
Abstract
The objective of this study was to investigate factors influencing one’s decision to become a live kidney donor under the framework of sociotechnical systems, by expanding the focus to include larger organizational influences and technological considerations. Semi-structured interviews were conducted with live kidney donors who donated through University of Louisville Health, Trager Transplant Center, a mid-scale transplant program, in the years 2017 through 2019. The interview transcripts were analyzed for barriers and facilitators to live kidney donation within a sociotechnical system. The most salient facilitators included: having an informative, caring, and available care team; the absence of any negative external pressure toward donating; donating to a family or friend; and the ability to take extra time off work for recovery. The most recurrent barriers included: short/medium-term (<1 year) negative health impacts because of donation; the need to make minor lifestyle changes (e.g., less alcohol consumption) after donation; and mental health deterioration stemming from the donation process. The sociotechnical systems framework promotes a balanced system comprised of social, technical, and environmental subsystems. Assessing the facilitators and barriers from the sociotechnical system perspective revealed the importance of and opportunities for developing strategies to promote integration of technical subsystem, such as social media apps and interactive AI platforms, with social and environmental subsystems to enable facilitators and reduce barriers effectively.
Introduction
The first successful kidney transplantation took place in 1954 and occurred between living identical twins (Reese et al., 2015). Since then, kidney transplants have saved many lives and are often the best way to save the life of someone in kidney failure. Living-donor kidney transplantation (LDKT) is the gold-standard, most cost-effective treatment (Karlberg & Nyberg, 1995; Matas & Schnitzler, 2004) with significantly better outcomes compared to other kidney replacement therapies including dialysis and deceased-donor kidney transplants. The average life expectancy on hemodialysis is 3 years (Stokes, 2011) compared to over 10 years in kidney transplant recipients. In kidney transplants, the average time of graft survival is 12 years for deceased-donor kidney transplants while it is 17 years for LDKT (Medin et al., 2000; Poggio et al., 2021). Despite the clear advantages of LDKT, there are simply not enough live donors to help all who are in need. According to the Health Resources and Services Administration (HRSA) under the US Department of Health and Human Services (DHHS), 77% of all kidney transplants were through deceased donors in 2020. Thus, researchers have investigated how to reduce this gap and encourage more live kidney donation (LKD) (e.g., Irving et al., 2012; Kranenburg et al., 2007; Ruck et al., 2018; Tushla et al., 2015). These studies tend to focus more narrowly on the donor and their immediate social environment. The current study aims to further investigate factors influencing one’s decision to become a live kidney donor by expanding the focus to include larger organizational influences and technological considerations. In particular, we frame these factors from the sociotechnical systems perspective, which could help us evaluate the current system under a new lens and find strategies to promote LKD more effectively.
The sociotechnical framework distinguishes three integrated parts of an organizational structure: social, technical, and environmental subsystems (including internal and external) (Hendrick & Kleiner, 2001; Kleiner, 2008). Trist and Bamforth (1951) led the earliest studies that resulted in the formulation of the sociotechnical perspective. They studied coal miners in Britain in the 1940s and 1950s and investigated the impact of a new form of mining “shortwall” versus the traditional “longwall” mining. The introduction of new technology, such as mechanical coal cutters and conveyer belts, was expected to dramatically increase productivity. However, a technology-driven approach failed to consider how to best integrate the new technology with the social subsystem and instead resulted in poor performance, absenteeism, and a myriad of other problems as the social work structure was completely rearranged to optimize the new technology in ways that were harmful to the workers and their social network. The solution was to develop a hybrid approach called the “composite longwall method,” which kept the main elements of the new technology, while thoughtfully integrating it with the previous social structure and network. This type of joint optimization of the social and technological subsystems to meet the demands of the external environment formed the basis of the sociotechnical systems framework that has been applied to other settings, including health care. Sociotechnical systems theory has been used and discussed prominently in the medical informatics literature (e.g., Aarts, 2013; Aarts & Gorman, 2007; Ash et al., 2007; Berg, 1999; Harrison et al., 2007; Westbrook et al., 2007). Although there is no one “sociotechnical approach” (Aarts & Gorman, 2007), all studies that rely on a sociotechnical perspective have a high-level recognition that organizational and health systems at large have a substantial influence in shaping technology and that the technology and context are intertwined (Aarts & Gorman, 2007). We apply the same framework to the realm of LKD to extend the focus beyond the current and potential live kidney donors and clinical staff, to also include the larger external environment that influences LKD, as well as technologies that may be integrated to support and facilitate one’s journey through the LKD process. We chose this sociotechnical systems framework to use a larger organizational systems perspective to understand strategies, technologies, and external environmental considerations that may be integrated to support and facilitate LKD.
In the larger organization of LKD, the social subsystem is comprised of the live kidney donors, their friends and family, the donor recipients, and the health care team. The social subsystem also includes these individuals’ beliefs, attitudes, social networks, etc. The technical subsystem includes not just the health IT (e.g., donor health records) but also technology such as social media apps that connect donor support groups. Physical environmental and local contextual factors are part of the internal environment. The external environment includes any external influences such as available funding support for live kidney donors. Ideally, the social and technical subsystems, as well as the internal environment, are balanced, or “jointly optimized,” to function optimally. The sociotechnical systems theory is used to frame the findings of the current study.
Methodology
As a methodological approach, we used content analysis (e.g., Krippendorff, 2018) to shape our research objective to elicit barriers and facilitators to LKD within a sociotechnical systems perspective and to guide our data collection and analysis of findings. We conducted interviews with live kidney donors both remotely via teleconferencing and in person, socially distanced due to the COVID-19 pandemic. We used semi-structured interview technique to explore the decision-making process leading to becoming a live kidney donor. The study location was University of Louisville Health, Trager Transplant Center, which serves a patient population that is about 80% (middle-income) Caucasians. The transplant program performs about 15–20 LDKTs per year. This study was approved by the University of Louisville’s Institutional Review Board (IRB) (IRB # 20.0440).
Recruitment
The participants for this study were recruited from a list of those individuals who completed LDKT during the time frame of January 2017 to December 2019 at the transplant program. They were contacted either by phone or email. Once a donor expressed interest in participating, the interview was scheduled in the setting they preferred (in person at a university conference room or virtual via MS Teams). After the interview was scheduled, the written informed consent form was sent for review prior to the interview.
Semi-Structured Interviews
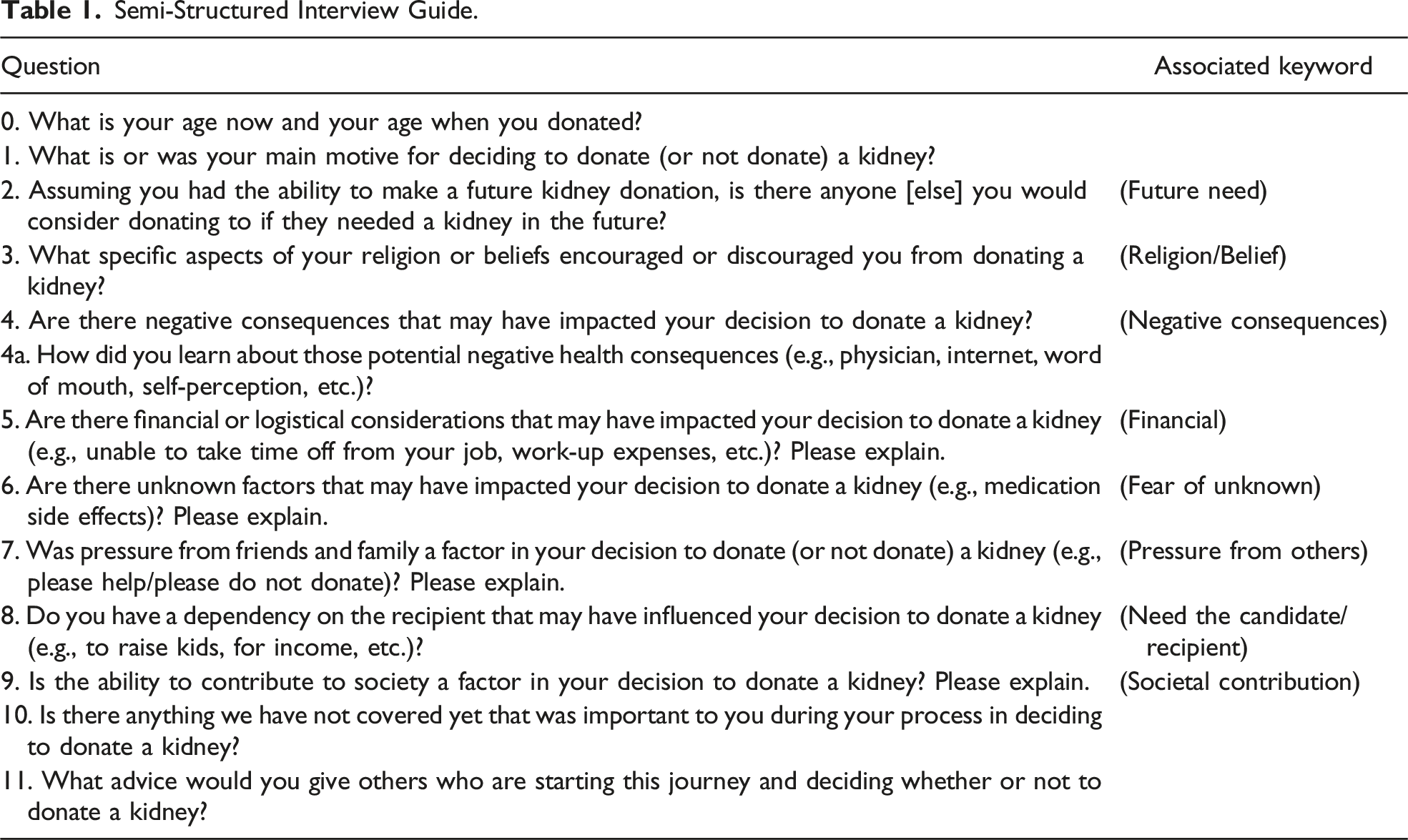
Semi-Structured Interview Guide.
Analysis
The semi-structured interviews provided qualitative data for analysis to identify barriers and facilitators to LKD. Consistent with content analysis, the interview responses were broken down into smaller segments, which are easier to analyze for an overarching code of that segment. Segmenting includes dividing the data into smaller, more meaningful parts. It can be a word, a sentence, phrase, or a full paragraph. It does not have a set length but rather simply needs to have an overarching meaning or theme to the researcher (Johnson & Christensen, 2019).
Codes and Definitions.

Once the codebook was created, the lead author (RC) and another member of the research team (CW) used the codebook to code the remaining 18 interviews. Each of these codes were filtered into their own category and analyzed individually. The lead author analyzed each code individually to find associated facilitators and barriers with a second team member confirming or suggesting edits to each. This type of auditing procedure by a second analyst is considered an acceptable alternative to using independent coders for ensuring validity of the analysis (Holden, 2010).
Results
A total of 20 donors (13 females and 7 males) were enrolled in this study to talk about their journey as a live kidney donor at the interviews. The ages of the participants at the time of donation ranged from 23 to 68 years of age. The mean age of the participants was 48.4 years old, while the mean age at the time of donation was 46.2 years old.
Barriers.

Facilitators.

Barriers
The codes representing barriers included Short/Medium-Term (<1 year) Effect, Long-Term (≥1 year) Effect, and Donor Health (Table 3).
Short/Medium-Term Negative Health Effects
The weeks and months following donation can be tough on the donor, creating a physical barrier. Specifically, one donor described their experience: The only thing that surprised me was how horrible I felt for the first month or so after the transplant. I knew I’d heard, they had told me it’s usually more difficult on the person who gives the kidney rather than the recipient, but I just didn’t realize how that was going to be until I experienced it.
For context, most donors undergo laparoscopic nephrectomy. While a laparoscopic surgical procedure minimizes scarring and recovery time compared to open surgery, donors may still experience a long and difficult recovery. Another donor talked about their exhaustion: I had like extreme exhaustion, and not like initially after the surgery, but I went back to work like 4 weeks after. And I was probably like the most tired, I mean, than I've ever been in my whole life, to where I wanted to cry every day when I came home from work. And I was like that for probably a good like six, seven months.
Post-Donation Lifestyle
Long-term (≥1 year) effects on the donor, regarding lifestyle changes after donating, can be a hard adjustment. For example, donors can no longer take ibuprofen, and they must limit alcohol intake (Balliet et al., 2019). One donor shared her specific fear in relation to her history of migraine: I have a history of migraine headaches and I control my migraines a lot with NSAIDs, ibuprofen, Aleve, things like that. Well, I knew that after I donated the kidney, that I would be discouraged from taking those things. I ended up in the hospital for four days, several months after the transplant, with an intractable migraine because I couldn't control it.
In relation to this, a common health fear of donors was that they may one day need a kidney as they fail to comply with expected lifestyle changes. Although this was not a prominent barrier found in our current study, two separate participants addressed this issue with the following quotes: What if 20 years down the road I need a kidney? They said you jump to the front of the line, of the register. I said, okay. That made me feel better. There’s chance that you could, the one kidney you have could fail and you’d go on the list. But the good thing about that is if you donate it, you go to the higher barter list. You’re not waiting so long.
Both participants are referring to the fact that if you are a live donor who then goes into kidney failure, you are awarded points to be put in a priority spot on the deceased donor list according to the National Kidney Registration (Health Resources & Services Administration (HRSA), n.d.).
Mental Health
Donors expressed experiencing concerns regarding their mental health being affected negatively during the process. One donor stated: I was really stressed before surgery and I guess I’d never been that stressed in my life because my body reacted in hives. I’ve never had that experience before this, and I’ve never had the experience after this, but I was so incredibly stressed about getting off painkillers.
Facilitators
While three clear barriers each with a unique code were apparent from the data, more facilitators emerged associated with nine unique codes (Table 4).
An Informative, Caring, and Available Team
Regarding the patient’s care team, quality care was important to the donors. One donor said: I think the support team that was available to us at the transplant center was absolutely outstanding. Their donor advocate team, I can’t say enough good things about them because they really made the process more transparent and helped me too and helped all of us to feel calm about it.
Majority of the participants referenced their care team during the interview. Along with being comforting and supportive, the care team being available for questions was also important. One donor stated: I thought of a question at five or six o'clock I could call her or text her. And she was very quick to return my call. I can’t say enough good things about the transplant center. They were super helpful, super informative, that really helped with everything along the way to make me feel very much at peace with the whole thing.
A Supportive Social System
Having a positive supportive social system was influential in a donor’s decision to donate. One donor explained: I had his support and my family support. So having that support was key. If I had not had their full support … So I needed two people’s full support, my husband and my mom. My husband to take care of the kids and my mom to come and stay with me in the hospital. If they had not been able to help me, I would not have been able to donate.
At the very least, the absence of any pressure not to donate was seen as helpful. For example, one donor noted: Actually, my family, it ... I was surprised that they were as okay with it as they were … I was like, “I think I’m going to do this.” So, then I told my mom and dad, and they were actually fine with it.
Alternatively, the lack of negative pressure was also desired during the donation journey. One participant refrained from telling anyone to avoid any unwanted or negative pressure: I actually at first didn’t tell anyone, not even my son. I only told my husband. Yeah. Yeah. Because I didn’t want that pressure.
Another participant mentioned that a social media (Facebook) support group dedicated to support kidney transplant donors and recipients was influential for her decision-making.
Sufficient Time off for Recovery
When talking about their Career, being able to take enough time off from work (or school) to recover was important. One donor said: So I was able to schedule all of my testing and everything when I was off of work. If I wouldn’t have been a teacher, then yeah, I don’t know really how I would do that because I really can’t afford to have a forward for the amount of time that it took to accomplish all that.
Another donor felt so strongly about having time off for donation that they reached out to their state legislator to ask them to offer paid leave for being an organ donor: So the surgery was considered elective for my company and for me, so I took four vacation days and came back after six days …. So actually, I ended up reaching out to my State legislator …
In this case, the participant was advocating for time off work for live kidney donors who may be in more difficult work situations, without vacation days to use.
Financial Stability Prior to Donating
Being financially comfortable was also important to donors. Twelve participants described their financial situation prior to donating as important when deciding to donate. One individual described how they lessened the potential financial burden: Financial was a big decision in that because I am self-employed, so a friend did a GoFundMe thing for me to help.
In another example, when two brothers were candidates for LKD, the better financial situation for one of them was a major deciding factor: My financial situation allowed for it [becoming a live kidney donor] a lot better than one of my other brothers.
Recipient’s Declining Health
Seeing a declining health of the recipient or watching his/her experience with dialysis could motivate those witnessing to donate; these sentiments were expressed by 11 of the participants. Additionally, five participants talked about the rewarding feeling of seeing the recipient’s positive change in health post-transplant. One donor stated: I would just wish that there was a way that we can have people see how much of a benefit it is, because when I was watching my brother getting dialysis … He was just so sick and so sad all the time, and now that he’s got his donation, the kidney, he’s back to normal, doing pretty much normal things as far as his ability to do things.
Related Donation
Having a relationship with or knowing the recipient can encourage donation. Fifteen participants donated to either a close friend or family member with eleven participants donating specifically to a family member. When asking the participants their motive for donating, some of the responses were: “So for me, it was personal. My best friend, she went into kind of a sudden kidney failure,” “Well, to help my brother,” and “Well, I actually donated to my son. Just to give him a better quality of life obviously.”
The five participants who did not donate to a friend or family member are considered altruistic donors. An altruistic donor is a person who wishes to donate a kidney to a person with advanced kidney disease, who he or she does not know. This decision to donate comes from personal conviction (three participants) or faith inspiration (two participants).
Religion
Holding strong personal beliefs or belonging to a religion can positively influence the decision to donate. One donor felt particularly strong: All along, I felt like it was a calling that God placed on my heart. So just reach out and just make myself available.
Another donor shared: The family that I donated to, they’re very strict to the guidelines of their religion. For me I translate it more into trying to be a kind person. And that is a big portion of what religiously, what we believe in, is being a good person, doing unto others as we would like to have done unto us.
Empathy Attributable to Their Past Experience
Witnessing a successful kidney transplant and/or observing a kidney failure patient can lead to altruistic donation. One donor shared: I had a foot surgery … and in the basement … across the hall from the dialysis center. You just see them in there, and that’s, you’re not living at that point. You’re living for a machine and if you could’ve changed just one person to not be dependent on that machine.
Similarly, but a more positive experience, witnessing a successful kidney transplant, may have a similar impact in encouraging someone to donate. A separate donor stated: When I was working as a bedside nurse, I worked in the pediatric intensive care unit as a nurse. I saw children getting kidneys from people that they didn’t know and their lives being saved.
Donor’s Health
Seven participant donors specifically mentioned they had lived overall healthy lives prior to considering donating, positively impacting their confidence about going through the donation process. Having a healthy body prior to donating seemed to ease the decision to donate. When asked about if any unknown factors impacted their decision, one donor answered: No. No, I don’t really get sick. I’ve never broken a bone. I’ve never got surgery before.
Interaction With Previous Donor or Recipient
Seven participants shared that joining social media, talking in person with a donor, or reading a blog about a previous successful transplant story raised their comfort prior to the surgery. One donor shared: So I was actually talking with somebody else who is considering living organ donation and there is a site …, and it’s a lady, I think she’s out of Cincinnati. She wrote for a newspaper, did an article on living donors, ended up becoming a living donor herself. And so she set up this site where living donors can tell their stories, what was the surgery like? What was the recovery like? I happened across that site a couple of days before surgery and I was feeling pretty confident.
Sufficient Information
When asked about what advice they may give to someone considering this process, six participants mentioned about the importance of a well-informed decision. Of those, five participants extended their knowledge-base past what the transplant center gave them, either through hearing from other donors or doing online searching. One donor said: I went to [Transplant Center Name], watched a lot of YouTube videos, I listened to doctors talk about the procedure and just how much it really helps people.
Kidney Exchange
The option for a Living Kidney Exchange when the donor and their intended recipient are not a match is a strong facilitator. This was not a scripted question, but in the seven participants who brought it up, six mentioned that the availability of the Exchange motivated the donation, and they would have participated had they not been an initial match. One donor shared: I know they have this sort of, I don’t know what they call it anymore. They told me, but it’s like a chain of donations. So let’s say somebody in California needs a kidney, but they don’t have a match, but I’m a match for him. But the person in California that wants to be the donator was a match for my son. There’s some kind of big circle thing that you can do with that. And sometimes it’s three and four different kidneys that are all going on at the same time. And obviously we didn’t have to do that, but I could see that process where I knew I was helping the individual that I wanted to donate to, even though I was giving it to somebody in California, maybe. I could definitely see where I would do that.
Sociotechnical Systems Framework
The influencing factors identified through the semi-structured interviews can be framed using the sociotechnical systems framework. Most of these factors found in our study were heavily grounded in the social subsystem. These include facilitators such as (i) having an informative, caring, and available care team; (ii) a supportive social system and social support groups; (iii) related donation; (iv) personal religious beliefs; (v) witnessing a successful transplant or kidney failure patient; (vi) having a healthy body prior to donation; (vii) interacting with a prior donor; and (viii) having sufficient information. At the same time, some of these facilitators were also grounded in the technical subsystem. Specifically, there were statements that social support groups and interactions with prior donors (ii) leveraged social media, and acquiring sufficient information (viii) involved YouTube videos. Barriers within the social subsystem include (i) potential negative health effects; (ii) lack of understanding of post-donation expectations; and (iii) negative impact on mental health. While there was no explicit statement related to the technical subsystem, some of these barriers could be ameliorated by utilizing social media as well as online education.
Figure 1 illustrates the sociotechnical system that visually shows the joint optimization of the subsystems for a potential live kidney donor’s experience through donation. Each of these subsystems could play a role in the potential donor’s experience and ultimately their decision to donate or not. Assessing the factors from the sociotechnical systems perspective reveals design opportunities to build support structures within the technological subsystem to help maximize facilitators and minimize barriers to LKD. While further specifications of such designs need to be established in coordination with all stakeholders, that is, donors, recipients, and their family members, transplant teams, as well as web engineers, some of the examples include, for instance, additional support groups (social subsystem) that can be enabled through thoughtfully designed apps and social media, such as Facebook (technical subsystem). Similarly, transplant centers can make more explicit effort to identify web-based financial resources (technical subsystem) to support donor candidates with financial needs and facilitate the communications (external environment). Live kidney donor experience with the sociotechnical system.
Discussion
The facilitators and barriers found under the current study were comparable to those found in previous qualitative studies on perceptions, decision-making, and barriers/facilitators to organ donation. These previous studies have identified several factors that can contribute to decision-making for living donation (Asghari et al., 2022), including the social influence of family members (Irving et al., 2012), recipients and potential donors (Barnieh et al., 2011; Waterman et al., 2006), health care professionals (Sandal et al., 2019), and medical (Min et al., 2018) and financial (Przech et al., 2018; Tushla et al., 2015) barriers. For example, Irving et al. (2012) performed a systematic review of the qualitative literature for factors that influence the decision to be an organ donor. This review broadly included all types of organ donation, as well as living and deceased donation. Their review of 18 studies found that the decision to be an organ donor was influenced by relational ties, religious beliefs, cultural influences, family influences, body integrity, previous interactions with the health care system, the individual’s knowledge about the organ donation process, and major reservations about the process of donation. More recently, Ruck et al. (2018) investigated donation-related concerns specifically for LKD. They found that in addition to a variety of personal donation-related concerns, potential donors frequently hear donation-related concerns from family members and friends. Our study is largely consistent with these previous qualitative studies in terms of perceptions of donors, their decision-making to become a donor, and barriers/facilitators, but differs on how these are framed within a larger sociotechnical system, with a particular emphasis on the larger external environment that influences donation, as well as technologies that may be integrated to support and facilitate one’s journey through donation.
The barriers revealed by this study could provide insights into the ways to facilitate donation by addressing them. It is not surprising that donors worry about the negative consequences of donation as there is obvious discomfort with any procedure. Preparing donors for the levels of pain and discomfort they may feel could help lessen that shock after surgery. Similarly, donors could benefit from being offered other medications or advice for how to deal with headaches, slight pain, and fevers that may have required ibuprofen pre-donation. The donor who suffered migraines before and after the transplant expressed that they wished they had their neurologist’s input before donating to better understand how to deal with their migraines post-donation. Another common health fear of donors as discussed in Ruck et al. (2018) was that they may one day need a kidney. Preparing donor candidates with knowledge on current kidney allocation policies and resources would benefit them. Aside from physical effects, five participants mentioned their mental health being affected throughout this process. It may be critical for all transplant centers to offer a counseling service during the whole process for donors, as well as for their families.
Although three barriers emerged from the interview data, it was clear that the participants felt strongly about donating and were willing to share reasons why they ultimately chose to donate. When looking to increase the donor pool, these are important aspects to keep in mind. Ensuring the donor’s care team is both helpful and empathetic is an overwhelmingly important factor to the potential donor to continue in their decision process. Standardizing the wording that potential donors hear may help to optimize that feeling, as well as provide a basis of common, informed knowledge for every potential donor. For many donors, being in a comfortable spot financially and taking time off from their job or career was an extremely important factor and one that other studies found as a strong barrier if that is not the case (Tushla et al., 2015). If more employers offered a paid leave for organ donors, it should help lessen the financial stressors suffered by people that might have otherwise shied away from donating. The concomitant effort to utilize existing resources also needs to be made. In the United States, 15 states passed tax deductions and one state passed a tax credit policy between 2004 and 2008 to help defray potential medical, lodging, and wage losses for federal employee live donors (Chatterjee et al., 2015; Venkataramani et al., 2012). Similar state-level tax deduction and paid leave laws have also been introduced (Wellington & Sayre, 2011). These policies are, however, known to have no impacts of increasing the number of donors thus far (Chatterjee et al., 2015; Venkataramani et al., 2012; Wellington & Sayre, 2011). More explicit effort to connect potential donors to available resources needs to be made to see the benefits of these policies. Finally, the benefit of witnessing a successful transplant and interacting with a prior donor was described by several donors. When potential donors are presented to transplant centers, it could be beneficial to connect them with a network of previous donors or read testimonies from prior donations.
Study Findings Within the Sociotechnical Systems Perspective
Reviewing positive and negative findings from within the sociotechnical systems perspective identified several opportunities to build support structures within the technological subsystem to help maximize facilitators and minimize barriers to donation. It is, however, important that these technologies will be developed through professionally and intentionally designed and organized user experience (UX) interaction design (Kushniruk & Patel, 2004). Recent advancement in web technology allows both transplant and donor candidates to access any information related to LKD. At the same time, an overwhelming amount of information exists on the web and social media, and one can easily be misinformed by inaccurate or contradictory information or be lost with incomprehensible materials that are not helpful to address the specific concerns of potential donors. In the current study, some donors who use Facebook support groups seem to have increased anxiety when combing through several other donor’s experiences and their worst-case scenarios. The interaction design could be promoted to more intentionally support donors and provide them with information that can ease their concerns. Here, emerging interactive AI platforms, such as ChatGPT, could be extended and utilized to support donor candidates. Ideally, such platforms are designed and promoted through the partnerships among transplant centers, web technology developers, live donors and donor candidates, and other stakeholders involved in living donation.
Limitations
Limitations of this study should be taken into consideration when interpreting the results. For example, the donors interviewed for this study were from a single transplant center. Including donors from other transplant centers with different donor profiles may have allowed us to explore and compare other factors that are unique to the populations that are served by each transplant center. Further, we used a convenience sample of donors who were willing to be interviewed for this study rather than using a recruitment strategy based on factors such as race, income level, and other demographical categories. Finally, we only interviewed those who completed donation. In order to gain a comprehensive picture of barriers, it is critical to interview those who gave up donating in the donor evaluation process
Conclusion
This research revealed facilitators and barriers to LKD and uniquely investigated LKD as a sociotechnical system. Assessing facilitators and barriers through this lens revealed the opportunity to facilitate LKD by developing strategies to integrate technical and social subsystems. These strategies could take forms of social media apps or interactive AI platforms. Such apps or platforms should offer evidence-based information to donor candidates throughout their donor evaluation process and be able to offer first-hand experiences of other donors. Health care systems, in specific transplant centers, can capitalize on these strategies and encourage the use of technical support groups for their patients, donors, and other stakeholders. If utilized, these have the potential to increase the donor pool and awareness of LKD effectively.
Footnotes
Authors’ Contributions
RC, MG, and JJS conceived and designed the study. RC and CW were responsible for the data collection. RC, CW, and JJS all contributed to the analysis and interpretation of the data. RC and JJS had principal responsibility for drafting the manuscript. All authors critically edited the manuscript and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an internal grant award from the University of Louisville’s Office of the Executive Vice President for Research and Innovation (EVPRI), Transdisciplinary/Multidisciplinary Collaboration Research Planning Grant (program # 54152). This work was also partially funded by an NSF award (NSF – ENG: SCH: / 2123683).