
Abstract
Birth trauma is a common experience, with 50% of birthing individuals perceiving their birth as traumatic. Using interpretive phenomenological analysis with an intersectional feminist trauma lens, this study aimed to understand how people experience healing from birth trauma. Eleven participants, who self-identified as having experienced and healed from a psychologically traumatic birth, were recruited. Data were collected through in-person interviews, follow-up phone interviews, and optional focus groups. The study identified five key themes related to the experience of healing from birth trauma: (1) seeking and strengthening support, (2) creating community and sharing stories, (3) empowerment as reframing the narrative and returning to self, (4) giving birth again, and (5) healing over time. The participants sought support from partners, friends, family, and healthcare providers, with some seeking professional therapy and medication. Creating communities and sharing stories, both in-person and online, helped reduce isolation and validate their experiences. For most participants, giving birth again was a major component of healing, providing opportunities for self-advocacy, regaining control, and experiencing patient-centered care. Empowerment is a key healing experience involving reframing narratives and self-acceptance. Healing was experienced as a nonlinear process over time, with moments of realization and reflection. Findings suggest that while psychological intervention is sometimes accessed, sharing stories, creating a community, and strengthening support systems over time are key components in moving forward from birth trauma. Interventions should integrate peer-led support and focus on reducing isolation and promoting community for those with birth trauma.
Introduction
Although the experience of childbirth is often idealized, for many individuals giving birth can be an overwhelming, distressing experience. Birth trauma is not uncommon; according to research, approximately 50% of birthing individuals perceive their birth experience as traumatic (Abdollahpour & Khadivzadeh, 2022; Alcorn et al., 2010). These traumatic experiences span a broad spectrum of emergency, high-risk deliveries to births that are medically routine and low risk.
Birth trauma can be understood as any overwhelming experience of a birthing person during the birthing process that leaves them with feelings that may include, but are not limited to, loss, distress, grief, sadness, shame, and anger (Leinweber et al., 2022).
Birth trauma can have both individual and communal impacts, affecting relationships between parents and children by causing poor attachment and bonding (Molloy et al., 2021; Murphy, 2020; Tsakmakis et al., 2023). Within two-parent households, individuals with birth trauma can experience either stark distancing or bonding with their partner (Attard et al., 2022). The experience of birth trauma can lead to flashbacks, anxiety, postpartum problems, hypervigilance (Ayers et al., 2018; Sandoz et al., 2022), tokophobia (fear of giving birth), poor maternal health outcomes, low breastfeeding rates, and posttraumatic stress disorder (PTSD) (Ayers et al., 2018; Bastos et al., 2015; Rowan et al., 2007; Sandoz et al., 2022). Individual birth trauma may cause intergenerational and intercommunal trauma at the psychological and epigenetic levels (Horsch & Stuijfzand, 2019).
Although awareness of birth trauma is increasing, research on the healing process remains limited. Moreover, commonly used interventions such as post-birth debriefings have shown minimal effectiveness in reducing posttraumatic stress (PTS) symptoms (Bastos et al., 2015). There remains limited funding for responsive initiatives that are not action or outcome-driven, such as peer support programs (L. Brown, 2018; Tseris, 2013, 2019a, 2019b). This may be at odds with healing processes that extend beyond individual symptomology and recovery (Burstow, 2003; Gilfus, 1999; Thompson, 2021; Tseris, 2019b). The focus of individual traumatic birth recovery (Asadzadeh et al., 2020; Ayers et al., 2018; Gamble et al., 2005; Taylor Miller et al., 2021) has not incorporated a lived understanding of trauma recovery. In a 2024 expert consensus article on recommendations for policy and practice, Ayers et al. (2024) called for future interventions to be driven by individuals with birth trauma and for the integration of trauma-informed care.
Previous phenomenological research on birth trauma has focused on birth trauma experiences (Beck, 2004, 2009; Butterworth et al., 2023; Rhodes, 2022; Sandercombe, 2020). While some studies have examined the experience of birth trauma and its impact on the postpartum period (Murphy, 2020), phenomenological research has not yet been conducted on the experience of healing birth trauma. This is part of a larger study (Middleton, 2025) aiming to address this gap by applying an intersectional feminist trauma lens to understand the experience of healing from birth trauma using interpretive phenomenological analysis (IPA).
Intersectional Feminist Trauma Theory
The emphasis on biomedical approaches to recovery (Asadzadeh et al., 2020; Ayers et al., 2018; Gamble et al., 2005; Taylor Miller et al., 2021) often does not incorporate a critical understanding of trauma and trauma healing. While biomedical approaches to trauma theory primarily focus on the individual, critical trauma approaches connect individual trauma to systemic causes and expand the impact of trauma collectively and intergenerationally (Hardy, 2023; Herman, 2015; Linklater, 2014). Critical trauma theories acknowledge the individual symptomology of trauma while striving to connect individual symptomology to larger social structures (L. Brown, 2018; Hardy, 2023; Herman, 2015; LeFrançois et al., 2012; Linklater, 2014; Menakem, 2017).
Intersectional feminist trauma theory combines intersectional feminist theory with feminist trauma theory. It understands that gender cannot be examined without the context of people’s various identities (Ahmed, 2017; Collins, 2015; Crenshaw, 1989; Lorde & Clarke, 2007) and that intersectionality of women’s lives must be viewed in concert with their multiple identities. Feminist trauma theory explains that gender-based trauma is produced and maintained by the systemic beliefs and actions of political and institutional powers (Tseris, 2013). A feminist trauma epistemological lens views the person as an expert in their lived experience, positioning the oppressed and marginalized as the best source of knowledge. Trauma symptoms are often normal responses to systemic oppression favoring the dominant group. This posits that trauma survivors are capable of healing and moving forward from traumatic experiences (Brown, 2018).
Methodology
This qualitative research project utilized IPA. IPA uses a hermeneutic phenomenological approach that understands a person’s lifeworld is intertwined with their identity, culture, beliefs, values, and past experiences, and helps form their understanding of their experiences (Suddick et al., 2020). IPA methodology focuses on how an individual makes sense of a given experience (Finlay, 2011; Smith et al., 2022; Smith & Nizza, 2021). IPA focuses on ideographic analysis (case by case) and does not strive to universalize the experience of a phenomenon (Smith et al., 2022).
Participants
In May 2024, the study used purposive sampling to recruit 11 participants in the Outaouais region (Canada). Smith et al. (2022) suggest that a sample of 10 is commonly regarded as the “gold standard” for IPA research. Participants were required to self-identify as having experienced, and healed from, a psychologically traumatic birth. As birth trauma research is largely dominated by white, able-bodied cis-women who are partnered with men, the aim of the research was to recruit at least 50% of participants who identified with at least one of the following criteria: LGBTQIA2+, Black, Indigenous, Racialized, disabled, trans/non-binary, or single parent by choice. Overall, nine of the 11 participants identified with at least one of these criteria (Figure 1). Participant self-identified demographics. Identities were self-reported by participants and reflect how individuals described their own lived identities. Participants could identify with multiple categories, and numbers therefore represent identity affiliations rather than discrete participants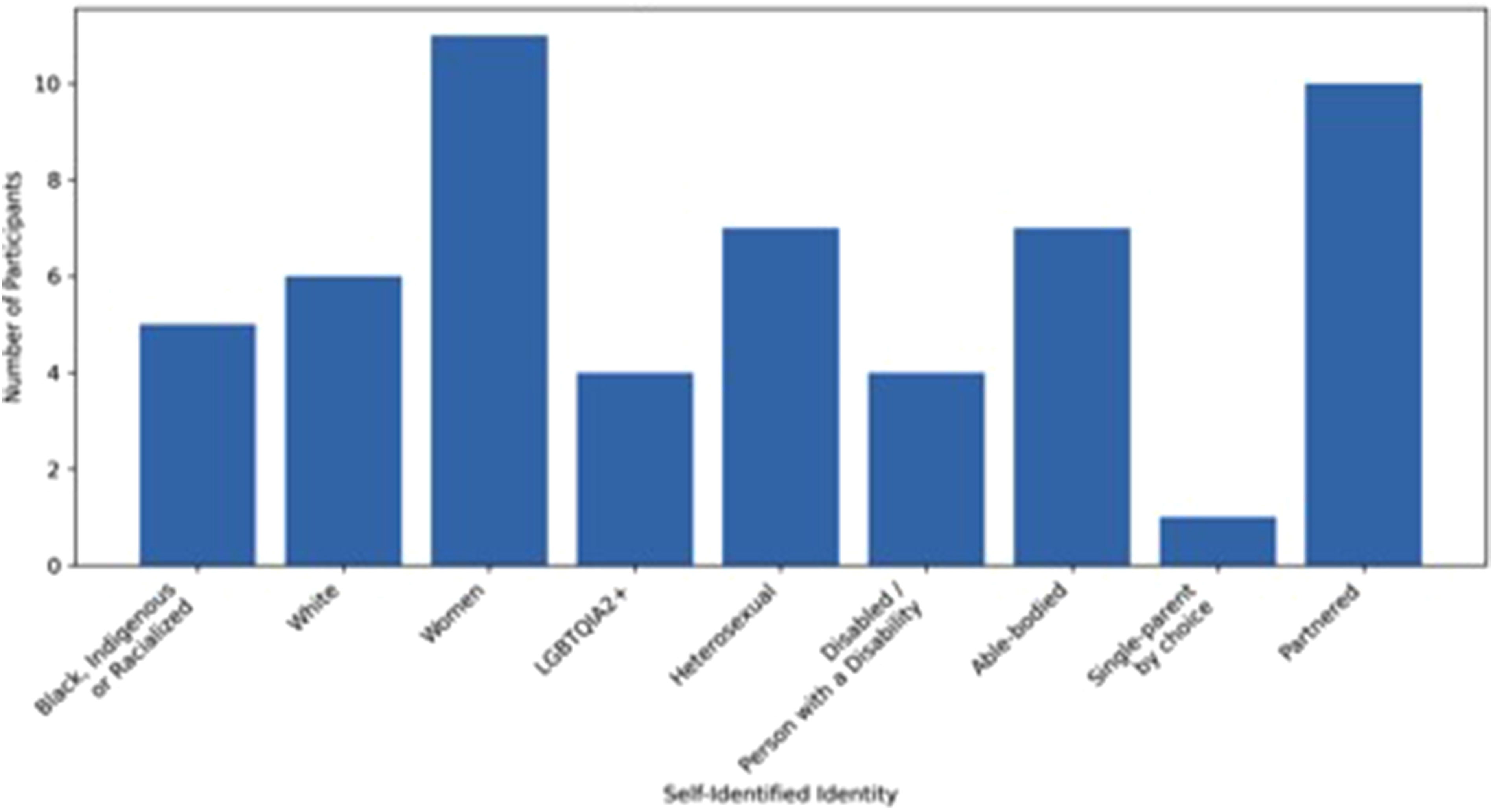
Potential participants contacted the lead researcher via email to express their interest in the study. They received an email outlining the scope and purpose of the research, along with a link to an initial demographic questionnaire, designed to confirm eligibility and collect relevant self-identified demographic information. Within one week, 84 individuals expressed interest, and 60 completed the eligibility and demographic questionnaire. Recruitment was subsequently closed.
Ethics and Positionality
This study received ethical approval from the researcher’s university ethics board. To ensure participant confidentiality, pseudonyms were assigned and identifying information was removed from the data. Written informed consent was obtained from participants prior to the individual interviews, and oral consent was reaffirmed at the beginning of each in-person interview. Additional written consent was obtained from those who chose to participate in the focus group. The study provided participants with a list of community-based resources following the interviews and offered up to three one-on-one counselling sessions with a private trauma therapist based in Ottawa.
While this study aimed to amplify and integrate a diverse range of voices, I acknowledge that my positionality shaped the research process. As a white, settler, queer, feminist social worker/midwife and someone who has personally experienced psychological birth trauma, my analysis was inevitably influenced by these intersecting identities and experiences. I approached the data through this lens, engaging in reflexivity to remain critically aware of how my background could shape interpretation and meaning-making. This included keeping a reflexive journal to critically examine my assumptions, monitor personal responses to participants’ narratives, and note any potential instances of transference throughout the research process. I also actively sought feedback from participants and colleagues. This was an independent research project; in the future, having a diverse committee of researchers would be key.
Data Collection
Participants were invited to take part in two semi-structured interviews and an optional focus group. All 11 participants completed both interviews. Although all 11 agreed to participate in the focus group, four attended, with most citing weather, work, and childcare as the primary reason for non-attendance. An interview guide was provided in advance. Depending on the participants’ choice, in-person interviews were conducted at their homes or at the researcher’s university. Individual interviews were approximately 90 min in length and audio recorded. The focus group lasted 120 min. The interview utilized Smith et al.’s (2022) approach. The first semi-structured interview included (1) making sense of the past and giving space to tell a birth story and (2) making sense of the present and healing from birth trauma. Questions were also asked to understand how people’s identities were integrated into their experiences of birth trauma and healing. The second follow-up phone interview was used to verify and clarify data and provide an opportunity for participants to add to their narratives. The final focus group was used as member checking and asked participants to reflect on whether their experience was reflected in the overall data analysis and asked participants for additional input on what they wanted the public to understand about birth trauma and healing. While member checking is not common in IPA research, it is accepted and encouraged in feminist phenomenology (Munhall, 1994; Tuffour, 2017).
Data Analysis
Data were analyzed using IPA as outlined by Smith et al. (2022), with an idiographic focus. Each case was analyzed individually and in full before moving to the next. Analysis followed the standard IPA stages: repeated reading of transcripts, exploratory noting, development of experiential statements (themes), examination of connections between themes, and consolidation of themes within and across cases.
Each interview was transcribed using the program Descript and the transcript verified by the researcher. As per IPA (Smith et al., 2022), each case study was individually and fully analyzed before moving to the next case. Transcripts were read and re-read using a reflexive approach to reflect positions of power and intersectionality. Initial highlighting and underlining were performed directly on the transcript to note potentially significant information. Exploratory noting was then performed directly on the transcript at the right margin. This noted anything that seemed important or interesting from the transcript, paying particular attention to how the participant discussed or understood the issue.
After exploratory noting was complete, experiential statements (themes) were constructed at the right margin of the transcript. These statements related directly to the participants’ experiences (Smith et al., 2022) and exploratory noting. Themes were then placed coherently on a table to compare the participants’ narratives. Feminist phenomenology specifically encourages researchers to notice and highlight how race, sex, gender, sexual orientation, and ability are revealed in the data. This was done through a reflective process, in which I kept a journal to write and reflect on the intention of the participant. A draft case analysis was then provided to the participants before the follow-up phone interviews. Overall, participants verified their case analyses.
After the phone interviews were complete and data were re-analyzed, themes from each individual case analysis were cross-compared to identify repeating themes to develop group experiential themes across cases. This was done by writing statements for each case on sticky notes and randomly scattering them on a wall. Statements were then cross-compared to identify repeating themes. Quotations were selected to examine this theme. This stage included writing reflecting on why the data were being grouped together, as well as going back to each manuscript to ensure the intention behind the quotation. This process was repeated for each question: What is the experience of birth trauma and what is the experience of healing from birth trauma?
Finally, prior to the focus group, draft data analysis was provided to the participants in the study. Notes from the final focus group were used to verify the data analysis and to add additional thoughts on what it meant to experience and heal from birth trauma. Overwhelmingly, participants agreed with the analysis and expressed that their experiences were reflected in the data analysis.
Findings
The study identified five key themes related to the experience of healing from birth trauma: (1) seeking and strengthening support, (2) creating community and sharing stories, (3) empowerment as reframing the narrative and returning to self, (4) giving birth again, and (5) healing over time.
Seeking and Strengthening Supports
Participants described healing as a process supported by seeking out and strengthening relationships, including deepening connections with friends, family members, partners, and midwives, as well as accessing professional therapy and, in certain cases, using medication. The ability to rely on existing support systems emerged as a key factor in participants’ experiences of psychological recovery. Here, Salma described how feeling cared for and loved by her husband played a significant role in her healing: There was one point when my husband said something really silly, and I started laughing hysterically. And he was like, “oh gosh you haven’t laughed like that since before the baby.” Because that is how we were, just laughing at each other’s silliness, and that completely went away. … And that was a moment I remember, laughter bubbling inside me and just exploding out of me. … I was “oh I haven’t felt like that in two and half years.”
Nunu reflected on the importance of having witnesses during her birth, noting the experience strengthened those relationships, helping alleviate feelings of isolation, guilt, and shame. She explained: He witnessed the pain that I had to undergo, and he said things that helped me recover. … He was saying, “I thought we are a family, but this child is 100% thanks to you. You carried the child, you made the child, all I could do was just sit there and encourage you.” I think that the fact he recognized my efforts and he recognized what had happened, it's helpful, and I do think our relationship has changed. There's more trust.
The validation Nunu received from her midwife also played a pivotal role in reshaping her understanding of the birth. She said: My midwife visited me on day one, day three, day five, and day seven. At every visit she would check in with me and ask me if I was feeling OK, if I needed more help, and if I wanted to hear what had happened. Eventually, she told me what had happened from her perspective and that was so helpful. I think having people witness and then [talk] to me about it made it feel like we are on the same boat.
Being able to ask questions at her own pace helped Nunu move forward while reducing isolation. For Sarah’s healing, strengthening and building a support system with friends was key. She said: I have five really good friends and my nursing friends, there's about eight of us. We're pretty close. And so just having all of them to confide in when things aren't great, and just like having those check-ins—it's huge. Just someone to talk to that is really compassionate and understanding.
While most people discussed strengthening social supports, others sought out professionals. Amy said, “After doing EMDR I really felt a shift in my body, I didn’t feel the same sort of discomfort thinking about it, I could feel a lightness in my body.” For Lynn, who was unable to function six months postpartum, seeing a psychologist and receiving both validation and a formal PTSD diagnosis was an important affirmation. Lynn said, “I also started taking medication which helped a lot because I couldn’t cope.” This experience was echoed by Marie who shared, “I went on medication, and then I upped the medication, and then I upped the medication again, and then I could talk about it.” In both cases, medication served as a supportive tool to engage more fully in therapeutic conversations, facilitating the emotional processing necessary for healing.
Creating Community and Sharing Stories
Sharing stories and creating communities, both online and face-to-face, helped reduce isolation and validate participants’ experiences. Julie said: Starting to talk about it with some of my close friends and having their reactions, which were uniformly like, “wow, I am so sorry that happened to you, that sounds awful.” It wasn’t people being like, “oh yeah, whatever, that’s giving birth, welcome to the real world.” … I felt more confident in telling my story … like I’m able to see myself telling the story but not invalidate my own feelings about it.
Julie shared how witnessing other people sharing their stories in an international Facebook group encouraged her to “break her silence.” She said: Reading those and feeling like “OK there is such a range to experience giving birth” and that kind of everything in it is OK to talk about, maybe not in every circle, but there are safe places that you can share and not feel judged.
The anonymity and being able to witness without sharing were key to Julie’s healing and reduced isolation. For Kate, the online community helped her access support that was unavailable to her locally: “I started writing a lot. I started blogging and learning from other mothers online that I didn’t know, but who were also writing. … Building some of that intellectual community and connecting with other people who had had adverse experiences, I didn’t feel so alone.”
Engaging intellectually and sharing experiences with others who experienced birth trauma online illustrates the value of expanding one-on-one peer support initiatives. It also highlights the importance of recognizing and incorporating additional forms of community support. Marie described how being part of a supportive community facilitated her transition toward healing. She said: “I started to enter the world again.”
Being able to access a group specifically in the afternoon was important for Marie to highlight because the intersection of postpartum depression (PPD), physical disability, and caring for a newborn made attending morning groups feel impossible. Lena described benefits of a postpartum support group, but also the limitations: “I was the only one without a male partner. There were a few bisexual women partnered to men. Like, they would often bring that up and I’m like, OK, cool. But it’s isolating and it’s very different.”
The intersection of identifying as a lesbian and being a single parent by choice represents a significant and often overlooked dimension to healing.
Empowerment as Reframing the Narrative and Returning to Self
Empowerment was experienced as reframing the narrative and self-acceptance. Reframing the narrative involved making sense of what occurred during the birth and shifting blame away from the self. Returning to self encompassed recognizing and accepting personal limitations, self-forgiveness expressing needs and wants, and establishing healthy boundaries. By working with a trauma therapist, Lynn was able to begin to shift her understanding. She said: We went over chunks of time and it helped me break down my thought process of guilt and understanding the trauma in my body and all sorts of things, I couldn’t have done anything in the moment because I wasn’t a healthcare provider at that time, I was in fight or flight … there was too much going. … Changing the narrative through therapy was super helpful, it was the most helpful thing.
Attending psychoeducational workshops helped increase awareness of birth trauma, while also providing participants with opportunities to connect with others with similar experiences. Sarah said: Around eight months is when I really started realizing this was birth trauma, when I attended a workshop with a friend, and I was like, “I have PTSD.” I had all the cardinal signs … The facilitator would flip through the slides and I was like, “Oh, that's me. Oh, that's me. Oh, that's me. Like, this is me.”
Attending this workshop helped Sarah understand her feelings. She was able to identify herself in the information, which subsequently reduced her isolation by normalizing her symptoms of birth trauma. Meanwhile, reframing the narrative has helped Nunu shift over time from a negative to a positive sense of self. Nunu said: For some time I felt like, “OK, maybe my body was not suitable for birth or pregnancy.” I felt like, “oh, maybe if I was taller and larger, then the birth process might be easier.” But now another part that has played into it is also raising the child and seeing the child is healthy and happy … now I see her and my perception has shifted from a more negative perception to, “wow, she's half my size, and I delivered her. This is wonderful. This is incredible.”
For Marie, self-acceptance was linked to her identity as a person with a disability. She said: Sometimes with a disability, you have to be a hero and overcome all the challenges, or you’re worried you’re going to be perceived as a victim. I think in my life I’ve coped with having a very visible difference and disability by being very optimistic. So, I go towards the hero side. I carry that as an individual. I carry that in my life everywhere. A lot of what happened, none of it was positive. I was not a hero at any moment. It’s almost like I had to admit defeat … I think I’m still recovering honestly because I think I’m really accepting what my limitations are.
Self-acceptance was understood in terms of self-awareness and boundaries, as Maddy said: I think being able to talk openly about my birth experience—not just the fact that I have a child who's not alive but actually talking about what birth was like for me and not fearing that it was going to re-traumatize me in having those conversations. Working on knowing when it’s a safe place to have those conversations, because initially my brain was like, “well, I'm going to talk about it and I'm going to rah, rah, rah make something of this.” And I think as I'm journeying further in this, just knowing when that's helpful for me and when it's not, so even answering around how many children I have, to me that's tied to my birth trauma … I used to feel this obligation to be like, “I have two children” and now I think I've accepted the safety [of] not everyone having to know my full story all the time.
Julie further reflected on how her identity as a Korean American and an adoptee contributed to her self-belief and her ability to move forward. She said: What had happened right before my son was born was George Floyd was murdered and everybody discovered racism existed for the first time. And that was a really hard time for me because people were discovering that anti-Black racism existed, but in general, it was a general awakening for racialized people. So for me, I had a big racial awakening where I became the most secure in my identity as an Asian woman and as a racialized person. Because I remember in 2015, I had, friends who were people of colour, Black, Asian, brown, etc. And they were like, “Hey, do you consider yourself a person of colour?” And I immediately was like, “no. I don't, like I'm Asian, but I don't consider myself a person of colour.” By the time 2021 rolled around, I definitely felt like I was, and I felt like there [were] people who were able to voice stories of resilience in a way that I had never been able to tell for myself. Like, they were giving voice—there [was] a lot of anti-Asian violence, and I felt like there was a community to lean-on. The weight of being a person of color in western society is exhausting. So in that way, I felt like I had come out kind of on the other side of it, feeling proud of my resilience. That there was a community that my identity could speak to, I felt like a part of a community in a way that I never felt like I was allowed to be a part of it before. This is a long way to say that I actually do think my identity played a role in my healing because even though I don't think the incident happened to me because I was racialized, I think, the skills that I had built from my journey of discovery had put me in a place to feel more confident in my own feelings and confident in my own ability to persevere. And then, as an adoptee, I feel like, I've survived all this other stuff. I know I can handle it because I've handled so many other things.
Kate also experienced healing as the ability to take care of oneself and the confidence to meet your own needs and not trust the systems. She said: I will ask my doctors questions. I will do my research ahead of time. I will look up whatever drugs I'm on to find out what are the side effects and the various interplay between many things. I would say I experienced healing as overall confidence. Because I had to.
Kate’s experience reflects a shift from disempowerment to empowerment, marked by the loss of trust in the healthcare system that contributed to the original trauma.
Giving Birth Again
Giving birth again provided many participants with an opportunity to regain a sense of control over their birthing experiences. For most, the act of giving birth again was healing regardless of whether it aligned with their expectations. The healing process was facilitated through experiences of self-advocacy, regained autonomy, and receiving client-centered, compassionate care. As Marie said: I think going through it a second time was part of what was pivotal to my healing because I was able to repave a lot of those traumatic memories with new ones with different experiences, like the C-section was completely different. I was ready. It was calm. It was chill. I felt happy. I had my baby. I could latch him and nurse him right away. I had all the support there for me when I got home because I knew what I would need.
Feeling prepared by planning was a key factor for Marie. Regaining control was experienced as being in charge and centered during birth. Salma said: I feel like giving birth again was ultimately where the healing took place. I felt like this is my birth! I never felt that the first time around … it was happening to me the first time around. Second time around, I was making it happen … I felt in charge.
Many individuals with birth trauma experience feeling out of control of their own birth. Making it happen and self-advocacy was accepting and understanding “the system will not take care of you.” Sarah said: I’d be like, “So these are my worries. My worry is I’m gonna go into labour [planning an elective caesarean section].” The doctors are like, “don’t worry, like, that won't happen.” And I’m like, “you don’t get it.” After that appointment, I went home to my husband and I said, “they don’t think that anything’s gonna happen again. And it might not, but if it does, no one’s prepared for it.” So he’s like, “what do we do?” I was like, “we make a plan. We make a plan if something happens to me, what we do. We make a plan if something happens to a baby, what we do. And we make a plan if like, there’s something happens to me and the baby, what do we do?”
This shift to self-advocacy gave Sarah power back, making her in control “in case” plans do not go as intended. Planning for the worst-case scenario was highlighted by most participants who gave birth again; it made people feel more in control.
For some people like Kate, unexpected birth trauma continued postpartum, where she experienced substantial breastfeeding issues. She said, “We had a plan ahead of time. If this happens and that happens with the nursing, we’re going to call it. So, we ended up transitioning my second child to formula in two weeks instead of three months. Because we figured, if the baby’s losing weight and has failure to thrive, then maybe it's not so much about the lactation.” Planning meant avoiding adverse impacts on the baby and the participant’s mental health. Many participants chose to undergo an elective caesarean section, and for most, it was a way of controlling their births and avoiding perineal recovery. Kate said: I remember talking to my GP at the beginning when I was just first pregnant, I'm like, “can I get a planned C-section?” He's like, “you'll have to talk to this person about that.” “Can I get a planned C-section? Can I get a planned C-section?” Very determined. I didn't fear labour, not at all. In fact, I think I would have had a much better labour second time around and would have had my choices hopefully more in my control. It was just, I didn't want to have to take five months to recover again.
Experiencing client-centered care was a major component of participants’ recovery. Being listened to by care providers and validated in their previous experiences helped create trust and lead to healing. Irene said, “Our OB had said, like, ‘I’ll do whatever you want to do. If you want to be nowhere near a hospital, I can give you a list of people that’ll help you do it at home’ and he was really generous and shared that they had had a stillbirth and shared his family’s story as to how they got to where they are.” This disclosure reduced Irene’s sense of isolation, strengthened the therapeutic alliance, and positioned her firmly at the center of decision-making about her care.
For Sarah, whose second birth was more medically complex and life-threatening, finally being seen and listened to by healthcare providers shifted the feeling of trauma from her first birth. Sarah said: The doctor came over and I was like kind of delusional and she was like, “I might have to do a hysterectomy,” and I was like, “I'm not ready for that.” She's like, “it's either that or it's no you, so you have to decide.” And she's like, “I think it's a good idea, because I think it's important that we try to, to get you through this.” And I was like, “OK.”
This shift from birth being something “done to you” to an experience “shared with you” reinstated a sense of agency and connection to Sarah’s birthing process.
Healing Through Time
Participants consistently described healing from birth trauma as a nonlinear, evolving process with no definitive endpoint. Participants articulated healing as comprising multiple moments of insight and clarity. Many reported gaining a clearer understanding of their experiences and their impact over time. For some, specific moments marked a noticeable shift in which they recognized healing was occurring. Healing takes a long time, as Amy said: I think being a midwife is also a unique experience dealing with birth trauma because you don't know when you'll be triggered … you're constantly reminded of it. I still feel like I’m healing, there's probably still a little bit more I could do, but I think that's more just around my own body image, which I feel like is lifelong.
Even those who had experienced healing from birth trauma were in a constant state of healing. Marie discussed the process of acknowledging, addressing, and recovering from trauma: It took a long time for me to realize all this stuff happened. And then it took a long time for it all to hit me—four months postpartum and it all hit me finally. And then it was this long process to recover.
Time was essential for recovery. Sarah emphasized healing as a process that unfolded gradually. She said: I remember being in the hospital bed after everything had happened and thinking for the first time, “you've done everything, you couldn't have done anything more. This was your all.” So that was the first step. … I remember going to see my doctor after a month of work. My family doctor was just like, “I’m so proud of you.” He said, “most people just probably wouldn't do what you've done.” He's like, “there are some people who just don't have the fight.” I think it's probably like that. I don't know. Is it healing? I don't know, but it was that first moment where I was like “It's gonna be OK.” … It's been a long road, but I think I've been healing the whole time and I feel like I've been making progress.
A pivotal healing point highlighted by participants who gave birth again included when they realized they wanted to have another baby. Salma said: Time healed … it came back just gently over time. And that's when, and all of a sudden, we’re like, “Hey, let’s have another baby.” And the funny thing is, I thought, “Oh, I'm good.” I'm over the trauma of my first birth. Everything's good, right? Like I am ready to try for an unmedicated birth. I'm going back in.
Healing as a process is reflected in Salma’s experience of gently returning to herself through identifiable moments that marked the beginning of healing. These moments gradually accumulated, leading to a sense of readiness to give birth again.
Participants described healing as gaining clarity about their needs and boundaries about aspects of their birth experience that may remain unresolved or difficult to process, knowing what they were willing to engage with and what they wished to avoid. Kate said: There are milestones of healing. Healing? Yes. Healed? No. Not even physically. … But when I embraced the idea of having another baby, when I was able to have another pregnancy and find joy in it, not fear, I think I was healed—or healed enough at that point that I was able to joyfully move forward into new risk and new possibility.
Discussion
After a traumatic birth, participants sought support from their communities. A supportive partner, family member, or friend is an important element in healing. Attard et al. (2022) demonstrated that birthing people felt like they recovered better when the experience of birth trauma was shared among partners. Having someone who witnessed the birth and was then able to validate and support them in the postpartum period was highlighted by many of the participants. Conversely, having an unsupportive partner or family member discredited the experience and increased isolation and shame. A trauma survivor’s ability to be seen, heard, and validated in their experience can be a factor in the development of PTSD (Herman, 2015; Van der Kolk, 2015).
Encouraging healthcare providers helped participants like Nunu feel validated and supported postpartum, notably through client-centered and continuous care. In Elmir et al. (2010), participants quoted client-centered care as the most important aspect to prevent birth trauma. Additionally, Horan et al. (2022) demonstrated the use of a trauma-informed care model and interprofessional collaboration to help people heal from birth trauma. Despite this research being based on one case study, the importance of client-led care and continuity of care in all areas of perinatal care remains. Within a feminist trauma framework, Brown (2018) discussed the importance of building trust and moving at the client’s pace when talking about and processing trauma.
Some participants sought psychological support and medication, which they found to be key elements of their healing. Specifically, the need for therapy focused on PTS was emphasized. While traumatic births are associated with increased rates of PPD and anxiety, these mental health outcomes must also be understood in relation to the broader context of birth trauma itself (Ayers, 2014; Türkmen et al., 2021). This means validating and recognizing the role of traumatic birth in postpartum mental health presentations (Polmanteer et al., 2019).
A systematic review conducted in 2021 examined the effectiveness of early interventions delivered by midwives or psychologists (within 72 h postpartum) on the development of a PTSD diagnosis versus standard care. The review concluded that early trauma intervention reduced PTSD symptoms up to 12 weeks postpartum (2021). However, an additional meta-analysis (Shorey et al., 2023) revealed that psychological interventions were effective at reducing “fear of childbirth,” but they were not as effective at reducing postpartum anxiety and depression following a traumatic childbirth. In addition, trauma-focused interventions such as eye movement desensitization and reprocessing (EMDR) that Amy cited as major component in her healing have shown significant reductions in postpartum and PTS symptoms, such as flashbacks and intrusive thoughts, without readmission at both 6 and 12 weeks when compared to the usual treatment group (Chiorino et al., 2020).
From a feminist trauma perspective, creating a community and sharing stories within communities are vital components of healing from trauma. Herman considers this to be the second stage of recovery, called “reconstructing the story” (Herman, 2015). Psychotherapists also discuss the importance of creating a story and telling it in therapeutic work for those with birth trauma (Gough & Giannouli, 2020). In a study on survivors of sexual violence, Tseris (2019b) emphasized that while psychological interventions were often beneficial in helping participants reframe their experiences, these interventions alone did not alleviate feelings of isolation. Instead, the study found that incorporating a feminist trauma approach, which actively encourages survivors to engage with others in a supportive community, was crucial. Every participant in this study discussed the importance of creating and connecting with communities, whether online or in-person, to reduce isolation.
Participants highlighted the need to connect with communities that share similar lived identities, underscoring the importance of support groups tailored to individuals’ intersectional identities. Such spaces acknowledge how identities and systemic oppression shape experiences of trauma and recovery. Both communities and academics (Ahmed, 2012; Blackwell, 2018; Lorde & Clarke, 2007) emphasize the necessity of dedicated spaces such as Black, Indigenous, and Racialized spaces, Queer spaces, and Disabled-only spaces for collective healing and validation. Participants in Parmenter et al.’s (2025) IPA research on Black, Indigenous and Racialized People, Queer, and Trans healing emphasized the value of intersectional healing spaces that foster belonging, empowerment, and mutual support.
Storytelling and story-listening helped to alleviate feelings of isolation by fostering solidarity and providing validation through interactions that not only normalized participants’ experiences but also contributed to broader awareness and recognition of birth trauma as a legitimate and shared phenomenon. Sharing stories within online and in-person communities has been shown to have a positive effect, helping people construct the narrative, seek validation, and support others who have experienced similar traumatic births (Blainey & Slade, 2015; Brammer, 2014). A random control trial (Di Blasio et al., 2015) demonstrated that purposeful journaling about the individual’s deepest feelings and thoughts regarding their birth can alleviate PTS symptoms.
In this study, becoming empowered meant reframing narratives of their birth and returning to self. These elements shape people’s experiences of healing from birth trauma. The goal of feminist counselling is client empowerment and raised consciousness (L.Brown, 2018). According to feminist trauma therapists, Tseris (2019b) and Herman (1992), becoming empowered means to overcome internalized oppression, such as negative beliefs, attitudes, or limitations, and gain psychological strength to confront and resist external barriers from various sources, such as family, society, and institutions. Previous research has examined posttraumatic growth following traumatic childbirth (Beck & Watson, 2016; Ketley et al., 2024; Sawyer & Ayers, 2009). Similarly to Ketley et al. (2024), participants in the study reconceptualized their experiences in ways that shifted narratives of weakness. Becoming empowered and feeling resilient was also emphasized by Beck and Watson (2016), who found that women who experienced posttraumatic growth felt “unbreakable.” Feeling empowered to create boundaries and identify needs in all realms of life was also identified in a research project on resilience following childbirth (A. Brown, 2018). Brown found that resiliency following traumatic birth was often expressed as being able to identify needs and communicate those needs to healthcare providers as well as other people in their lives. Importantly, for some, this meant accepting limitations and rejecting internalized oppression, such as ableism. Reclaiming birth as a pathway to healing from birth trauma is particularly emphasized in research focusing on Indigenous and Black communities (Cidro et al., 2018, 2020; Rhodes, 2022; Suarez, 2020). This work highlights the importance of supporting Indigenous and Black birth workers and returning birth to community contexts as acts of resistance and healing.
Giving birth again was considered a major component of healing for those participants who did give birth again. Previous studies have found that positive birth experiences are often healing experiences following a traumatic birth (Beck et al., 2018; Wahlbeck et al., 2018). Further, collaborative care between healthcare providers and birthing persons can lead to an empowering and healing future birth experience (Horan et al., 2022). The positive impacts of subsequent birthing experiences are discussed in autoethnographic (Scuro, 2018) and phenomenological research (Thompson, 2021). Similarly, participants in those two studies expressed that the experience of giving birth provided them with an understanding of how to advocate and create an alternative birthing experience. They sought supportive care providers and created a birth plan which addressed their previous traumatic experience (Scuro, 2018). Importantly, people experienced their birth as healing regardless of whether it met their expectations. Despite the mode of delivery, being centered during the birth and communicated to in a transparent, direct manner made people feel like the birth was happening with them versus to them.
The role of time in healing from birth trauma has not been explicitly addressed in the existing literature. While many individuals experience PTS symptoms following childbirth, only a small proportion (approximately 4%) go on to develop PTSD (Ayers et al., 2018). This may suggest that distance from the traumatic event may mitigate symptoms and facilitate recovery. For most participants, they discussed healing as a long process experienced in stages, with moments in which they realized they were moving forward. This is consistent with Herman’s (2015), Trauma and Recovery, conceptualizing trauma recovery as occurring in stages. As participants gained distance from the traumatic event, they moved through different phases of recovery and their understanding of what constituted healing shifted. This suggests their current interpretations of healing may continue to evolve. Time can provide a critical opportunity for reflection, meaning-making, and adaptive action.
Limitations
As in most phenomenological studies, small sample size is often cited as a limitation to phenomenological research (Tuffour, 2017). While IPA does not seek to generalize findings, the number of participants may limit the transferability of findings to broader research on birth trauma recovery. Additionally, phenomenological research involves the interpretation of participants’ experiences through the lens of the researcher. This interpretative process, while central to IPA, introduces the possibility that the analysis may not fully align with participants’ intended meanings and is shaped by the researcher’s own perspectives. Future studies could benefit from involving a more diverse team of researchers in participant recruitment, interviewing, and data analysis.
This study was guided by intersectional feminist trauma theory, which understands trauma as defined by the individual and recognizes people as resilient and capable of recovery. This framework allows for a broader range of lived experiences to be acknowledged and centered. While this inclusivity is a strength, it also represents a limitation. The study did not use DSM-5 definitions or clinical diagnostic criteria to define trauma or trauma recovery, nor did it restrict participation based on DSM-5 thresholds. Although many of the participants would likely meet criteria for PTS or PTSD, the absence of clinical diagnostic measures may raise questions regarding clinical legitimacy from a biomedical perspective.
Conclusion and Clinical Implications for Practice
The purpose of this study was to understand how people experience healing from birth trauma using an IPA approach. Healing is often complex, can be multifaceted, and may change with time. To date, much of the existing research on birth trauma recovery has prioritized individual expert-led interventions. This study suggests that, while psychological intervention is sometimes accessed, sharing stories, creating a community, and strengthening support systems over time are key components in moving forward. This perspective can challenge the limitations of biomedical models by expanding recovery approaches that integrate informal peer-led and community approaches. Integrating the lived experiences of those recovering from birth trauma is essential for the development of client-centered programs and services. This includes the incorporation of peer-led support initiatives that can mitigate isolation and foster a community among those with birth trauma. Additionally, validation and empathetic engagement from partners, support people, and healthcare providers play a crucial role in facilitating recovery following traumatic birth.
Footnotes
Acknowledgements
The research project acknowledges the PhD research committee that provided technical assistance and general feedback: Dr. Patricia McGuire, Dr. Nimo Bokore, and Dr. Ivy Bourgeault.
Ethical Considerations
This study was approved by Carleton University Research Ethics Board-A (Approval Number: 121178).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.