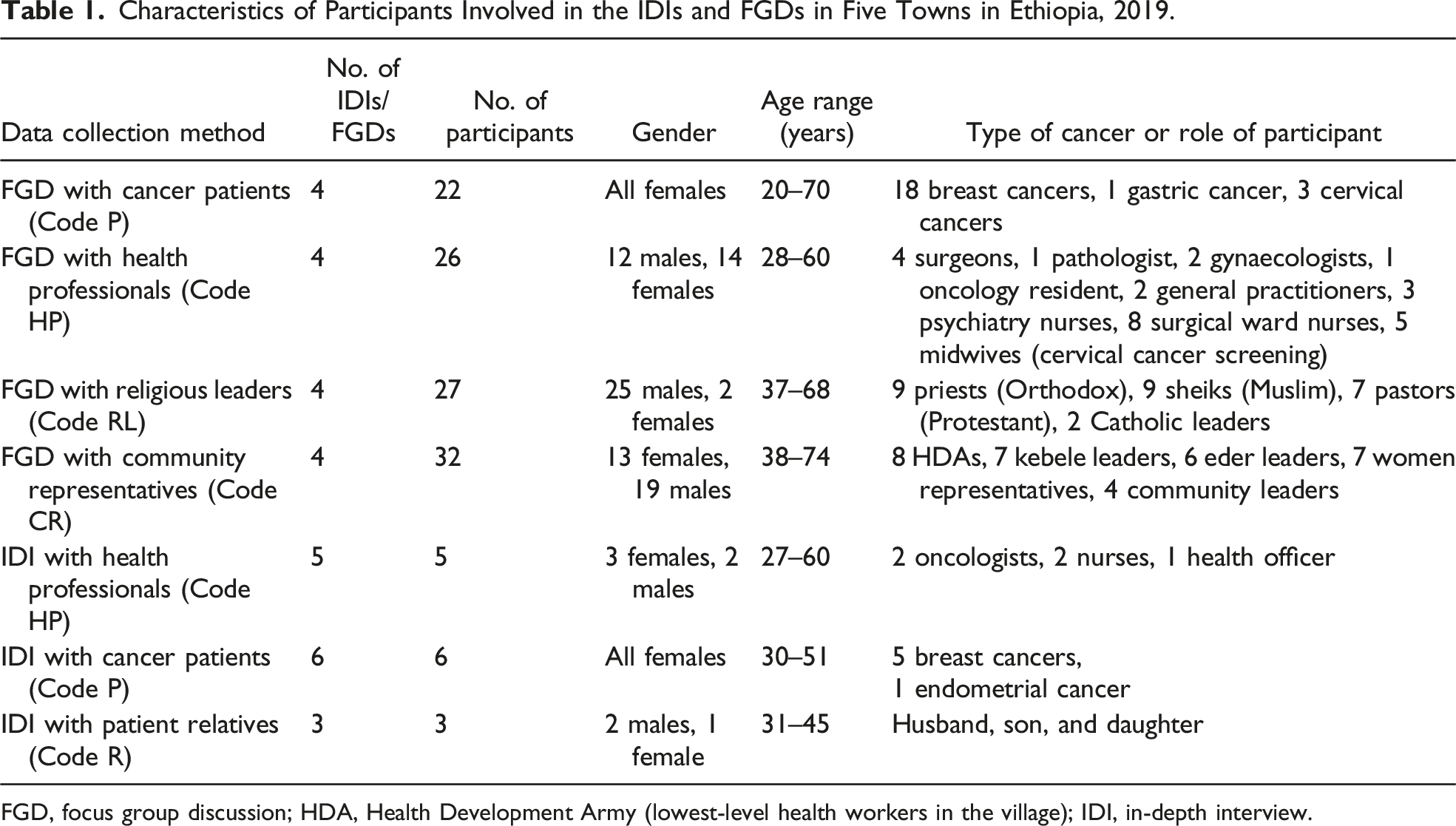
FGD, focus group discussion; HDA, Health Development Army (lowest-level health workers in the village); IDI, in-depth interview.
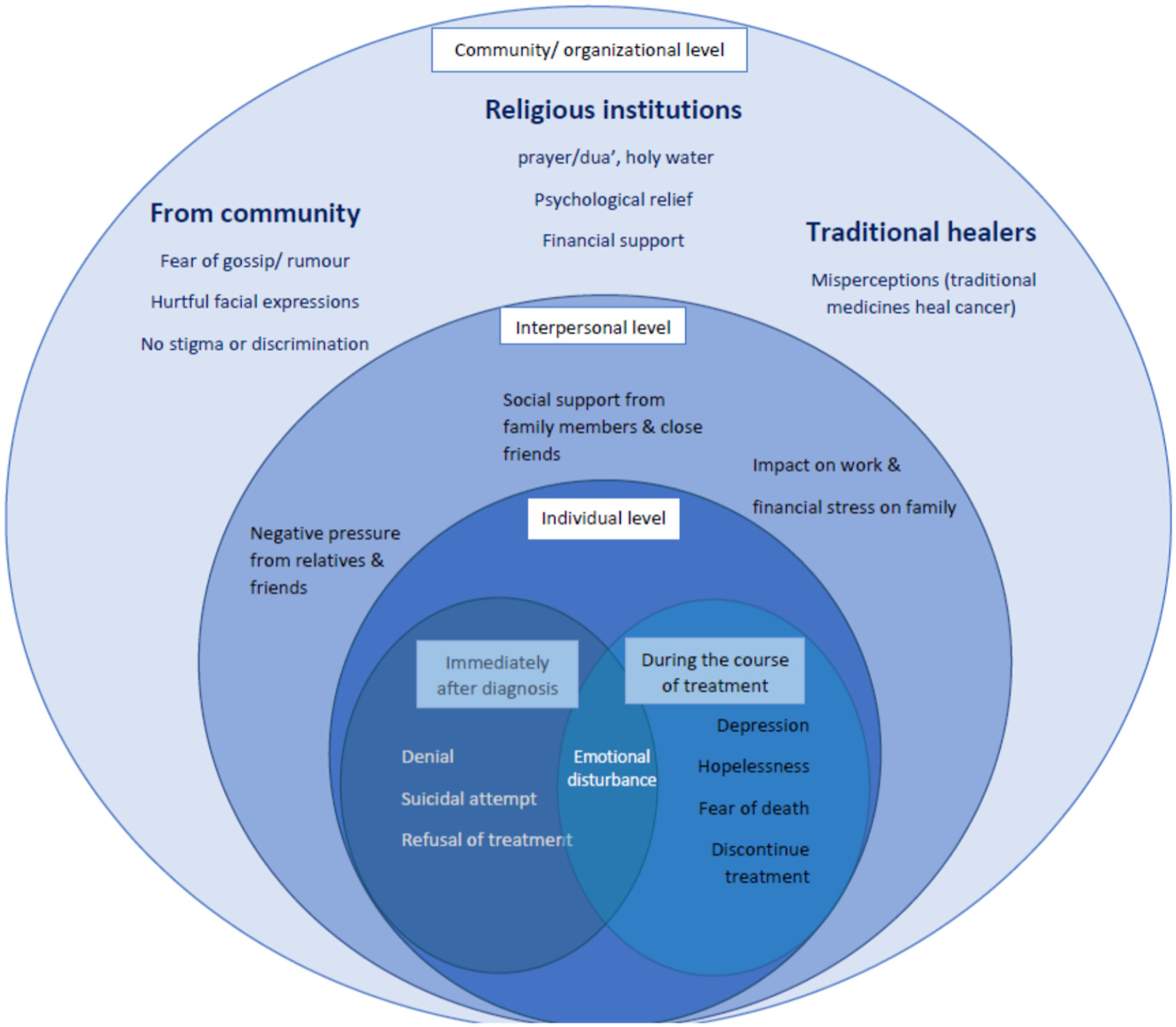
The social-ecological model of psychosocial problems among cancer patients in Ethiopia.
Theme 1: Psychosocial Challenges at Individual Level
This theme describes the psychosocial problems that each cancer patient feels about themselves, influenced by the knowledge, attitude, perception, and sociodemographic characteristics of the patient. We further subcategorized these problems into two sub-themes: (a) challenges immediately after diagnosis and (b) challenges during the course of treatment.
Sub-Theme I: Immediately After Diagnosis
(a) Emotional distress:
Our participants mentioned that many cancer patients became very emotional when they were first informed as having cancer. This is related to their perception of the disease in a way that many patients directly associate cancer with death. Furthermore, many cancer patients, especially breast cancer patients, did not expect to have a serious illness because most of the time they presented with a small, painless lump. They reported being shocked by the news, as illustrated by the following quote: The name by itself is very scary … I was shocked, cried … I felt so bad ummm … different feelings at the same time. (IDI-P01: age 36 years, BC patient, AA) (b) Suicidal risk:
Some of the patients who had received a diagnosis of breast cancer reported attempting suicide after receiving the news of their diagnosis, as demonstrated by the following quotes: It really damages your mind when you are told as having breast cancer for the first time … my brother was with me and I just ran away from him and tried to commit suicide. I wanted to be hit by a car. (IDI-P04: age 35, BC patient, AA) … we were forced to hide sharp materials from her since she wanted to kill herself. We were even considering it as evil spirit. (FGD-CR06: community representative, Hossana) (c) Denial:
Denial was one of the major problems observed among cancer patients at the time of diagnosis. Both health professionals and the patients reported that it is very difficult for the majority of cancer patients to accept the diagnosis immediately. For this reason, those patients who were diagnosed in a government hospital went to private clinics and those who were diagnosed in rural areas usually travelled to Addis Ababa or a nearby city in order to repeat the tests and confirm the diagnosis. Since I didn’t believe the result, I requested the doctor to give me another prescription to repeat the test. Then, the result was the same. (IDI-P04: age 35, BC patient, AA)
Denial was a very common problem not only at the time of diagnosis but even during the course of treatment. The health professionals mentioned that some patients, especially those with advanced cancer, still remained in a fluctuating state of denial even after they were convinced and started the treatment. Health professionals reported their observation in the following quote: They are in denial and do not want to hear any negative outcome or progress. Some patients want to go to private facility because they want to listen something promising. (IDI-HP04: nurse, government, AA) (d) Refusal of treatment:
Surgeons who were interviewed reported that many cancer patients refused surgical treatments specifically for total removal of the breast (mastectomy) because it is the most common surgical procedure offered for breast cancer patients in Ethiopia. … when they hear the word cancer, the first thing which comes into their mind is death. So they immediately want to go home refusing surgery. (FGD-HP04: surgeon, Hossana)
Sub-Theme II: During the Course of Treatment
(a) Emotional disturbance:
At the time of diagnosis, cancer patients also reported that the treatment and its side effects brought emotional instabilities that might have serious psychological implications in their life, as illustrated by the following quote: Umm ... it’s hard … you feel so tired, you don’t have hair, and your emotion is fluctuating. Even sometimes, you become irritable to those people who are taking care of you. Crying … (IDI-P01: age 36, BC patient, AA) (b) Hopelessness, feeling depressed, and fear of death:
In this study, the other most commonly mentioned psychological problem among cancer patients was feeling sad/depressed. As the health professionals reported, many cancer patients feel depressed from the date of diagnosis and while receiving treatment. These patients perceive that the disease will not be cured and assume they will die immediately. The hopelessness observed is demonstrated in the following quote: Cancer kills the hope of living both the patient and their family. Even HIV patients do not lose hope as cancer patients do. Because they know that they can survive long taking the ART drugs. (FGD-CR02: community representative, Hossana) (c) Non-adherence to treatment:
Our participants reported that many cancer patients discontinue treatment because of financial constraints (transport cost, medication, accommodation, etc.). Most cancer patients in peripheral sites needed to travel to Addis Ababa or nearby cities in order to obtain treatment. Another reason was that some patients assumed that the disease was cured after having surgery and the wound was healed without receiving systemic treatment. On the other hand, there were patients who expected a fast recovery after taking the medication, and when they did not observe any improvement in their health, they became discouraged and searched for alternatives such as traditional medicines. Giving late appointments and a lack of adequate information were other reasons for discontinuation of treatment among cancer patients. The following quote illustrates this: Usually, patients go to the health center then, they will be referred to hospital and again to Addis Ababa. In between, the patients spend a lot of money without getting any treatment and they suffer a lot. (FGD-CR08: HDA, Hossana)
Theme 2: Psychosocial Challenges at Interpersonal Level
In this study, we observed the relationship between cancer patients and their family members and close friends in two directions: from family members and close friends to the cancer patient (both positive and negative sides); and how the disease affected family members and also the work and social life of the cancer patient.
Sub-Theme I: Social Support From Family Members and Close Friends to Cancer Patients
Despite several psychosocial challenges identified in this study, we identified that almost all the cancer patients received strong social support from family members and close friends, starting from diagnosis until the end of treatment, as illustrated by the following quotes: My families are very supportive. They sacrificed and invested a lot for my treatment. (FGD-P02: age 33, BC patient, Woliso) My children, my husband and all my neighbors encourage and support me. (FGD-P02: age 50, BC patient, Hossana)
It is revealed that there is a strong social support in the community even after the patients died. Health professionals we interviewed stated that cancer patients often receive support from family members and the general community. Diseases like cancer, HIV, cardiac and kidney illnesses are chronic debilitating diseases which we have to start the supportive care immediately after diagnosis. The level of care continues even after the patient dies, which includes supporting the family after their loss. This is called Bereavement stage. The good thing in our country, our community has a very good social structure. In Ethiopia, people support each other for 3 or more days after death. People still go there for support even after 7 or 8 days especially relatives from far stay with them. Regarding cancer, patients usually feel better emotionally when being exposed to religious urge. (IDI-HP01: oncologist, AA)
In addition, the importance of psychosocial support was acknowledged by most of our participants and suggested different mechanisms on how best to involve different stakeholders and capitalize on the already existing social structure and health care system. For instance, community representatives from Butajira stated as follows: Counseling and education about cancer should be given by health care providers, while the edir (small supporting social structure) and religious leaders will mobilize the people to participate as the community strictly abide to edir rules and will not be absent. It will also be good if religious leaders are involved because they have great acceptance and respect by the people. In collaboration with the kebele (small administration unit) and edir leaders and with that of health extension workers and health development armies. (FGD-CR03: community representative, Butajira) I think psyhcosocial support should be part of the care. Intensive counseling plus bringing similar cases together and talking about the disease is very useful. We need to arrange a room for such kind of session to learn from each other, as it will be better than given by the health care provider. So psychosocial service is important especially for cancer patients, it is very essential. (FGD-HP07, health officer, Butajira)
Sub-Theme II: Impact of the Disease on Family Members and the Work/Social Life of Patients
All the participants, including patients’ relatives, health professionals, and community representatives, reported that the disease had a negative impact on the family members and the work and social life of the patients, as demonstrated by the following quotes: …. she was a merchant and very active to do any kind of work. But as you can see her now, she is very weak and someone needs to take care of her at home. (IDI-R01: son, Assela) … all the family members will be negatively affected. Cancer makes the whole family very poor and to be dependent on others. (FGD-CR02: community representative, Hossana)
Theme 3: Psychosocial Challenges at the Community/Organizational Level
This theme encompasses the existing external factors that had a positive or negative influence on the psychosocial health of cancer patients in the community. These factors include community perceptions, norms/beliefs, and cultural/religious practices; therefore, we categorized them into three levels: (i) from the general community; (ii) religious institutions; and (iii) traditional treatment.
Sub-Theme I: From the Community
Concerning stigma and discrimination, we found contradictory findings reflecting the presence of self-stigma due to negative pressures coming from the community. Even though the community members do not instantly stigmatize or discriminate cancer patients, many patients preferred to isolate themselves from different social gatherings and did not want to talk about their disease to anyone other than their family members and close friends, as illustrated by the following quote: To tell you the truth, it’s very difficult to talk about this issue in our community. Nobody knows that I have cancer except my family and few friends. I don’t want to talk about it. Because people’s reaction is psychologically touching. So, I don’t want to be emotionally disturbed. The society is very challenging and I need to live carefully. (FGD-P05: age 33, BC patient, Waliso)
In this study, we tried to explore the reasons why patients want to hide their diagnosis and isolate themselves from the community. Among the several reasons they mentioned, fear of rumour or gossip and fear of being very emotional were the most commonly mentioned reasons. In some cases, the attendants were the ones who forced cancer patients to be isolated or not to actively engage in social gatherings due to the sickness itself and the weariness of such events. Our participants reported that community members assume that all cancer patients will die immediately and they often show them pity when sharing their sadness. In addition, some patients stated that they feel very emotional when people talk about their disease and whenever someone comes to their house to visit them. The following quotes support these findings: People usually talk behind your back and gossip each other when they see you from far. I feel so bad whenever people act like this. They always remind me my illness. (FGD: P02, age 27, BC patient, Waliso) Our community assume that cancer patients will die immediately. So, I don’t want people to show me pity face and say “emtse.” I don’t want that; it reminds me as I will die soon. (IDI-P01: age 36, BC patient, AA)
In contrast, our results revealed that community members believe that cancer will not be transmitted from person to person despite their low awareness level about the disease. Thus, stigma and discrimination towards cancer patients did not emerge as one of the psychosocial challenges in the community, and the health professionals also commented that they never encountered this kind of complaint from their patients. We feel so sad for cancer patients and there is no stigma and discrimination on these patients. We have never seen such kind of thing until now. (FGD-CR02: kebele leader, Butajira) Here our community is integrated by a number of social activities. The society provides support for patients, do not discriminate or stigmatize them. However the patients usually hide their problem and they do not want to talk or have contact with other person. (FGD-RL: priest, Butajira)
Sub-Theme II: Religious Institutions
In this study, we discovered that there were different religious places that provide spiritual support for cancer patients in the community. Many cancer patients practice their own religious rituals, such as praying, dua (prayer in the Muslim community), and drinking holy water. I can say almost all cancer patients come to our monasteries and historical religious places especially for holy water. Umm … there are patients who are totally cured and there are also others who passed away in those places. This depends on the strength of their faith. (FGD-RL08: priest, Hossana)
Among the several reasons why cancer patients visited religious places, cost and extended duration of medical treatment and pressure from community members were identified. However, the main reason was due to the strong perception in the community: people believed that cancer is a dangerous disease that requires God’s/Allah’s intervention in order to survive after being diagnosed with the disease. Therefore, many patients visited those places to be cured from the disease and gain psychological relief. Most of the time cancer patients come to our church for three main reasons, first for prayer (to be healed), second for financial support, and third to get psychological relief since most of them are hopeless. (FGD-RL06: pastor, Butajira)
Our results also identified that many cancer patients refused or discontinued medical treatment and stayed in religious places for an extended duration. Afterwards, they returned back to the health facilities with complications and at an advanced stage of the disease in which there was no option to provide curative treatment other than giving supportive care. Some people prefer to visit other places like religious places. I personally met many patients who refused the treatment and they returned back after the disease is metastasized. (IDI-HP02: oncologist, AA)
Sub-Theme III: Traditional Healers
(a) Community perception:
The community believes that traditional medicines can heal any lumps/tumours. They assume that local herbal treatments applied on a swelling can help to burst the wound and dry it immediately. In addition, the community perceives that cancer cannot be cured by medical treatment. For these reasons, there are several herbalists/traditional healers in the community that provide herbal medicines for cancer and other chronic illnesses. The community believe that cancer cannot be cured by medical treatment. So, people always advise us to take her to a herbalist. (IDI-R02: husband, Assela) (b) Practice:
Some patients reported that they took traditional medicine either before coming to the health facility or even after they started the medical treatment. Some of these patients stated that they do not believe that traditional medicine can cure cancer, but they tried these treatments because of a lack of other alternatives and because of pressure from the community. On the other hand, few patients believed that traditional medicine could totally cure cancer and even shared their experience. Sister told me as I have to take the tablet for 5 yrs. But I took some herbal medicine in between and I am fine now. (FGD-P05: age 44, BC patient, Butajira)
Discussion
This study revealed that cancer patients face several unique psychosocial challenges at different stages of the disease trajectory. These challenges occur at individual and interpersonal levels, as well as in the relationship with communities and institutional systems of care. Immediately after diagnosis, many cancer patients expressed shock, fear, and even attempted suicide when they were informed that they had cancer.
A cancer diagnosis can create a threat to one’s general sense of security and orderliness in life (Gorman, 2003). Even for early-stage treatable cancers, many people retain deep-seated fears that any cancer represents pain, suffering, and death. The emotional disturbance is highly associated with the awareness within the community, which is why it is important to differentiate and understand the prognosis of the different types of cancer. In our study, the majority of participants were breast cancer patients, with some diagnosed at an early stage of the disease. However, all of them were extremely shocked at the time of diagnosis. This might be because of lack of adequate knowledge and the perceived severity of the disease in the community (Chaka et al., 2018; Geremew et al., 2018). The majority of people are not aware of treatable cancers and assume that cancer cannot be cured even if it is diagnosed at an early stage and treatment is given to the patient: they directly link the word ‘cancer’ with death, which is why many patients suffer from severe emotional distress when they hear the word ‘cancer’. Similar findings were reported from a study conducted among adolescent cancer patients in the United States (Head & Iannarino, 2019). Another study also stated, “For many, cancer is synonymous with death, and fear is a rational and primal response” (Penson et al., 2005). This is consistent with a previously conducted study on the disclosure of cancer diagnosis in Ethiopia, which reported that both health professionals and family members tried to avoid the word ‘cancer’ and preferred to use other similar words to talk about the illness with the patient (Abebe & Abebe, 2017).
A similar type of perception towards cancer treatment was also reported from other African countries, such as Nigeria (Jedy-Agba et al., 2017), Cameroon (Kaninjing et al., 2018), Botswana (Anakwenze et al., 2018), and Ghana (Gyedu et al., 2018). This unbalanced perception might be attributed to high cancer mortality rates in Africa (American Cancer Society [ACS], 2022; Bray et al., 2018), including Ethiopia (Eber-Schulz et al., 2018; Gizaw et al., 2017). In particular, a lack of good success stories makes the situation more difficult to persuade the community that cancer patients can be cured and live longer. In addition, there is no patient support group organized by survivors, and those patients who were treated and cured from cancer usually do not go public to increase public awareness (Wondimagegnehu et al., 2023). In contrast, a large-scale study conducted among advanced cancer patients in 11 countries across the world reported that 55% of patients receiving palliative care inaccurately perceive that their cancer is curable (Yennurajalingam et al., 2018); this huge variation in perception towards the curability of cancer might be due to geographical differences (the majority of the data in the above-mentioned study was from developed countries), methodological differences, and the fact that it was hospital-based with only advanced cancer patients, compared to our study that included community representatives and religious leaders.
Depression, hopelessness, and fear of death were the other identified psychosocial challenges in this study. Several systematic reviews and explanatory studies reported that these symptoms are very common among cancer patients, either at the time of diagnosis or during the course of treatment (Doherty et al., 2019; Saleh Baqutayan, et al., 2012; Wondimagegnehu, et al., 2019; Zainal et al., 2013). However, the reported variation in the percentage and severity of symptoms might be explained by the difference in the site and stage of cancer, the type of treatment received, the social structure, and the psychosocial support received.
Although the magnitude of refusals for medical treatment was not determined in this study, our results suggested that several cancer patients refused surgical or any kind of treatment immediately after diagnosis. This finding is in line with a previous quantitative study stating that one in five cancer patients refuse surgery or discontinue medical treatment in peripheral hospitals of Ethiopia (Wondimagegnehu et al., 2022). Conversely, a study in the United States reported that only .4% and .9% of cancer patients refused surgical and radiation therapy, respectively (Aizer et al., 2014). The main reasons for refusal should be explored further, but possible explanations might include lack of trust in the medical treatment, bad experience of other patients, fear of complications, and also false beliefs (the cause of cancer is an evil spirit that should be treated with spiritual customs only).
We also found that some cancer patients discontinued medical treatment for several reasons. Financial constraint was one of the major reasons explored in this study. Due to the complex nature of the disease, cancer requires local and systemic treatment for an extended duration of time, and it is known that each type of treatment is expensive and not affordable for many cancer patients. For this reason, many developed countries use different mechanisms to minimize the financial burden on patients: subsidizing the medication cost, including it in health insurance fees or linking patients with different supporting organizations, and other means. However, in Ethiopia and other LMICs, the absence of a health insurance system (Travado et al., 2017) means that cancer patients have to pay all the diagnostic and treatment costs from their own pockets. According to a study in Cameroon, only 1% of cancer patients used private insurance and 1% received support from the government to pay for treatment (Price et al., 2012). In addition, because of the limited number of cancer centres in Ethiopia, the majority of cancer patients and their caregivers need to travel to the capital city, which exposes them to additional transport and accommodation costs. Such extra costs exacerbate the financial stress on the whole family and can even make treatment impossible. The above-mentioned study found that 23% of patients travelled more than 7 hours to reach a cancer centre and that 40% of patients spent more than $200 on a single round of chemotherapy (Price et al., 2012). Similarly, a study in Ethiopia found that 74.4% of patients experienced catastrophic health expenditure, with a mean overall cost of $2366 per patient. Chemotherapy was one of the main reasons for such high expenditure (Kasahun et al., 2020). Another study in Malawi reported that around two-thirds of cancer patients frequently request financial and food support, suggesting a high prevalence of economic and psychosocial needs in such settings (Herce et al., 2014).
This study also identified that cancer patients discontinue medical treatment because of pressure from the community to visit traditional healers and religious places. Traditional treatment is still considered to be one of the effective treatment options for many chronic illnesses in LMICs, especially in Africa. Several studies conducted in different parts of the continent reported that many cancer patients took traditional medicine or at least tried it once (Anakwenze et al., 2018; Jedy et al., 2017; Kaninjing, 2018).
Even though spirituality is one of the components of psychosocial support recommended for patients with chronic illness, our study found that religious beliefs and practices may negatively influence cancer patients either to accept and start treatment immediately after diagnosis or to discontinue medical treatment. Similar studies in Nigeria and Ghana reported that there is a significant association between religion and late-stage diagnosis among breast cancer patients (Gyedu et al., 2018; Jedy et al., 2017). These studies revealed the impact of religion on screening practice, early diagnosis, and adherence to treatment in cancer care. Another qualitative study from India described the link between cancer care and religion from a different angle, looking at the impact of cancer on religion. The participants reported that cancer affected their faith and even changed their religion while few became closer to God due to their illness (Elsner, 2012). Similar findings were reported from Malaysia, with cancer considered to be a lesson from God and suffering seen as educational theodicy: getting closer to God (Ahmadi et al., 2019). Our study also explored the link between faith and the curability of cancer and found that the Ethiopian community strongly believed that someone can be cured from cancer if he/she has a strong faith in God/Allah and properly practices the religious rituals. Previous studies conducted in different parts of the country also came up with similar findings concerning religious practices and the utilization of traditional medicine among cancer patients (Chaka, 2018; Dereje et al., 2020; Gebremariam et al., 2019). The misconception by patients, their family, and community that cancer is not curable negatively affected patients’ acceptance of treatment and, as a result, caused the patients to look for alternative approaches.
Nevertheless, cancer patients in Ethiopia receive social support from family, friends, and significant others; our results also revealed that they are forced to hide themselves from social activities due to peoples’ reaction around them. The community members are unintentionally disrupting patients’ emotional well-being assuming that they are providing social care. Similarly, a qualitative study done in Liberia narrated about the wholistic nature of cancer patients and how the interaction of various environmental, social, and interpersonal factors attribute the psychosocial well-being of cancer patients (Lusaka et al., 2023).
The findings of this study suggest the need to design, integrate, and provide culturally acceptable psychosocial services in the routine cancer care of Ethiopia. Challenges identified at individual, interpersonal, and community levels may offer guidance on how and where to intervene and who to involve in the establishment and implementation of a supportive care system in the continuum of cancer care. Therefore, an educational session on how to approach and provide emotional and other supportive care should be given for family members/care givers and the general community at large. According to a recent scoping review, providing different types of supportive services in less-resourced settings, even when health systems are fragmented and fragile, can improve mental health, physical health, and the quality of life of cancer patients (Cabanes et al., 2022). Even though the importance of psychosocial services for cancer patients has been well proven, previous study in Ethiopia showed there are no structured psychosocial services for cancer patients (Wondimagegnehu et al., 2023). The need for increased community engagement, primary palliative care capacity development, and the support of local and national decision-makers is also emphasized to expand supportive care through considering the various dimensions of patients (Lusaka et al., 2023). Similarly in Ethiopia, attention should be given for provision of comprehensive palliative care as majority of cancer patients are diagnosed at advanced stage of the disease and require various form of psychosocial services that should be integrated in the routine cancer care and existing social structure.
One of the strengths of this study is fulfilling the principle of maximum variation, in that the data were collected from cancer patients, patients’ relatives, health professionals, community representatives, and religious leaders, which enhanced the completeness and representativeness of the data. The other strengths of the study are the large sample size, the use of a mixed data collection technique (both IDIs and FGDs), and the study being conducted in both urban and rural areas.
One limitation of this study is that the majority of the participants involved in this study were breast cancer patients, which slightly skewed our participants to more females than males. However, an attempt was made to include other types of cancers, such as gastric, endometrial, and cervical cancer. Another limitation of the study is that traditional healers were not included, even though we initially planned to involve them; we approached two herbalists in Butajira, but they were not willing to be interviewed.
Conclusion and Recommendation
In this study, at an individual level, emotional distress, denial, and suicidal attempts were the most common challenges immediately after diagnosis, while depression, hopelessness, and fear of death were identified as problems during the course of treatment. At an interpersonal level, we found that cancer patients had strong social support from family members and close friends. However, the involvement of family members in major decisions had a negative influence on adherence to treatment.
Due to this and several other reasons, many cancer patients refused or discontinued treatment and visited religious places or traditional healers, returning back to the health facility at an advanced stage of the disease. Even though there was no stigma or discrimination in the community, this study also revealed that the majority of cancer patients isolated themselves from social gatherings because they did not want to talk about their disease.
Therefore, psychosocial services that include individual counselling and psychoeducation should be provided for cancer patients in health facilities. Health professionals need to routinely screen cancer patients for comorbid diseases such as depression and anxiety and provide appropriate emotional support as needed. Importantly, family and close friends need to be supported and counselled about the treatment in order to avoid contradictory advice being given to the patients. Health education programmes should be organized to improve patient and public awareness that cancer is a curable/treatable disease, using a patient support group, such as cancer survivors, to improve the emotional, psychosocial, and clinical outcomes of cancer. Religious leaders and traditional healers should be involved and work collaboratively with health professionals in the provision of psychosocial services for cancer patients; they should also be informed about the treatment concepts of common cancers and the importance of timely management. In order to gain a complete picture of the problem, we recommend a larger study that includes traditional healers and patients with different cancer types who may have unique psychosocial problems depending on the anatomic site of origin.
Footnotes
Acknowledgments
The authors would like to thank the College of Health Sciences, Addis Ababa University, for the ethical review process. They would also like to thank the study participants, health facilities, and the funding organization.
Author Contributions
All authors conceived and designed the study. A.W., A.A., and E.J.K. prepared the interview guides and A.W. conducted the IDIs and moderated the FGDs. Data analysis and interpretation of the findings was performed by A.W., who also drafted the manuscript. A.A. and B.Z. were actively involved in data interpretation and rewriting the manuscript. M.A., S.T., and E.J.K. critically reviewed the different versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Else-Kroener-Fresenius Foundation through Martin Luther University, Halle-Wittenberg, Germany, Grant No.: 2018_HA31SP. This study was also supported by a grant from the German Academic Exchange Service to Martin Luther University, Halle-Wittenberg, Germany (ID: 57216764), and a grant from the Hospital Partnerships programme through the Deutsche Gesellschaft für Internationale Zusammenarbeit, funded by the Ministry for Economic Cooperation and Development (ID: 81281315).
Ethical Statement
Informed Consent
Written informed consent was taken from all participants. Confidentiality and anonymity of the participants was maintained.